chapter 27 essential concepts in molecular pathology companion site for molecular pathology author:...
TRANSCRIPT

Chapter 27Essential Concepts in Molecular
Pathology
Companion site for Molecular PathologyAuthor: William B. Coleman and Gregory J. Tsongalis
Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
2
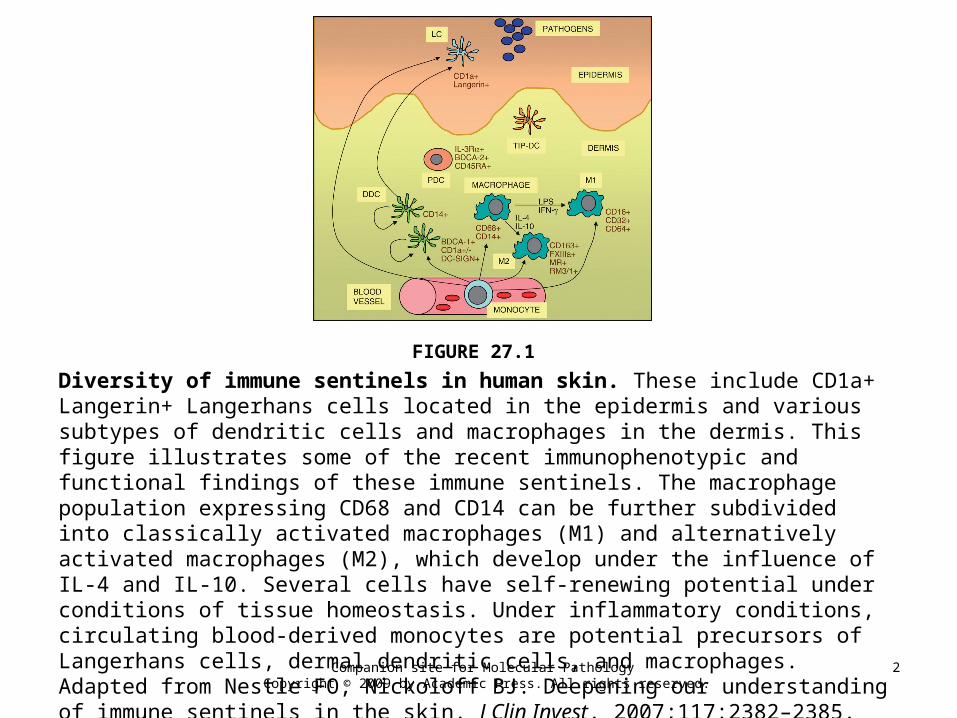
FIGURE 27.1
Diversity of immune sentinels in human skin. These include CD1a+ Langerin+ Langerhans cells located in the epidermis and various subtypes of dendritic cells and macrophages in the dermis. This figure illustrates some of the recent immunophenotypic and functional findings of these immune sentinels. The macrophage population expressing CD68 and CD14 can be further subdivided into classically activated macrophages (M1) and alternatively activated macrophages (M2), which develop under the influence of IL-4 and IL-10. Several cells have self-renewing potential under conditions of tissue homeostasis. Under inflammatory conditions, circulating blood-derived monocytes are potential precursors of Langerhans cells, dermal dendritic cells, and macrophages. Adapted from Nestle FO, Nickoloff BJ. Deepening our understanding of immune sentinels in the skin. J Clin Invest. 2007;117:2382–2385.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
3
FIGURE 27.2
Genomic and functional domain organization of the transcription factor p63. At least six different isoforms can be generated by use of alternative translation initiation sites or alternative splicing. The main isoform expressed in human skin is ΔNp63α. Autosomal dominant mutations in the DNA binding domain of the p63 gene lead to ectrodactyly, ectodermal dysplasia, and clefting (EEC) syndrome. In contrast, autosomal dominant mutations in the SAM domain result in ankyloblepharon, ectodermal dysplasia, and clefting (AEC) syndrome. A number of other ectodermal dysplasia syndromes may also result from mutations in the p63 gene.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
4
FIGURE 27.3
Illustration of the integral structural macromolecules present within hemidesmosome-anchoring filament complexes and the associated forms of clinical epidermolysis bullosa that result from autosomal dominant or autosomal recessive mutations in the genes encoding these proteins.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
5
FIGURE 27.4
Clinico-pathological consequences of mutations in the gene encoding keratin 14 (KRT14), the major intermediate filament protein in basal keratinocytes. (A) The clinical picture shows autosomal dominant Dowling-Meara epidermolysis bullosa simplex. (B) The electron micrograph shows keratin filament clumping and basal keratinocyte cytolysis (bar = 1 μm).

