chapter 20:radiation biology - human health campus · repairing radiation-induced dna damage...
TRANSCRIPT
IAEAInternational Atomic Energy Agency
Slide set of 97 slides based on the Chapter authored by
J. WONDERGEM
of the IAEA publication (ISBN 978-92-0-131010-1):
Diagnostic Radiology Physics:
A Handbook for Teachers and Students
Objective:
To familiarize students with the action of ionizing radiation
on living matter.
Chapter 20: Radiation Biology
Slide set prepared
by E.Okuno (S. Paulo, Brazil,
Institute of Physics of S. Paulo University)

IAEA
20.1. Introduction
20.2. Radiation Injury to DNA
20.3. DNA Repair
20.4. Radiation-Induced Chromosome Damage and Biological Dosimetry
20.5. The Cell Cycle
20.6. Survival Curve Theory
20.7. Concepts of Cell Death
20.8. Cellular Recovery Processes
20.9. Relative Biological Effectiveness
20.10. Carcinogenesis (Stochastic)
20.11. Radiation Injury to Tissues (Deterministic)
20.12. Radiation Pathology; Acute and Late Effects
20.13. Radiation Genetics: Radiation Effects on Fertility
20.14. Foetal Irradiation
Chapter 20. TABLE OF CONTENTS
Diagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,2

IAEA
20.1. INTRODUCTION
Diagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,3
• Radiation biology (radiobiology) is the study of the
action of ionizing radiations on living matter
• physical
• chemical
• biological
variables that affect
dose response at the
cellular
tissue
whole body
levels at dose and dose
rates relevant to
diagnostic radiology
An overview of the biological effects of ionizing radiation is
given, with attention paid to the:
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,4
20.1. INTRODUCTION
20.1.1. Deterministic and stochastic responses
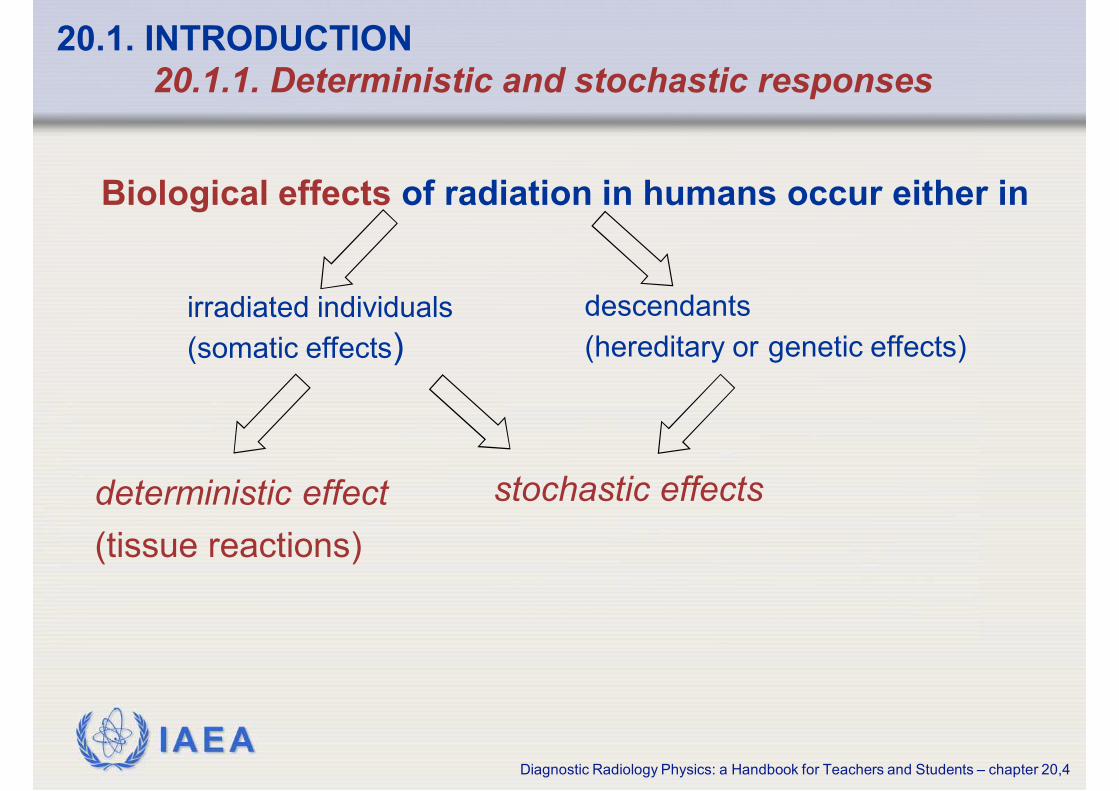
Biological effects of radiation in humans occur either in
irradiated individuals
(somatic effects)
descendants
(hereditary or genetic effects)
deterministic effect
(tissue reactions)
stochastic effects

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,5
• Result from cell loss or damage e.g. moist desquamation from
interventional cardiology
• Most organs or tissues of the body are unaffected by the loss of a few
cells, however, if the number of cells lost is sufficiently large, there is
observable harm and hence loss of tissue/organ function
• Above a threshold dose, the severity of the effect necessarily increases
with increasing dose. This threshold varies from one effect to another
• May occur a few hours or days after exposure (i.e. early skin reaction)
or may require months or years before expression (i.e. cataract of the
eye lens)
20.1. INTRODUCTION
20.1.1. Deterministic and stochastic responses
Deterministic effects

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,6
20.1. INTRODUCTION
20.1.1. Deterministic and stochastic responses
Stochastic effects
• Are probabilistic effects: the probability of the occurrence of an effect is
a function of dose
• The severity of an effect is not a function of dose
• The probability of the occurrence of an effect increases with dose
• Are assumed to exhibit no threshold dose below which they cannot
occur
• The major stochastic effects of concern at typical diagnostic radiology
levels are cancers and genetic effects. They are exclusively late effects
because they do not appear until years after radiation exposures

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,7
20.1. INTRODUCTION
20.1.2. Diagnostic radiology
There is a large range in
the amount of radiation
dose given by various
diagnostic procedures
0 2 4 6 8 10 12 14
1997–2007
1991–1996
1980–1990
1970–1979
Health care level I (UNSCEAR report 2008)
Average effective dose per examination (mSv)
Angiography
CT scan
Mammography
Abdomen X-ray
Chest radiography
In a small number of procedures, radiation damage to tissue
can occur in skin reactions from long interventional procedures

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,8
20.1. INTRODUCTION
20.1.2. Diagnostic radiology
• The amount of energy deposited in the tissue of patients as a
result of diagnostic radiology examinations or interventional
procedures is typically a number of orders of magnitude less than
delivered during radiation oncology
Consequently the detriment caused is largely confined to
stochastic effects
• The occupational dose, although orders of magnitude lower than
that of the patient during a single procedure, may become
considerable for a worker performing large numbers of procedures,
and especially if needed shielding precautions are not observed
Consequently there is an increasing incidence of injury to the lens
of the eye for some workers, for example, during interventional
procedures
patient
worker

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,9
20.1. INTRODUCTION
20.1.3. International Organisations on Radiation effects
BEIR (Biological Effects of
Ionizing Radiation)
UNSCEAR (United Nations
Scientific Committee on the
Effects of Atomic Radiation)
ICRP(International Commission
on Radiological Protection)
is involved in recommendation
and development of guidelines in
the field of radiation protection
Collect and analyze data from the
recent literature regarding
biological effects of ionizing
radiation
Report periodically on risk
estimates for radiation induced
cancer and hereditary effects

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,10
20.2. RADIATION INJURY TO DNA
20.2.1. Structure of DNA
Deoxyribonucleic acid (DNA) contains the genetic
information of the cell
Ref. Nature, vol 171, page 737, 1953
J. D. WATSON and F. H. C. CRICK
• The backbone of the DNA strand is made of
alternating sugar and phosphate groups
• A nucleotide is a subunit of DNA, and is
composed of a “base” linked to a sugar
(deoxyribose) and a phosphate group
• DNA is a large molecule and has a characteristic
double-helix structure consisting of
two strands, each made up of a sequence of
nucleotides
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,11
20.2. RADIATION INJURY TO DNA
20.2.1. Structure of DNA
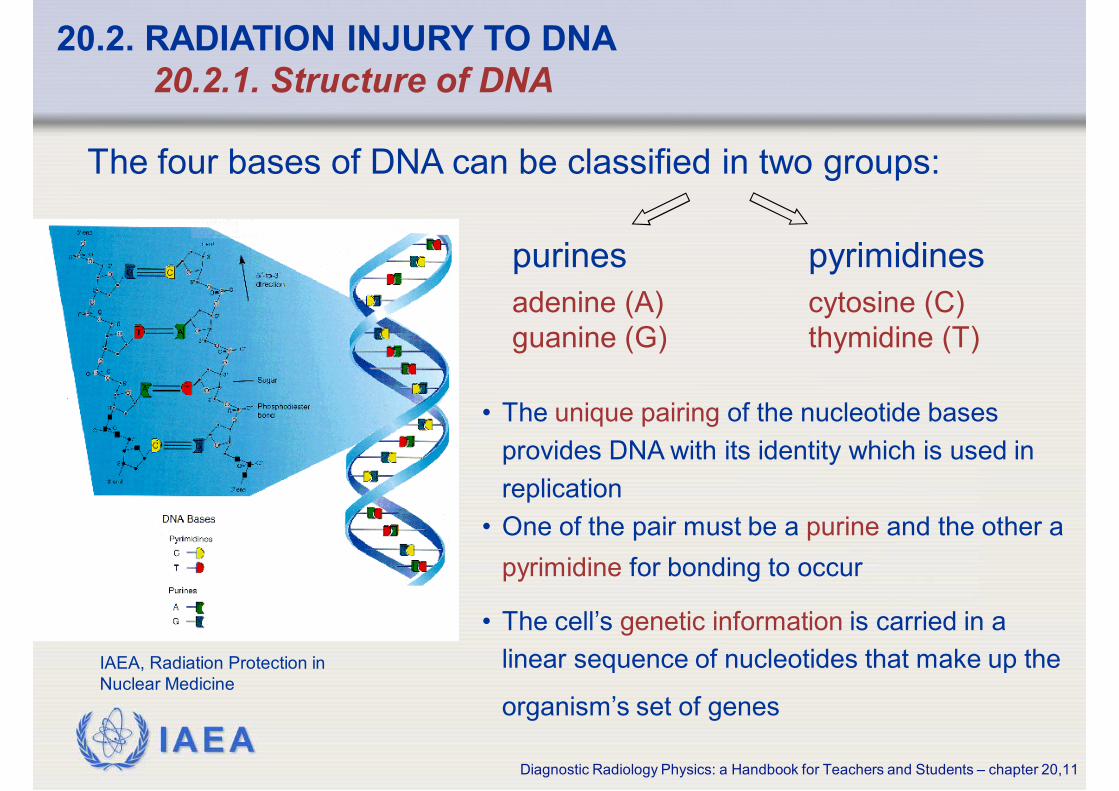
• The unique pairing of the nucleotide bases
provides DNA with its identity which is used in
replication
• One of the pair must be a purine and the other a
pyrimidine for bonding to occur
• The cell’s genetic information is carried in a
linear sequence of nucleotides that make up the
organism’s set of genes
The four bases of DNA can be classified in two groups:
purines pyrimidines
adenine (A)
guanine (G)
cytosine (C)
thymidine (T)
IAEA, Radiation Protection in
Nuclear Medicine

