cesarean section rates in italy by hospital payment mode: an
TRANSCRIPT

Cesarean Section Rates in Italy byHospital Payment Mode: An AnalysisBased on Birth CertificatesRoberto Bertollini, MD, MPH, Domenico DiLallo, MD, Teresa Spadea,PhD, and Carlo Perucci, MD
IndrdudionCesarean section (CS) deliveries
have consistently increased in the pastdecades in Europe, North America, andthe Pacific.' In the United States one outof four deliveries took place by CS in1988,2 and CS is the most common surgi-cal procedure.3 High CS rates are also ob-served in developing countries such asBrazil4 and Puerto Rico.5
Several explanations and hypotheseshave been offered to explain this impres-sive change in medical practice, such as apolicy of subsequent cesarean delivery af-ter a first cesarean, reluctance to deliverbreech babies vaginally, and fear of mal-practice suit.6
The use of CS for delivery is associ-ated with nonclinical factors: socioeco-nomic status of women,7 physician prac-tice style,89 physician work schedule,10and private or clinic care.11 It has beenshown in the United States that source ofpayment for obstetrical care is stronglyassociated with CS use, with women pri-vately insured having the highest CSrate.12 This observation was not con-firmed in other countries with differenthealth care systems.
In a previous preliminary report fo-cusing on 1985 data regarding the Lazioregion of Italy, we observed a high overallfrequency ofCS (22.5%) and a higher ratein private maternities (32.3%), wherewomen pay all expenses for delivery.13 Toconfirm this preliminary finding and inves-tigate CS time trends, we analyzed birthcertificate data for single infants born in1985 through 1987 to women resident inthe Lazio region. We compared the ratesof CS by hospital payment mode aftercontrolling, with logistic regression anal-ysis, for the potential confounding effectsof age, parity, birth weight, gestationalage, presentation at birth, and day of de-livery.
Materials and MehodsThe study was based on an analysis
of the birth certificates of single infants
(live or stillborn) weighing more than 500g and born to women resident in Lazio, alarge region of central Italy, in the years1985 through 1987. The largest city of theregion is Rome, and the total regional pop-ulation is about 5 100 000. Birth certifi-cates are collected by the Medical BirthRegistry coordinated by the Epidemiol-ogy Unit of the Regional Health Author-ity. Data on births are routinely linked todeath certificates regarding deaths in thefirst year of life. The characteristics of theregistry and the validation of data are de-scnibed elsewhere.14
Hospital of birth was classified ac-cording to mode of medical care payment.There are three types of maternities in theItalian National Health Service (NHS): (1)NHS public hospitals, where medical careis provided free of any charge; (2) NHSprivate hospitals, where NHS pays a por-tion of the expenses (e.g., daily fees andmedication) and the patient is responsilblefor physician fees and special services(e.g., individual room); and (3) privatehospitals, where patients pay all expensesand no support is provided by NHS.
There are 96 maternities in the region(56NHS public hospitals, 26NHS privatehospitals, and 14 private hospitals), with atotal of about 47 000 births per year. Allprivate hospitals are small unitswith a lownumber of births (e.g., the mean in 1986was 191 births per year). Only 5 hospitalshave more than 1500 births per year; 2 areteaching hospitals.
The initial cohort considered for thepresent study consisted of 139 284 singlebirths; 2618 subjects were excluded (90home births and 2528 with unknown in-formation on mode ofdelivery and/or hos-pital of birth). The final cohort studied in-cluded 136 666 single hospital births. CS
The authors are with the Lazio Region Epi-demiology Unit, Rome, Italy.
Requests for reprints should be sent toRoberto Bertollini, MD, MPH, Lazio RegionEpidemiology Unit, Via di S. Costanza 53,00198, Roma, Italy.
This paper was submitted to the journalApril 30, 1991, and acceptedwith revisions Sep-tember 16, 1991.
American Journal of Public Health 257

Pubic Health Briefs
rates were obtained by dividing the num-ber ofcaesareans by the appropriate num-ber of births (per 100).
