characteristics, mortality, and outcome of higher-birth weight infants who require intensive care
TRANSCRIPT

FETUS, PLACENTA, AND NEWBORN
Characteristics, mortality, and outcome of higher -birth weight infants who require intensive care
Joseph B. Philips III, M.D., Helen M. Dickman, M.Ed., Michael B. Resnick, Ed.D., Robert M. Nelson, Jr., M.D., and Donald V. Eitzman, M.D.
Gainesville, Florida
The improved outcome of small infants who have received intensive care is well documented; however,
the mortality and morbidity of infants weighing ;;;,:2500 gm who require intensive care have not been
emphasized. During a 2-year period these infants accounted for 41% of admissions and 34% of all deaths in our nursery. The most common diagnoses were pulmonary disease (32%), asphyxia (22%), congenital
anomalies (18%), infant of diabetic mother (10%), hematologic disease (9%), and infection (4%). Mortality
was 11% with 50% of the deaths from lethal malformations, 26% from asphyxia, 13% from infection, and
11% from miscellaneous causes. One half of the deaths were potentially preventable. According to developmental follow-up, over 90% of the survivors were developing normally. Thus, while outcome for
survivors is usually good, mortality remains excessively high. This large and understudied group of infants
requires increased investigative emphasis. (AM. J. OBSTET. GYNECOL. 149:875, 1984.)
Since the implementation of the concept of neonatal intensive care in the past few decades, most attention has focused on the incidence, mortality, and outcome of increasingly smaller-birth weight infants. A plethora of reports have appeared which document the improved outlook for intact survival in these tiny infants.' Indeed, many of the units in which these infants are cared for are referred to as "premature nurseries." What then of the higher-birth weight infants who also require neonatal intensive care? Reports containing information concerning larger infants either describe the entire population of neonatal intensive care units2
• 3 or
focus on a specific problem such as asphyxia.4•
5 An extensive literature search failed to reveal a single report dealing comprehensively with higher-birth weight infants who require neonatal intensive care. The purpose of this report is to document the ex peri-
From the Department of Pediatrics, Division of Neonatology, and Regional Developmental Evaluation Clinic, University of Florida College of Medicine.
This project was funded in part under an agreement with the Department of Health and Rehabilitative Services, State of Florida, Children's Medical Services.
Received for publication October 6, 1983; accepted January 27, 1984.
Reprint requests: joseph B. Philips Ill, M.D., Division of Perinatal Medicine, University of Alabama in Birmingham, 525 Hillman Building, University Station, Birmingham, AL 35209.
ence with higher-birth weight infants (;?:2500 gm) in a regionalized neonatal intensive care unit.
Material and methods
All patients were admitted to the University of Florida Regional Neonatal Intensive Care Center during the years 1976 through 1978. Subjects were selected by a review of the patient log with use of a single selection criterion: birth weight ;?:2500 gm. Data re
corded included name, medical record number, birth weight, sex, race, primary and secondary diagnoses, origin (inborn or outborn), length of stay in the Regional Neonatal Intensive Care Center, length of hospitalization, mortality, and the need for oxygen, continuous positive airway pressure, or mechanical ventilation. An effort was made to establish only one primary diagnosis per patient, but this was not always possible (e.g., congenital heart disease and infection).
Verification of the accuracy of these data was accomplished by chart review of a 10% random sample of the study population.
Developmental follow-up patients were randomly enrolled at birth. Personnel from the University of Florida Regional Developmental Evaluation Clinic attempted to maintain contact with all follow-up patients.
The Bayley scales of infant development were administered at 6, 12, and 24 months of adjusted postnatal age (15, 21, and 33 months of postconceptual age), and the
875
876 Philips et al.
140
130
120
110
"' 100
f-z 90 .., ~ 80 0..
