ch09 anaesthetics
TRANSCRIPT
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 1/21
By Justine Barry 3rd year student (October 2008)
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 2/21
For many children and young people having surgery, this may be their first and only experience of a hospital
environment. Admissions must be carefully planned to avoid any distress to the child and family, so careneeds to be provided by staff who are educated in the needs of the child/young person and their carers(RCN 2004).
Recommendations by the Royal College of Nursing suggest:
Specialist knowledge is needed to assess, plan, evaluate and implement the care required to meet the
needs of the child/young person and family.
Information must be pitched at a correct level to patient and parent so they can make an informed choiceabout the procedures.
The nurse must ensure the parent understands what to expect at the time of induction, offer supportduring and after this procedure, and keep them fully informed of progress.
The aim of this presentation is to provide a basic introduction to anaesthetics so you can relatethis to your practice on the ward. This will help you understand the need for
Pre and post operative observations, to gain a better understandingof drugs used in theatres and become familiar with the MDT’s involved.
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 3/21
• The word anaesthesia means theloss of the sensations of touch,pressure, pain and temperature inany part of the body, or in the wholeof it.
• Anaesthesia can be given in various
ways and does not always makeyou unconscious; it can just be usedto stop pain in an area of the body,this is called a local anaesthetic.
• A general anaesthetic is used
when you need
to be in a state ofcontrolled unconsciousness andfree of pain during a test oroperation. A combination of drugsgiven either as gas to breathe intothe lungs, or as an injection (NHS2008).
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 4/21
Analgesia Relaxation
Hypnosis
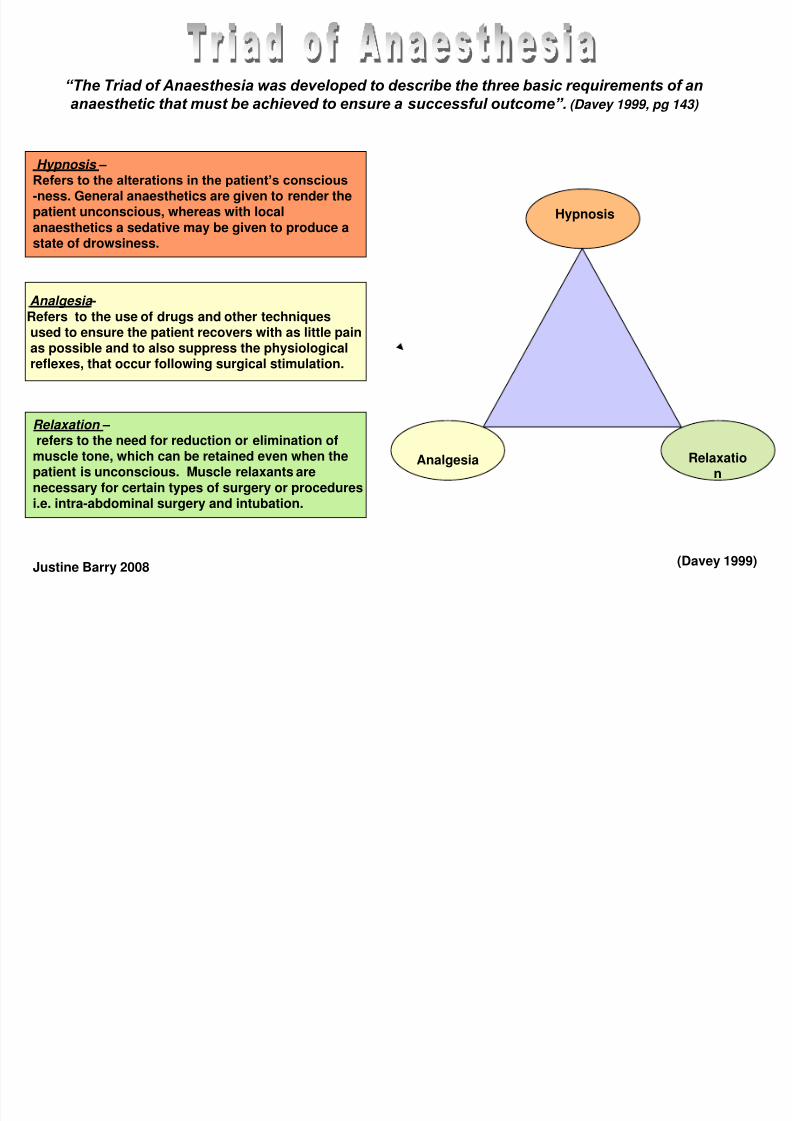
“The Triad of Anaesthesia was developed to describe the three basic requirements of an
anaesthetic that must be achieved to ensure a successful outcome”. (Davey 1999, pg 143)
Relaxation – refers to the need for reduction or elimination ofmuscle tone, which can be retained even when thepatient is unconscious. Muscle relaxants arenecessary for certain types of surgery or proceduresi.e. intra-abdominal surgery and intubation.
Hypnosis – Refers to the alterations in the patient’s conscious
-ness. General anaesthetics are given to render thepatient unconscious, whereas with localanaesthetics a sedative may be given to produce astate of drowsiness.
Analgesia -Refers to the use of drugs and other techniquesused to ensure the patient recovers with as little painas possible and to also suppress the physiologicalreflexes, that occur following surgical stimulation.
