chapter 4 the physical requirements for invasive ca ... · coronary angiography / 78 conclusion /...
TRANSCRIPT

71CHAPTER 4: Coronary Angiography
Chapter 4Coronary angiographyKjell C. Nikus
DESCripTion oF Coronary angiography / 71Technique / 71
inDiCaTionS anD ConTrainDiCaTionS / 71
CoMpLiCaTionS / 72
Coronary anaToMy anD VariaTionS / 72
angiographiC Coronary arTEry DiSEaSE / 75
Coronary arTEry anoMaLiES / 75Bridging / 75Fistulae / 76
CoLLaTEraL CirCULaTion / 76
angiographiC aSSESSMEnT oF Coronary FLoW / 76Angiographic Assessment of Myocardial Blood Flow / 76
angiographiC FaCTorS DETErMining ECg ChangES in aCUTE Coronary SynDroMES / 77Anterior STEMI / 77Inferior STEMI / 77Lateral STEMI / 77Non–ST-Segment Elevation Acute Coronary Syndromes / 77
anCiLLary METhoDS To STUDy aThEroSCLEroTiC LESionS / 77Intravascular Ultrasound / 78Novel Invasive Imaging Modalities / 78Invasive Evaluation of the Physiologic Significance of Stenotic
Lesions / 78
MULiTMoDULar iMaging in ConJUnCTion WiTh Coronary angiography / 78
ConCLUSion / 78
The physical requirements for invasive CA performed in a cath-eterization laboratory include a radiographic system, equipment for physiologic data monitoring and acquisition instrumenta-tion, and equipment for emergency patient care. High-resolution x-ray imaging is required for optimal visualization of the coro-nary tree, including arterial side branches. Traditional film-based cineangiography has in large part been replaced by digital tech-nology. The digital technique enables immediate online review, quantitative computer analysis, image manipulation capabilities, and increased storage capabilities. During the last few years, direct digital imaging with flat panel technique has become the standard in many catheterization laboratories.
TECHNiquE■■
Angiography is performed under local anesthesia with small-diameter catheters introduced through a transarterial sheath. The outer diameter of the catheter is specified using French units, where one French unit (F) = 0.33 mm. Normally, 4- or 5-F catheters are used for diagnostic purposes. In the majority of cases, either the femoral or the radial route is used. Through the catheters, which are introduced over a guide wire, iodinated contrast media is injected selectively into the left and right coro-nary arteries. A few angiographic projections (varying degrees of left, right, cranial, and caudal angulation) are used to enable visualization of the whole coronary tree without superimposition of multiple vessels.
inDiCaTionS anD ConTrainDiCaTionSCA is used to establish or rule out the presence of coronary stenoses, define therapeutic options, and determine prognosis. CA is also used as a research tool for follow-up after invasive procedures or pharmacologic therapy. The American College of Cardiology/American Heart Association (ACC/AHA) Task Force and the European Society of Cardiology established the indica-tions for CA.1,2 Patients with suspected CAD who have severe stable symptoms and those with certain high-risk features for an adverse outcome should have CA. High-risk criteria include low ejection fraction and poor exercise capacity on an exercise test.
In patients with non–ST-segment elevation acute coronary syndromes (unstable angina and myocardial infarction) with high-risk features (eg, ongoing ischemia, heart failure), CA is recommended during the hospitalization.3,4 In patients with acute ST-segment elevation myocardial infarction (STEMI), guidelines recommend CA in the acute phase for most patients.5,6 Primary percutaneous intervention (PCI) is usually performed in the same procedure, immediately after the diagnostic CA, in these patients.
There are no absolute contraindications for CA. Relative con-traindications include febrile untreated infection, severe ane-mia, severe electrolyte imbalance, active bleeding, acute renal failure, and ongoing stroke. Risk factors for significant compli-cations after CA include advanced age, morbid obesity, bleeding diathesis, recent stroke, and dissection or severe atheromatosis of the thoracic aorta.
DESCripTion oF Coronary angiographyInvasive coronary angiography (CA) remains the standard for identifying coronary artery narrowings related to coronary artery disease (CAD). Selective CA, which was first performed by F. Mason Sones in 1959, enables correlation of different clinical syndromes and electrocardiography (ECG) findings with coronary artery anatomy. The method provides the most reliable information for determining appropriate therapy in patients with CAD. CA has become a routine procedure per-formed on an ambulatory basis in many centers. Technical and logistic improvements have improved patient safety.
04-Wagner_Ch04_p_071-080.indd 71 12/18/10 10:10:44 AM

72 SECTioN i: Current Methods and Their Applications for Cardiovascular Multimodal imaging
CoMpLiCaTionSWith modern technical equipment, major complications are uncommon (<1%) in diagnostic procedures.7 Vascular com-plications related to the arterial puncture site are the most frequent complications. Mortality risk is 0.1% or less. Allergic contrast reactions, worsening kidney function, and cerebro-vascular accidents are rare complications. Ventricular fibrilla-tion may be provoked by contrast injection into a small side branch, typically the conal branch of the right coronary artery (RCA). Iatrogenic coronary artery dissection is a potential life-threatening complication, which usually is handled by either emergent coronary artery stenting or bypass surgery.
CORONARY ANATOMY AND VARIATIONSThe Coronary Artery Surgery Study (CASS) investigators estab-lished the nomenclature that is most often used for coronary artery description.8 Minor modifications to the criteria were pro-vided by the Bypass Angioplasty Revascularization Investigators (BARI).9 The coronary artery circulation is composed of two principal arteries, the left coronary artery (LCA) and the RCA, arising from the aorta. The two principal coronary arteries and their larger branches are arranged on the surface of the heart (extramural vessels) and give rise to branches that penetrate the myocardium (intramural vessels). The major epicardial vessels and their second- and third-order branches can be visualized by CA. The network of smaller intramyocardial branches generally is not seen. Not infrequently, the extramural vessels may be cov-ered in part by myocardium and surrounded by cardiac muscle (termed myocardial bridging; see later section “Bridging”). Variations in the branching pattern are extremely common in the human heart. According to the BARI classification, the RCA is predominant in approximately 85% of individuals, providing the posterior descending (PD; ie, posterior interventricular) branch and at least one posterolateral (PL) branch (Figs. 4–1 to 4–3).9 In 7% to 8% of individuals, the coronary circulation is left-dominant; the PL, the PD, and the atrioventricular (AV) nodal branches are all supplied by the terminal portion of the left circumflex coronary artery (LCx; Figs. 4–4 and 4–5). In another 7% to 8% of hearts, there is a codominant or balanced system, in which the RCA gives rise to the PD branch and the LCx gives rise to all the PL branches and, in some individuals, also to a parallel PD branch that supplies part of the interven-tricular septum (Figs. 4–6 and 4–7).