"- 70 0
a: 60 .., "' :::;; 50 :::> z 40
30
10
LENGTH OF STAY IN RNICC (Days)
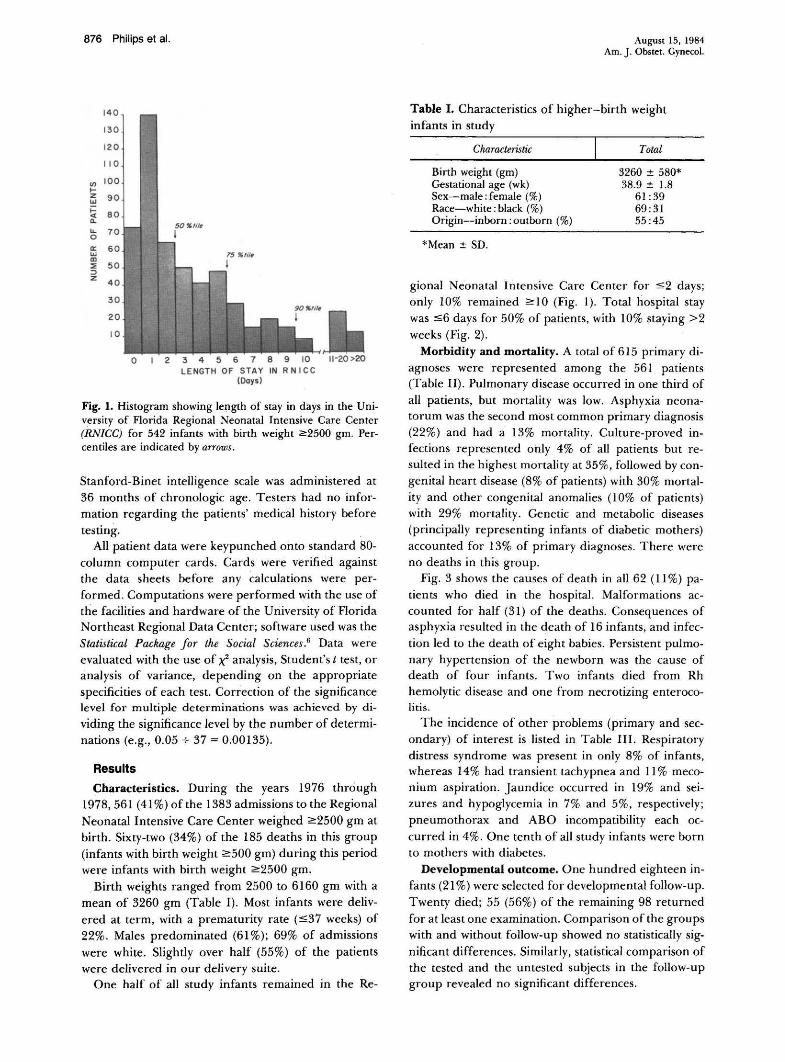
Fig. 1. Histogram showing length of stay in days in the University of Florida Regional Neonatal Intensive Care Center (RNICC) for 542 infants with birth weight 2:2500 gm. Percentiles are indicated by arrows.
Stanford-Binet intelligence scale was administered at 36 months of chronologie age. Testers had no information regarding the patients' medical history before
testing. All patient data were keypunched onto standard 80-
column computer cards. Cards were verified against the data sheets before any calculations were performed. Computations were performed with the use of the facilities and hardware of the University of Florida Northeast Regional Data Center; software used was the Statistical Package for the Social Sciences.6 Data were evaluated with the use of X: analysis, Student's t test, or analysis of variance, depending on the appropriate specificities of each test. Correction of the significance level for multiple determinations was achieved by dividing the significance level by the number of determinations (e.g., 0.05 + 37 = 0.00135).
Results
Characteristics. During the years 1976 through 1978, 561 ( 41%) of the 1383 admissions to the Regional Neonatal Intensive Care Center weighed ~2500 gm at birth. Sixty-two (34%) of the 185 deaths in this group (infants with birth weight ~500 gm) during this period were infants with birth weight ~2500 gm.
Birth weights ranged from 2500 to 6160 gm with a mean of 3260 gm (Table 1). Most infants were delivered at term, with a prematurity rate (::S:37 weeks) of 22%. Males predominated (61 %); 69% of admissions were white. Slightly over half (55%) of the patients were delivered in our delivery suite.
One half of all study infants remained in the Re-
August 15, 1984 Am. J. Obstet. Gynecol.
Table I. Characteristics of higher-birth weight infants in study
Characteristic
Birth weight (gm) Gestational age (wk) Sex-male:female (%) Race-white: black(%) Origin-inborn: outborn (%)
*Mean± SD.
