center for post-acute care · center for post -acute care advisory board meeting april 14, 2015...
TRANSCRIPT
CENTER FOR POST-ACUTE CARE
ADVISORY BOARD MEETING
Tuesday, April 14, 2015 10:00 am – 2:30 pm
CALIFORNIA HOSPITAL ASSOCIATION BOARD ROOM
1215 K Street, Suite 800 Sacramento, CA 95814

CENTER FOR POST-ACUTE CARE Tuesday, April 14, 2015
10:00AM-2:30PM California Hospital Association- Board Room
1215 K Street, Suite 800 Sacramento, CA 95814
Call-in: (800) 882-3610; Passcode: 0523939#
Adobe Connect: http://connectpro16666225.adobeconnect.com/r98jppbkq1e/ ITEM SUBJECT REPORTING PAGE *Action Item
I. CALL TO ORDER/INTRODUCTIONS Hirose
− Post-Acute Care Advisory Board Roster
1
II. MINUTES OF PREVIOUS MEETING
A. Post-Acute Care Advisory Board Meeting − January 28, 2015 Meeting Minutes* Recommendation: Approve meeting minutes
Hirose
6
III. CHAIR REPORT
10
A.
B.
C.
Welcome and Meeting Review Advisory Board Membership Update*
Recommendation: Approve appointment of Ann Gors to advisory board. Recommendation: Appoint nominating committee for 2016 advisory board
CHA Board of Trustees
Hirose
Hirose
Hirose
IV. VICE PRESIDENT REPORT
11
A. CHA Case Management Committee Blaisdell/Rogers 12
B.
C.
− Case Management Memo Annual Meeting − Attendee evaluation summary Post-Acute PPS “Tool kit” materials − http://www.calhospital.org/post-acute-care-discussion
Blaisdell
Blaisdell
13

Center for Post-Acute Care Advisory Board Meeting April 14, 2015
D.
E.
Advisory Board Member Survey − January 2013 summary memo Congressional Advocacy Day
Blaisdell/All
All
18
V. STATE ISSUES
20
A.
B.
C.
State Legislation − Post-acute care bill summary Free Standing Emergency Departments − Discussion memo Coordinated Care Initiative − DPL 15-003
Glaser/Blaisdell
Blaisdell
Blaisdell
22
26
31
VI. FEDERAL AFFAIRS
45
A.
B.
Federal Legislation − SGR Section by section summary − CHA SGR support letter Federal Regulatory Update − Federal Regulatory Calendar − MedPAC
o Post-acute care trends
Blaisdell/Keefe
Blaisdell/Keefe
47 53
54
LUNCH
VII. REPORTS
A.
B.
C.
D.
Inpatient Rehabilitation & Therapy Services Forum − Report of forum activities − MA IRF memo Skilled Nursing & Subacute Care Forum − Report of forum activites − APL 15-004 Home Health & Hospice Forum − Report of forum activities Other
Walters
Hekimian
Glomp
89
91
93
95
101
Center for Post-Acute Care Advisory Board Meeting April 14, 2015 VIII. OTHER BUSINESS
103
A.
B.
Health Care Reform − KaufmanHall Report Member Updates
All
All
104
IX. NEW BUSINESS
All
X. NEXT MEETING
Hirose
In-Person Meeting:
Wednesday, July 22, 2015 10:00 am - 2:30 pm
Providence Saint Joseph Medical Center Strizka Conference Room #1
501 S. Buena Vista Street Burbank, CA 91505
XI. ADJOURNMENT
Hirose

Center for Post-Acute Care
2015 Advisory Board
Roster
Chair Chair-Elect Mivic Hirose, RN, MSN, CNS, Executive Administrator Laguna Honda Hospital and Rehabilitation Center 375 Laguna Honda Blvd. San Francisco, CA 94116 Phone: 415-759-2363 Fax: 415-759-2374 [email protected]
Term: 2011-2016
Pamela Chevreaux, MA, VP Ambulatory Services Long Beach Memorial Medical Center 2801 Atlantic Avenue Long Beach, CA 90806 Phone: 562-933-9010, 562-233-2556 (cell) Fax: 562-933-1904 [email protected]
Term: 2011-2017
Past -Chair David Brown, System Director of Rehabilitation Services Sharp HealthCare 2999 Health Center Drive San Diego, CA 92123 Phone: 858-939-3085 Fax: 858-939-3117 [email protected]
Term: 2011-2015
1

Members Maria Cecilia Alpasan, MA, OTR/L, Quality and Education Coordinator, Department of Rehabilitation Cedars-Sinai Medical Center 8700 Beverly Blvd. Los Angeles, CA 90048 Phone: 310-423-5243 [email protected]
Term: 2015-2017
Sheila Brown, RN, FACHE, Vice President, Continuum of Care Palomar Health 555 E. Valley Parkway Escondido, CA 92025 Phone: 760-739-3367 Fax: 760-739-3107 [email protected]
Term: 2014-2016 Judy Cook, RN, Administrative Director Seton Medical Center 1900 Sullivan Ave Daily City, CA 94015 Phone: 650-563-7123 Fax: 650-563-7129 [email protected]
Term: 2009-2015
Todd Cook, Chief Care Management Officer Providence Health & Services 501 South Buena Vista Street Burbank, CA 91505 Phone: 818-847-3307 Fax: 888-581-9031 [email protected]
Term: 2011-2017
Margaret Crane, Chief Executive Officer Barlow Respiratory Hospital 2000 Stadium Way Los Angeles, CA 90026 Phone: 213-202-6885 Fax: 213-202-6801 [email protected]
Term: 2011-2016
Adam Darvish, SVP Hospital Division Kindred Healthcare 200 Hospital Circle Westminster, CA 92683 Phone: 714-893-4541 x5147 Fax: 714-899-5057 [email protected]
Term: 2011-2017 Paul Giles, Director of Home Health Finance Dignity Health 20525 Via Lerida Yorba Linda, CA 92887 Phone: 415-987-6623 Fax: 415-591-2432 [email protected]
Term: 2014-2016
Linda Glomp, RN, BSN, MBA, Executive Director St. Joseph Health, Home Health, Hospice, Infusion Pharmacy, Private Duty 1100 West Stewart Drive Orange, CA 92863 Phone: 714-712-7236 Fax: 714-712-7157 [email protected]
Term: 2011-2017
2

Ann Gors, Chief Executive Officer Kentfield Rehabilitation & Specialty Hospital 1125 Sir Francis Drake Boulevard Kentfield, CA 94904 Phone: 415-485-3521 Fax: 415-485-3696 [email protected]
Term: 2015-2016
Lisa Harrold, LCSW, Director, Rehabilitation and Skilled Nursing Services Kaweah Delta Health Care District 840 S Akers Road Visalia, CA 93277 Phone: 559-624-3854 Fax: 559-741-4725 [email protected]
Term: 2015-2017
Walter Hekimian, MBA, Administrator Edgemoor DPSNF 655 Park Center Drive Santee, CA 92071 Phone: 619-596-5597 Fax: 619-596-5501 [email protected]
Term: 2014-2016
James Jackson, MPH, Hospital Administrator Alameda County Medical Center, Fairmont Campus 15400 Foothill Blvd. San Leandro, CA 94578 Phone: 510-895-7206 Fax: 510-895-4237 [email protected]
Term: 2014-2016 Jan Kroetz, RN, NM, NE-BC, Chief Patient Care Director Loma Linda University Medical Center- East Campus 25333 Barton Road Loma Linda, CA 92354 Phone: 909-558-6609 Fax: 909-558-6669 [email protected]
Term: 2013-2015
Josh Luke, Ph.D., FACHE, Interim Chief Executive Officer Memorial Hospital of Gardena 1145 W. Redondo Beach Blvd. Gardena, CA 90247 Phone: 310-538-6500 [email protected]
Term: 2015-2017
Shelly Necke, RN, BSN, Administrative Director, Transitional Care Unit Acute Rehabilitation Center, PIH Health 12401 Washington Blvd. Whittier, CA 90602 Phone: 562-698-0811 x12542 [email protected]
Term: 2015-2017
Jan Potts, RN, MBA, Chief Clinical Executive Sutter Care at Home 4830 Business Center Drive, Suite 140 Fairfield, CA 94534 Phone: 707-864-4556 Fax: 707-863-9043 [email protected]
Term: 2011-2017
3
Pamela Reger, Director, Continuing Care Services Kaiser Permanente 10990 San Diego Mission San Diego, CA 92108 Phone: 619-641-4026, (cell) Fax: 619-641-2025 [email protected]
Term: 2011-2017
Martha Samora, RN, CPHQ, FACHE, Chief Executive Officer HealthSouth Bakersfield Rehabilitation Hospital 5001 Commerce Drive Bakersfield, CA 93301 Phone: 661-864-4073 Fax: 661-633-5254 [email protected]
Term: 2015-2017 Tory Starr, MSN, PHN, CIC, Care Coordination Executive Sutter Health, Sacramento/Sierra Region 2700 Gateway Oaks Drive Sacramento, CA 95833 Phone: 916-887-7049 Fax: [email protected]
Term: 2015-2017
Robert Walters, PT, MBA, Director, Inpatient Rehabilitation Services John Muir Health 3480 Buskirk Ave., Suite 150 Pleasant Hill, CA 94523 Phone: 925-947-5252 Fax: 925-947-3390 [email protected]
Term: 2014-2016
Ex-Officio Patty Haggen, Executive Director, Neurosciences, Orthopedics & Rehabilitation John Muir Health 1601 Ygnacio Valley Road Walnut Creek, CA 94598 Phone: 925-941-4050 Fax: 925-947-3380 [email protected]
Regional Association Representatives Jaime Garcia, Regional VP Hospital Association of Southern California (HASC) 515 S Figueroa St, Suite 1300 Los Angeles, CA 90071-3300 Phone: 213-538-0700 Fax: 213-629-4272 [email protected]
Suzanne Ness, Regional VP Hospital Council of Northern & Central California 1215 K Street, Suite 730 Sacramento, CA 95814 Phone: 916-552-7534 Fax: 916-552-2618 [email protected]
4

Judith Yates, Senior VP Hospital Association of San Diego & Imperial Counties 5575 Ruffin Road, Suite 225 San Diego, CA 92123 Phone: 858-614-1557 Fax: 858-614-0201 [email protected]
Staff Patricia L. Blaisdell, FACHE, VP, Continuum of Care California Hospital Association 1215 K Street, Suite 800 Sacramento, CA 95814 Phone: 916-552-7553 Fax: 916-554-2253 [email protected]
Marisa Ward, Administrative Assistant California Hospital Association 1215 K Street, Suite 800 Sacramento, CA 95814 Phone: 916-552-7656 Fax: 916-554-2293 [email protected]
5

Center for Post-Acute Care Advisory Board Meeting Wednesday, January 28, 2015
1:00 pm – 5:00 pm Hilton Waterfront Beach Resort- Dolphin Room
21100 Pacific Coast Highway Huntington Beach, CA 92648
Present: Mivic Hirose, Pamela Chevreaux, David Brown, Maria Cecilia Alpasan,
Sheila Brown, Todd Cook, Margaret Crane, Adam Darvish, Linda Glomp, Lisa Harrold, Walter Hekimian, Jan Kroetz, Shelly Necke, Jan Potts, Rob Walters
By Phone: Paul Giles, Josh Luke
Staff: Duane Dauner, Dietmar Grellmann, Pat Blaisdell, Tracy Campbell, Marisa Ward
Staff by Phone: Alyssa Keefe, Barbara Glaser Regional Association Staff: Jaime Garcia, Suzanne Ness, Judith Yates Guests: Pamela Roberts, Melinda Staveley, Pam Dixon
I. CALL TO ORDER Chair Hirose called the meeting to order at 1:10 pm.
II. MINUTES OF PREVIOUS MEETING The minutes of the December 13, 2015 conference call were reviewed and approved.
III. CHAIR REPORT A. Meeting Welcome and Review
Chair-Elect Hirose provided an update on the most recent advisory board changes.
• Currently there are 22 board members and guidelines allow for 24 members. • Chair-elect Hirose moved to the position of Chair. • Pamela Chevreaux was appointed as Chair-elect. • Stan Berry resigned from advisory board. • Staff Blaisdell is speaking with Vibra to find a replacement to complete the term
for the position previously held by Ed Palacios.
6

IV. VICE PRESIDENT REPORT A. Board Orientation
Staff Blaisdell provided an overview of the 2015 board orientation materials.
B. Annual Meeting Past- Chair Brown and Staff Blaisdell provided an update on the 2015 annual meeting.
C. Post-Acute Care PPT “Tool Kit”
Staff Blaisdell provided an overview and the reviewed the comment process for the Post-Acute Care tool kit.
Staff Blaisdell will send out an email link to “tool kit” discussion.
V. REPORTS A. Inpatient Rehabilitation & Therapy Services Forum
Forum Chair Walters provided an update regarding issues impacting inpatient rehabilitation facilities and therapy services.
B. Skilled Nursing & Subacute Care Forum
Forum Chair Walter Hekimian provided an update on issues impacting hospital-based skilled nursing units and subacute care units.
C. Home Health & Hospice Forum Forum Chair Linda Glomp provided an update on issues impacting home health agencies and hospices.
• The Medicare and Medicaid Home Health Prospective Payment System Final Rule Summary was reviewed and discussed.
• The Medicare and Medicaid Conditions of Participation for Home Health Agencies was reviewed and discussed.
D. Long-Term Acute Care Hospitals
Staff Blaisdell provided an update on issues impacting long term acute care hospitals (LTCHs).
E. Other (TBD) New members were encouraged to join the Center for Post- Acute Care forums.
7

CHA Staff to forward information on forum dates and times.
VI. Public Advocacy
A. CHA Digital Advocacy Program
Staff Campbell provided an update on CHA’s digital advocacy plan and the Our Health California (OHC) community.
• Our Health California Flyer was distributed and members were encouraged to share stories and join OHC. Staff Blaisdell to forward information regarding OHC.
VII. Federal Update
A. Legislation
Staff Blaisdell provided an update on federal legislation of concern to CHA members and providers of post-acute care services. Staff Blaisdell delivered a presentation on the IMPACT ACT of 2014.
B. Regulatory Update
Staff Keefe provided an update regarding federal regulatory activity and a summary of program updates to the recovery audit contractor (RAC) program.
VIII. Quality Reporting
A. MAP Quality Measures Pamela Roberts provided an update on the Measures Application Partnership (MAP) recommendations for quality measures. Staff Keefe presented the CHA comment letter on Quality Reporting.
B. NQF Readmissions
Pamela Roberts provided an update on the NQF readmissions measures.
IX. State Update
A. State Legislative Outlook
8

Staff Glaser provided an overview of the upcoming state legislative session, including discussion of CHA’s legislative priorities and anticipated bill proposals.
B. State Budget
Staff Glaser provided an update on the state budget.
C. Cal MediConnect/CCI
Staff Blaisdell provided an update on the implementation of Cal MediConnect and the Coordinated Care Initiative, including updated enrollment information.
D. Summary of Labor and Employment Laws Staff Blaisdell provided a summary of the 2014 workplace laws that were passed/signed and effective January 1, 2015.
X. New Business
A. Member Updates
Chair Hirose invited members to share updates, announcements, and other items of interest.
XI. Next Meeting
In-Person Meeting: Tuesday April, 14, 2015
10:00 am – 2:30 pm California Hospital Association- Board Room
1215 K Street, Suite 800 Sacramento, CA 95814
XII. Adjournment
Chair Hirose adjourned the meeting at 4:55 pm.
9

April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Mivic Hirose, Chair Pamela Chevreaux, Chair-elect SUBJECT: CHA Center for Post-Acute Care Chair Report SUMMARY Mivic Hirose chairs the Advisory Board of the Center for Post-Acute Care. Hirose and Chair-elect Pamela Chevreaux represent the Center on the CHA Board of Trustees. ACTION REQUESTED To provide an update on CHA Board of Trustees activity
To provide an update on Center advisory board membership
To identify a nominating committee to review and make recommendations the 2016
advisory board. DISCUSSION The Center for Post-Acute Care represents the interests of CHA member post-acute care providers, including inpatient rehabilitation hospitals and units, long-term acute care hospitals, distinct-part skilled-nursing facilities, and home health agencies. As a part of CHA, the Center for Post-Acute Care serves as the primary public policy arm of the hospital association for post-acute care issues. The Advisory Board consists of no more than 24 members, representative of the types, location, and size of institutional members. The Chair and Chair-elect of the Advisory Board serve on the CHA Board of Trustees. Ann Gors, CEO, Kentfield Rehabilitation & Specialty Hospital, has been selected to complete the term of advisory board membership previously held by Ed Palacios.
10

April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Patricia Blaisdell, Vice President, Continuum of Care SUBJECT: CHA Center for Post-Acute Care Vice President Report SUMMARY The CHA Center for Post-Acute Care offers representation for CHA members who provide inpatient rehabilitation, long-term acute care, skilled nursing, and home health and hospice services. ACTION REQUESTED
To review feedback from the 2015 annual meeting and to provide an update on planning for the 2016 annual meeting.
To provide an update on the development and comment process for the Post-Acute Care tool kit, and determine next steps as appropriate.
To provide information and solicit input regarding the CHA Case Management Committee
To assess member interest in conducting a survey on advisory board operations and effectiveness.
To solicit feedback and input regarding future Washington DC advocacy event
DISCUSSION
The Vice President for the Post-Acute Care provides support to the Center for Post-Acute Care and members of the advisory board.
The Center holds an annual meeting each year, which educational sessions and policy updates of interest to post-acute care providers.
Advisory board members had previously suggested that Center staff develop presentation materials that may be accessed and used by members to support communications about post-acute care services, their role in the continuum of care and health care reform, and the work of the Center. A draft outline has been developed and is posted for discussion on the CHA website.
Attachments Attendee evaluation summary January 2013 advisory board member survey summary memo Case Management Memo
11

April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Patricia Blaisdell, Vice President, Continuum of Care SUBJECT: CHA Case Management Committee CHA will establish a state-wide case management committee. Membership of the new committee will include leadership, case managers, and other key staff from CHA member hospitals and health systems. Reflecting the scope and emerging role of case management in our member organizations, the new committee will be staffed by a team of two CHA issue managers, Pat Blaisdell, VP Continuum of Care, and Debby Rogers, VP Clinical Performance and Transformation. The goals of the proposed committee are to provide support for member hospitals and health systems on case management issues, and to solicit input for CHA advocacy on key areas, including care coordination, discharge planning, health care reform, and others. The establishment of a case management committee will allow CHA to effectively address current case management issues on behalf of our members, while at the same time preparing for the changes that affect the full continuum of care. During the next several weeks, Rogers and Blaisdell will solicit input from a range of members and association staff. The information gleaned during the interviews will be used to develop committee structure, membership and to identify priority issues for the committee’s work. We welcome your suggestions and input. Background The role of hospital case managers has grown increasingly prominent in recent years. Case managers are leaders in hospital and health system efforts to address critical operational and policy issues, such as readmission penalties, observation status, and discharge planning for complex patients. At the same time, emerging changes to reimbursement and the transition from a fee-for-service system to one based on episodes of care underscore the need for a greater focus on care coordination and case management throughout the continuum of care. Hospital case managers perform a number of specific and essential functions. Discharge planning includes the development and implementation of medically appropriate discharge plans, including admission to a post-acute care facility and identification and referral to community-based medical services. Case managers also conduct utilization review by seeking necessary care authorizations, monitoring levels of care, and appealing medical denials. As health care reform proceeds, case managers are increasingly engaged in care coordination, including readmission reduction and management of care transitions.
12

EVALUATION RESULTS
Question Number of Responses Responses (Out of 5)
Question Yes No
Were you provided with substantive written materials?
Did the program contain signifigant professional and/or practical content?
Speaker Overall Rating (Out of 5) Effectiveness of Teaching Methods
Significant Current Intellectual or
Practical ContentC. Duane Dauner 4.79 4.95Katy Fike 4.84 4.95Gretchen Alkema 4.55 4.79Pamela Roberts 4.62 4.83Chris Jones 4.46 4.76Jan Potts 4.58 4.75Brenda Schmitthenner 4.42 4.68Cedric Terrell 4.61 4.84Barbara Gage 4.08 4.84Kelsey Mellard 4.57 4.57 4.78Patricia Blaisdell 4.81 4.81 4.91Robert Klugman 4.95 4.95 4.95Sheree Kruckenberg 4.41 4.41 4.80Andy Edeburn 5.00 5.00 5.00
Overall program rating
4.794.844.554.624.46
2015 Center for Post-Acute Care — Huntington Beach*January 29-30
Attendees were asked to evaluate the conference and speakers on the following five point scale: 1-poor 2-fair 3-average 4-above average 5-excellent
Did this program meet your educational objectives?
Did the program update or keep you informed of your professional responsibilities?
Was the environment suitable for learning?Have you ever attended a CHA educational seminar?
5.002
4.584.424.61
39
0
42 0
1227
2
42
140
335
4.08
13

EVALUATION RESULTS
2015 Center for Post-Acute Care — Huntington Beach*January 29-30
Attendees were asked to evaluate the conference and speakers on the following five point scale: 1-poor 2-fair 3-average 4-above average 5-excellent
Question
Were you provided with substantive written materials?
Did the program contain signifigant professional and/or practical content?
Cutting edge information
Speaker Overall Rating (Out of 5) Effectiveness of Teaching Methods
Significant Current Intellectual or
Practical ContentC. Duane Dauner 4.79 4.95
Katy Fike 4.84 4.95
Along with asking participants to silence cell phones, its important to remind that talking during speaker presentations is inappropriate and the noise impacts others at the table
Perhaps best content yet
Very knowledgeable, good specifics and resources
Overall program ratingDid this program meet your educational objectives?
Have you ever attended a CHA educational seminar?
Excellent. I greatly appreciate the global "state of the union" and climate from national and local level
Awesome!Amazing
Excellent update on specific products/services
Actually several bits of new info!
Fantastic! Thank you for your work!
Online was good
Great welcome and kick off
Need to up his time to answer questions-great knowledge
Did the program update or keep you informed of your professional responsibilities?
Was the environment suitable for learning?Too cold
4.79
Always informative and thought provokingExciting opportunities
I'm fairly new to rehab and this is very helpful
Excellent array of high quality speakersTopics were all great!
Maybe charge $10.00 or so for printed presentationsFiles provided but I would be willing to pay an additional fee in the future for a prepared manual
1227
239
042
140
Had trouble with the downloadingHandouts difficult to print outEspecially appreciated the technology discussion
A bit cold on ThursdayA little cool at times but otherwise pleasantLove this hotel except too cold in meeting roomsNeed conference Wi-Fi access to follow presentations seamlessly
Need free Wi-Fi, especially if handouts are not provided (printed)Would prefer long tablesCold on Thursday but other than that- food excellent, room good
4.84
Yes No
335
042
52
Excellent
14

EVALUATION RESULTS
2015 Center for Post-Acute Care — Huntington Beach*January 29-30
Attendees were asked to evaluate the conference and speakers on the following five point scale: 1-poor 2-fair 3-average 4-above average 5-excellent
Speaker Overall Rating (Out of 5) Effectiveness of Teaching Methods
Significant Current Intellectual or
Practical ContentGretchen Alkema 4.55 4.79
Panel Presentation
Pamela Roberts 4.62 4.83Chris Jones 4.46 4.76Jan Potts 4.58 4.75Brenda Schmitthenner 4.42 4.68Cedric Terrell 4.61 4.84Barbara Gage 4.08 4.84Great content, very detailed
A lot of data to put together- thank youKelsey Mellard 4.57 4.78
Patricia Blaisdell 4.81 4.91
Good to see this summaryAlways good infoRobert Klugman 4.95 4.95
Loved the humor
Sheree Kruckenberg 4.41 4.80Very enlightening
Very informative!!
Andy Edeburn 5.00 5.00
Good speaker-would like to hear moreFabulous!
Very noisy during breakout sessions. Hard to hear some speakersInformative
Share care models that work
4.95
Data-driven discussion engaging speaking styleKnowledgeable, funny and great speakerExcellent speaker (2)A bit biased? Very funny
4.81
Comforting
4.57
4.08
5.00
4.41
Awesome presentationGreat note to end on- very encouraging info!
Hope to hear even more progress for mental health in the future
Intelligent synopsis regarding where we are and where to go
Excellent speaker and conference. I greatly appreciate the comprehensive, informative content and most especially humor with realistic insights to the future or post-acute care. Thank you
Would have liked more specifics on how bridge acute services and PAC. Talk very general would have liked to have each one present to entire group rather than breakout. Didn't have enough time for strategies to prevent re-admit for Pamela breakoutEffective way of "speed dating" on these important topics
Difficult to listen with multiple discussions in one roomLoved the idea of speed dating, but logistics difficult
She did a good job with a dry topic
Excellent content, delivery-very effective presentationsKelsey is an excellent speaker- very clearHope for the future
Great work- thank you
Especially outstanding through use of humor and his expertise
4.614.424.584.464.62
4.55
This was a bit rushed; hard to hear due to background noiseSeparate room would be good. Group discussion was too distracting and difficult to hear. Panel provided good information. Would have been nice to have the handout at the time of the talk
15
EVALUATION RESULTS
2015 Center for Post-Acute Care — Huntington Beach*January 29-30
Attendees were asked to evaluate the conference and speakers on the following five point scale: 1-poor 2-fair 3-average 4-above average 5-excellent
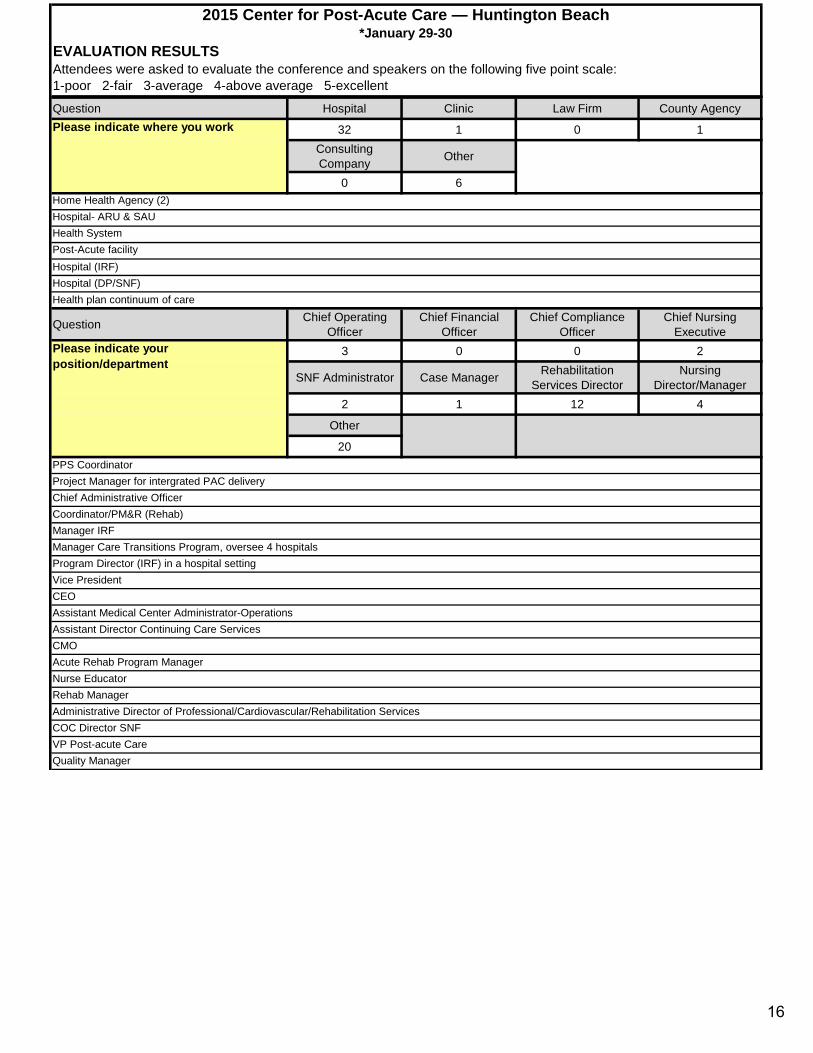
Question Hospital Clinic Law Firm County Agency
32 1 0 1Consulting Company Other
0 6
Question Chief Operating Officer
Chief Financial Officer
Chief Compliance Officer
Chief Nursing Executive
3 0 0 2
SNF Administrator Case Manager Rehabilitation Services Director
Nursing Director/Manager
2 1 12 4
Other
20
Please indicate where you work
Project Manager for intergrated PAC delivery
CMO
Hospital (IRF)
Please indicate your position/department
Hospital- ARU & SAUHome Health Agency (2)
PPS Coordinator
Chief Administrative OfficerCoordinator/PM&R (Rehab)Manager IRFManager Care Transitions Program, oversee 4 hospitalsProgram Director (IRF) in a hospital settingVice PresidentCEOAssistant Medical Center Administrator-OperationsAssistant Director Continuing Care Services
Acute Rehab Program ManagerNurse EducatorRehab ManagerAdministrative Director of Professional/Cardiovascular/Rehabilitation Services
Health plan continuum of careHospital (DP/SNF)
Post-Acute facilityHealth System
COC Director SNFVP Post-acute CareQuality Manager
16

