cellular physiology of skeletal, cardiac, and smooth · pdf filecellular physiology of...
TRANSCRIPT

~~~
Cellular Physiologyof Skeletal, Cardiac,and Smooth Muscle
~~~
\.fLLS
~
of each of the types df muscleto facilitate communication between
takes the form of the postsynap-junction. Neuromuscular junctions (i.e..
in cardiac and smooth muscle. Intransmission does not initiate contraction; it
. neuromuscular
cardiac
important
~

~
Branched structure of cardiac muscle
Actin
FIGURE 9- 1. Electrical coupling of cardiac myocytes.
Skeletal Muscle Contracts in Response toNeuromuscular Synaptic TransmissionThe mature skeletal muscle cell has a single neuromuscu-lar junction where acetylcholine (ACh) receptors are con-centrated (p. 209). A single muscle cell responds to onlya single neuron. However, a single neuronal axon maybifurcate to innervate several individual muscle cells. Thegroup of muscle cells innervated by a single neuron isreferred to as a motor unit.
The neuromuscular junction is the focus of Chapter 8.Briefly, the ACh released by the presynaptic nerve termi-nal binds to inotropic (nicotinic) ACh receptors at theneuromuscular junction. These receptors are nonselectivecation channels that open when ACh binds to a specificsite on the channel, and a depolarizatlen known as theend-plate potential is produced. If this end-plate poten-tial exceeds the threshold for activating Na+ channels, anaction potential results. Generation of an action potentialinitiates the sequence of processes leading to contraction.The ACh is rapidly inactivated by acetylcholinesterase, anenzyme that is manufactured by the muscle cell, andmuscle contraction stops a few milliseconds after neuronalactivity ceases.
Cardiac Muscle Contracts in Response to thePropagation of Electrical Signals from OneCardiac Cell to Another Across Gap JunctionsCardiac muscle cells also have chemical synapses, but thesympathetic and parasympathetic branches of the auto-nomic nervous system (see Chapter 15) use these synap-
231Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9
ses to modulate, rather than to initiate, cardiac musclefunction. In contrast to skeletal muscle, cardiac musclecontraction is triggered by electrical signals from neigh-boring cardiac muscle cells. These electrical impulses orig-inate in the pacemaker region of the hean, the sinoatrialnode (p. 489), which spontaneously and periodically gen-erates action potentials. To facilitate direct electrical com-munication between cardiac muscle cells, the sarcolemmaof cardiac muscle is specialized to contain gap junctions(p. 164), electrical synapses that couple neighboring cells(Fig. 9-1). When an action potential is initiated in onecell, current flows through the gap junctions and depolar-izes neighboring cells. If depolarization causes the mem-brane potential (V m) to be more positive than threshold,self-propagating action potentials occur in the neighboringcells as well. Thus, the generation of an action potential isjust as critical for initiating contraction in cardiac muscleas it is in skeletal muscle.
Smooth Muscles May Contract in Response toEither Neuromuscular Synaptic Transmissionor Electrical CouplingLike skeletal muscle, smooth muscle receives synaptic in-put from the nervous system. However, the synaptic in-put to smooth muscle differs from that to skeletal musclein two ways. First, the neurons are pan of the autonomicnervous system rather than the somatic nervous system(see Chapter 15). Second, the neuron makes multiplecontacts with a smooth muscle cell. At each contactpoint, the axon diameter expands to form a varicositythat contains the presynaptic machinery. The varicosity isin close proximity to the postsynaptic membrane of thesmooth muscle cell, but there is relatively little specializa-tion of the postsynaptic membrane. Rather than the neu-rotransmitter receptors being closely clustered at the neu-romuscular junction, as in skeletal muscle, in smoothmuscle the receptors are spread more widely across thepostsynaptic membrane.
The mechanisms of intercellular communication amongsmooth muscle cells are more diverse than are those ofskeletal or cardiac muscle. In some organs, smooth mus-cle is innervated in a manner similar to skeletal muscle inthat each smooth muscle cell receives synaptic input.However, a difference is that a smooth muscle cell mayreceive input from more than one neuron. Moreover,there is little electrical coupling among these smoothmuscle cells (Le., few gap junctions). As a result, eachsmooth muscle cell may contract independently of itsneighbor. Because this type of smooth muscle behaves asmultiple, independent cells or groups of cells, it is calledmultiunit smooth muscle (Fig. 9-2A). Note that the"multi" in "multiunit" refers to the muscle fibers' actingindependently of one another as multiple units. Multiunitsmooth muscles are capable of finer control. Indeed, mul-tiunit smooth muscle is found in the iris and ciliary bodyof the eye, the piloerector muscles of the skin, and someblood vessels.