(Davey 1999)Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 5/21
KRAPP (2002)
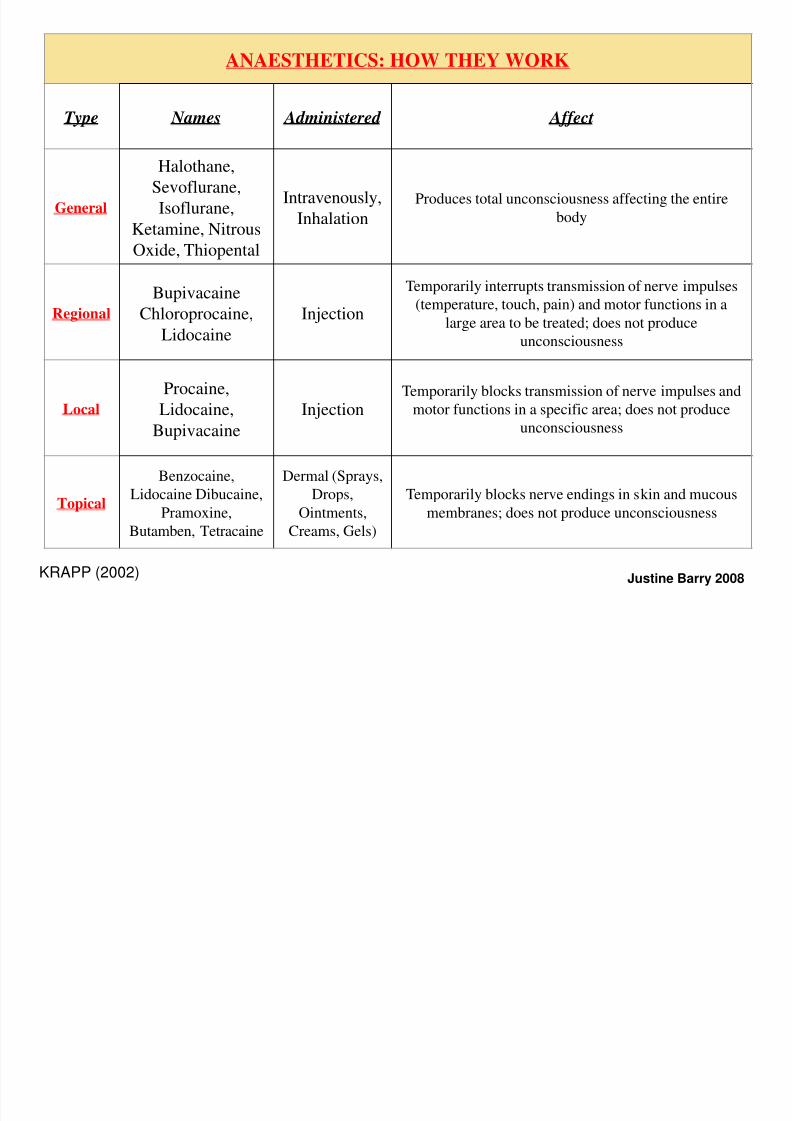
ANAESTHETICS: HOW THEY WORK
Type Names Administered Affect
General
Halothane,
Sevoflurane,
Isoflurane,
Ketamine, Nitrous
Oxide, Thiopental
Intravenously,
Inhalation Produces total unconsciousness affecting the entire
body
Regional
Bupivacaine
Chloroprocaine,
Lidocaine
Injection
Temporarily interrupts transmission of nerve impulses
(temperature, touch, pain) and motor functions in a
large area to be treated; does not produce
unconsciousness
Local
Procaine,
Lidocaine,Bupivacaine
Injection
Temporarily blocks transmission of nerve impulses and
motor functions in a specific area; does not produceunconsciousness
Topical
Benzocaine,
Lidocaine Dibucaine,
Pramoxine,
Butamben, Tetracaine
Dermal (Sprays,
Drops,
Ointments,
Creams, Gels)
Temporarily blocks nerve endings in skin and mucous
membranes; does not produce unconsciousness
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 6/21
1
2
3
4
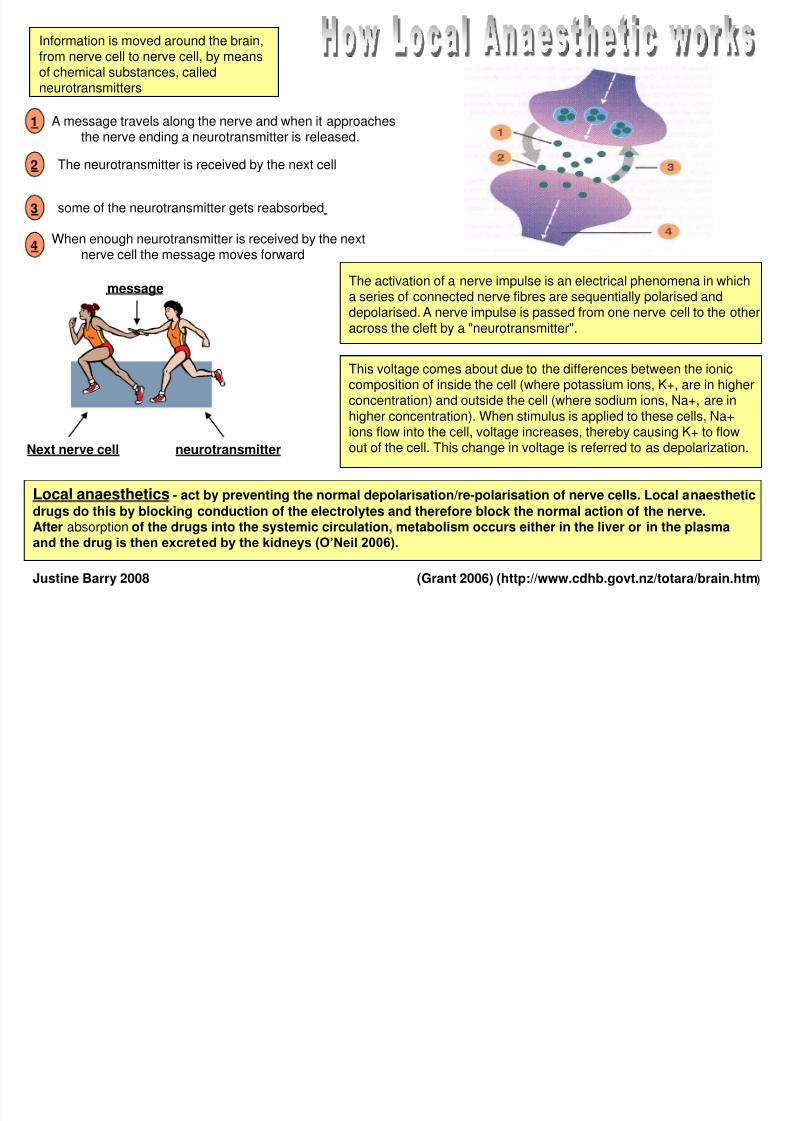
A message travels along the nerve and when it approaches
the nerve ending a neurotransmitter is released.
The neurotransmitter is received by the next cell
some of the neurotransmitter gets reabsorbed
When enough neurotransmitter is received by the nextnerve cell the message moves forward
(Grant 2006) (http://www.cdhb.govt.nz/totara/brain.htm)
neurotransmitterNext nerve cell
message
The activation of a nerve impulse is an electrical phenomena in whicha series of connected nerve fibres are sequentially polarised anddepolarised. A nerve impulse is passed from one nerve cell to the otheracross the cleft by a "neurotransmitter".
This voltage comes about due to the differences between the ioniccomposition of inside the cell (where potassium ions, K+, are in higherconcentration) and outside the cell (where sodium ions, Na+, are in
higher concentration). When stimulus is applied to these cells, Na+ions flow into the cell, voltage increases, thereby causing K+ to flowout of the cell. This change in voltage is referred to as depolarization.