EVALUATION RESULTS
2015 Center for Post-Acute Care — Huntington Beach*January 29-30
Attendees were asked to evaluate the conference and speakers on the following five point scale: 1-poor 2-fair 3-average 4-above average 5-excellent
Suggestions for next year's topics
All of them- reducing readmissions, conversation with President, managing care transitions in a value-based system, post-acute care modelManagement of high risk patients. Building intergrated modelBundled payment option. Readmissions reduction
Management of Medicare population. Reducing readmission. Bundled payment pilot. Transitioning value-based system. Building intergrated future focus
All
Duane Dauner, Katy Fike (2), Robert Klugman, Andy Edeburn
Policy issues *great that mental health was incorporated into the discussion
Content and networking in a great environment. Good breaks for informal networking and to remain attentive. Excellent CHA team. Great job! Thank you, Cheryl
Content !
More discussion regarding breaking down silo approach to health vs social issues
More on the role of community-based care transitions while supporting the continuum of care. Integration of advanced care planning with care transitions. Any successful Palliative Care programs? Thank you
Format and speaker were great. Would like sharing successful practices around chosen experiences
Home health programs. Palliative Care programs. Alzheimer's and Dementia Care programsPhysician communication and alignment strategies. Physician leadership development. Repeat Katy Fike's presentation with updateSite neutral payment updateI look forward to anything that they will present. They are always in tune with our learning needs. Thank you so much!Financial loss related to waste of medications. How brilliant young people will save healthcare. Community health literacy
How can those of us that run acute hospital services and acute rehabilitation services integrate care systems to benefit patient care? How can IRFs prepare for the coming financial impacts as payers begin to rapidly ratchet reimbursements?
Addressing patient choice and patient centered care to ensure patient family rights are protected and advocated. Financial should not drive solely- Managed Care/ACO, etc.
Do another "speed dating"- Also, continue to update on latest data regarding ACOs, building care management, etc.There was a lot of overlap of information in presentations although all presentations were good
Emerging ideas on how to deal with new regulations
Contacts made latest information on industry, good referrals for state-of-the-art programs/services and products
Assuring the strength and position and leadership of advocacy for PAC within the "service line" "care line" "systems of care" structure and model (e.g.. "Neuroscience/Orthopedics and Physical Rehab service line") that have emerged across the continuum.
Need some sort of Wi-Fi that works. Speed dating-neat idea, may want to use two rooms
Readmissions
Management of high risk Medicare and operations. Managing care transitions in a value based system. Reducing readmissions across the continuum
Great update! Wonderful venue. Exemplary professional presenters/experts!
Great deal of information, great variability in subject, great speakers
Safe patient handling
Concrete view of future healthcare and options. New technology applications (really exciting). Behavioral health issuesTechnology and Innovation. Conversation with Duane Dauner
Appreciate the additional time for networkingReducing readmissions across the continuumUpdates from CHA on post-acute care
What areas of the seminar were most beneficial?
17

January 30, 2013 TO: Center for Post-Acute Care Advisory Board FROM: Patricia Blaisdell, Vice President, Post-Acute Care Services SUBJECT: Center Transition
Background The Center for Post-Acute Care represents the interests of CHA member post-acute care providers, including inpatient rehabilitation hospitals and units, long-term acute care hospitals, distinct-part skilled-nursing facilities and home health agencies. As a part of CHA, the Center for Post-Acute Care serves as the primary public policy arm of the hospital association for post-acute care issues.
The establishment of the CHA Center for Post-Acute Care began in late 2010, and has been guided by an executive leadership group including chairs of the legacy CHA specialty centers, (Center for Medical Rehabilitation Services (CMRS) and Hospital Services for Continuing Care (HSCC)), as well as provider committee chairs and the chair of CHA Alliance for Post-Acute Care. During the last several months of 2012, this leadership group met and identified several key steps to support the continued transition to the Center for Post-Acute Care and the work of the advisory board.
Member Feedback A critical step in the transition planning process was the collection of information from current members regarding the board activities and how they could be improved. A survey was conducted in August of 2011. Board members were asked to rate the effectiveness of the board on a scale of 1 – 5, with 5 being “Very Effective”. Results were as follows:
Rating Response Percent 1 0% 2 0% 3 16.7% 4 61.1% 5 22.2%
Overall, members commented that the transition from the previous IRF and SNF specialty centers to the Center for Post-Acute Care was progressing well. Some respondents observed that they believe that the new Center would provide an effective structure for future work on behalf of CHA members. Several commenters noted that the board would benefit from additional time and effort to become more integrated and cohesive, and that new members may need additional support during their first few months on the board.
18

Action Steps Several actions were identified by the leadership group.
1. Board Meetings a. Establish time frames for reports and discussion items b. Encourage full participation c. Adhere to Working Agreements/Rules of Engagement d. Evaluate meeting effectiveness – “Plus/Delta” or post-meeting survey.
2. New Member Support a. Pair with incumbent board member (peer mentor) b. Provide additional orientation/support
3. Forums a. Transition current “committees” to “forums” b. Promote inclusive member access and participation c. Function:
i. Disseminate information to members ii. Provide mechanism for member discussion and input into CHA
activities. d. Forum chairs serve on the Advisory Board.
19
April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Patricia Blaisdell, Vice President, Continuum of Care Barbara Glaser, Senior Legislative Advocate SUBJECT: State Affairs Update SUMMARY Regulatory and legislative activities at the state level have significant implications for CHA member post-acute care providers. ACTION REQUESTED To provide an overview of the upcoming state legislative session, including discussion of
CHA’s legislative priorities and anticipated bill proposals. To provide an update on the state budget. To provide an update on the implementation of Cal MediConnect and the Coordinated
Care Initiative (CCI) DISCUSSION Current state legislative and regulatory issues will be reviewed and discussed, with an emphasis on implications for hospitals and for hospital and health system post-acute care providers, and the identification of recommended actions. State Legislation The legislature reconvened on January 5, 2015. During the month of April, bills will be heard in policy committees. CHA has identified legislative priorities for the current legislative session, and will monitor proposed legislation. Details on all of our high-priority health care-related bills CHA is tracking this legislative session may be accessed at the CHA website. Cal MediConnect/ Coordinated Care Initiative Implementation of Cal MediConnect and the Coordinated Care Initiative (CCI) is ongoing. CHA members have reported several issues with program implementation, including enrollment of ineligible/exempted beneficiaries, inconsistent communication with plans regarding coverage and authorization procedures, and physician participation and consequences for access and continuity of care.
20

Post-Acute Care Update April 14, 2015
Page 2
Association staff members at both state and regional levels are actively involved in communication with DHCS personnel, plan personnel, hospitals and other key stakeholders. Attachments Post-acute care bill summary Free Standing Emergency Departments memo DPL 15-003
21
KEY STATE ISSUES POST-ACUTE CARE LEGISLATION April 9, 2015 Details on all of our high-priority health care-related bills CHA is tracking this legislative session may be accessed at the CHA website at www.calhospital.org/key-state-issues. MEDI-CAL AB 366 Bonta (D-Alameda) Would repeal implementation of prior year Medi-Cal rate reductions, which include the 10 percent reduction to Medi-Cal providers and the retroactive amount owed to the state by hospital-based skilled-nursing facilities; increase payment rates for outpatient health care providers to that of Medicare payment levels; increase hospital Medi-Cal DRG rates on a one-time basis and require annual increases thereafter; and require the state to reimburse Medi-Cal managed care plans at the upper end of their rate range. To be heard in Assembly Health Committee 4/14 CHA Co-Sponsor Amber Ott/Barbara Glaser SB 243 Hernandez (D-Azusa) SB 243 is identical to AB 366. Would repeal implementation of prior year Medi-Cal rate reductions, which include the 10 percent reduction to Medi-Cal providers and the retroactive amount owed to the state by hospital-based skilled-nursing facilities; increase payment rates for outpatient health care providers to that of Medicare payment levels; increase hospital Medi-Cal DRG rates on a one-time basis and require annual increases thereafter; and require the state to reimburse Medi-Cal managed care plans at the upper end of their rate range. To be heard in Senate Health Committee 4/22 CHA Co-Sponsor Amber Ott/Barbara Glaser CARE COORDINATION AB 1518 Committee on Aging & Long Term Care Would expand the number of Medi-Cal waivers and require DHCS to expedite processing of waiver applications for individuals who are is acute care facilities pending placement in a skilled nursing facility. To be heard in Assembly Health Committee 4/21 Follow Pat Blaisdell/Barbara Glaser
22

SB 675 Liu (D-La Canada Flintridge) Would require hospitals and any health facilities that provide inpatient medical rehabilitation services to record the name of a family caregiver, if any, to notify that caregiver when the patient is discharged, and to provide explanation, live training, and telephonic technical assistance regarding the patient’s care needs to the family caregiver. To be heard in Senate Health Committee Oppose Unless Amended Pat Blaisdell/ David Perrott/Debby Rogers/Barbara Glaser/ Tanya Robinson-Taylor
SKILLED NURSING FACILITIES
AB 927 McCarty (D-Sacramento) Would expand disclosure requirements for applicants for a license to operate a skilled nursing facility. Would require denial of application licenses if a person named in the application was a director, officer, general partner of owner of even limited interested in a licensee or any parent organization of a licensee of a facility, during the seven-year period before the application, during which that facility had a violation that resulted in specific actions or outcomes. To be heard in Assembly Health Committee 4/14 Concerns Pat Blaisdell/Jackie Garman/Barbara Glaser
SB 779 Hall (D- Los Angeles) Would require the Department of Public Health to develop regulations for nurse staffing in skilled nursing facilities that include separate staff-to-patient ratios for certified nurse assistants in skilled nursing facilities. Specifies minimum ratios for CNAs for each eight hour shift, as well as posting requirements. To be heard in Senate Health Committee 4/22 Oppose Unless Amended Pat Blaisdell/ BJ Bartleson/Barbara Glaser/Connie Delgado
AB 348 Brown (D – San Bernardino) Would establish timelines for completion of complaint investigations by CDPH for skilled nursing facilities and associated requirements for reporting to complainants. Passed the Assembly Health Committee 4/7 To be heard in Assembly Aging and Long-Term Care Committee Support Pat Blaisdell/Debby Rogers/Barbara Glaser
23
AB 918 Stone (D – Scotts Valley) As introduced, would require skilled nursing facilities and behavioral health facilities to report to protection and advocacy each death or serious injury occurring during or related to the use of seclusion or behavioral restraints. Passed the Assembly Health Committee To be heard in Assembly Appropriations Committee Amended to eliminate hospitals and SNFs - Follow Sheree Kruckenberg/David Perrott/Pat Blaisdell/Barbara Glaser/Connie Delgado
HOME HEALTH
SB 390 Bates (R – Laguna Niguel) Would prohibit registered nurses or licensed vocational nurses from being required to have a minimum period of professional nursing experience, provided they have successfully completed a skills and competency training program administered by a licensed home health agency, which includes at least 80 hours of clinical orientation, didactic, simulation and hands-on training. To be Heard in Senate Health Committee 4/15 Follow BJ Bartleson/Pat Blaisdell/Sheree Kruckenberg/Connie Delgado/Barbara Glaser
END-OF-LIFE/PALLIATIVE CARE AB 637 Campos (D – San Jose) Would authorize the signature of a nurse practitioner or a physician assistant, acting under the supervision of a physician and within authorized scope of practice to sign the Physician Orders for Life Sustaining Treatment (POLST) form. Passed the Assembly Judiciary Committee 4/7 Follow, Hot Pat Blaisdell/Jackie Garman/ David Perrott/Barbara Glaser SB 19 Wolk ( D-Davis) Would establish a state-wide POLST registry. Would mandate submission of completed POLST forms in most instances. Heard in Senate Health, Judiciary 4/8 Support Pat Blaisdell/BJ Bartleson/David Perrott SB 128 Wolk (D-Davis)
24
Would enact the End of Life Option Act authorizing adults who meet certain qualifications, and who have been determined by their attending physician to be suffering from a terminal illness, to make a request for medication for the purpose of ending their own life. The bill provides that such a death would have no effect on a will, health care service plan or health insurance contract, and provides civil and criminal immunity. Passed the Senate Judiciary 4/7 Oppose Jackie Garman/Barbara Glaser MENTAL HEALTH AB 1300 Ridley Thomas (D-Los Angeles) Will modernize sections 5150, 5151 and 5152 of the Welfare and Institutions Code or Lanterman-Petris-Short Act. This bill makes clarifying changes to better define the various steps of a 5150 detention process to ensure consistent statewide application and to ensure that patients receive the most appropriate care in the least restrictive environment appropriate to their needs. To be heard in Assembly Health 4/14 CHA-Sponsored Sheree Kruckenberg/Judy Wolen NURSING SERVICES
SB 323 Hernandez (D-Azusa) Would allow Nurse Practitioners (NPs) to practice to the full extent of their education and training to ensure access to health care delivery systems for millions of Californian’s who now have access to coverage through the Affordable Care Act (ACA). To be heard in Senate Business and Professions Committee April 20. Support BJ Bartleson/Connie Delgado INSURANCE
SB 190 Beall (D- San Jose) Would require insurance policies issued after January 1, 2016, to include coverage for post-acute residential transitional rehabilitation services resulting from an acquired brain injury. To be heard in Senate Health Committee 4/22 Follow Dietmar Grellmann/Pat Blaisdell/Tanya Robinson-Taylor
25
March 17, 2015
TO: Center for Post-Acute Care Advisory Board
FROM: C. Duane Dauner, President/CEO
SUBJECT: Free-Standing Emergency Departments
A. SUMMARY
Several years ago, CHA sponsored a bill that would allow free-standing emergency
departments (FSEDs) in urban and rural areas, with parameters applied to the two
settings. The bill failed because of opposition from the Administration, California
Medical Association (CMA), California American College of Emergency Physicians
(CalACEP), consumer groups, labor unions, payers and others. No non-hospital entities
supported the bill.
Today, the circumstances have changed, including: enactment of the Affordable Care
Act (ACA); movement from Fee-For-Service (FFS) to other payment arrangements and
from volume to “value”; consolidation of providers into various types of arrangements
and systems; technological advancements in information technology, clinical services and
telemedicine/telehealth; expanding engagement and decision-making by consumers;
changing work forces and scope of practice rules; expanding regulatory overlays and
increasing consumer demands for convenient, customer-oriented health care.
Several situations exist in rural and urban areas where inpatient acute care services are
facing closure. For the affected communities, closing of inpatient beds means loss of all
hospital-related services. In most communities, complete loss of ambulatory services
means access to basic health care would be compromised.
Conversations with stakeholders and interest groups that opposed the legislation CHA
previously sponsored lead to a definitive conclusion: “A bill authorizing FSEDs, even
with limitations for rural and urban areas, will be opposed universally.” Consequently,
preserving access to care may be the only viable choice.
Options for amending CHA-sponsored spot bill, AB 579 (Obernolte), are:
26

Center for Post-Acute Care Advisory Board Page 2
March 17, 2015
1. Limit the bill to authorize FSEDs in a location where the inpatient hospital
facilities are closed, provided the FSED is included in the license of a general
acute care (GAC) hospital.
2. Authorize a FSED within defined proximity limits to the hospital under which the
FSED is licensed.
3. Authorize FSEDs, with or without parameters or conditions.
ACTION REQUESTED
Discussion and advice on the above three options for FSEDs. Your
recommendations will be presented to the CHA Board of Trustees in April.
B. BACKGROUND
Approximately 45 states legally allow FSEDs. In an estimated 16 states, there are about
400 FSEDs – the majority of which are hospital-affiliated, with a smaller number being
independent of hospital affiliation and/or physician owned. Some states require special
licensing for FSEDs or allow them to operate under the parent hospital’s license. Many
states’ regulations require accreditation, which many FSEDs receive, often from The
Joint Commission through their affiliated hospitals or as an ambulatory care facility.
C. CALIFORNIA REGULATORY CONSIDERATIONS
1. Use of Term “Emergency Services”
California law limits emergency services to licensed emergency departments (EDs),
which, as interpreted the California Department of Public Health (CDPH), requires the
emergency department (ED) to be located in a hospital building that includes inpatient
and other basic services required for licensing. There appears to be legal authority under
Health and Safety Code Section 1798.175 for a free-standing, non-hospital operated
emergency service, but this model is untested. Currently, there are three levels of
hospital-based EDs: comprehensive (9), basic (296) and standby (34). Except for the
adoption of nurse staffing ratios for EDs and changes in physical plant requirements by
OSPHD, the core requirements for all three levels of ED services have not materially
changed in more than 39 years. A comparison of the core requirements for basic and
standby EDs is shown in Appendix 1.
In response to the marketing of urgent care centers as “emergi-centers,” legislation was
enacted in 1986 to allow only two types of providers to use the term “emergency
services” or any derivative of “emergency” in marketing: hospitals with licensed EDs
and certified, 24-hour, non-hospital emergency service providers (non-hospital ES). The
statute is part of the Emergency Medical Services System Act (EMS Act) and falls within
the jurisdiction of the California Emergency Medical Services Agency. A summary of
27

Center for Post-Acute Care Advisory Board Page 3
March 17, 2015
the requirements for a non-hospital ES is located in Appendix 1; while the law has been
in effect for 28 years, we are unaware of any providers that have operated a non-hospital
ES.
California Health & Safety Code 1798.101 (b) permits a local EMS agency to designate a
receiving facility for “patients requiring emergency medical services” in an isolated rural
area without a hospital ED. Four clinics have been designated by local EMS agencies
under this law.
2. Distance for Off-Site Hospital Services
Both California law and federal Medicare regulations have adopted mileage limits for the
consolidation of a hospital facility and off-site service locations under a single license
and provider number.
a) California Licensing Laws: Under California law, a hospital may consolidate off-
site physical plants on its license if they are operated under common governance,
administration and medical staff with the main hospital, and if they are located
within 15 miles of the main hospital. The statute permits CDPH to approve an
extension of the 15-mile limit if one or more off-site physical plants are located in
a rural area, or the off-site physical plant provides only outpatient services.
b) Federal Provider-Based Rules: Under the Medicare provider-based rules, also
applicable to Medi-Cal, a hospital (including a critical access hospital) may bill
under its hospital provider number for services provided in off-site locations that,
among other standards, are:
i. on the hospital license;
ii. administratively, clinically and financially integrated with the main
hospital; and located within 35 miles of the main hospital, subject to a
few, limited exceptions.
3. Emergency Medical Treatment and Labor Act (EMTALA)
If an off-site ED is operated under a hospital license and submits claims under the
hospital’s Medicare program number, it will be required to comply with the Emergency
Medical Treatment and Labor Act (EMTALA) regulations. A non-hospital ES not
submitting claims under a hospital’s Medicare provider number would not be subject to
EMTALA regulations.
4. CDPH Position on Off-Site EDs
CDPH has approved consolidated licenses that include an off-site basic or standby ED
located in a seismic-compliant acute care building that also houses basic hospital
services. CDPH appears to have been more flexible as to the required level of acute or
28
Center for Post-Acute Care Advisory Board Page 4
March 17, 2015
support services for some standby EDs that are located in rural hospitals or in
consolidated off-site rural facilities of hospitals.
A 2012 Freestanding ED Feasibility Report by the Abaris Group included an email from
a CDPH representative indicating that a hospital cannot operate an off-site ED under a
consolidated license because an ED is not a separately licensed facility. However, the
author suggests that program flexibility may be available for new models of care “if they
are able to supply sufficient evidence that patient safety and quality of care will not be
compromised by the proposed alternative.” Reliance on the email is challenging, though,
since the nine listed requirements for ensuring patient safety and quality of care
incorporate the standards for a basic ED, rather than the less restrictive standards for a
standby ED. The email is unclear as to whether the standards must be met at the location
of the off-site ED or at the main hospital facility.
5. Legislative History
In the past decade, three bills (below) were introduced in the state Legislature to permit
free-standing EDs; none were passed. The Los Angeles County LEMSA developed a
pilot program allowing Centinela Hospital to accept ambulance traffic at its LA airport
location, which was abandoned after a bill in the Legislature faced significant opposition.
AB 835 (2003) – a spot bill that was not heard in committee.
AB 1050 (2005) – pilot program for free-standing EDs as receiving centers; the
bill was opposed by CNA, SEIU and Cal-ACEP, and was not heard in committee.
AB 1862 (2012) – pilot program for up to four free-standing EDs meeting basic
ED standards; the bill was unofficially opposed by CMA and Cal-ACEP, and not
heard in committee.
6. Reimbursement Considerations
CMS only recognizes an ED as a hospital-based service, which may be located off-site
from the main hospital, with two types:
Type A: dedicated EDs that are open 24 hours a day; and
Type B: dedicated EDs that do not meet the Type A definition (e.g., open less
than 24/7).
Type A dedicated EDs generally receive a higher reimbursement rate than Type B.
CMS may treat a non-hospital-based ED as a clinic, and pay the clinic rates that are
significantly lower than hospital-based rates. As there are no FSEDs in California, it is
unclear how Medi-Cal would treat free-standing EDs that are not part of a hospital for
29

Center for Post-Acute Care Advisory Board Page 5
March 17, 2015
reimbursement purposes. In other states, some commercial managed care plans contract
with FSEDs.
7. Other States
a) Texas
Texas has the highest number of FSEDs — 60 hospital-affiliated and more
than100 independent, non-consolidated FSEDs. They have the only statewide
association of freestanding emergency centers, the Texas Association of
Freestanding Emergency Centers (TAFEC). Before 2009, the independent FSECs
were not required to be licensed by the state. While Texas hospital-based FSECs
fall under their hospital license, independent FSECs had no licensing
requirements. In 2009, TAFEC sponsored Texas House Bill 1357 requiring all
independent FSECs to be licensed, develop hospital transfer agreements and
adhere to quality standards. They must accept all patients, including Medicare
and Medicaid, regardless of their ability to pay. They are subject to compliance to
the federal EMTALA.
Texas law does allow a FSED to be open 12 hours per day, provided they are
within 10 miles of an acute care hospital. However, these constitute only a small
number of licensed FSEDs. The bill also amended the insurance code statute to
add a freestanding emergency medical care facility under the emergency care
definition for billing, consistent with a hospital-based emergency department. The
Texas Department of Insurance requires payers to pay FSECs at the insured in-
network benefit level for all services. A copy of the BlueCross BlueShield of
Texas patient information sheet is enclosed (see Appendix 2).
The Texas College of Emergency Physicians (TCEP) reports high levels of
physician satisfaction with smaller patient loads. Some refer to it as, “the private
practice of emergency care.” Many physicians work in both FSECs and hospital-
based emergency departments. While most are joint accredited, the physicians
are working to show improved outcomes, particularly with stroke and STEMI
patients who get initial treatment at FSECs and immediate transfer to a higher
level of care. The Texas Hospital Association reports that the FSEDs have
reduced some overcrowding, and the legislation now provides for established
transfer protocols. However, there is concern that the independent FSEDs are
locating in areas of high commercial payer coverage. None are located in rural
areas, and the confusion that may occur by some not billing Medicaid/Medicare.
TCEP, TAFEC and the Texas Hospital Association have been working in
partnership and plan to hold the first FSEC conference this June in Dallas.
30

Center for Post-Acute Care Advisory Board Page 6
March 17, 2015
b) Washington
The Washington State Hospital Association (WSHA) indicated that there are five
hospital-affiliated FSEDs in Washington, and a sixth is being considered. There
is no stated regulation preventing a hospital from developing a free-standing
emergency department as part of their existing hospital license. There are no
independent FSEDs in Washington.
Swedish Medical Center developed the first FSED in 2005, which has now been
converted to a full service hospital. Currently, Swedish operates three FSEDs in
the Seattle area, with other systems operating the other two FSEDs.
All FSEDs in Washington comply with EMTALA, accept ambulances for ED
level I, offer basic emergency care, accept all Medicaid/Medicare patients and are
open 24/7. If needed, patients are transferred to the primary licensed hospital or,
in some situations, to a closer hospital as per agreements.
Other services provided at these FSED sites include primary care, specialty care,
surgery centers and observation beds.
c) Georgia
Recently, several rural hospitals in Georgia closed, and the Governor requested a
commission be formed to study the feasibility of FSEDs in the state. At this time
there are no FSEDs in Georgia.
The Rural Hospital Stabilization Committee prepared a financial modeling report
for Georgia in 2014 titled “Freestanding Emergency Department, Preliminary
Financial Models,” which showed poor reimbursement levels and questionable
financial sustainability of Georgia’s FSEDs. The findings concluded that, “While
freestanding EDs could help rural residents in states such as Georgia, they don’t
address the underlying socio-economic issues. The demographics will still be the
same, with many people lacking health insurance or having bare-bones coverage
and thus unable to pay the high bills associated with free standing EDs.”
A subsequent report from the committee issued on February 20, 2015,
recommends a Four Site “Hub & Spoke” Pilot Program that requires the Georgia
Department of Community Health, State Office of Rural Health to oversee a
proposed pilot program to build out an integrated “hub and spoke” model to
prevent the over-utilization of the ED as a primary care access point.
The goal of the “hub and spoke” model is to best use existing and new technology
to ensure that patients are being treated in the most appropriate setting, relieving
some of the cost pressures on the smallest rural hospitals’ EDs.
31
Center for Post-Acute Care Advisory Board Page 7
March 17, 2015
The report does not address FSEDs. However, the committee determined that in
order to maintain and protect the fragile rural hospital infrastructure, existing
Certificate of Need (CON) laws need to be maintained. Further, the committee
recommends the expansion of the scope of practice for mid-level providers, such
as nurse practitioners and physician assistants.
8. Important Considerations
a) Emergency Care Access
The ACA has embraced the goals set forth in the triple aim: improve care,
improve health and reduce costs. As a result, hospitals must realign their
financial infrastructure to focus less on inpatient volume and more on ambulatory
coordinated care and prevention. Many hospitals are vulnerable or at risk,
particularly those with high government-sponsored patients or low inpatient
volume. As accountable care organizations and other outpatient coordinated care
initiatives expand, some hospitals will be forced to close, jeopardizing their
communities’ access to emergency care. While the need for inpatient beds is
decreasing, demand remains high for emergent, urgent and ambulatory services.
In addition, many EDs are struggling to address the increasing number of ED
visits, despite a 12 percent increase in ED bed stations added by existing hospitals
over the past five years. ED visits have increased 13 percent, while inpatient
admissions and inpatient bed capacity have declined. EDs are not only providing
lifesaving care. They are now becoming a staging area for acutely ill patients, for
the use of complex diagnostic technology, and for providing coverage for offices
and clinics. The combined effects of growth in ED visits, more comprehensive
and complex evaluations and fewer inpatient beds have resulted in extended ED
lengths of stay, reducing efficient patient flow.
b) Emergency Department Physicians
While the California American College of Emergency Physicians (Cal ACEP)
continues to oppose the concept of FSEDs, the American College of Emergency
Physicians (ACEP) supports FSEDs and has a Freestanding Emergency Centers
Section that recently published, “Freestanding Emergency Departments -- an
Information Paper,” which defines and supports the use of FSEDs. The ACEP
board liaison to this group is a past president of Cal ACEP and an ED physician in
Northern California.
CHA has been meeting with CalACEP to discuss emergency services and where
there may be opportunities to collaborate.
32
Center for Post-Acute Care Advisory Board Page 8
March 17, 2015
c) Emergency Department Evolution
While most critics focus on the high costs of emergency care, EDs are playing a
vital role in preventing hospital admissions and reducing overall health care
costs. The average cost of an inpatient stay is ten times the cost of an average
ED visit. Washington data has found that the majority of FSEDs were
appropriately selecting these facilities for the services provided.
d) FSED Performance
FSEDs are increasing across the nation due to their ability to offer access for
patients seeking emergency care. They are often more convenient, readily
accessible, licensed, closely regulated, fully equipped for medical emergencies
and required to have an emergency physician at all times. Their wait times are
consistently lower than hospital-based EDs, and a majority of them are open 24/7.
In early studies on FSED quality performance, Texas and Washington have
indicated stroke and STEMI care equal to that of hospital- based EDs, as well as
high patient satisfaction.
CDD:rf
Attachments
33

Center for Post-Acute Care Advisory Board Page 9
March 17, 2015
Appendix 1
Comparison of Emergency Services
Basic ED
Standby ED Non-Hospital ES
Legal Basis Title 22, §70411 et
seq.
Title 22, §70649 et
seq.
H&S Code
§1798.175(b)
Location Hospital building Hospital building??? Free-standing
Hours of Operation 24/7 24/7 24/7
Physicians Must be on duty at all
times
Must be on duty or
available at all times
Must be on duty or
available at all times
Radiology Services Must be available Not addressed Available or on-call
Lab Services Must be available Not addressed Available or on-call
Surgery Services Must be immediately
available
Not addressed Not required
Post-Anesthesia
Recovery
Must be available Not addressed Not required
Intensive Care Service Must be available Not required Not required
Blood Service Must be available Not required Not required
Staffing Subject to nurse
staffing ratios
RN on duty at all
times; not subject to
nurse staffing ratios
for EDs
Personnel must be
experienced to treat
life/limb threatening
conditions
On-Call Must have a roster of
on-call specialties
Must have a roster of
on-call specialties
Must have a roster of
on-call specialties
Receive Ambulances Yes Rural areas ???
Advertising/Holding
Out
Can use “emergency
services”
Can use “emergency
services” only in rural
areas (but not
enforced???)
Can use “emergency
services”
34

