chapter 36 abdominal and genitourinary trauma. national ems education standard competencies trauma...
TRANSCRIPT

Chapter 36Chapter 36
Abdominal and Genitourinary Trauma

National EMS Education Standard CompetenciesNational EMS Education Standard Competencies
Trauma
Integrates assessment findings with principles of epidemiology and pathophysiology to formulate a field impression to implement a comprehensive treatment/disposition plan for an acutely injured patient.

National EMS Education Standard CompetenciesNational EMS Education Standard Competencies
Abdominal and Genitourinary Trauma
• Recognition and management of:− Blunt versus penetrating mechanisms
− Evisceration
− Impaled object

National EMS Education Standard CompetenciesNational EMS Education Standard Competencies
• Pathophysiology, assessment, and management of:− Solid and hollow organ injuries
− Blunt versus penetrating mechanisms
− Evisceration
− Injuries to the external genitalia
− Vaginal bleeding due to trauma
− Sexual assault
− Vascular injury
− Retroperitoneal injuries
IntroductionIntroduction
• Abdominal cavity extends from diaphragm to pelvis− Injuries can be life threatening.
− Contains several vital organ systems

IntroductionIntroduction
• Damage from trauma can be decreased by:− Empty bladder
− Toned abdominal muscles

IntroductionIntroduction
• Perform assessment and intervention quickly and cautiously.− Delays can have disastrous consequences.
− Blunt abdominal trauma is the leading cause of morbidity and mortality.

IntroductionIntroduction
• Trauma to the GU system can result from blunt or penetrating trauma− Consider when injuries involve:
• Lower rib cage
• Abdomen
• Pelvis
• Upper legs

IntroductionIntroduction
• Your field account is the only source of information for understanding the events and mechanism that led to trauma.− Critical for injuries that are not apparent

Anatomic RegionsAnatomic Regions
• Cavity extends from diaphragm to pelvic brim
• Divided into three sections:− Anterior abdomen
− Flanks
− Posterior abdomen

Anatomic RegionsAnatomic Regions
Anatomic RegionsAnatomic Regions
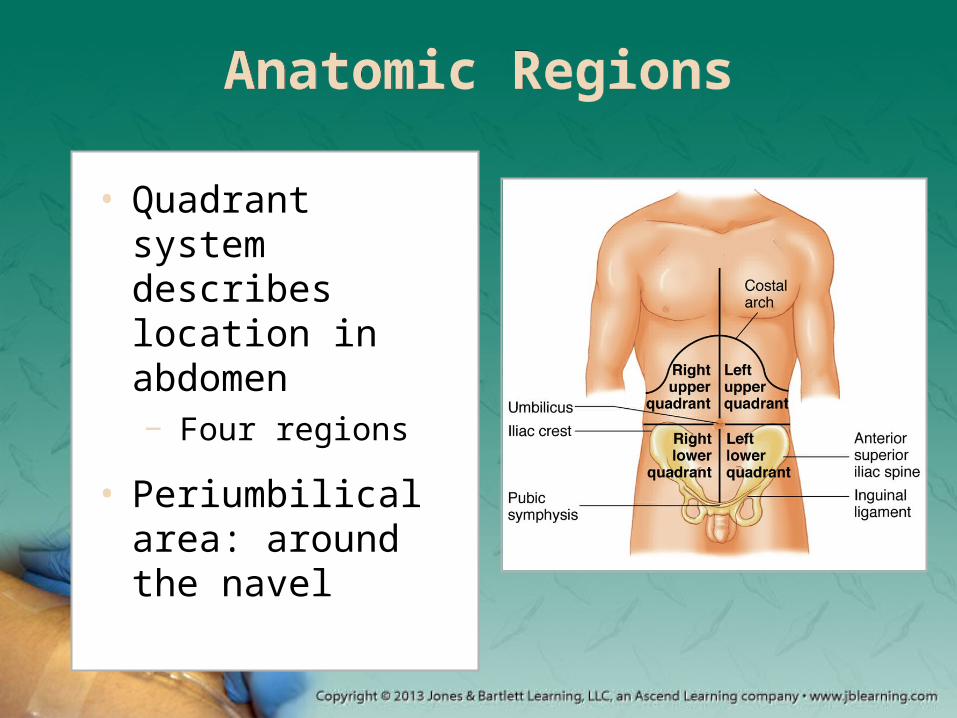
• Quadrant system describes location in abdomen− Four regions
• Periumbilical area: around the navel

