chemotherapy in anal cancer ?lessons for vulva anzgog 2013 michelle vaughan
TRANSCRIPT
Chemotherapy in Anal cancer?Lessons for vulva
ANZGOG 2013Michelle Vaughan
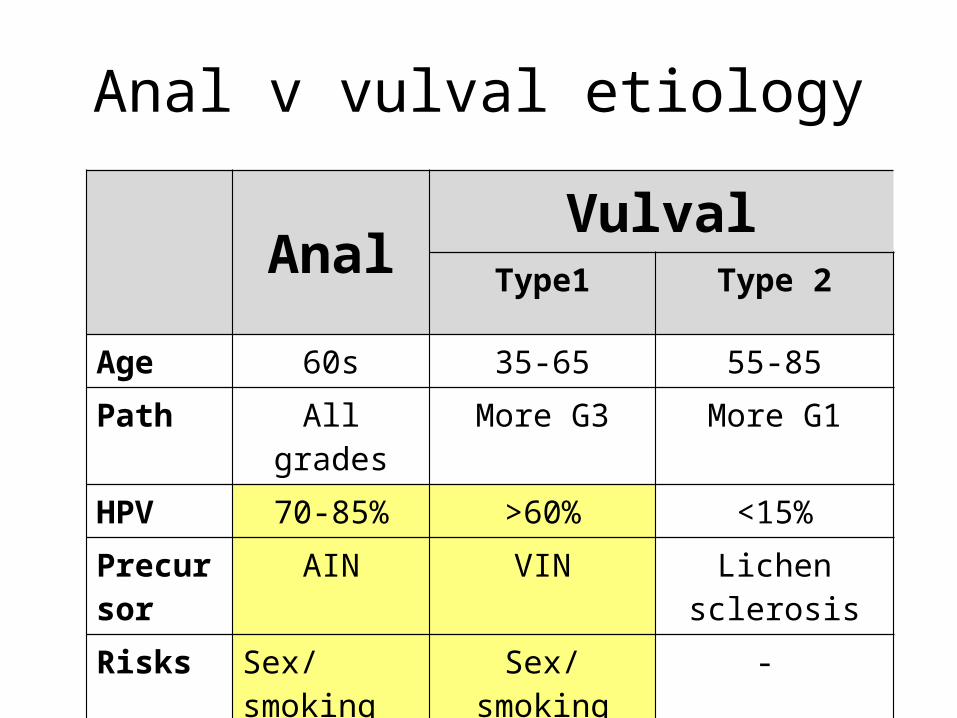
Anal v vulval etiology
Anal VulvalType1 Type 2
Age 60s 35-65 55-85Path All grades More G3 More G1HPV 70-85% >60% <15%Precursor
AIN VIN Lichen sclerosis
Risks Sex/smoking Sex/smoking -
VULVAL & ANAL CANCER