The proximal or main segment of the LCA is known as the left main (LM) coronary artery (see Fig. 4–3). The left anterior descending (LAD) coronary artery is a direct continuation of the main trunk; it runs along the anterior interventricular groove (see Fig. 4–5). It may terminate before the left ventricu-lar (LV) apex or at the apex (see Fig. 4–3). In most cases, the LAD “wraps” around the apex into the posterior interventricular groove (see Fig. 4–5). One or more left diagonal (LD) branches arise from the LAD, subtending the anterolateral part of the LV (Fig. 4–8). The LAD also gives rise to approximately 10 septal branches (Fig. 4–9; see also Fig. 4–8). One of the proximal
FigUrE 4–1. right anterior oblique projection of the right coronary artery in right dominant circulation. the large posterior descending (pD) branch subtends the inferior part of the heart giving off small inferoseptal branches (white arrows). In this case, the pD branch reaches the left ventricular apex. a borderline significant stenosis is located at the take-off of the right ventricular (rV) and right acute marginal (raM) branches. total occlusion of the artery at this point would result in right ventricular transmural ischemia with St-segment elevation in the right-sided electrocardiogram leads (V3r-V5r) and less often in lead V1. rpD, right posterior descending branch.
FigUrE 4–2. Left anterior oblique projection of the right coronary artery (rCa) in right dominant circulation. at the crux cordis (white arrow), the point where the atrioventricular and interventricular grooves converge, the artery bifurcates into the posterior descending (pD) and posterolateral (pL) branches. the pD branch runs along the interventricular groove, whereas the pL branches spread out over the infero (postero) lateral aspect of the heart. rpD, right posterior descending branch; rpL, right posterolateral branch.
septal branches is usually larger than the others and supplies the region of the bundle of His and bundle branches of the conduction system (see Fig. 4–9). The LCx arises from the LM and gives off branches to the upper lateral LV wall and the left
04-Wagner_Ch04_p_071-080.indd 72 12/18/10 10:10:45 AM
73CHAPTER 4: Coronary Angiography
atrium (see Fig. 4–3). In approximately two-thirds of cases, the LCx terminates between the lateral margin of the LV and the posterior interventricular sulcus (Fig. 4–10). The left obtuse marginal (OM) branches arise at a right or an acute angle from the LCx and descends vertically toward the apex of the heart
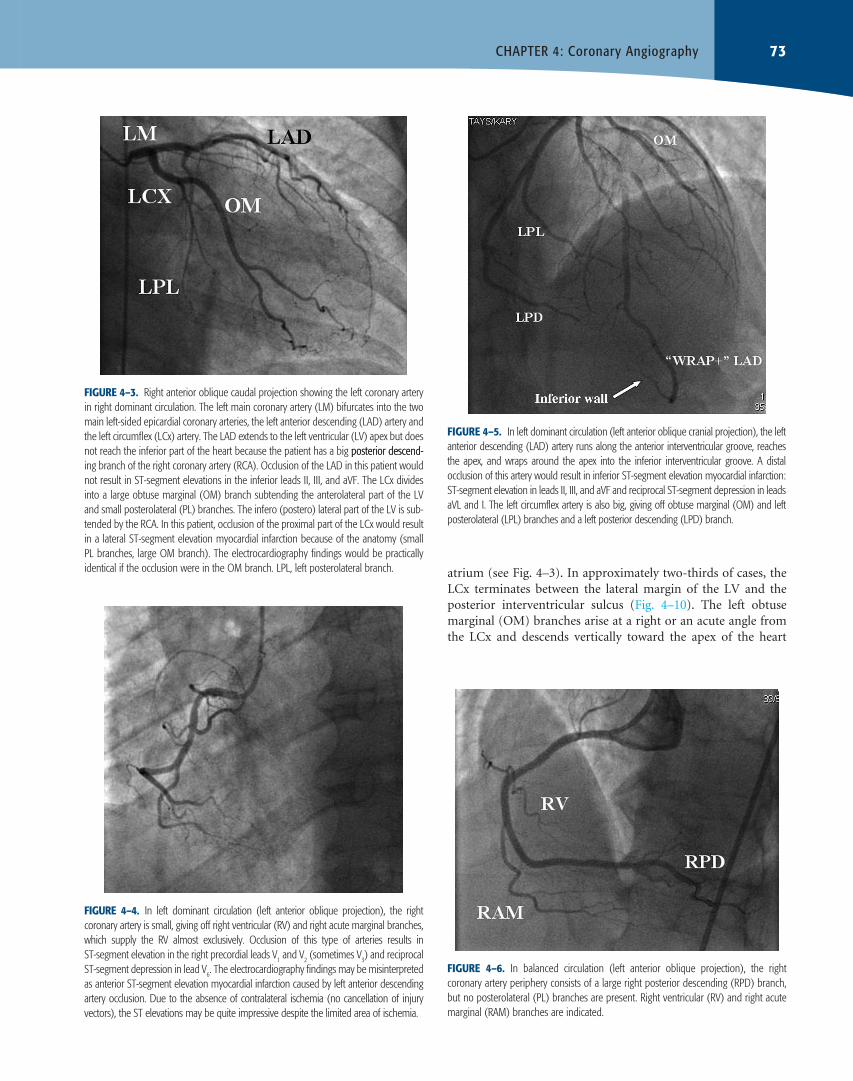
FigUrE 4–5. In left dominant circulation (left anterior oblique cranial projection), the left anterior descending (LaD) artery runs along the anterior interventricular groove, reaches the apex, and wraps around the apex into the inferior interventricular groove. a distal occlusion of this artery would result in inferior St-segment elevation myocardial infarction: St-segment elevation in leads II, III, and aVF and reciprocal St-segment depression in leads aVL and I. the left circumflex artery is also big, giving off obtuse marginal (OM) and left posterolateral (LpL) branches and a left posterior descending (LpD) branch.
FigUrE 4–6. In balanced circulation (left anterior oblique projection), the right coronary artery periphery consists of a large right posterior descending (rpD) branch, but no posterolateral (pL) branches are present. right ventricular (rV) and right acute marginal (raM) branches are indicated.