Center for Post-Acute Care Advisory Board Page 10
March 17, 2015
Appendix 2
35

Center for Post-Acute Care Advisory Board Page 11
March 17, 2015
36
State of California—Health and Human Services Agency Department of Health Care Services
JENNEFIER KENT EDMUND G. BROWN JR. DIRECTOR GOVERNOR
DATE: March 27, 2015 DUALS PLAN LETTER 15-003
SUPERSEDES DUALS PLAN LETTER 14-004 TO: CAL MEDICONNECT MEDICARE-MEDICAID PLANS SUBJECT: CONTINUITY OF CARE PURPOSE: The purpose of this Duals Plan Letter (DPL) is to clarify and provide guidance about continuity of care provided by Medicare-Medicaid Plans (MMPs) that are participating in the Duals Demonstration Project, called Cal MediConnect. BACKGROUND: In January 2012, Governor Brown announced his intent to enhance health outcomes and beneficiary satisfaction for low-income Seniors and Persons with Disabilities (SPDs) by shifting service delivery away from institutional care to home and community-based settings. To implement this goal, the Legislature passed and Governor Brown signed Senate Bill (SB) 1008 (Chapter 33, Statutes of 2012), SB 1036 (Chapter 45, Statutes of 2012) and SB 94 (Chapter 37, Statutes of 2013), which authorized the implementation of the Coordinated Care Initiative (CCI). The three major components of CCI are:
1. A three-year Duals Demonstration Project (Cal MediConnect) for Duals (individuals eligible for Medicare and Medicaid) that combines the full continuum of acute, primary, institutional, and home and community-based services into a single benefit package, delivered through an organized service delivery system;
2. Mandatory Medi-Cal managed care enrollment for Duals; and
3. The inclusion of Long-Term Services and Supports (LTSS) as a Medi-Cal managed care benefit for SPD beneficiaries who are eligible for Medi-Cal only, and for SPD Duals.
The seven CCI counties participating in Cal MediConnect are Los Angeles, Orange, Riverside, San Bernardino, San Diego, San Mateo and Santa Clara. Cal MediConnect is a voluntary program; however, those Duals who opt-out of Cal MediConnect must still enroll in a Medi-Cal managed care health plan (MCP) for their Medi-Cal benefits (including Duals who are enrolled in a Medicare Advantage [MA] plan). Full-benefit Duals enrolled in an MCP for their Medi-Cal benefits and who opt-out of Cal
Managed Care Quality and Monitoring Division
1501 Capitol Avenue, P.O. Box 997413, MS 4400 Sacramento, CA 95899-7413
Phone (916) 449-5000 Fax (916) 449-5005 www.dhcs.ca.gov 37
DUALS PLAN LETTER 15-003 Page 2 MediConnect, or are not eligible for Cal MediConnect, will continue to receive their Medicare services either through Medicare fee-for-service or an MA plan. Continuity of care requirements for Cal MediConnect are defined in Welfare and Institutions (W&I) Code, Sections (§§) 14182.17 and 14132.275. These requirements are also set forth in the Memorandum of Understanding (MOU) between the Centers for Medicare and Medicaid Services (CMS) and the Department of Health Care Services (DHCS). The MOU establishes the following requirements:
• CMS and DHCS require each MMP to ensure that each beneficiary continues to have access to medically necessary items and services, as well as medical and LTSS providers;
• DHCS requires each participating MMP to follow continuity of care requirements established in current law;
• As part of the process to ensure that continuity of care and coordination of care requirements are met, an MMP must perform a Health Risk Assessment (HRA) within the timeframes specified in DPL 13-002.1 As part of the HRA, the MMP must ask the beneficiary if there are upcoming health care appointments or treatments scheduled and assist the Beneficiary to initiate the continuity of care process at that time if the beneficiary chooses to do so;
• Upon the beneficiary’s request, an MMP must allow the beneficiary to continue receiving services from out-of-network providers for primary and specialty care services and maintain his or her current providers and service authorizations at the time of enrollment for:
o A period up to six months for Medicare services if the criteria are met under W&I Code §14132.275(l)(2)(A); and
o A period of up to 12 months for Medi-Cal services if the criteria are met under W&I Code §14182.17(d)(5)(G).
• Medicare Part D transition rules and rights will continue as provided in current law and regulation for the entire integrated formulary associated with the MMP.
CAL MEDICONNECT PROVIDER CONTINUITY OF CARE REQUIREMENTS: The MMP must attempt to determine if the beneficiary has a pre-existing provider relationship through previous utilization data, the HRA process, and, as needed, contact with the provider. Upon request by the beneficiary, or other authorized person as noted below, an MMP must offer continuity of care with an out-of-network provider to all Cal MediConnect beneficiaries if all of the following circumstances exist:
1 DPL 13-002 is available at: http://www.dhcs.ca.gov/formsandpubs/Documents/MMCDAPLsandPolicyLetters/DPL2013/DPL13-002.pdf.
38
DUALS PLAN LETTER 15-003 Page 3
• The beneficiary has an existing relationship with a primary or specialty care provider. An existing relationship means the beneficiary has seen an out-of-network primary care provider (PCP) at least once or a specialty care provider at least twice during the 12 months prior to the date of his or her initial enrollment in the MMP for a non-emergency visit;
• The provider is willing to accept payment from the MMP based on the current Medicare or Medi-Cal fee schedule, as applicable; and
• The MMP does not have any documented quality of care concerns that would cause it to exclude the provider from its network.
If a beneficiary changes MMPs, the continuity of care period may start over one time. If the beneficiary changes MMPs a second time (or more), the continuity of care period does not start over, meaning that the beneficiary does not have the right to a new six or 12 month period. If the beneficiary opts out of Cal MediConnect and later reenrolls in Cal MediConnect, the continuity of care period does not start over. If a beneficiary changes MMPs, this continuity of care policy does not extend to the providers in the previous MMP’s network that now may be out-of-network providers in the new MMP. Consistent with the provisions of the MOU, MMPs are not required to provide continuity of care with an out-of-network provider if any of the following circumstances exist:
• An MMP is not required to provide continuity of care for services not covered by Medi-Cal or Medicare;
• The following providers are not eligible for continuity of care: providers of durable medical equipment (DME), transportation, other ancillary services, or carved-out services (however, continuity of services is required as noted in the “Background” section above in this DPL); and/or
• The provider does not agree to abide by the MMP’s utilization management policies.
Requirements for Delegated Entities
• When a beneficiary transitions into an MMP, and if the beneficiary has an existing relationship with a PCP that is in the MMP’s network, as determined through 1) the HRA process; 2) review of prior utilization data; 3) or the beneficiary’s request, the MMP must assign the beneficiary to the PCP, unless the beneficiary chooses a different PCP. If the MMP contracts with delegated entities, the MMP must assign the beneficiary to a delegated entity that has the beneficiary’s preferred PCP in its network;
• As a reminder, when a beneficiary transitions into an MMP, if the beneficiary has
an existing relationship with a PCP and/or specialist that is in the MMP’s network, and the beneficiary wishes to continue to see these providers, the MMP must allow the beneficiary to continue treatment with these providers for the continuity
39
DUALS PLAN LETTER 15-003 Page 4
of care period regardless of whether these providers are, or are not, in the network of the prime plan’s delegated entity to which the beneficiary is assigned, as long as the continuity of care requirements are met. For example, if a beneficiary has an existing relationship with a PCP and a specialist with the assigned Independent Physicians Association #1 (IPA #1) as well as a specialist in another IPA (IPA #2), where both IPAs are delegated entities of the same MMP, the MMP must assign the beneficiary to IPA #1 and allow the beneficiary to continue treatment with both specialists.
The continuity of care agreement for the specialist in IPA #2 would last for up to six months for Medicare services and up to 12 months for Medi-Cal services.
Procedures for Requesting Continuity of Care Beneficiaries, their Authorized Representatives on file with Medi-Cal, or their providers, may make a direct request to an MMP for continuity of care. Only those providers who treat beneficiaries, who are eligible for continuity of care, as noted above, may make a request to the MMP for continuity of care. MMPs must, at a minimum, accept requests for continuity of care over the telephone, according to the requestor’s preference, and cannot require that the requester complete and submit a paper or computer form. To complete a telephone request, the MMP may take any necessary information from the requester over the telephone. MMPs must accept and approve retroactive requests for continuity of care that meet all continuity of care requirements noted above, with the exception of the requirement to abide by the MMP’s utilization management policies. The services that are the subject of the request must have occurred after the beneficiary’s enrollment into the MMP, and the MMP must have the ability to demonstrate that there was an existing relationship between the beneficiary and provider prior to the beneficiary’s enrollment into the MMP. MMPs must only approve retroactive requests that meet the following requirements:
• Have dates of services that occur after September 29, 2014;
• Have dates of services within 30 calendar days of the first date of service for which the provider is requesting, or has previously requested, continuity of care retroactive reimbursement; and
• Are submitted within 30 calendar days of the first service for which retroactive continuity of care is being requested or denial from another entity when the claim was incorrectly submitted.
When a request for continuity of care is made, the MMP must begin to process the request within five working days after receipt of the request. However, as noted below, the request must be completed in three days if there is a risk of harm to the beneficiary. The continuity of care process begins when the MMP starts the process to determine if there is a pre-existing relationship and enters into an agreement with the provider.
40

DUALS PLAN LETTER 15-003 Page 5 The MMP should determine if a relationship exists through use of data provided to the MMP by CMS and DHCS, such as FFS utilization data from Medicare or Medi-Cal. A beneficiary or his or her provider may also provide information to the MMP that demonstrates a pre-existing relationship with a provider. A beneficiary may not attest to a pre-existing relationship (instead actual documentation must be provided) unless the MMP makes this option available to him or her. Following identification of a pre-existing relationship, the MMP must contact the provider and make a good faith effort to enter into a contract, letter of agreement, single-case agreement or other form of relationship to establish a continuity of care relationship for the beneficiary. Request Completion Timeline Each continuity of care request must be completed within:
• 30 calendar days from the date the MMP received the request;
• 15 calendar days if the beneficiary’s medical condition requires more immediate attention, such as upcoming appointments or other pressing care needs; or
• Three calendar days if there is risk of harm to the beneficiary.
A continuity of care request is considered completed when:
• The beneficiary is informed of his or her right of continued access or if the MMP and the out-of-network FFS or prior plan provider are unable to agree to a rate;
• The MMP has documented quality of care issues; or
• The MMP makes a good faith effort to contact the provider and the provider is non-responsive for 30 calendar days.
Requirements after the Request Process is Completed If an MMP and the out-of-network FFS or prior plan provider are unable to reach an agreement because they cannot agree to a rate or the MMP has documented quality of care issues with the provider, the MMP will offer the beneficiary an in-network alternative. If the beneficiary does not make a choice, the beneficiary will be assigned to an in-network provider. Beneficiaries maintain the right to pursue an appeal or grievance through the Medicare and Medi-Cal processes. If a provider meets all of the necessary requirements, including entering into a contract, letter of agreement, single-case agreement or other form of relationship with the MMP, the MMP must allow the beneficiary to have access to that provider for the length of the continuity of care period unless the provider is only willing to work with the MMP for a shorter timeframe. In this case, the MMP must allow the beneficiary to have access to that provider for the shorter period of time.
41
DUALS PLAN LETTER 15-003 Page 6 At any time, beneficiaries may change their providers regardless of whether or not a continuity of care relationship has been established. When the continuity of care agreement has been established, the MMP must work with the provider to establish a care plan for the beneficiary. Upon approval of a continuity of care request, the MMP must notify the beneficiary of the following within seven calendar days:
• The request approval or denial, and if denied, the beneficiary’s appeal and grievance rights;
• The duration of the continuity of care arrangement;
• The process that will occur to transition the beneficiary’s care at the end of the continuity of care period; and
• The beneficiary’s right to choose a different provider from the MMP’s provider network.
The MMP must also notify the beneficiary 30 calendar days before the end of the continuity of care period about the process that will occur to transition the beneficiary’s care at the end of the continuity of care period. This process must include engaging with the beneficiary and provider before the end of the continuity of care period to ensure continuity of services through the transition to a new provider. MMP Extended Continuity of Care Option MMPs may choose to work with a beneficiary's out-of-network provider past the six or 12 month continuity of care period, but MMPs are not required to do so. Beneficiary and Provider Outreach and Education MMPs must inform beneficiaries of their continuity of care protections and must include information about these protections in their beneficiary information packets and handbooks. This information must include how a beneficiary and provider initiate a continuity of care request with the MMP. These documents must be translated into threshold languages and must be made available in alternative formats, upon request. MMPs must provide training to call center and other staff who come into regular contact with beneficiaries about the continuity of care protections for beneficiaries. Provider Referral Outside of the MMP Network An approved out-of-network provider must work with the MMP and its contracted network and cannot refer the beneficiary to another out-of-network provider without authorization from the MMP. In such cases, the MMP will make the referral, if medically necessary, and if the MMP does not have an appropriate provider within its network.
42
DUALS PLAN LETTER 15-003 Page 7 DME, Transportation, and Other Ancillary Services For DME, transportation and other ancillary services, MMPs must provide continuity of care for services in accordance with W&I Code §§ 14132.275 and 14182.17(d)(5)(G), as noted in the “Background” section of this DPL, but are not obligated to use out-of-network providers that are determined to have a pre-existing relationship, for the applicable six or 12 months. Nursing Facilities A beneficiary who is a resident of a nursing facility (NF) prior to enrollment will not be required to change NFs during the duration of Cal MediConnect if the facility is licensed by the California Department of Public Health, meets acceptable quality standards and the facility and MMP agree to Medicare rates if the service is a Medicare service, or Medi-Cal rates if the service is a Medi-Cal service, in accordance with the three-way contract. This provision is automatic, meaning the beneficiary does not have to make a request to the MMP to invoke this provision. The MMP must determine the duration of residency through the same process specified previously for verifying a pre-existing provider relationship, which is through historical utilization data or documentation from the beneficiary or provider. DOCUMENTATION REVIEW: MMPs must submit the following documents to CMS and DHCS within 20 days of the issuance of this revised DPL in connection with MMP continuity of care:
• Policy and procedures delineating operations that have been revised based on this DPL; and
• Forms applicable to the process, including call scripts for completion of continuity of care requests by telephone that have been revised based on this DPL.
ADDITIONAL CONTINUITY OF CARE PROVISIONS UNDER CALIFORNIA LAW: In addition to the protections set forth above, Cal MediConnect beneficiaries also have rights to protections set forth in current state law pertaining to continuity of care. In accordance with W&I Code §14185(b), MMPs must allow beneficiaries continued use of any (single-source) drugs that are part of a prescribed therapy (by a contracting or non-contracting provider) in effect for the beneficiary immediately prior to the date of enrollment, whether or not the drug is covered by the MMP, until the prescribed therapy is no longer prescribed by the contracting physician. Additional requirements pertaining to continuity of care are set forth in Health and Safety (H&S) Code §1373.96 and require all health plans in California to, at the request of a beneficiary, provide for the completion of covered services by a terminated or non-participating health plan provider. Under this section, health plans are required to complete services for the following conditions: acute, serious chronic, pregnancy, terminal illness, the care of a newborn child between birth and age 36 months, and surgeries or other procedures that were previously authorized as a part of a documented course of treatment. Health plans must allow for the completion of these
43
DUALS PLAN LETTER 15-003 Page 8 services for certain timeframes which are specific to each condition and defined under H&S Code §1373.96. If you have any questions regarding this DPL, please contact Brian Hansen, Managed Care Quality and Monitoring Division at [email protected]. Sincerely, Original Signed by Sarah C. Brooks Sarah Brooks, Chief Managed Care Quality and Monitoring Division Department of Health Care Services
44
April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Patricia Blaisdell, Vice President, Continuum of Care Alyssa Keefe, Vice President, Federal Regulatory Affairs. SUBJECT: Federal Affairs Update SUMMARY Regulatory and legislative activities at federal level have significant implications for CHA member post-acute care providers. ACTION REQUESTED To provide an update regarding federal legislation of concern to CHA members and
providers of post-acute care services To provide an update regarding federal regulatory activity of concern to CHA members
and providers of post-acute care services DISCUSSION Current legislative and regulatory issues will be reviewed and discussed, with an emphasis on implications for hospitals and for hospital and health system post-acute care providers, and the identification of recommended actions. Federal legislation The House overwhelmingly passed H.R. 2, The Medicare Access and CHIP Reauthorization Act (MACRA), in a bipartisan vote of 392-37. Only two members of the California delegation, Republican Reps. Darrell Issa and Tom McClintock, voted against the legislation. Notably, the bill does not include implementation of site-neutral payments for IRFs for certain specified conditions, but does limit post-acute care payment updates and extends and modifies the therapy cap extension process.
Federal Regulation CHA maintains a full-time presence in Washington, D.C., to effectively advocate on legislative and regulatory policy, and collaborates on policies and strategies for health care issues with the American Hospital Association and other national health care organizations. On behalf of
45
Post-Acute Care Federal Update April 15, 2015
Page 2
members, CHA provides input on developing federal legislation and regulatory proposals, and helps shape national positions on important health care issues.
During coming weeks, CMS will issue proposed rules for prospective payment systems (PPS) for several providers, including IRF, SNF, and LTCH. CHA will complete summaries and analyses of the proposed rules for members, and will work with members to develop comments for submission to CMS.
CHA monitors the work of the Medicare Payment Advisory Commission (MedPAC). MedPAC has recommended the Congress enact legislation to eliminate difference in payment rates between IRFs and SNFs for certain conditions. MedPAC continues to discuss and evaluate other trends and potential reforms for post-acute care.
Attachments SGR Section by section summary CHA SGR Support Letter Federal Regulatory Calendar MedPAC- Post-acute care trends
46
Prepared by the Staff of the House Energy and Commerce and Ways and Means Committees
H.R. 2 MEDICARE AND CHIP REAUTHORIZATION ACT (MACRA) Section by Section
TITLE I—SGR REPEAL AND MEDICARE PROVIDER PAYMENT MODERNIZATION The legislation repeals the flawed Sustainable Growth Rate (SGR) formula and replaces it with the bicameral, bipartisan agreement to return stability to Medicare physician payments. The SGR formula is a cap on aggregate spending on physicians’ services where exceeding the cap resulted in punitive recoupments in subsequent years. The formula was passed into law in the Balanced Budget Act of 1997 to control physician spending, but it has failed to work. Since 2003, Congress has spent nearly $170 billion in short-term patches to avoid unsustainable cuts imposed by the flawed SGR. The most recent patch will expire on March 31st. Based on H.R. 1470, the bicameral, bipartisan unified Committee bill to replace the SGR, this policy removes the imminent threat of draconian cuts to Medicare providers and ensures a 5-year period of stable annual updates of 0.5 percent to transition to a new system. The new system moves Medicare away from a volume-based system towards one that rewards value, improving the quality of care for seniors. For more information, click here. TITLE II—MEDICARE AND OTHER HEALTH EXTENDERS Subtitle A—Medicare Extenders Sec. 201. Extension of work Geographic Practice Cost Index (GPCI) floor. Boosts payments for the work component of physician fees in areas where labor cost is lower than the national average. The provision extends the existing 1.0 floor on the “physician work” cost index until January 1, 2018. Sec. 202. Extension of therapy cap exceptions process. The Medicare program currently limits (“caps”) the amount of annual per-patient therapy expenditures. Congress created an exceptions process in 2006 that allows patients to exceed the cap based on medical necessity. This provision extends the therapy cap exceptions process until January 1, 2018 and reforms the process of medical manual review to help support the integrity of the Medicare program. Sec. 203. Extension of ambulance add-ons. Extends the add-on payment for ground ambulance services, including in super-rural areas until January 1, 2018. Sec. 204. Extension of increased inpatient hospital payment adjustment for certain low-volume hospitals. This provision extends Medicare Low-Volume hospital payments. The Centers for Medicare and Medicaid Services (CMS) has traditionally provided an additional payment to hospitals for the higher costs associated with operating a hospital with a low volume of discharges. This provision extends special add-on payments until October 1, 2017.
March 24, 2015
47

Prepared by the Staff of the House Energy and Commerce and Ways and Means Committees
Sec. 205. Extension of the Medicare-dependent hospital (MDH) program. MDHs are rural hospitals with no more than 100 beds that serve a high percentage of Medicare beneficiaries. MDHs are paid based on a blend of current prospective payment system rates and costs. This provision extends special payments to MDHs until October 1, 2017. Sec. 206. Extension for specialized Medicare Advantage (MA) plans for special needs individuals. MA special needs plans (SNPs) are plans that may limit enrollment to certain populations, such as beneficiaries dually eligible for both Medicare and Medicaid or those suffering from certain chronic conditions. This provision extends authority for SNPs through December 31, 2018. Sec. 207. Extension of funding for quality measure endorsement, input, and selection. Funds the National Quality Forum’s (NQF) review, endorsement and maintenance of quality and resource use measures, as well as the NQF and Secretary regarding the pre-rulemaking process and measure dissemination and review activities. The provision provides funding for each of fiscal years 2016 and 2017. Sec. 208. Extension of funding outreach and assistance for low-income programs. Provides additional funding for outreach and education activities for Medicare beneficiaries through September 30, 2017, including State Health Insurance Programs, Area Agencies on Aging, Aging and Disability Centers, and the National Center for Benefits Outreach and Enrollment. Sec. 209. Transition and Extension of Medicare reasonable cost contracts. This provision would allow for a smooth transition policy for cost plans that no longer meet statutory requirements to operate under Medicare in their service area. This policy outlines rules and beneficiary protections for cost plans to transition to Medicare Advantage plans. Sec. 210. Medicare Home Health Rural Add-On. This policy extends a three percent add-on to payments made for home health services provided to patients in rural areas through January 1, 2018. Subtitle B—Other Health Extenders Sec. 211. Permanent extension of the qualifying individual (QI) program. This program assists low-income Medicare beneficiaries with incomes between 120 percent and 135 percent of poverty (currently between $14,124 - $15,890 a year) in covering the cost of their Medicare Part B premium. This provision makes the QI program permanent. Sec. 212. Permanent extension of transitional medical assistance (TMA). TMA allows low-income families to maintain their Medicaid coverage for up to one year as they transition from welfare to work. This provision extends TMA permanently.
March 24, 2015
48

Prepared by the Staff of the House Energy and Commerce and Ways and Means Committees
Sec. 213. Extension of special diabetes program for type I diabetes and for Indians. Extends both the Type I Diabetes and Type II Indian Health Service programs through fiscal year 2017. Sec. 214. Extension of abstinence education. Extends abstinence only programs and associated funding through fiscal year 2017. Sec. 215. Extension of personal responsibility education program (PREP). Extends the PREP program and associated funding for one year through fiscal year 2017. PREP provides states, community groups, tribes, and tribal organizations with grants to implement evidence-based, or evidence-informed, innovative strategies for teen pregnancy and HIV/STD prevention, youth development, and adulthood preparation for young people. Sec. 216. Extension of funding for family-to-family health information centers. Extends the Family-to-Family Health Information Centers funding through fiscal year 2017. This program, administered by the Health Resources and Services Administration (HRSA), provides grants to support family-staffed organizations in each state to assist families of children with disabilities or special health care needs. Sec. 217. Extension of health workforce demonstration project for low-income individuals. Extends this program at the current funding level, which provides funding to help low-income individuals obtain education and training in high-demand, well-paid, health care jobs, through fiscal year 2017. Sec. 218. Extension of maternal, infant, and early childhood home visiting programs. Extends the Maternal, Infant, and Early Childhood Home Visiting Program funding through fiscal year 2017. This program provides states, territories, and tribes with grants to support evidence-based in-home visiting programs for at-risk families. Sec. 219. Tennessee disproportionate share hospital (DSH) allotment for fiscal years 2015 through 2025. The Medicaid statute requires that states make DSH payments to hospitals treating large numbers of low-income patients. States receive an annual DSH allotment, which is the maximum amount of federal matching funds a state is permitted to claim for Medicaid DSH payments. Hawaii and Tennessee have had different DSH arrangements provided through multiple previous laws due to unique past circumstances. This legislation provides parity by treating Tennessee like other states, thus providing an annual DSH allotment for fiscal years 2015 through 2025. Sec. 220. Delay in effective date for Medicaid amendments relating to beneficiary liability settlements. In December 2013, the Bipartisan Budget Act of 2013 overturned a circuit court case dealing with Medicaid estate recovery, allowing a state to recover medical expense claims from any portion of a Medicaid beneficiary settlement, potentially allowing a state to commandeer money set aside for a beneficiary’s future care or living expenses. The Protecting Access to Medicare Act of 2014 package delayed this provision until October 1, 2016. The legislation provides an additional delay, until October 1, 2017.
March 24, 2015
49