Information is moved around the brain,from nerve cell to nerve cell, by meansof chemical substances, calledneurotransmitters
Local anaesthetics - act by preventing the normal depolarisation/re-polarisation of nerve cells. Local anaesthetic
drugs do this by blocking conduction of the electrolytes and therefore block the normal action of the nerve.After absorption of the drugs into the systemic circulation, metabolism occurs either in the liver or in the plasmaand the drug is then excreted by the kidneys (O’Neil 2006).
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 7/21
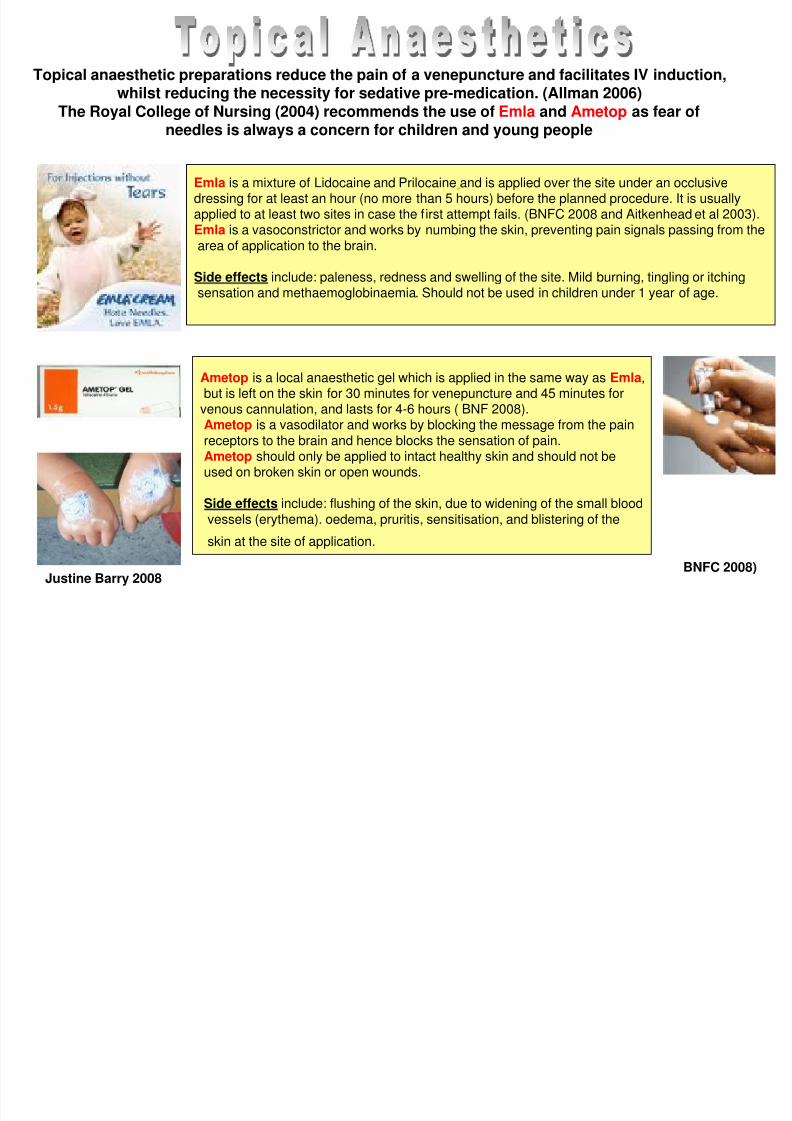
Topical anaesthetic preparations reduce the pain of a venepuncture and facilitates IV induction,whilst reducing the necessity for sedative pre-medication. (Allman 2006)
The Royal College of Nursing (2004) recommends the use of Emla and Ametop as fear ofneedles is always a concern for children and young people
Emla is a mixture of Lidocaine and Prilocaine and is applied over the site under an occlusivedressing for at least an hour (no more than 5 hours) before the planned procedure. It is usuallyapplied to at least two sites in case the first attempt fails. (BNFC 2008 and Aitkenhead et al 2003).Emla is a vasoconstrictor and works by numbing the skin, preventing pain signals passing from thearea of application to the brain.
Side effects include: paleness, redness and swelling of the site. Mild burning, tingling or itchingsensation and methaemoglobinaemia. Should not be used in children under 1 year of age.
Ametop is a local anaesthetic gel which is applied in the same way as Emla,but is left on the skin for 30 minutes for venepuncture and 45 minutes for
venous cannulation, and lasts for 4-6 hours ( BNF 2008).Ametop is a vasodilator and works by blocking the message from the painreceptors to the brain and hence blocks the sensation of pain.Ametop should only be applied to intact healthy skin and should not beused on broken skin or open wounds.
Side effects include: flushing of the skin, due to widening of the small bloodvessels (erythema). oedema, pruritis, sensitisation, and blistering of the
skin at the site of application.