FigUrE 4–4. In left dominant circulation (left anterior oblique projection), the right coronary artery is small, giving off right ventricular (rV) and right acute marginal branches, which supply the rV almost exclusively. Occlusion of this type of arteries results in St-segment elevation in the right precordial leads V1 and V2 (sometimes V3) and reciprocal St-segment depression in lead V6. the electrocardiography findings may be misinterpreted as anterior St-segment elevation myocardial infarction caused by left anterior descending artery occlusion. Due to the absence of contralateral ischemia (no cancellation of injury vectors), the St elevations may be quite impressive despite the limited area of ischemia.
FigUrE 4–3. right anterior oblique caudal projection showing the left coronary artery in right dominant circulation. the left main coronary artery (LM) bifurcates into the two main left-sided epicardial coronary arteries, the left anterior descending (LaD) artery and the left circumflex (LCx) artery. the LaD extends to the left ventricular (LV) apex but does not reach the inferior part of the heart because the patient has a big posterior descend-posterior descend-ing branch of the right coronary artery (rCa). Occlusion of the LaD in this patient would not result in St-segment elevations in the inferior leads II, III, and aVF. the LCx divides into a large obtuse marginal (OM) branch subtending the anterolateral part of the LV and small posterolateral (pL) branches. the infero (postero) lateral part of the LV is sub-tended by the rCa. In this patient, occlusion of the proximal part of the LCx would result in a lateral St-segment elevation myocardial infarction because of the anatomy (small pL branches, large OM branch). the electrocardiography findings would be practically identical if the occlusion were in the OM branch. LpL, left posterolateral branch.
04-Wagner_Ch04_p_071-080.indd 73 12/18/10 10:10:47 AM
74 SECTioN i: Current Methods and Their Applications for Cardiovascular Multimodal imaging
(see Fig. 4–3). In approximately one-third of individuals, the LM trifurcates; the intermediate (IM) branch (ramus intermedius) comes off between the LAD and the LCx (see Fig. 4–9). The direct origin of the LAD and the LCx by separate ostia from the aorta without an LM coronary artery is a rare occurrence.
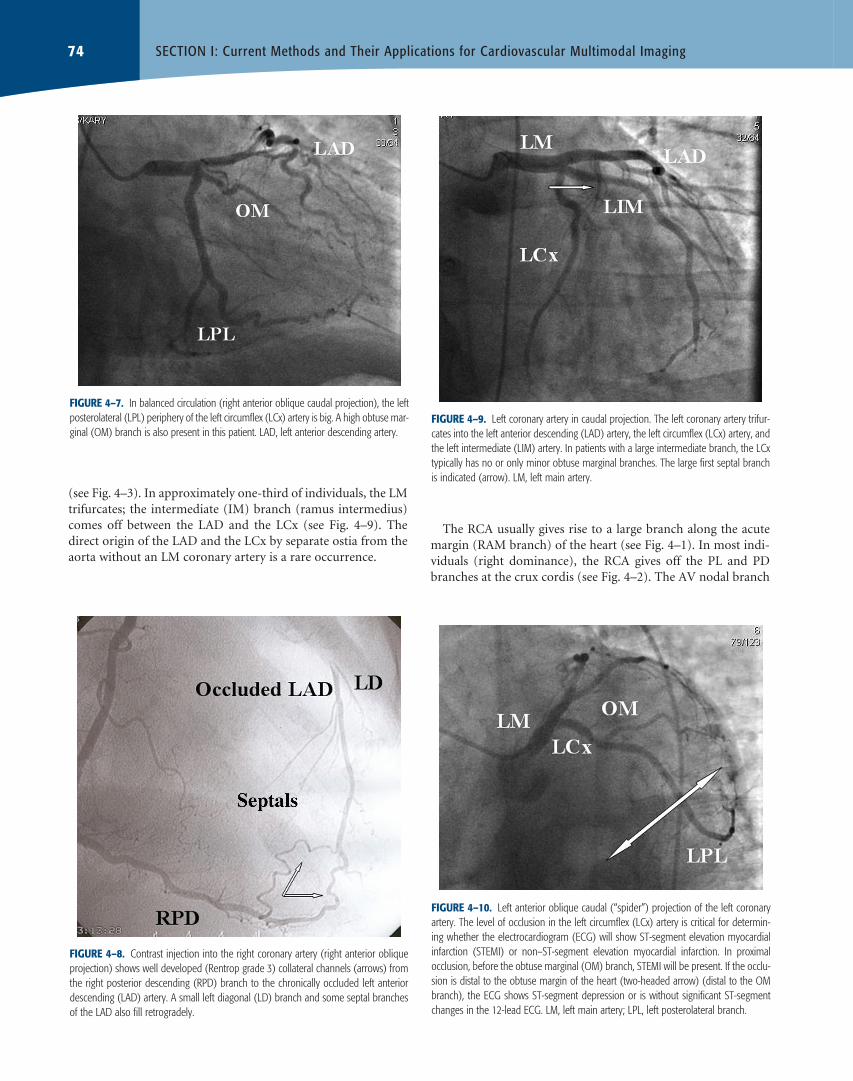
FigUrE 4–7. In balanced circulation (right anterior oblique caudal projection), the left posterolateral (LpL) periphery of the left circumflex (LCx) artery is big. a high obtuse mar-ginal (OM) branch is also present in this patient. LaD, left anterior descending artery.
FigUrE 4–8. Contrast injection into the right coronary artery (right anterior oblique projection) shows well developed (rentrop grade 3) collateral channels (arrows) from the right posterior descending (rpD) branch to the chronically occluded left anterior descending (LaD) artery. a small left diagonal (LD) branch and some septal branches of the LaD also fill retrogradely.
FigUrE 4–9. Left coronary artery in caudal projection. the left coronary artery trifur-cates into the left anterior descending (LaD) artery, the left circumflex (LCx) artery, and the left intermediate (LIM) artery. In patients with a large intermediate branch, the LCx typically has no or only minor obtuse marginal branches. the large first septal branch is indicated (arrow). LM, left main artery.
FigUrE 4–10. Left anterior oblique caudal (“spider”) projection of the left coronary artery. the level of occlusion in the left circumflex (LCx) artery is critical for determin-ing whether the electrocardiogram (eCG) will show St-segment elevation myocardial infarction (SteMI) or non–St-segment elevation myocardial infarction. In proximal occlusion, before the obtuse marginal (OM) branch, SteMI will be present. If the occlu-sion is distal to the obtuse margin of the heart (two-headed arrow) (distal to the OM branch), the eCG shows St-segment depression or is without significant St-segment changes in the 12-lead eCG. LM, left main artery; LpL, left posterolateral branch.