LOCAL CONTROL is dominant aim of treatmentIndolent natural historyMets are rare (<10% as a 1st event)Chemo given to help RT with local control
(Uncommon paradigm for chemotherapists!)
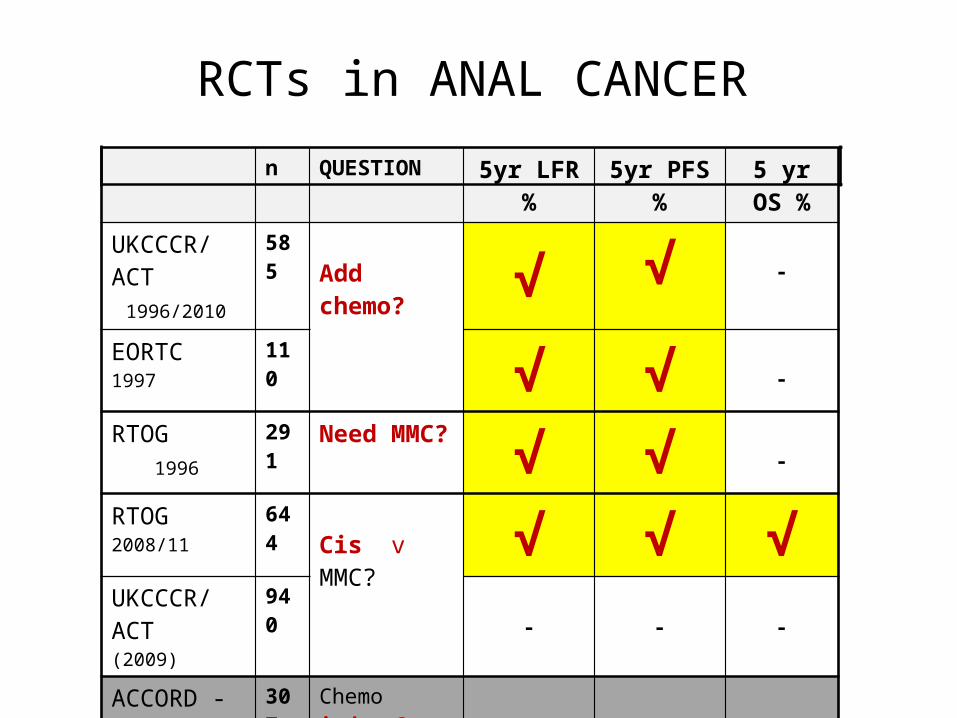
RCTs in ANAL CANCERn QUESTION 5yr LFR % 5yr PFS % 5 yr OS %
UKCCCR/ACT 1996/2010
585Add chemo? √ √ -
EORTC 1997
110 √ √ -
RTOG 1996
291 Need MMC? √ √ -
RTOG 2008/11 644Cis v MMC? √ √ √
UKCCCR/ACT(2009)
940- - -
ACCORD -03 307 Chemo induct?HD RT? - - -
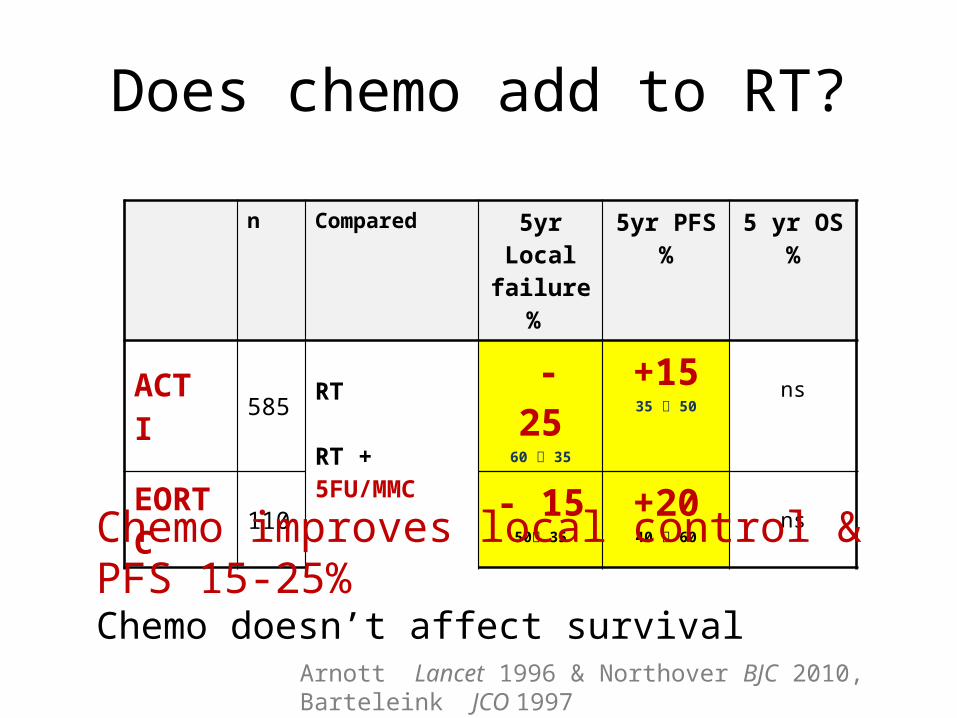
Does chemo add to RT?
