characteristics of vulnerable plaque: structural ... · • unstable angina pectoris ... lp nc nc...
TRANSCRIPT

Characteristics of Vulnerable Characteristics of Vulnerable Plaque: Structural Observations Plaque: Structural Observations and Natural History Insights from and Natural History Insights from
the Core Pathology Laboratorythe Core Pathology Laboratory
2323rdrd AprilApril, , 20082008
Renu Virmani, MDCVPath Institute Inc., 19 Firstfield Road,
Gaithersburg,Maryland, USA
Conflict of Interest StatementWithin the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below.
Physician Name: Renu Virmani, M.D.
Company/Relationship:Research GrantsMedtronic AVE; Guidant; Abbott; GE Healthcare; Takeda; Atrium Medical Corp.; ev3; Conor Medsystems; TopSpin Medical (Israel) Ltd.; Paracor Medical, Inc.; OrbusNeich; Terumo Corp.; Vascular Therapies, LLC; CardioKinetix; Osiris Therapeutics, Inc.; Edwards Life Sciences; Biomerix; Nitinol Device and Components; Sorin Biomedica Cardio S.r.l; 3F Therapeutics; Hancock Jaffee Labs, Inc.; Cardiovascular Device Design; Coaptus; Biotegra; Cardica, Inc.; Cordis Corp.; Cryo Vascular Systems, Inc.; CVRx, Inc.; diaDexus, Inc.; InfraReDx, Inc.; Kensey Nash Corp.; Medeikon Corp.; MedNova USA, Inc.; Microvention, Inc.; Oregon Medical Laser Center; Spectranetics Corp.; Takeda Pharmaceuticals North America; Toray Industries, Inc.; Vascular Concepts; Volcano Therapeutics, Inc.; BioSensors International; Alchimer S.A. and Relisys.
Consultant: Medtronic AVE; Guidant; W.L. Gore; CryoVascular Systems, Inc.; Volcano Therapeutics Inc.; Precient Medical; Medeikon; CardioMind, Inc.; Direct Flow; and Atrium Medical Corp.
Employment 25%: Cardiovascular Research FoundationDo not own any stock in any company.
Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below.
Physician Name: Renu Virmani, M.D.
Company/Relationship:Research GrantsMedtronic AVE; Guidant; Abbott; GE Healthcare; Takeda; Atrium Medical Corp.; ev3; Conor Medsystems; TopSpin Medical (Israel) Ltd.; Paracor Medical, Inc.; OrbusNeich; Terumo Corp.; Vascular Therapies, LLC; CardioKinetix; Osiris Therapeutics, Inc.; Edwards Life Sciences; Biomerix; Nitinol Device and Components; Sorin Biomedica Cardio S.r.l; 3F Therapeutics; Hancock Jaffee Labs, Inc.; Cardiovascular Device Design; Coaptus; Biotegra; Cardica, Inc.; Cordis Corp.; Cryo Vascular Systems, Inc.; CVRx, Inc.; diaDexus, Inc.; InfraReDx, Inc.; Kensey Nash Corp.; Medeikon Corp.; MedNova USA, Inc.; Microvention, Inc.; Oregon Medical Laser Center; Spectranetics Corp.; Takeda Pharmaceuticals North America; Toray Industries, Inc.; Vascular Concepts; Volcano Therapeutics, Inc.; BioSensors International; Alchimer S.A. and Relisys.
Consultant: Medtronic AVE; Guidant; W.L. Gore; CryoVascular Systems, Inc.; Volcano Therapeutics Inc.; Precient Medical; Medeikon; CardioMind, Inc.; Direct Flow; and Atrium Medical Corp.
Employment 25%: Cardiovascular Research FoundationDo not own any stock in any company.