Anatomic RegionsAnatomic Regions
• Peritoneum: membrane that lines the cavity
• Mesentery: double fold of tissue in abdomen

Anatomic RegionsAnatomic Regions
• Internally divided into three regions:− Peritoneal space
− Retroperitoneal space
− Pelvis

Anatomic RegionsAnatomic Regions

Abdominal Organs and Vital Vessels
Abdominal Organs and Vital Vessels
• Abdomen contains many organs− Solid organs
− Hollow organs
• Abdomen also contains vital vessels

Abdominal Organs and Vital Vessels
Abdominal Organs and Vital Vessels

Abdominal Organs and Vital Vessels
Abdominal Organs and Vital Vessels

Solid OrgansSolid Organs
• Liver: largest organ in the abdomen− Functions include:
• Detoxifying the blood
• Processing hemoglobin before it is stored
• Regulating blood clotting
• Removing bacteria from the bloodstream
• Regulating fat

Solid OrgansSolid Organs
• The spleen is highly vascular.− Functions include filtering and storing blood.
− If the body needs extra blood, the spleen provides it to the circulatory system.
− Detects pathogenic organisms and produces lymphocytes

Solid OrgansSolid Organs
• The pancreas is located under the liver and behind the stomach.− Acinar cells produce and secrete enzymes that
aid in digestion.
− Secretes insulin from the islets of Langerhans

Hollow OrgansHollow Organs
• The stomach is an intraperitoneal organ.− Concave on its right and convex on its left side
• Uppermost part: fundus
• Largest part: body
• Lower part: antrum

Hollow OrgansHollow Organs
• Three layers of the stomach wall:− Longitudinal
muscle
− Circular layer
− Oblique layer

Hollow OrgansHollow Organs
• Blood is supplied to the stomach from the celiac trunk.− Blood is returned via the portal vein
• The stomach contains acid to assist in digestion.
Hollow OrgansHollow Organs
• Small and large intestines − Run from stomach to
anus
− Digest and absorb water and nutrients
• Gallbladder− Saclike organ on the
lower surface of the liver
− Reservoir for bile

Hollow OrgansHollow Organs
• Duodenum: first part of the small intestine
• Pylorus: circumferential muscle at the end of the stomach
• Cecum: pouch at junction of small and large intestine

Hollow OrgansHollow Organs
• Colon: large intestine − Absorbs sodium and other ions
− Excretes other metallic ions into wastes
− The last 20 cm is the rectum.

Organs of the Genitourinary System
Organs of the Genitourinary System
• The abdomen contains organs of the urinary system.− Kidneys filter blood and excrete waste.
− Urinary bladder: hollow, muscular sac
− Ureters: thick-walled, hollow tubes

Organs of the Genitourinary System
Organs of the Genitourinary System
• The abdomen contains organs of the reproductive system.
The female reproductive system

Organs of the Genitourinary System
Organs of the Genitourinary System
The male reproductive system

The DiaphragmThe Diaphragm
• Dome-shaped muscle
• Separates the thoracic cavity from the abdominal cavity

PhysiologyPhysiology
• Some abdominal trauma can cause shock due to blood loss.− Bleeding may produce few signs and
symptoms.

PhysiologyPhysiology
• Organs most frequently injured after blunt trauma include:− Spleen and liver
• If a patient has unexplained symptoms of shock, suspect abdominal trauma.

PhysiologyPhysiology
• Hollow organs are more resilient.− More likely to be injured and burst when full
• May cause toxins to be released into the abdominal cavity
• Spillage can cause peritonitis.

PhysiologyPhysiology
• Two types of peritonitis:− Chemical peritonitis
• May have sudden onset
− Bacterial peritonitis • May develop over
several hours
• Also classified as: − Primary
• Infection travels from blood or lymph nodes into peritoneum.
− Secondary • Infection travels
from GI or biliary tract into the peritoneum.