Prepared by the Staff of the House Energy and Commerce and Ways and Means Committees
Sec. 221. Extension of funding for Community Health Centers and National Health Service Corps Fund and Teaching Health Centers. The fund for the Community Health Center (CHC) Program will expire in September 2015. These dedicated mandatory funds supplement annual spending for the CHC program. In 2013, the most recent data available, 1,302 federally funded health centers located in all 50 states, the District of Columbia, and six U.S. territories, distributed evenly between urban and rural areas, served 22.7 million patients across 9,518 sites. Meanwhile, the vast majority of the 90 million visits to health centers were for primary medical care. This provision will provide two additional years of this funding through fiscal year 2017. The funding for the National Health Service Corps (NHSC) will end in 2015. The NHSC helps bring health care professionals to the areas where they are needed the most by providing scholarships and loan repayment in exchange for a commitment of service in an underserved community. This provision will fund the NHSC for an additional two years through fiscal year 2017. The Teaching Health Center Graduate Medical Education Payment Program expanded residency training in community-based settings. Residents are trained in family and internal medicine, pediatrics, obstetrics and gynecology, psychiatry, and general and pediatric dentistry through this program. This provision adds additional funding for the program through fiscal year 2017. TITLE III— The Children’s Health Insurance Program (CHIP) CHIP covers more than 8 million children and pregnant women in families that earn income above Medicaid eligibility levels. While the CHIP program is authorized through 2019, no new funding is available after fiscal year 2015. This provision preserves and extends CHIP, funding the program fiscal year 2017. TITLE IV—OFFSETS Subtitle A—Medicare Reforms Sec. 401. Medigap. Some Medigap plans on the market today provide first-dollar coverage for beneficiaries – which means the plan pays the deductibles and co-payments so that the beneficiary has no out-of-pocket costs. Beginning in 2020 – for new enrollees only – this provision would limit coverage to costs above the amount of the Part B deductible (currently $147 a month). Sec. 402. Income-related premium adjustment for Parts B and D. The portion of the Medicare Part B and Part D premium that a beneficiary pays is based on the beneficiary’s income. This policy would increase the percentage that Medicare beneficiaries with modified adjusted gross income (MAGI) between $133,501 and $160,000 ($267,001-$320,000 for a couple) from 50 percent to 65 percent. Beneficiaries that have incomes at $160,001 and above ($320,001 and above for a couple) would pay 80 percent. Additionally, current law freezes the
March 24, 2015
50
Prepared by the Staff of the House Energy and Commerce and Ways and Means Committees
income thresholds through 2019, at which point the income thresholds would be indexed to inflation as if they had not been frozen. Starting in 2018, this policy would update the threshold for inflation based on where they were in 2019. This provision would also apply to Part D premiums, meaning that beneficiaries who have income above the set thresholds are assessed an income-related monthly adjustment amount in addition the base Part D monthly premium. Subtitle B—Other Offsets Sec. 411. Market basket reductions. Medicare reimbursements for post-acute care providers will increase by no more than 1.0 percent in fiscal year 2018. Sec. 412. Medicaid DSH. Medicaid DSH payments provide additional payments to hospitals that serve a disproportionate number of low-income patients. Currently, reductions in state DSH allotments are scheduled to begin in fiscal year 2017. This policy would delay Medicaid DSH cuts until fiscal year 2018 and add another year of DSH cuts in 2025. Sec. 413. Levy on Medicare providers for nonpayment of taxes. Under current law, the Department of the Treasury may impose a levy of up to 30 percent against Medicare service providers with tax delinquencies. This provision will permit the Treasury to impose a levy of up to 100 percent on tax delinquent Medicare service providers. Sec. 414. Adjustments to inpatient hospital payment rates. The American Taxpayer Relief Act (ATRA) of 2012 required CMS to retrospectively recoup $11 billion in Medicare overpayments to hospitals. Hospitals are scheduled to receive a one-time 3.2 percentage points payment increase in Fiscal Year (FY) 2018. This section provides for the anticipated hospital payment increase of 3.2 percentage points to be phased in at 0.5 percentage points per year over 6 years beginning in fiscal year 2018. TITLE V—MISCELLANEOUS Subtitle A— Protecting the Integrity of Medicare Act of 2015 (PIMA). This legislation includes bipartisan provisions that strengthen Medicare’s ability to fight fraud and build on existing program integrity policies. Significant provisions include prohibiting Social Security numbers on Medicare cards, reducing wrongful or improper Medicare payments, removing duplicative Medicare Secondary Payer reporting requirements, and eliminating civil money penalties for inducements to physicians to limit services that are not medically necessary. This legislation passed out of the Committee on Ways and Means with bi-partisan support. Subtitle B—Other provisions Sec. 521. Delay of two-midnights. Per CMS regulation, the two-midnight policy requires a patient stay of two-midnights in a hospital to qualify for inpatient status in most instances; stays less than that will be paid as an outpatient visit. This provision allows CMS to continue use of
March 24, 2015
51
Prepared by the Staff of the House Energy and Commerce and Ways and Means Committees
the Medicare Administrative Contractor (MAC) “probe and educate” program to assess provider understanding and compliance with the “two-midnight rule,” on a pre-payment basis, through September 30, 2015. Sec. 522. Requiring bid surety bonds and State licensure for entities submitting bids under the Medicare durable medical equipment, prosthetics, orthotics, and supplies (DMEPOS) competitive acquisition program. This bill makes modifications to the DMEPOS competitive acquisition program. It prohibits the Secretary of Health and Human Services (HHS) from accepting a bid from a DMEPOS entity for a bidding area unless the entity: (1) meets state licensure requirements applicable within a product category; and (2) has obtained a bid surety bond of between $50,000 and $100,000 for each such geographic area. Suppliers whose bids are at or below the median price but do not accept a contract forfeit their surety bond. This bill passed out of the Ways & Means Committee via voice vote and passed the House floor via voice vote on March 16. Sec. 523. Payment for global surgical packages. This provision reverses the CMS decision to eliminate the bundled payment for surgical services that span a 10 and 90-day period. It requires CMS to periodically collect information on the services that surgeons furnish during these global periods beginning not later than 2017 and use that information to ensure that the bundled payment amounts for surgical services are accurate. The Secretary has the authority to delay a portion of payment for services with a 10 and 90-day global period to incentivize reporting of information. The Secretary can cease the collection of information from surgeons once the needed information can be obtained through other mechanisms, such as clinical data requires and electronic medical records. Sec. 524. Secure Rural Schools. Provides a two-year extension of Secure Rural Schools and Community Self-Determination Act of 2000. This program allows for payments to mitigate impacts on counties containing national forested public lands with declining timber revenues. It enables flexibility for county elections to spend payments over two years or the normal timeframe at a five percent reduction from fiscal year 2013 funding levels per current law. Sec. 525. Exclusion from PAYGO scorecards.
March 24, 2015
52
March 24, 2015 Dear Member of the California Delegation:
On behalf of the nearly 400 hospital and health system members of the California Hospital Association,
we wish to express our support for H.R. 2, The Medicare Access and CHIP Reauthorization Act
(MACRA).
Congress, health care providers and their patients have struggled with the flawed sustainable growth
rate (SGR) methodology and the many short term attempts to fix it. We support this permanent
resolution.
The bipartisan legislation is important to hospitals not only for what it does – repealing the SGR and
extending the Children’s Health Insurance Program – but also for what it does not do. We are pleased
that the bill does not embrace several flawed, unsound policies that would be harmful to California’s
hospitals and the patients they care for. Specifically, the bill rejects changes to the area wage index
and the rural floor which would have cost California hospitals as much as $200 million this year
alone. The measure also rejects cuts to graduate medical education, Medicare bad debt payments,
rural hospitals, hospital outpatient departments (known as site-neutral cuts) and cuts for certain
rehabilitation services. The bill does not allow an additional delay in the implementation of ICD-10.
The bill is helpful to California’s Medicaid disproportionate share hospitals and blocks a coding off-
set for all hospitals proposed by the Centers for Medicare & Medicaid Services. It also helps
hospitals by extending for six months the enforcement of the so called two-midnight rule and several
other important programs.
Once again, hospitals have been asked to contribute to the financing of the overall package; however,
we understand the urgent need to advance a permanent fix for SGR and an extension of CHIP, and
we appreciate the careful balance of payment changes and structural improvements to the Medicare
program overall.
Thank you for your continued support of California hospitals and the patients we serve. We look
forward to working with you on other initiatives important to Californians and California hospitals
and we urge all members of the California delegation to support H.R. 2.
Thank you for your consideration .
Sincerely, C. Duane Dauner President/CEO
53
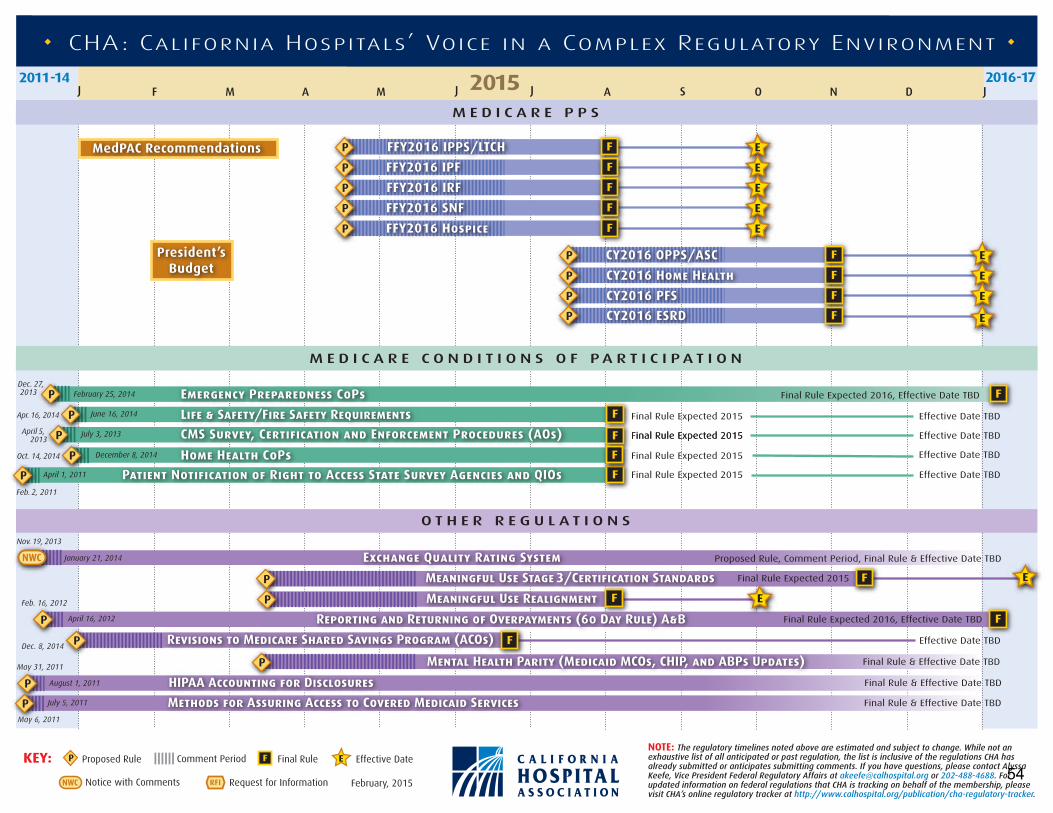
NOTE: The regulatory timelines noted above are estimated and subject to change. While not an exhaustive list of all anticipated or past regulation, the list is inclusive of the regulations CHA has already submitted or anticipates submitting comments. If you have questions, please contact Alyssa Keefe, Vice President Federal Regulatory Affairs at [email protected] or 202-488-4688. For updated information on federal regulations that CHA is tracking on behalf of the membership, please visit CHA’s online regulatory tracker at http://www.calhospital.org/publication/cha-regulatory-tracker.
KEY: Comment PeriodProposed Rule Final Rule
Request for Information February, 2015
Effective Date
Notice with CommentsNWC
J F AM M J J A S O N D J2016-172011-14 2015
M E D I C A R E P P S
M E D I C A R E C O N D I T I O N S O F P A R T I C I P A T I O N
O T H E R R E G U L A T I O N S
CHA: California Hospitals’ Voice in a Complex Regulatory Environment
FFY2016 IPPS/LTCHMedPAC Recommendations
President’sBudget
FFY2016 IPF
FFY2016 IRF
FFY2016 SNF
FFY2016 Hospice
CY2016 OPPS/ASC
Apr. 16, 2014
Oct. 14, 2014
April 5, 2013
Dec. 27, 2013
Feb. 2, 2011
Emergency Preparedness CoPs
Life & Safety/Fire Safety Requirements
CMS Survey, Certification and Enforcement Procedures (AOs)
Home Health CoPs
CY2016 Home Health
CY2016 PFS
Effective Date TBDFinal Rule Expected 2015
Effective Date TBD
Final Rule Expected 2016, Effective Date TBD
Exchange Quality Rating SystemNov. 19, 2013
January 21, 2014
February 25, 2014
June 16, 2014
July 3, 2013
December 8, 2014
Feb. 16, 2012
Meaningful Use Stage 3/Certification Standards
Meaningful Use Realignment
Reporting and Returning of Overpayments (60 Day Rule) A&B
Revisions to Medicare Shared Savings Program (ACOs) Effective Date TBD
Mental Health Parity (Medicaid MCOs, CHIP, and ABPs Updates) Final Rule & Effective Date TBD
HIPAA Accounting for Disclosures Final Rule & Effective Date TBD
Methods for Assuring Access to Covered Medicaid Services Final Rule & Effective Date TBD
CY2016 ESRD
Patient Notification of Right to Access State Survey Agencies and QIOs
NWC
Effective Date TBD
Proposed Rule, Comment Period, Final Rule & Effective Date TBD
Final Rule Expected 2015Final Rule Expected 2015
Final Rule Expected 2015
Final Rule Expected 2015 Effective Date TBDApril 1, 2011
Final Rule Expected 2015
Final Rule Expected 2016, Effective Date TBDApril 16, 2012
August 1, 2011
July 5, 2011
Dec. 8, 2014
May 31, 2011
May 6, 2011
54
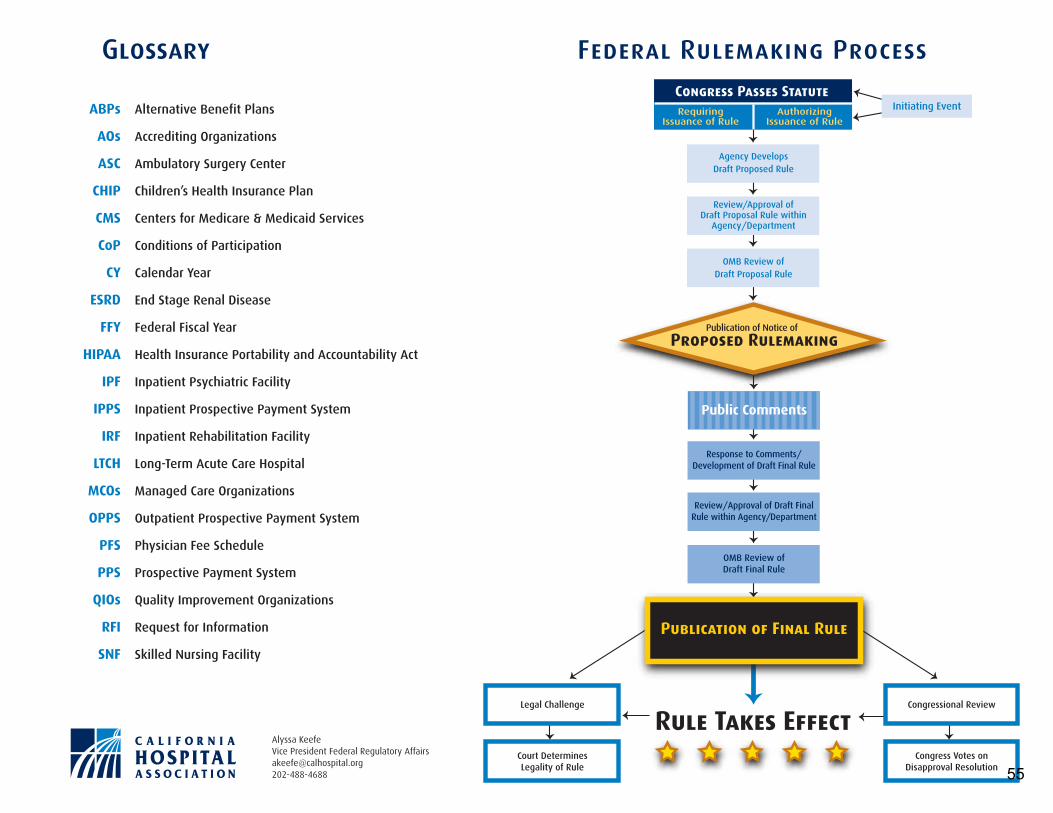
Rule Takes Effect
Glossary
ABPs Alternative Benefit Plans
AOs Accrediting Organizations
ASC Ambulatory Surgery Center
CHIP Children’s Health Insurance Plan
CMS Centers for Medicare & Medicaid Services
CoP Conditions of Participation
CY Calendar Year
ESRD End Stage Renal Disease
FFY Federal Fiscal Year
HIPAA Health Insurance Portability and Accountability Act
IPF Inpatient Psychiatric Facility
IPPS Inpatient Prospective Payment System
IRF Inpatient Rehabilitation Facility
LTCH Long-Term Acute Care Hospital
MCOs Managed Care Organizations
OPPS Outpatient Prospective Payment System
PFS Physician Fee Schedule
PPS Prospective Payment System
QIOs Quality Improvement Organizations
RFI Request for Information
SNF Skilled Nursing Facility
Congress Passes StatuteRequiring
Issuance of RuleAuthorizing
Issuance of Rule
Agency DevelopsDraft Proposed Rule
OMB Review ofDraft Proposal Rule
Legal Challenge
Court DeterminesLegality of Rule
Congressional Review
Congress Votes onDisapproval Resolution
Response to Comments/Development of Draft Final Rule
Review/Approval of Draft FinalRule within Agency/Department
OMB Review ofDraft Final Rule
Publication of Final Rule
Public Comments
Publication of Notice of
Proposed Rulemaking
Review/Approval ofDraft Proposal Rule within
Agency/Department
Initiating Event
Federal Rulemaking Process
Alyssa Keefe Vice President Federal Regulatory Affairs [email protected] 202-488-4688 55

Medicare’s post-acute care: trends and ways to
rationalize payments
C H A p t e R7
56

R e C o M M e n D A t I o n
7 The Congress should direct the Secretary of Health and Human Services to eliminate the differences in payment rates between inpatient rehabilitation facilities (IRFs) and skilled nursing facilities for selected conditions. The reductions to IRF payments should be phased in over three years. IRFs should receive relief from regulations specifying the intensity and mix of services for site-neutral conditions.
COMMISSIONER VOTES: YES 17 • NO 0 • NOT VOTING 0 • ABSENT 0
57

159 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
Medicare’s post-acute care: trends and ways to rationalize payments
Chapter summary
Post-acute care (PAC) providers offer important recuperation and
rehabilitation services to Medicare beneficiaries recovering from an acute
hospital stay. PAC providers include skilled nursing facilities (SNFs), home
health agencies (HHAs), inpatient rehabilitation facilities (IRFs), and long-
term care hospitals (LTCHs). Medicare’s payments to the more than 29,000
PAC providers totaled $59 billion in 2013, more than doubling since 2001.
The Commission has frequently observed that Medicare’s payments for PAC
are too generous and that its payment systems have shortcomings. The high
level of payments results both from base rates that are generous relative to
the actual cost of services and from weaknesses in the payment systems that
encourage providers to increase payments by strategically conducting patient
assessments, increasing the amount of therapy they provide, and selecting
certain types of patients over others. There is also significant variation
in financial performance within categories of providers (e.g., ownership,
freestanding vs. hospital based). Biases in the HHA and SNF prospective
payment systems make certain patients, and the services provided to them,
more profitable than others. Meanwhile, quality of care, as measured by the
Commission, has not considerably improved, raising questions about the value
of the program’s purchases. In addition, providers’ costs per unit of service
vary enormously. Medicare has a responsibility to better its payment systems
to ensure access for beneficiaries, appropriately reimburse providers for the
In this chapter
• Trends in post-acute care
• Site-neutral payments for select conditions treated in inpatient rehabilitation facilities and skilled nursing facilities
• Private sector ideas for managing post-acute care
• Conclusion
C H A p t e R 7
58

160 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
patients they treat, and control costs for the beneficiary and taxpayer alike. It is up
to providers to address their cost per unit of care.
But the Commission’s concerns about PAC go beyond the shortcomings of the
setting-specific payment systems. The need for PAC is not well defined. Similar
patients are treated in different settings at widely varying cost to the Medicare
program. Placement decisions often reflect local practice patterns, the availability
of PAC in a market, patient and family preferences, and financial arrangements
between a PAC provider and the referring hospital. Reflecting this ambiguity,
Medicare per capita spending on PAC varies more than any other covered service,
which is only partly explained by the large differences in the availability of LTCHs
and IRFs across markets.
Because PAC can be appropriately provided in a variety of settings, Medicare
ideally would pay for PAC using one payment system with payments based on
patient characteristics, not on the site of service. Such fundamental payment
reforms within fee-for-service (FFS) Medicare are on the distant horizon. The
Commission recommended that CMS collect common patient assessment data
from the PAC settings to enable more complete comparisons of providers’ costs
and outcomes. Under the Improving Medicare Post-Acute Care Transformation
(IMPACT) Act of 2014, PAC providers will begin collecting uniform assessment
data in 2018. After the Secretary of Health and Human Services has collected two
years of data, she is required to submit a report to the Congress recommending a
uniform payment system for PAC. The IMPACT Act also requires the Commission
to develop a prototype prospective payment system spanning the PAC settings,
using the uniform assessment data gathered previously during CMS’s Post-Acute
Care Payment Reform Demonstration (completed in 2011). The Act requires the
Commission to submit a report in 2016 presenting an approach for a cross-setting
PAC payment system.
In the near term, the Commission maintains that Medicare can and should move in
the direction of uniform payments by aligning payments across settings for select
conditions. Consistent with the Commission’s approach to site-neutral payments
in the ambulatory and acute care sectors, the Commission used criteria to identify
conditions that may be appropriate for site-neutral payments between IRFs and
SNFs. For the select conditions, the majority of cases are treated in SNFs and
the risk profiles of patients treated in IRFs and SNFs are similar, yet Medicare’s
payments made to IRFs are considerably higher than those made to SNFs. To
ensure that it proceeded cautiously, the Commission also examined differences in
outcomes for patients treated in both settings. Because PAC providers do not collect
uniform patient assessment information, it is difficult to compare outcomes. Key
59

161 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
measures (such as changes in patients’ function) are not uniformly collected and
cannot be adequately risk adjusted. However, neither CMS’s PAC demonstration,
which gathered comparable data, nor other research has found consistent
differences in outcomes between the two settings. Where differences in outcomes
have been detected, researchers concede that the comparisons cannot fully control
for selection differences between the settings.
The Commission recommends that the Congress direct the Secretary to establish
site-neutral payments between IRFs and SNFs for select conditions, using
criteria such as those the Commission examined. For the selected conditions, the
Commission recommends that the IRF base payment rate be set equal to the average
SNF payment per discharge for each condition. The additional payments many
IRFs receive for teaching programs and treating low-income patients and high-cost
outliers are not changed by this policy. The policy should be implemented over
three years to give IRFs time to adjust their cost structures and to give policymakers
time to monitor the effects of the change on beneficiaries and providers. As part
of the policy, IRFs should be relieved from the regulations governing the intensity
and mix of services for the site-neutral conditions. CMS should use its rule-making
process to first propose criteria to select conditions appropriate for a site-neutral
payment policy and then to identify conditions that would be subject to the site-
neutral policy. In this way, the Secretary can gather input from key stakeholders.
The Commission has also considered private sector strategies that FFS Medicare
could pursue to direct beneficiaries to higher quality, more cost-effective providers.
Although FFS Medicare is more limited in the tools it can use to manage care,
certain options could be explored that shift use toward high-value providers while
respecting beneficiaries’ freedom of choice. ■
60

163 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
trends in post-acute care
Post-acute care (PAC) providers offer important recuperation and rehabilitation services to Medicare beneficiaries recovering from an acute hospital stay. PAC providers include skilled nursing facilities (SNFs), home health agencies (HHAs), inpatient rehabilitation facilities (IRFs), and long-term care hospitals (LTCHs). Among beneficiaries enrolled in fee-for-service (FFS) Medicare and discharged from an acute care hospital in 2013, 42 percent went on to post-acute care: 20 percent were discharged to a SNF, 17 percent were discharged to an HHA, 4 percent were discharged to an IRF, and 1 percent were discharged to an LTCH. Medicare is the dominant payer in all but the SNF setting; it is a minority payer in SNFs because most SNFs are predominantly nursing homes providing long-term care, which Medicare does not cover.
Medicare’s outlays for PAC are substantial. In 2013, Medicare paid for 9.6 million PAC encounters (IRF and LTCH discharges, home health episodes, and SNF stays) to more than 29,000 PAC providers. Between 2001 and 2012, program payments to PAC providers doubled to $59 billion. Yet despite this heavy investment, the need for PAC is not well defined, and Medicare gives providers considerable latitude in delineating which patients they admit among the patients referred to them by hospitals. Placement decisions often reflect a variety of nonclinical factors such as local practice patterns, the availability of PAC in a market, patient and family preferences, and financial arrangements between a PAC provider and the referring hospital (Buntin 2007). Reflecting this ambiguity, Medicare per capita spending on PAC varies more than any other covered service, which is only partly explained by the large differences in the availability of LTCHs and IRFs across markets. The Commission and others have noted that similar patients are treated in different settings with widely varying program payments, reflecting the separate systems Medicare uses to establish payments for each setting (Gage et al. 2011, Medicare Payment Advisory Commission 2014a).1
Complicating the comparison of patients, outcomes, and costs of care across PAC settings is the lack of uniform assessment information about the patients treated in the various PAC settings. In 2014, the Commission recommended that PAC providers gather uniform assessment information from all four settings, which the Congress mandated in the Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014. These data
are critical to evaluating providers’ selection practices, costs, and outcomes.
The most notable trend in the program’s spending across PAC settings is the high and sustained level of Medicare margins (a measure that compares program payments with the costs to treat its beneficiaries) relative to other settings. For example, Medicare margins for HHAs and SNFs have been above 10 percent every year since 2001. Consistently high Medicare margins indicate that program payments are set too high relative to the costs of treating Medicare beneficiaries and are thus a poor use of taxpayer dollars. Another signal that payment rates are too high is the growth in the number of for-profit providers, especially among HHAs. Although the overall number of IRFs and SNFs has not increased, the share of for-profit providers in these industries has climbed.
Another trend in Medicare PAC is the wide variation in Medicare margins. Across all PAC settings, Medicare margins are higher in for-profit facilities compared with nonprofit facilities, and in freestanding providers compared with hospital-based providers. The disparity in margins reflects very different costs per unit of service. In general, larger, freestanding, for-profit facilities have lower unit costs (after controlling for differences in case mix and wages) than smaller, hospital-based, nonprofit facilities. Larger, freestanding providers may be able to achieve more economies of scale. In addition, for-profit entities may be more focused than their nonprofit counterparts on controlling costs so as to maximize returns to investors. In general, Medicare policy should not subsidize providers’ inefficiencies except to ensure access (for example, in remote rural locations).
Across all settings, the margin trends are consistent with some providers maximizing revenues by taking advantage of payment system rules and shortcomings. These revenue approaches include strategically assessing patients to take advantage of the case-mix groups, providing additional (potentially unnecessary) therapy to increase revenues (in the case of SNFs and HHAs), and admitting patients who may not need the setting’s intensity of care. Further, in HHAs and SNFs, the prospective payment system (PPS) designs result in payments for therapy services that are much higher than these services’ costs. As a result, providers benefit financially when they furnish therapy services that may not be medically necessary. The Commission recommended revisions to the SNF and HHA payment systems that would redistribute payments across different types of cases and dampen the
61

164 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
patient assessment data are needed for Medicare to develop a common PAC payment system. The recently enacted IMPACT Act includes new requirements for uniform data collection beginning in 2018. After the Secretary of Health and Human Services has collected data for two years, she is required to submit a report to the Congress recommending a uniform payment system for PAC. The Act also requires the Commission to develop a prototype PPS to span the PAC setting using data CMS gathered during its PAC demonstration and to report to the Congress in July 2016. Given the timing of the data gathering and analysis, the implementation of a uniform payment system could be achieved in 2023 at the earliest. In the near term, carefully crafted site-neutral policies can begin the process of establishing one price for similar patients, regardless of the setting in which the care is provided.
site-neutral payments for select conditions treated in inpatient rehabilitation facilities and skilled nursing facilities
The Commission’s annual review of Medicare payment adequacy for FFS providers has two objectives: (1) to recommend an appropriate aggregate level of payments using the update and (2) to ensure that payments are equitable across providers and patients. As a prudent purchaser, the program should not pay more for care in one setting than in another if the care can be provided safely in a lower cost setting. Rather than base its payments on the setting in which a beneficiary is treated, Medicare should base its payments on the resources needed to treat patients in the most efficient setting, adjusting for patient severity differences that could affect providers’ costs. Even as Medicare moves toward integrated payment and delivery systems, the FFS payments underlying these reforms should reflect the most cost-effective site of care.
Price differentials based on site of service create distortions in provider incentives. For example, previous Commission analyses found that when hospital outpatient department payments are not aligned with rates paid for the same services in a physician’s office, hospitals have an incentive to acquire physician practices and bill for these services at the higher hospital outpatient rate, increasing program spending and out-of-pocket costs for beneficiaries. Thus, the Commission has recommended a reduction or elimination of price differences for office
incentives to select certain patients over others and to provide care for financial rather than clinical reasons. The Commission also recommended, and the Congress has partly implemented, revisions to the LTCH PPS to lower payments for patients who are not chronically critically ill.
Despite the large increase in program spending on PAC, quality has not consistently improved among the settings and the measures the Commission tracks. Improvements have generally been nominal or nonexistent. For example, across the measures the Commission tracks, SNF quality did not substantially improve for many years; more recent trends indicate improvements in some measures and no change in others. Similarly, in home health care, there have been improvements in functional change but no improvement in hospitalization rates. IRFs have achieved nominal improvements in quality, while observed LTCH measures have been stable or slightly improved. These lackluster results raise questions about the value of Medicare’s purchases of PAC.
The Commission works to improve Medicare’s payments for PAC in several ways. First, through its annual review of payment adequacy and its recommendations to revise the Medicare PPSs, the Commission seeks to establish an aggregate level of payments commensurate with the cost to efficiently treat beneficiaries, as well as a more equitable distribution of payments across types of cases, to help ensure access for beneficiaries. Second, to align incentives and improve care across settings, the Commission has recommended penalties to HHAs and SNFs with high readmission rates. These policies would align PAC providers’ interests with those of hospitals and support the already growing interest in hospitals and accountable care organizations (ACOs) partnering with high-quality PAC providers. The Congress enacted a SNF readmission policy to begin in 2018.
While these revisions within individual PAC settings will increase the value of Medicare’s purchases, the Commission’s primary concern is that having separate payment systems for post-acute care does not facilitate rational pricing, encourage coordinated care, or establish a set of consistent incentives across providers. The patient populations in the four PAC settings overlap to some extent, and some PAC services are offered in more than one setting. Yet, because the payment systems differ, Medicare has different prices for similar patients based on the site of service. The Commission believes that Medicare needs a more uniform approach to payment for PAC and continues to make recommendations toward this goal. Uniform
62

165 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
visits and selected ambulatory services provided in physicians’ offices and hospital outpatient departments. The Commission also has recommended that payments to long-term care hospitals for non-chronically critically ill patients should be equal to those for comparable patients in acute care hospitals (Medicare Payment Advisory Commission 2014b, Medicare Payment Advisory Commission 2012).
In June 2014, the Commission reported on its analysis of payment differences for select services provided by SNFs and IRFs (Medicare Payment Advisory Commission 2014a). While both settings furnish rehabilitation services to beneficiaries after a hospitalization, there are several important differences in the way Medicare pays for SNF and IRF services (see online Appendix 7-A, available at http://www.medpac.gov). Medicare pays for patients admitted to SNFs on a per day basis, but pays on a per discharge basis for patients admitted to IRFs.2 Many IRFs receive separate payments for teaching, disproportionate share, or outliers, whereas SNFs do not. In addition, IRFs must meet a threshold compliance regarding the facility’s mix of cases; SNFs do not have this requirement. In addition, each setting has different services and requirements (see online Appendix 7-A, available at http://www.medpac.gov). IRFs are licensed as hospitals and have more extensive requirements regarding the amount of therapy and the frequency and level of medical supervision their patients receive. IRF patients must be able to tolerate and are expected to benefit from an intensive therapy program (often interpreted as requiring three hours of therapy a day). IRF requirements may cut in opposite ways for patient referrals. On the one hand, patients who require additional nursing or physician care may be more likely to go to IRFs; on the other hand, patients must be able to tolerate intensive therapy.
The Commission found that for selected conditions, IRFs and SNFs care for patients with similar risk profiles, despite differences in the mix of services provided and Medicare’s facility requirements. Often, SNFs care for more severely ill patients, most likely because of the intensive therapy requirement for IRF patients. Our research and analysis did not consistently find differences in patient outcomes. Yet, Medicare’s spending for beneficiaries who used IRFs was more than 60 percent higher than for comparable patients who used SNFs during the initial PAC stay, and IRF patients continued to have higher spending during the 30 days after discharge from facilities. Since SNF and IRF patients are often similar but do not uniformly have different outcomes, it
is not clear what Medicare is purchasing with its higher IRF payments. In some cases, the disparity in Medicare’s payments for patients treated in IRFs and SNFs could influence providers’ decisions about settings of care and may result in excessive program spending.
Identifying conditions for site-neutral paymentsTo identify possible conditions and services for site-neutral policies, the Commission used a consistent set of criteria previously described (Medicare Payment Advisory Commission 2014a). We examined conditions for which the majority of patients were treated in SNFs in markets (defined as hospital service areas) with both types of providers.3 In addition, we compared the risk profiles of patients treated in both settings to assess whether SNFs treat the same complexity as patients referred to IRFs.To err on the side of caution, we also examined differences in outcomes. Ideally, we would compare risk-adjusted outcomes, but the Commission recognizes that this information is often not available.
In the Commission’s June 2014 Report to the Congress, we examined three high-volume conditions: major joint replacement, hip and femur procedures, and stroke (Medicare Payment Advisory Commission 2014a). The majority of beneficiaries recovering from the orthopedic conditions were treated in SNFs. These patients were similar to orthopedic patients in IRFs in terms of their average risk scores, age, comorbidities, functional status at admission, predicted cost for therapy and nontherapy ancillary services, and eligibility for Medicaid as well as Medicare.
The Commission’s analysis of stroke as a potential condition for site-neutral payment was inconclusive. Stroke severity can vary widely, and patients with stroke may suffer from a wide range of comorbidities. We found that, although similar or larger shares of patients treated in SNFs had comorbidities, IRFs treat the majority of stroke patients. Therefore, at this time, the Commission did not include stroke in a site-neutral policy (see online Appendix 7-A, available at http://www.medpac.gov, for a discussion of the stroke results), although it is possible that a subset of stroke cases could be considered in the future.
In our consideration of the two orthopedic conditions for a site-neutral policy, we also compared outcomes for patients treated in the two settings. The differences were mixed, in large part because not all the measures were risk adjusted. CMS’s PAC demonstration found that
63