The RCA usually gives rise to a large branch along the acute margin (RAM branch) of the heart (see Fig. 4–1). In most indi-viduals (right dominance), the RCA gives off the PL and PD branches at the crux cordis (see Fig. 4–2). The AV nodal branch
04-Wagner_Ch04_p_071-080.indd 74 12/18/10 10:10:48 AM

75CHAPTER 4: Coronary Angiography
arises from the PL branch. The most proximal side branch, the conus branch, subtends the right part of the interventricular septum to a varying extent (Fig. 4–11). In approximately 50% of individuals, the conus branch takes off directly from the aorta, either through a separate ostium (two-thirds of individuals) or through a common ostium with the RCA (one-third of individu-als). The branch to the sinus node arises from the proximal RCA in the majority of individuals (see Fig. 4–11). In approximately 45% of human hearts, the sinus node is supplied by a branch arising within the first few millimeters of the course of the LCx.
angiographiC Coronary arTEry DiSEaSECAD is defined as more than 50% angiographic diameter steno-sis in one or more of the epicardial coronary arteries. Based on disease severity, obstructive CAD is classified as single-, double-, or triple-vessel disease. Stenoses less than 50% are considered as non–symptom generating, except in cases with dynamic obstruction. It has been suggested that acute coronary syndromes predominantly occur at the site of coronary stenoses with less than 50% diameter reduction,10 presumably related to thin-cap fibroatheromas. This finding has been questioned in more recent studies.11 Scoring systems have been developed to more specifically characterize the coronary vasculature with respect to the number of lesions and their functional impact, location, and complexity.12,13 Recently, the SYNTAX score was developed as an angiographic grading tool.14
Coronary arTEry anoMaLiESCoronary artery anomalies occur in 1% to 5% of individuals and represent those angiographic findings in which the origin, course, or termination of the arteries is infrequently encountered.15,16 Coronary anomalies may or may not cause myocardial isch-emia. High take-off above the junction of the sinus and from the tubular part of the aorta and multiple coronary ostia usually represent no major clinical problems but may pose a challenge for the interventionalist to perform selective CA.
Some coronary artery anomalies are very difficult to visual-ize at angiography, and even if they are visualized, their course may be delineated inaccurately. Hence, multimodular imaging should be considered in cases with signs of myocardial ischemia or unexplained syncope in young individuals, where no other etiologies are evident.
Anomalous origin of the LCA from the pulmonary artery (ALCAPA) is one of the most serious congenital coronary artery anomalies. Approximately 90% of untreated infants die in the first year of life, and only a few patients survive to adult-hood.17 CA usually helps confirm the diagnosis of ALCAPA and demonstrates collateral circulation between the RCA and LCA and a coronary “steal” phenomenon into the pulmonary artery. Anomalous origin of the RCA from the pulmonary artery (ARCAPA) is a very rare congenital abnormality.
Anomalous origin of a coronary artery from the opposite (or noncoronary) sinus (ACOS) taking an interarterial (ie, between the aorta and the pulmonary artery) course carries a high risk for sudden cardiac death. The RCA arises from the left sinus of Valsalva as a separate vessel or as a branch of a single coronary artery in 0.03% to 0.17% of patients who undergo angiogra-phy.18 The most common course of an anomalous RCA arising from the left sinus of Valsalva is interarterial; this variant can be associated with sudden cardiac death in up to 30% of patients. The LCA arises from the right sinus of Valsalva as a separate vessel or as a branch of a single coronary artery in 0.09% to 0.11% of patients who undergo angiography.19 An interarterial course may be seen in up to 75% of patients with this anomaly, who are at high risk for sudden cardiac death due to the acute angle of the ostium, the stretch of the intramural segment, and the compression between the commissure of the right and left coronary cusps.
Duplication of the LAD artery in otherwise normal hearts has been reported to occur in 0.13% to 1% of the general population.20 Duplication of the LAD artery consists of a short LAD artery, which courses and terminates in the anterior inter-ventricular sulcus without reaching the apex, and a long LAD artery, which originates from either the LAD artery proper or the LCA and then enters the distal anterior interventricular sul-cus and courses to the apex. In patients having bypass surgery, the cardiac surgeon needs to be informed about this anomaly to be able to place the arteriotomy optimally.
BRidgiNg■■
Myocardial bridging is caused by a band of myocardial muscle overlying a segment of a coronary artery. It is most commonly
FigUrE 4–11. the conus branch more often takes off as the first side branch of the right coronary artery than via a separate ostium of the aorta. It subtends the right side of the interventricular septum and the right ventricular outflow tract. patients with large conus branches do not show St-segment elevation in lead V1 in anterior St-segment elevation myocardial infarction caused by left anterior descending artery occlusion (protection of the right side of the septum by the side branch). the small side branch to the sinus node is indicated by an arrow. rpD, right posterior descending branch.
04-Wagner_Ch04_p_071-080.indd 75 12/18/10 10:10:49 AM

76 SECTioN i: Current Methods and Their Applications for Cardiovascular Multimodal imaging
localized in the middle segment of the LAD artery. There is some discrepancy between the prevalence of myocardial bridging at angiography (0.5%-2.5%) and the prevalence at pathologic analysis (15%-85%).21 The cause for this discrepancy is presumed to be the fact that myocardial bridging often occurs without overt symptoms, so that patients are rarely referred for CA. In some cases, however, myocardial bridging is respon-sible for angina pectoris, myocardial infarction, life-threatening arrhythmias, or even death. The standard of reference for diag-nosing myocardial bridges is CA, at which a typical “milking” effect and a “step down–step up” phenomenon induced by systolic compression of the tunneled segment may be seen. In multidetector computed tomography, myocardial bridging is present in approximately one-third of cases. By this method, the intramyocardial location of the involved coronary arterial seg-ment is easily recognized. Myocardial bridging does not cause ischemia in the vast majority of individuals.
FiSTulAE■■
Coronary artery fistula is a condition in which a communica-tion exists between one or two coronary arteries and either a cardiac chamber, the coronary sinus, the superior vena cava, or the pulmonary artery. This condition is seen in approximately 0.1% to 0.2% of all patients who undergo selective CA.22 It more commonly involves the RCA (60% of cases) than the LCA (40%). In coronary artery fistula, the involved coronary artery is dilated because of increased blood flow and is often tortuous to an extent determined by the shunt volume. The most common site of drainage is the right ventricle (45% of cases), followed by the right atrium (25%) and the pulmonary artery (15%).23 The fistula drains into the left atrium or left ventricle in less than 10% of cases. When the shunt leads into a right-sided cardiac chamber, the hemodynamics resemble those of an extracardiac left-to-right shunt; when the connection is to a left-sided cardiac chamber, the hemodynamics mimic those of aortic insuffi-ciency. Myocardial perfusion may be diminished for that por-tion of the myocardium supplied by the abnormally connecting coronary artery. This situation represents a hemodynamic steal phenomenon and may lead to myocardial ischemia.