Mechanism of InjuryMechanism of Injury
• Trauma is the leading cause of death in patients ages 1 to 44 years.− About 80% of all significant traumas involve the
abdomen.
Blunt TraumaBlunt Trauma
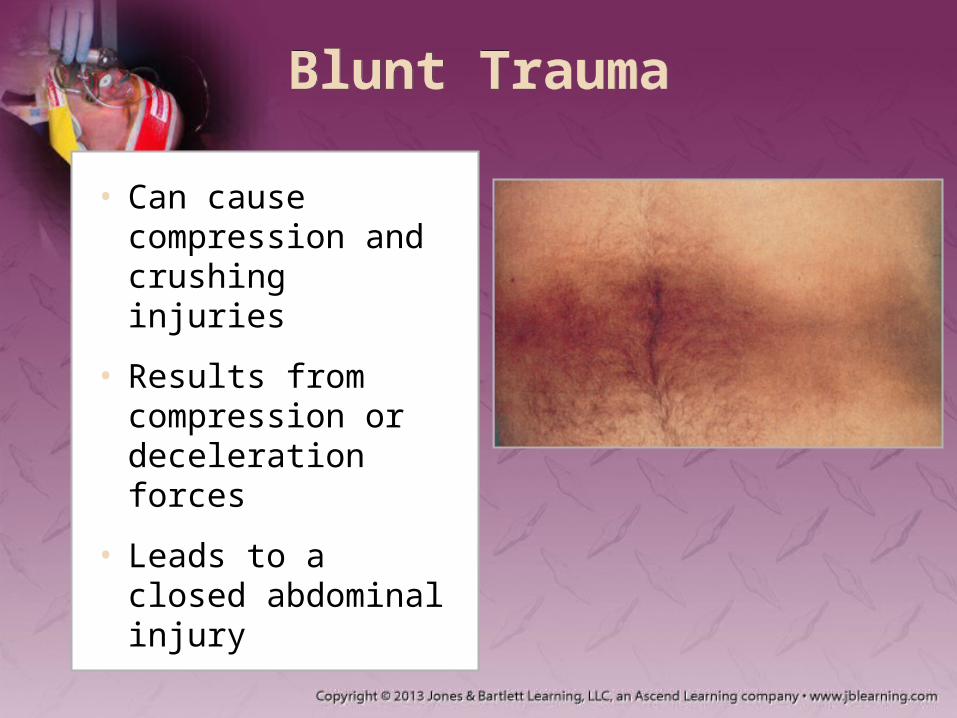
• Can cause compression and crushing injuries
• Results from compression or deceleration forces
• Leads to a closed abdominal injury

Blunt TraumaBlunt Trauma
• Common MOI—Shearing− Caused by rapid deceleration
• Organs continue forward motion, causing tear
− Signs of abdominal bleeding may include:• Referred shoulder pain
• Unexplained hypotension
• Multiple traumas present
Blunt TraumaBlunt Trauma
• Common MOI—Crushing− Abdominal contents are crushed between:
• Anterior abdominal wall, and
• Spinal column
− Results from direct strikes or falling objects

Blunt TraumaBlunt Trauma
• Common MOI—Compression− Results from direct blow or external
compression from a fixed object
− Forces will deform hollow organs.• Can rupture the small intestine or diaphragm

Penetrating TraumaPenetrating Trauma
• Results from low-velocity gunshot or stab wounds
• Causes an open abdominal injury
• Gunshot wounds cause more injury than stab wounds.

Penetrating TraumaPenetrating Trauma
• Damage is a function of energy imparted.− Kinetic energy = Mass/2 × Velocity2
− Velocity delivered is divided into three levels:• Low velocity (< 200 ft per second)
• Medium velocity (200–2,000 ft per second)
• High-velocity (> 2,000 ft per second)

Penetrating TraumaPenetrating Trauma
• Contributors to the extent of injury include: − Trajectory or direction the projectile traveled
− Distance the projectile traveled
− Profile of the bullet

Motor-Vehicle CrashesMotor-Vehicle Crashes
• Five typical patterns of impact − Frontal
− Lateral
− Rear
− Rotational
− Rollover

Motor-Vehicle CrashesMotor-Vehicle Crashes
− Ejection from vehicle
− Death of passenger
− Falls greater than 15′, or three times patient’s height
− Unrestrained occupants
− High-speed crash
− Pedestrian crash
− Motorcycle crash
− Penetrating wounds to head, chest, or abdomen
• Consider transporting the patient if one of the following is present:

Motor-Vehicle CrashesMotor-Vehicle Crashes
• Seat belts can cause blunt trauma to the abdominal organs.
Motorcycle Falls or CrashesMotorcycle Falls or Crashes
• No structural protection exists.− Protection: protective devices worn by driver
• Helmets do not protect for severe cervical injury.
− Consider transport to a trauma center with:• Crashes at speeds greater than 20 mph
• Separation of rider and motorcycle

Falls from HeightsFalls from Heights
• Body’s position or orientation determine types of injuries and survivability.
• Forces can be dissipated by:− Surface the person has fallen
− Degree to which surface can deform under force

Falls from HeightsFalls from Heights
• A fall produces acceleration at 9.8 m/sec2.− Height plus stopping distance predict magnitude
of forces.
• Transport patients to a trauma center if falls are greater than 20 ft.
Blast InjuriesBlast Injuries
• Generated fragments can travel at velocities of 4,500 fps
• Injuries may be from four mechanisms:• Primary blast
• Secondary blast
• Tertiary blast
• Quaternary blast

General PathophysiologyGeneral Pathophysiology
• Hemorrhage is a concern with abdominal trauma.− Estimation of blood volume lost is difficult.
− Signs and symptoms depend on:• Volume of blood lost
• Rate of loss

General PathophysiologyGeneral Pathophysiology
• Increased hypovolemia results in agitation and confusion.− The heart increases rate and stroke volume.
• Increased hypoperfusion leads to ischemia and heart failure.

General PathophysiologyGeneral Pathophysiology
• Injuries can result in organ spillage into the abdominal cavity.− Will eventually result in localized pain
• Localized if contamination is confined
• Generalized if entire peritoneal cavity is involved

Patient AssessmentPatient Assessment
• During evaluation, look for evidence of hemorrhage or spillage of bowel contents.− Have a high index of suspicion.
− Provide tissue perfusion and oxygen delivery.

Patient AssessmentPatient Assessment
• Evaluation must be systematic.
• Examine for: − Bruising
− Road rash
− Localized swelling
− Lacerations
− Distention or pain
© D
r. P
. Ma
razz
i/Pho
to R
ese
arc
he
rs, I
nc.

Patient AssessmentPatient Assessment
• Look for shock not proportional to external evidence.
• Abdominal organs are susceptible to significant bleeding. − Can be fatal

Patient AssessmentPatient Assessment
• When assessing a genitourinary injury:− Provide privacy for the patient.
− Look for blood on the undergarments.
− Only inspect the external genitalia if: • The patient reports pain.
• There are external signs of injury.

Scene Size-UpScene Size-Up
• Scene safety is priority.
• Penetrating or blunt trauma is caused by an external force.− Situation may be dangerous to the paramedic.

Primary AssessmentPrimary Assessment
• Form a general impression.− Note the manner in which the patient is lying.
• Body or abdominal movement irritates inflamed peritoneum.
• Patient may also present with guarding.

Primary AssessmentPrimary Assessment
• Airway and breathing− Keep airway clear of vomitus.
• Note the nature of the vomitus.
− Assess for adequate breathing.• Supplemental oxygen with a nonrebreathing mask
may be necessary.

Primary AssessmentPrimary Assessment
• Circulation− Superficial abdominal injuries usually don’t
produce external bleeding.
− To determine stage of shock, evaluate: • Pulse and skin color
• Temperature
• Condition

Primary AssessmentPrimary Assessment
• Circulation (cont’d)− When caring for genitourinary emergency,
remember the system is very vascular.
− To determine the presence of shock:• Assess pulse rate and quality.
• Determine skin condition, color, and temperature.
• Check capillary refill time.

Primary AssessmentPrimary Assessment
• Circulation (cont’d)− Closed injuries do not have visible signs of
bleeding.
− If the patient is visibly bleeding, control it.
− Consider the MOI, and expose that body part.

Primary AssessmentPrimary Assessment
• Transport decision− Abdominal injuries call for short on-scene time.
− Patients should be evaluated at the highest trauma center available.
Primary AssessmentPrimary Assessment
• Transport decision (cont’d)− Patients with a genitourinary system injury
should be taken to a trauma center.
− Treatment may require a specialist.