BNFC 2008)Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 8/21
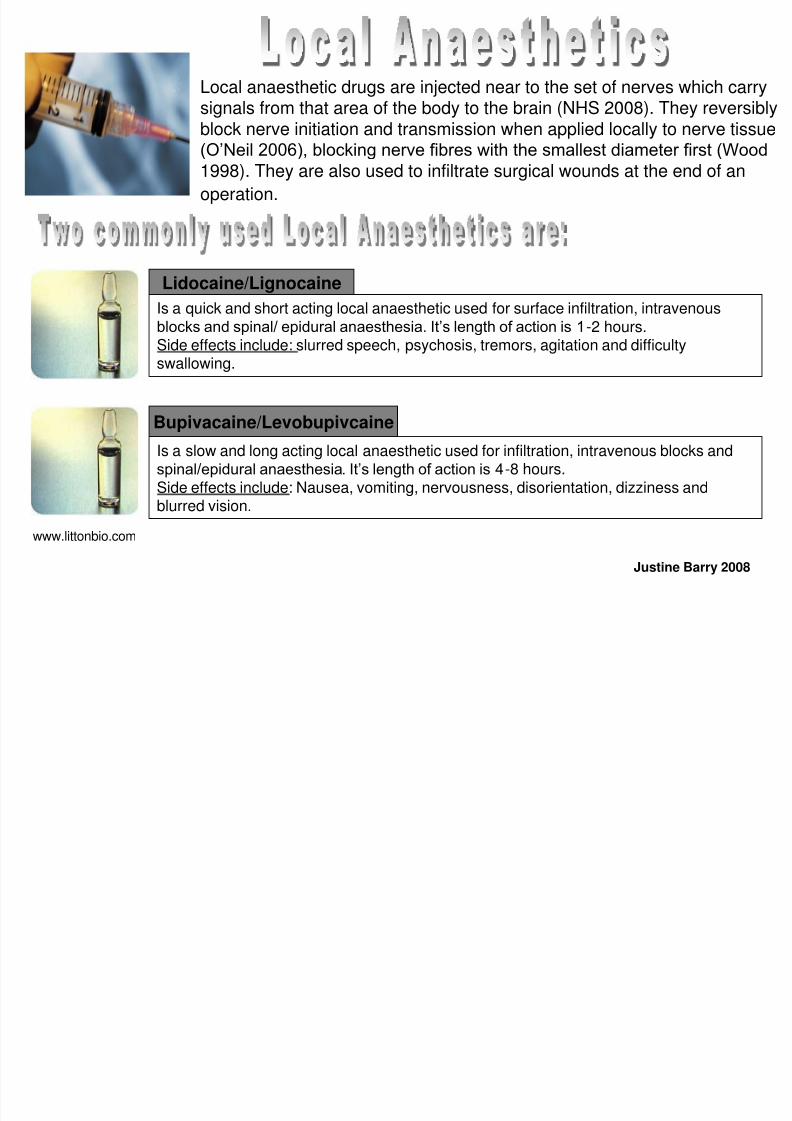
Local anaesthetic drugs are injected near to the set of nerves which carrysignals from that area of the body to the brain (NHS 2008). They reversiblyblock nerve initiation and transmission when applied locally to nerve tissue(O’Neil 2006), blocking nerve fibres with the smallest diameter first (Wood
1998). They are also used to infiltrate surgical wounds at the end of an
operation.
Is a quick and short acting local anaesthetic used for surface infiltration, intravenousblocks and spinal/ epidural anaesthesia. It’s length of action is 1-2 hours.Side effects include: slurred speech, psychosis, tremors, agitation and difficultyswallowing.
Is a slow and long acting local anaesthetic used for infiltration, intravenous blocks andspinal/epidural anaesthesia. It’s length of action is 4-8 hours.Side effects include: Nausea, vomiting, nervousness, disorientation, dizziness andblurred vision.
www.littonbio.com
Lidocaine/Lignocaine
Bupivacaine/Levobupivcaine
Justine Barry 2008

8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 9/21
Regional anaesthesia is used for operations on larger or deeper parts of the body. Localanaesthetic drugs are injected near to the set of nerves which carry signals from that
area of the body to the brain.
https:// healthlibrary.epnet.com .http://surgerycenter.spinalmedicine.com
Spinal Block Spinal anaesthesia is a major form of regional
anaesthesia, performed by injecting an anaesthetic drug between twoof the vertebrae of the lower back into the fluid between the discs. Thisblocks the nearby spinal nerves, causing a complete loss of feelingfrom that point down the body (NHS 2008).
Biers Block- Local Anaesthetic is injected into the limb, where the
blood flow is impeded by the application of a tourniquet, the drug isthen rapidly taken up from the venous system by the peripheral nerves
(Anaesthesia UK 2008).
“Epidural anaesthesia requiresa fine tube catheter to be left in the epidural
space, through which further injections or aninfusion of anaesthetic drugs can be given. Drugs
can also be given down the epidural catheter
after the operation to provide continuing painrelief in the postoperative period”
(NHS 2003, pg 16).
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 10/21
General anaesthesia is the induction of a balanced state of unconsciousness,
accompanied by the absence of pain sensation and the paralysis of skeletal muscle overthe entire body. It is induced through the administration of anaesthetic drugs and is used
during major and other invasive surgical procedures (Krapp, K. Cengage, G. (2002).
There are two major types of anaesthetics used for general anaesthesia, inhalation and
intravenous anaesthetics.
Inhalation anaesthetics, which are sometimes called volatile anaesthetics, are compounds that enter thebody through the lungs and are carried by the blood to body tissues (NDA 1998).The most commonly used anaesthetic vapours used in paediatrics are Sevoflurane, Halothane and Isoflurane. Inhalation anaesthetics act either by amplifying inhibitory function or decreasing excitatorytransmission at the nerve endings in the brain.
Volatile anaesthetics are seldom used alone, a combination of inhalation anaesthetics and intravenousdrugs is called balanced anaesthesia. Ideally, inhalation agents should provide a quick induction andemergence from anaesthesia, good analgesia, muscle relaxation, quick changes and easy maintenanceof anaesthesia (Wenker 1999).
Intravenous anaesthetics may be used to either induce anaesthesia or for the maintenance of anaesthesiathroughout a surgical procedure. TIVA is a total intra-venous anaesthesia, a technique where all drugs aregiven IV (BNFC 2008).
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 11/21
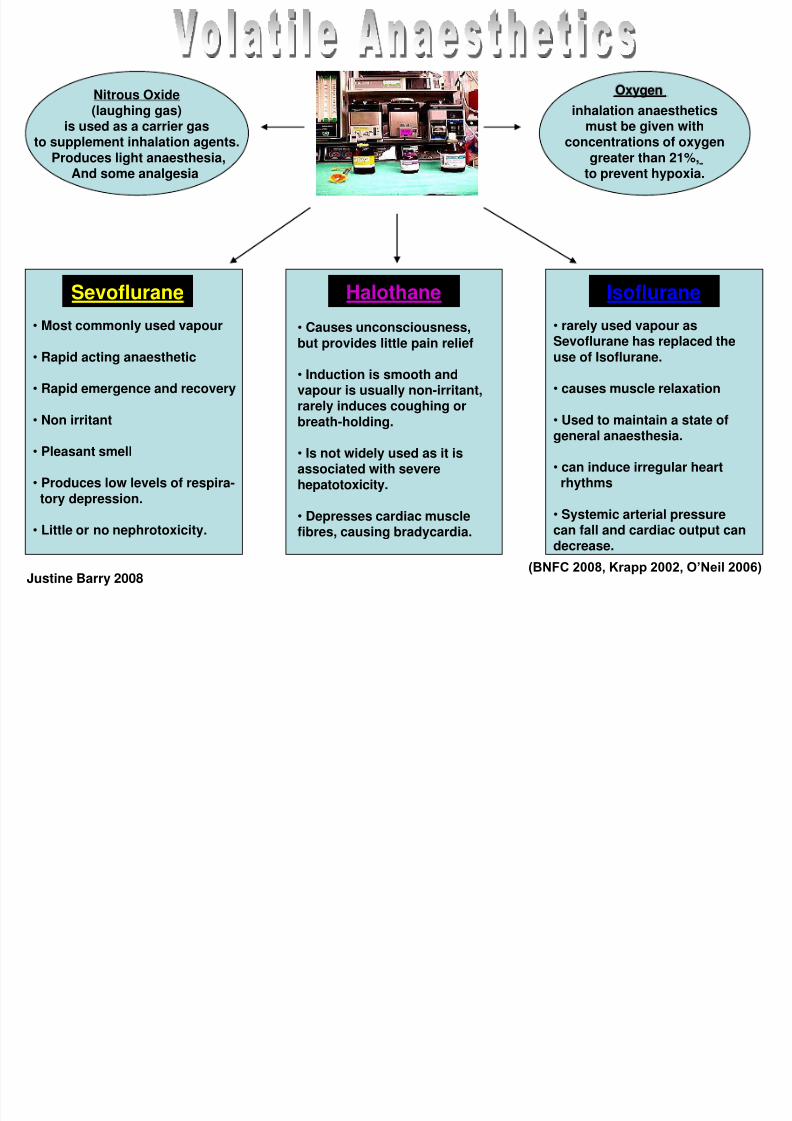
Sevoflurane Halothane Isoflurane
• Causes unconsciousness,but provides little pain relief
• Induction is smooth andvapour is usually non-irritant,rarely induces coughing orbreath-holding.
