challenging cases from clinical practice eric e. schmidt, o.d., faao omni eye specialists...
TRANSCRIPT

Challenging Cases From Clinical Practice
Eric E. Schmidt, O.D., FAAOOmni Eye Specialists
Wilmington, [email protected]

A Diagnostic Quandary
• 76 y/o WM cc: OD hurts, “like a toothache”• Pain is worse at night, lasts for 3-6 hrs.• 3 occurrences over past 2 weeks• VA has decreased since 1st episode• Type I DM – BS 130 today, sliding scale• MD says BP is “way hi recently”• BP med

Quandary Exam
• VA – OD 20/100 ph 20/80-2 OS 20/40 ph NIEOM – no rest.PERRL mg (-)SLE – K – cl OU
Conj – cl OULens – 2+/2+/1+ OD, 2+NS, 1+PSC OSAC – quiet OU, Gr 2 VH OU
IOP – 18 OD, 18 OS
Quandary cont
• Gonio – OD 3,2,2,1 OS 2,2,2,2
• DFE – Should you dilate these eyes?

Quandary Retina
• NPDR OU (OS > OD)• No CSME• No NVD, NVE• C/D - .3/.3 OU
• Anything else?

What is your differential diagnosis?
• How you treat this depends upon your diagnosis!!!>>>@@@@****

Quandary options
• Cataract extraction• PI OU• Glaucoma drops• Blood work• Refer to Internist• Refer to Retina• SLT OU• Retinal/ONH Imaging

I Rx’d Lumigan OU QHS
• Ordered labs– CBC – low RBC– ESR – 80mm/Hr– A1c – 5.3– C-RP – normal
• 2 wk f/up
2 week exam
• Pain had returned even w/ Lumigan• VA worsening• AC- mild cell OD, d & q OS• Angles – unchanged OU• IOP – 17mm OU• Retina – scattered h/MA OU, disk heme OS• Does this change your mind?
TA biopsy vs PI
• Pros and cons for each
• How did our man end up?

A Strange Cup Of Tea
• 68 y/o African –American• Treated for NTG x 12 yrs• Seidel’s scotomas OU• Notch at 2:00 OS• NTG well controlled w/ Lumigan OU QHS– (IOP ~ 11mm Hg)
• VF and rims now stable• VA stable at 20/20 OU

Routine Follow-Up?
• No subjective complaints• VA OD 20/30, OS 20/20• NI w/ refraction• When asked again – OD did feel “kind of
funny.”• PERRL mg (-), EOM- no restrictions• SLE – OS normal - OD as shown
Oh Yeah...
• IOP 42mm Hg OD, 14mm Hg OS
• What’s your next step?
• What is your differential diagnosis?

Glaucomatocyclitic Crisis
• Unilateral increased IOP w/ accompanying iritis
• No predispositioning, no precursors• Absence of all other findings• Mildly symptomatic• Diagnosis of exclusion• R/O ACG, NVG, Inflammatory G, PDS
Treatment
• Gonio is the key to the diagnosis• Lower IOP– Aqueous suppressors
• Quiet the anterior chamber reaction– PF QID– Taper quickly
• IOP sequelae?
Case Of The Sudden Vision Loss
• 17 y/o BM awoke that AM; “couldn’t see” out of OS.
• “somewhat painful”• Looked in mirror, noticed eye was totally white• Denies trauma• No precursors
Exam
• VA s Rx - OD 20/30, OS LP• Pupils - OD Round, reactive no inverse APD,
OS - not visible• SLE - OD prominent K nerves, no edema,
no bulb inj, OS as shown
• IOP 15 OD, 32 OS

Sudden Loss Question 1What other tests would you perform?
• 1. Gonioscopy• 2. Keratometry/Topography• 3. DFE• 4. Corneal pachometry• 5. VF• 6. Gonio & K Topo• 7. DFE & Gonio• 8. Pachometry & Keratometry

Sudden Loss Question 2What Is Your Diagnosis?
• 1. Angle Closure Glaucoma• 2. Corneal Edema• 3. Corneal Hydrops• 4. Corneal Perforation• 5. Pupillary block glaucoma• 6. Fuch’s dystrophy
Sudden Loss Question 3How would you treat it?
• 1. Adsorbonac 5% QID, TXE 0.5OS• 2. Penetrating Keratoplasty• 3. Betimol 1/2% OS BID, Eflone QID• 4. Pressure patch, Atropine OS• 5. BCL, Quixin OS QID• 6. BCL, Lotemax OS QID• 7. Eflone OS QID, Adsorbonac 5% OS QID
The Case Of The Low IOP
• The history :– 72 y/o BF w/ long-standing POAG– Trusopt BID, Xalatan QHS, Betimol ½ BID– IOP - hi teensOU– C/D - .8/.8 OD, 85/.85OS lamina visible OU– VF- OD mild double arcuate
OS- Seidel’s scotoma supVA – OD 20/70 OS 20/25SLE – cataracts OD > OS