166 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
Appendix 7-A, available at http://www.medpac.gov). Across the conditions, SNFs typically treated the majority of the most severely ill patients, as measured by the severity of illness at discharge from the hospital using all-patient refined–severity of illness levels (Table 7-A6 in online Appendix 7-A, available at http://www.medpac.gov). We also compared the severity of illness of patients treated in SNFs in markets with and without IRFs and found them to be similar, suggesting that, for the select conditions, SNFs treat comparable severity mixes of patients, regardless of whether there is an IRF in the market. Finally, CMS’s PAC demonstration found considerable overlap in the functional status at admission between patients admitted to SNFs and IRFs (the patients in their analysis spanned all conditions, not just the 17 studied here). We conclude that for the selected conditions, SNFs can treat patients who are discharged to IRFs, and in markets without IRFs, they do.
outcomes for patients treated in IRFs and snFs
It is difficult to compare outcomes for patients treated in different settings because of the lack of comparable assessment information about patients’ function and cognitive abilities at admission and at the end of treatment. This type of analysis is exactly the reason the Commission recommended the collection of uniform information across PAC settings, which the Congress mandated in 2014. Even with comparable data, there is no way to fully control for the selection of certain types of patients by providers, which is reinforced by program requirements. We fully expect to see differences in outcomes between IRFs and SNFs because IRFs tend to treat healthier patients who must be able to tolerate intensive therapy.
But to proceed cautiously, we compared four outcomes for SNFs and IRFs—hospital readmission rates, changes in functional status, mortality rates, and total Medicare spending during the 30 days after discharge from the qualifying stay—and examined the literature comparing outcomes across the two settings (see text box on outcomes, pp. 168–169). The comparisons yielded mixed results, in part because some of the measures were not risk adjusted. Ideally, all measures would be risk adjusted, but the data needed for risk adjustment were not always available, and even when they were, we could not fully control for differences in patient mix because of selection.
Observed differences in readmission rates for IRF and SNF patients were effectively eliminated with risk adjustment. The PAC demonstration conducted by CMS gathered comparable patient assessment information for beneficiaries treated in participating SNFs and IRFs and enabled careful,
risk-adjusted rates of readmission and changes in patient mobility were comparable, and while IRFs had larger improvements in patients’ self-care across all types of cases, their gains were comparable with patients treated in SNFs for musculoskeletal conditions. Spending during the 30 days after discharge from an IRF was higher than the spending after discharge from a SNF. Unadjusted mortality rates were lower for IRFs, but differences would narrow with risk adjustment. The Commission concluded that the two orthopedic conditions (represented by five Medicare severity–diagnosis related groups (MS–DRGs)) would be a good starting point for site-neutral payments.
To identify additional conditions for consideration, we examined conditions frequently treated in IRFs but for which the majority of patients are treated in SNFs (Table 7-A1 in online Appendix 7-A, available at http://www.medpac.gov).4 Seventeen conditions met the criterion of having the majority of cases treated in SNFs; the MS–DRGs comprised other orthopedic, pulmonary, cardiac, and infection conditions. They make up about 17 percent of IRF cases and spending. When the 17 conditions are combined with the 5 orthopedic conditions we previously reported on in June 2014, the share of spending and cases increases to 30 percent of total IRF spending and cases.
There are large payment differences for the patients treated in IRFs and SNFs for the conditions we examined. On a per stay basis, total Medicare payments in 2012 (including the add-on payments made to many IRFs) averaged 64 percent higher for patients treated in IRFs compared with those treated in SNFs.5 Excluding these add-on payments, IRF payments were 49 percent higher than those made to SNFs (Table 7-A2 in online Appendix 7-A, available at http://www.medpac.gov).
similarity of patients treated in IRFs and snFs
To assess the similarity of risk profiles of patients treated in IRFs and SNFs, we compared their demographics and comorbidities. In markets with both IRFs and SNFs, patients treated in SNFs were older and more likely to be female or dually eligible for Medicare and Medicaid compared with patients treated in IRFs (Table 7-A3 in online Appendix 7-A, available at http://www.medpac.gov). In 2012, either the patients treated in IRFs and SNFs had similar Medicare risk scores (the hierarchical condition categories, or HCCs) or the patients treated in SNFs had higher scores (Table 7-A4 in online Appendix 7-A, available at http://www.medpac.gov). The most common comorbidities either were more frequent in SNFs or were similar between the two settings (Table 7-A5 in online
64

167 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
cross-setting study of the patients and their outcomes. The evaluation found that risk-adjusted readmission rates and changes in patients’ mobility were comparable between the two settings across all patients and for the four subgroups of patients examined (nervous system, respiratory, circulatory, and musculoskeletal) (Gage et al. 2011). Changes in self-care were larger for patients treated in IRFs compared with patients treated in SNFs, although there was no difference between the settings for the musculoskeletal patients. An IRF-industry sponsored study of 13 groups of conditions found that differences in readmission rates varied by condition group (DaVanzo et al. 2014).
Some researchers have focused on comparing mortality rates of patients treated in both settings. We examined mortality rates without risk adjustment during the SNF and IRF stays and during the 30 days after discharge and found that both were higher for patients treated in SNFs compared with patients treated in IRFs. The difference in rates partly reflects differences in the patient populations: SNF patients were older and often had more comorbidities. It is likely the differences would be much smaller after risk adjustment, but we would expect some differences to remain. Each setting’s mortality rates reflect inherent differences in the patient population. Because IRF patients must be able to tolerate and benefit from intensive therapy, we would expect their mortality rates to be very low. Furthermore, because post-acute services are restorative, not curative, it is not the best measure of outcomes for these settings. The IRF industry–sponsored study found that compared with IRFs, SNFs had higher mortality rates during the two years after discharge (DaVanzo et al. 2014). Given the differences between the populations, we would expect patients treated in SNFs to be more likely to die within the next two years compared with patients treated in IRFs.
Finally, we examined Medicare spending during the 30 days after discharge from IRFs and SNFs. We found that program spending was 7 percent higher for beneficiaries discharged from IRFs than for beneficiaries discharged from SNFs. Although IRF patients had considerably lower costs for readmission, they had much higher subsequent PAC spending, perhaps because patients continued to need rehabilitation (see Table 7-A7 in online Appendix 7-A, available at http://www.medpac.gov).
establishing a site-neutral policy for IRFs and snFsIdeally, Medicare would pay for PAC using a single payment system that based payments on patient
characteristics, not the site of service. Such fundamental payment reforms within FFS Medicare are on the distant horizon. As required by the IMPACT Act of 2014, the Commission is developing a prototype prospective payment system to span the PAC settings using the uniform assessment data gathered as part of CMS’s PAC payment demonstration. The law also requires PAC providers to submit patient assessment data using a uniform assessment tool beginning in 2018 and requires the Secretary of Health and Human Services to recommend a uniform payment system for PAC based on two years of uniform patient assessment data. Thus, a new PAC payment system is unlikely to be in place until 2023 at the earliest.
However, the Commission believes that Medicare should not delay reforms that encourage cost-effective care. Even as Medicare moves toward integrated payment and delivery systems, Medicare can and should move in the direction of uniform payments by establishing a site-neutral policy for IRFs and SNFs to align payments across the two settings for select conditions. For each condition selected, the Commission’s site-neutral policy would set the IRF base payment at the average rate paid to SNFs for patients with that condition.6 Specifically, CMS would replace the IRF base rate with the average payment per discharge for the same case type for a SNF in the same geographic location. The policy would not change the additional payments many IRFs receive for teaching programs and treating low-income patients and high-cost outliers. At the same time, for patients with conditions paid under the site-neutral policy, IRFs would be relieved of certain regulatory requirements that govern patient care, such as the requirement for intensive therapy, the frequency of physician visits, and the physician-conducted preadmission screening and the postadmission evaluation.7 Waiving these requirements would lower IRFs’ costs of treating patients with site-neutral conditions. (Regulatory requirements for IRFs would remain the same for conditions not affected by the site-neutral policy.) To identify candidate conditions for a site-neutral policy between IRFs and SNFs, Medicare should establish a set of criteria that considers how frequently the condition is treated in SNFs and the similarity of the risk profile. Outcomes should also be compared to ensure that they do not substantially differ between the two settings.
For conditions not affected by the site-neutral policy, CMS should refine and recalibrate the IRF case-mix groups (CMGs), establish new average standardized costs for the non-site-neutral cases, and recalibrate the weights associated with each CMG. The selection of
65

168 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
budget neutrality for these cases; aggregate IRF payments for them would be held to the same aggregate payments these cases receive currently. Such recalibration is typically undertaken by CMS when new case-mix systems are implemented.
A set of relative weights would be estimated using all cases to retain add-on payments at current levels for all cases. IRF PPS add-on payments for teaching program status and share of low-income patients would be calculated by multiplying the applicable IRF teaching and low-income percentages by the wage- and case-
the final conditions for a site-neutral policy may remove certain CMGs entirely from the IRF PPS or remove select conditions within a CMG. Because the waiving of certain regulations for treating the site-neutral conditions may lower the costs of the site-neutral cases, the cost of cases remaining under the IRF PPS could increase relative to the average cost, even if actual cost is unchanged. Thus, without recalibration, payments for cases remaining under the IRF PPS could increase simply as a result of the site-neutral policy. Recalculating the relative weights for the cases remaining under the IRF PPS is a way to retain
Comparing outcomes of rehabilitation care in skilled nursing facilities and inpatient rehabilitation facilities
Researchers and policymakers have frequently sought to compare outcomes for patients treated in different post-acute care settings.
Such comparisons are generally compromised by a lack of comparable assessment information about patients’ function and cognitive abilities at admission and at the end of treatment. Even with comparable data, there is no way to fully control for the patient selection by providers—selection that is reinforced by program requirements such as the requirement that patients admitted to inpatient rehabilitation facilities (IRFs) be able to tolerate and benefit from intensive therapy.
Studies of costs and outcomes of patients treated in skilled nursing facilities (SNFs) compared with IRFs have largely focused on patients needing rehabilitation following a stroke, hip fracture, or joint replacement. Overall, research studies do not conclusively identify a particular post-acute care setting as having better outcomes for rehabilitation patients. Studies of patients after joint replacement and hip fracture do not have consistent conclusions (Buntin et al. 2010, Dejong et al. 2009a, DeJong et al. 2009b, Deutsch et al. 2006, Deutsch et al. 2005, Herbold et al. 2011, Mallinson et al. 2014, Mallinson et al. 2011, Munin et al. 2005, Walsh and Herbold 2006). Studies of stroke patients found that patients in IRFs had better outcomes than those in SNFs, though selection bias could have contributed to these findings (Buntin et al. 2010, Deutsch et al. 2006).
A 2010 CMS report to the Congress analyzed peer-reviewed research on the effectiveness of IRFs compared with other post-acute care settings and concluded that many studies are limited because they do not adequately control for selection bias (Gage et al. 2010). The report also found inconsistent results across studies comparing outcomes for lower extremity joint replacement patients and hip fracture patients in IRFs and SNFs. The report was unable to conclude definitively whether shifts in discharge destination due to the IRF compliance threshold have affected beneficiaries’ access to appropriate rehabilitation services. The ambiguous results of these studies may also suggest that reasonable treatment approaches may differ across beneficiaries. Some patients may be more appropriate for longer stays in less intensive settings while others benefit from shorter, more intensive therapy (Stineman and Chan 2009).
Standardized data from the Continuity Assessment Record and Evaluation (CARE) tool—a uniform post-acute care assessment tool tested through the Medicare Post-Acute Care Payment Reform Demonstration (PAC–PRD)—can help CMS compare outcomes for rehabilitation care across settings. The demonstration used the CARE tool to compare outcomes across sites of care, including readmission to the hospital and improvements on two functional measures, mobility and self-care function. The 2011 report summarizing the findings compared outcomes among IRFs, SNFs, home health agencies, and long-term care hospitals
(continued next page)
66

169 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
requiring that a certain proportion of all patients have 1 of 13 conditions specified by CMS as typically requiring intensive rehabilitation. An IRF’s compliance rate is calculated by dividing the total number of compliant conditions (the numerator) by the total number of cases (the denominator). Some of the conditions that meet the Commission’s criteria for site-neutral payment—such as hip fracture and amputations—are among CMS’s list of compliant conditions. If patients with these conditions can be treated appropriately in SNFs, they likely do not require the intensity of the IRF setting. Thus, conditions that are
mix-adjusted IRF rate. For site-neutral cases with extraordinarily high costs, an outlier payment would be calculated using the IRF PPS fixed loss amount.
Revising the IRF compliance requirements
The implementation of site-neutral payment for IRFs and SNFs would necessitate changes to the IRF compliance rule. The intent of this rule is to distinguish IRFs from acute care hospitals (not from SNFs). Currently, to qualify as an IRF for Medicare payment, facilities must meet a compliance threshold (the “60 percent rule”)
Comparing outcomes of rehabilitation care in skilled nursing facilities and inpatient rehabilitation facilities (cont.)
(Gage et al. 2011). Risk-adjusted readmission rates that controlled for differences in patient acuity did not differ significantly between IRFs and SNFs.
On functional outcomes, the risk-adjusted analysis of data from the PAC–PRD found no significant difference in the average degree of improvement in mobility, but did find a somewhat higher gain in self-care outcomes among patients who received care from IRFs compared with patients treated in SNFs (Gage et al. 2011). But differences in outcomes varied by clinical condition. The demonstration study examined improvement in self-care for the subgroups of patients with musculoskeletal and nervous system conditions, two conditions for which beneficiaries typically receive significant amounts of therapy. For nervous system conditions, the average risk-adjusted gain in self-care improvement was higher in IRFs than in SNFs. In contrast, for musculoskeletal conditions, there was no significant difference in the risk-adjusted degree of improvement between IRF and SNF patients. Where results varied, the difference in improvement among settings was relatively small, less than 5 points on a 100-point scale.
Although the PAC–PRD was able to control for differences in patients to a degree unparalleled by most other research, the study did not randomly assign patients to post-acute care settings, so unobserved factors regarding patient characteristics may have remained and influenced outcomes. For example, the more intensive therapy requirements in IRFs may have resulted in IRFs attracting patients who were more engaged or more motivated to improve. Likewise, factors such as informal
caregiver support that were not included in the model could have influenced both the likelihood of referral to different post-acute care providers and patient outcomes.
There is very little literature comparing outcomes across many conditions. An industry-sponsored study compared several outcomes of patients treated in IRFs and SNFs and found differences across conditions (DaVanzo et al. 2014). To risk adjust the comparisons of the outcomes, the study matched various characteristics of the IRF patients to the patients treated in SNFs, though measures of function were not among the adjusters. Of the various groupings of conditions the study examined, six overlapped with those considered by the Commission. Hospital readmission rates were not consistently better for patients treated in IRFs: They were lower for two condition groups, higher for one, and no different for three condition groups. Four measures—mortality rates, average days alive (a corollary of mortality rate), days residing at home, and program spending—examined outcomes over two years. Given the differences in ages and comorbidities between patients treated in IRFs and SNFs, the study unsurprisingly found that IRFs had lower mortality rates and more days alive, while there were no differences in the number of days patients resided at home between the two settings for patients with hip or knee replacement or other orthopedic condition groups. Emergency room visits per 1,000 patients were no different between the 2 settings for 5 of the 6 conditions, and IRFs had fewer ER visits than SNFs for 1 condition. The spending over two years was higher for patients treated in IRFs for four condition groups and no different for two. ■
67

170 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
considered candidates for the policy in addition to the orthopedic conditions (5 MS–DRGs) previously identified. A site-neutral policy would lower total program spending (including the add-on payments) for the 22 conditions by 7 percent.8 The impact on total payments is tempered by two factors. First, the conditions represent a minority of IRF cases. Second, the policy assumes site-neutral payments would not change the add-on payments many IRFs receive for the site-neutral conditions. In 2012, the estimated reductions to aggregate IRF base payments would have totaled $497 million: $309 million for the 17 additional conditions and $188 million for the 5 orthopedic conditions. If a different set of conditions were selected for site-neutral policy, the impact would be different.
Like many major changes to payment policy, the site-neutral policy should be phased in over multiple years. This time frame would give IRFs time to adjust their cost structures and admitting practices and would give policymakers time to evaluate the initial effects of the policy. The Commission considered a period of three years for fully transitioning payments for site-neutral conditions, a time period used in other policies. During the transition, payments for site-neutral conditions could be a blend of IRF and SNF payments, such as a 75 percent IRF/25 percent SNF blend in the first year, a 50/50 blend in the second year, and a 25/75 blend in the third year, with site-neutral payments fully implemented in the fourth year.
The effects on spending assume the current SNF PPS. The Commission has recommended that the SNF PPS be revised so that payments are based on patient characteristics, not the amount of therapy provided. Under the proposed design, payments would be higher for patients whose clinical and functional characteristics increase their need for services. The proposed redesign is assumed to be budget neutral, so that aggregate SNF payments would be the same as under current policy. Our prior work found that the site-neutral effects on IRFs would not be substantially different under a revised SNF PPS (Medicare Payment Advisory Commission 2014a). Differences in effects between current SNF policy and the proposed redesign would depend on the final selection of conditions for the site-neutral policy.
Likely effects of site-neutral payments on IRF patient mix and volume
We cannot estimate how IRF costs, patient mix, and volume would change in response to a site-neutral policy.
appropriate for site-neutral payment should not count toward the 60 percent rule. Furthermore, the Commission has commented before that more refined criteria are needed to identify patients appropriate for IRFs (Medicare Payment Advisory Commission 2013). The criteria have already narrowed the hip and knee replacement cases and arthritis conditions that count toward the 60 percent rule. Likely there are subsets of other conditions that are appropriate for IRF care and should count toward IRF compliance; conversely, others are not appropriate for IRF care and should not count. The Commission believes that detailed criteria should be developed for all 13 conditions under the 60 percent rule.
The site-neutral policy is not intended to make it more difficult for IRFs to maintain compliance, but this unintended consequence could result if the current threshold policy were not refined. Under a site-neutral policy, the fairer way to calculate the compliance rate would be to remove the site-neutral cases from the numerator and denominator; however, mathematically, this change would lower a facility’s compliance rate. Thus, reducing the conditions that count toward the compliance threshold could necessitate a reduction in the threshold itself. For example, nine of the conditions we identified as candidates for a site-neutral policy are among the specified conditions counting toward the 60 percent compliance threshold. If these conditions were selected for site-neutral payment, CMS would calculate each IRF’s compliance threshold by subtracting the number of IRF cases with the nine conditions from both the numerator and the denominator. Removing these cases from the calculation would lower the share of cases meeting the compliance threshold; policymakers therefore might consider lowering the compliance threshold correspondingly. Any change to the compliance threshold should be empirically based, with consideration of the set of conditions selected for site-neutral payments and whether those conditions currently count toward threshold compliance. Consistent with current practice, IRFs are likely to continue to treat cases that do not count toward compliance, keeping the share of noncompliant cases below the threshold so they retain their status to be paid as an IRF for conditions unaffected by the site-neutral policy. For facilities treating a large share of site-neutral cases, CMS would need to consider whether they continued to meet the IRF conditions of participation.
Likely effects of a site-neutral policy on program spending
We assessed the impact of a site-neutral policy on payments for the 17 conditions the Commission
68
171 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
possible that some IRFs would again adjust their mix of cases to preferentially admit those paid under the IRF PPS, with site-neutral cases shifting to SNFs. However, industry reaction to site-neutral payment would likely differ across facilities because, with the waiving of requirements, facilities could change their cost structures and service mix to accommodate the change in payment.
An IRF’s ability to shift its patient mix toward cases not affected by a site-neutral policy would depend in part on characteristics of the market in which it is located. IRFs located in markets without competitors might find it easier to shift their mix of patients toward those cases that the average SNF is not staffed or equipped to manage, such as patients receiving rehabilitation care for burns or traumatic brain injury. IRFs that compete with other IRFs or specialized SNFs to treat IRF-compliant cases might be limited in the extent to which they can shift their focus toward non-site-neutral cases.
The Commission’s analysis indicates that, if some portion of site-neutral cases shifted to SNFs, the SNF industry would have the capacity to treat these cases. In 2012, although the average SNF occupancy rate was high (82 percent), the additional volume associated with movement of site-neutral conditions from IRFs to SNFs would be small relative to total SNF volume. Furthermore, one-quarter of SNFs had occupancy rates at or below 76 percent, indicating capacity to treat additional cases. Average occupancy rates also varied by market (defined as hospital service areas). One-quarter of markets had an average occupancy rate at or below 76 percent and one-quarter had an average occupancy rate at or above 91 percent. In markets with very high SNF occupancy rates, accessing a SNF bed could become more difficult, depending on the extent to which IRFs shifted their case mix.
The method used by the Secretary to identify site-neutral cases could encourage IRFs to change their coding of cases to shift cases out of site-neutral conditions to case-mix categories not affected by the policy, thereby retaining IRF PPS–based payments. For example, if IRF case-mix groups were used, IRFs could shift their coding to avoid those groups. Instead, the use of the hospital MS–DRG system to identify cases would minimize such coding changes. Further, using MS–DRGs as at least part of the method to identify cases for site-neutral payments will allow IRFs and auditors to clearly identify cases as eligible for site-neutral payment before admission. Finally, the MS–DRG system would provide a consistent way to
With greater regulatory flexibility to adjust their service intensities, IRFs are likely to continue to treat site-neutral conditions, especially given their relatively low occupancy rates (the average is 63 percent) and the high profit margins possible under the SNF PPS. Because some regulations would be waived for site-neutral conditions, IRFs could adjust their cost structures by varying the number of physician face-to-face visits each week and providing fewer hours of therapy each day, as IRF clinicians deem necessary. Such changes would reduce IRF costs for treating site-neutral conditions, thereby leveling the playing field between IRFs and SNFs.
Still, facilities would likely vary in how quickly they could adjust their variable costs. Larger facilities have more options for adjusting those costs (for example, by adjusting the staffing for an entire nursing unit). However, many small IRFs are hospital based, so their affiliation with acute care hospitals affords them opportunities to adjust their cost structures. The Commission’s analysis indicates that a large share of acute care hospitals’ costs is variable.
Despite lower payments, site-neutral cases could still be profitable for some IRFs or could cover a facility’s patient care costs and contribute toward covering a facility’s fixed costs (and would be preferable to an empty bed). Hospital-based IRFs could continue to boost total hospital margins (they add about a percentage point to the overall hospital margin). Under the current IRF PPS, hospital-based facilities have break-even Medicare margins, but their contribution margin (a measure of whether Medicare payments cover direct patient care costs) is a healthy 35 percent. Once IRFs have adjusted their cost structures, they—like SNFs—may find that Medicare’s SNF payments are highly profitable while achieving comparable outcomes. And because some hospital-based IRFs are low cost (in 2013, 40 percent of the facilities in the lowest cost quartile were hospital based), we believe hospital-based IRFs can manage their costs to remain profitable. Still, as IRFs change the mix of services, therapy intensity, and lengths of stays for cases paid under a site-neutral policy, it will be important to monitor outcomes and the quality of care furnished to these patients.
It is possible that some IRFs would opt to no longer treat patients with site-neutral conditions. After CMS began enforcing the compliance threshold in 2004, IRFs significantly shifted their mix of patients, admitting more cases that counted toward the compliance threshold. It is
69
172 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
with some patients benefiting from longer, less therapy-intensive stays and others benefiting from shorter, more intensive stays.
Under a site-neutral payment policy, the cost-sharing liability of beneficiaries who were shifted to SNFs would remain the same if they stayed less than 21 days. For the conditions considered for site-neutral payment, the vast majority (94 percent) of IRF users had stays of 20 days or less. Patients who were shifted to SNFs and stayed 21 or more days would have higher financial liability than they do currently. However, because most beneficiaries have supplemental coverage and the most common policies cover SNF payments, beneficiary liability for most will not change. Some beneficiaries could opt to go home rather than be admitted to SNFs. For them, cost sharing would depend on whether they opted to receive home health care (with no cost sharing) or outpatient therapy services (with 20 percent copayments).9
Given the similarity in readmission rates and functional outcomes between IRFs and SNFs, we expect that patient outcomes would not be affected by the implementation of a site-neutral policy. However, monitoring both access to and quality of care for site-neutral conditions in both settings would be important. This monitoring, which the Commission plans to conduct, will focus on detecting inappropriate provider responses, such as impairing access to care for beneficiaries and furnishing poorer quality of care resulting in worse outcomes. The analysis will consider access to services in markets with high SNF occupancy rates and the potential changes in coding to avoid site-neutral payments.
Recommendation on site-neutral payments for IRFs and snFs for select conditionsThe Commission’s recommendation extends site-neutral payment policies to PAC, starting with select conditions treated in IRFs and SNFs. Because the policy would require some changes to the IRF PPS that are set in statute, our recommendation is directed to the Congress. The Secretary should use a set of criteria such as those considered by the Commission to identify appropriate conditions for site-neutral payment. For the selected conditions, the Commission’s recommendation would set the IRF base rate at the average payment per discharge made to SNFs. By aligning payments between the two settings, Medicare would move away from paying for services based on the setting in which they are provided and toward a common payment for comparable patients.
categorize patients treated in IRFs and SNFs since the SNF and IRF payment systems use different case-mix groups. Critics of this approach posit that MS–DRGs are too broadly defined to identify site-neutral conditions. MS–DRGs could be supplemented with specific diagnoses coded by the hospital or other patient characteristics not subject to manipulation by IRFs, which would mitigate any disadvantages of using MS–DRGs while avoiding the incentives for IRFs to code cases specifically to avoid site-neutral payments.
Hospitals that have affiliations with IRFs may have a greater incentive to code inpatient cases more favorably (avoiding site-neutral conditions), so CMS and the Commission would need to closely monitor their coding practices. For example, certain respiratory conditions lend themselves to alternative coding that could avoid the site-neutral policy. Entities that operate both IRFs and SNFs, including hospitals (185 of the approximately 900 hospitals with IRFs also have SNFs) may have an advantage over other providers to direct cases to one setting or another to maximize total facility revenue.
Likely effects of site-neutral payments on beneficiaries
The effects on beneficiaries would depend on how IRFs responded to the site-neutral policies, but we expect the impact would be small. Clinicians, in consultation with patients and their families, would continue to be the decision makers about where patients received rehabilitation care after discharge from the hospital. The site-neutral policy is not intended to preempt the clinician’s prerogative to select the best and most appropriate setting for beneficiaries. Further, the site-neutral policy does not change the program’s benefits for beneficiaries. It simply pays providers a different rate for select conditions. Beneficiaries could still be admitted to IRFs, and IRF days would not count toward the 100-day limit of SNF care following a 3-day hospital stay.
Many IRFs are likely to continue to treat these conditions, so the impact on beneficiaries would be minimal. Access to care would remain at current levels. Beneficiary financial liability would not change since most beneficiaries meet the inpatient deductible during their preceding acute hospital stay. The comparability of most outcomes for patients treated in SNFs and IRFs indicate that even if IRFs changed the services they provide, patient outcomes would not necessarily be affected. Moreover, optimal treatments are likely to differ across patients,
70
173 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
requirements would be expected to lower IRFs’ costs. A three-year transition would give IRFs time to adjust their cost structures and provide policymakers time to monitor the initial effects of the policy.
I M p L I C A t I o n s 7
spending
• The site-neutral policy would lower IRF base rates to the average payment per stay made to SNFs in the same geographic location for the same condition. Add-on payments IRFs receive (for having a teaching program or treating low-income patients or high-cost outlier cases) are not changed by this policy. Over five years, the site-neutral policy would lower program spending relative to current policy by between $1 billion and $5 billion. This estimate is consistent with the Commission’s estimate of the reductions in payments for a fully implemented policy.
Beneficiary and provider
• The policy lowers payments to IRFs for site-neutral conditions, but the Commission believes many IRFs will continue to treat these cases. IRFs are likely to adjust their cost structures in response to the regulatory relief and continue to admit patients with site-neutral conditions. To the extent that IRFs elect not to treat these patients, some SNFs could experience a commensurate increase in volume.
• We do not anticipate that a site-neutral policy would negatively affect beneficiaries. We expect many IRFs will continue to treat patients with these conditions and, for these beneficiaries, the effects will be minimal. The site-neutral policy will not change the SNF benefit, and the IRF days paid at site-neutral rates will not count toward the 100-day SNF benefit. Some beneficiaries’ care may be shifted to SNFs but—because we do not see significant differences between the two settings in terms of readmission rates and mortality—much of their care is expected to be comparable. Cost-sharing liability is not expected to increase for the vast majority of beneficiaries, though it could increase for the small number of beneficiaries who are shifted to SNFs and whose stays exceed 20 days. However, most beneficiaries have supplemental coverage and the most common policies cover the SNF copayments, so the actual cost sharing for most beneficiaries would remain unchanged.
R e C o M M e n D A t I o n 7
the Congress should direct the secretary of Health and Human services to eliminate the differences in payment rates between inpatient rehabilitation facilities (IRFs) and skilled nursing facilities for selected conditions. the reductions to IRF payments should be phased in over three years. IRFs should receive relief from regulations specifying the intensity and mix of services for site-neutral conditions.
R A t I o n A L e 7
To identify conditions appropriate for site-neutral payments, the Secretary should establish a set of criteria to identify conditions for the site-neutral policy. For its own criteria, the Commission considered whether the majority of patients were treated in SNFs (thus ensuring that the setting is safe for the treatment of the condition) and whether the patients treated in IRFs and SNFs had similar risk profiles. The Commission also evaluated the research on outcomes for the select conditions to be certain that IRFs did not consistently have higher quality. There is little evidence that IRFs consistently have better outcomes than SNFs. The Secretary should publish the criteria applied and data analyses conducted to identify proposed conditions and should use a notice-and-comment period to gather information in making its final selections. This process will help ensure that the Secretary proceeds cautiously in selecting criteria and conditions for the site-neutral policy. The Commission offers its criteria and analyses of 22 orthopedic, pulmonary, cardiac, and infection conditions to inform the Secretary’s process.
For the conditions selected by the Secretary, the base payments to IRFs should be set at the average payment per discharge paid to SNFs for the select set of conditions. The Secretary should replace the IRF base rate with the average payment per discharge for a SNF in the same geographic location for the same case type. The additional payments many IRFs receive for teaching programs and treating low-income patients and high-cost outliers should not change.
As part of a site-neutral policy, the Secretary should relieve IRFs of the regulatory requirements related to the intensity and mix of services furnished to beneficiaries with the select conditions. Requirements for consideration include providing daily intensive therapy, the weekly face-to-face physician visits, and the physician-conducted preadmission and postadmission evaluation. Waiving these
71