• Is not widely used as it isassociated with severehepatotoxicity.
• Depresses cardiac musclefibres, causing bradycardia.
• Most commonly used vapour
• Rapid acting anaesthetic
• Rapid emergence and recovery
• Non irritant
• Pleasant smell
• Produces low levels of respira-tory depression.
• Little or no nephrotoxicity.
• rarely used vapour asSevoflurane has replaced theuse of Isoflurane.
• causes muscle relaxation
• Used to maintain a state ofgeneral anaesthesia.
• can induce irregular heartrhythms
• Systemic arterial pressurecan fall and cardiac output candecrease.
Nitrous Oxide(laughing gas)
is used as a carrier gas
to supplement inhalation agents.Produces light anaesthesia,
And some analgesia
inhalation anaestheticsmust be given with
concentrations of oxygengreater than 21%,
to prevent hypoxia.
(BNFC 2008, Krapp 2002, O’Neil 2006)
Oxygen
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 12/21
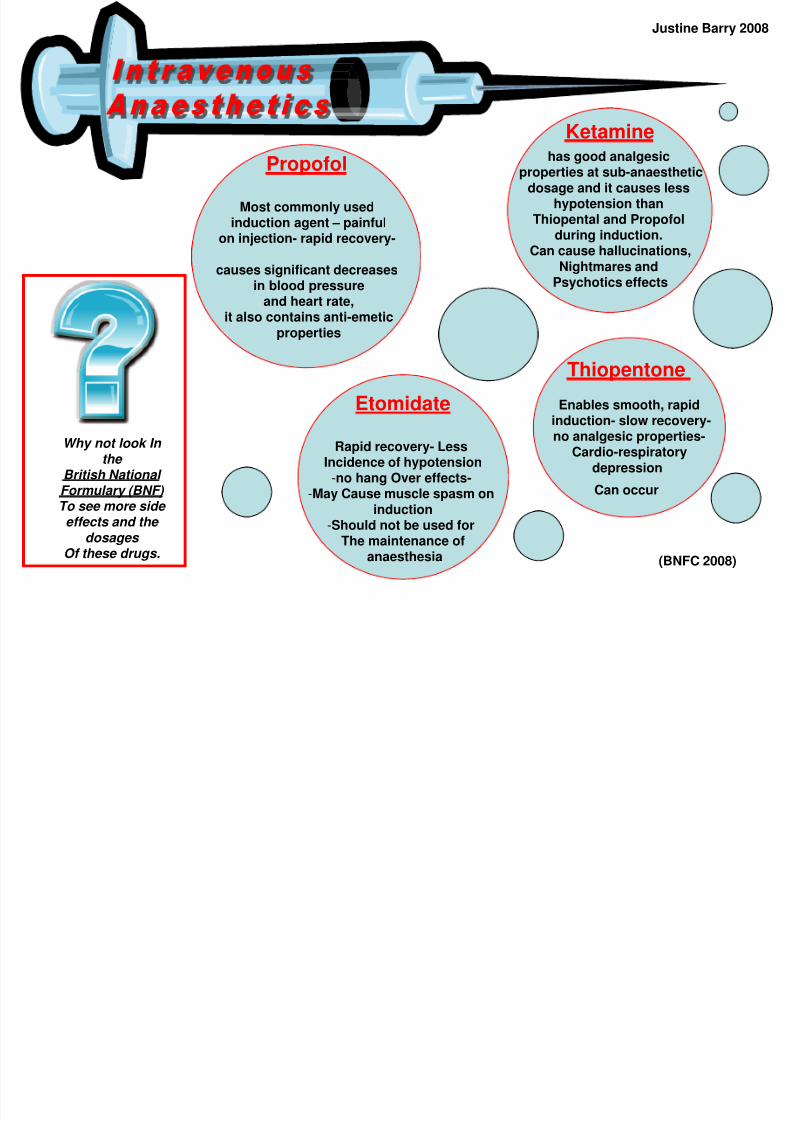
Etomidate
Rapid recovery- LessIncidence of hypotension
-no hang Over effects--May Cause muscle spasm on
induction-Should not be used for
The maintenance of
anaesthesia
Thiopentone
Enables smooth, rapid
induction- slow recovery-no analgesic properties-
Cardio-respiratorydepression
Can occur
has good analgesicproperties at sub-anaesthetic
dosage and it causes lesshypotension than
Thiopental and Propofolduring induction.