In contrast to multiunit smooth muscle, the smoothmuscle cells of most organs have extensive intercellularcommunication in the manner of cardiac muscle cells. In
ntercalated
Z-line

232 9 I Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
I
,11 this type of smooth muscle, gap junctions pennit electri-cal communication between neighboring cells. This com-munication allows coordinated contraction of many cells.Because these cells contract as a single unit, this type ofsmooth muscle is called unitary smooth muscle (Fig. 9-28). Unitary smooth muscle is the predominant smoothmuscle type within the walls of visceral organs such asthe gastrointestinal tract, the uterus, and many blood ves-sels. For this reason, unitary smooth muscle is often re-ferred to as visceral smooth muscle. Among unitarysmooth muscles, variation in the strength of intercellularcoupling from organ to organ leads to variation in thespatial extent of a single unit. For example, in the blad-der, extensive coupling among cells defines large func-tional units, which allows the muscular wall of the blad-der to contract in synchrony. On the other hand, thesmooth muscle cells of blood vessels couple to Connsmaller, independently functioning units that are moreakin to multiunit smooth muscle. In fact, electrical cou-pling of smooth muscle units exhibits a tissue-specificcontinuum from multiunit to unitary coupling.
Action Potentials of Smooth Muscles May BeBrief or ProlongedWhereas both skeletal muscle and cardiac muscle produceaction potentials that initiate ~ontraction, smooth musclecells produce a wide range of V m variations that caneither initiate or modulate contraction. Action potentialsthat are similar to those seen in skeletal muscle are 0b-served in unitary smooth muscle and in some multiunitmuscle. Uke cardiac muscle cells, some smooth musclecells exhibit prolonged action potentials that are charac-terized by a prominent plateau. Still other smooth musclecells cannot generate action potentials at all. In thesecells, V m changes in a graded fashion (p. 173) rather thanin the all-or-none manner of action potentials. The stimulithat produce a graded respol1K of V m include manycirculating and local humoral factors, as well as mechani-cal stimuli such as stretching the cell. These graded V mchanges may be either hyperpolarizing or depolarizing;they sum temporally as well as spatially. If the summationof graded de polarizations brings V m above threshold - in
BA
a smooth muscle cell capable of producing an actionpotential-an action potential will then ensue.
Action potentials are usually seen in unitary (visceral)smooth muscle. These action potentials typically have aslower upstroke and longer duration (up to -100 IDS)than do skeletal muscle action potentials (-2 IDs). Theaction potential in a smooth muscle cell can be a simplespike, a spike followed by a plateau, or a series of spikeson top of slow waves of VIII (Fig. 9-3A). In any case, theupstroke or depolarizing phase of the action potentialreflects opening of voltage-gated Ca2+ channels. The in-ward Ca2+ current further depolarizes the cell andthereby causes still more voltage-gated Ca2+ channels toopen. Thus, some smooth muscle cells can undergo thesame type of regenerative depolarization that is seen inskeletal muscle. However, the rate of rise of the actionpotential in smooth muscle is lower because Ca2+ chan-nels open more slowly than do Na+ channels in skeletaland cardiac muscle (p. 189). Repolarization of the smoothmuscle cell is also relatively slow. Two explanations maybe offered for this slower repolarization. First, voltage-gated Ca2+ channels, which are responsible for the depo-larization phase of the action potential, inactivate slowly.Second, the repolarization phase of the action potentialreflects the delayed activation of voltage-gated K+ chan-nels and, in some cases, Ca2+ -activated K+ channels.
Some smooth muscle cells have fast, voltage-gated Na+channels. However, even when these channels arepresent, they do not appear to be necessary for generatingan action potential. Their main role may be to allow morerapid activation of voltage-gated Ca2+ channels and thuscontribute to a faster rate of depolarization.