Natural History of Atherosclerosis
• Systemic factors - hyperlipidemia, diabetes mellitus, smoking, hypertension, age and sex, hsCRP, Lp-PLA2, etc.
• Local factors: at branch points, e.g., carotid bifurcation, abdominal aorta just above bifurcation coronary branch point, and arch vessels at take off, are the sites of atherosclerosis manifestation
• Thrombosis occurs in the coronary arteries at focal points and is most often seen in the proximal segments of the three main coronary arteries (systemic coagulation factors play a role), and occur at sites where there are underlying plaque characteristic that result in thrombosis

Branch points are the sites of atherosclerosis and occur in areas of low shear
A
Carotid ArteryLeft Coronary arteryC
Low shear
High shearBlood flow

Lesions with ThrombiLesions with Thrombi
• Plaque Rupture• Plaque Erosion• Calcified Nodule

Causes of Coronary ThrombosisCauses of Coronary Thrombosis
Calcified noduleCalcified noduleErosionErosion
ThTh NC
CalcifiedNodule
FC
RuptureRupture
Th
RuptureSiteNC
Th
Th
Th Th Th
Virmani R, et al. Arterioscler Thromb Vasc Biol 2000;20:1262

MΦ
T cells SMCs
HLA-DR
ThTh
NC
A
B
Th
NC Gross and Light MicroscopicFeatures of Plaque Rupture
60% of Thrombi in Sudden Coronary Death occur form Plaque Rupture
E
D
G
F
C
Th
NC
Fig 3-1

Plaque Erosion: 30-35% of thrombi in SCDPlaque erosion in a 33 year-old female complaining of chest pain for two-weeks and discharged from the emergencyroom with a diagnoses of anxiety.
A
E
C
D FMΦ
T-cells PLT Fibrin
NC
B
SMCs

Necrotic core
Th
Lumen
Th
Lumen
Plaque rupture Plaque erosion Calcified noduleCalcified nodule
Clinical and Morphologic Difference in Plaques Associated Clinical and Morphologic Difference in Plaques Associated with Luminal Thrombiwith Luminal Thrombi
ThTh
60% thrombi in SCDM>F, Older, Ca++
Eccentric = concentricGreater % stenosisMacs, T cells,HLADr
30-35% thrombi in SCDM=F, youngerUsually eccentricLesser % stenosisSMC rich, proteoglycans
2-7% thrombi in SCD, calcified platesM>F, older, mid RCAUsually eccentricStenosis variableNodules of bone

Acute Coronary SyndromeAcute Coronary Syndrome• Acute Myocardial Infarction
– >90% have coronary thrombi, usually occlusive– 65-75% from plaque rupture– 25-35% from plaque erosion (Arbustini E, et al. Heart 1999)
• Unstable Angina Pectoris– 70% have thrombi, mostly non-occulsive (Mizuno K, et al. Lancet
1991. Ueda Y et al. JACC 1996) – Distribution weather rupture or erosion, unknown
• Sudden Coronary Death– 60% have thrombi- 60% rupture, 35% erosion, 2-5% calcified
nodule)– 40% have stable plaques with >75% x-sectional narrowing (no
thrombus)– 40% have HMI and 15% AMI (Virmani R, et al. ATVB 2000

Development of Human Coronary AtherosclerosisPathologicintimal thickening
Fibrouscap atheroma
Thin-capFibroatheroma
IntimalIntimalthickening
IntimalIntimalxanthomathickening xanthoma
LP NCNC
FC
Extracellular lipid
Necrotic coreCholesterol clefts
Calcified plaque
Healed thrombus
Macrophage foam cells HemorrhageThrombus
Smooth muscle cells
Collagen
FC = fibrous capLP = lipid pool NC = necrotic core

Thin-Cap Atheroma (Vulnerable Plaque) Components
• Necrotic core• Thin fibrous cap (< 65 µm)• Cap infiltrated by macrophages and
lymphocytes• Cap composition – type 1 collagen and
few smooth muscle cells

Thin cap Fibroatheroma (Vulnerable Plaque)
AA AB
Movat
nc
nc
Fibrous cap CD68
nc
AC
AE AF
vWFCD68
AD

Morphologic Characteristics of Plaque Rupture and Thin-cap Fibroatheromas
NecroticCore (%)
Fibrous capThickness (µm)
SMCs(%)
T-lymph
CalcificationScore
MΦs(%)Plaque type
Rupture
Thin-capFibroatheroma
P value
34±17
23±17
0.01
23±19
<65µm
26±20
14±10
0.005
0.002±0.004
6.6±10.4
ns
4.9±4.3
6.6±10.4
ns
1.53±1.03
0.97±1.1
0.014
Mean values are represented ± standard deviation. Abbreviations: MΦs= macrophages,SMCs= smooth muscle cells, T-lymph= T-lymphocytes
Kolodgie F, et al. Current Opinion in Cardiology 2001;16:285