Can cause hallucinations,Nightmares and
Psychotics effects
Propofol
Most commonly usedinduction agent – painful
on injection- rapid recovery-
causes significant decreasesin blood pressure
and heart rate,it also contains anti-emetic
properties
Why not look In the
British National Formulary (BNF) To see more side effects and the
dosages
Of these drugs. (BNFC 2008)
Ketamine
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 13/21
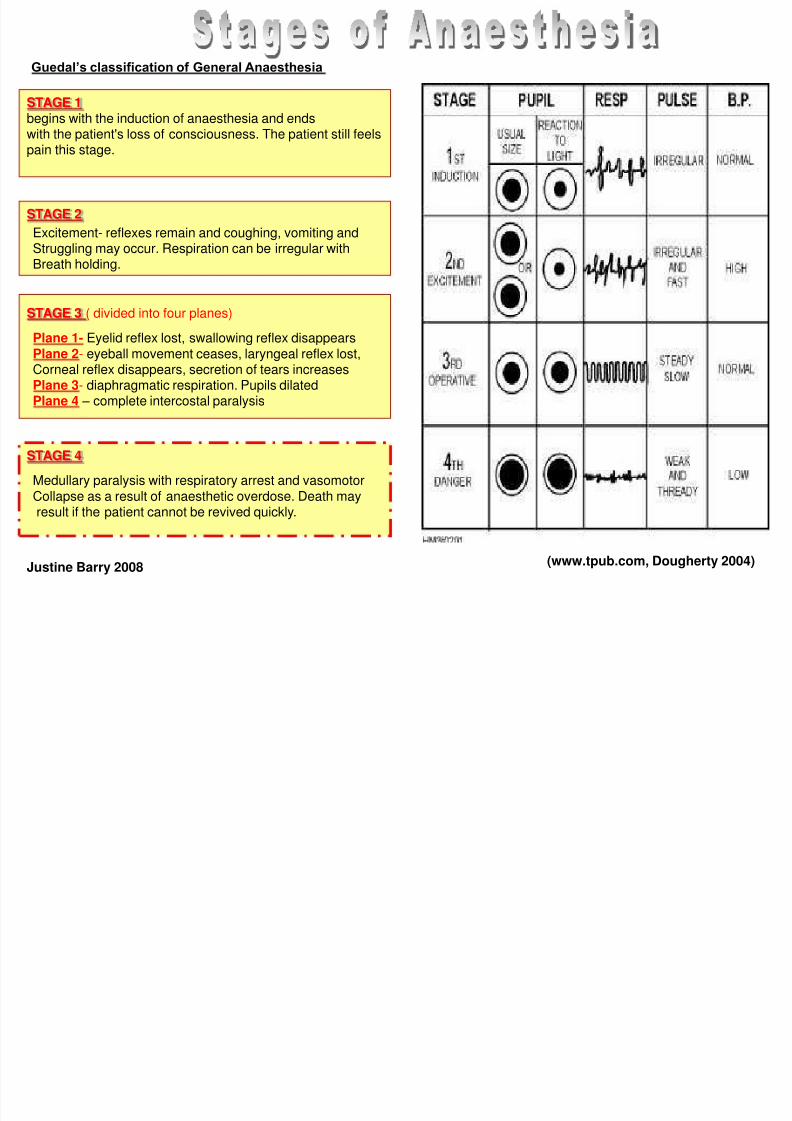
(www.tpub.com, Dougherty 2004)
STAGE 1begins with the induction of anaesthesia and ends
with the patient's loss of consciousness. The patient still feelspain this stage.
STAGE 2
STAGE 3 ( divided into four planes)
STAGE 4
Excitement- reflexes remain and coughing, vomiting andStruggling may occur. Respiration can be irregular withBreath holding.
Plane 1- Eyelid reflex lost, swallowing reflex disappearsPlane 2- eyeball movement ceases, laryngeal reflex lost,Corneal reflex disappears, secretion of tears increasesPlane 3- diaphragmatic respiration. Pupils dilatedPlane 4 – complete intercostal paralysis
Medullary paralysis with respiratory arrest and vasomotorCollapse as a result of anaesthetic overdose. Death mayresult if the patient cannot be revived quickly.
Guedal’s classification of General Anaesthesia
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 14/21
Drugs are sometimes, given to reduce fear and anxiety in the pre-operative patient,to relieve pain and discomfort when present, and to increase the action ofanaesthetic agents. Sedative pre-medication is rarely used in day-case patients asthe effects can be unpredictable and can cause excessive drowsiness post-
operatively (RCN 2004).A number of the drugs used also provide some degree of pre-operative amnesia.The choice will vary with the individual child, the nature of the operative procedureand the anaesthetic to be used. The choice also varies between elective andemergency operations. Oral administration is preferred where possible but it is notaltogether satisfactory; the rectal route should only be used in exceptionalcircumstances. (BNFC 2008)“Anticipation of the need for analgesia and pre-emptive treatment should be thenorm” (Doyle 2007, pg 146). The following are common drugs used for paediatric
premedication.
- (Benzodiazepines) is a oral premedicant commonly used to sedate children and given 30-60 minutesbefore the procedure. This sedative relieves anxiety and causes amnesia, useful for reducing thelikelihood of unpleasant memories of the procedure.
Midazolam
Paracetamol
Brufen
- Has anti-pyretic and analgesic properties, do not cause respiratory depression (unlikeopioid analgesics), are less irritant to the stomach than NSAID’s. Given orally, rectally and intravenously. Onset of action is approx 30 minutes.
- used to treat mild-moderate pain, do not depress respiration or impair gastro-intestinal motility and
don’t cause dependence. They are a useful alternative to opioids (side effects of which includerespiratory and cardiovascular depression) for the relief of post-operative pain. Onset of actionis approx 30 minutes.