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
6
FIGURE 27.5
Spectrum of clinical abnormalities associated with dominant mutations in keratin 5 (KRT5). (A) Missense mutations in the nonhelical end domains result in the most common form of EB simplex, which is localized to the hands and feet (Weber-Cockayne variant). (B) A specific mutation in keratin 5, p.P25L, is the molecular cause of epidermolysis bullosa simplex associated with mottled pigmentation. (C) Heterozygous nonsense or frame shift mutations in the KRT5 gene leads to Dowling-Degos disease.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
7
FIGURE 27.6
Laminin-332 mutations result in junctional epidermolysis bullosa. (A) Laminin-332 consists of three polypeptide chains: α3, β3, and γ2. (B) Immunogold electron microscopy shows laminin-332 staining at the interface between the lamina lucida and lamina densa subjacent to a hemidesmosome (bar = ?50 nm). (C) Loss-of-function mutations in any one of these genes encoding the three polypeptides chains results in Herlitz junctional epidermolysis bullosa, which is associated with a poor prognosis, usually with death in early infancy.
Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
8
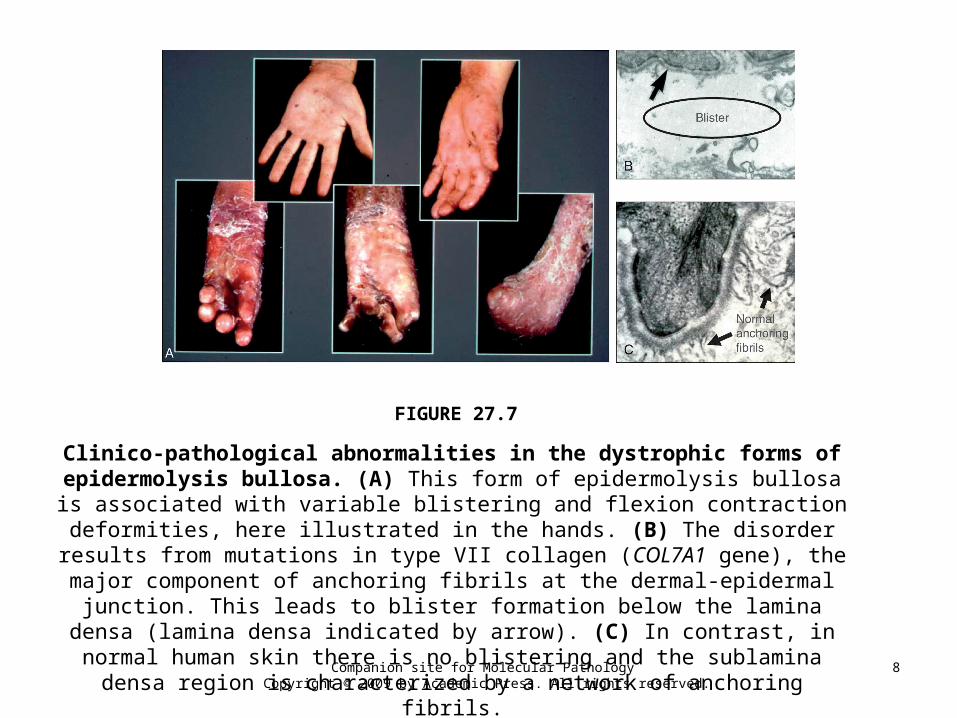
FIGURE 27.7
Clinico-pathological abnormalities in the dystrophic forms of epidermolysis bullosa. (A) This form of epidermolysis bullosa is associated with variable blistering
and flexion contraction deformities, here illustrated in the hands. (B) The disorder results from mutations in type VII collagen (COL7A1 gene), the major component of
anchoring fibrils at the dermal-epidermal junction. This leads to blister formation below the lamina densa (lamina densa indicated by arrow). (C) In contrast, in normal human skin there is no blistering and the sublamina densa region is characterized by
a network of anchoring fibrils.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
9
FIGURE 27.8
Protein composition of the desmosome linking two adjacent keratinocytes. The major transmembranous proteins are the desmogleins
and the desmocollins. Several desmosomal plaque proteins, including desmoplakin, plakophilin, and plakoglobin, provide a bridge that links
binding between the transmembranous cadherins and the keratin filament network within keratinocytes.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
10
FIGURE 27.9
Clinical abnormalities associated with inherited gene mutations in desmosome proteins. (A) Recessive mutations in plakophilin 1 result in nail dystrophy and skin
erosions. (B) Woolly hair is associated with several desmosomal gene abnormalities, particularly mutations in desmoplakin. (C) Recessive mutations in plakophilin 1 can
result in extensive neonatal skin erosions, particularly on the lower face. (D) Recessive mutations in desmoplakin can lead to skin blistering. (E) Autosomal
dominant mutations in desmoplakin do not result in blistering, but can lead to striate palmoplantar keratoderma.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
11
FIGURE 27.10
Abnormalities and therapeutic potential for inflamed skin in psoriasis. There is increasing evidence for a role of tissue resident immune cells in the
immunopathology of psoriasis. New therapies may be developed by (1) antagonizing local cytokines and chemokines, such as IFN-α; (2) blocking of adhesion molecules
(e.g., integrins) and costimulatory molecules within the tissue; (3) modification of keratinocyte proliferation and differentiation (e.g., use of corticosteroids or vitamin D
preparations); (4) blocking of entry of dermal T-cells into the epidermis; and (5) modification of the micro-environment, including the extracellular matrix. Adapted from Boyman O, Conrad C, Tonel G, et al. The pathogenic role of tissue-resident
immune cells in psoriasis. Trends Immunol. 2007;28:51–57.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
12
FIGURE 27.11
Clinical pathology resulting from auto-antibodies against desmosomes or hemidesmosomes. (A) Pemphigus vulgaris resulting
from antibodies against desmoglein 3. (B) Bullous pemphigoid associated with antibodies against type XVII collagen. (C) Mucous membrane
pemphigoid associated with antibodies to laminin-332..