174 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
extent that these practices prove successful in referring beneficiaries to appropriate sites of care and lowering readmissions, broader adoption of these practices within FFS has the potential to improve care for beneficiaries and lower costs for the program.
Some FFS provider organizations have concerns about the information on preferred providers they are allowed to present without violating beneficiary freedom of choice rules. In general, “soft steering” is achieved by describing the relative merits of using a preferred provider: higher quality of care, more integrated medical staffs, and better coordinated care. If preferred networks are allowed, CMS should clarify what is and is not allowed in guiding decision making.
Future efforts could permit tighter linkages between ACOs and preferred networks. Because some ACOs are at financial risk for the cost of care, CMS could consider allowing those ACOs to establish formal networks to direct beneficiaries to high-value providers. Likewise, CMS could consider allowing hospitals to partner with high-value PAC providers, though many issues would need to be resolved to ensure hospitals acted responsibly. CMS would need to establish criteria for defining “preferred” status, such as network adequacy, quality and cost measures, and capabilities for managing special care (such as tracheostomy and ventilator care). An idea to explore is whether hospitals would also have to earn this “right” to maintain preferred networks by meeting certain benchmarks, such as achieving low readmission rates or other indicators that suggest they could responsibly manage preferred PAC networks.
A second strategy Medicare could use is to expand beneficiary incentives to use certain settings or providers over others. The PAC cost-sharing structure has not significantly changed since Medicare’s inception. Inherent in this structure are financial incentives, unrelated to clinical decisions, that encourage the use of certain settings over others and for certain time periods. For example, the SNF cost-sharing requirement creates an incentive for providers to keep beneficiaries for 20 days, regardless of whether they need this much care. Alternately, cost-sharing incentives could be created to encourage beneficiaries to use preferred providers that offer high-value care. However, changes to beneficiary cost sharing would also have to be sensitive to the amounts beneficiaries already incur. For example, policies could lower the incurred cost sharing when beneficiaries select providers that meet standards for quality and cost of care.
private sector ideas for managing post-acute care
The Commission examined strategies used by private sector entities to explore additional ways to more effectively manage PAC. A contractor and Commission staff interviewed PAC benefit management vendors, PAC providers participating in CMS’s PAC Bundled Payment for Care Improvement Initiative, and officials at health systems with Medicare Advantage (MA) plans or ACOs.
FFs and MA plans differ in the approaches they take The approaches used by FFS entities (for example, ACOs, providers, and integrated health systems that are paid FFS) and MA plans to manage PAC differ considerably. FFS entities typically guide patient decisions about the choice of PAC setting and provider, whereas MA plans typically establish rules about PAC use. In part, this difference reflects the differences in Medicare rules governing each. MA plans can establish networks of providers in which services are covered and use prior authorization and recertification to direct where enrollees go and how much care they receive, with an appeals process tempering this control somewhat. In contrast, even FFS entities at financial risk (ACOs and entities participating in CMS’s bundling initiatives) must allow beneficiaries the freedom to select the provider of their choice and cannot use tiered provider payments, beneficiary copayments, or prior authorization to influence service use. FFS providers must rely on “softer” approaches that guide decisions made by clinicians and patients toward using lower cost, higher quality providers.
strategies to manage post-acute care under FFs MedicareDiscussions with private sector entities identified two strategies that FFS Medicare could pursue to better manage PAC. First, some ACOs have established partnerships with selected PAC providers. Under this arrangement, ACOs select PAC partners by reviewing the cost and quality metrics for each provider and its geographic coverage. Hospital discharge planning teams then choose from the selected pool of PAC providers when referring patients. Although preferred networks may narrow beneficiary choice, they create a preferred set of higher quality PAC providers that could improve care for beneficiaries without impairing access to care. The process is intended to guide, but not dictate, decision making; beneficiaries retain their choice about where to go. To the
72

175 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
Conclusion
The complexity and cost of PAC indicates that Medicare needs a range of policies to ensure the appropriate and efficient use of these services. In the near term, the Commission is recommending policies that ensure that program payments under PPS are commensurate with costs, a particularly important policy given the high payments for several PAC settings. In addition, Medicare can begin to move toward site-neutral payments where there is clear overlap in the services provided, such as for certain patients served by SNFs and IRFs. In the longer run, Medicare is beginning efforts to develop a common payment system that will eliminate the adverse incentives and inefficiencies resulting from multiple uncoordinated systems.
The Commission’s review of private sector practices suggests that further efforts to improve the management of PAC services in FFS are possible. A refined referral process, one that better supports beneficiary choice by providing beneficiaries with better information about available providers, could encourage the use of higher quality providers. These approaches could be particularly appropriate for ACOs or other models of delivery reform where hospitals and other providers are at risk for the cost of care and quality indicators. However, other approaches may be necessary when no entity is available to assume these risks (for example, holding PAC providers accountable for quality like the Commission has recommended for SNFs and home health agencies). Other changes may include aligning incentives for referring physicians and beneficiaries (for example, through the expanded use of quality information for comparing different PAC providers or by creating incentives through reformed PAC cost sharing). ■
strategies to manage post-acute care under managed careThree strategies—prior authorization for the use of high-cost PAC settings, contracting with third-party vendors to manage PAC, and establishing networks that include high-value providers—are used by MA plans. All involve restricting, to varying degrees, beneficiary choice. Prior authorization would require beneficiaries to get approval before the program covered the care, which is not allowed under Medicare rules. Under the traditional FFS program, beneficiaries may be given information about the relative advantages of some providers or settings, but the beneficiary ultimately is free to choose a setting and provider. In addition, to implement prior authorization would require significant administrative resources to identify the settings that would require approval, develop the standards to determine coverage, and establish a process for review and appeals of decisions.
Under a third-party vendor arrangement, a benefit manager receives a monthly fee to manage (and is at financial risk for) the use of PAC. Beneficiaries may appreciate some of the education tools (such as care pathways that detail expected care through the episode) and extra assistance these vendors can provide. However, some beneficiaries may not want their PAC services influenced by an entity that is not their regular source of care. The benefits of guiding beneficiary decision making toward higher value care would need to be evaluated relative to the cost of inserting an additional administrative layer into the placement decision-making process.
A network of preferred providers would identify high-value providers, and beneficiaries who use them would incur lower cost sharing compared with beneficiaries who use out-of-network providers. In this way, freedom of choice is retained, but beneficiaries could face different financial liabilities, depending on their use of in-network or out-of-network providers. MA plans often establish formal networks, delineating where care is covered and generally excluding coverage for out-of-network care. Beneficiary freedom of choice is preserved because beneficiaries choose to enroll in an MA plan.
73
176 Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
1 Each payment system uses its own unit of payment. Skilled nursing facilities are paid on a per day basis, the home health prospective payment system pays for care in 60-day episodes, and the LTCH and IRF systems pay on a per discharge basis.
2 Summaries of the SNF and IRF PPSs are available at http://www.medpac.gov/-documents-/payment-basics.
3 Majority refers to the percentage of patients discharged to an IRF or SNF who went to SNFs. It does not consider other discharge destinations.
4 To assess whether the majority of cases were treated in SNFs, we examined shares of cases treated in each setting in markets with both types of facilities. Our reasoning is that if the majority of cases elect to go to SNFs even in markets with an IRF, the condition can generally be considered safe in the SNF. Nationwide, the number of SNFs far outnumbers the IRF count. Three-quarters of markets (defined as hospital service areas, or HSAs) do not have IRFs, but the majority of beneficiaries (69 percent) live in markets with at least one IRF. Almost all HSAs with IRFs also have at least one SNF. Because IRFs and SNFs use different case-mix classification systems, we identified comparable conditions using the MS–DRG of the preceding acute care hospital stay.
5 For each condition, we summed the daily payments for each SNF stay to compare them with the stay-based payments for IRFs. The average SNF payment excludes the separate payments for outpatient services furnished to SNF patients but excluded from the SNF PPS. Because the services must be infrequent to be excluded from the SNF daily rate, we do not think the average SNF payments would differ substantially from the payments reported here.
6 Each condition’s average SNF payment reflects the average SNF length of stay and mix of SNF case-mix groups for that condition.
7 Having a facility provide two levels of care would not be a unique policy for Medicare. Under current swing bed policies, some rural hospitals provide both acute inpatient hospital and skilled nursing facility services.
8 An industry-sponsored study examined the impact of a site-neutral policy for stroke, unilateral joint replacement, and hip and femur procedures, including a broader set of conditions (DaVanzo et al. 2014). This study modeled the President’s budget proposals for fiscal years 2014 and 2015 to narrow (but not eliminate) differences in payments between SNFs and IRFs. The proposals allow 25 percent of the difference in overhead costs between SNFs and IRFs and allows 33 percent of the difference in patient care costs. Its findings are similar to the estimates of the three conditions we examined in June 2014.
9 For beneficiaries who opt to receive outpatient therapy services, their care could be limited by the annual per beneficiary limits placed on these services.
endnotes
74

177 Repo r t t o t h e Cong r e s s : Med i ca r e Paymen t P o l i c y | Ma r ch 2015
Buntin, M. B. 2007. Access to post-acute rehabilitation. Archives of Physical Medicine and Rehabilitation 88, no. 11 (November): 1488–1493.
Buntin, M. B., C. H. Colla, P. Deb, et al. 2010. Medicare spending and outcomes after postacute care for stroke and hip fracture. Medical Care 48, no. 9 (September): 776–784.
DaVanzo, J., A. Dobson, A. El-Gamil, et al. 2014. Assessment of patient outcomes of rehabilitation care provided in inpatient rehabilitation facilities and after discharge. Vienna, VA: Dobson DaVanzo and Associates.
Dejong, G., S. D. Horn, R. J. Smout, et al. 2009a. Joint replacement rehabilitation outcomes on discharge from skilled nursing facilities and inpatient rehabilitation facilities. Archives of Physical Medicine and Rehabilitation 90, no. 8 (August): 1284–1296.
DeJong, G., W. Tian, R. J. Smout, et al. 2009b. Long-term outcomes of joint replacement rehabilitation patients discharged from skilled nursing and inpatient rehabilitation facilities. Archives of Physical Medicine and Rehabilitation 90, no. 8 (August): 1306–1316.
Deutsch, A., C. V. Granger, A. W. Heinemann, et al. 2006. Poststroke rehabilitation: Outcomes and reimbursement of inpatient rehabilitation facilities and subacute rehabilitation programs. Stroke 37, no. 6 (June): 1477–1482.
Deutsch, A., C. V. Granger, R. C. Fiedler, et al. 2005. Outcomes and reimbursement of inpatient rehabilitation facilities and subacute rehabilitation programs for Medicare beneficiaries with hip fracture. Medical Care 43, no. 9 (September): 892–901.
Gage, B., L. Smith, M. Morley, et al. 2011. Post-Acute Care Payment Reform Demonstration: Report. Prepared under contract to the Centers for Medicare & Medicaid Services. Baltimore, MD: CMS. http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Reports/Research-Reports-Items/PAC_Payment_Reform_Demo_Final.html.
Gage, B., L. Smith, L. Coots, et al. 2010. Analysis of the classification criteria for inpatient rehabilitation facilities (IRFs): Report to Congress. Prepared by RTI International for the Centers for Medicare & Medicaid Services. Baltimore, MD: CMS.
Herbold, J. A., K. Bonistall, and M. B. Walsh. 2011. Rehabilitation following total knee replacement, total hip replacement, and hip fracture: A case-controlled comparison. Journal of Geriatric Physical Therapy 34, no. 4 (October–December): 155–160.
Mallinson, T., A. Deutsch, J. Bateman, et al. 2014. Comparison of discharge functional status after rehabilitation in skilled nursing, home health, and medical rehabilitation settings for patients after hip fracture repair. Archives of Physical Medicine and Rehabilitation 95, no. 2 (February): 209–217.
Mallinson, T. R., J. Bateman, H. Y. Tseng, et al. 2011. A comparison of discharge functional status after rehabilitation in skilled nursing, home health, and medical rehabilitation settings for patients after lower-extremity joint replacement surgery. Archives of Physical Medicine and Rehabilitation 92, no. 5 (May): 712–720.
Medicare Payment Advisory Commission. 2014a. Report to the Congress: Medicare and the health care delivery system. Washington, DC: MedPAC.
Medicare Payment Advisory Commission. 2014b. Report to the Congress: Medicare payment policy. Washington, DC: MedPAC.
Medicare Payment Advisory Commission. 2013. MedPAC comment letter on the Centers for Medicare & Medicaid Services’ proposed rule entitled: Medicare Program; Inpatient Rehabilitation Facility Prospective Payment System for Federal Fiscal Year 2014; Proposed Rule. June 25.
Medicare Payment Advisory Commission. 2012. Report to the Congress: Medicare payment policy. Washington, DC: MedPAC.
Munin, M. C., K. Seligman, M. A. Dew, et al. 2005. Effect of rehabilitation site on functional recovery after hip fracture. Archives of Physical Medicine and Rehabilitation 86, no. 3 (March): 367–372.
Stineman, M. G., and L. Chan. 2009. Commentary on the comparative effectiveness of alternative settings for joint replacement rehabilitation. Archives of Physical Medicine and Rehabilitation 90, no. 8 (August): 1257–1259.
Walsh, M. B., and J. Herbold. 2006. Outcome after rehabilitation for total joint replacement at IRF and SNF: A case-controlled comparison. Archives of Physical Medicine and Rehabilitation 85, no. 1 (January): 1–5.
References
75

Medicare’s post-acute care: Trends and ways to
rationalize payments
7O n l i n e A p p e n d i x e s
76
site-neutral payments for select conditions treated in inpatient
rehabilitation facilities and skilled nursing facilities
7-AO n l i n e A p p e n d i x
77