(BNFC 2008)Justine Barry 2008
http://labs ansci uiuc edu
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 15/21
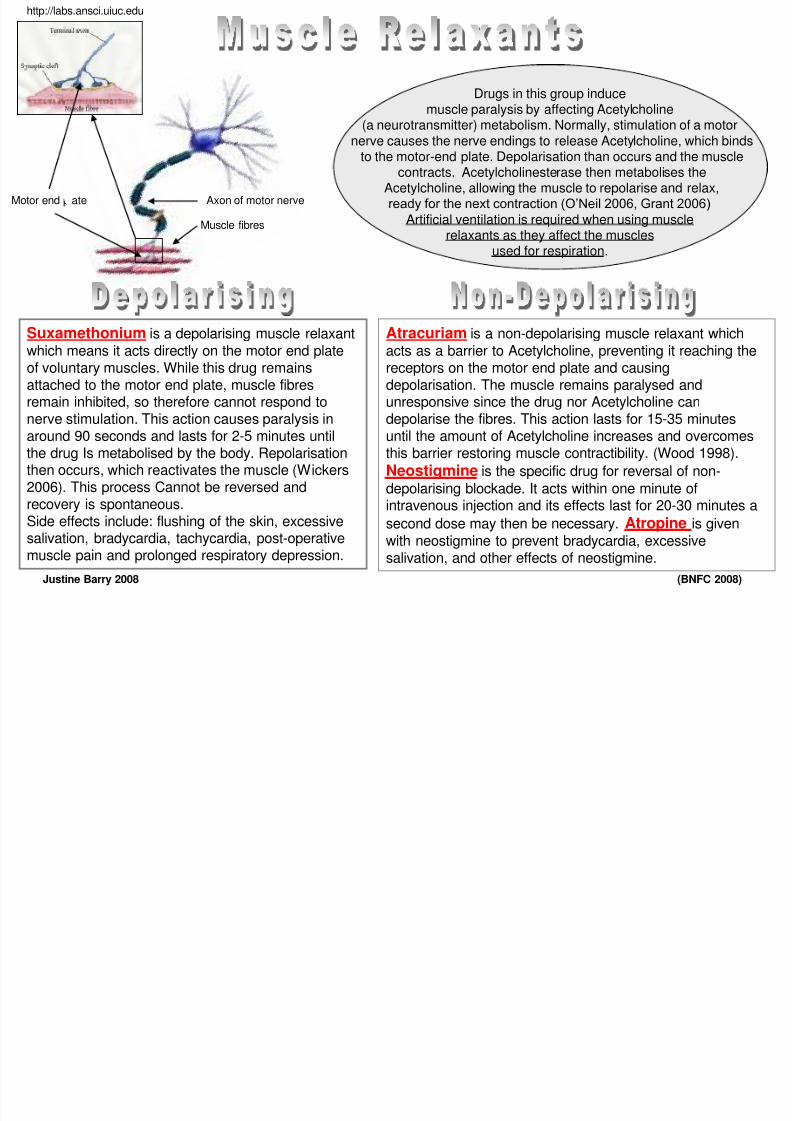
Suxamethonium is a depolarising muscle relaxant
which means it acts directly on the motor end plateof voluntary muscles. While this drug remainsattached to the motor end plate, muscle fibresremain inhibited, so therefore cannot respond to
nerve stimulation. This action causes paralysis inaround 90 seconds and lasts for 2-5 minutes untilthe drug Is metabolised by the body. Repolarisationthen occurs, which reactivates the muscle (Wickers2006). This process Cannot be reversed andrecovery is spontaneous.Side effects include: flushing of the skin, excessivesalivation, bradycardia, tachycardia, post-operative
muscle pain and prolonged respiratory depression.
Atracuriam is a non-depolarising muscle relaxant which
acts as a barrier to Acetylcholine, preventing it reaching thereceptors on the motor end plate and causingdepolarisation. The muscle remains paralysed andunresponsive since the drug nor Acetylcholine can
depolarise the fibres. This action lasts for 15-35 minutesuntil the amount of Acetylcholine increases and overcomesthis barrier restoring muscle contractibility. (Wood 1998).
Neostigmine is the specific drug for reversal of non-
depolarising blockade. It acts within one minute ofintravenous injection and its effects last for 20-30 minutes a
second dose may then be necessary. Atropine is given
with neostigmine to prevent bradycardia, excessive
salivation, and other effects of neostigmine.
Motor end plate Axon of motor nerve
Muscle fibres
Drugs in this group inducemuscle paralysis by affecting Acetylcholine
(a neurotransmitter) metabolism. Normally, stimulation of a motor
nerve causes the nerve endings to release Acetylcholine, which bindsto the motor-end plate. Depolarisation than occurs and the muscle
contracts. Acetylcholinesterase then metabolises theAcetylcholine, allowing the muscle to repolarise and relax,ready for the next contraction (O’Neil 2006, Grant 2006)
Artificial ventilation is required when using musclerelaxants as they affect the muscles
used for respiration.
http://labs.ansci.uiuc.edu
(BNFC 2008)Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 16/21
Opiates such as Morphine and
Fentanyl, are potent analgesicswhich play a major role in themanagement of moderate andsevere pain in children. They areused for reducing pain, anaestheticand surgical distress and they areoften used pre, Intra and post-operatively. Opiates can be given via
intramuscular, intravenous,oraltopical and intrathecal routes.
The side effects of opiates include:euphoria, respiratory depression,depression of the coughing reflex,nausea and vomiting, reduction ofsmooth muscle contraction and
cardiovascular depression.
Opiate Antagonists, such as Naloxone and Nalorphine, supportthe patient’s respiratory and
cardiovascular system duringreversal of anaesthesia and post-
operative care.
(BNFC 2008, Dougherty 2004, Doyle 2007 and O’Neil 2006)
Paracetamol and Non-Steroidal Anti Inflammatory Drugs (NSAID’s) arecommonly used non-opioids used for managing pain following minorsurgical procedures or when the pain following major surgery begins tosubside.NSAID’s such as Diclonfenac and Ibuprofen, provide better painrelief than paracetamol and can be used alone or in combination withparacetamol and opioids. Side effects of NSAID’s include coagulation
problems,Renal impairment, diarrhoea, nausea and gastrointestinal
disturbances limit their use.
“Paracetamol remains the most popular and widely used prescribedanalgesic and antipyretic and forms the mainstay of almost all analgesic
regimens” (Doyle 2007, pg 156). Paracetamol has a very good safety record and can be given orally, IVand rectally. Side effects are rare, but can include: rashes, blooddisorders and hypotension reported on infusion.
“Analgesics are a complex group of drugs….they act by either reducing
capacity of the nerve fibres to sense pain or by reducing pain recognition by the higher Centres of the brain.”
(O’Neil 2006, pg 109)
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 17/21
An Anaesthetist is “A medically qualified doctor who cares for a patient during a surgical
procedure and administers either a general or regional anaesthetic. Anaesthetists alsoassess the state of a patient’s health before a planned surgical procedure, and are often
involved in caring for the patient post-surgery. Most specialists in intensive care and painmanagement are anaesthetists” (NHS 2003, pg 50).
Anaesthetists are supported in their work by other members of the healthcare team. The following are just four of the many professionals involved.
Operating Department Practitioners (ODPS) and Anaesthetic Nurse“ are integral to operatingpractice and safe, effective care”. (Wicker and O’Neil 2006, pg 243). Their duties include: assisting the
anaesthetist in maintaining anaesthesia, recording fluid balance, transfusions and recording thepatient’s vital signs. (Moss 2007) Recovery Nurse – is post-operatively responsible for maintaining a safe patient airway, monitoring ofvital signs, checking wound sites, assessing the patients pain level and if necessary, administeringanalgesia. After complete recovery, completion of documentation and a concise handover is deliveredto ward staff. (Moss 2007)
Pain Team- are staffed by consultant anaesthetists and registered specialistnurses offering guidance on pain control for patients with: surgical, medical,trauma and acute post-operative pain. All patients with epidural analgesiaand morphine infusions are followed up by the pain team. The acute painservice also provides continuing education and support for the other ward-based staff who may be involved in the monitoring and provision of
pain relief. (AAGBI 2001)Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 18/21
“All patients should have had a basic physical examination of the cardiovascular and
respiratory systems conducted by a medical practitioner. The anaesthetic room is not theappropriate place for an anaesthetist to see an un-assessed patient for the first time prior tosurgery. The hospital system must allow time for patients to be seen pre-operatively by the
anaesthetist. If this is not the case, elective operations may have to be cancelled.The pre-operative visit also provides an ideal opportunity for teaching trainees and otherhealthcare staff about pre-anaesthetic assessment” (AAGBI 2001 pg 4).