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
13
FIGURE 27.12
Illustration of hemidesmosomal structural proteins and the autoimmune diseases associated with antibodies directed against these individual
protein components.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
14
FIGURE 27.13
Salt-split skin technique to diagnose immunobullous disease. Incubation of normal human skin in 1 M NaCl overnight at 4°C results in cleavage through the
lamina lucida. This results in separation of some proteins to the roof of the split and some to the base (above and below pink line on the schematic). In the skin labeling shown, immunoglobulin from a patient's serum binds to the base of salt-split skin.
Further analysis revealed that the antibodies were directed against type VII collagen. This technique is useful in delineating bullous pemphigoid from epidermolysis bullosa
acquisita, both of which are associated with linear IgG at the dermal-epidermal junction in intact skin.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
15
FIGURE 27.14
Clinical consequences of disruption of desmoglein 1 in human skin. (A) Staphylococcal toxins cleave the extracellular part of desmoglein 1 and
result in staphylococcal scalded skin syndrome. (B) Inherited autosomal dominant mutations in desmoglein 1 can result in striate palmoplantar
keratoderma. (C) Auto-antibodies against desmoglein 1 result in pemphigus foliaceus, which is associated with superficial blistering and crusting in
human skin.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
16
FIGURE 27.15
The SHH signaling pathway. (A) In the absence of SHH, PATCHED constitutively represses smoothened, a transducer of the SHH signal. (b) Binding of the ligand SHH to PTCH relieves its inhibition of SMO and transcriptional activation occurs through the GLI family of proteins, resulting in activation of target genes. (c) Mutations in SHH or PTCH or SMO may be associated with basal cell carcinomas, both in sporadic tumors as well as in certain genodermatoses, such as xeroderma pigmentosum, that are associated with an increased risk of BCC. Germinal mutations in the PTCH gene underlie Gorlin's syndrome.(Based on original figures published by (2)).

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
17
FIGURE 27.16
Potential for targeted therapies in melanoma. Recent improvement in defining the genetics of melanoma has led to the development of targeted therapeutic agents that are directed at specific molecular aberrations involved in tumor proliferation and resistance to chemotherapy.Adapted from Singh M, Lin J, Hocker TL, et al. Genetics of melanoma tumorigenesis. Br J Dermatol. 2008;158:15–21.

Companion site for Molecular Pathology Copyright © 2009 by Academic Press. All rights reserved.
18
FIGURE 27.17
Roles for chemokine receptors and possible therapeutic manipulation in cutaneous T-cell lymphoma. Chemokine receptors may have important roles in enabling malignant T-cells to enter and survive in the skin. (1) Homing: Activation of T-cell integrins permits T-cell adhesion to endothelial cells in the skin and subsequent binding to extracellular matrix proteins. T-cells can then migrate along a gradient of chemokines (e.g., CCL17 and CCL27) to the epidermis. (2) Activation: chemokine receptors allow T-cells to interact with dendritic cells such as Langerhans cells, leading to T-cell activation and release of inflammatory cytokines. (3) Inhibition of apoptosis: chemokine receptor engagement can lead to up-regulation of PI3K and AKT, which are pro-survival kinases. T-cells can therefore survive and proliferate in the skin. (4) Chemokine-antigen fusion proteins can be used to target tumor antigens from cutaneous T-cell lymphoma cells to CCR6+ presenting dendritic cells that can stimulate host anti-tumor immunity. (5) Chemokine toxin molecules can also target specific chemokine receptors found on cutaneous T-cell lymphoma cells to mediate direct killing.Adapted from Hwang ST, Janik JE, Jaffe ES, et al. Mycosis fungoides and Sezary syndrome. Lancet. 2008;371:945–957.