CoLLaTEraL CirCULaTionAfter total or near-total occlusion of a coronary artery, per-fusion of ischemic myocardium occurs through collaterals, which are vascular channels that interconnect epicardial coro-nary arteries. Previously occluded vessel branches are usually manifested as truncated stumps on angiography. The part of the vessel distal to the occlusion is frequently filled late in the contrast injection by antegrade (“bridging”) collaterals or collat-erals that originate from the same or an adjacent vessel. In fresh total occlusions, typically represented by STEMI, no collateral flow may be evident from CA. Functioning collaterals maintain myocardial viability but are not as effective as the native vessel for oxygen distribution. Some grade of effort angina is typi-cal for patients with occluded coronary arteries and collateral
flow. The Rentrop classification is used for defining the grade of established coronary filling.24 Briefly, grade 0 represents no col-Briefly, grade 0 represents no col-lateral opacification, grade 1 represents filling of side branches, and grade 2 represents partial and grade 3 complete filling of the main branch by collateral vessels (see Fig. 4–8).
angiographiC aSSESSMEnT oF Coronary FLoWIn 1985, the Thrombolysis in Myocardial Infarction (TIMI) investigators introduced a simple, quantitative grading of coro-nary flow to assess the efficiency of coronary reperfusion thera-py.25 This grading system has been widely accepted as a standard in the angiographic grading of coronary blood flow both in clinical trials and as a useful tool in routine clinical work. TIMI flow grade 0 represents no antegrade flow beyond the vessel obstruction. TIMI flow grade 1 represents perfusion of contrast material distal to the occlusion, but the entire coronary bed distal to the occlusion is not opacified. TIMI flow grade 2 repre-sents slower rate of entry of contrast material into the distal ves-sel when compared with other areas of the coronary tree. TIMI flow grade 3 represents normal contrast filling. TIMI flow grade 3 has been associated with improved outcome in acute STEMI, but normal blood flow in the epicardial vessels does not neces-sarily equate to normal myocardial blood flow.
To overcome limitations of the original TIMI flow grad-ing system, a quantitative measure, the TIMI frame count, was introduced.26 In this method, the number of cine frames required for contrast material to reach standard distal coronary landmarks of a coronary artery is counted. In addition, the length of the corresponding artery is taken into consideration by introducing vessel-corrected TIMI frame counts. Corrected TIMI frame count ≤27 frames was defined as normal epicardial perfusion. TIMI frame counting is an objective and quantitative index of epicardial blood flow and is an independent predic-tor of in-hospital mortality after acute myocardial infarction. The method is simple and reproducible but, like the TIMI flow grade, is not a specific measure of myocardial blood flow.
ANgiogRAPHiC ASSESSMENT oF MyoCARdiAl ■■Blood Flow
Optimal reperfusion therapy has been defined in several studies as achievement of normalization of both epicardial coronary perfu-sion and myocardial perfusion. The so-called no-reflow phenome-non, an open epicardial artery without flow into the myocardium, predicts adverse clinical events and left ventricular remodeling. Two different angiographic methods have been described for assessment of myocardial perfusion on the angiogram. One is myocardial blush grade,27 an index based on the intensity of contrast opacity of the infarcted area, and the other is TIMI myocardial perfusion grading,28 which focuses on the velocity of contrast opacity clearance. Both methods have proven useful for the assessment of microvascular flow and prediction of clinical outcomes after myocardial infarction. It has been proposed that the duration of blush reflects the perfusion level of myocardium.
04-Wagner_Ch04_p_071-080.indd 76 12/18/10 10:10:49 AM

77CHAPTER 4: Coronary Angiography
However, visual assessment of these methods is categorical, sub-jective, and operator dependent, and quantitative angiographic indexes of myocardial perfusion are under development.29
angiographiC FaCTorS DETErMining ECg ChangES in aCUTE Coronary SynDroMESIn the preangiography era, autopsy was used as the gold stan-dard for ECG correlations with anatomy. It was not until the early 1970s, that the field of ECG in ischemic heart disease began to flourish, concomitantly with the advent of CA, echocardiog-raphy, and nuclear medicine.30 In the absence of confounding factors, like left bundle branch block (LBBB), the ECG contains clinically important information about the culprit artery, size of artery, and site of occlusion in the acute occlusive stage of an acute myocardial infarction. This is true especially for the hyper-acute occlusive stage (“preinfarction syndrome”), represented in the ECG by ST-segment elevation without new Q waves, or signs of myocardial reperfusion (inverted T waves).31 This represents the “golden hour” for reperfusion treatment. Many investigators have correlated ECG findings in acute STEMI with CA and found wide variation in sensitivity and specificity. A number of anatomic factors, easily appreciated from CA, affect the predictive power of the ECG in these situations.
Knowledge of morphologic ECG interpretation enables indi-vidual decision making in the acute phase of STEMI. Decisions about type of reperfusion therapy and where to send the patient (local hospital vs tertiary care center) can be based on the ECG findings and the clinical history of the patient.32 The diagnostic information in the ECG should also be used in the catheteriza-tion laboratory by the invasive cardiologist. Especially in mul-tivessel disease, where the infarct-related artery has opened, the ECG pinpoints the culprit lesion, which needs to be treated. In cases with cardiogenic shock, when ECG data for culprit artery identification are used optimally, a guiding catheter may be inserted immediately into the culprit artery, saving critical min-utes to open the occluded artery.
ANTERioR STEMi■■
In anterior STEMI, when the maximal ST-segment elevation is in leads V
2 to V
4, the culprit artery is almost exclusively the LAD.