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,12
20.2. RADIATION INJURY TO DNA
20.2.2. Radiation chemistry; direct and indirect effects
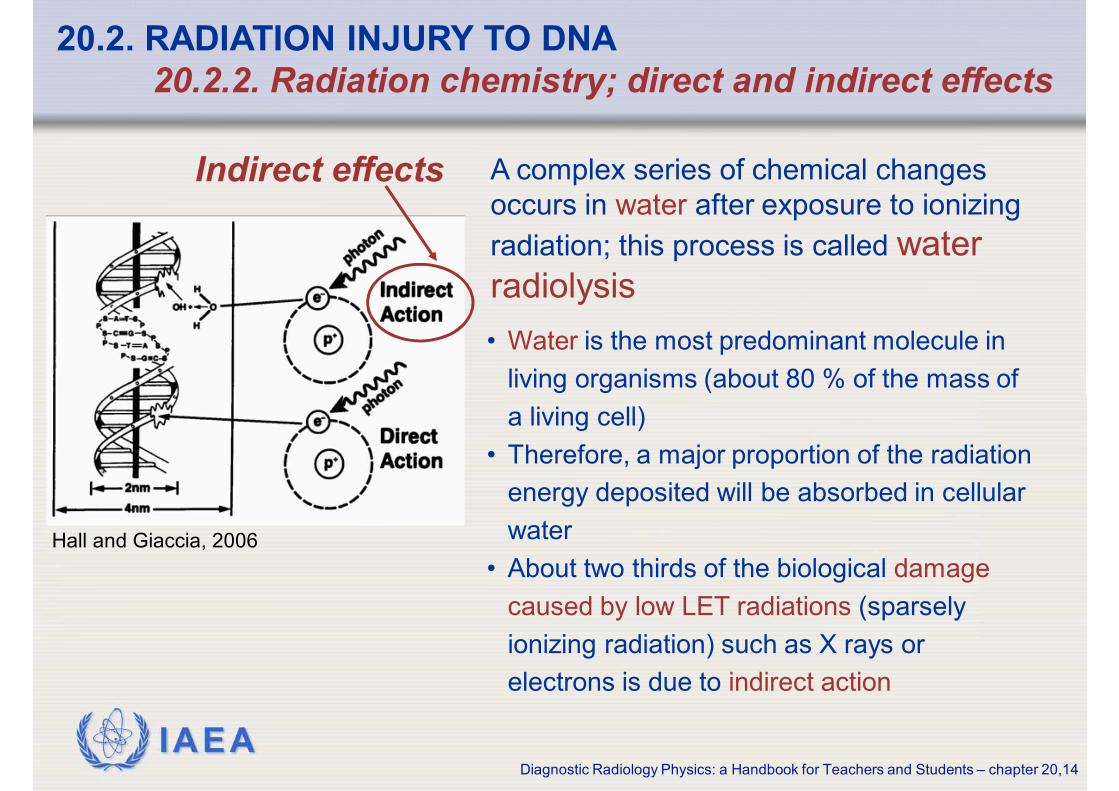
• When ionizing radiation energy is
deposited in a certain macromolecule,
associated with observable biological
effects, such as DNA, it is called a
direct effect of ionizing radiation
• The radicals formed, namely the hydrated electron (eaq-), the hydrogen
atom (H·) and the hydroxyl radical (OH·), are able to diffuse far enough to
reach and damage the critical targets
This is referred to as indirect action of ionising radiation
• Alternatively, photons may be absorbed in
the water of an organism causing
excitation and ionization in the water
molecules
Hall and Giaccia, 2006

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,13
The interactions of ionizing radiation with matter lead to loss of
radiation energy through ionization, and the formation of free
radicals
20.2. RADIATION INJURY TO DNA
20.2.2. Radiation chemistry; direct and indirect effects
• react rapidly (10-10 s) with neighbouring molecules and produce
secondary DNA or lipid radicals
• are fragments of molecules having unpaired electrons, which have
high reactivity with cellular molecules and, therefore, have a short
life
• are generated in great number by ionizing radiation due to the
process of energy absorption and breakage of chemical bonds in
molecules
• are known to play a major role on biological tissues and organisms
Free Radicals:
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,14
• Water is the most predominant molecule in
living organisms (about 80 % of the mass of
a living cell)
• Therefore, a major proportion of the radiation
energy deposited will be absorbed in cellular
water
• About two thirds of the biological damage
caused by low LET radiations (sparsely
ionizing radiation) such as X rays or
electrons is due to indirect action
20.2. RADIATION INJURY TO DNA
20.2.2. Radiation chemistry; direct and indirect effects
Hall and Giaccia, 2006
A complex series of chemical changes
occurs in water after exposure to ionizing
radiation; this process is called water
radiolysis
Indirect effects
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,15
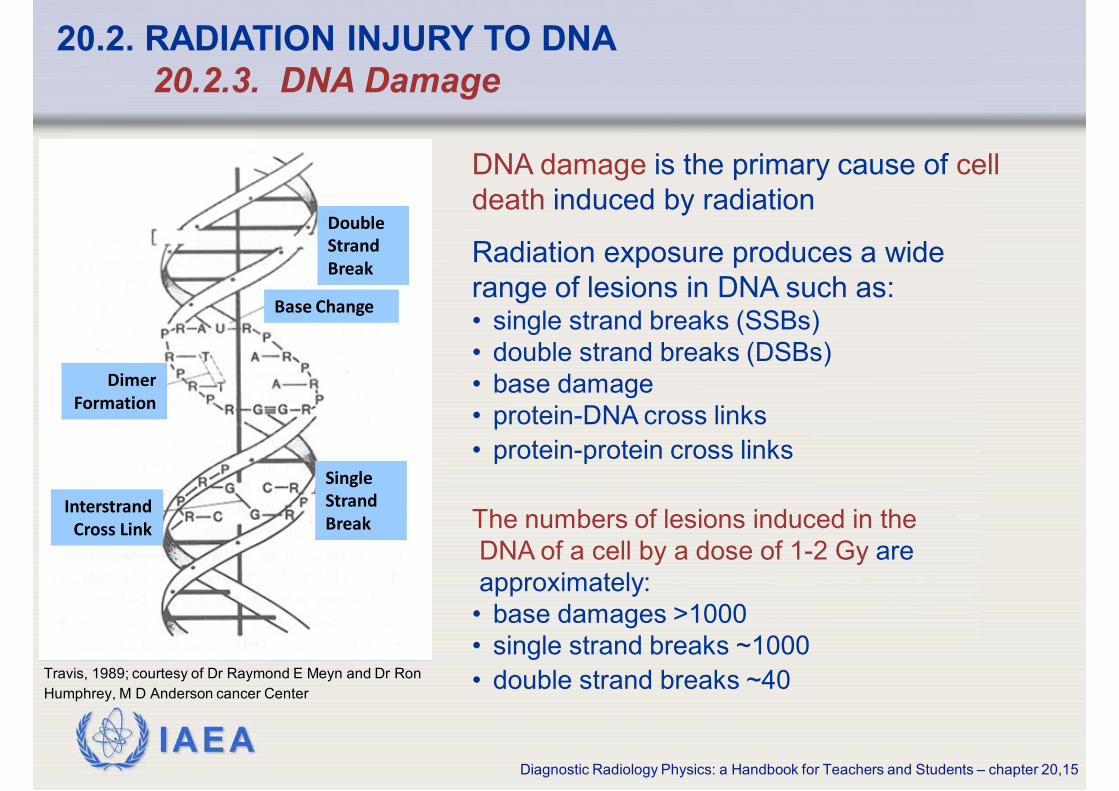
DNA damage is the primary cause of cell
death induced by radiation
Radiation exposure produces a wide
range of lesions in DNA such as:• single strand breaks (SSBs)
• double strand breaks (DSBs)
• base damage
• protein-DNA cross links
• protein-protein cross links
20.2. RADIATION INJURY TO DNA
20.2.3. DNA Damage
The numbers of lesions induced in the
DNA of a cell by a dose of 1-2 Gy are
approximately:
• base damages >1000
• single strand breaks ~1000
• double strand breaks ~40
Double
Strand
Break
Base Change
Dimer
Formation
Single
Strand
BreakInterstrand
Cross Link
Travis, 1989; courtesy of Dr Raymond E Meyn and Dr Ron
Humphrey, M D Anderson cancer Center