In some unitary smooth muscle, repolarization is sodelayed that the action potential contour displays a prom-inent plateau. These plateau potentials may be severalhundred milliseconds in duration, as in cardiac muscle.Plateau action potentials occur in smooth muscle of thegenitourinary tract, including the ureters, bladder, anduterus. The long V m plateau allows the entry of Ca2+ tocontinue for a longer period and thus allows [Ca2+)1 toremain high for a longer period, thereby prolonging thecontraction.

mV
0 100Time (msec)
~~
(Voltage-gated ea2+ channels close;~temal ea2+ concentration decreases
~I SIowh~don I~
FIGURE 9-3. Action potentials and slow waves in smooth muscle.
Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle I 9 233
Slow wavesPlateau
200 400Time (msec)
0 . 10Time (see)
OJ
.[ Action potential spike I

234 9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
Some Smooth Muscle Cells Can InitiateSpontaneous Electrical ActivityAlthough smooth muscle cells undergo changes in V rn inresponse to neural, hormonal, or mechanical stimulation,many smooth muscle cells are capable of initiating spon-taneous electrical activity. In some cells, this spontaneousactivity results from pacemaker currents. These currentsresult from time- and voltage-dependent properties of ioncurrents that produce either a spontaneous increase ininward, or depolarizing, currents (e.g., voltage-gated CaHcurrents) or a spontaneous decrease in outward, or hyper-polarizing, currents (e.g., voltage-gated K+ currents). Thepacemaker currents cause the cell to depolarize until V rnreaches threshold, triggering an action potential.
In other smooth muscle cells, this spontaneous electri-cal activity results in regular, repetitive oscillations in Vrn.These V rn oscillations occur at a frequency of several oscil-lations per minute and are referred to as slow waves(Fig. 9-38). One hypothesis for the origin of slow-wavepotentials suggests that voltage-gated Ca2+ channels-ac-tive at the resting Vrn-depolarize the cell enoughactivate more voltage-gated Ca2+ channels. This activationresults in progressive depolarization and Ca2+ influx. Theincrease in [CaHI, activates Ca2+ -dependent K+ channels,which leads to progressive hyperpolarization and termina-tion of the depolarization phase of the wave. These peri-odic depolarizations and [CaHJj increases cause periodic,tonic contractions of the smooth muscle. When the am-plitude of the slow V rn waves is sufficient to depolarizethe cell to threshold, the ensuing action potentials lead tofurther Ca2+ influx and phasic contractions.
Other hypotheses to explain spontaneous electrical andmechanical activity in smooth muscle cells are based onoscillatory changes in other intracellular ions or mole-cules. For example, increased [Ca2+1. during an actionpotential might stimulate Na-Ca exchange and lead to acyclic increase in [Na+1. and thus an increase in the rateof Na+ extrusion by the electrogenic Na-K pump. Alterna-tively, the inositol l,4,S-triphosphate CIP)) receptor chan-nel (p. 100) might spontaneously open and release Ca2+.The effect on [CaHII would be self-reinforcing because ofCa2+-activated CaH release via the IP) receptor. At high[CaHI., this channel is inhibited and the Ca2+ releaseevent is terminated, followed by re-uptake of Ca2+ intothe sarcoplasmic reticulum (SR). The K:aHI, increasesmay themselves lead to periodic electrical activity by stim-ulating Ca2+ -activated inward and outward currents.
Some Smooth Muscles Contract WithoutAction PotentialsWhereas action-potential generation is essential for initiat-ing contraction of skeletal and cardiac muscle, manysmooth muscle cells contract despite being unable to gen-erate an action potential. As discussed previously, Vrn os-cillations can lead to tonic contractions in the absence ofaction potentials. Action potentials usually do not occurin multiunit smooth muscle. For example, in the smoothmuscle that regulates the iris, excitatory neurotransmitterssuch as norepinephrine or ACh cause a local depolariza-tion, the junctional potential, which is similar to the
end-plate potential in skeletal muscle. juntials spread electrotonically (Le., in a grthroughout the muscle fiber, thereby alterilfecting the entry of Ca2+ through voltal(l-type) Ca2+ channels. Changes in Vm-b)mechanism - may also modulate the activizyme phospholipase C, which cleaves photo release the intracellular second messengcerol (DAG) and IP3 (p. 100). Both these segers are modulators of contractile force. In taction potentials, some unitary smooth mU5some vascular smooth muscle, also contractsgraded V m changes.