History TakingHistory Taking
− Types of vehicles
− Speed of travel
− How vehicles collided
− Other information:• Use of seat belts
• Air bag deployment
• Patient’s position
• Obtain the following with blunt trauma caused by a motor-vehicle crash:

History TakingHistory Taking
• If a patient has stab wounds, determine: − Type of knife
− Angle of entry
− Number of wounds
• In a gunshot case, determine: − Type of gun
− Number of shots
− Estimated distance

Secondary AssessmentSecondary Assessment
• Inspect the abdomen.− May involve ecchymosis, abrasions, lacerations
− Note blood from vagina or rectum.
− Peritonitis could result in decreased or absent abdominal sounds.

Secondary AssessmentSecondary Assessment
• Perform palpation and percussion.− Start with the quadrant furthest from injury.
• Note whether the patient has hematuria.− Dark brown: bleeding in upper urinary tract
− Bright red: bleeding in lower portion of tract

Secondary AssessmentSecondary Assessment
• Determine if the patient is pregnant.− Risk of massive blood loss is increased
− Management should start with the ABCs.
− Tilt patients at least 15° to the left to prevent vena cava syndrome.

Secondary AssessmentSecondary Assessment
• New technologies include:− Portable ultrasound machines
− Telemedicine
• Misconception: patients without pain or abnormal vital signs are unlikely to have serious injuries.

Secondary AssessmentSecondary Assessment
• Abdominal trauma may include:− Abdominal
evisceration
− Injury to the diaphragm
• Signs of rupture may include:− Abdominal pain
− Abdominal sounds in the chest
− Sunken abdomen

Secondary AssessmentSecondary Assessment
• Examine the patient’s neck and chest.
• Assess the patient’s pain.− Somatic pain: sharp and localized
− Visceral pain: deep aching with cramping

Secondary AssessmentSecondary Assessment
• Perform a thorough full-body exam. − Conduct en route.
− Assess the same structures as the rapid exam but more methodically.

ReassessmentReassessment
• Field documentation should include:− Seat belt use
− Location, intensity, quality of pain
− Nausea or vomiting
− Contour of abdomen
− Ecchymosis or open areas on soft-tissue
− Rebound tenderness, guarding, rigidity, spasm, localized pain

ReassessmentReassessment
• Field documentation should include (cont’d):− Changes in LOC and vital signs
− Other injuries found
− Alcohol, narcotics, analgesic
− Results of assessment

Emergency Medical CareEmergency Medical Care
• Ensure an open airway.
• Establish IV access.
• Apply pressure dressings if necessary.
• Apply a: − Cardiac monitor
− Pulse oximetry
− Capnography
• Transport to a hospital or trauma center.

Emergency Medical CareEmergency Medical Care
• Administering pain medication is controversial.− Consult with medical direction en route.

EviscerationEvisceration
• Protrusion of abdominal organs through a wound− Apply a sterile
dressing over the evisceration.
− Transport to the closest hospital.

EviscerationEvisceration
• Strangulation of the bowel causes decreased blood flow to the protruding part.
• Patients may feel more comfortable with knees bent.− Encourage not to cough or bear down.

Impaled ObjectsImpaled Objects
• Stabilize the object.
• Transport patient in the position found.
• Significant infection may develop.− Intervene early.
© C
ust
om
Med
ica
l Sto
ck P
ho
to

Pathophysiology of Specific Injuries
Pathophysiology of Specific Injuries
• Abdominal trauma can be life threatening.− May bleed profusely
− May produce peritonitis and systemic infection

Injuries to Solid Abdominal Organs
Injuries to Solid Abdominal Organs
• Liver injuries− Suspect with:
• Right-sided chest and abdominal trauma
• Fractures to the 7th and 9th ribs
− Suspect laceration when penetration involves: • Right upper abdomen
• Right lower chest

Injuries to Solid Abdominal Organs
Injuries to Solid Abdominal Organs
• Spleen injuries− Ruptured spleens have been reported in cases
where contact was minor.• If ruptured, blood spills into the peritoneum.

Injuries to Solid Abdominal Organs
Injuries to Solid Abdominal Organs
• Spleen injuries (cont’d)− Suspect spleen lacerations if:
• 9th through 10th ribs are fractured
• Left upper quadrant tenderness
• Hypotension
• Tachycardia
• Left shoulder pain appears 1 to 2 hours after injury

Injuries to Solid Abdominal Organs
Injuries to Solid Abdominal Organs
• Pancreas injuries− High-energy forces are needed to damage
− Patients present with vague upper and midabdominal pain radiating into the back.