3 Repor t to the Congress: Medicare Payment Pol icy | March 2015
Medicare’s rules regarding services furnished in iRFs and snFs
While there is overlap in the patients that skilled nursing facilities (SNF) and inpatient rehabilitation facilities (IRF) treat, the mix of services they provide differs. Compared with SNFs, IRFs have more extensive requirements regarding the amount of therapy and the frequency and level of medical supervision their patients receive. To qualify for a covered IRF stay, a beneficiary must be able to tolerate and benefit from intensive therapy, typically described as consisting of three hours of therapy a day at least five days a week. In addition, a beneficiary must require active and ongoing therapy in at least two modalities. IRFs must use a coordinated interdisciplinary team approach to care led by a physician, and the rehabilitation services must be supervised by a rehabilitation physician through face-to-face visits at least three days a week. IRFs must also meet all conditions of participation for acute care hospitals, including 24-hour nursing availability, and patients must meet medical necessity criteria.
In comparison, SNF patients generally receive less therapy. Days assigned to the highest rehabilitation (ultra-high) case-mix groups (54 percent of SNF rehabilitation days) receive 720 or more minutes a week of therapy (slightly less than 2.4 hours a day), use one therapy modality 5 days per week, and a second modality 3 days per week. Days assigned to the very high rehabilitation case-mix groups (25 percent of rehabilitation days) receive between 500 and 719 minutes of therapy a week in at least one therapy modality five days a week. Services in SNFs are not necessarily supervised by a rehabilitation physician, and registered nurses are not required to be onsite around the clock. SNFs are required to coordinate their care using interdisciplinary teams that include, but are not necessarily led by, physicians. For SNF stays to be covered by Medicare, physicians must certify at admission that the beneficiary requires daily skilled services. Recertifications, which can be conducted by nurse practitioners or physicians’ assistants, must also be done at day 14 and at least every 30 days thereafter.
IRFs must comply with the 60 percent rule, which requires that at least 60 percent of all cases an IRF admits have at least 1 of 13 conditions that CMS has determined typically require intensive rehabilitation therapy.1 The intent of the 60 percent rule is to distinguish IRF care from acute hospital care, by identifying patients who would benefit
from this intensive rehabilitation setting. Cases can qualify based on the diagnosis codes for the primary condition or certain comorbidities. Stroke, hip fracture, and a subset of joint replacement conditions are among the 13 qualifying conditions. However, most of the clinical categories are defined broadly. Of the 13 conditions, only hip and knee replacement and arthritis are defined with specific clinical factors that limit which cases count toward the 60 percent rule (e.g., counting only joint replacements for patients who are over 85 years old, are obese, or underwent bilateral procedures).
Medicare pays for patients admitted to SNFs on a per day basis. For the vast majority of days (92 percent), payments vary in large part by the amount of rehabilitation therapy a patient receives and a patient’s ability to perform activities of daily living.2 The patient classification system uses a handful of diagnoses to assign days to resource utilization groups for medically complex patients.3 There are no additional payments for facilities having a teaching program or treating low-income patients or high-cost outlier cases. Base payments to rural and urban facilities differ, and payments are adjusted for differences in wages across areas.
In contrast, for patients admitted to IRFs, Medicare pays on a per discharge basis. IRF patients are classified into case-mix groups based on the patient’s relatively broad primary reason for rehabilitation care (e.g., stroke, neurological disorder, hip fracture), age, and level of functional impairment at admission.4 Within case-mix groups, patients are further categorized into one of four payment tiers based on the presence of certain comorbidities that have been identified as increasing the cost of care.5 Payments per discharge are adjusted for the facility’s wage index and whether the facility is located in a rural area. Unlike SNFs, IRFs may also qualify for additional payments per discharge—which we refer to as “add-on payments” here—for having a teaching program, treating low-income patients, or having high-cost outlier stays.6
identifying conditions for site-neutral payments
To identify conditions that could be appropriate for site-neutral payments, we looked at conditions frequently treated in IRFs. Consistent with prior work, we used the Medicare severity–diagnosis related group (MS–DRG) of
78
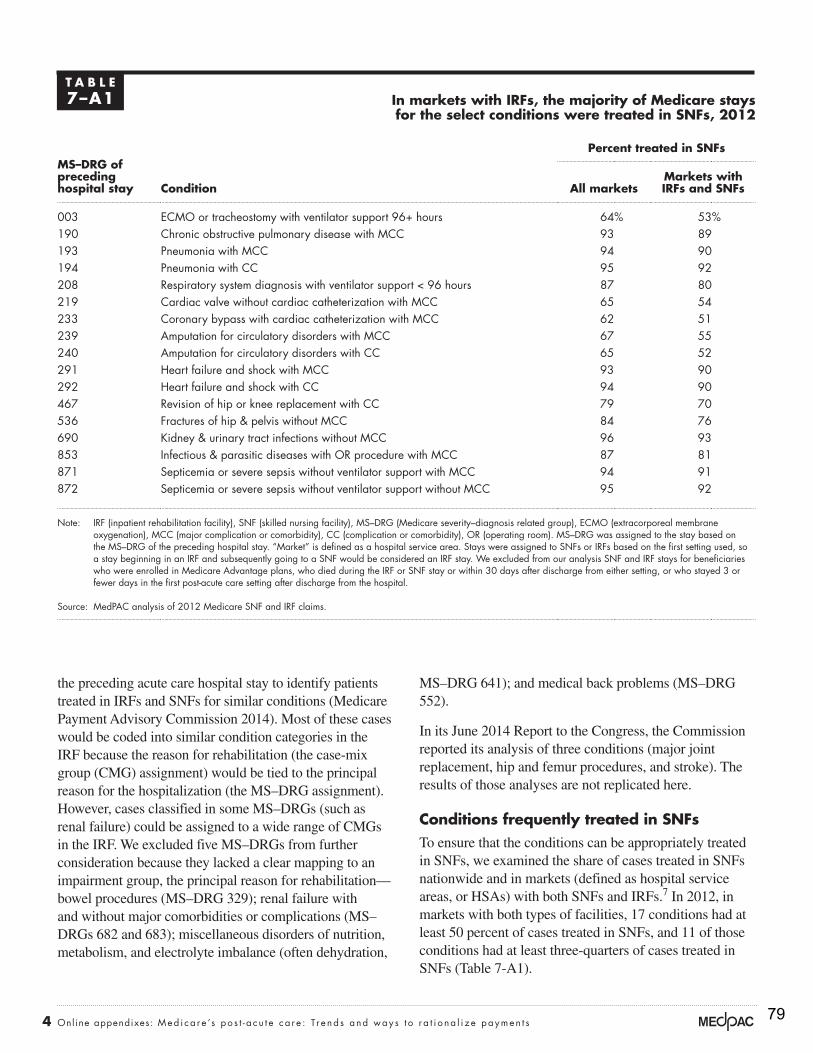
4 Online appendixes: Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
MS–DRG 641); and medical back problems (MS–DRG 552).
In its June 2014 Report to the Congress, the Commission reported its analysis of three conditions (major joint replacement, hip and femur procedures, and stroke). The results of those analyses are not replicated here.
Conditions frequently treated in snFs To ensure that the conditions can be appropriately treated in SNFs, we examined the share of cases treated in SNFs nationwide and in markets (defined as hospital service areas, or HSAs) with both SNFs and IRFs.7 In 2012, in markets with both types of facilities, 17 conditions had at least 50 percent of cases treated in SNFs, and 11 of those conditions had at least three-quarters of cases treated in SNFs (Table 7-A1).
the preceding acute care hospital stay to identify patients treated in IRFs and SNFs for similar conditions (Medicare Payment Advisory Commission 2014). Most of these cases would be coded into similar condition categories in the IRF because the reason for rehabilitation (the case-mix group (CMG) assignment) would be tied to the principal reason for the hospitalization (the MS–DRG assignment). However, cases classified in some MS–DRGs (such as renal failure) could be assigned to a wide range of CMGs in the IRF. We excluded five MS–DRGs from further consideration because they lacked a clear mapping to an impairment group, the principal reason for rehabilitation—bowel procedures (MS–DRG 329); renal failure with and without major comorbidities or complications (MS–DRGs 682 and 683); miscellaneous disorders of nutrition, metabolism, and electrolyte imbalance (often dehydration,
T A B l e7–A1 in markets with iRFs, the majority of Medicare stays
for the select conditions were treated in snFs, 2012
Ms–dRG of preceding hospital stay Condition
percent treated in snFs
All marketsMarkets with iRFs and snFs
003 ECMO or tracheostomy with ventilator support 96+ hours 64% 53%190 Chronic obstructive pulmonary disease with MCC 93 89193 Pneumonia with MCC 94 90194 Pneumonia with CC 95 92208 Respiratory system diagnosis with ventilator support < 96 hours 87 80219 Cardiac valve without cardiac catheterization with MCC 65 54233 Coronary bypass with cardiac catheterization with MCC 62 51239 Amputation for circulatory disorders with MCC 67 55240 Amputation for circulatory disorders with CC 65 52291 Heart failure and shock with MCC 93 90292 Heart failure and shock with CC 94 90467 Revision of hip or knee replacement with CC 79 70536 Fractures of hip & pelvis without MCC 84 76690 Kidney & urinary tract infections without MCC 96 93853 Infectious & parasitic diseases with OR procedure with MCC 87 81871 Septicemia or severe sepsis without ventilator support with MCC 94 91872 Septicemia or severe sepsis without ventilator support without MCC 95 92
Note: IRF (inpatient rehabilitation facility), SNF (skilled nursing facility), MS–DRG (Medicare severity–diagnosis related group), ECMO (extracorporeal membrane oxygenation), MCC (major complication or comorbidity), CC (complication or comorbidity), OR (operating room). MS–DRG was assigned to the stay based on the MS–DRG of the preceding hospital stay. “Market” is defined as a hospital service area. Stays were assigned to SNFs or IRFs based on the first setting used, so a stay beginning in an IRF and subsequently going to a SNF would be considered an IRF stay. We excluded from our analysis SNF and IRF stays for beneficiaries who were enrolled in Medicare Advantage plans, who died during the IRF or SNF stay or within 30 days after discharge from either setting, or who stayed 3 or fewer days in the first post-acute care setting after discharge from the hospital.
Source: MedPAC analysis of 2012 Medicare SNF and IRF claims.
79
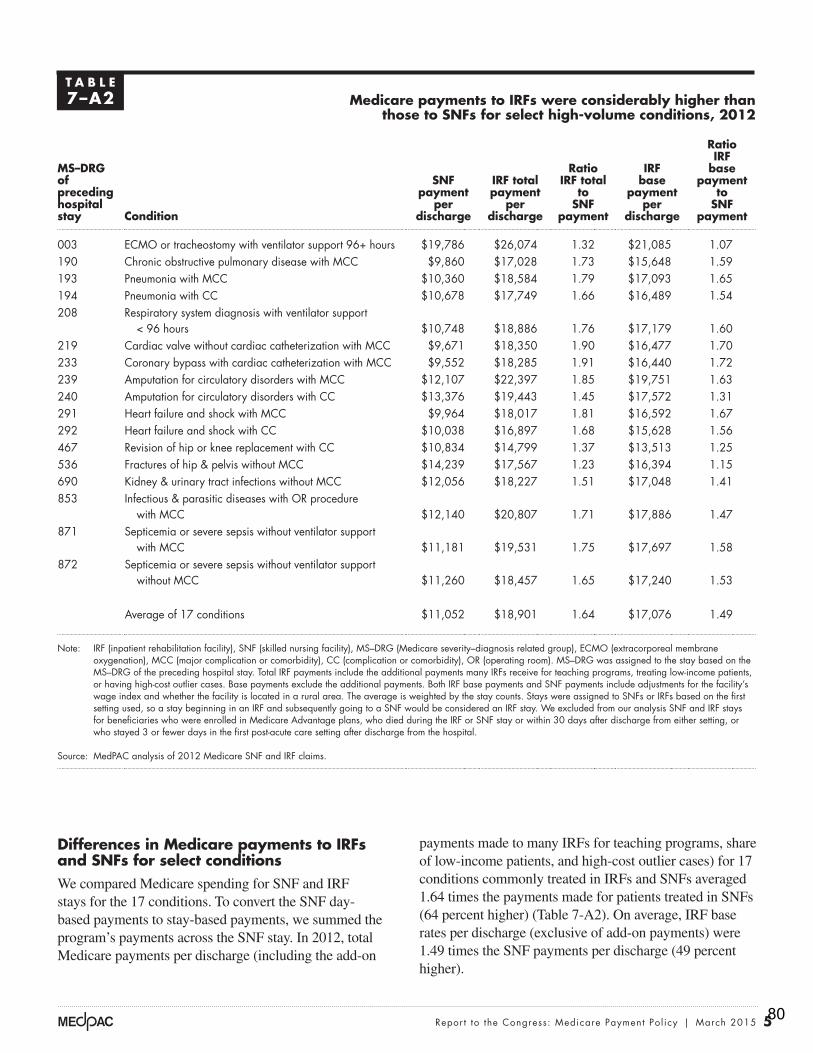
5 Repor t to the Congress: Medicare Payment Pol icy | March 2015
payments made to many IRFs for teaching programs, share of low-income patients, and high-cost outlier cases) for 17 conditions commonly treated in IRFs and SNFs averaged 1.64 times the payments made for patients treated in SNFs (64 percent higher) (Table 7-A2). On average, IRF base rates per discharge (exclusive of add-on payments) were 1.49 times the SNF payments per discharge (49 percent higher).
differences in Medicare payments to iRFs and snFs for select conditionsWe compared Medicare spending for SNF and IRF stays for the 17 conditions. To convert the SNF day-based payments to stay-based payments, we summed the program’s payments across the SNF stay. In 2012, total Medicare payments per discharge (including the add-on
T A B l e7–A2 Medicare payments to iRFs were considerably higher than
those to snFs for select high-volume conditions, 2012
Ms–dRG of preceding hospital stay Condition
snF payment
per discharge
iRF total payment
per discharge
Ratio iRF total
to snF
payment
iRF base
payment per
discharge
Ratio iRF
base payment
to snF
payment
003 ECMO or tracheostomy with ventilator support 96+ hours $19,786 $26,074 1.32 $21,085 1.07190 Chronic obstructive pulmonary disease with MCC $9,860 $17,028 1.73 $15,648 1.59193 Pneumonia with MCC $10,360 $18,584 1.79 $17,093 1.65194 Pneumonia with CC $10,678 $17,749 1.66 $16,489 1.54208 Respiratory system diagnosis with ventilator support
< 96 hours $10,748 $18,886 1.76 $17,179 1.60219 Cardiac valve without cardiac catheterization with MCC $9,671 $18,350 1.90 $16,477 1.70233 Coronary bypass with cardiac catheterization with MCC $9,552 $18,285 1.91 $16,440 1.72239 Amputation for circulatory disorders with MCC $12,107 $22,397 1.85 $19,751 1.63240 Amputation for circulatory disorders with CC $13,376 $19,443 1.45 $17,572 1.31291 Heart failure and shock with MCC $9,964 $18,017 1.81 $16,592 1.67292 Heart failure and shock with CC $10,038 $16,897 1.68 $15,628 1.56467 Revision of hip or knee replacement with CC $10,834 $14,799 1.37 $13,513 1.25536 Fractures of hip & pelvis without MCC $14,239 $17,567 1.23 $16,394 1.15690 Kidney & urinary tract infections without MCC $12,056 $18,227 1.51 $17,048 1.41853 Infectious & parasitic diseases with OR procedure
with MCC $12,140 $20,807 1.71 $17,886 1.47871 Septicemia or severe sepsis without ventilator support
with MCC $11,181 $19,531 1.75 $17,697 1.58872 Septicemia or severe sepsis without ventilator support
without MCC $11,260 $18,457 1.65 $17,240 1.53
Average of 17 conditions $11,052 $18,901 1.64 $17,076 1.49
Note: IRF (inpatient rehabilitation facility), SNF (skilled nursing facility), MS–DRG (Medicare severity–diagnosis related group), ECMO (extracorporeal membrane oxygenation), MCC (major complication or comorbidity), CC (complication or comorbidity), OR (operating room). MS–DRG was assigned to the stay based on the MS–DRG of the preceding hospital stay. Total IRF payments include the additional payments many IRFs receive for teaching programs, treating low-income patients, or having high-cost outlier cases. Base payments exclude the additional payments. Both IRF base payments and SNF payments include adjustments for the facility’s wage index and whether the facility is located in a rural area. The average is weighted by the stay counts. Stays were assigned to SNFs or IRFs based on the first setting used, so a stay beginning in an IRF and subsequently going to a SNF would be considered an IRF stay. We excluded from our analysis SNF and IRF stays for beneficiaries who were enrolled in Medicare Advantage plans, who died during the IRF or SNF stay or within 30 days after discharge from either setting, or who stayed 3 or fewer days in the first post-acute care setting after discharge from the hospital.
Source: MedPAC analysis of 2012 Medicare SNF and IRF claims.
80
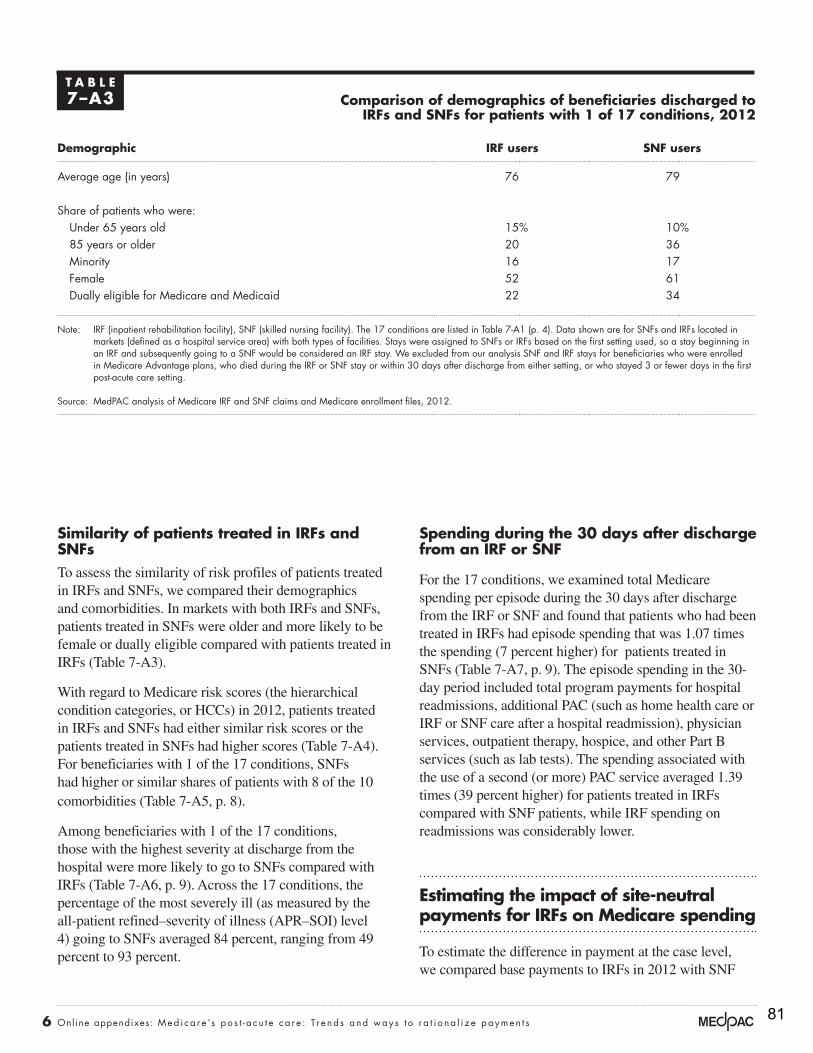
6 Online appendixes: Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
spending during the 30 days after discharge from an iRF or snF
For the 17 conditions, we examined total Medicare spending per episode during the 30 days after discharge from the IRF or SNF and found that patients who had been treated in IRFs had episode spending that was 1.07 times the spending (7 percent higher) for patients treated in SNFs (Table 7-A7, p. 9). The episode spending in the 30-day period included total program payments for hospital readmissions, additional PAC (such as home health care or IRF or SNF care after a hospital readmission), physician services, outpatient therapy, hospice, and other Part B services (such as lab tests). The spending associated with the use of a second (or more) PAC service averaged 1.39 times (39 percent higher) for patients treated in IRFs compared with SNF patients, while IRF spending on readmissions was considerably lower.
estimating the impact of site-neutral payments for iRFs on Medicare spending
To estimate the difference in payment at the case level, we compared base payments to IRFs in 2012 with SNF
similarity of patients treated in iRFs and snFsTo assess the similarity of risk profiles of patients treated in IRFs and SNFs, we compared their demographics and comorbidities. In markets with both IRFs and SNFs, patients treated in SNFs were older and more likely to be female or dually eligible compared with patients treated in IRFs (Table 7-A3).
With regard to Medicare risk scores (the hierarchical condition categories, or HCCs) in 2012, patients treated in IRFs and SNFs had either similar risk scores or the patients treated in SNFs had higher scores (Table 7-A4). For beneficiaries with 1 of the 17 conditions, SNFs had higher or similar shares of patients with 8 of the 10 comorbidities (Table 7-A5, p. 8).
Among beneficiaries with 1 of the 17 conditions, those with the highest severity at discharge from the hospital were more likely to go to SNFs compared with IRFs (Table 7-A6, p. 9). Across the 17 conditions, the percentage of the most severely ill (as measured by the all-patient refined–severity of illness (APR–SOI) level 4) going to SNFs averaged 84 percent, ranging from 49 percent to 93 percent.
T A B l e7–A3 Comparison of demographics of beneficiaries discharged to
iRFs and snFs for patients with 1 of 17 conditions, 2012
demographic iRF users snF users
Average age (in years) 76 79
Share of patients who were: Under 65 years old 15% 10%85 years or older 20 36Minority 16 17Female 52 61Dually eligible for Medicare and Medicaid 22 34
Note: IRF (inpatient rehabilitation facility), SNF (skilled nursing facility). The 17 conditions are listed in Table 7-A1 (p. 4). Data shown are for SNFs and IRFs located in markets (defined as a hospital service area) with both types of facilities. Stays were assigned to SNFs or IRFs based on the first setting used, so a stay beginning in an IRF and subsequently going to a SNF would be considered an IRF stay. We excluded from our analysis SNF and IRF stays for beneficiaries who were enrolled in Medicare Advantage plans, who died during the IRF or SNF stay or within 30 days after discharge from either setting, or who stayed 3 or fewer days in the first post-acute care setting.
Source: MedPAC analysis of Medicare IRF and SNF claims and Medicare enrollment files, 2012.
81
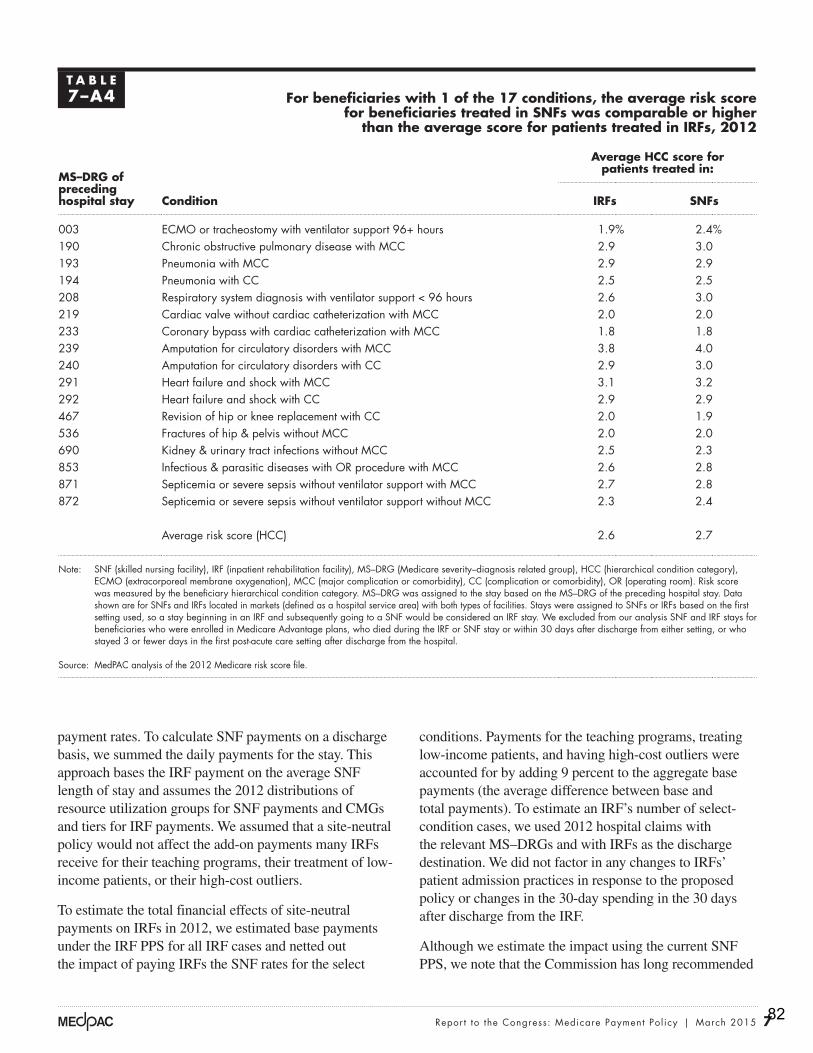
7 Repor t to the Congress: Medicare Payment Pol icy | March 2015
conditions. Payments for the teaching programs, treating low-income patients, and having high-cost outliers were accounted for by adding 9 percent to the aggregate base payments (the average difference between base and total payments). To estimate an IRF’s number of select-condition cases, we used 2012 hospital claims with the relevant MS–DRGs and with IRFs as the discharge destination. We did not factor in any changes to IRFs’ patient admission practices in response to the proposed policy or changes in the 30-day spending in the 30 days after discharge from the IRF.
Although we estimate the impact using the current SNF PPS, we note that the Commission has long recommended
payment rates. To calculate SNF payments on a discharge basis, we summed the daily payments for the stay. This approach bases the IRF payment on the average SNF length of stay and assumes the 2012 distributions of resource utilization groups for SNF payments and CMGs and tiers for IRF payments. We assumed that a site-neutral policy would not affect the add-on payments many IRFs receive for their teaching programs, their treatment of low-income patients, or their high-cost outliers.
To estimate the total financial effects of site-neutral payments on IRFs in 2012, we estimated base payments under the IRF PPS for all IRF cases and netted out the impact of paying IRFs the SNF rates for the select
T A B l e7–A4 For beneficiaries with 1 of the 17 conditions, the average risk score
for beneficiaries treated in snFs was comparable or higher than the average score for patients treated in iRFs, 2012
Ms–dRG of preceding hospital stay Condition
Average HCC score for patients treated in:
iRFs snFs
003 ECMO or tracheostomy with ventilator support 96+ hours 1.9% 2.4%190 Chronic obstructive pulmonary disease with MCC 2.9 3.0193 Pneumonia with MCC 2.9 2.9194 Pneumonia with CC 2.5 2.5208 Respiratory system diagnosis with ventilator support < 96 hours 2.6 3.0219 Cardiac valve without cardiac catheterization with MCC 2.0 2.0233 Coronary bypass with cardiac catheterization with MCC 1.8 1.8239 Amputation for circulatory disorders with MCC 3.8 4.0240 Amputation for circulatory disorders with CC 2.9 3.0291 Heart failure and shock with MCC 3.1 3.2292 Heart failure and shock with CC 2.9 2.9467 Revision of hip or knee replacement with CC 2.0 1.9536 Fractures of hip & pelvis without MCC 2.0 2.0690 Kidney & urinary tract infections without MCC 2.5 2.3853 Infectious & parasitic diseases with OR procedure with MCC 2.6 2.8871 Septicemia or severe sepsis without ventilator support with MCC 2.7 2.8872 Septicemia or severe sepsis without ventilator support without MCC 2.3 2.4
Average risk score (HCC) 2.6 2.7
Note: SNF (skilled nursing facility), IRF (inpatient rehabilitation facility), MS–DRG (Medicare severity–diagnosis related group), HCC (hierarchical condition category), ECMO (extracorporeal membrane oxygenation), MCC (major complication or comorbidity), CC (complication or comorbidity), OR (operating room). Risk score was measured by the beneficiary hierarchical condition category. MS–DRG was assigned to the stay based on the MS–DRG of the preceding hospital stay. Data shown are for SNFs and IRFs located in markets (defined as a hospital service area) with both types of facilities. Stays were assigned to SNFs or IRFs based on the first setting used, so a stay beginning in an IRF and subsequently going to a SNF would be considered an IRF stay. We excluded from our analysis SNF and IRF stays for beneficiaries who were enrolled in Medicare Advantage plans, who died during the IRF or SNF stay or within 30 days after discharge from either setting, or who stayed 3 or fewer days in the first post-acute care setting after discharge from the hospital.
Source: MedPAC analysis of the 2012 Medicare risk score file.
82

8 Online appendixes: Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
outcomes showed mixed results. To better understand the referral of stroke patients to IRFs and SNFs, the Commission undertook additional analyses. These analyses underscored the wide variation in stroke cases and practice patterns across markets. Given the lack of a clear explanation of when SNFs or IRFs are used for stroke cases, the Commission decided not to include the condition in a site-neutral policy at this time.
interviews with practitioners revealed widely varying referral patterns We interviewed 12 practitioners who treat or refer stroke patients. They included a director of a unit at a major teaching hospital dedicated to the treatment of stroke patients, an internist at the Department of Veterans Affairs who conducts research on stroke outcomes, geriatricians who direct units for elderly patients at hospitals, medical directors at nursing homes, and hospital managers who guide placement decisions. All practice in markets with IRFs. The themes we heard prompted additional data analysis on three topics: the patient’s health status (as measured by the severity of illness using the APR–SOI), the severity of the stroke, and whether IRF use was related to their occupancy rates.
that the SNF PPS be redesigned to base payments on patient characteristics and not the amount of therapy furnished to patients (Medicare Payment Advisory Commission 2008). The alternative design is more sensitive to differences in patient comorbidities and care needs compared with the current SNF PPS, offering better risk adjustment for payments. Prior Commission analysis estimated that payments under the recommended alternative PPS design for SNFs would be comparable to current payments (it is intended to be budget neutral overall), so we did not estimate these (Medicare Payment Advisory Commission 2014).
including stroke in a site-neutral policy
The Commission examined stroke for inclusion in a site-neutral policy. In June 2014, we reported that the majority of stroke cases were treated in IRFs, not the lower payment SNF setting. In addition, there were differences between the patients treated in the two settings. IRFs treated younger and less sick stroke patients, perhaps because older, sicker patients cannot always tolerate the intensive therapy required in IRFs. Our analysis of
T A B l e7–A5 For beneficiaries with 1 of the 17 conditions, snF users are more
likely to have common comorbidities compared with iRF users, 2012
share of patients with common comorbidities iRF users snF users
Share of patients with:Chronic obstructive pulmonary disease 28% 36%Congestive heart failure 33 37Diabetes without complications 19 20Heart failure and shock 18 20Major depressive, bipolar, paranoid disorders 6 12Polyneuropathy 20 17Renal failure 29 34Rheumatoid arthritis 9 8Specific heart arrhythmias 32 37Vascular disease 28 36
Note: SNF (skilled nursing facility), IRF (inpatient rehabilitation facility), HCC (hierarchical condition category). The 17 conditions are listed in Table 7-A1. Polyneuropathy is nerve damage to peripheral nerves (beyond the brain and spinal cord) and can result from uncontrolled diabetes. Data shown are for SNFs and IRFs located in markets (defined as a hospital service area) with both types of facilities. Stays were assigned to SNFs or IRFs based on the first setting used, so a stay beginning in an IRF and subsequently going to a SNF would be considered an IRF stay. We excluded from our analysis SNF and IRF stays for beneficiaries who were enrolled in Medicare Advantage plans, who died during the IRF or SNF stay or within 30 days after discharge from either setting, or who stayed 3 or fewer days in the first post-acute care setting after discharge from the hospital.
Source: MedPAC analysis of the 2012 Medicare risk score file.
83

9 Repor t to the Congress: Medicare Payment Pol icy | March 2015
T A B l e7–A6 For beneficiaries with 1 of the 17 conditions, the most severely ill
are more likely to go to snFs compared with iRFs, 2012
Ms–dRG of preceding hospital stay Condition
ApR–sOi 4 (the most severely ill)
percent treated in iRF
percent treated in snF
003 ECMO or tracheostomy with ventilator support 96+ hours 47% 53%190 Chronic obstructive pulmonary disease with MCC 12 88193 Pneumonia with MCC 11 89194 Pneumonia with CC 9 91208 Respiratory system diagnosis with ventilator support < 96 hours 20 80219 Cardiac valve without cardiac catheterization with MCC 47 53233 Coronary bypass with cardiac catheterization with MCC 51 49239 Amputation for circulatory disorders with MCC 42 58240 Amputation for circulatory disorders with CC 46 54291 Heart failure and shock with MCC 12 88292 Heart failure and shock with CC 9 91467 Revision of hip or knee replacement with CC 21 79536 Fractures of hip & pelvis without MCC 19 81690 Kidney & urinary tract infections without MCC 7 93853 Infectious & parasitic diseases with OR procedure with MCC 20 80871 Septicemia or severe sepsis without ventilator support with MCC 10 90872 Septicemia or severe sepsis without ventilator support without MCC 7 93
Weighted average of 17 conditions 16 87
Note: IRF (inpatient rehabilitation facility), SNF (skilled nursing facility), MS–DRG (Medicare severity–diagnosis related group), APR–SOI (all-patient refined–severity of illness), ECMO (extracorporeal membrane oxygenation), MCC (major complication or comorbidity), CC (complication or comorbidity), OR (operating room). Data shown are for SNFs and IRFs located in markets (defined as a hospital service area) with both types of facilities. Stays were assigned to SNFs or IRFs based on the first setting used, so a stay beginning in an IRF and subsequently going to a SNF would be considered an IRF stay. We excluded from our analysis SNF and IRF stays for beneficiaries who were enrolled in Medicare Advantage plans, who died during the IRF or SNF stay or within 30 days after discharge from either setting, or who stayed 3 or fewer days in the first post-acute care setting after discharge from the hospital.
Source: MedPAC analysis of the 2012 Medicare inpatient hospital claims.
T A B l e7–A7 Medicare spending per episode in 30 days after discharge from iRFs is
higher than stays that began in snFs for 17 conditions examined, 2012
initial stay setting
spending during 30 days after discharge from initial pAC setting
subtotal subsequent pAC Hospital readmission Other services
IRF $12,053 $6,761 $3,532 $1,760SNF $11,240 $4,852 $4,696 $1,692
Ratio IRF to SNF 1.07 1.39 0.75 1.04
Note: IRF (inpatient rehabilitation facility), SNF (skilled nursing facility), PAC (post-acute care). The 17 conditions are listed in Table 7-A1. “Other services” includes physician, outpatient therapy, and other Part B services. Stays were assigned to SNFs or IRFs based on the first setting used, so a stay beginning in an IRF and subsequently going to a SNF would be considered an IRF stay. We excluded from our analysis SNF and IRF stays for beneficiaries who were enrolled in Medicare Advantage plans, who died during the IRF or SNF stay or within 30 days after discharge from either setting, or who stayed 3 or fewer days in the first post-acute care setting after hospital discharge. Data shown are for SNFs and IRFs located in markets (defined as a hospital service area) with both types of facilities.
Source: MedPAC analysis of Medicare IRF and SNF claims, 2012.
84

10 Online appendixes: Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
to tolerate the intensive therapy required in IRFs and therefore are more likely than less severely ill beneficiaries to be treated in SNFs. This pattern of the more severely ill patients being treated in SNFs was persistent across most of the 16 comorbidities we examined.
A medical society for physical medicine and rehabilitation gave us a list of comorbidities and complexities more appropriate for placement in an IRF compared with a SNF. We found that several of these conditions (such as insulin-dependent diabetes or tracheostomy care) were infrequently treated in either setting. More common comorbidities were more likely to be treated in SNFs, though some of the differences in the shares of patients treated in SNFs and IRFs were small.
Use of iRFs and snFs for patients recovering from severe strokes
A second theme was that selection of the setting was based on the severity of the stroke. We did not have data on the severity of the stroke but examined three proxies. First, we looked at the share of patients recovering from dominant side paralysis, who are expected to have a more difficult rehabilitation (Grider 2007). Among all stroke patients, those with paralysis were more likely to be referred to IRFs (64 percent compared with 57 percent) (Table 7-A9, p. 11). However, those with dominant-side paralysis were slightly less likely to be treated in IRFs (66 percent) compared with cases with nondominant side paralysis (69 percent).
Each interviewee reported having “clear” decision-making rules about how IRFs were used; however, there was little agreement about those rules except that IRF patients needed to be able to tolerate and benefit from intensive therapy and have the potential to go home in the time frame of a typical IRF stay (two weeks). Some told us the sickest patients go to SNFs because the patients cannot tolerate intensive therapy; others told us they go to IRFs because the nursing and physician coverage was higher in that setting. Neither comorbidities nor the need for special services dictated the choice of setting. We heard that patients recovering from mild strokes could be discharged home, not needing the services of either setting (and should not count toward IRF compliance). Given the wide range in what we heard, we concluded that placement was likely to vary by the capabilities of the SNFs in the market.
Use of snFs and iRFs for severely ill stroke patients
We examined the severity of illness of patients during the hospital stay because this variation can influence placement decisions. We found that while 57 percent of stroke patients were treated in IRFs, the use of IRFs and SNFs differed by severity of illness, as measured by the APR–SOI (Table 7-A8). Across the three MS–DRGs, SNFs treated the majority (56 percent) of the most severely ill beneficiaries (APR–SOI 4), while IRFs treated the majority (56 percent) of the least severely ill (APR–SOI 1). The most severely ill patients are less likely
T A B l e7–A8 share of cases treated in snFs and iRFs by severity level,
in markets with both types of facilities, 2011
Ms–dRG of preceding hospital stay Condition
ApR–sOi 1 ApR–sOi 2 ApR–sOi 3 ApR–sOi 4
percent treated
in iRF
percent treated
in snF
percent treated
in iRF
percent treated
in snF
percent treated
in iRF
percent treated
in snF
percent treated
in iRF
percent treated
in snF
64 Stroke with MCC 56% 44% 58% 42% 48% 52% 40% 60%65 Stroke with CC 56 44 67 33 54 46 44 5666 Stroke, no CC/MCC 68 32 63 37 52 48 0 0
Total 56 44 67 33 54 46 44 56
Note: SNF (skilled nursing facility), IRF (inpatient rehabilitation facility), APR–SOI (all-patient refined–severity of illness), CC (complication or comorbidity), MCC (major complication or comorbidity). APR–SOI is a measure of patient severity of illness. Patients in APR–SOI 1 are the least severely ill; patients in APR–SOI 4 are the most severely ill. “Market” is defined as a hospital service area.
Source: MedPAC analysis of 2011 hospital claims.
85
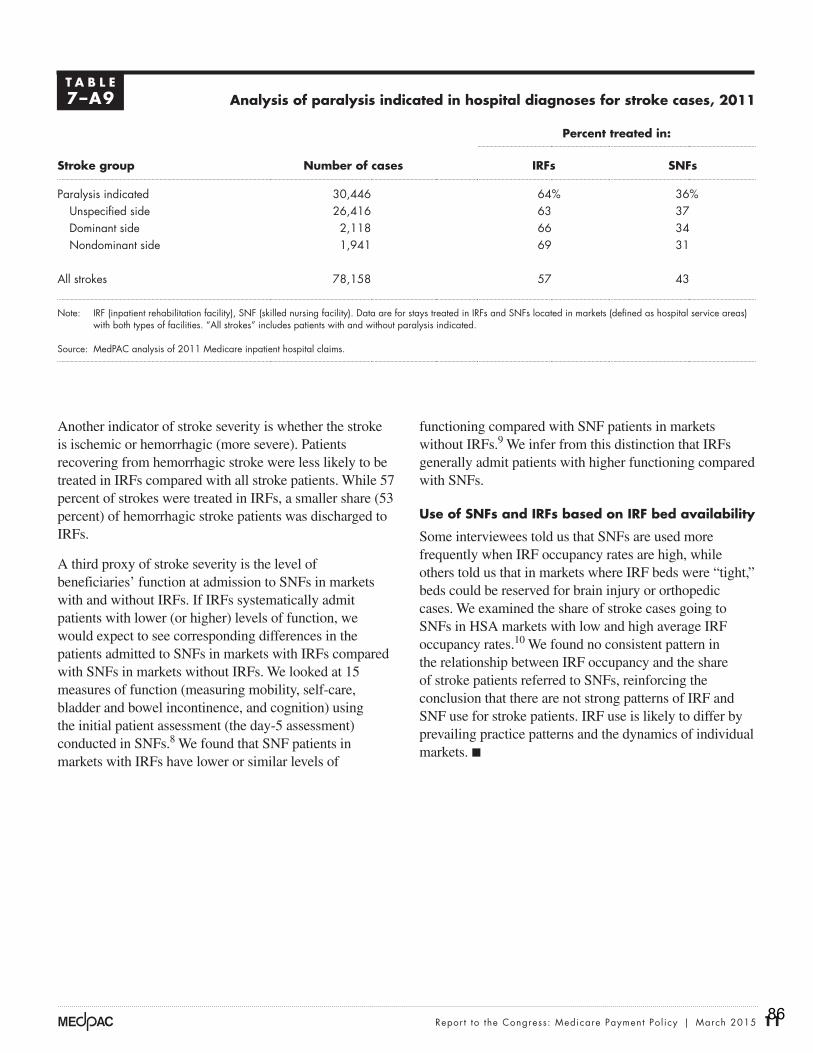
11 Repor t to the Congress: Medicare Payment Pol icy | March 2015
functioning compared with SNF patients in markets without IRFs.9 We infer from this distinction that IRFs generally admit patients with higher functioning compared with SNFs.
Use of snFs and iRFs based on iRF bed availability
Some interviewees told us that SNFs are used more frequently when IRF occupancy rates are high, while others told us that in markets where IRF beds were “tight,” beds could be reserved for brain injury or orthopedic cases. We examined the share of stroke cases going to SNFs in HSA markets with low and high average IRF occupancy rates.10 We found no consistent pattern in the relationship between IRF occupancy and the share of stroke patients referred to SNFs, reinforcing the conclusion that there are not strong patterns of IRF and SNF use for stroke patients. IRF use is likely to differ by prevailing practice patterns and the dynamics of individual markets. ■
Another indicator of stroke severity is whether the stroke is ischemic or hemorrhagic (more severe). Patients recovering from hemorrhagic stroke were less likely to be treated in IRFs compared with all stroke patients. While 57 percent of strokes were treated in IRFs, a smaller share (53 percent) of hemorrhagic stroke patients was discharged to IRFs.
A third proxy of stroke severity is the level of beneficiaries’ function at admission to SNFs in markets with and without IRFs. If IRFs systematically admit patients with lower (or higher) levels of function, we would expect to see corresponding differences in the patients admitted to SNFs in markets with IRFs compared with SNFs in markets without IRFs. We looked at 15 measures of function (measuring mobility, self-care, bladder and bowel incontinence, and cognition) using the initial patient assessment (the day-5 assessment) conducted in SNFs.8 We found that SNF patients in markets with IRFs have lower or similar levels of
T A B l e7–A9 Analysis of paralysis indicated in hospital diagnoses for stroke cases, 2011
stroke group number of cases
percent treated in:
iRFs snFs
Paralysis indicated 30,446 64% 36%Unspecified side 26,416 63 37Dominant side 2,118 66 34Nondominant side 1,941 69 31
All strokes 78,158 57 43
Note: IRF (inpatient rehabilitation facility), SNF (skilled nursing facility). Data are for stays treated in IRFs and SNFs located in markets (defined as hospital service areas) with both types of facilities. “All strokes” includes patients with and without paralysis indicated.
Source: MedPAC analysis of 2011 Medicare inpatient hospital claims.
86
12 Online appendixes: Med i ca r e ’s po s t - a c u t e ca r e : Tr e nd s and way s t o r a t i o na l i z e paymen t s
1 The 13 qualifying conditions are stroke; spinal cord injury; congenital deformity; amputation; major multiple trauma; hip fracture; brain injury; neurological disorders; burns; three arthritis conditions for which appropriate, aggressive, and sustained outpatient therapy has failed; and hip or knee replacement when bilateral, when body mass index is 50 or more, or when the patient is age 85 or older.
2 For more information, see the Commission’s SNF Payment Basics document at http://medpac.gov/documents/payment-basics/skilled-nursing-facility-services-payment-system-14.pdf?sfvrsn=0.
3 Days assigned to a case-mix group that considers diagnoses or special service use (such as ventilator or tracheostomy care) account for less than 10 percent of SNF days.
4 There are five special case-mix groups for patients discharged before the fourth day (short-stay outliers) and for those few who die during their stay.
5 The first and highest paid tier includes codes for comorbidities associated with renal dialysis, tracheostomy, and paralysis of vocal cords. The codes in the second tier are related to difficulty swallowing and certain infections. The third tier includes a variety of comorbidities associated with more than 900 ICD–9–CM codes, including paralysis, pneumonia, morbid obesity, and a range of infections. The fourth tier is for patients with no comorbidities associated with higher costs of care.
6 For more information, see the Commission’s IRF Payment Basics document at http://medpac.gov/documents/payment-basics/inpatient-rehabilitation-facilities-payment-system-14.pdf?sfvrsn=0.
7 Nationwide, the number of SNFs far outnumbers the IRF count. Three-quarters of markets (defined as hospital service areas, or HSAs) do not have IRFs, but the majority of beneficiaries (69 percent) live in markets with at least one IRF. Almost all HSAs with IRFs also have at least one SNF. To assess whether the majority of cases are treated in SNFs, we examined shares of cases treated in each setting in markets with both types of facilities. Our reasoning is that if the majority of cases elect to go to SNFs, even in markets with an IRF, then the condition can generally be considered safe in the SNF.
8 The measures include the Barthel score, bowel incontinence, bladder incontinence, locomotion, bed mobility, transfer support, walking, hygiene, toileting, bathing, dressing, eating, short-term memory, making self understood, and cognitive skills for decision making.
9 Patients treated in SNFs in markets with IRFs had lower functioning for the measures of incontinence, instruments of activities of daily living, and cognition, while the measures of mobility were comparable.
10 To calculate the average IRF occupancy rate in the HSA, we weighted each IRF’s occupancy rate by its bed count.
endnotes
87