Total
3260 ± 580* 38.9 ± 1.8
61:39 69:31 55:45
gional Neonatal Intensive Care Center for ::s:2 days; only 10% remained 2::10 (Fig. 1). Total hospital stay was ::S:6 days for 50% of patients, with 10% staying >2
weeks (Fig. 2). Morbidity and mortality. A total of 615 primary di
agnoses were represented among the 561 patients (Table II). Pulmonary disease occurred in one third of
all patients, but mortality was low. Asphyxia neonatorum was the second most common primary diagnosis (22%) and had a 13% mortality. Culture-proved infections represented only 4% of all patients but resulted in the highest mortality at 35%, followed by congenital heart disease (8% of patients) with 30% mortality and other congenital anomalies (10% of patients) with 29% mortality. Genetic and metabolic diseases (principally representing infants of diabetic mothers) accounted for 13% of primary diagnoses. There were no deaths in this group.
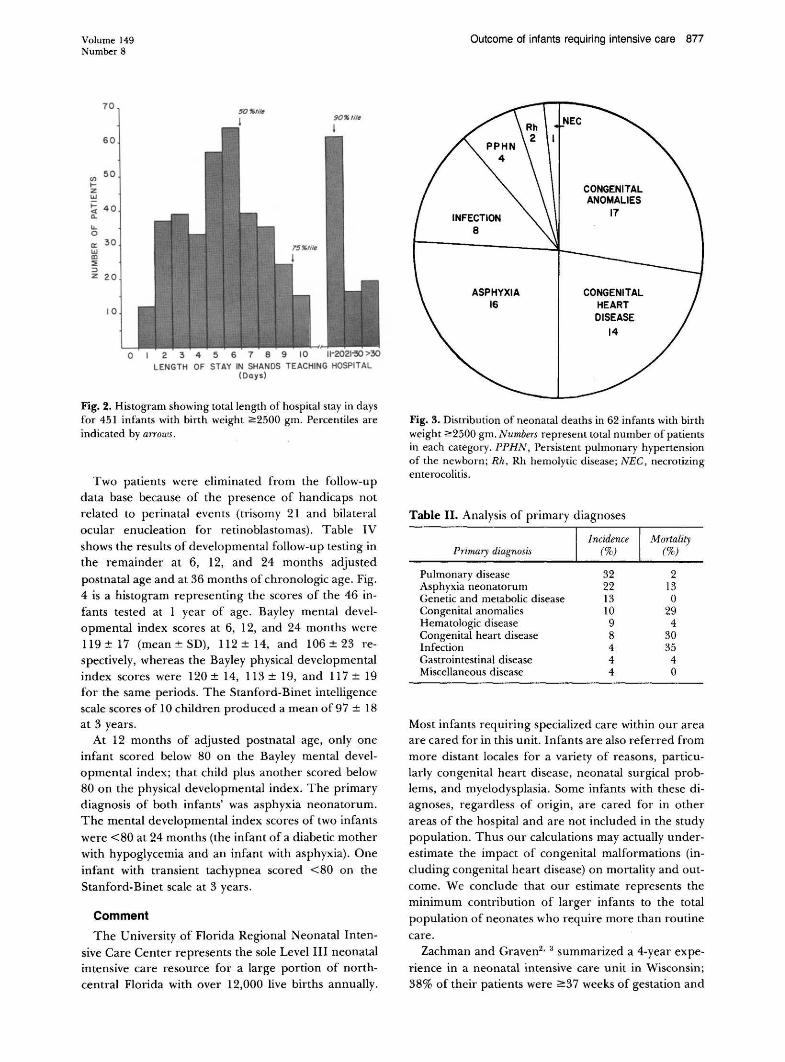
Fig. 3 shows the causes of death in all 62 (11 %) patients who died in the hospital. Malformations accounted for half (31) of the deaths. Consequences of asphyxia resulted in the death of 16 infants, and infection led to the death of eight babies. Persistent pulmonary hypertension of the newborn was the cause of death of four infants. Two infants died from Rh hemolytic disease and one from necrotizing enterocolitis.
The incidence of other problems (primary and secondary) of interest is listed in Table III. Respiratory distress syndrome was present in only 8% of infants, whereas 14% had transient tachypnea and 11% meconium aspiration. Jaundice occurred in 19% and seizures and hypoglycemia in 7% and 5%, respectively; pneumothorax and ABO incompatibility each occurred in 4%. One tenth of all study infants were born to mothers with diabetes.
Developmental outcome. One hundred eighteen infants (21 %) were selected for developmental follow-up. Twenty died; 55 (56%) of the remaining 98 returned
for at least one examination. Comparison of the groups with and without follow-up showed no statistically significant differences. Similarly, statistical comparison of the tested and the untested subjects in the follow-up group revealed no significant differences.