Injuries to Solid Abdominal Organs
Injuries to Solid Abdominal Organs
• Diaphragm injuries− Signs and symptoms: ventilatory compromise
− Injuries are not isolated.
− May result from blunt and penetrating trauma

Injuries to Hollow Intraperitoneal Organs
Injuries to Hollow Intraperitoneal Organs
• Injuries to the small and large intestines− Most common from penetrating trauma
− Rupture causes peritonitis.
− Stomach rupture causes: • Rapid burning epigastric pain
• Rigidity
• Rebound tenderness

Injuries to Hollow Intraperitoneal Organs
Injuries to Hollow Intraperitoneal Organs
• Stomach injuries− Commonly result from penetrating trauma
− Trauma results in the spilling of acidic material.
− Antacid medications may delay symptoms.

Retroperitoneal InjuriesRetroperitoneal Injuries
• Injuries to this area do not present with signs and symptoms of peritonitis.− Occasionally bleeding can lead to:
• Grey Turner sign
• Cullen sign

Vascular InjuriesVascular Injuries
• Penetrating trauma is the major cause.
• Often masked by other injuries
• Significance depends on: − How many vessels were injured
− length of time since the injury

Duodenal InjuriesDuodenal Injuries
• Rupture may occur in high-speed deceleration injuries.− Contents spill into the retroperitoneum.
− Contamination causes abdominal pain or fever.
• Close proximity to other organs
Kidney InjuriesKidney Injuries
• Generally caused by large forces
• Suspect injury with: − Fractures of the
11th and 12th ribs
− Flank tenderness

Kidney InjuriesKidney Injuries
• Rupture presents with: − Pain on inspiration
− Gross hematuria
• Penetrating renal trauma occurs with wounds in the abdomen or lower chest.

Ureter InjuriesUreter Injuries
• Difficult to identify
• Rarely lead to an immediate life-threatening condition

Bladder and Urethra InjuriesBladder and Urethra Injuries
• Associated with other significant injuries
• May result in bladder rupture or laceration− Based on severity of mechanism and degree of
bladder distention
• Usually associated with pelvic injuries

Bladder and Urethra InjuriesBladder and Urethra Injuries
• Rupture is associated with a high mortality rate.− Trauma often causes damage to other organs
or vascular structures.
− Urine may spill into the abdominal cavity.

Assessment of Specific Injuries
Assessment of Specific Injuries
• Signs may not develop until a significant amount of blood is lost.− Bleeding can cause tenderness or distention.
• Liver injuries result in blood and bile into the peritoneal cavity.
Assessment of Specific Injuries
Assessment of Specific Injuries
• Signs/symptoms of splenic rupture are nonspecific.− Only Kehr sign
may be present.

Assessment of Specific Injuries
Assessment of Specific Injuries
• Pancreatic injuries have subtle or absent signs.− Suspect after localized blow to the midabdomen
− Patients report vague upper and midabdomenal pain radiating to the back.

Assessment of Specific Injuries
Assessment of Specific Injuries
• Findings of vascular injures depends on whether or not the bleeding is contained.
• Blunt renal trauma may present as flank pain and hematuria.

Assessment of Specific Injuries
Assessment of Specific Injuries
• Suspect bladder injury if: − Trauma to the lower abdomen or pelvis
− Inability to urinate
− Blood in the penile opening
− Tenderness on palpation of suprapubic region
• Signs and symptoms are nonspecific.

Assessment of Specific Injuries
Assessment of Specific Injuries
• Signs of peritoneal irritation may indicate intraperitoneal bladder rupture.
• Ultrasound may be used in the field.

Management of Specific Injuries
Management of Specific Injuries
• Maintain a high index of suspicion.
• Management of solid organ injuries includes: − Providing rapid transport
− Monitoring vital signs

Management of Specific Injuries
Management of Specific Injuries
• Care of bladder and urethra injuries: − Secure the airway.
− Address breathing issues.
− Support the circulatory system.
− Immobilize the spine if necessary.