n Compared 5yr Local failure %
5yr PFS % 5 yr OS %
ACT I 585 RT
RT + 5FU/MMC
- 2560 35
+1535 50
ns
EORTC 110- 15
50 35
+2040 60
ns
Arnott Lancet 1996 & Northover BJC 2010, Barteleink JCO 1997
Chemo improves local control & PFS 15-25%Chemo doesn’t affect survival
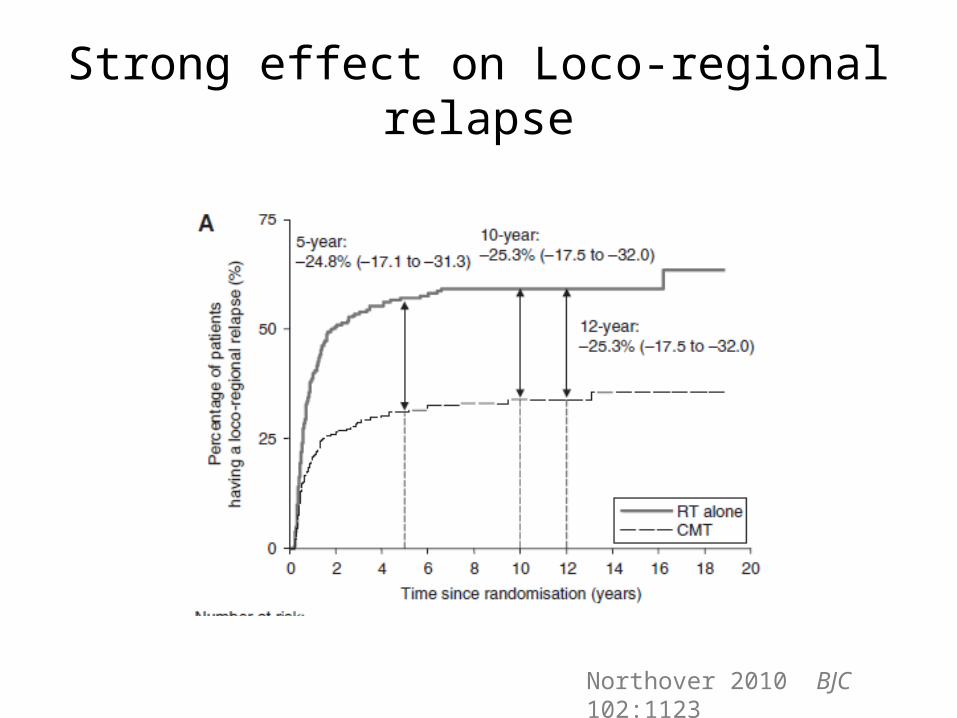