Some smooth muscle cells contract witholin V m' For example, a neurotransmitter c:receptor, activate a G protein, and lead to tof IP 3, which in turn leads to the release of ~SR. The eventual depletion of Ca2+ stores i:Jin turn stimulate Ca2+ influx across the C4via so-called store-operated Ca2+ channels.
MUSCLE CONTRACTION
Striated Muscle Cells Are Densely Pwith Myofibrlls That Contain Orderof Thick and Thin Filaments
As summarized in Figure 9-4A, each indivmuscle cell (or myocyte or fiber) contains a carray of smaller, cylindrical elements callethat have the diameter of a Z disk (p. 45). ]myofibrils comprises repeating units, or sanconsist of smaller interdigitating filaments caments. These myofilaments come in two ty9-4B), thick filaments composed primarily 0thin filaments composed primarily of actinsarcomere extends from one Z disk to anjmeres stacked end to end make up a mrepeating sarcomeres are most highly orgaskeletal and cardiac muscle and impan a strance. Thus, both skeletal and cardiac muscleto as striated muscle.
In smooth muscle, striations are not visi~actin and myosin are present in smooth musrelationship between actin and myosin (thifilaments) is less highly organized. The actinoriented mainly parallel or oblique to the Ioncell. Multiple actin filaments appear to joindense regions called dense bodies, which armediately beneath the cell membrane, as wethe interior of the myocyte. The thick filamerspersed among the thin filaments in smoothare far less abundant than in skeletal or carnic
-rL:- 1;1~ n.c: ~T.. ') to 8 nm in diaml
to

A FROM MUSCLE TO MYOFILAMENTS
Thickthin filaments(myofilaments)
FIGURE 9-4. Structure of the sarcomere,
"each myofibril to its neighbors. These interconnections';align the sarcomeres and give skeletal and, to a lesser; (xtent, cardiac muscle its striated appearance.
The thick filaments are 10 run in diameter and, init$triated muscle, 1.6 fLm in length. They lie betWeen and1Panially interdigitate with the thin filaments. This partial;1nterdigitation results in alternating light and dark bandsialong the axis of the myofibril (see Fig, 9-4C). The lightbands, which represent regions of the thin filament thatdo not lie alongside thick filaments, are known as Iihands because they are isotropic to polarized light. The Zdisk is visible as a dark perpendiculadine at the center ofthe I band. The dark bands, which represent the myosinfilaments, are known as A bands because they are aniso-
;troPic to polarized light. During contraction, the A bands;~ unchanged in length whereas the I bands shonen.'it, Within the A bands, the pivoting heads of the thick
yosin filaments, the molecular motors, establish cross-. dges to the thin actin filaments. As discussed later, the
enosine triphosphate (ATP)-dependent cycle of makingbreaking cross-bridges causes the actin filament to be
Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9 U5
B MODEL OF A SARCOMERE
H~ I~oo. '. .'.
/Actin Myosin
C ELECTRON MICROGRAPH OF SARCOMEREA band
..r ,
I band
One sarcomere
drawn over the myosin filament and thereby results inmuscle contraction.
The Thin and Thick Filaments AreSupramolecular Assemblies ofProtein Subunits
THIN FILAMENTS. Thin filaments (Fig. 9-5A) consist ofactin, tropomyosin, and troponin. The backbone of thefilament is a double-stranded a-helical polymer of actinmolecules. Each helical turn of a single strand of filamen-tous or F-actin consists of 13 individual actin monomersand is approximately 70 nm long. F-actin is associatedwith two important regulatory, actin-binding proteins:tropomyosin and troponin.
Individual tropomyosin molecules consist of two iden-tical a helices that coil around each other and sit near thetwo grooves that are formed by the two helical actinstmnds. Head-ta-tail contact between neighboring tropo-myosin molecules results in two nearly continuous helical

2)6 9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
A THIN FILAMENT
Ca2+ (bound: Trapanin complexto troponin : ~complex) ~ Tn\.. TnC TnI
I ' If'Actin' Tropomyosin Myosin binding site'
B MYOSIN MOLECULE
Heads of myosinheavy chain (81)
rRegulatorylight chain
/Alkalilight chainH_~
of heavy chainsTail region of heavy chains
C INTERACTION OF THIN AND THICK FILAMENTS
Myosin head bound I
to actin filament at
myosin binding site
FIGURE 9-5. Structure of thin and thick filaments.
filaments that shadow the actin double helix. The lengthof a single tropomyosin molecule corresponds to aboutseven actin monomers (Le., a half turn of the actin helix).As we shall see later, the role of tropomyosin is to inter-fere with the binding of myosin to actin.