Volume 149 Number 8
70
60
(/) 50
.... z UJ ;::: 40 <[ <l.
lL 0
0:: 30 UJ CD ::!: ::> z 20
10
50"/i/~ 90"/i/6
4 5 6 8 9 LENGTH OF STAY IN SHANDS TEACHING HOSPITAL
(Days)
Fig. 2. Histogram showing total length of hospital stay in days for 451 infants with birth weight ~2500 gm. Percentiles are indicated by arrows.
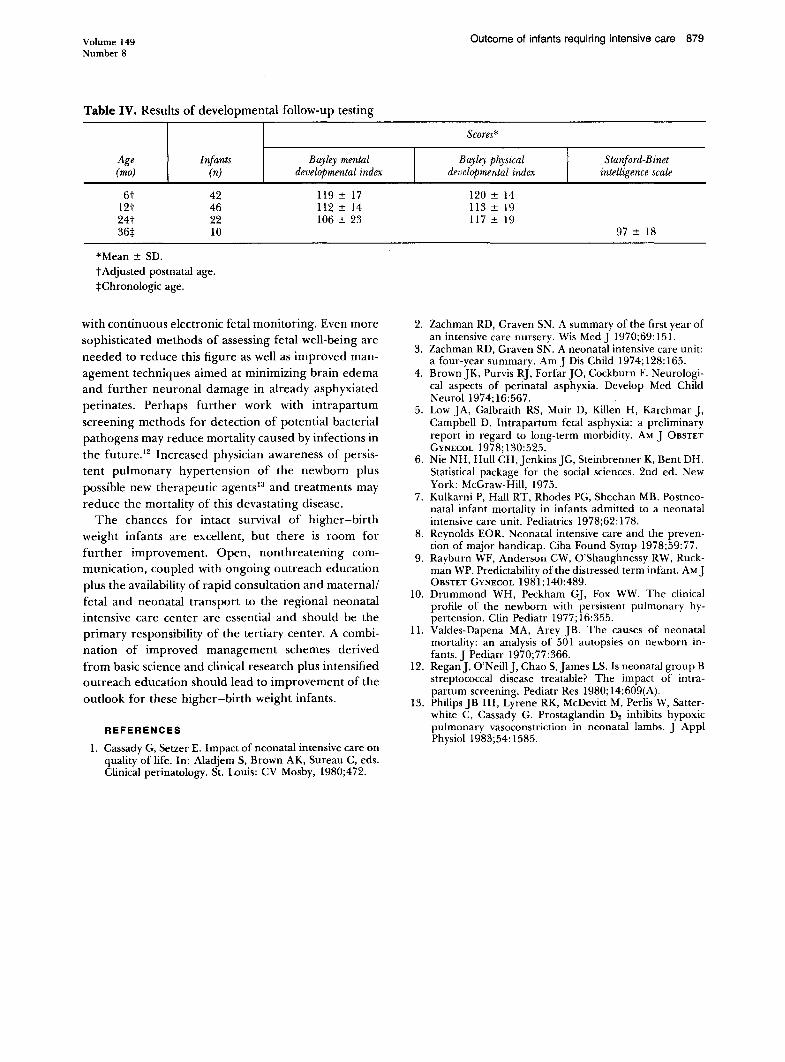
Two patients were eliminated from the follow-up data base because of the presence of handicaps not related to perinatal events (trisomy 21 and bilateral ocular enucleation for retinoblastomas). Table IV shows the results of developmental follow-up testing in the remainder at 6, 12, and 24 months adjusted
postnatal age and at 36 months of chronologie age. Fig. 4 is a histogram representing the scores of the 46 infants tested at 1 year of age. Bayley mental developmental index scores at 6, 12, and 24 months were 119± 17 (mean±SD), 112± 14, and 106±23 respectively, whereas the Bayley physical developmental index scores were 120± 14, 113± 19, and 117± 19 for the same periods. The Stanford-Binet intelligence scale scores of 10 children produced a mean of97 ± 18 at 3 years.
At 12 months of adjusted postnatal age, only one infant scored below 80 on the Bayley mental developmental index; that child plus another scored below 80 on the physical developmental index. The primary diagnosis of both infants' was asphyxia neonatorum. The mental developmental index scores of two infants
were <80 at 24 months (the infant of a diabetic mother with hypoglycemia and an infant with asphyxia). One
infant with transient tachypnea scored <80 on the Stanford-Binet scale at 3 years.
Comment
The University of Florida Regional Neonatal Inten
sive Care Center represents the sole Level III neonatal intensive care resource for a large portion of northcentral Florida with over 12,000 live births annually.