13 Repor t to the Congress: Medicare Payment Pol icy | March 2015
Grider, D. 2007. Roadmap to ICD-10-CM: Understanding the ICD-10-CM draft guidelines for diseases of the nervous system. http://djk9qtinkh46n.cloudfront.net/ppdf/ICD-10-February-20071.pdf.
Medicare Payment Advisory Commission. 2014. Report to the Congress: Medicare and the health care delivery system. Washington, DC: MedPAC.
Medicare Payment Advisory Commission. 2008. Report to the Congress: Reforming the delivery system. Washington, DC: MedPAC.
References
88
April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Robert Walters, Chair, Inpatient Rehabilitation and Therapy Services Forum SUBJECT: Report of Forum Activities SUMMARY
The Inpatient Rehabilitation and Therapy Services Forum provides input into the work of the Center and advises CHA leadership on issues of concern to providers of inpatient rehabilitation facilities and therapy services.
Robert Walters chairs the Inpatient Rehabilitation and Therapy Services Forum and represents the forum on the advisory board of the Center for Post-Acute Care.
ACTION REQUESTED To provide attendees an update regarding issues impacting inpatient rehabilitation
facilities (IRFs) and therapy services.
DISCUSSION
A. IRF/SNF Site-Neutral Payment The Medicare Payment Advisory Commission (MedPAC) continues to consider investigate post-acute care payment reform, including specific proposals for the development and implementation of site-neutral payment for certain patients cared for in skilled nursing facilities (SNFs) and inpatient rehabilitation facilities (IRFs). Under these proposals, payments to IRFs would be modified to levels consistent with those paid to SNFs, for individuals who have certain diagnoses. CHA successfully advocated that IRF/SNF site-neutral not be included in recent SGR legislation.
89

Report of Forum Activities- Inpatient Rehabilitation and Therapy Services Forum April 14, 2015
Page 2
B. Durable Medical Equipment
CHA continued its work to address member concerns regarding the ability of hospitals to obtain medically necessary durable medical equipment (DME) since the initiation of the CMS Competitive Bidding Program for the durable medical equipment prosthetics, orthotics and supplies (DMEPOS). CHA is engaged in ongoing communication with CMS Region IX personnel on this issue.
C. Managed Medicare Authorization
Several CHA member IRFs reported that they encounter difficulty obtaining authorizations for admission to inpatient rehabilitation from Medicare Advantage (MA) plans, even in cases where a patient/beneficiary clearly meets Medicare criteria for IRF services. CHA staff members Blaisdell and Keefe initiated communication on this issue with personnel at Region IX of the Centers for Medicare & Medicaid Services (CMS) and requested clarification of MA criteria and obligations, as well as information regarding how to proceed when services are denied. CHA Staff requested additional information and support from CMS regional personnel on this issue. Regulatory information and resources for problem solving were provided to members.
Attachment MA IRF memo
90
Date: March 9, 2015 TO: Center for Post-Acute Care Inpatient Rehabilitation & Therapy Services Forum FROM: Pat Blaisdell, Vice President SUBJECT: Managed Medicare/Medicare Advantage (MA) Authorizations for IRF Background A number of IRF members have reported that they encounter difficulty obtaining authorizations for admission to inpatient rehabilitation from Medicare Advantage (MA) plans, even in cases where a patient/beneficiary clearly meets Medicare criteria for IRF services. Members have requested clarification of MA criteria and obligations, as well as information regarding how to proceed when services are denied. CHA Staff requested additional information and support from CMS regional personnel on this issue. Coverage Requirements The Medicare Managed Care Manual, available at the link below, provides information regarding the rights of Medicare beneficiaries who enroll in MA plans as well as plan responsibilities of the plans. For example: The following requirements apply with respect to the rule that MAOs must cover the costs of Original Medicare benefits:
• Benefits: MA plans must provide or pay for medically necessary Part A (for those entitled) and Part B covered items and services. • Access: MA enrollees must have access to all medically necessary Parts A and B services. However, MA plans are not required to provide MA enrollees the same access to providers that is provided under Original Medicare.
http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs-Items/CMS019326.html?DLPage=2&DLSort=0&DLSortDir=ascending Appeal rights MA Appeals Process In instances where authorization is denied, beneficiaries have the right to appeal the decision to the plan. Additional information on the appeal process is available the following link: http://www.hhs.gov/omha/process/level1/l1_c.html. Plans must respond to an appeal for expedited review process within 72 hours. If the plan upholds the denial, an automatic independent review entity (IRE) must review within 72 hours. QIO Review Process Individuals who are receiving services in an inpatient hospital, skilled nursing facility, home
91

health agency or comprehensive rehabilitation facility, you may request an immediate review by a Quality Improvement Organization. This issue was discussed during a recent meeting with representatives of CMS Region IX. Please see Q & A below.
CHA Question: Does the QIO review appeal requests when the Medicare Advantage (MA) beneficiary is being discharged from an acute inpatient setting and would like to go into an acute rehab facility; however their MA plan is sending the MA beneficiary to get rehab at a lower level of care such as to a SNF? CMS: Under the above circumstance, CMS encourages the attending physician to work directly with the MA plan on discharge planning. If the attending physician prescribes inpatient acute rehab, and where the MA plan wants to send the patient to get rehab at a lower level of care such as a SNF, the MA plan must obtain concurrence from the physician before discharge.
§422.620 (d) (d) Physician concurrence required. Before discharging an enrollee from the inpatient hospital level of care, the MA organization must obtain concurrence from the physician who is responsible for the enrollee's inpatient care. §422.622 (a) Enrollee's right to an immediate QIO review. An enrollee has a right to request an immediate review by the QIO when an MA organization or hospital (acting directly or through its utilization committee), with physician concurrence determines that inpatient care is no longer necessary.
Once the discharge plan is in place, and the plan is to transfer the patient to acute inpatient rehabilitation – the transfer is considered acute to acute and the notice/QIO appeal process does not apply. If on the other hand, the discharge is to a skilled facility for continue care and rehab, then the beneficiary must be given proper notice/QIO appeal process does apply. The QIO will conduct these types of appeals anytime the beneficiary or their representative disputes the established discharge disposition.
92
April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Walter Hekimian, Chair, Skilled Nursing and Subacute Care Services Forum SUBJECT: Report of Forum Activities SUMMARY
The Skilled Nursing and Subacute Care Services Forum provides for member input into the work of the Center and advises CHA leadership on issues of concern to providers of hospital-based skilled nursing facilities and subacute care units.
Walter Hekimian chairs the Skilled Nursing and Subacute Care Services Forum and represents the forum on the advisory board of the Center for Post-Acute Care.
ACTION REQUESTED To provide attendees an update regarding issues impacting hospital-based skilled nursing
units and subacute care units.
DISCUSSION A. DP/SNF Medi-Cal Rate Reductions CHA continues to advocate for the elimination of the “clawback,” or retroactive recoupment of reimbursement for services provided by distinct part skilled nursing facilities for the time period from June 1, 2011 to September 30, 2013 (August 31, 2013 for rural facilities). CHA leadership is engaged in direct discussions with HHS/DHCS. At present, DHCS indicates that it plans to proceed with implementation of recoupment in late May. Recoupment will reportedly be initiated via a 5% withhold on future check writes. Facilities will receive notification prior to the beginning of recoupment, and will be able to request alternative payment arrangements.
93

Report of Forum Activities – Skilled Nursing and Subacute Care Services Forum April 14, 2015
Page 2
B. IRF/SNF Site-Neutral Payment The Medicare Payment Advisory Commission (MedPAC) continues to consider investigate post-acute care payment reform, including specific proposals for the development and implementation of site-neutral payment for certain patients cared for in skilled nursing facilities (SNFs) and inpatient rehabilitation facilities (IRFs). Under these proposals, payments to IRFs would be modified to levels consistent with those paid to SNFs, for individuals who have certain diagnoses. CHA successfully advocated that IRF/SNF site-neutral not be included in recent SGR legislation. C. ePOC The California Department of Public Health (CDPH) is initiating an electronic plan of correction (ePOC) for SNF surveys. CHA is working with CDPH to preview training materials and will provide support for education and training. D. PASRR The California Department of Health Care Services (DHCS) has requested CHA participation in its efforts to improve the timeliness and completion of the Pre-Admission Screening and Resident Review (PASSR), as mandated by CMS. A PASSR is required for all individuals admitted to a skilled nursing facility to determine the presence of a mental illness or developmental disability and the need for additional resources or services. E. CCI The Department of Health Care Services (DHCS) has released all plan letter (APL) 15-004. The letter clarifies the responsibilities of Medi-Cal managed care health plans to provide coverage of nursing facility services under the Coordinated Care Initiative for beneficiaries who are not enrolled in Cal MediConnect. The APL includes information on payment rates and policies, timelines and continuity of care.
F. CMS 5-Star Program The Centers for Medicare & Medicaid Services (CMS) announced changes to the five-star quality rating system for skilled-nursing facilities (SNFs), effective Feb. 20, 2016. According to CMS, the goals of the changes are to provide more precise and meaningful quality information.
Attachment APL 15-004
94
State of California—Health and Human Services Agency Department of Health Care Services
JENNIFER KENT EDMUND G. BROWN JR. DIRECTOR GOVERNOR
DATE: February 12, 2015 ALL PLAN LETTER 15-004
TO: ALL MEDI-CAL MANAGED CARE HEALTH PLANS SUBJECT: MEDI-CAL MANAGED CARE HEALTH PLAN REQUIREMENTS FOR
NURSING FACILITY SERVICES IN COORDINATED CARE INITIATIVE COUNTIES FOR BENEFICIARIES NOT ENROLLED IN CAL MEDICONNECT
PURPOSE: The purpose of this All Plan Letter (APL) is to clarify the responsibilities of Medi-Cal managed care health plans (MCPs) to provide coverage of nursing facility (NF) services as required under the Coordinated Care Initiative (CCI) for MCP beneficiaries in CCI counties who are not enrolled in the Duals Demonstration Project, herein referred to as Cal MediConnect. BACKGROUND: In January 2012, Governor Brown announced his intent to enhance health outcomes and beneficiary satisfaction for low-income Seniors and Persons with Disabilities by shifting service delivery away from institutional care to home and community-based settings. To implement that goal, Governor Brown enacted the CCI by signing Senate Bill (SB) 1008 (Chapter 33, Statutes of 2012), SB 1036 (Chapter 45, Statutes of 2012), and SB 94 (Chapter 37, Statutes of 2013). One component of the CCI is the provision of Long Term Services and Supports (LTSS), including NF services, by MCPs in CCI counties. REQUIREMENTS: The Department of Health Care Services (DHCS) is issuing this guidance, and requesting resubmission of certain MCP Policies and Procedures (P&Ps), in recognition that there will continue to be an ongoing need to ensure MCP readiness as well as a smooth implementation of the CCI and the transition of critical NF services to MCPs. PROVIDER CONTRACTS: MCP contracts with providers shall comply with all applicable CCI requirements. PROMPT PAYMENT AND ELECTRONIC CLAIMS: MCPs shall pay providers, including institutional providers, in accordance with the prompt payment provisions contained in each MCP’s contract with DHCS, including the
Managed Care Quality and Monitoring Division
Managed Care Operations Division 1501 Capitol Avenue, P.O. Box 997413, MS 4400
Sacramento, CA 95899-7413 Phone (916) 449-5000 Fax (916) 449-5005
www.dhcs.ca.gov 95

ALL PLAN LETTER 15-004 Page 2 ability to accept and pay electronic claims. This requirement is established under Welfare and Institutions Code (W&I) Section 14186.3(c)(5) that applies to NF services provided through MCPs in CCI counties. For NF services provided through MCPs in CCI counties, MCPs shall pay 90 percent of all clean claims from contracted NF service providers within 30 calendar days after the date of receipt of the claim, and 99 percent of all clean claims within 90 calendar days, unless the contracted provider and MCP have agreed in writing to a faster alternate payment schedule. The date of receipt shall be the date the MCP receives the claim, as indicated by its date stamp on the claim. The date of payment shall be the date of the check or other form of payment. MCPs shall also pay all claims submitted by contracted NF service providers in accordance with Health and Safety Code (H&S) Sections 1371 – 1371.39 if:
1) The timeline provided by these sections is less than the timeline provided above; and
2) The contracted provider and MCP have not agreed in writing to a faster alternate payment schedule.
MCPs shall pay non-contracted provider claims in accordance with H&S Sections 1371–1371.39 and/or other applicable laws and regulations. An MCP shall be subject to any remedies, including interest payments, provided for in these sections if the MCP fails to meet the standards specified in these sections. For NF services provided through MCPs in CCI counties, if the submitting provider requests electronic processing, the MCP shall accept the submission of electronic claims and pay claims electronically. REIMBURSEMENT FOR MEDI-CAL NF SERVICES: For Medi-Cal NF services provided through MCPs in CCI counties, MCPs shall reimburse providers at rates that are not less than Medi-Cal Fee-for-Service (FFS) rates, as published and revised by DHCS, including retroactive payment of any additional rate increment based on DHCS retroactive rate adjustments, for equivalent services for the date(s) of service. LEAVE OF ABSENCE AND BEDHOLDS: Pursuant to W&I Code Section 14186.1(c)(4), for NF services provided through MCPs in CCI counties, MCPs shall include as a covered benefit any leave of absence or bedhold
96

ALL PLAN LETTER 15-004 Page 3 that a NF provides in accordance with the requirements of Title 22, California Code of Regulations (CCR), Section 72520 or California’s Medicaid State Plan.1 Medi-Cal requirements for bedhold and leave of absence are detailed in Title 22, CCR, Sections 51535 and 51535.1. MEDICARE COINSURANCE AND DEDUCTIBLES: For long term care (LTC) services, MCPs shall pay the full Medicare coinsurance and deductibles. Please see APL 13-0032 for more information about this requirement. MEDI-CAL SHARE OF COST: MCPs shall process claims submitted by NFs consistent with Medi-Cal guidelines for share of cost (SOC), as outlined in the Medi-Cal Long-Term Care Provider Manual.3 When a Medi-Cal beneficiary has an LTC aid code and an SOC, an NF will subtract the SOC that is paid or obligated to be paid from the claim amount. The MCP shall pay the balance. In addition, as required by the Johnson v. Rank settlement agreement, if a beneficiary spends part of the SOC on “non-covered” medical services or remedial services or items, the NF will subtract those amounts from the beneficiary’s SOC. The NF will adjust the amount on the claim, and the MCP shall pay the balance. As a result of the Johnson v. Rank lawsuit, Medi-Cal beneficiaries, not their providers, can elect to use the SOC funds to pay for necessary, non-covered, medical or remedial-care services, supplies, equipment, and drugs (medical services) that are prescribed by a physician and part of the plan of care authorized by the beneficiary’s attending physician. The physician’s prescriptions for SOC expenditures must be maintained in the beneficiary’s medical record. A “medical service” is considered a non-covered benefit if either of the following is true:
1) The medical service is rendered by a non-Medi-Cal provider; or
2) The medical service falls into the category of services for which an authorization request must be submitted and approved before Medi-Cal (DHCS or the MCP) will pay, and either an authorization request is not submitted or an authorization
1 The California State Plan can be accessed at the following link: http://www.dhcs.ca.gov/formsandpubs/laws/Pages/CaliforniStatePlan.aspx 2APL 13-003 can be accessed at the following link: http://www.dhcs.ca.gov/formsandpubs/Documents/MMCDAPLsandPolicyLetters/APL2013/APL13-003.pdf. 3 DHCS guidelines regarding Johnson v. Rank requirements, and additional SOC requirements that are not listed in this APL, are available in the Medi-Cal Provider Manual at the following links: http://files.medi-cal.ca.gov/pubsdoco/publications/masters-mtp/part2/shareltc_l00.doc. http://files.medi-cal.ca.gov/pubsdoco/publications/masters-mtp/part1/share_z01.doc.
97
ALL PLAN LETTER 15-004 Page 4
request is submitted but is denied by Medi-Cal (DHCS or the MCP) because the service is not considered medically necessary.
CONTINUITY OF CARE: MCPs must provide continuity of care with an out-of-network provider, including NF service providers, for up to 12 months when:
1) The MCP is able to determine that the beneficiary has an ongoing relationship with the provider (self-attestation is not sufficient to provide proof of a relationship with a provider). An existing relationship means the beneficiary has resided in an out-of-network NF at least once during the 12 months prior to the date of his or her initial enrollment in the MCP, unless otherwise specified in this APL;
2) The provider is willing to accept the higher of the MCP’s contract rates or Medi-Cal FFS rates; and
3) The provider meets the MCP’s applicable professional standards and has no disqualifying quality-of-care issues (W&I Code Section 14182.17 and APL 13-023).4
If a beneficiary was residing in an out-of-network skilled nursing facility (SNF) when the beneficiary transitioned into the MCP, the MCP shall offer the beneficiary the opportunity to return to the out-of-network SNF after a medically necessary absence, such as a hospital admission, for the duration of Cal MediConnect. This requirement does not apply if the beneficiary is discharged from the SNF into the community or a lower level of care. For more information regarding provider continuity of care requirements that apply to beneficiaries receiving NF services, including a definition of “quality-of-care issues” and methods to verify an ongoing provider relationship, please see APL13-023.5 In addition to the requirements in APL 14-021,6 the following requirements apply:
1) MCPs in CCI counties shall maintain continuity of care by recognizing any treatment authorizations made by DHCS for NF services that were in effect when the beneficiary enrolled into the MCP. MCPs shall honor such treatment authorizations for 12 months or for the duration of the treatment authorization if
4 APL 14-021 can be accessed at the following link: http://www.dhcs.ca.gov/formsandpubs/Documents/MMCDAPLsandPolicyLetters/APL2014/APL14-021.pdf. 5 See link above 6 See link above
98

ALL PLAN LETTER 15-004 Page 5
the remaining authorized duration is less than 12 months, following enrollment of a beneficiary into the MCP; and
2) A beneficiary who is a resident of an NF prior to enrollment will not be required to change NFs during the duration of Cal MediConnect if the facility is licensed by the California Department of Public Health, meets acceptable quality standards, and the facility and MCP agree to Medi-Cal rates in accordance with the MCP contract with DHCS. This provision is automatic (a beneficiary does not have to make a request to the MCP to invoke this provision).
CHANGE IN BENEFICIARY’S CONDITION AND DISCHARGE: W&I Code Section 14186.3(c)(4) applies to NF services provided through MCPs in CCI counties. Pursuant to this section, an NF may modify its care of a beneficiary or discharge the beneficiary if the NF determines that the following specified circumstances are present:
1) The NF is no longer capable of meeting the beneficiary’s health care needs;
2) The beneficiary’s health has improved sufficiently so that he or she no longer needs NF services; or
3) The beneficiary poses a risk to the health or safety of individuals in the NF.
The MCP may request documentation from the NF to verify that the facility’s care modification was made for the allowable reasons noted above. When these circumstances are present, the MCP shall arrange and coordinate a discharge of the beneficiary and continue to pay the NF the applicable rate until the beneficiary is successfully discharged and transitioned into an appropriate setting. NFs retain current responsibility for discharge planning. The MCP may also arrange and coordinate a discharge of the beneficiary if the MCP determines that one, or more, of the three circumstances noted above are present, or if the facility does not meet the MCP’s network standards because of documented quality of care concerns. AUTHORIZATION OF MEDI-CAL SERVICES: W&I Code Section 14186.3(c)(2) applies to NF services provided through MCPs in CCI counties. Pursuant to this section, MCPs shall authorize utilization of NF services for their beneficiaries when medically necessary. The MCP shall maintain standards for determining levels of care and authorizing services for Medi-Cal services that are consistent with policies established by the federal Centers for Medicare and Medicaid
99
ALL PLAN LETTER 15-004 Page 6 Services (CMS) and with the criteria for authorizing Medi-Cal services specified in Title 22, CCR, Section 51003. DELEGATION OVERSIGHT: MCPs are responsible for ensuring that delegates comply with all applicable state and federal laws and regulations and other contract requirements and DHCS guidance, including APLs. MONITORING: DHCS will closely monitor beneficiary access to Medi-Cal NF services and quality outcomes. DHCS will enforce appropriate prime plan oversight of delegate compliance with the prime plan’s policies and procedures. DHCS also monitors quality through regular MCP submission of DHCS-specified health care service quality data. For additional information about this APL, please contact your Managed Care Operations Division contract manager. Sincerely, Original Signed by Sarah C. Brooks Sarah Brooks, Chief Managed Care Quality and Monitoring Division Department of Health Care Services
100
April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Linda Glomp, Home Health and Hospice Forum SUBJECT: Report of Forum Activities SUMMARY
The Home Health and Hospice Forum provides for member input into the work of the Center and to advise CHA leadership on issues of concern to providers of home health and hospice services and agencies operated by or affiliated with CHA member hospitals.
Linda Glomp chairs the Home Health and Hospice forum and represents the forum on the advisory board of the Center for Post-Acute Care.
ACTION REQUESTED To provide attendees an update regarding issues impacting home health agencies and
hospices.
DISCUSSION A. Home Health 5- Star Program The Centers for Medicare & Medicaid Services (CMS) has finalized the methodology for a star ratings program to be added to the Home Health Compare (HHC) website. HHC star ratings will be published beginning in July, and preview reports will be available to providers in late March or early April.
B. Face to Face Certification Requirements
Requirements for face-to-face certification requirements were modified effective January 1, 2015, under the provision of the home health prospective payment system (HH PPS) final rule.
101

Report of Forum Activities- Home Health and Hospice Forum April 14, 2015
Page 2
Members report continued difficulties with identifying and developing compliant practices, especially in coordination with physicians. CHA is in communication with Noridian, the Medicare Administrative Contractor (MAC) for clarification and additional information.
102
April 14, 2015 TO: Center for Post-Acute Care Advisory Board FROM: Patricia Blaisdell, Vice President, Continuum of Care SUBJECT: Post-Acute Care Issues SUMMARY The CHA Center for Post-Acute Care provides an opportunity to share and discuss issues of significance to post-acute care providers and hospitals. ACTION REQUESTED To provide an opportunity for review and discussion of emerging issues and perspectives
regarding post-acute care services. DISCUSSION As health care reform proceeds, there is increasing interest in the role of post-acute care in achieving optimal patient outcome and controlling costs. In addition, increasing utilization of post-acute care services and associated growth in spending has resulted in greater scrutiny on the role and use of post-acute care services in the continuum of care. Attachment KaufmanHall Report
103
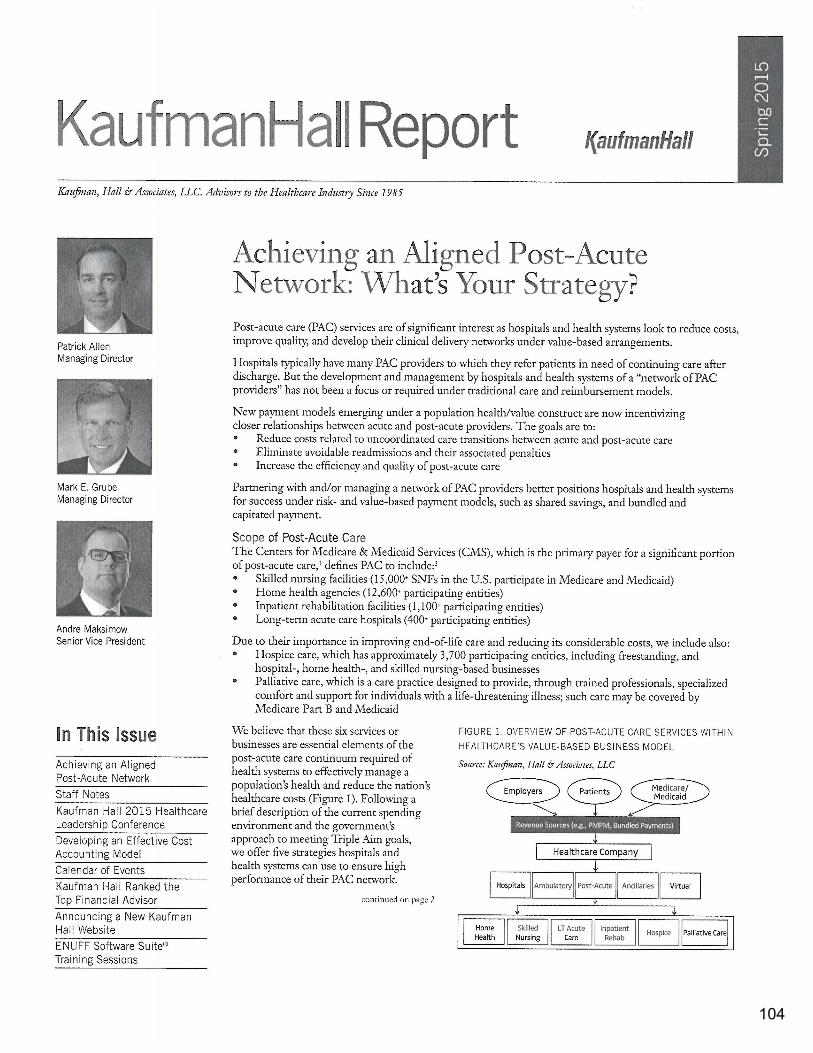
104
105

106

107

108