Relationship of Fibrous Cap Thickness to Macrophage Infiltration
0
1
2
3
4
5
6
Cell Mean for % Kp-1
P = 0.03P = 0.06
Less
than
65
µm
66 -
200
µm
201
-300
µm
Mor
e th
an 3
00 µ
m

Remodeling in Varying CoronaryLesion Morphologies
B.A.
IEL-
Expe
cted
IEL
(mm
2
3
)
Eros
ion
Stab
le
Thin
cap
ath
erom
a
Plaq
ue h
emor
rhag
e
Acu
te ru
ptur
e
Hea
led
rupt
ure
Tota
l occ
lusi
on
IEL-
Expe
cted
IEL
(/pla
que
area
)
54321
2
1
0
-1
Eros
ion
Stab
le
Thin
cap
ath
erom
a
Plaq
ue h
emor
rhag
e
Acu
te ru
ptur
e
Hea
led
rupt
ure
Tota
l occ
lusi
on
0-1-2-3

Plaque rupture with mild non Plaque rupture with mild non occlusive thrombus: occlusive thrombus: mechanism by which mechanism by which
plaques progressplaques progress
2829389
Proximal
Rupture site
th
th
th
th
3mm6mm
9mm

Do TCFAs lead to plaque progression ?Do TCFAs lead to plaque progression ?Movat pentachrome
Sirius red Sirius red with polarized lightBurke AP, et al. Circulation 2001

Mean % stenosis increases with number of prior rupture sites
0
10
20
30
40
50
60
70
80
90
1 2 3 40
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4
Number of prior ruptures, acute rupture sites
Mean
% s
teno
sis
B
Mean
% s
teno
sis
ANumber of prior ruptures, healed rupture sites
Burke, A P et al. Circulation 2001;103:9364-940

Thin-cap FibroatheromaRecent Intraplaque Hemorrhage is seen at
Multiple sites in Patients Dying SCD
A
a
B
b
00.51
1.52
2.53
3.54
4.55
Plaquerupture
Plaqueerosion
Severe CAD>75%
Plaque Hemorrhage
Virmani R, et al. ATVB 2005

Consequence of Extravasated Erythrocytes Outside the
Vasculature• Free cholesterol content of erythrocyte membrane
exceeds that of all other cells in the body, with lipid constituting 40% of the weight
• Yeagle in 1985 showed that extravasated erythrocytes contain free cholesterol and Arbustini et al. in 2002 showed macrophage infiltration in intimal plaques in pulmonary trunk of patients with pulmonary hypertension at sites containing erythrocyte membranes
We examined tissues from nonvascular location to determine the effect of hemorrhage
• Pericardial hemorrhage• Intratumor hemorrhage (atrial hemangiomas, papillary
carcinoma of kidney etc)Kolodgie FD, et al. New Engl J Med 2003

E
H
Thin Fibrous Cap Atheroma
Phase Separation of Erythrocyte-Derived CholesteroIin Coronary and Non-Coronary Diseases
Hemorrhagic Pericarditis
F
E
HemorrhagePeriphery
HemorrhageCore
RBCs
MΦ
C
A
BD GpA
MΦ
GpA

Plaque Types Studied Plaque Types Studied A. B.Pathologic Intima Thickening
Fibroatheroma ‘Late’ Core
CD68
NC
Fibroatheroma ‘Early’ Core
LP
CD68
NC
CD68
C.Thin Cap FibroatheromaD.
NC
CD68

Morphometric Analysis of Hemorrhagic Events in Human Morphometric Analysis of Hemorrhagic Events in Human Coronary Plaques from Sudden Death VictimsCoronary Plaques from Sudden Death Victims
Necrotic Core(mm2)
GpAScore
MΦ(mm2)IronPlaque Type
PIT no core(n=129)FA early core(n=79)FA late core(n=105)TCFA(n=52)
0.09±0.04
0.23±0.07
*0.94±0.11
*1.60±0.20
0.07±0.05
0.17±0.08
*0.41±0.09
*1.24±0.24
0.0
0.06±0.02
*0.84±0.08
*1.95±0.30
0.002±0.001
0.018±0.004
*0.059±0.007
*0.142±0.016
Values are reported as the means±SE, *p<0.001 versus early core. The number in parenthesis represent thenumber of lesions examined;the total number= 365. MΦ = macrophages
Kolodgie FD, et al. New Engl J Med 2003