Pre-operative checklist the Patient Agreement to Investigation/Treatment formis completed and signed. side and site of the operation is marked and this isdocumented.
the patient should be starved as per the trust pre-operative guidelines and the times of the last food/fluidsnoted on the checklist. any jewellery needs to be removed to prevent possibleburns from the diathermy or loss into an open wound.(Digger 2005)
The ward staff must take all the patients medical recordsand documents to the anaesthetic room in order fortheatre staff to correctly check the patient’s details.
“Ward staff, the collecting/receiving staff
from theatres, the Anaesthetist and the surgeon/surgical team have linked, but separate responsibilities. The potential
for human error is such that patient
checking must be a shared responsibility that can never be delegated to a single person” (Digger 2005, pg 5).
The Objectives of Pre-Operative assessment
The aim in assessing patients before anaesthesia andSurgery is to improve outcome. This is achieved by:
• identifying potential anaesthetic difficulties
• identifying existing medical conditions
• improving safety by assessing and quantifying risk • allowing planning of peri-operative care• providing the opportunity for explanation and discussion • allaying fear and anxiety
Good pre-operative assessment will help to:• reduce costs
• increase efficiency of operating theatre time
Such action should:• reduce the number of patients who fail to attend on the day
of surgery• reduce cancellation of surgery for clinical reasons
Patients should have access to easily understood information.Such information may be conferred through patient advocates
or via information sheets in an appropriate language.(AAGBI 2001, pg 6)Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 19/21
The immediate postoperative care is as critical as the intra-operative careand the child should be taken to a recovery area with trained staff (NDA 1998)
The recovery nurse will obtain a full account of:
• the operation that has been performed
• instructions from the anaesthetist with regards to positioning of the patient, O2 therapy, IV fluids and painmanagement.
• Instructions from the surgeon about drains, packs, catheters and recommencement of oral feeding.
Children are observed on a 1:1 nurse to patient ratio and are continuously monitored for oxygensaturation (Sa02), temperature, blood pressure (BP), colour, respirations, and consciousness . All vitalsigns are recorded at five minute intervals to detect any signs of deterioration, distress or pain. Childrenare nursed on a tilting trolley to protect the child’s airways should they vomit.
Oxygen is given initially to post-operative patients on reversal of anaesthesia toencourage the transport of anaesthetic gases across the alveolar/capillary membrane
in the lungs and out of the body. Supplemental oxygen is often required in higherconcentrations because of the increase in the metabolic rate caused by surgery, sinceit results in physiological stress and trauma (Hughes 2004).
This is essential in order to gain and relay accurateinformation to ward staff, which will facilitatesmooth and on going transition of care. (CMMC
2004)
Why not look at effects Of post-operative
Complications PONV And Hyperthermia?
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 20/21
Please return this CD for the next person to use. If you require a copy either print or save
to a pen-drive.
Thank you.
ByJustineBarry3 rd year student (October 2008)
DISC
DISCERE
HERE
Justine Barry 2008
8/2/2019 Ch09 Anaesthetics
http://slidepdf.com/reader/full/ch09-anaesthetics 21/21
• AAGBI (2001) Pre-operative assessment and the role of the Anaesthetist. AAGBI. London• Aitkenhead, A.R, Rowbotham, D.J, and Smith. G. (2003) Textbook of Anaesthesia. 4th Ed. Churchill Livingstone.
London.• Allman K.G and Wilson, I.H.(2006) Oxford Handbook of Anaesthesia. 2nd Ed. Oxford University Press. Oxford.
• British National Formulary. (2008) BNF for Children. British Medical Journal. London.• Central Manchester and Manchester Children’s University Hospitals (2004) procedure for the care of the child in
the recovery room following general anaesthesia. NHS.• Davey A, Ince, C,S (1999) Fundamentals of Operating Theatre Practice. Cambridge University Press. Cambridge.• Davis, P.J Motoyama, E.K (2006) Smith’s Anaesthesia for Infants and Children. 7th Ed. Mosby Elsevier. USA.• Dougherty L, Lister S (2004) The Royal Marsden Hospital Manual of Clinical Nursing Procedures. 6th Ed.
Blackwell. Oxford• Doyle, E (2007) Paediatric Anaesthesia. Oxford University Press. Oxford.• Grant A, Waugh A (2006) Ross and Wilson- Anatomy and Physiology in Health and Illness. 10th Ed. Churchill
Livingstone. London. Digger T (2005) The Dudley Group Of Hospitals NHS Trust- Policy For Safe PatientPreparation Prior To Surgery.
• Hughes E (2004) Principles of post-operative patient care. Nursing Standard . 19, 5, 43-51. Date of acceptance:July 12 2004.
• Krapp, K. Cengage, G. (2002)."Anesthesia, General." Encyclopaedia of Nursing & Allied Health. Ed. 2002.• Moss, M (2007) Central Manchester and Manchester Children’s University Hospitals- Student Welcome pack
(surgical). CMMC.• NHS (2003) Clinical standards for Anaesthesia-Scotland. NHS Quality Improvement Scotland. Glasgow.• O’Neill J, Wicker P (2006) Caring For The Perioperative Patient. Blackwell Publishing. Oxford • Royal College of Nursing (2004) Children/young people in day surgery. RCN. London
• Wenker O: Review of Currently Used Inhalation Anaesthetics; Part I. The Internet Journal of Anaesthesiology1999; Vol3N2:
• http://www.ispub.com/journals/IJA/Vol3N2/inhal1.htm ; Published April 1, 1999; Last Updated April 1, 1999 .• https://healthlibrary.epnet.com Spinal and Epidural Anaesthesia by Rosalyn Carson-DeWitt, MD• http://www.nwfsc.noaa.gov• http://www.frca.co.uk – Anaesthesia UK-Guanethidine Biers blocks (2008)• www.nda.ux.ac.uk- (1998) Paediatric Anaesthesia Review. Issue 8 Article 2.