Outcome of infants requiring intensive care 877
INFECTION 8
ASPHYXIA 16
CONGENITAL ANOMALIES
17
CONGENITAL HEART DISEASE
14
Fig. 3. Distribution of neonatal deaths in 62 infants with birth weight ~2500 gm. Numbers represent total number of patients in each category. PPHN, Persistent pulmonary hypertension of the newborn; Rh, Rh hemolytic disease; NEG, necrotizing enterocolitis.
Table II. Analysis of primary diagnoses
Primary diagnosis
Pulmonary disease Asphyxia neonatorum Genetic and metabolic disease Congenital anomalies Hematologic disease Congenital heart disease Infection Gastrointestinal disease Miscellaneous disease
32 22 13 10 9 8 4 4 4
Mortality (%)
2 13 0
29 4
30 35
4 0
Most infants requiring specialized care within our area are cared for in this unit. Infants are also referred from more distant locales for a variety of reasons, particularly congenital heart disease, neonatal surgical problems, and myelodysplasia. Some infants with these diagnoses, regardless of origin, are cared for in other areas of the hospital and are not included in the study population. Thus our calculations may actually underestimate the impact of congenital malformations (including congenital heart disease) on mortality and outcome. We conclude that our estimate represents the minimum contribution of larger infants to the total
population of neonates who require more than routine
care. Zachman and Graven2
• 3 summarized a 4-year expe
rience in a neonatal intensive care unit in Wisconsin; 38% of their patients were ~37 weeks of gestation and

878 Philips et al.
IB
17
16
15
14
13 (/)
1- 12 z UJ II t= "" 10 Cl.
"- 9 0
a: B UJ
7 m :IE :> z 6
5
4
3
2
I
0
r--
~
,..---
,---~
I "'80 80·89 90•99 100"109 110-119 120·129130•139
BAYLEY M 0 I at 12 mos.
IB
17
16
15
14
13
~ 12
~II \i 10 Cl.
"- 9 0
B a: UJ 7 m ::1: 6 :> z
5
4
3
2
I
0
--
80 80·89 90•99 100•109 110•119 120•129130·139
BAYLEY P 0 I at 12 mos.
August 15, 1984 Am. J. Obstet. Gynecol.
Fig. 4. Histograms showing the distribution of scores on the Bayley scales of infant development for 46 follow-up infants at 12 months of adjusted postnatal age. Mental developmental index (MDI) is shown at left and physical developmental index (PDI) at right.
Table III. Incidence of selected problems
Problem
Prematurity Oxygen therapy Mechanical ventilation Jaundice Transient tachypnea Meconium aspiration Infant of diabetic mother Respiratory distress syndrome Continuous positive airway
pressure Seizures Hypoglycemia Pneumothorax ABO incompatibility
Incidence (%)
22 19 18 19 14 11 10 8 8
7 5 4 4
mortality was 22%. Similarly, Kulkarni et aJ.1 found that 42% of infants admitted to an intensive care unit in Missouri weighed over 2500 gm; neonatal mortality was 12%. These data support our observation that there is a large cadre of higher-birth weight infants who require specialized care in the newborn period.
The outlook for higher-birth weight neonates who require intensive care and survive seems to be good.8
We found only five of 53 follow-up patients who were developing abnormally as a possible result of perinatal events. Three of these had asphyxia. Rayburn et al.9
have shown that only one third of distressed neonates are predicted during the antenatal period. Even in normal populations or among those receiving optimal care, approximately 6% of children will score <80 on standardized tests. Thus we would have predicted that
three infants in our follow-up group would be handi
capped, perhaps from events not related to the perinatal period.
Most disturbing in our data, however, are the mortality figures. The cause of death of one half of the patients who died was potentially preventable disease rather than malformation. Twenty-four of these 31 died of asphyxia or infection. Persistent pulmonary hypertension of the newborn, a rather newly delineated entity, 10 was diagnosed in only eight patients, but four died. Erythroblastosis fetalis continues to cause deaths in spite of the availability of excellent preventive management. It appears unlikely that this particular disease will ever vanish entirely.
Valdes-Dapena and Arey 11 reported postmortem findings in 521 infants who died in the first 28 days of postnatal life for the years 1960 through 1966. Fifty-six infants weighed <:::2,501 gm. Thirty-six percent had congenital anomalies, 30% infiammatory lesions, 11% evidence of fetal anoxia, 11% trauma, and 7% erythroblastosis fetalis; 5% were infants of diabetic mothers. When one accounts for late-onset infections and improved obstetric care in the management of maternal diabetes as well as Rh isoimmunization and prevention
of birth trauma, these figures are remarkably similar to ours.