In a minority of cases, the LM coronary artery, the LD, the LCx, or the RCA may be the culprit artery. In anterior STEMI, both the level of LAD occlusion and the size of the artery modify the ECG pattern. When the occlusion is proximal to the first LD branch, the anterolateral segment of the LV will be involved in the ischemic process, and ST-segment elevation will be present in lead aVL. Typically, reciprocal ST-segment depression is seen in lead III. However, if the LAD is large, wrapping around the LV apex, ischemia of two anatomically opposite regions, the anterolateral and the inferior, results in a cancellation of injury vectors, with resultant attenuation of the ST-segment elevations. If the occlusion is distal to the first diagonal branch, the size of the artery will determine the ECG pattern. In small LADs, the ST segments in the extremity leads will be isoelectric (anteroseptal
ischemia), whereas in large LADs, there will be ST-segment elevation in the inferior leads II, III, and aVF, with reciprocal ST-segment depression in lead aVL (see Fig. 4–5). In some cases with anterior STEMI with proximal occlusion of the LAD, there is no ST-segment elevation in lead aVL. Instead, the ECG shows ST-segment elevation in lead aVR and ST-segment depression in lead V
6.33
iNFERioR STEMi ■■
In patients with ST-segment elevation maximally in the inferior leads II, III, and aVF, the culprit artery is either the RCA or the LCx. Many different algorithms have been developed to deter-mine the infarct-related artery.34 These algorithms are mainly based on the fact that in RCA occlusions, the ischemic area is located more inferiorly and to the right, whereas in LCX occlu-sion, the injury vector points more into the posterior and lateral directions. In Figs. 4–1, 4–4, 4–5, and 4–10, anatomic aspects that determine the ECG patterns are presented. Involvement of the right ventricle induces ST-segment elevation in the right-sided precordial leads (V
3R-V
5R) and, in some cases, also in lead
V1 (- V
2 - V
3).
lATERAl STEMi ■■
When the maximal ST-segment elevation is in leads I, aVL, V5,
or V6, the LCx is usually the culprit artery (see Fig. 4–3). In addi-
tion, a few cases with distal LAD occlusions may present with this pattern due to apicolateral ischemia.
NoN–ST-SEgMENT ElEvATioN ACuTE CoRoNARy ■■SyNdRoMES
Information about coronary anatomy from the ECG is more limited in cases with non–ST-segment elevation acute coronary syndromes. However, there are situations where the CA find-ings can be predicted with high certainty. If the ECG shows widespread ST-segment depression, maximally in leads V
4
and V5 with inverted T waves in these leads, and concomitant
ST-segment elevation in lead aVR (circumferential subendo-cardial ischemia), there is a high probability of left main and/or severe three-vessel CAD.35 This represents a high-risk subgroup with a high in-hospital event rate. CA on an emergency basis is recommended. ST-segment depression maximally in the right-sided chest leads (irrespective of the direction of the T wave) represents a mirror-image STEMI, where the ischemia is on the posterior wall of the LV. Additional leads V
7 to V
9 typically show
ST elevations. The coronary artery occlusion is typically distal to the first obtuse marginal branch of a small LCx (see Fig. 4–10).
ANCILLARY METHODS TO STUDY ATHEROSCLEROTIC LESIONSCA quantifies luminal obstruction. The degree of stenosis is usu-ally reported by comparing diseased segments of the coronary tree with nearby segments without evident stenosis. However, CA is limited in its ability to quantitate the extent of distribution of atherosclerosis. The vessel lumen filled with contrast media
04-Wagner_Ch04_p_071-080.indd 77 12/18/10 10:10:49 AM

78 SECTioN i: Current Methods and Their Applications for Cardiovascular Multimodal imaging
is well appreciated by CA, but the method gives practically no information about the characteristics of the vessel wall. In cases with evenly distributed atherosclerotic plaques, the CA finding may even be interpreted as normal or near-normal. Advances in the understanding of the pathophysiology of atherosclerotic plaque demonstrate that in certain stages of plaque progression, the plaque is vulnerable to rupture. Vulnerable plaques may go undetected by CA. One clear advantage with CA is the pos-sibility to continue the diagnostic workup with other invasive methods with the patient still in the catheterization laboratory. Both anatomy and physiology of the coronary arteries can be easily studied with these ancillary methods.
iNTRAvASCulAR ulTRASouNd■■
Intravascular ultrasound (IVUS) visualizes the arterial wall in a format analogous to a histologic cross-section. IVUS provides detailed information about the quality and extent of atherosclerotic lesions in the vessel wall. IVUS is well suited as an ancillary method to CA to be performed simultaneously. The IVUS catheter is introduced into the coronary artery through a guiding catheter over a thin wire. Longitudinal or three-dimensional display of the coronary artery wall for tissue characterization is best performed with an automatic pullback device. Soft plaques can be differentiated from fibrotic lesions, and calcification within the vessel wall causes echo dropout behind the calcification. Thrombi and dissections are visible on IVUS. For diagnostic purposes, IVUS is indicated in bor-derline significant or angiographically suboptimally visualized lesions, such as tortuous coronary anatomy. IVUS studies have demonstrated that coronary atherosclerosis is more diffuse than appreciated by the use of CA.36 One drawback with IVUS is the lack of solid data for its value in guiding therapeutic decisions.
NovEl iNvASivE iMAgiNg ModAliTiES■■
Even higher resolutions of plaques are provided by optical coher-ence tomography, a catheter-based imaging modality introduced during the last few years.37,38 The method enables measurement of the thickness of the fibrous cap, which is considered critical for the risk of plaque disruption with sudden thrombotic vessel occlusion. Integrated backscatter analysis (“virtual histology”) converts radiofrequency backscatter signals provided by ultra-sound into color-coded regions to characterize different types of atherosclerotic plaques.38 The real value of these promising new methods to guide therapy needs to be proven.