Troponin is a heterotrimer consisting of troponin T(which binds to a single molecule of tropomyosin), tropo-nin C (which binds Ca2+), and troponin I (which binds toactin and inhibits contraction). Troponin C is closely re-lated to another Ca2+-binding protein, calmodulin (CaM;p. 102). Thus, each troponin heterotrimer interacts with asingle tropomyosin molecule, which in turn interacts withseven actin monomers. The troponin complex also inter-acts directly with the actin filaments. The coordinatedinteraction among troponin, tropomyosin, and actin al-lows actin-myosin interactions to be regulated by changesin [Ca2+)j.
THICK FILAMENTS. Uke thin actin filaments, thick fila-ments are polymers of proteins (see Fig. 9-5B). Thickfilaments are bipolar assemblies composed of multiple
myosin-II molecules. Each myosin-II molecule is a hex-amer (actually a double trimer) composed of two inter-twined heavy chains, two regulatory light chains, and twoalkali (or essential) light chains. The two heavy chainshave three regions: a rod, a hinge, and a head region. Therod ponions are a helices that wrap around each other.At the hinge regions, the molecule flares open to form twoglobular heads, which are the cross-bridges between thethick and thin filaments of the sarcomere. The heads ofthe heavy chains-also called S1 fragments-each p0s-sess a site for binding actin as well as a site for bindingand hydrolyzing ATP. The head ponion of each myosinforms a complex with two light chains, one regulatoryand one alkali. The alkali light chain plays an essentialrole in stabilizing the myosin head region. The regulatorylight chain, as its name implies, regulates the ATPaseactivity of myosin. The activity of the myosin regulatorylight chain is in turn regulated via phosphorylation byCa2+ -dependent and Ca2+ -independent kinases.
Figure 9-SC summarizes the interaction between athin filament and a single pair of head groups from themyosin of a thick filament.
In All Three Muscle Types, An Increase in[Ca2+]1 Triggers Contraction By Removing theInhibition of Cross-Bridge CyclingUnderlying muscle contraction is a cycle in which myo-sin-II heads bind to actin, these cross-bridges becomedistoned, and finally the myosin heads detach from actin.Energy for this cycling comes from the hydrolysis of ATP.However, if unregulated, the cycling would continue untilthe myocyte was depleted of ATP. It is not surprising,then, that skeletal, cardiac, and smooth muscle each havemechanisms for regulating cross-bridge cycling. In allthree cell types, an increase in [Ca2+]t initiates and allowscross-bridge cycling to continue. During this excitatoryincrease, [Ca2+lt may rise from its resting level of lessthan 10-7 M to greater than 10-5 M. The subsequentdecrease in [Ca2+]i is the signal to cease cross-bridgecycling and relax.
Regardless of the muscle type, Ca2+ modulates contrac-tion through regulatory proteins rather than interactingdirectly with the contractile proteins. In the absence ofCa2+, these regulatory proteins act in concen to inhibitactin-myosin interactions, thus inhibiting the contractileprocess. When Ca2+ binds to one or more of these pro-teins, a conformational change takes place in the regula-tory complex that releases the inhibition of contraction.
Myosin (thickfilament)
SKELETAL MUSCLE. The heterotrimeric troponin mole-cule contains the key CaB -sensitive regulator troponin C(Fig. 9-M). Each troponin C molecule in skeletal mus-cle has two high-affinity CaB -binding sites that partici-pate in binding of troponin C to the thin filament. Ca2+binding to these high-affinity sites does not change duringmuscle activation. Each troponin C molecule in skeletalmuscle also has two additional, low-affinity Ca2+ -bindingsites. Binding of CaB to these low-affinity sites induces aconformational change in the troponin complex that hastwo effects. The first effect is that the C terminus of the

INITIATION OF CROSS-BRIDGE CYCLINGIN SKELETAL AND CARDIAC MUSCLE
/Actin Tropomyosin "--r-'
Troponlncomplex
B INITIATION OF CROSS-BRIDGE CYCLING IN SMOOTH MUSCLE
0.2<-
" ~(.vCalmodulin
The role of Ca2+ in triggering muscle contraction. MlCI<, myosin light chain kinase.
bitory troponin I moves away from the actinltropomy-filament, thereby permitting the tropomyosin mole-to move. According to one hypothesis, the other, transmitted through troponin T, is to push tropo-
{tnyosin away from the myosin-binding site on the actininto the actin groove. With the sterle hindrance re-
, the myosin head is able to interact with actin andin cross-bridge cycling.
Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9 2)7
Ca2+i-.~
e,
/'Active calmodulin!MLCK complex
CARDIAC MUSCLE. The regulatory mechanism withincardiac muscle is similar to that of skeletal muscle, al-though troponin C from cardiac muscle has just a single,active low-affinity Ca2+ -binding site.
SMOOTH MUSCLE. An entirely different mechanism con-trols cross-bridge turnover in smooth muscle. Here. anincrease in [Ca2+ L initiates a slow chain of events that

238 9 I Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
ultimately increases the ATPase activity of the myosin (seeFig. 9-68). The first step is the binding of four Ca2+ ionsto calmodulin, which, as we noted earlier, is closely re-lated to troponin C. Next, the Ca2+ -CaM complex acti-vates an enzyme known as myosin light chain kinase(MLCK), which in turn phosphorylates the regulatorylight chain that is associated with the myosin-II molecule.Phosphorylation of the light chain alters the conformationof the myosin head, which greatly increases its ATPaseactivity and allows it to interact with actin and act as amolecular motor. Thus, in smooth muscle, CaM ratherthan troponin C is the Ca2+ -binding protein responsiblefor transducing the contraction-triggering increases in[Ca2+],. Note that in smooth muscle, contraction cannotbegin until MLCK increases the ATPase activity of myo-sin, which is a time-consuming process. In skeletal andcardiac muscle, on the other hand, the ATPase activity ofthe myosin head is constitutively high, and cross-bridgecycling can begin as soon as the tropomyosin is movedout of the way.
The mechanism just outlined activates the thick fila-ments in smooth muscle. Other mechanisms act on thethin filaments of smooth muscle to remove the tonicinhibition to actin-myosin interactions that are caused bysteric hindrance. Two proteins-caldesmon and cal-ponin-tonically inhibit the interaction between actinand myosin. Both are Ca2+-CaM-binding proteins, andboth bind to actin and tropomyosin. Calponin, which isfound in a fixed stoichiometry with tropomyosin and ac-tin (one calponin-one tropomyosin-seven actin mono-mers), tonically inhibits the ATPase activity of myosin. Aswe saw earlier, the increase in [CaB], that triggers smoothmuscle contraction activates Ca2+ -CaM. Besides activatingMLCK, this Ca2+ -CaM complex has two effects on cal-ponin. First, Ca2+ -CaM binds to calponin. Second, Ca2+-CaM activates Ca2+-CaM-dependent protein kinase,which phosphorylates calponin. Both effects reduce cal-ponin's inhibition of myosin's ATPase activity. like cal-ponin, caldesmon also tonically inhibits the ATPase activ-ity of myosin in smooth muscle.
During the Cross-Bridge Cycle, ContractileProteins Convert the Energy of A TPHydrolysis Into Mechanical En-:rgyThe cross-bridge cycle that we introduced in the previoussection occurs in five steps (Fig. 9-7). Initially, the myo-sin head is attached to an actin filament after the "powerstroke" from the previous cycle and after the actomyosincomplex has released adenosine diphosphate (ADP). Inthe absence of ATP, the system could remain in this rigidstate for an indefinitely long period, as is indeed the casein rigor monis. In this rigid state, the myosin head is at a45-degree angle with respect to the actin and myosinfilaments.
Step 1: ATP binding. ATP binding to the head of themyosin heavy chain (MHC) reduces the affinity of myo-sin for actin, causing the myosin head to release fromthe actin filament. If all cross-bridges in a muscle werein this state, the muscle would be fully relaxed.