Consistent with past research,15-17variables potentially predictive of CSwere considered: maternal age, parity,gestational age, birth weight, presentationat birth, and day of the week of birth(weekday vs Sunday). The latter variablewas considered because it had been asso-ciated with CS frequency in a previousanalysis.18 The Italian birth certificatedoes not include information on compli-cations ofpregnancy such as previous CS,dystocia, and fetal distress.
The strength of the association be-tween CS rate, hospital payment, and theother predictive variables was evaluatedusing the odds ratio (OR); 95% confidenceintervals (CIs) of the ORs were obtainedusing the test-based method.19 Timetrends were evaluated using the extendedMantel-Haenszel test.20
To assess the constancy of the rela-tionship between payment source and CSrates, the data were stratified by matemalage, parity, birth weight, gestational age,presentation at birth, and day of deliveryand the adjusted ORs calculated accord-ing to the Mantel-Haenszel method.21 Tofurther validate the findings derived fromthe above method, logistic regressionanalysis was employed to simultaneouslyestimate the independent effect of pay-ment mode adjusted for the other predic-tive variables. The results ofthe multivari-ate analysis closely agreed with those ofthe tabular one. No statistical criteria
(such as the stepwise procedure)were em-ployed to select variables tobe included inthe model. Tests of significance for modelselection depend on the size ofthe studiedpopulation, and, in large studies such asthe present one, any trivial variable mayhave a highly significant association withthe event under study (small P values)regardless of its epidemiological and clin-ical meaning.22 Adjusted ORs and 95%CIs were derived from the estimated re-gression coefficient.23 An interaction term(parity by maternal age) was included inthe equation to take into account the jointeffect of these two variables.
ResulsThe overall rate of CS in the years
1985 through 1987 among the 136 666women delivenng single infants in Lanziowas 23.1% (Table 1). A marked statisti-cally significant time trend (P < .0001)was observed over the time period studied(from 22.3% in 1985 to 24.3% in 1987).Provisional data for 1988 indicated a rateof 25.2% (R.B., unpublished data, 1991).Operative deliveries (forceps plus vac-uum) constituted 2.8% of total deliverieswithout significant time trends.
A strong relationship was found be-tween mode of hospital payment and CSrate. Women delivering in private hospitalshad the highest CS rate (34.7%), while therate of abdominal deliveries was lowest inNHS public hospitals (21.3%) (Table 2).
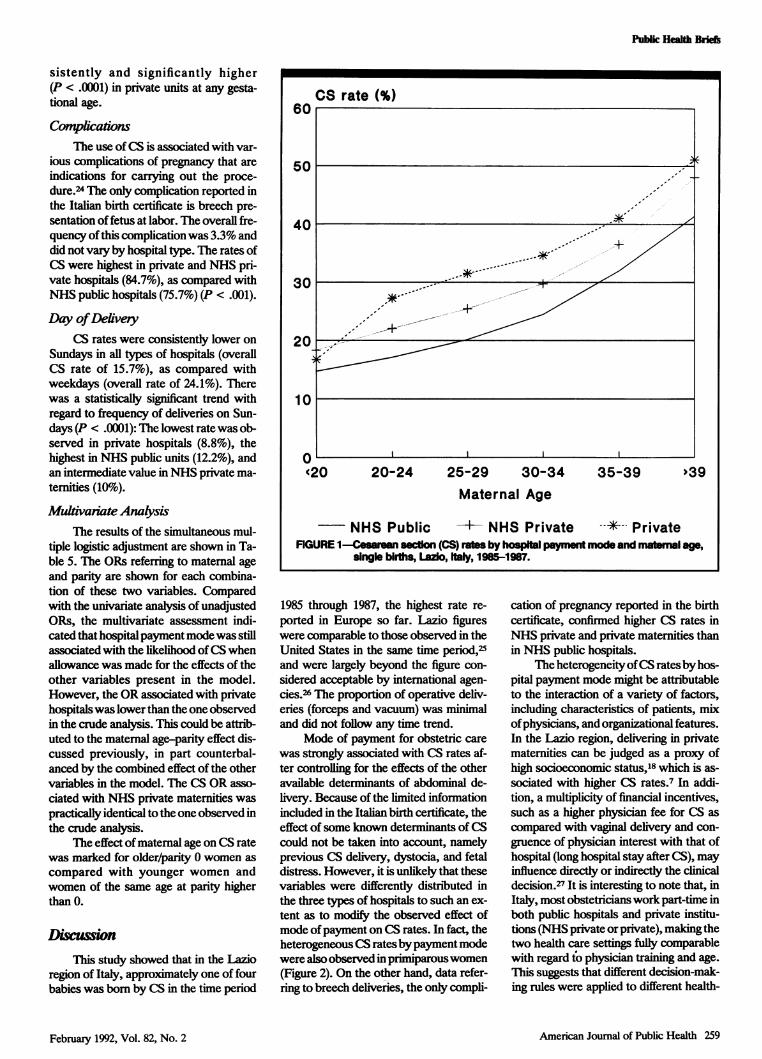
MatemalAgeThe CS rate increased with matemal
age: rates ranged from 16.4% amongwomen younger than 20 years to 43.8%among those older than 39, an OR of 3.97(95% CI = 3.54, 4.45). The rate was18.2% among women 20 through 24,21.7% among women 25 through 29,26.4% among women 30 through 34, and33.9% among women 35 through 39.