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,16
There are experimental data showing that:
• initially-produced DSBs correlate with radiosensitivity
and survival at lower dose
• unrepaired or mis-repaired DSBs also correlate with
survival after higher doses
• there is a causal link between the generation of DSBs
and the induction of chromosomal translocations with
carcinogenic potential
20.2. RADIATION INJURY TO DNA
20.2.3. DNA Damage
Double
Strand
Break
Base Change
Dimer
Formation
Single
Strand
BreakInterstrand
Cross Link
Travis, 1989; courtesy of Dr Raymond E Meyn and Dr Ron
Humphrey, M D Anderson cancer Center
Double strand breaks (DSBs) play a critical
role in cell killing, carcinogenesis and
hereditary effects

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,17
20.3. DNA REPAIR
DNA repair mechanisms:
• base excision repair (BER)
• mismatch repair (MR)
• nucleotide excision repair (NER)
respond to damage such as base oxidation, alkylation, and strand
intercalation
There are multiple enzymatic mechanisms of detecting and
repairing radiation-induced DNA damage
Excision repair consists of cleavage of the damaged DNA strand by enzimes that
cleave the polynucleotide chain on either side of the damage and enzymes which
cleave the end of a polynucleotide chain allowing removal of a short segment
containing the damaged region
DNA polymerase can then fill in the resulting gap using the opposite undamaged
strand as a template

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,18
20.3. DNA REPAIR
For double strand breaks there are two primary repair pathways:
HR repair utilizes sequence homology
with an undamaged copy of the broken
region and hence can only operate in
late S- or G2- phases
Undamaged DNA from both strands is
used as templates to repair the
damage
The repair process of HR is error-free
NHEJ repair operates on blunt ended
DNA fragments
This process involves the repair
proteins recognizing lesion termini,
cleaning up the broken ends of the
DNA molecule, and the final ligation of
the broken ends
Repair by NHEJ operates throughout
the cell cycle but dominates in G1/S-
phases
The process is error-prone because it
does not rely on sequence homology
non-homologous end joining (NHEJ) and homologous recombination (HR)

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,19
20.3. DNA REPAIR
DNA repair mechanisms are important for the recovery of
cells from radiation and other damaging agents
Unrepaired or mis-repaired damage to DNA
will lead in the exposed cell to:
cell deathcancer or
hereditary effects
when severe often leads to:might lead to:
mutations and/or chromosome damage

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,20
20.4. RADIATION-INDUCED CHROMOSOME DAMAGE AND
BIOLOGICAL DOSIMETRY
When the repair of DNA-double strand breaks is incomplete there may
be serious implications for a cell, namely it may lead to chromosomal
damage (aberrations)
Aberrant (damaged) chromosomes:
• rings generated when broken ends rejoin with other broken ends
• dicentrics (chromosomes having two centromeres)
• translocations
• other chromosome aberrations
Chromosomes:
• can be found in the nucleus of the cell in the living cell
• consist of DNA and proteins forming a threadlike structure
containing genetic information arranged in a linear sequence

IAEA
20.4. RADIATION-INDUCED CHROMOSOME DAMAGE AND
BIOLOGICAL DOSIMETRY
Diagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,21
• Dicentrics and rings are
“unstable” aberrations and are
lethal to the cell and as a
consequence they are not
passed on to progeny
• Symmetric translocations and
small deletions are in general
non lethal
• When translocations occur in
germ cells they may lead to an
increase in hereditary effects in
the offspring Inversion
Symmetrical
(Stable)Breaks
Intrachange
Asymmetrical
(Unstable)
Centric
Ring
Interchange
Translocation DicentricAdapted from IAEA - Biodosimetry: available methods and role in dose assessment and prognosis

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,22
20.4. RADIATION-INDUCED CHROMOSOME DAMAGE AND
BIOLOGICAL DOSIMETRY
• Structural chromosome aberrations can be used as an indicator of
radiation exposure
• Chromosome analysis in mitotic spreads (karyotyping), micronucleus
formation and fluorescent in situ hybridisation (FISH) can detect
unrepaired DNA damage in chromatids by radiation and a variety of
DNA damaging agents
• These cytological techniques are used in biodosimetry (assays to
estimate the radiation dose based on the type and/or frequency of
chromosomal aberrations in the exposed cells/tissues)
• Biodosimetry has provided an important tool for assessing doses in
known or suspected cases of acute (unwanted) radiation exposure

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,23
20.5. THE CELL CYCLE
The cell cycle has two well defined time
periods:
• Mitosis (M), where division takes place
• the period of DNA-synthesis (S)
The S and M portions of the cell cycle are
separated by two periods (gaps) G1 and G2
• Cells in a growing population (e.g. skin, gut, bone marrow), but
not resting fully differentiated G0 phase cells, participate in the cell
cycle and thus are more sensitive to radiation
• Replication of the genome occurs in the S-phase and mitotic
propagation to daughter generations occurs in the G2/M phases

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,24
20.5. THE CELL CYCLE
Typical cell generation times are 10 – 40 hours with
the:
• G1 phase taking about 30 %
• S- phase 50 %,
• G2 phase 15 %
• M- phase 5 % of the cell cycle time
There are checkpoints at the G1/S
and G2/M boundaries that ensure the
fidelity of genomic processing