Low IOP cont
• Px underwent combined procedure OD• 6 wks S/P surgery VA OD 20/20– IOP 3 OD, 21 OS– G meds OS Only
• 2 ½ years later:– Pain OD, VA 20/50 OD– 3+ bulb inj, 2+ AC cell– IOP – 3mm OD, 17mm OS– Fundus- hazy view

What is your management plan?
• 1. EP QID OD• 2. EP Q2H OD• 3. Atropine ½% OD, PF OD QID• 4. Retinal referral• 5. Glaucoma referral• 6. Vigamox OD QID
I Rx’d EP OD QID, HA5% OD BID
• 2 days later-– VA 20/50-2– Eye feels better– AC rxn 1+ cell– DFE- as shown

What is your diagnosis?
• 1. Choroidal detachment• 2. Posterior Uveitis• 3. Retinal detachment• 4. Retinoschisis• 5. Retinal tear
What are you going to do with this?
• 1. Retinal referral• 2. Glaucoma referral• 3. Pred Forte OD Q2H• 4. Close observation• 5. Run out of the door screaming!• 6. Calling Dr McGreal!

Why has this occurred?
• Prolonged hypotension?• Bleb problems?• Ciliary body shutdown?• Prolonged uveitis?
• **** Check The Bleb****

2 holes in surface of bleb
• Now what?– 1. BCL– 2. Vigamox OD QID– 3. PF QID– 4. BCL, TXE ½ QAM– 5. BCL, Vigamox TID– 6. Vigamox TID, TXE ½ QAM– 7. Vigamox TID, TXE ½ QAM, BCL

Trabeculectomy post-op
• Don’t want IOP too low for too long• Bleb management is the key– IOP hi, bleb hi– IOP hi, bleb flat– IOP low, bleb low– IOP low, bleb high
• Know what to look for, know how to treat

Causes of Ocular Hypotony
• 1. Wound Leak• 2. Ciliary Body Shutdown• 3. Choroidal detachment• 4. Retinal Detachment• 5. Uveitis

Choroidal Effusion
• Accumulation of Fluid in suprachoroidal space• Caused by trauma, hypotony or inflammation• Clinical Features:– Anterior displacement of choroid in annular,
lobular or flat arrangement– Must differentiate from RD– Can occur days, weeks or months post-op

Choroidal detachment
• CONSERVATIVE TREATMENT!!!• PANIC NOT!!!!– Patch if wound leak– Monitor closely if no wound leak– Try to elevate the IOP– Steroids???

The Case Of The “Sore Eye”
• 17 y/o WM CC: “Itch and Pain OD”• 3 weeks duration and it’s getting worse• Initially very itchy, now it is painful• FB sensation, photophobia, tearing• No known trauma, Rx’d Vasocon TID• Ext – Ptosis RUL, frank injection• SLE – AC –d & q, 1+ mucus d/c
What is the diagnosis?
• 1. Allergic conjunctivitis• 2. Corneal abrasion• 3. Bacterial keratitis • 4. Dellen• 5. Vernal keratoconjunctivitis

• How Do You Know It’s Not Infectious???

What Is The Best Treatment?
• 1.BCL and Gentamicin QID• 2. BCL and Xibrom BID• 3. BCL and Zymar QID• 4. Lotemax OD QID• 5. Vigamox OD TID• 6. Tobradex OD QID• 7. Vigamox and Nevanac TID each• 8. Some combination of these
Does She Or Doesn’t She?
• A Glaucoma Conundrum– 51 y/o WF– No family hx of G– BCVA 20/20 OD, OS– SLE – normal– C/D - .65/.75 OD, .65/.70 OS– IOP – 23 OD, 23 OS @ 8:40 AM– 22/22 @10:20AM, 25/26@3:30PM– Does she have glaucoma?

Based on this info would you...
• Start therapy?
• Get more data?
• Follow with routine care?

Additional Information
• Gonioscopy – Gr 4 360 degrees OU
• PMH: Htn, hypercholesterolemia
• Meds: Vasotec, Lipitor
• Pachs – OD 652, OS 668• Now would you treat?

Now what would you do?
• What is her “actual “ IOP?
• What is your target IOP for her?
• What type of glaucoma does she have?
• Which drop would you prescribe?

One last piece of the puzzle
• In our office IOP readings were...
– 23/21 gat, 18.0/16.3 Pascal
– 23/21 GAT, 18.3/17.3 Pascal
• Does this change anything?

As Many Disease As She Pleases
• 77 WF• Macular hole repair OS 8 yrs prior• Subsequent SRNVM w/ large macular scar• VA OD 20/20, OS HM@6’ – stable for 5 yrs• Recently complained of HA “alot” over OS• Says her vision OS is worsening, “it will go
black at times!”

Exam
• VA OD 20/25- OS – LP• SLE – OD no change, OS – 2+ PCO• DFE –OD - D,M,V,P wnl OS small macular
bleed adjacent to macular scar• ONH - .1/.1 OD pink, .15/.15 OS large area of
PPA• What now?• Did we forget something?