CS rates in private hospitalswere sig-nificantly higher than those in NHS pri-vate and public hospitals in all age classes,except among theyoungerwomen (Figure1). In the lattergroup, women delivering inNHS private institutions experienced thehighest CS rate (18.3% vs 14.7% in NHSpublic and 16.6% in private hospitals); thedifference among the three types of hos-pitals was of borderline statistical signifi-cance (P = .055). The CS rate amongwomen older than 39 was extremely highin the private hospitals (51.1%).
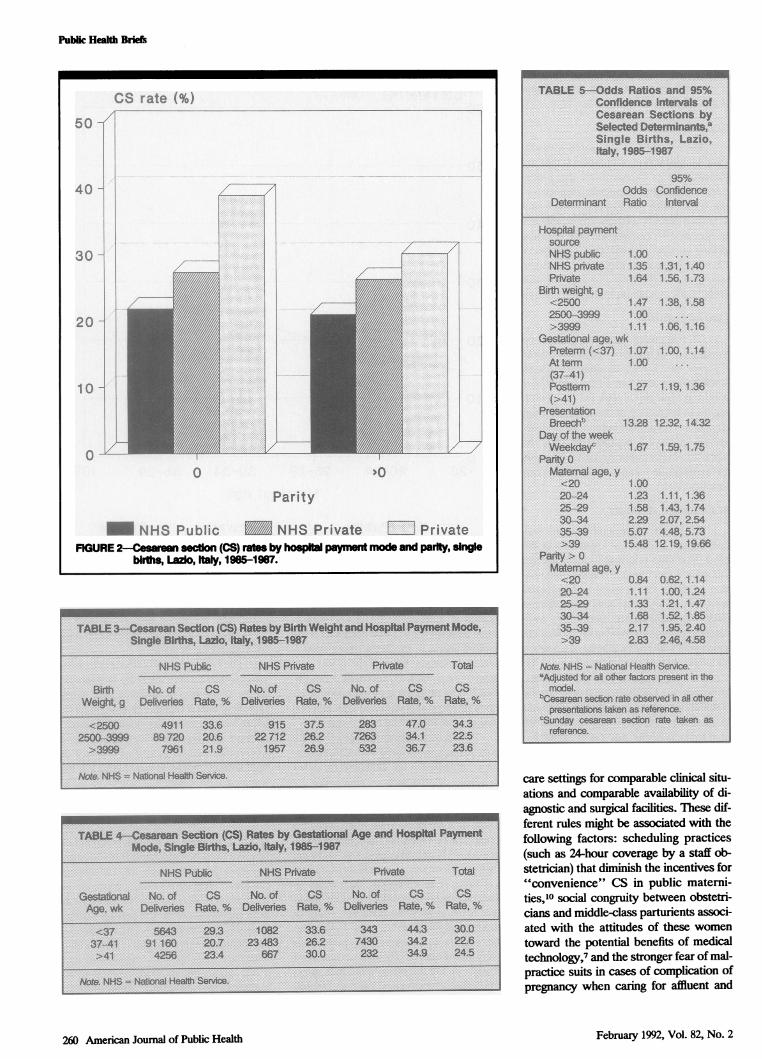
PantyThe rate of CS significantly de-
creasedwith parity (23.9% for parity 0 and22.4% for parity higher than 0). Withineach parity class, the highest CS rate wasobserved in private hospitals (Figure 2).Since delivering in private hospitals can bejudged as a proxy of the socioeconomicstatus of women,18 and considering thatmost affluent women tend to be of lowerparity and older maternal age,7 the ORs ofCS ratesby hospital typewere adjustedbymaternal age and parity distribution. Theadjusted OR,n of CS in private hospitalswas 1.58 (95% CI = 1.50, 1.66), as com-pared with 1.96 in the crude analysis;no important change was observed forNHS private hospitals (ORh = 1.32 vsO1crude = 1-34)-
Birth Weight and GestationalAgeThe rates of CS were highest among
women who delivered low-birth-weight(LBW) infants (34.3%), decreased with in-creasing birth weight (22.5%), and slightlyincreased for large babies (23.6%) (Table3).