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,25
20.5. THE CELL CYCLE
Radiosensitivity differs throughout the cell
cycle with, in general:
• late S-phase being most radio resistant
• G2/M being most radiosensitive
• G1 phase taking an intermediate position
• The greater proportion of repair by HR than by NHEJ in late S phase
may explain the resistance of late S phase cells
• Chromatin compaction and poor repair competence (reduced enzyme
access) could explain the high radiosensitivity in G2/M phase
• Resting cells, not involved in the cell cycle, are even more resistant to
radiation when compared to late S-phase cells
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,26
20.6. SURVIVAL CURVE THEORY
20.6.1. Survival curves
• The generally accepted standard for measuring the
radiosensitivity of a cell population is
“the retention of reproductive integrity”
i.e. the ability of a cell to undergo more than
5-6 cell divisions and produce a viable colony
containing at least 50 cells
• This is referred to as cell survival
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,27
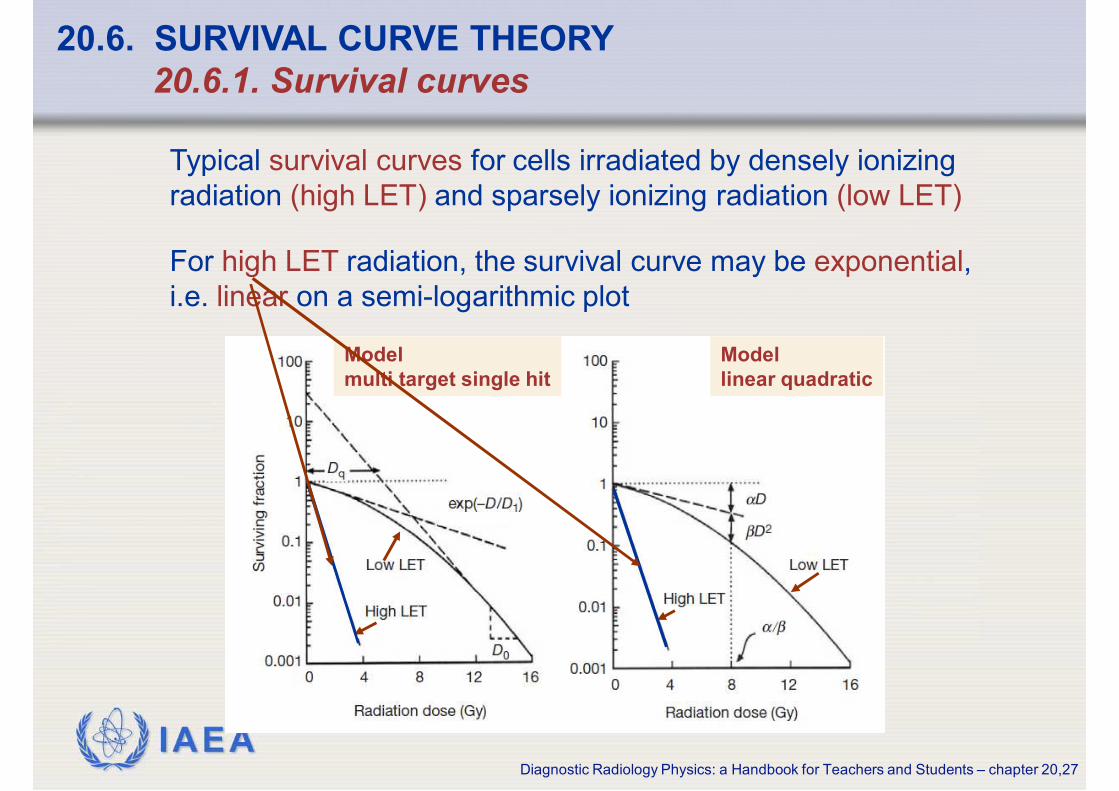
Typical survival curves for cells irradiated by densely ionizing
radiation (high LET) and sparsely ionizing radiation (low LET)
20.6. SURVIVAL CURVE THEORY
20.6.1. Survival curves
For high LET radiation, the survival curve may be exponential,
i.e. linear on a semi-logarithmic plot
Model
linear quadratic
Model
multi target single hit
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,28
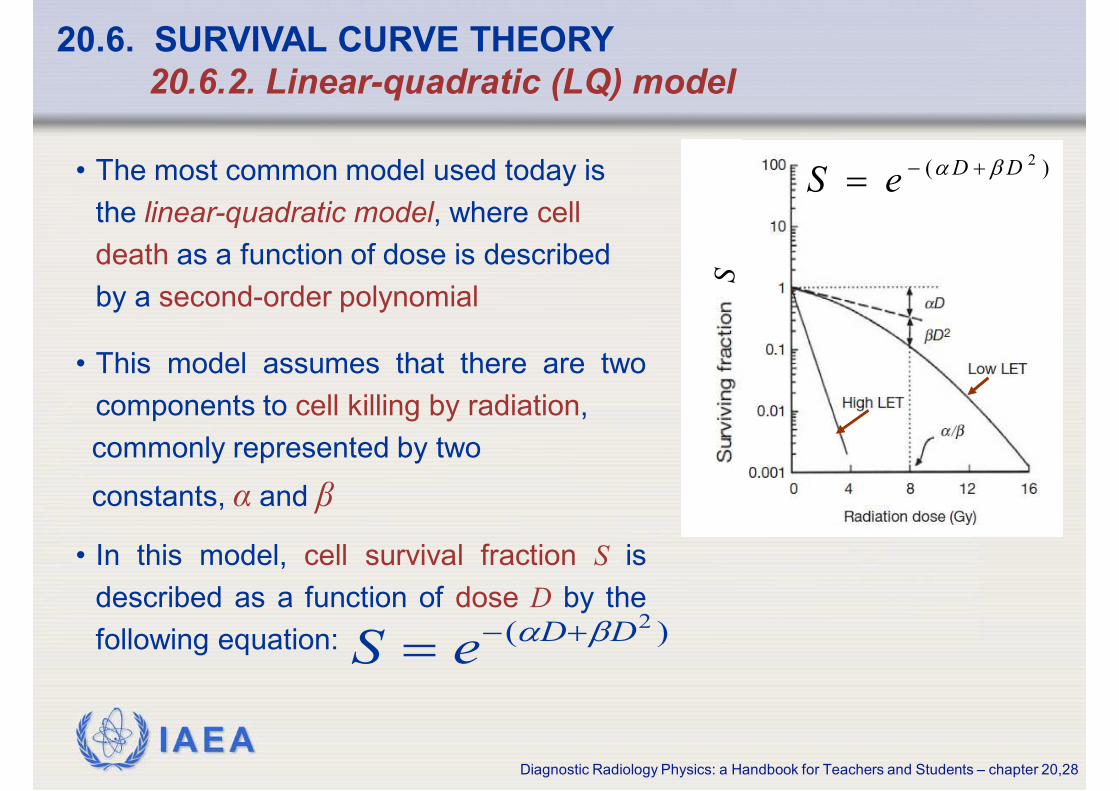
20.6. SURVIVAL CURVE THEORY
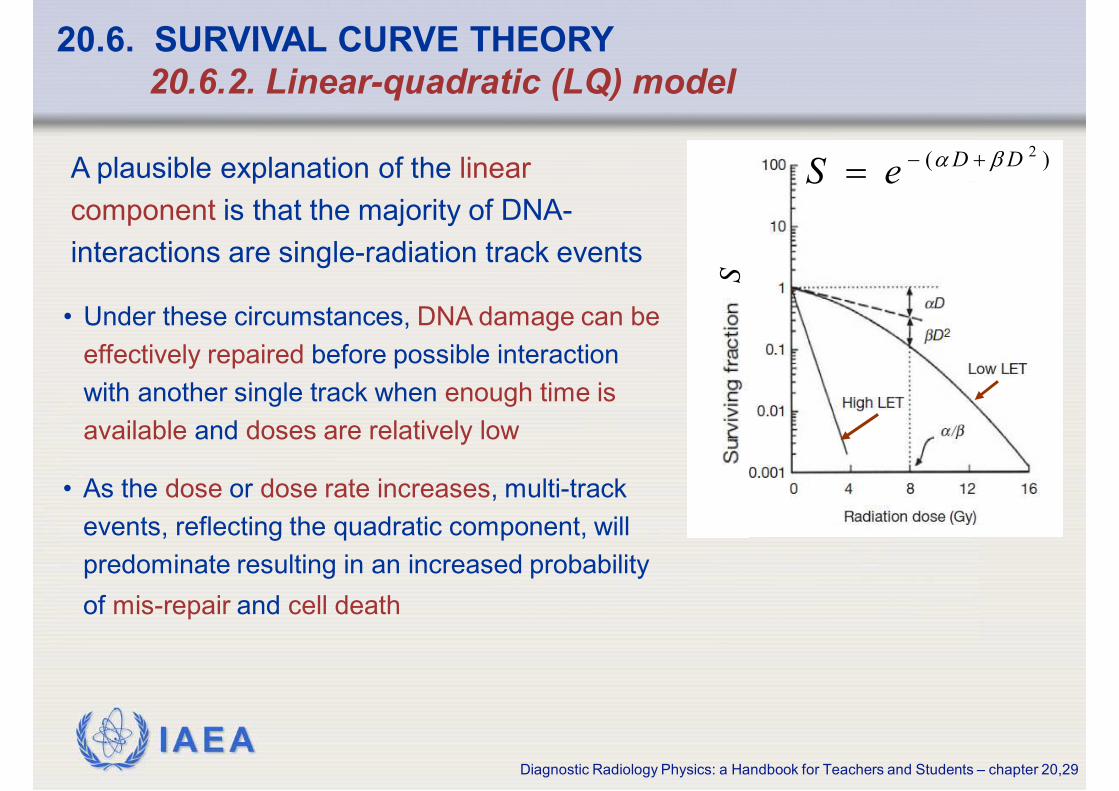
20.6.2. Linear-quadratic (LQ) model
• This model assumes that there are two
components to cell killing by radiation,
commonly represented by two
constants, α and β
• In this model, cell survival fraction S is
described as a function of dose D by the
following equation:
• The most common model used today is
the linear-quadratic model, where cell
death as a function of dose is described
by a second-order polynomial
)( 2DDeS βα +−=
)( 2DDeS βα +−=
S
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,29
20.6. SURVIVAL CURVE THEORY
20.6.2. Linear-quadratic (LQ) model
A plausible explanation of the linear
component is that the majority of DNA-
interactions are single-radiation track events
• Under these circumstances, DNA damage can be
effectively repaired before possible interaction
with another single track when enough time is
available and doses are relatively low
• As the dose or dose rate increases, multi-track
events, reflecting the quadratic component, will
predominate resulting in an increased probability
of mis-repair and cell death
)( 2DDeS βα +−=
S

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,30
20.6. SURVIVAL CURVE THEORY
20.6.3. Target theory
The target theory is based upon the idea that there
are n targets in a cell, all of which must be “hit” to kill
the cell
An alternative older model is the single-hit
single-target model described by:
D0 is effectively the reciprocal of α (of LQ model)
and represents the dose which reduces survival to
e -1 or 37 %
0/ DDeS−
=
0/ DDeS−
=
S

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,31
20.6. SURVIVAL CURVE THEORY
20.6.3. Target theory
• This is reliable at high dose but not at low dose,
because it does not describe accurately the
‘shoulder’ region at low doses, even if another
single-hit term is added
• The log-linear relationship is consistent with data
from some bacteria but it does not apply in
eukaryotic cells (except at high LET), which show
shouldered survival curves that can be
accommodated by a single-hit multi-target model
described by:
nDDeS )1(1 0/−
−−=
n is the number of targets
0/ DDeS−
=
S

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,32
20.7. CONCEPTS OF CELL DEATH
• Radiation doses in the order of several sieverts may lead
to cell loss
• Cells are generally regarded as having been “killed” by
radiation if they have lost reproductive integrity, even if
they physically survived
Loss of reproductive integrity can occur by:
• apoptosis
• necrosis
• mitotic catastrophe
• induced senescence
although all but the last of these
mechanisms ultimately results in
physical loss of the cell, this may
take a significant time to occur
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,33
20.7. CONCEPTS OF CELL DEATH
Necrosis
• is a form of cell death associated with loss of cellular membrane
activity
• cellular necrosis generally occurs after high radiation doses
Apoptosis or programmed cell death:
• can occur naturally or result from insult to the cell environment
• occurs after low doses of irradiation in particular cell types:
lymphocytes
serous salivary gland cells
certain cells in the stem cell zone in testis and intestinal crypts
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,34
20.7. CONCEPTS OF CELL DEATH
Reproductive cell death
• is a result of mitotic catastrophe (cells attempt to divide
without proper repair of DNA damage) which can occur in
the first few cell divisions after irradiation
• it occurs with increasing frequency after increasing doses
Senescent cells
• are metabolically active but have lost the ability to divide
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,35
20.8. CELLULAR RECOVERY PROCESSES
At higher doses and dose rates (i.e.
multiple radiation exposures during
interventional cardiology), cellular
recovery may play an important role in
the fixation of the radiation damage
IAEA
Due to cellular recovery an increase in cell
survival can be expected when the same
dose is given as:
• 2 fractions separated by 2 or more
hours compared to the
• single fraction
This greater survival is attributed to:
sub-lethal damage repair (SLDR)
between dose fractions
Diagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,36
20.8. CELLULAR RECOVERY PROCESSES
20.8.1. Sub-lethal and potentially lethal damage repair