Ancillary Tests
• IVFA – no evidence of new SRNVM• OCT – Plush NFL, no SRNVM• ESR – 20mm/Hr• C-RP – 0.8
• What now? Is she just crazy?• Are you sure we haven’t overlooked anything?
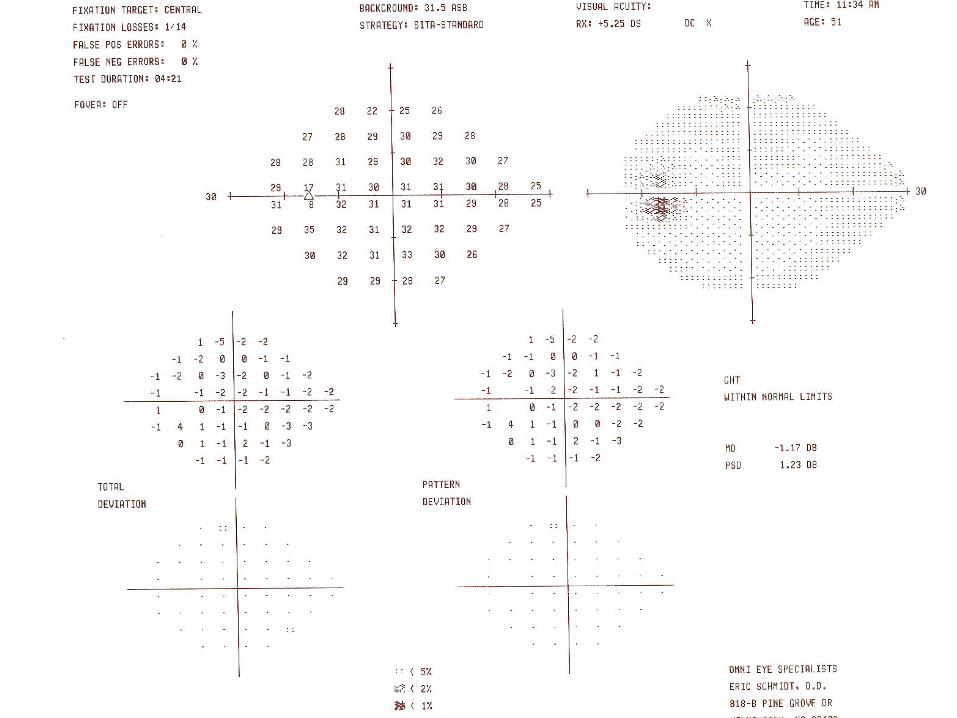
Explain the VF result
• NOW what would you do?

MRI
• Suprasellar mass with impingement on ON• Probable glioma• Underwent resection
• Craniopharyngioma!

The Case of Newfound Eyes
• 70 y/o F referred for chronic sore eyes• POH: Punctal plugs 3 yrs prior – moderate
improvement initially• Meds: Synthroid, Adalat, Calcium, ASA,
Refresh Tears QID• CC: Eyes burn and sting. Very red worse at
times. Mild stringy d/c. Vision seems worse• “I’m Allergic to everything!”

Newfound Data
• VA OD 20/25, OS 20/30• Ext: normal except for “ruddy” complexion• SLE: Lids – 1+ debris OU 1+ Meib inspissation OU 1+ bulb injection few papillae OU K – diffuse SPK OU Lens – 1+ NS OU
Which test do you want to do next?
1. Amsler grid2. Corneal topography3. Rose-Bengal Stain4. Schirmer’s strip5. TBUT6. Zone Quik

What is your diagnosis?
• 1. Ocular Surface Disease• 2. Blepharitis• 3. Ocular rosacea• 4. VKC• 5. Allergic conjunctivitis• 6. Bacterial conjunctivitis
What is the clinical key to making this diagnosis?
• 1. Look under the lids – check for papillae• 2. Look at the cornea – check for RB staining• 3. Look at her tears – check Schirmer’s test• 4. Look at her cheeks – check for
telangiectasia• 5. Look at her daughter – check for a wedding
ring

Considering that…
• She has punctal plugs,• She is using Patanol OU BID• She is using AT a lot• Has a Schirmer’s test of 3mm OD, 6mm OS• She has corneal staining• She continues to be symptomatic

How are you going to treat Newfound?
• 1. Doxycycline 100mg QD• 2. Lotemax OU QID• 3. Systane OU Q2H• 4. Refresh PM ung OU QHS• 5. Polysporin Ung OU QHS• 6. Restasis OU Q12H• 7. Acular LS OU TID• 8. Some combo of these

What I Did with Newfound
• RX Doxy 100 QAM• FML OU QID • AT PRN
• 1mth later she felt much better, lids were much clearer, no NaFl or RB staining
• Now what?

Long term therapy for Newfound?
• 1. Doxy 50 QD and AT• 2. Optive OU QID• 3. Restasis OU BID and AT OU QID• 4. Restasis BID and Doxy 50 QD• 5. FML OU BID and AT BID• 6. Lotemax BID and Restasis BID• 7. Doxy 100 QD and AT TID• 8. Vitamins and Flax seed oil