Strong effect on Loco-regional relapse
Northover 2010 BJC 102:1123
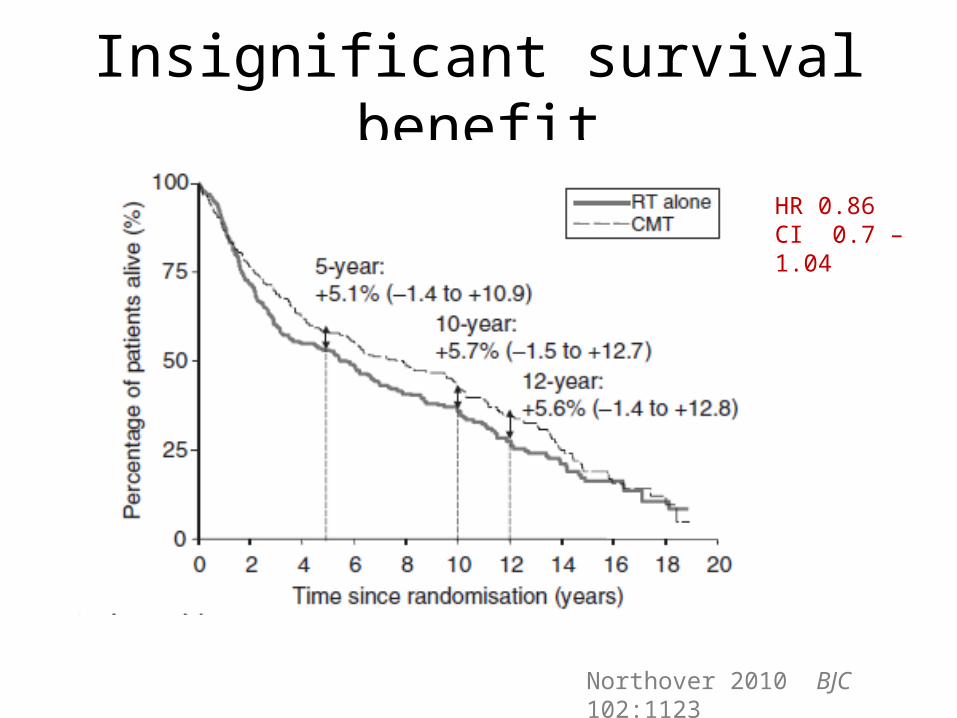
Insignificant survival benefit
HR 0.86 CI 0.7 – 1.04
Northover 2010 BJC 102:1123
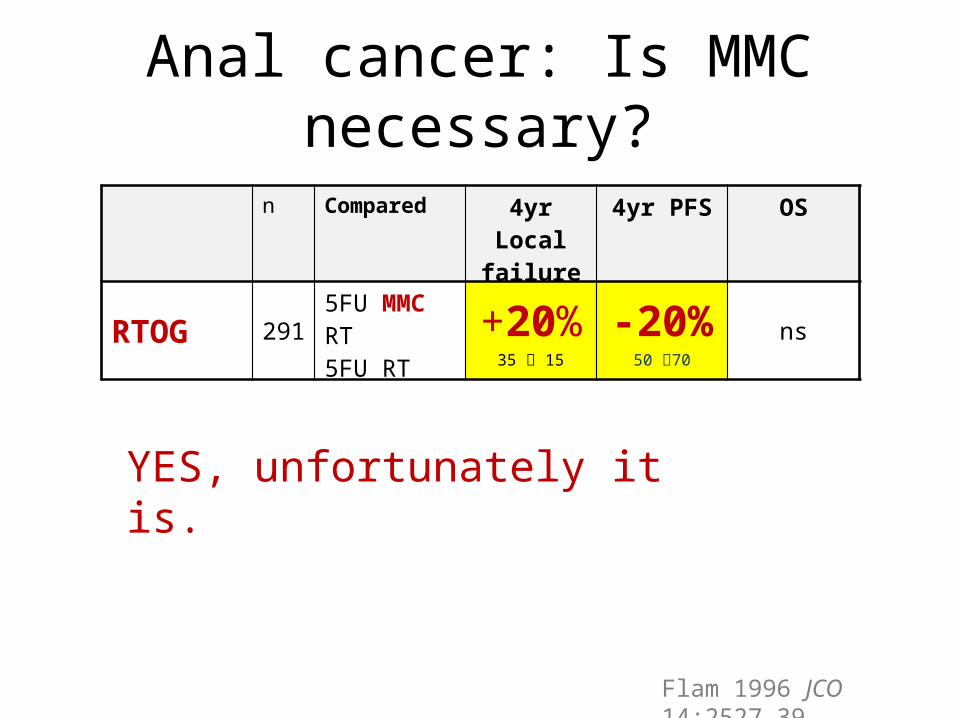
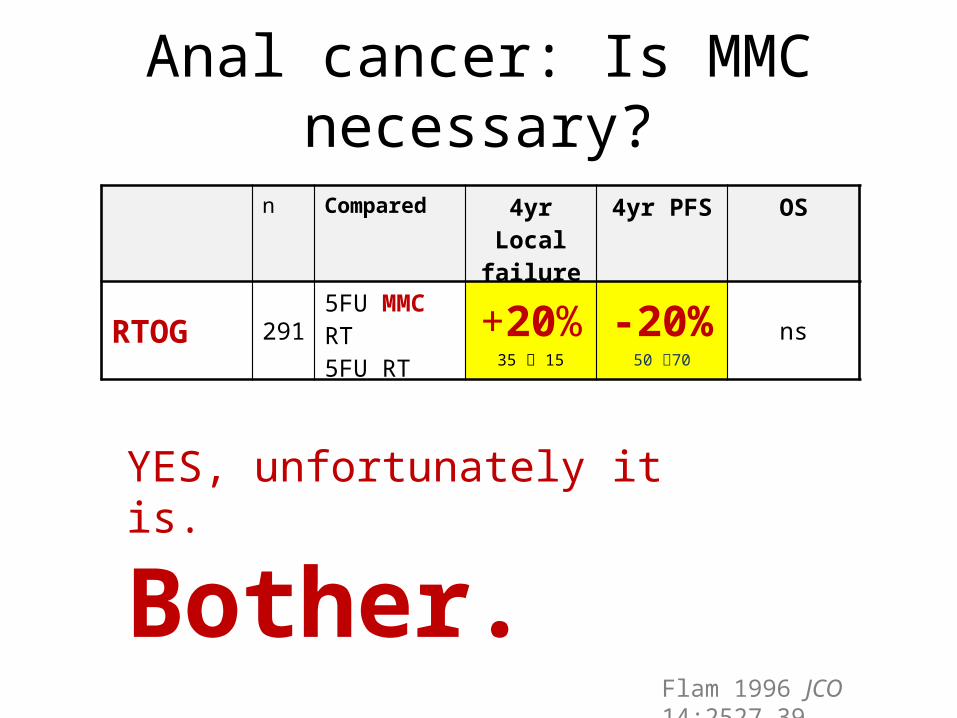
Anal cancer: Is MMC necessary?