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,37
20.8. CELLULAR RECOVERY PROCESSES
20.8.1. Sub-lethal and potentially lethal damage repair
• T½ is the half time of repair, defined as the time it takes for
half the repair to take place
T½ ≈ ½ to 1 h for cells in culture, but can be longer for tissues
Thus full repair may take 6 - 8 hours and can be longer in tissues
In central nervous system (CNS) it may be greater than 24 hours
• The recovery ratio is a measure of sub-lethal damage repair
(SLDR) and is given by :
dose single a as dose total the receiving cells of survival
dose split a receiving cells of survivalSLDR =
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,38
20.8. CELLULAR RECOVERY PROCESSES
20.8.1. Sub-lethal and potentially lethal damage repair
• Potentially lethal damage repair (PLDR) is determined
by delayed plating experiments
• In such experiments contact inhibited (i.e. confluent cell cultures)
cells are:
- irradiated
- incubated for various periods
- subsequently reseeded
• Analysis of cell survival by colony assay then gives a measure of
this type of repair

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,39
20.8. CELLULAR RECOVERY PROCESSES
20.8.2. Fractionation effect
• The ‘shoulder’ or the curvature of a survival curve is
usually considered to be a reflection of the repair capacity
of a cell population
• In terms of the target theory this can be thought of as
arising from the concept that sub-lethal DNA damaging
events must be accumulated to allow sub-lesion
interactions for cell killing to occur

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,40
20.8. CELLULAR RECOVERY PROCESSES
20.8.3. Dose rate effects
• The successive increase of cell survival with declining dose rate
is consistent with the role of time in repair
• The dominance of repair at low dose rate eliminates the
shoulder/curvature of the survival curve and results in a straight
but shallower line on a semi-logarithmic plot, with good separation
of survival between cell lines with different repair capacity. This is
due to the cells having different radiosensitivities
• Repair during irradiation is:
- negligible at dose rates of 1- 5 Gy/min
- significant at dose rates <100 mGy/min

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,41
20.9. RELATIVE BIOLOGICAL EFFECTIVENESS
Equal doses of different types of radiation produce unequal
biological effects
• Comparison of effects of different types of radiation is
expressed as Relative Biological Effectiveness (RBE), defined
as:
• Historically the reference used was 250 kV X rays but more recently
Co-60 radiation has become the standard
effect biological same the produce to radiation test from Dose
effect biological given a produce to radiation standard from Dose=RBE

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,42
20.9. RELATIVE BIOLOGICAL EFFECTIVENESS
RBE - Relative Biological Effectiveness
• varies with cell system endpoint
• varies with dose
• is higher at lower doses and low dose rates
• is lower for high doses with a single fraction than for multiple
small fractions
For radiation protection purposes (at low doses and low dose
rates), the ICRP has described the effectiveness of radiations of
differing qualities by a series of Radiation Weighting Factors (wR)

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,43
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.1. Mechanism of multistage carcinogenesis
The development of cancer in
tissues is assumed to be a
multi-stage process that can be
sub-divided into four phases:
This subdivision is an over- simplification yet it provides a suitable
frame work for the identification of specific molecular and cellular
changes involved
neoplastic initiation
promotion
conversion
progression

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,44
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.1. Mechanism of multistage carcinogenesis
Neoplastic initiation leads to the irreversible potential of normal
cells for neoplastic development by creating unlimited proliferative
capacity
• Further neoplastic development of initiated cells depends on promotional
events which involves intercellular communication, e.g. by growth factors,
hormones or environmental agents
This results in the proliferation of the initiated pre-neoplastic cells in a
semi-autonomous manner
• There is good evidence that this event results from one or more
mutations in a single cell which is the basis of the clonal evolution of the
cancer

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,45
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.1. Mechanism of multistage carcinogenesis
During the process of conversion of the
pre-neoplastic cells into fully malignant cells:
• additional mutations in other genes are accumulated,
probably facilitated by increasing loss of genomic stability
• The subsequent progression into an invasive cancer
depends on still more mutations in the unstable genome

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,46
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.1. Mechanism of multistage carcinogenesis
There is strong evidence from animal studies and
some human studies that the risk of radiation-induced
cancer may be influenced by various genes, such as
mutations of the:
• Rb gene (predisposing for retinoblastoma and osteosarcoma)
• BRCA1 gene (predisposing for early breast cancer and ovarian
cancer)
or the presence of polymorphisms (SNPs: single nucleotide
polymorphisms) in the gene
However, at the present state of knowledge the role of genetic
susceptibility on individual risks of radiation-induced cancer cannot
be resolved definitively, although there is general agreement that it
will be important

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,47
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.2. Mechanism of mutation induction
Mutations e.g. by the translocation of
a promoter, may result in an
increased rate of proliferation
Proto-oncogene mutations to
oncogenes are thus classified as
“gain-of-function” mutations
Two classes of cancer-associated
genes have been identified:
tumour suppressor genproto-oncogenes
Normal genes involved in growth
regulation
Genes involved in growth regulation of
normal cells and that prevent excessive cell
proliferation
The critical mutation in these genes are
“loss-of-function” mutations which may be
the result of partial or complete loss of the
gene structure, e.g. by deletions. Since
radiation-induced DNA damage preferentially
causes deletions, it is generally assumed
that the inactivating mutation of tumour
suppressor genes is the most probable
mechanism for the induction of cancer by
radiation
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,48
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.2. Mechanism of mutation induction
• There is good evidence that many, if not most cancers, are the clonal
descendants of a single neoplastic cell and, furthermore, that a
single double strand break may, although with an extremely low
probability, cause a deletion in a specific DNA sequence, e.g. of a
tumour suppressor gene
• It has hence been argued that, in principle, a single mutational event
in a critical gene in a single target cell in vivo can create the potential
for neoplastic development
• Thus, a single radiation track traversing the nucleus of an
appropriate target cell has a finite probability, albeit very small, of
generating the specific damage of DNA that results in the initiating
mutation
• This argument would strengthen the hypothesis that the risk of
radiation induced cancer increases progressively with increasing
dose, and there is no lower threshold

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,49
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.3. Risk models
In order to evaluate the health effects of radiation on exposed
populations or workers, the incidence or frequency of a certain
effect is studied in both the exposed and non exposed control
group
Risk estimates derived from these studies are
generally presented as
• RR (relative risk)
• ERR (excess relative risk)
• EAR (excess absolute risk)
per unit of radiation dose

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,50
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.3. Risk models
Excess Relative Risk (ERR)
1−= RRERR
Excess Absolute Risk (EAR)
0RREAR r −=
Relative Risk (RR)
group exposed-non the in effect same the offrequency
group exposed the in cases) cancer of number (i.e. effect certain a offrequency =RR
0R
RRR r=

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,51
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.3. Risk models
For assessing the risk of radiation-induced cancer in humans
two conceptually different models are used:
• This model assumes that the effect is to
increase the natural incidence at all ages
subsequent to exposure by a given factor
• Because the natural or spontaneous
cancer incidence rises significantly in old
age, this model predicts a larger number
of radiation-induced cancers in old age
• This model is favoured by the BEIR
committee estimating risks after radiation
exposure
relative-riskabsolute-risk
• This model assumes that
radiation induces a “crop” of
cancers over and above the
natural incidence and
unrelated to it
• After the latency period has
passed, the cancer risk
returns to “spontaneous”
levels

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,52
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.4. Time course and latency period
Epidemiological information derived from:
• the life span study (LSS) of the A-bomb survivors in Japan
• data from other studies
has provided the main source of risk estimates currently used in
radiation protection
is the time interval between exposure to
irradiation and the appearance of cancer
• Leukaemia has a minimum latency of about 2 years after exposure; the
pattern of risk over time peaks after ten years (most cases occur in the
first 15 years) and decreases thereafter
• Solid tumours show a longer latency than leukaemia, by anything from
10 to 60 years or even more
Latency period

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,53
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.5. Dose response relationship for cancer
• The linear non-threshold (LNT) hypothesis was introduced by
the ICRP as the best practical approach to managing risk from
radiation exposures to low dose/low dose rates
• The LNT model postulates that there is a linear relationship
between radiation dose and health risk without a threshold at low
doses
It means that there is no level of radiation exposure that can be
assumed to have no associated health risk
• The slope of the linear dose-response curve provides the risk
coefficient (cancer risk per unit radiation dose received)
appropriate for low level exposures

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,54
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.6. Dose and dose-rate effectiveness factor (DDREF)
Both BEIR and UNSCEAR committees considered that there is a
dose-rate effect for low energy transfer radiation, with fewer
malignancies induced if a given dose is spread out over a period of
time at low dose rate than if it is delivered in an acute exposure
Comparison of the:
• Japanese data of A-bomb survivors with those of other
• epidemiological studies including multiple medical and
chronic exposures
have demonstrated that the risk calculated in proportion of the
dose differs

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,55
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.6. Dose and dose-rate effectiveness factor (DDREF)
• The DDREF is defined as the factor by which radiation
cancer risks observed from large acute doses should
be reduced when the radiation is delivered at low dose
rate or in a series of small dose fractions
• For general purposes in radiological protection,
the ICRP recommends a
for doses below 200 mSv at any dose rate and
for higher doses if the dose rate is < 100 mSv/hDDREF = 2
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,56
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.7. Cancer risk
The ICRP recommendations for radiation protection purposes are
based on the Japanese and other epidemiological studies
The risk coefficients for cancer lethalithy
non radiation workers
• 5x10-2 per Sv
• 10x10-2 per Sv for high doses and
dose rates
high doses: higher than 200 mSv
high dose rates: higher than 100 mSv/h
These estimates show mean values
for the whole population
workers
• 4x10-2 per Sv
• 8x10-2 per Sv for high doses and
dose rates

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,57
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.7. Cancer risk
• There is ample evidence that cancer risk is
not only dependent on the dose but also on
the age at exposure and to a lesser extend
also on gender
• In most cases, those exposed at an early
age are more susceptible than those
exposed at later times and females are
slightly more susceptible than males
Since not all radiation exposures concern
the whole body but only a region or just a
part of the body, tissue weighing factors (wT )
should be taken into account
Hall and Giaccia, 2006, adapted from ICRP:
Recommendations. Annals of the ICRP Publication 60,
Oxford, England, Pergamon Press, 1990
From a single small dose of irradiation
Relatice risk model with DDREF=2
(
)
(y)