For each birth-weight class, CS ratessignificantly increased in going from NHShospitals to the other two categories(P < .0001), although in private units alower proportion ofLBWand large babiesat higher risk of CS were reported.
CS rates among women who deliv-ered prematurely were highest (30.0%o),decreased for full-term pregnancies, andincreased again for postmature babies(24.5%) (Table 4). Again, rates were con-
258 American Journal of Public Health February 1992, Vol. 82, No. 2
Public Health Briefs
sistently and significantly higher(P < .0001) in private units at any gesta-tional age.
ComplicationsThe use ofCS is associated with var-
ious complications of pregnancy that areindications for carrying out the proce-dure.24 The only complication reported inthe Italian birth certificate is breech pre-sentation of fetus at labor. The overall fre-quency ofthis complication was 3.3% anddid not vary by hospital type. The rates ofCS were highest in private and NHS pri-vate hospitals (84.7%), as compared withNHS public hospitals (75.7%) (P < .001).
Day ofDelveryCS rates were consistently lower on
Sundays in all types of hospitals (overallCS rate of 15.7%), as compared withweekdays (overall rate of 24.1%). Therewas a statistically significant trend withregard to frequency of deliveries on Sun-days (P < .0001): The lowest rate was ob-served in private hospitals (8.8%), thehighest in NHS public units (12.2%), andan intermediate value in NHS private ma-ternities (10%).
Mulivanate AnalysisThe results of the simultaneous mul-
tiple logistic adjustment are shown in Ta-ble 5. The ORs refening to maternal ageand parity are shown for each combina-tion of these two variables. Comparedwith the univariate analysis of unadjustedORs, the multivariate assessment indi-cated that hospital paymentmodewas stillassociated with the likelihood ofCS whenallowance was made for the effects of theother variables present in the model.However, the OR associated with privatehospitalswas lower than the one observedin the crude analysis. This could be attrb-uted to the maternal age-parity effect dis-cussed previously, in part counterbal-anced by the combined effect of the othervariables in the model. The CS OR asso-ciated with NHS private maternities waspractically identical to the one observed inthe crude analysis.
The effect ofmaternal age on CS ratewas marked for older/parity 0 women ascompared with younger women andwomen of the same age at parity higherthan 0.
DiwsusionThis study showed that in the Lazio
region of Italy, approximately one of fourbabies was bom by CS in the time period
CS~~~~~~rat_(%
CS rate(%60
50
40
30
20
10
(20 20-24 25-29 30-34 35-39 >39Maternal Age
NHS Public i - NHS Private -* PrivateFIGURE 1-Cesarean section (CS) rtes by hospal Mt mode and matmal age,
single birth, Lazo, Italy, 1985-1987.
1985 through 1987, the highest rate re-ported in Europe so far. Lazio figureswere comparable to those observed in theUnited States in the same time period,25and were largely beyond the figure con-sidered acceptable by international agen-cies.26 The proportion of operative deliv-eries (forceps and vacuum) was minimaland did not follow any time trend.