Clearly, efforts directed toward early detection and management of fetal distress, neonatal infections, and persistent pulmonary hypertension of the newborn are likely to have the most immediate impact on the mortality of higher-birth weight infants. Seven of the asphyxia-related deaths occurred in our own delivery population, although over 85% of labors are followed
Volume 149 Number 8
Table IV. Results of developmental follow-up testing
Age Infants (mo) (n)
6t 42 I2t 46 24t 22 36* IO
*Mean± SD. t Adjusted postnatal age. *Chronologie age.
Bayley mental developmental index
119 ± I7 112 ± I4 I06 ± 23
with continuous electronic fetal monitoring. Even more
sophisticated methods of assessing fetal well-being are
needed to reduce this figure as well as improved man
agement techniques aimed at minimizing brain edema
and further neuronal damage in already asphyxiated
perinates. Perhaps further work with intrapartum
screening methods for detection of potential bacterial
pathogens may reduce mortality caused by infections in
the future. 12 Increased physician awareness of persis
tent pulmonary hypertension of the newborn plus
possible new therapeutic agents13 and treatments may
reduce the mortality of this devastating disease.
The chances for intact survival of higher-birth
weight infants are excellent, but there is room for
further improvement. Open, nonthreatening com
munication, coupled with ongoing outreach education
plus the availability of rapid consultation and maternal/
fetal and neonatal transport to the regional neonatal
intensive care center are essential and should be the
primary responsibility of the tertiary center. A combi
nation of improved management schemes derived
from basic science and clinical research plus intensified outreach education should lead to improvement of the
outlook for these higher-birth weight infants.
REFERENCES
I. Cassady G, Setzer E. Impact of neonatal intensive care on quality of life. In: Aladjem S, Brown AK, Sureau C, eds. Clinical perinatology. St. Louis: CV Mosby, I980;472.
Outcome of infants requiring intensive care 879
Scores*
I Bayley physical
I Stanford-Binet
developmental index intelligence scale
I20 ± I4 II3 ± I9 II7 ± I9
97 ± I8
2. Zachman RD, Graven SN. A summary of the first year of an intensive care nursery. Wis MedJ I970;69:I5l.
3. Zachman RD, Graven SN. A neonatal intensive care unit: a four-year summary. Am] Dis Child I974;I28:I65.
4. BrownJK, Purvis RJ, Forfar JO, Cockburn F. Neurological aspects of perinatal asphyxia. Develop Med Child Neuroli974;I6:567.
5. Low JA, Galbraith RS, Muir D, Killen H, Karchmar J, Campbell D. Intrapartum fetal asphyxia: a preliminary report in regard to long-term morbidity. AM J 0BSTET GYNECOL I978; I30: 525.
6. Nie NH, Hull CH, Jenkins JG, Steinbrenner K, Bent DH. Statistical package for the social sciences. 2nd ed. New York: McGraw-Hill, I975.
7. Kulkarni P, Hall RT, Rhodes PG, Sheehan MB. Postneonatal infant mortality in infants admitted to a neonatal intensive care unit. Pediatrics I978;62: I78.
8. Reynolds EOR. Neonatal intensive care and the prevention of major handicap. Ciba Found Symp I978;59:77.
9. Rayburn WF, Anderson CW, O'Shaughnessy RW, Ruckman WP. Predictability of the distressed term infant. AM J 0BSTET GYNECOL I98I;I40:489.
IO. Drummond WH, Peckham GJ, Fox WW. The clinical profile of the newborn with persistent pulmonary hypertension. Clin Pediatr I977; I6: 355.
II. Valdes-Dapena MA, Arey JB. The causes of neonatal mortality: an analysis of 50 I autopsies on newborn infants. J Pediatr I970;77:366.
I2. Regan], O'Neill], Chao S,James LS. Is neonatal group B streptococcal disease treatable? The impact of intrapartum screening. Pediatr Res 1980; I4:609(A).
I3. Philips JB Ill, Lyrene RK, McDevitt M, Perlis W, Satterwhite C, Cassady G. Prostaglandin D2 inhibits hypoxic pulmonary vasoconstriction in neonatal lambs. J Appl Physiol I983;54: I585.