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,58
males age of exposure (y)
5 15 30 50 70
Stomach 65 46 28 25 14
Colon 285 204 125 113 65
Liver 50 36 22 19 8
Lung 261 180 105 101 65
Prostate 80 57 35 33 14
Bladder 177 127 79 76 47
Other 672 394 198 140 57
Thyroid 76 33 9 1 0.1
All solid 1667 1076 602 507 270
Leukemia 149 105 84 84 73
All cancers 1816 1182 686 591 343
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.7. Lifetime attributable risk of cancer incidence from BEIR VII, (2006)
Number of cases per 100,000 persons exposed to a single dose of 0.1 Gy
These estimates are obtained as combined estimates based on relative and absolute risk transport and have been
adjusted by a DDREF of 1.5, except for leukemia, which is based on a linear-quadratic model
Stomach 85 61 36 32 19
Colon 187 134 82 73 45
Liver 23 16 10 9 5
Lung 608 417 242 230 147
Breast 914 553 253 70 12
Uterus 42 30 18 13 5
Ovary 87 60 34 25 11
Bladder 180 129 79 74 47
Other 719 409 207 148 68
Thyroid 419 178 41 4 0.3
All solid 3265 1988 1002 678 358
Leukemia 112 76 63 62 51
All cancers 3377 2064 1065 740 409
Stomach 85 61 36 32 19
Colon 187 134 82 73 45
Liver 23 16 10 9 5
Lung 608 417 242 230 147
Breast 914 553 253 70 12
Uterus 42 30 18 13 5
Ovary 87 60 34 25 11
Bladder 180 129 79 74 47
Other 719 409 207 148 68
Thyroid 419 178 41 4 0.3
All solid 3265 1988 1002 678 358
Leukemia 112 76 63 62 51
All cancers 3377 2064 1065 740 409
females age of exposure (y)5 15 30 50 70

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,59
20.10. CARCINOGENESIS (STOCHASTIC)
20.10.7. Lifetime attributable risk of cancer mortality from BEIR VII, (2006)
Number of cases per 100,000 persons exposed to a single dose of 0.1 Gy
males age of exposure (y)
5 15 30 50 70
Stomach 34 25 16 13 8
Colon 139 99 61 57 36
Liver 37 27 16 14 8
Lung 264 182 107 104 71
Prostate 15 10 7 7 7
Bladder 38 27 17 17 15
Other 255 162 94 77 36
All solid 781 533 317 289 181
Leukemia 71 70 64 71 69
All cancers 852 603 381 360 250
These estimates are obtained as combined estimates based on relative and absolute risk transport and have been
adjusted by a DDREF of 1.5, except for leukemia, which is based on a linear-quadratic model
females age of exposure (y)5 15 30 50 70
Stomach 48 34 21 19 13
Colon 86 62 38 35 25
Liver 20 14 9 8 5
Lung 534 367 213 204 140
Breast 214 130 61 19 5
Uterus 10 7 4 3 2
Ovary 47 34 20 18 10
Bladder 51 36 23 22 19
Other 287 179 103 86 47
All solid 1295 862 491 415 265
Leukemia 52 52 51 54 52
All cancers 1347 914 542 469 317
Stomach 48 34 21 19 13
Colon 86 62 38 35 25
Liver 20 14 9 8 5
Lung 534 367 213 204 140
Breast 214 130 61 19 5
Uterus 10 7 4 3 2
Ovary 47 34 20 18 10
Bladder 51 36 23 22 19
Other 287 179 103 86 47
All solid 1295 862 491 415 265
Leukemia 52 52 51 54 52
All cancers 1347 914 542 469 317

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,60
20.11. RADIATION INJURY TO TISSUES (DETERMINISTIC)
20.11.1. Tissue and organ anatomy
• Tissues and organs in the human body are composed of
many different cells
• The majority of cells in tissues and organs are differentiated
and have developed a specific morphology and function
• In many tissues and organs, but not all, the rate of death of
differentiated cells is balanced by renewal from a “pool” of
tissue stem cells in order to maintain a healthy state and
function

IAEA
20.11. RADIATION INJURY TO TISSUES (DETERMINISTIC)
20.11.1. Tissue and organ anatomy
Diagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,61
• Since radiation may lead to sterilization of dividing
cells, in particular tissue stem cells, terminally
differentiated (mature) cells can no longer be
replaced
• Lack of replacement can eventually result in a loss
of sufficient numbers of functioning cells and as a
consequence a loss of tissue and/or organ integrity
and function

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,62
20.11. RADIATION INJURY TO TISSUES (DETERMINISTIC)
20.11.1. Tissue and organ anatomy
• Tissue and organ reactions are generally
classified under deterministic effects
• Above a certain threshold (sufficient number of cells
sterilized by radiation), the severity of the effect will
increase steeply with increasing radiation dose
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,63
20.11. RADIATION INJURY TO TISSUES (DETERMINISTIC)
20.11.2. Expression and measurements of damage
The radiosensitivity of the cells of a number of normal tissues
can be determined directly using in situ assays in the
laboratory
Considerable variability in sensitivity is apparent within and
between the different tissues and organs
Detailed knowledge about radiation-induced
normal tissue effects comes primarily from
experience with:
• radiotherapy patients
• radiation accidents
• laboratory studies, mainly with rodents

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,64
20.11. RADIATION INJURY TO TISSUES (DETERMINISTIC)
20.11.2. Expression and measurements of damage
For the study of the response of individual organs, one widely used
approach is to define a level of functional deficit and to determine the
percentage of irradiated individuals (or animals in laboratory studies)
that express at least this level of damage following different radiation
dosesThis approach results in
sigmoidal dose response curves
ICRP publication 103, 2007
In any exposed population, there is
individual variation in radiosensitivity
which is influenced by several factors
including:
• hormonal status
• age
• state of health of the individuals
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,65
20.11. RADIATION INJURY TO TISSUES (DETERMINISTIC)
20.11.2. Expression and measurements of damage
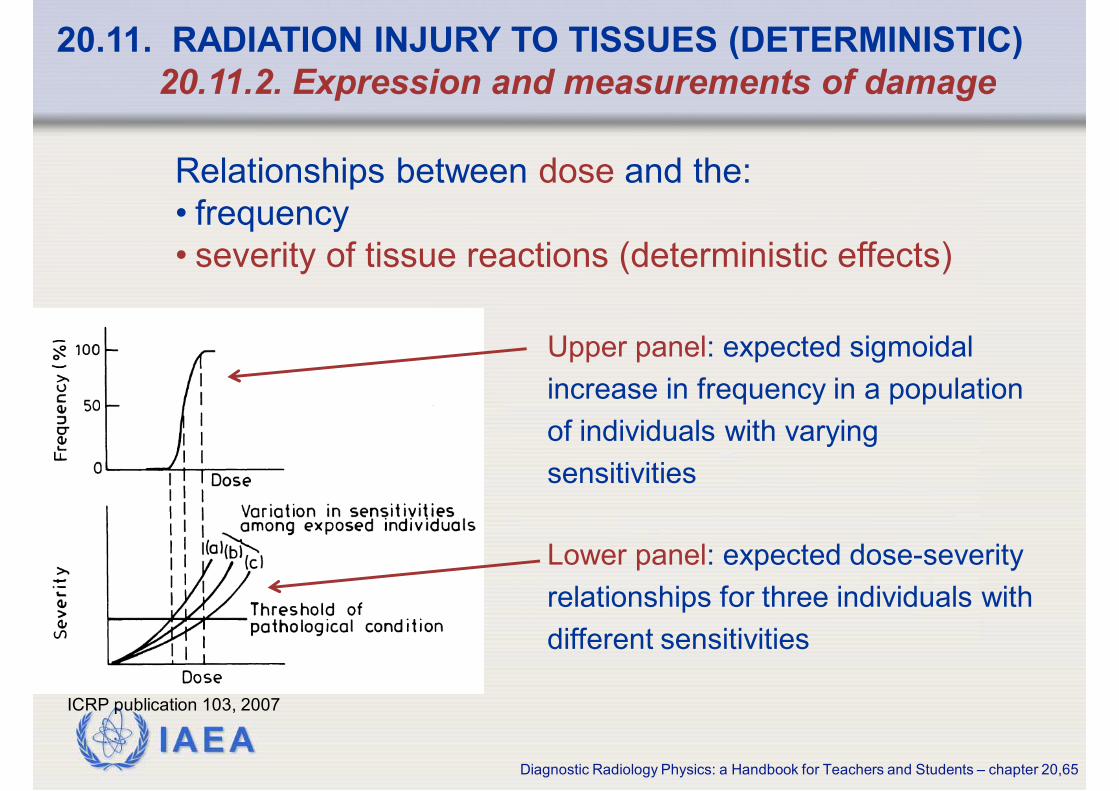
Upper panel: expected sigmoidal
increase in frequency in a population
of individuals with varying
sensitivities
ICRP publication 103, 2007
Relationships between dose and the:
• frequency
• severity of tissue reactions (deterministic effects)
Lower panel: expected dose-severity
relationships for three individuals with
different sensitivities

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,66
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.1. Acute and late responding normal tissues
• Radiation-induced cell death in normal tissues generally occurs
when the cells attempt to divide (mitosis)
• Tissue tends to respond on a time scale similar to that of the normal
rate of loss of functional cells in the tissue
Traditionally the effects of radiation on normal tissues, based largely
on functional and histopathological endpoints, has been classified,
according to the time of clinical symptoms after the exposure to
manifest, into:
within a few weeks
early (or acute) responses
many months or years
late responses