iNvASivE EvAluATioN oF THE PHySiologiC ■■SigNiFiCANCE oF STENoTiC lESioNS
The presence of myocardial ischemia is an important risk factor
for an adverse clinical outcome. Revascularization of stenotic
coronary lesions that induce ischemia can improve a patient’s
functional status and outcome. For stenotic lesions that do not induce ischemia, however, the benefit of revascularization is less clear, and medical therapy alone is likely to be equally effective.39 Especially in patients with multivessel CAD, determining which
lesions cause ischemia and warrant stenting can be difficult. CA, the standard technique for guiding PCI in patients with multivessel CAD, may underestimate or overestimate a lesion’s
functional severity. Fractional flow reserve (FFR) is an index of the physiologic significance of a coronary stenosis and is defined as the ratio of maximal blood flow in a stenotic artery to normal maximal flow.40 It can be easily measured during CA
by calculating the ratio of distal coronary pressure measured
with a coronary pressure guidewire to aortic pressure measured
simultaneously with the guiding catheter. FFR in a normal coronary artery equals 1.0. An FFR value of 0.80 or less identifies ischemia-causing coronary stenoses with an accuracy of more than 90%.41 The information provided by FFR is similar to that obtained with myocardial perfusion studies, but it is more spe-cific and has a better spatial resolution because every artery or segment is analyzed separately and masking of one ischemic area by another, more severely ischemic zone is avoided. Deferring
PCI in nonischemic stenotic lesions as assessed by FFR is asso-ciated with an annual rate of death or myocardial infarction of approximately 1% in patients with single-vessel CAD, which is lower than the rate after routine stenting.39 However, deferring PCI in lesions with an FFR of less than 0.75 to 0.80 may result in worse outcomes than those obtained with revascularization.42 It was recently shown that routine measurement of FFR in patients with multivessel CAD who are undergoing PCI with drug-eluting stents significantly reduces the rate of the composite end point of death, nonfatal myocardial infarction, and repeat revascularization at 1 year.40
MULiTMoDULar iMaging in ConJUnCTion WiTh Coronary angiographyIt is not unusual to find normal or near-normal coronary arteries in patients with a clinical picture of acute coronary syndrome. Takotsubo cardiomyopathy, first described in Japan in 1991,43 is a cardiac syndrome characterized by ECG features mimicking acute STEMI, transient LV dysfunction, and minimal release of biomarkers of myocardial injury.44 LV ventriculography per-formed in conjunction with CA shows a typical pattern of apical dyskinesis and basal hyperkinesis.
Another clinical entity encountered in the era of invasive STEMI treatment is acute pulmonary embolism. Patients with acute chest discomfort and ST-segment elevations in the right precordial leads and angiographically normal coronary arteries typically show hyperkinetic contractions on LV ventriculogram. Bedside echocardiography can easily be performed after the invasive evaluation, followed by pulmonary angiography for definite diagnosis. In massive pulmonary embolism, catheter-directed thrombectomy can be performed with the patient in the catheterization laboratory through a transvenous catheter.45
ConCLUSionCA is the standard for identifying coronary artery narrowing related to CAD. New diagnostic methods like cardiac computed
04-Wagner_Ch04_p_071-080.indd 78 12/18/10 10:10:49 AM

79CHAPTER 4: Coronary Angiography
tomography allow noninvasive anatomic assessment of the coronary tree and offer alternatives especially for patients with low or intermediate probability for coronary artery stenoses. Available tests, including CA, all have advantages and draw-backs. The choice of imaging method should be tailored to each person based on the clinical judgment of patient risk, clinical history, and local expertise. CA will remain the method of choice in situations with high probability for an invasive thera-peutic procedure, especially in acute coronary syndromes.
rEFErEnCES 1. Scanlon PJ, Faxon DP, Audet AM, et al. ACC/AHA guidelines for coro-
nary angiography: executive summary and recommendations. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Coronary Angiography) developed in collaboration with the Society for Cardiac Angiography and Interventions. Circulation. 1999;99:2345-2357.
2. Fox K, Garcia MA, Ardissino D, et al. Guidelines on the management of stable angina pectoris: executive summary: the Task Force on the Management of Stable Angina Pectoris of the European Society of Cardiology. Eur Heart J. 2006;27:1341-1381.
3. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction–2002: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). Circulation. 2002;106:1893-1900.
4. Bertrand ME, Simoons ML, Fox KA, et al. Management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2002;23:1809-1840.
5. Antman EM, Hand M, Armstrong PW, et al. 2007 focused update of the ACC/AHA 2004 guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the Canadian Cardiovascular Society endorsed by the American Academy of Family Physicians: 2007 Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Management of Patients with ST-Elevation Myocardial Infarction, writing on behalf of the 2004 writing committee. Circulation. 2008;117:296-329.
6. Van de Werf F, Ardissino D, Betriu A, et al. Management of acute myocar- Van de Werf F, Ardissino D, Betriu A, et al. Management of acute myocar-Van de Werf F, Ardissino D, Betriu A, et al. Management of acute myocar-Management of acute myocar-dial infarction in patients presenting with ST-segment elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2003;24:28-66.
7. Reddy BK, Brewster PS, Walsh T, et al. Randomized comparison of rapid ambulation using radial, 4 French femoral access, or femoral access with AngioSeal closure. Catheter Cardiovasc Interv. 2004;62:143-149.
8. Principal Investigators of CASS and Their Associates. National Heart, Lung and Blood Institute Coronary Artery Surgery Study (CASS). Circulation. 1981;63(Suppl 1):I1-I81.
9. The BARI Protocol. Protocol for the Bypass Angioplasty Revascularization Investigation. Circulation. 1991;84(Suppl V):V-1–V-27.
10. Ambrose JA, Tannenbaum MA, Alexopoulos D, et al. Angiographic pro- Ambrose JA, Tannenbaum MA, Alexopoulos D, et al. Angiographic pro-Ambrose JA, Tannenbaum MA, Alexopoulos D, et al. Angiographic pro-Angiographic pro-gression of coronary artery disease and the development of myocardial infarction. J Am Coll Cardiol. 1988;12:56-62.
11. Manoharan G, Ntalianis A, Muller O, et al. Severity of coronary arte-rial stenoses responsible for acute coronary syndromes. Am J Cardiol. 2009;103:1183-1188.
12. Leaman DM, Brower RW, Meester GT, et al. Coronary artery atherosclero-sis: severity of the disease, severity of angina pectoris and compromised left ventricular function. Circulation. 1981;63:285-299.
13. Ryan TJ, Faxon DP, Gunnar RM, et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation. 1988;78:486-502.
14. Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention. 2005;1:219-227.
15. von Kodolitsch Y, Franzen O, Lund GK, et al. Coronary artery anoma- von Kodolitsch Y, Franzen O, Lund GK, et al. Coronary artery anoma-von Kodolitsch Y, Franzen O, Lund GK, et al. Coronary artery anoma-Coronary artery anoma-lies part II: recent insights from clinical investigations. Z Kardiol. 2005; 94:1-13.
16. Kim SY, Seo JB, Do KH, et al. Coronary artery anomalies: classification and ECG-gated multi-detector row CT findings with angiographic correlation. Radiographics. 2006;26:317-333.
17. Wesselhoeft H, Fawcett JS, Johnson AL. Anomalous origin of the left coro-nary artery from the pulmonary trunk. Its clinical spectrum, pathology, and pathophysiology, based on a review of 140 cases with seven further cases. Circulation. 1968;38:403-425.
18. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients under-going coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28-40.