Plaque Vasa VasorumPlaque Vasa Vasorum• Plaque capillaries are observed in atherosclerotic
plaques with plaque thickness > 0.5 mm, suggesting that wall ischemia may be a determinant of neovascularization.
• Heistead and Armstrong reported a 5 fold increase in intimal/medial blood flow from proliferating micro vessels in monkeys fed a high cholesterol diet for 17 months. (Arteriosclerosis 1986)
• Plaque Vv may be a potential source of inflammation within the plaque [expression of VCAM-1, ICAM-1 and E-selectin has been shown in plaque Vv (O’Brian, et al. AJP 1994).
• Inflammation and matrix composition of atherosclerotic plaques may also influence angiogenesis.
Virmani R, et al., Arteriosclero Throm Vac Biol 2005;20:1262

Adventitial Vasa Vasorum Adventitial Vasa Vasorum Heterogeneity among different Heterogeneity among different
vascular bedsvascular beds
0
0.5
1
1.5
2
2.5
3
Coronary Renal Carotid Femoral
Vasa vasorumdensity/mm2
P<0.05P<0.05
P<0.05
P<0.05
Adv
entit
ial v
asa
vaso
rum
/mm
2
Low vasa vasorum density in internal thoracic artery may be responsible for the low incidence of atherosclerosis
Gallili et al. J Vasc Surg 2004;40:529 and J Thorac Cardiovasc Surg 2005;129:767

Vasa vasorum at various stages of
plaque development
Adaptive Intimal thickeningVv in adventitia
Fibroatherma Abnormal Vv Fibroatherma with leaky Vv

Intraplaque Vasa Vasorum in Coronary Intraplaque Vasa Vasorum in Coronary Plaques with a Necrotic CorePlaques with a Necrotic Core
A B150 µm thick sections stained with Ulex
nc nc
Virmani R, et al., Arteriosclero Throm Vac Biol 2005;20:1262
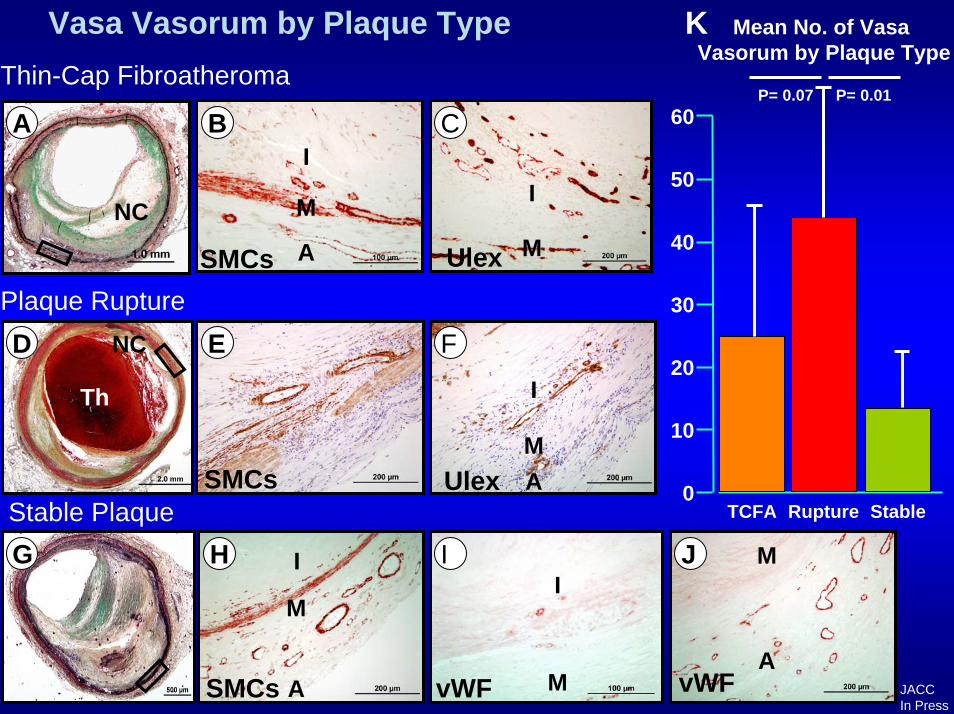
Vasa Vasorum by Plaque Type K Mean No. of Vasa Vasorum by Plaque Type
Thin-Cap Fibroatheroma
Plaque Rupture
UlexStable Plaque
I
vWF
M
A
A
M
vWF
I
MSMCs
I
M
A
SMCs
SMCs
M
Ulex
I
M
I
A
A
I
ED
B C
H J
F
G
0
10
20
30
40
50
TCFA Rupture Stable
Th
NC
60P= 0.07 P= 0.01
NC
JACCIn Press