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,67
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.2. Pathogenesis of acute and late effects
• Acute responses occur primarily in tissues with rapid cell renewal,
where cell division is required to maintain the function of the organ
Because many cells express radiation damage during mitosis, there is
early death and loss of cells by radiation
Examples of early responding tissues are:
• bone marrow
• gastrointestinal tract
• skin
In these tissues the acute radiation responses
have been related to death of critical cell
populations such as the stem cells in the cripts of
the: • bone marrow
• small intestine
• basal layer of the skin
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,68
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.2. Pathogenesis of acute and late effects
In lymphoid and myeloid tissue, death by apoptosis plays an important
role in the temporal response of these tissues to irradiation
In the crypts of the small bowel there is a fraction of stem cells that die
by apoptosis, while other cells die by a mitosis-linked death
Radiation-induced apoptosis has
also been detected in many cells
and tissues, such as:
• lymphoid
• thymic
• hematopoietic
• spermatogonia
• salivary gland
• intestinal crypts
Acute responses

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,69
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.2. Pathogenesis of acute and late effects
Late responses tend to occur under normal conditions in organs
whose parenchymal cells divide:
infrequently rarely
liver or kidney central nervous system
or muscle
Depletion of the parenchymal cell population due to entry of
cells into mitosis, with the resulting expression of radiation
damage and cell death, will thus be slow

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,70
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.2. Pathogenesis of acute and late effects
• Late responses also occur in tissues that manifest early
reactions, such as skin/subcutaneous tissue and intestine,
but the nature of these reactions (subcutaneous fibrosis,
intestinal stenosis) is quite different from the early reactions
• One common late reaction is the slow development of tissue
fibrosis and vascular damage that occurs in many tissues and
is often seen in cancer patients a number of years after
radiation treatment

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,71
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.3. Radiation-induced skin reaction
The skin consists of a :
relatively thin epidermis
• renews rapidly (15-30 days)
much thicker underlying dermis
• is highly vascularised
connective tissue
hair follicles
sweat glands
sebaceous glands
nerve endings
• contains

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,72
• The early erythema is believed to be related to the release of
5-hydroxy-tryptamine by mast cells, increasing vascular permeability
• Similar mechanisms may lead to the early nausea and vomiting observed
following irradiation of the intestine
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.3. Radiation-induced skin reaction
• A second and more severe erythema develops after a latent period of
8-10 days, mainly due to an inflammatory reaction of the skin
It is bright red in colour, limited to the radiation field, and accompanied
by a sensation of heat and itching
• early transient erythema similar to sunburn
• occurs within a few hours after irradiation
• reaches a peak value within 24 hours
A wide-variety of expressions of radiation-induced skin effects
have been described
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,73
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.3. Radiation-induced skin reaction
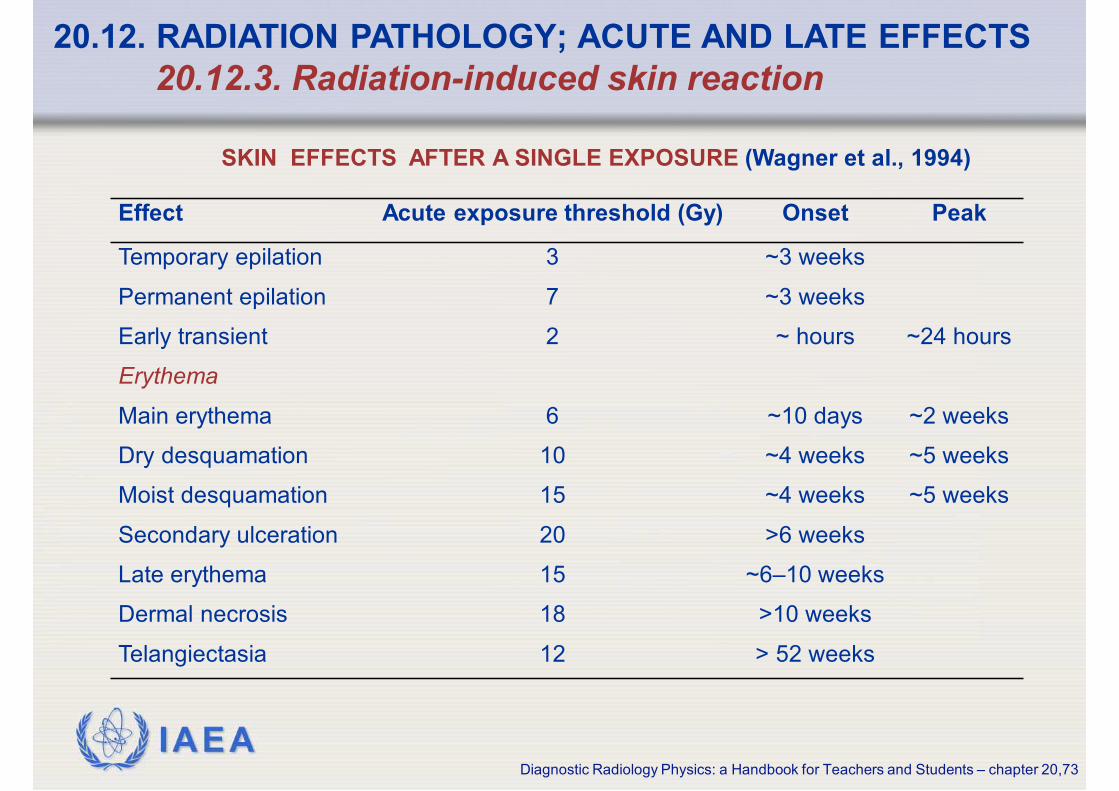
SKIN EFFECTS AFTER A SINGLE EXPOSURE (Wagner et al., 1994)
Effect Acute exposure threshold (Gy) Onset Peak
Temporary epilation 3 ~3 weeks
Permanent epilation 7 ~3 weeks
Early transient 2 ~ hours ~24 hours
Erythema
Main erythema 6 ~10 days ~2 weeks
Dry desquamation 10 ~4 weeks ~5 weeks
Moist desquamation 15 ~4 weeks ~5 weeks
Secondary ulceration 20 >6 weeks
Late erythema 15 ~6–10 weeks
Dermal necrosis 18 >10 weeks
Telangiectasia 12 > 52 weeks
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,74
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.3. Radiation-induced skin reaction
• Expression of moist desquamation and ulceration depends on
the relative rates of cell loss and cell proliferation of the basal
cells
• They occur more rapidly in murine (7 to 10 days) than in
human skin (2 to 4 weeks)
• The extent of these reactions and the length of time for
recovery depend on the dose received and the volume (area)
of skin irradiated, because early recovery depends on the
number of surviving basal cells that are needed to repopulate
the tissue

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,75
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.3. Radiation-induced skin reaction
Demarcated erythema above
right elbow at 3 weeks after
radiofrequency cardiac
catheter ablation
Koenig et al 2001
• Transient erythema in human skin occurs
after single doses greater than 2 Gy
• Main erythema occurs at doses greater than
about 7 Gy
• Moist desquamation and ulceration occur
after single doses of 15 to 20 Gy
After the desquamation reaches a peak value,
recovery and regeneration of the epidermis
will start from islands of surviving cells in the
basal layer

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,76
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.4. Radiation-induced cataract formation
• The lens of the eye contains transparent lens fibres and a
small number of dividing cells limited to the pre-equatorial
region of the epithelium within the lens capsule
• During life, the progeny of these mitotic cells differentiate into
lens fibres and accrete at the equator
• It has been known for many years that the lens of the eye is
very sensitive to radiation. Radiation even may lead to total
blindness
• If dividing epithelium is injured by radiation, opacity (spots or
cloudiness) of the lens (cataract) will develop because there is
no mechanism for removal of injured cells and abnormal fibres

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,77
20.12. RADIATION PATHOLOGY; ACUTE AND LATE EFFECTS
20.12.4. Radiation-induced cataract formation
Moderate doses of radiation can produce cataracts in a few
individuals, with the incidence increasing to 100 % in individuals
exposed to a single dose of 2 Gy or higher
• The frequency of cataracts varies with exposure to:
chronic doses – lower frequency
acute doses – higher frequency
• The time period between exposure and the appearance of cataract
might vary between about 6 months and 30 years. The radiation dose
greatly influences the latent period
• In general it can be stated that, the higher the dose the shorter the latent
period

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,78
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.1. Target cells for infertility
Radiation exposure to the gonads may lead to temporary or
permanent sterility or to hereditary effects in the offspring of the
exposed individuals, depending on the dose
The reproductive organs (gonads) of the human species are
in which the gametes are developed
• spermatozoa (in males)
• the ovum (in females)
• the testis (in males)
• the ovaries (in females)

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,79
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.1. Target cells for infertility
Effect of irradiation on Spermatogenesis:
• The process in which male spermatogonia develop into mature
spermatozoa is called spermatogenesis and starts with puberty
• The initial development starts with the spermatogonial stem cells,
which first proliferate to spermatogonia (type A and B), and then
differentiate into spermatocytes, (primary and secondary)
• The spermatocytes undergo meiosis to become haploid spermatids
Without further cell divisions, the spermatids differentiate into
spermatozoa
• The whole process will takes approximately 74 days in humans

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,80
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.1. Target cells for infertility
• The sensitivity of germ cells to a given dose of radiation is strongly
related to the stage they are in at the time they are irradiated
• Recovery of spermatogenesis will occur from the stem cell compartment
when the exposure is below the sterilisation dose Depending on the
dose, recovery to pre-irradiation levels of sperm might take 2 to 3
months up to several years
Effect of irradiation on Spermatogenesis:
The primary effect of radiation on the male reproductive system is:
• damage
• depopulation of the spermatogonia
eventually resulting in depletion of mature sperm in the testis