Mode of payment for obstetric carewas strongly associated with CS rates af-ter controlling for the effects of the otheravailable determinants of abdominal de-livery. Because of the limited infornationincluded in the Italian birth certificate, theeffect of some known determinants ofCScould not be taken into account, namelyprevious CS delivery, dystocia, and fetaldistress. However, it is unlikely that thesevariables were differently distnbuted inthe three types of hospitals to such an ex-tent as to modify the observed effect ofmode ofpayment on CS rates. In fact, theheterogeneous CS ratesbypayment modewere also observed in prmiparous women(Figure 2). On the other hand, data refer-ring to breech deliveries, the only compli-
cation of pregnancy reported in the birthcertificate, confirmed higher CS rates inNHS private and private maternities thanin NHS public hospitals.
The heterogeneity ofCS ratesbyhos-pital payment mode might be attributableto the interaction of a variety of factors,including characteristics of patients, mixofphysicians, and organizational features.In the Lazio region, delivering in privatematernities can be judged as a proxy ofhigh socioeconomic status,18 which is as-sociated with higher CS rates.7 In addi-tion, a multiplicity of financial incentives,such as a higher physician fee for CS ascompared with vaginal delivery and con-gruence of physician interest with that ofhospital (long hospital stay after CS), mayinfluence directly or indirectly the clinicaldecision.27 It is interesting to note that, inItaly, most obstetricians work part-time inboth public hospitals and private institu-tions (NHS private or private), making thetwo health care settings fully comparablewith regard to physician training and age.This suggests that different decision-mak-ing rules were applied to different health-
American Joumal of Public Health 259
I
February 1992, Vol. 82, No. 2
Public Health Briefs
care settings for comparable clinical situ-ations and comparable availability of di-agnostic and surgical facilities. These dif-ferent rules might be associated with thefollowing factors: scheduling practices(such as 24-hour coverage by a staff ob-stetrician) that diminish the incentives for"convenience" CS in public materni-ties,10 social congruity between obstetri-cians and middle-class parturients associ-ated with the attitudes of these womentoward the potential benefits of medicaltechnology,7 and the stronger fear of mal-practice suits in cases of complication ofpregnancy when caring for affluent and
260 American Journal of Public HealthF
CS rate (%)
50
40
30-
20 -
, ~~~~~~~~~~~~~.
o
10~~~~~ 1
Parity
- NHS Public NHS Private El PrivateFIGURE2-Ceaan section (CS) rats by hospital nt mode and parity, single
blrfs, Lazo, taly, 1965-1987.
February 1992, Vol. 82, No. 2

PubLic Health Briefs
more educatedwomen, although malprac-tice suits in obstetrics are not common inItaly. All these elements may interact withphysician practice style, which is associ-ated with variability of CS use.8 The de-cision to undertake a CS section is, in fact,not guided by unequivocal criteria; on thecontrary, it is associated with a markedinterobserver and, more surprising, in-traobserver variability.28
In summary, our analysis ofbirth cer-tificate data showed that the CS rate in1985 through 1987 in the Lazio region wasone of the highest ever reported. No ten-dency toward a leveling off of the rate, asobserved in other countries,25 was de-tected. This finding, together with the as-sociation ofCS rate and hospital paymentmode, was of great concern and under-lines the urgent need for adopting regionaland national strategies to reduce the use ofabdominal delivery to more acceptablelevels. El
AcknowledgmentsWe thank Dr. Pamela Pantano for her help indata collection and collation. We are also grate-ful to Dr. Francesco Forastiere and Dr. MarinaDavoli for their useful comments on the firstdraft of the manuscript.
References1. Notzon FC, Placek PJ, Taffel SM. Com-
parisons of national cesarean-section rates.NEni JMed. 1987;316:386-389.
2. Taffel SM, Placek PJ, Moien M. 1988 U.S.cesarean-section rate at 24.7 per 100births-a plateau? N Engl J Med.1990;323:199-200. Letter.
3. Rutkow IM. Obstetric and gynecologic op-erations in the United States, 1979 to 1984.Obstet GynecoL 1986;67:755-759.
4. Rodrigues J. Urban hospital cesarean sec-tion delivery rates in Paraiba State, Brazil,1977-1981. Am J Public Health.1988;78:704-705.