Pathophysiology of Injuries to the Male Genitalia
Pathophysiology of Injuries to the Male Genitalia
• Injuries to the testicle or scrotal sac− Loss of fertility is the major concern.
− Blunt trauma is caused by motor vehicle crashes, physical assaults, sports injuries
− Penetrating trauma is caused by stabbings, gunshots, blasts, or animal bites
Pathophysiology of Injuries to the Male Genitalia
Pathophysiology of Injuries to the Male Genitalia
• Penis injuries− Priapism can have nontraumatic causes.
− A fractured penis may occur if erect and: • Impacted against partner’s pubic symphysis
• Bent too far via self-manipulation

Assessment of Injuries to the Male Genitalia
Assessment of Injuries to the Male Genitalia
• Contusions result in painful hematomas.
• Rupture and torsion are difficult to identify.
• Intrascrotal bleeding does not require much force.
Assessment of Injuries to the Male Genitalia
Assessment of Injuries to the Male Genitalia
• Penile fracture may present as pain and a large hematoma.
• When penetrating trauma occurs:− Control hemorrhage.
− Assess the patient for other injuries.

Management of Injuries to the Male Genitalia
Management of Injuries to the Male Genitalia
• Treat with attention to hemorrhage or evisceration.− Apply gentle compression and ice packs.
− Provide pain relief and emotional support.

Management of Injuries to the Male Genitalia
Management of Injuries to the Male Genitalia
• If Fournier gangrene occurs, provide prompt transport to the hospital.
• Attempt to recover an amputated penis.
• If an object is placed around the penis or testicles, do not attempt removal.

Pathophysiology of Injuries to the Female Genitalia
Pathophysiology of Injuries to the Female Genitalia
• Blunt trauma may result from: − Motor vehicle crashes
− Saddle type injuries
• Penetrating trauma may result from: − Stabbings to the lower
pelvis
− Gunshot wounds

Assessment of Injuries to the Female Genitalia
Assessment of Injuries to the Female Genitalia
• Signs of trauma may include: − Hematomas and ecchymosis
− Bleeding from the vagina
− Tenderness on palpation of the lower pelvis

Management of Injuries to the Female Genitalia
Management of Injuries to the Female Genitalia
• Use compression for external hemorrhage.
• Administer replacement fluids if hypotensive.
• Do not attempt to remove any object that is stuck in the vaginal canal.

SummarySummary
• Unrecognized abdominal trauma is the leading cause of unexpected death in trauma patients.
• The abdomen contains many vital organs and structures.
• The quadrant system is generally used to describe a location in the abdomen.
• The peritoneum is a membrane that lines the abdominal cavity. Abdominal trauma can lead to peritonitis.
SummarySummary
• The retroperitoneal space is the area behind the peritoneum.
• When a patient has experienced trauma to the chest or abdomen, you should suspect that he or she also has additional internal abdominal injuries.
• Injury to the abdomen may be slow to develop, and can be fatal.

SummarySummary
• Solid organs have a large blood supply and can easily be crushed by blunt trauma.
• Injury to hollow organs can cause the release of toxins into the abdominal cavity, causing major peritonitis.
• At least two thirds of all abdominal injuries involve blunt trauma.
• Penetrating trauma causes open abdominal injury.
SummarySummary
• During assessment, note the manner in which the patient is lying. Prioritize the ABCs.
• Assessment should never delay patient care and transport!
• Try to obtain as many details about an injury as possible.
• Peritonitis can take hours to days to develop.

SummarySummary
• Generally, management of patients with abdominal trauma is straightforward:− Ensure a secure airway.
− Establish intravenous access and fluid replacement.
− Minimize hemorrhaging with pressure dressings.
− Apply a cardiac monitor and oxygen therapy, and then transport.

SummarySummary
• Pelvic fractures can result in damage to the major vascular structures.
• Because of the forces required to break the pelvis, if the patient has a pelvic fracture, suspect multisystem trauma.

CreditsCredits
• Chapter opener: © Mark C. Ide
• Backgrounds: Green–Jones & Bartlett Learning; Purple–Jones & Bartlett Learning. Courtesy of MIEMSS; Blue–Courtesy of Rhonda Beck; Red–© Margo Harrison/ShutterStock, Inc.
• Unless otherwise indicated, all photographs and illustrations are under copyright of Jones & Bartlett Learning, courtesy of Maryland Institute for Emergency Medical Services Systems, or have been provided by the American Academy of Orthopaedic Surgeons.