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,81
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.1. Target cells for infertility
Effect of irradiation on oogenesis:
• The process in which primary oocytes develop into the ovum (egg
cell) is called oogenesis and starts with puberty and ends with
menopause
• In contrast to spermatogenesis where new sperms are produced
all the time, the female can only produce a limited number of egg
cells since, after the foetal stage, oocytes no longer divide
• At birth a fixed number of oocytes are present and their number
diminishes steadily with age

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,82
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.1. Target cells for infertility
Effect of irradiation on oogenesis:
• During development from the primary oocyte to ovum, the
developing oocytes are very sensitive to radiation while the
primary oocytes and the ovum are less sensitive
• Maturation from primary oocyte to mature egg cells lasts several
months. Every month one mature egg cell (occasionally two or
three) is released during the menstrual cycle
• In the case of radiation exposure of one or both of the ovaries it is
recommended to delay a wanted pregnancy by at least 6 months
because in this period the developing and more radiosensitive
oocytes have been ovulated

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,83
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.2. Doses necessary for temporary and permanent infertility
• 1.0 Gy leads to a temporary reduction in the number of
spermatozoa
• 1.5 Gy leads to temporary sterility
• 2.0 Gy results in temporary sterility (for several years)
• 5.0 to 6.0 Gy (acute) can produce permanent sterility
In males, a dose of
• of 0.65 to 1.50 Gy will lead to a reduced fertility
• greater than 6.0 Gy produces sterility
The “sterility” dose is smaller for older women who have
fewer primary oocytes
In females, a dose

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,84
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.3. Genetic effects
At low doses, radiation may cause damage to the germinal cells
in the gonads which:
• do not lead to cell death
• but may lead to DNA-damage gene mutations
an increase in hereditary disease in the
offspring of exposed parents

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,85
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.3. Genetic effects
• Mendelian (mutation in a single gene)
• chromosomal
• multifactorial diseases
• Although animal studies clearly show the hereditary effects of
radiation, no hereditary effects have been observed in human
populations exposed to radiation
• For example no significant increase in heritable diseases was found
in a study on 70,000 children of Japanese A-bomb survivors whose
parent had received a conjoint radiation dose to their gonads of
0.15 Gy on average
Hereditary diseases are classified into three major categories:

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,86
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.3. Genetic effects
Based on mouse data:
the doubling dose is estimated to be 1 Gy, for
low dose-rate exposures
Doubling dose is the dose necessary to double the spontaneous
mutation frequency
There is no good reason to assume that in humans, the
doubling dose may differ significantly from that in mice
The mutation doubling dose does not give any useful
information on the risk of heritable disease. Therefore, the
mouse doubling dose is combined with information derived
from human population genetics to estimate the risk of
heritable disease in the progeny of irradiated people

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,87
20.13. RADIATION GENETICS: RADIATION EFFECTS ON FERTILITY
20.13.3. Genetic effects
The fact that the risk factor for workers is lower than the risk
factor for the whole population is due to the fact that the age
structure of both groups differs
For protection purposes, ICRP recommend a
risk factor for hereditary disease of:
• 0.2 % per Sv for members of the public
• 0.1 % per Sv for workers
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,88
20.14. FOETAL RADIATION
20.14.1. Foetal radiation effects vs. gestational date
• the radiation dose
• the stage of development at the time of exposure
Radiation-induced lethality and specific gross
abnormalities in the embryo and foetus are
dependent on two factors:
• pre-implantation (day 1 to 10)
• organogenesis (day 11 to 42)
• growth stage (day 43 to birth)
Between conception and birth, the foetus passes
through three basic stages of development:

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,89
20.14. FOETAL RADIATION
20.14.1. Foetal radiation effects vs. gestational date
• foetal or neonatal death
• malformations
• growth retardation
• congenital defects
• cancer induction
The principal effects of radiation on a foetus are:
• death of the conceptus
• early spontaneous abortion
Those embryos, however, which survive this
stage, develop normally
Embryos in the pre-implantation stage are very
radiosensitive and radiation damage inevitably will lead to:

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,90
20.14. FOETAL RADIATION
20.14.1. Foetal radiation effects vs. gestational date
• However, in most cases the damage to the foetus is too severe for
survival, ultimately resulting in neonatal death
• During this period the developing brain is very sensitive to radiation
• Irradiation during the foetal period (after week 6) results in a much
lower incidence of gross organ malformation abnormalities and mental
retardation
In the human early foetus, radiation exposure during the period of
major organogenesis will lead to the development of abnormalities,
mostly related to the:
• central nervous system (brain defects
and/or mental retardation)
• skeleton
• organ systems

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,91
20.14. FOETAL RADIATION
20.14.2. What to do when the foetus has been exposed to radiation?
• Systematic studies of the effect of radiation on the developing
embryo have been conducted in laboratory animals, particularly
mice and rats
• In experimental studies, no damage to the intrauterine
development of animals has been found for doses < 100 mGy
• In the studies of the Hiroshima children there is evidence for a threshold
dose of >100 mGy
• The risk of severe mental retardation increases rapidly to a value of 40 %
at 1 Gy
• In the later stages of pregnancy, the threshold dose may be higher
• At foetal doses >500 mGy, there can be significant foetal damage, the
magnitude and type of which is a function of dose and stage of pregnancy
IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,92
20.14. FOETAL RADIATION
20.14.2. What to do when the foetus has been exposed to radiation?
• The findings of a probable threshold of 100 mGy will influence
the advice to be given to pregnant women after a diagnostic
radiology procedure
• After abdominal CT investigations, careful analysis of the
radiation dose to the uterus as well as medical anamnestic
exploration has to be performed
• According to the ICRP- publication 84, termination of
pregnancy at foetal doses of less than 100 mGy is not justified
based upon radiation risk
• At foetal doses between 100 and 500 mGy, the decision
should be based upon the individual circumstances

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,93
20.14. FOETAL RADIATION
20.14.2. What to do when the foetus has been exposed to radiation?
The issue of pregnancy termination is undoubtedly
managed differently around the world
It is complicated by individual:
• ethical
• moral
• religious beliefs
• laws or regulations at a local or national level
This complicated issue involves much more than radiation protection
considerations and require the provision of counselling for the patient
and her partner

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,94
20.14. FOETAL RADIATION
20.14.2. What to do when the foetus has been exposed to radiation?
• Regarding the radiation induced risk of cancer, the ICRP-
publication 103 considers the life-time cancer risk following in-
utero exposure will be similar to that following radiation in early
childhood, i.e., at most, about three times of that of the
population as a whole (>15 % per Sv)
• So far no effect of gestational date on the cancer risk has been found
There is always a certain risk in a pregnant population not
exposed to radiation of:
spontaneous abortion (larger than 15 %)
intrauterine growth retardation (about 4 %)
genetic abnormalities (between 4-10 %)
major malformation (between 2-4 %)

IAEA
• HALL, E., GIACCIA, A.J., Radiobiology for the Radiologist, 6th edn,
Lippincott Wilkins & Williams, Philadelphia, USA (2006)
• INTERNATIONAL ATOMIC ENERGY AGENCY, Radiation Oncology
Physics: A Handbook for Teachers and Students, IAEA, Vienna (2005).
http://www-naweb.iaea.org/nahu/dmrp/publication.asp
• INTERNATIONAL ATOMIC ENERGY AGENCY, Radiation Biology: A
Handbook for Teachers and Students, Training Course Series, 42,
IAEA, Vienna (2010). http://www-
pub.iaea.org/MTCD/publications/PDF/TCS-42_web.pdf
• INTERNATIONAL ATOMIC ENERGY AGENCY, Radiobiology modules
in the “Applied Sciences of Oncology” distance learning course.
Available on CD Contact: [email protected], or downloadable
for free from the IAEA website:
http://www.iaea.org/NewsCenter/News/2010/aso.html
BIBLIOGRAPHY
Diagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,95
IAEA
BIBLIOGRAPHY
Diagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,96
• INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION,
Pregnancy and Medical Radiation ICRP Publication 84, Pergamon Press,
Oxford and New York (2000)
• INTERNATIONAL COMMISSION ON RADIOLOGICAL PROTECTION,
Recommendations of the ICRP, ICRP Publication 103, Annals of the ICRP
Volume 37/2-4, Elsevier (2008). via www.sciencedirect.com
• JOINER, M.C., VAN DER KOGEL, A.J., (Eds), Basic Clinical Radiobiology,
4th edn., Hodder Arnold, London, UK, (2009)
• KOENIG, T.R., WOLFF, D., METTLER, F.A., WAGNER, L.K., Skin injuries
from fluoroscopically guided procedures: part 1, characteristics of
radiation injury, AJR Am J Roentgenol 177 1 (2001) 3-11

IAEADiagnostic Radiology Physics: a Handbook for Teachers and Students – chapter 20,97
• NATIONAL RESEARCH COUNCIL OF THE NATIONAL ACADEMIES,
Health risks from exposure to low levels of ionizing radiation; BEIR VII
phase 2, Committee to Assess Health Risks from Exposure to Low
Levels of Ionizing Radiation, National Academies Press, Washington,
DC (2006). http://www.nap.edu/openbook.php?isbn=030909156X
• TANNOCK, HILL, BRISTOW, HARRINGTON, (Eds), The Basic
Science of Oncology, Chapters 14 & 15, 4th edn., McGraw Hill,
Philadelphia, (2005)
• WAGNER, L.K., EIFEL, P.J., GEISE, R.A., Potential biological effects
following high X-ray dose interventional procedures, J Vasc Interv
Radiol 5 1 (1994)
BIBLIOGRAPHY