Adventitia
0
20
40
60
80
100
120
140
Normal PIT FA TCFA Rupture
Mea
n Ve
ssel
Den
sity
(# o
f ves
sels
/mm
2 )
Adventitia
0
20
40
60
80
100
120
140
Normal PIT FA TCFA Rupture
Mea
n Ve
ssel
Den
sity
(# o
f ves
sels
/mm
2 )
MAMA MA
FANormal PIT
MA
MA
Plaque RuptureTCFA
Adventitial Vasa Vasorum In Varying Plaque Morphologies(Ulex Europaeus)
Intimal - Medial Border
0
10
20
30
40
50
60
70
80
Normal PIT FA TCFA Rupture
Mea
n Ve
ssel
Den
sity
(# o
f ves
sels
/mm
2 )
Intimal - Medial Border
0
10
20
30
40
50
60
70
80
Normal PIT FA TCFA Rupture
Mea
n Ve
ssel
Den
sity
(# o
f ves
sels
/mm
2 )
FANormal PIT
M
M M
NC
MMTCFA
Intimal-Medial Border Vasa Vasorum in Varying Plaque Morphologies (CD31/CD34)
Plaque Rupture

Intimal-Medial Border T Cell Densities and % Macrophage Infiltration at Vaso Vasorum Hotspots in Varying Plaque Morpholgies
M
T Cell Densities (UCHL-1)
M
M
PIT Late FA Rupture
MM
Macrophage Infiltration (CD68)
M

T cellpericore
0
100
200
300
400
500
600
PIT Early Core Late Core TCFA Rupture
I-M border
0
100
200
300
400
500
600
700
800
900
normal PIT Early CoreLate Core TCFA Rupture
Neointima
0
100
200
300
400
500
600
700
800
normal PIT Early CoreLate Core TCFA Rupture
Adventitia
0
200
400
600
800
1000
1200
normal PIT Early Core Late Core TCFA Rupture
P=0.02
*
*P=0.0007 *
*
P<0.0001 P=0.20
* *
**
*=significant VS. normal

ConclusionsPlaques occur focally at branch points in the
presence of systemic risk factorsThe morphologic characteriestics most predictive
for the presence of unstable vs. stable plaque is necrotic core size, plaque area and to a lesser extent macrophage infiltration.
Intra plaque hemorrhages from leaky vv are responsible for enlargement of necrotic core, macrophage infiltration and progressive luminal narrowing
Non invasive detection of vulnerable plaques is the only mechanism through which morbidity and mortality for CAD can be reduced or eliminated.

Progression of stenosiscausingStable
Angina Pectoris
Asymptomaticprogression
ofstenosis
Acute Coronary Syndrome-Unstable Angina
-Myocardial Infarction-Sudden Coronary Death
Thrombosed Plaque
High Risk/Vulnerable Plaque
Asymptomatic Atherosclerosis
Normal Coronary Arteries
Over decades may develop
Which over years, may lead to
Which may progress, in an unpredictable manner to Which leads to
Development of atherosclerosis and Progression to ThrombosisDevelopment of atherosclerosis and Progression to Thrombosis
Severe stenosis
Occlusive Non-occlusiveNon-occlusiveErosion Plaque Rupture
Terminology for high risk and Vulnerable Coronary ArteryPlaque, Aug 29, 2003, Santorini, Greece
65%30% 5%
Chronic total occlusion
Erosion Plaque rupture
Calcified nodule
Normal Artery
Asymptomatic Atherosclerosis
Vulnerable plaque