YES, unfortunately it is.
Flam 1996 JCO 14:2527-39
n Compared 4yr Local failure
4yr PFS OS
RTOG 291 5FU MMC RT5FU RT
+20%35 15
-20%50 70
ns
Anal cancer: Is MMC necessary?
YES, unfortunately it is.
Bother.
Flam 1996 JCO 14:2527-39
n Compared 4yr Local failure
4yr PFS OS
RTOG 291 5FU MMC RT5FU RT
+20%35 15
-20%50 70
ns
MMC is toxic
…So can we replace it?
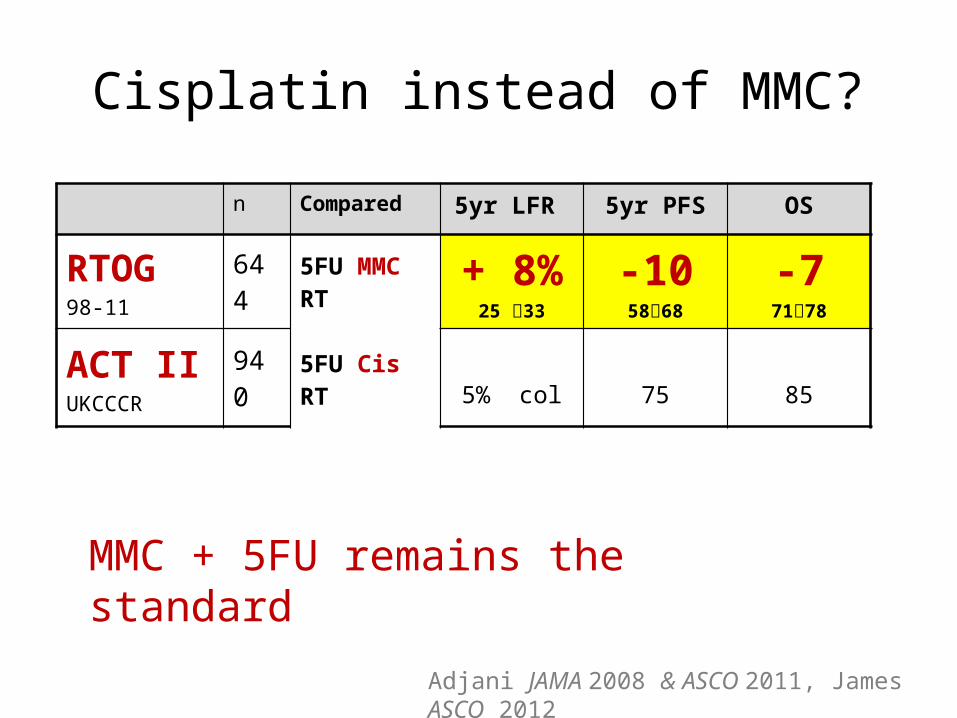
Cisplatin instead of MMC?