19. Chaitman BR, Lesperance J, Saltiel J, et al. Clinical, angiographic, and hemodynamic findings in patients with anomalous origin of the coronary arteries. Circulation. 1976;53:122-131.
20. Sajja LR, Farooqi A, Shaik MS, et al. Dual left anterior descending coronary artery: surgical revascularization in 4 patients. Tex Heart Inst J. 2000;27:292-296.
21. Amoroso G, Battolla L, Gemignani C, et al. Myocardial bridging on left anterior descending coronary artery evaluated by multidetector computed tomography. Int J Cardiol. 2004;95:335-337.
22. Said SA, el Gamal MI, van der Werf T. Coronary arteriovenous fistulas: collective review and management of six new cases—changing etiology, presentation, and treatment strategy. Clin Cardiol. 1997;20:748-752.
23. McNamara JJ, Gross RE. Congenital coronary artery fistula. Surgery. 1969;65:59-69.
24. Rentrop KP, Cohen M, Blanke H, et al. Changes in collateral chan- Rentrop KP, Cohen M, Blanke H, et al. Changes in collateral chan-Rentrop KP, Cohen M, Blanke H, et al. Changes in collateral chan-Changes in collateral chan-nel filling immediately after controlled coronary artery occlusion by an angioplasty balloon in human subjects. J Am Coll Cardiol. 1985;5: 587-592.
25. The TIMI Study Group. The Thrombolysis in Myocardial Infarction (TIMI) trial: phase I findings. N Engl J Med. 1985;312:932-936.
26. Gibson CM, Murphy SA, Rizzo MJ, et al. Relationship between TIMI frame count and clinical outcomes after thrombolytic administration. Thrombolysis in Myocardial Infarction (TIMI) Study Group. Circulation. 1999;99:1945-1950.
27. van’t Hof AW, Liem A, Suryapranata H, et al. Angiographic assessment of myocardial reperfusion in patients treated with primary angioplasty for acute myocardial infarction: myocardial blush grade. Zwolle Myocardial Infarction Study Group. Circulation. 1998;97:2302-2306.
28. Gibson CM, Cannon CP, Murphy SA, et al. Relationship of TIMI myo- Gibson CM, Cannon CP, Murphy SA, et al. Relationship of TIMI myo-Gibson CM, Cannon CP, Murphy SA, et al. Relationship of TIMI myo-Relationship of TIMI myo-cardial perfusion grade to mortality after administration of thrombolytic drugs. Circulation. 2000;101:125-130.
29. Ding S, Pu J, Qiao ZQ, et al. TIMI myocardial perfusion frame count: a new method to assess myocardial perfusion and its predictive value for short-term prognosis. Catheter Cardiovasc Interv. 2010;75:722-732.
30. Sclarovsky S. Electrocardiography of Acute Myocardial Ischaemic Syndromes. London, United Kingdom: Martin Dunitz Ltd; 1999.
31. Eskola MJ, Holmvang L, Nikus KC, et al. The electrocardiogram window of opportunity to treat vs. the different evolving stages of ST-elevation myocardial infarction: correlation with therapeutic approach, coronary anatomy, and outcome in the DANAMI-2 trial. Eur Heart J. 2007;28: 2985-2991.
32. Nikus KC, Eskola MJ, Niemela KO, et al. Modern morphologic elec-trocardiographic interpretation—a valuable tool for rapid clinical deci-sion making in acute ischemic coronary syndromes. J Electrocardiol. 2005;38:4-6.
33. Eskola MJ, Nikus KC, Holmvang L, et al. Value of the 12-lead electrocar-diogram to define the level of obstruction in acute anterior wall myocardial infarction: correlation to coronary angiography and clinical outcome in the DANAMI-2 trial. Int J Cardiol. 2009;131:378-383.
34. Fiol M, Cygankiewicz I, Carrillo A, et al. Value of electrocardiographic algorithm based on “ups and downs” of ST in assessment of a culprit artery in evolving inferior wall acute myocardial infarction. Am J Cardiol. 2004;94:709-714.
35. Nikus KC, Eskola MJ, Virtanen VK, et al. ST-depression with negative T waves in leads V4-V5—a marker of severe coronary artery disease in non-ST elevation acute coronary syndrome: a prospective study of angina
04-Wagner_Ch04_p_071-080.indd 79 12/18/10 10:10:49 AM

80 SECTioN 1: Current Methods and their Applications for Cardiovascular Multimodal imaging
at rest, with troponin, clinical, electrocardiographic, and angiographic cor-relation. Ann Noninvasive Electrocardiol. 2004;9:207-214.
36. Mintz GS, Painter JA, Pichard AD, et al. Atherosclerosis in angiographi-cally “normal” coronary artery reference segments: an intravascular ultrasound study with clinical correlations. J Am Coll Cardiol. 1995;25: 1479-1485.
37. Prati F, Regar E, Mintz GS, et al. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: physical principles, methodology of image acquisition, and clinical applica-tion for assessment of coronary arteries and atherosclerosis. Eur Heart J. 2010;31:401-415.
38. Garcia-Garcia HM, Gonzalo N, Regar E, et al. Virtual histology and opti-cal coherence tomography: from research to a broad clinical application. Heart. 2009;95:1362-1374.
39. Pijls NH, van Schaardenburgh P, Manoharan G, et al. Percutaneous coro-nary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER study. J Am Coll Cardiol. 2007;49:2105-2111.
40. Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213-224.
41. Pijls NH, Van Gelder B, Van der Voort P, et al. Fractional flow reserve. A useful index to evaluate the influence of an epicardial coronary stenosis on myocardial blood flow. Circulation. 1995;92:3183-3193.
42. Legalery P, Schiele F, Seronde MF, et al. One-year outcome of patients submitted to routine fractional flow reserve assessment to determine the need for angioplasty. Eur Heart J. 2005;26:2623-2629.
43. Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultane- Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultane-Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultane-Myocardial stunning due to simultane-ous multivessel coronary spasms: a review of 5 cases. J Cardiol. 1991;21: 203-214.
44. Pernicova I, Garg S, Bourantas C, et al. Takotsubo cardiomyopathy: a review of the literature. Angiology. 2010;61:166-173.
45. Kuo WT, Gould MK, Louie JD, et al. Catheter-directed therapy for the treatment of massive pulmonary embolism: systematic review and meta-analysis of modern techniques. J Vasc Interv Radiol. 2009;20:1431-1440.
04-Wagner_Ch04_p_071-080.indd 80 12/18/10 10:10:49 AM