5. Notzon FC. International differences in theuse of obstetric interventions. JAMA.1990;263:3286-3291.
6. Taffel SM, Placek PJ, Liss T. Trends in theUnited States cesarean section rate andreasons for the 1980-85 rise. AmJ PublicHealth. 1987;77:955-959.
7. Gould JB, Davey B, Stafford RS. Socio-economic differences in rates of cesareansection. N EngIJMed. 1989;321:233-239.
8. Goyert GL, Bottoms SF, Treadwell MC,Nehra PC. The physician factor in cesareanbirth rates. N Engi J MedL 1989;320:706-709.
9. De Mott RK, Sandmire HF. The GreenBay cesarean section study I. The physi-cian factor as a determinant on cesareanbirth rates. Am J Obstet Gynecol.1990;162:1593-1599.
10. Fraser W, Usher RH, McLean FH, et al.Temporal variation in rates ofcesarean sec-tion for dystocia: does 'convenience' play arole?AmJ Obstet GynecoL 1987;156:300-304.
11. Haynes de Regt R, Minkoff ILL, FeldmanJ, Schwarz RH. Relation ofprivate or cliniccare to the cesarean birth rate. N Engi JMed. 1986;315:619-624.
12. Stafford RS. Cesarean section use andsource of payment: an analysis of Califor-nia hospital discharge abstracts.AmJPub-lic Health. 1990;80:313-315.
13. Bertollini R, Di Lallo D, Rapiti E, PerucciCA. Cesarean section rates in Italy.Am JPublic Heakh. 1987;77:1554. Letter.
14. Bertollini R, Di Lallo D, Perucci CA, et al.Description and validation of the natalityand infant mortality information system inLazio. Neonatologica. 1988;2:26-34.
15. National Institutes of Health. CesareanChildbith: Report of the NICHD TaskForce on Cesarean Childbith Bethesda,Md: National Institutes of Health; 1981.DHHS publication no. (NIH) 82-2067.
16. Goldfarb MG. Who Receives Cesareans:
Patient and Hospital Characteristics.Rockville, Md: National Center for HealthService Research; 1984. DHHS publica-tion no. (PHS) 84-3345.
17. Williams RL, Chen PM. Controlling therise in cesarean section rates by the dis-semination of information from vital rec-ords. Am J Public Health. 1983;73:863-867.
18. Bertollini R, Di Lallo D, Di Lena P, Git-tarelli D, Papini P, Perucci CA. Rapportodel Sistema di Sorveglianza della natalitaemortalitA infantile nel Lazio. Anno 1985-86. Progetto Salute. 1990;14:1-178.
19. Miettinen 0. Estimability and estimation incase-referent studies. Am J Epidemiol.1976;103:226-235.
20. Schlesselman JJ. Case Control Studies.Design, Conduct, Analysis. New York,NY: Oxford University Press; 1982:203-206.
21. Mantel N, Haenszel W. Statistical aspectsof the analysis of data from retrospectivestudies of disease. J Natl Cancer Inst.1959;22:719-748.
22. Schlesselman JJ. Case Control Studies.Design, Conduct, Analysis. New York,NY: Oxford University Press; 1982:252-254.
23. Woolson RF. Statistical Methods for Bio-medical Research. New York, NY: JohnWiley and Sons; 1987.
24. Mann LI, GallantJ. Modem indications forcesarean section. Am J Obstet GynecoL1979;135:437-441.
25. Myers SA, Gleicher N. 1988 U.S. cesare-an-section rate: good news or bad? NewEngIJMeL 1990;3233:200. Letter.
26. World Health Organization. Appropriatetechnology for birth. Lancet. 1985;ii:436-437.
27. Stafford RS. The impact of nonclinical fac-tors on repeat cesarean section. JAMA.1991;265:59-63.
28. Barrett JFR, Jarvis GJ, MacDonald HD,Buchan PC, Tyrrell SN, Lilford RJ. Incon-sistencies in clinical decisions in obstetrics.Lancet. 1990;336:549-551.
February 1992, Vol. 82, No. 2 American Joumal of Public Health 261