MMC + 5FU remains the standard
n Compared 5yr LFR 5yr PFS OS
RTOG 98-11
6445FU MMC RT
5FU Cis RT
+ 8%25 33
-105868
-77178
ACT IIUKCCCR
940 5% col 75 85
Adjani JAMA 2008 & ASCO 2011, James ASCO 2012
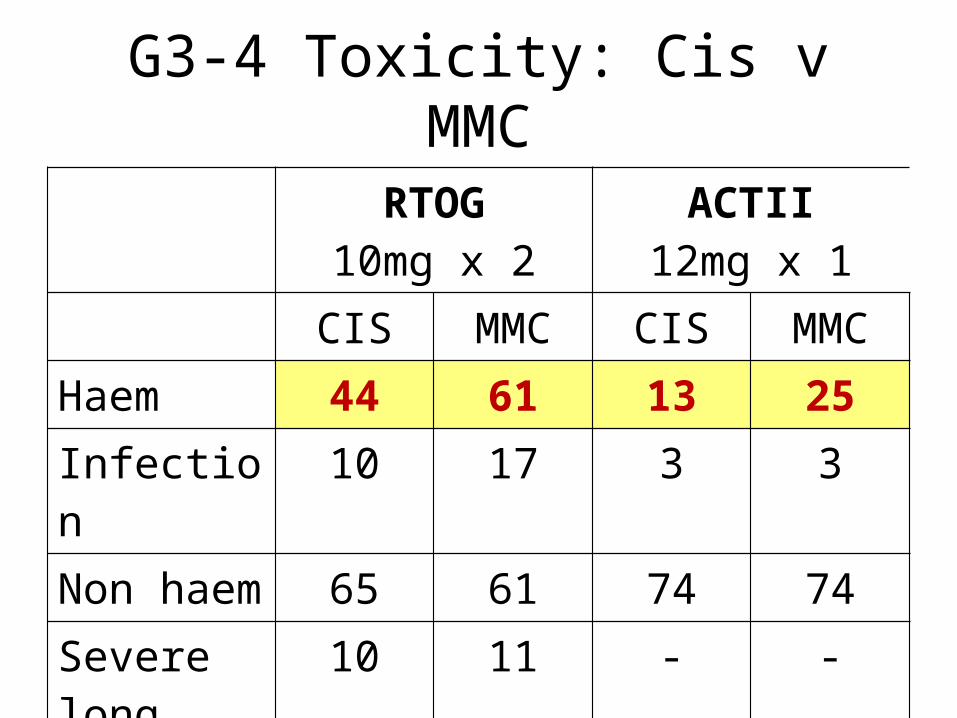
G3-4 Toxicity: Cis v MMC
RTOG10mg x 2
ACTII12mg x 1
CIS MMC CIS MMCHaem 44 61 13 25Infection 10 17 3 3Non haem 65 61 74 74Severe long 10 11 - -

Can we reduce the MMC dose?Dose Haem tox G 3-4
RTOG 10mg/m2 D1 + 29 61%
UKCCCR ACT II 12mg/m2 D1 25%
TOXICITY: Better with D1 only mitomycinEFFICACY???: Who knows?
So, What MMC dose?
• We will never know• Either is reasonable• If you use the RTOG 10mg/m2 D1 & D29
remember to: – Do weekly FBC– Dose reduce if nadirs wcc < 2.4!
SUMMARY
Anal cancer is similar to Vulval cancer
In anal cancer several large RCTS say:- Chemo adds PFS to RT- MMC adds PFS to 5FU chemo- MMC is better than cisplatin in 1 of 2 trials- More haem tox
?Argue for 5FU/MMC

thank you
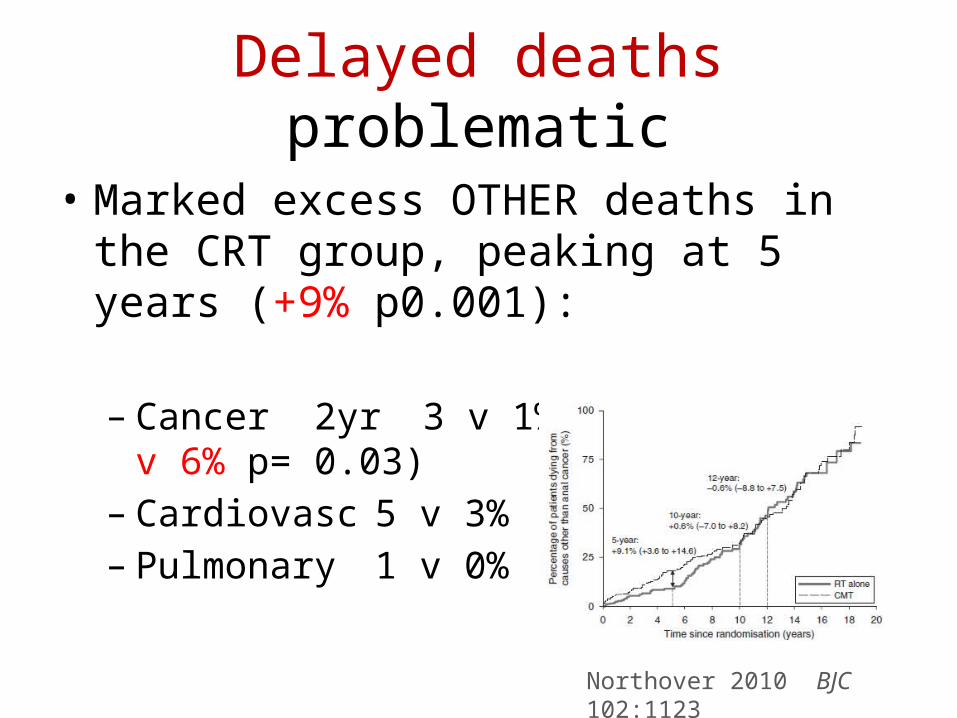
Delayed deaths problematic
• Marked excess OTHER deaths in the CRT group, peaking at 5 years (+9% p0.001):
– Cancer 2yr 3 v 1% (13yr =12 v 6% p= 0.03)– Cardiovasc 5 v 3%– Pulmonary 1 v 0%
Northover 2010 BJC 102:1123
Details of excess deaths:
• Cardiovascular– Spread in time course, median time about 1 year
• Second cancers - Mostly lung cancer (reflecting shared etiology), 8 v 2 in 1st 5 years, 26 v 16 after 5 years
SO: Late (+ acute) chemo toxicity possibly cancelling out survival benefit from reduction in anal cancer death in this population
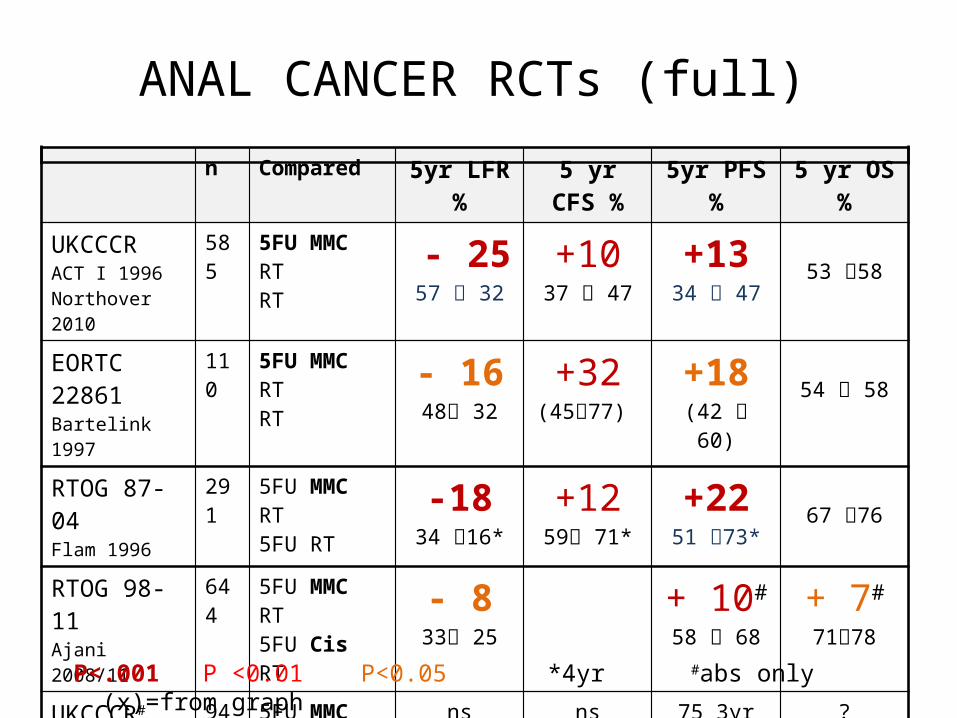
ANAL CANCER RCTs (full)n Compared 5yr LFR % 5 yr CFS % 5yr PFS % 5 yr OS %
UKCCCRACT I 1996 Northover 2010
585 5FU MMC RTRT - 25
57 32+1037 47
+1334 47
53 58
EORTC 22861Bartelink 1997
110 5FU MMC RTRT - 16
48 32+32
(4577) +18
(42 60)54 58
RTOG 87-04Flam 1996
291 5FU MMC RT5FU RT -18
34 16*+12
59 71*+22
51 73*67 76
RTOG 98-11Ajani 2008/11
644 5FU MMC RT5FU Cis RT - 8
33 25+ 10#
58 68+ 7#
7178
UKCCCR#
ACT II 2009940 5FU MMC RT
5FU Cis RTns ns 75 3yr ?
ACCORD-03#
Conroy 2009307 5FU Cis induct
HD RT28 83 70 78
P<.001 P <0.01 P<0.05 *4yr #abs only (x)=from graph