Step 2: ATP hydrolysis. The breakdown of ATP to ADP
and inorganic phosphate (Pi) occurs on the myosinhead; the products of hydrolysis are retained on themyosin. As a result of hydrolysis, the myosin headpivots around the hinge into a "cockedn position (per-pendicular or at a 90-degree angle to the thick andthin filaments). This rotation causes the tip of the myo-sin to move about 11 nm along the actin filament sothat it now lines up with a new actin monomer twomonomers further along the actin filament (see the boxtitled Measuring the Force of a Single Cross-BridgeCycle). Once again, if all cross-bridges in a musclewere in this state, the muscle would be fully relaxed.
Step 3: Cross-bridge formation. The cocked myosinhead now binds to its new position on the actin fila-ment. This binding reflects the increased affinity of themyosin-ADP-Pi complex for actin.
Step 4: Release of Pi from the myosin. Dissociation of Pifrom the myosin head triggers the power stroke, aconformational change in which the myosin headbends approximately 45 degrees about the hinge andpulls the actin filament about 11 nm toward the tail ofthe myosin molecule. This conformational changecauses the actin filament to be drawn along the myosinfilament, thereby generating force and motion.
Step 5: ADP release. Dissociation of ADP from myosincompletes the cycle, and the actomyosin complex is leftin a rigid state. The myosin head remains in the sameposition and at a 45-degree angle with respect to thethick and thin filaments. The ADP-free myosin com-plex remains bound to actin until another ATP bindsand initiates another cycle.
The ADP-free myosin complex (~attached state" in Fig.9- 7) would quickly bind ATP at the concentrations ofA TP normally found within cells. If unrestrained, thiscross-bridge cycling would continue until depleting thecytoplasm of ATP. At that time, the muscle would remainin the stiff ~attached state" because release of the cross-bridges from actin requires binding of ATP to myosin.
As discussed earlier, muscle cells do not regulate cross-bridge cycling by modifying [A TPI;. Instead, skeletal mus-cle and cardiac muscle control this cycle at the third stepby preventing cross-bridge formation until the tropomyo-sin moves out of the way in response to an increase in[Ca2+Jj. Smooth muscle controls the cycle at the secondstep by preventing A TP hydrolysis until the ATPase activ-ity of the myosin head increases in response to an in-crease in [Ca2+J,.
Although this general schema of cross-bridge cyclingoccurs in smooth muscle as well as skeletal and cardiacmuscle, the frequency of cross-bridge cycling in smoothmuscle is less than one tenth the frequency encounteredin skeletal muscle. This variation reflects differences inthe propenies of the various myosin isoforms that areexpressed in various cell types. Even though cross-bridgecycling occurs less frequently in smooth muscle, forcegeneration may be as great or greater, perhaps becausethe cross-bridges remain intact for a longer period witheach cycle. It is likely that this longer period duringwhich the cross-bridges are intact reflects a lower rate ofADP release from the smooth muscle isoform of myosin.

IS
POWER-STROKE STATE
P is released. Myosin heads change,~tion,. resulting in the power,~ke. The filaments slide pest each other.
l1Ie cross-bridge cycle in skeletal and cardiac muscle. Each cycle advances the myosin head by two actin monomers, or approximately:\GURE 9-7.,1 nm,
Because A TP Stores Are Small, the CellMust Regenerate the ATP Needed ForMuscle Contraction
Each cross-bridge cycle consumes one molecule of ATP.In skeletal muscle, the entire cellular slare of ATP issufficient to allow only a few seconds of continuous max-imal contraction. Therefore, the muscle cell must resyn-thesize A TP from ADP at a rate comparable to the rate ofI\TP consumption. Skeletal muscle has specialized energy>tores that permit rapid regeneration of ATP. The mostreadily available pool of this energy is the high-energyphosphate bond of phosphocreatine. The enzyme creati1l£mosphotransferase transfers the high-energy phosphate ofphosphocreatine to ADP, thereby rephosphorylating ADPto ATP. The phosphocreatine content of skeletal muscle isadequate to replenish the ATP pool several times, but it isstill inadequate for sustaining the energy needs of con-tracting muscle for more than 10 seconds.
Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9 239
RELEASED STATE
COCKED STATE
In comparison with the energy stored as phosphocrea-tine, glycogen is a far more abundant energy sourcewithin skeletal muscle. Glycogen that has been previouslystored by muscle can be enzymatically degraded to pyru-vic acid. Degradation of glycogen to pyruvate is rapid andliberates energy that the cell invests in phosphorylatingADP to yield ATP. Pyruvate can be further degradedalong with other foodstuffs by oxidative metabolism, whichover the long term is the primary mechanism for theregeneration of ATP (p. 1220). The rate of ATP genera-tion by oxidative metabolism is limited by the rate ofoxygen delivery to the muscle. However, glycolytic forma-tion of pyruvate occurs independently of oxygen, as doesthe conversion of pyruvate to lactate. This anaerobic me-tabolism of muscle glycogen ensures that energy stores aresufficient to sustain muscle activity for nearly a minuteeven when oxygen is unavailable. In Chapter 59 we willdiscuss the aerobic and anaerobic metabolism of exercis-ing muscle in more depth.

240 9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
A SKELETAL MUSCLE
B
Plasma
FIGURE 9-8. Plasma-membrane invaginations. A, The transverse tubules (T tubules) are extensions of the plasma membrane, penetrating the musclecell at two points in each sarcomere: the junctions of the A and I bands. S, Smooth-muscle cells have rudimentary invaginations of the plasmamembrane, called caveoli, contacting with the sarcoplasmic reticttlum.
EXCIT A TlON-CONTRAcnON COUPLING
In our discussion of the mechanism of JIluscle contrac-tion, we saw that regardless of whethef' the muscle isskeletal, cardiac, or smooth, it is an increase in [Ca2+J;that triggers muscle contraction. The time during which[Ca2+Ji remains elevated determines the duration of mus-cle contraction. The process by which "excitation" triggersthe increase in [Ca2+JI is known as exdtation-contractioncoupling. Different kinds of myocytes have specializedmechanisms that regulate the entry of Ca2+ into the cyto-plasm, as well as remove Ca2+ from the cytoplasm oncethe stimulus for muscle contraction subsides. Ca2+ canenter the cytoplasm from the extracellular space throughvoltage-gated or ligand-gated ion channels, or alterna-tively, CaH can be released into the cytoplasm from theSR Thus, both extracellular and intracellular sources con-tribute to the increase in [Ca2+J;. However, the relativeimportance of these two sources varies among the differ-ent muscle types.
/'" Plasma/'" membrane
(sarcolemma)
TRIAD:
Sarcoplasmicreticulumcistema
Transversetubule
Sarcoplasmicreticulumcisterna
Sarcomere
Caveoli
~
-, ,~.~. :- -~4 . . . -
Invaginations of the Sarcolemma FacilitateCommunication Between the Surface of theCell and Its InteriorThe plasma membranes of muscle cells display invagina-tions that extend the surface membrane into the musclecell. In skeletal and cardiac muscle, these invaginationstake the form of radially projecting tubes called trans-verse tubules or T tubules (Fig. 9-BA). T tubules arehighly organized and penetrate the muscle at two pointsin each sarcomere: at the junctions of the A and I bands.A cross section through the A-I junction would show acomplex, branching array of T tubules penetrating to thecenter of the muscle cell and surrounding the individualmyofibrils. Along its length the tubule associates with twocisternae, which are specialized regions of the SR. Thesarcoplasmic reticulum is the muscle equivalent of theendoplasmic reticulum, and it serves as a storage orga-nelle for intracellular Ca2+. The combination of theT -tubule membrane and its two neighboring cisternae iscalled a triad; this structure plays a crucial role in the

~
Triad.
FIGURE 9-9. Excitation-contraction coupling In skeletal muscle. A tetrad of four l-type Ca2+ channels on the T tubules faces a single Ca2+-releasechannel of the SR, so that each l-type CaH channel interacts with the foot of one of the four subunits of the CaH -release channel. Note that half ofthe cr--release chlUUlels lack associations with l-type CaH channels. DHP, dihydropyridine; SR, sarcoplasmic reticulum.
coupling of excitation to cwntraction in skeletal and car-diac muscle. Smooth muscle, in contrast, has more rudi-mentary and shallow invaginations called c~veoli (see Fig.9-8B).
In Skeletal Muscle, Depolarizatl~n of theT-Tubule Membrane Leads to Ca2+ Releasefrom the Sarcoplasmic Reticulum at the TriadAction potentials originating from depolarizations at themotor end plate propagate along the skeletal musclemembrane and down the T tubules. Depolarization of thetriad region of the T tubules activates L-type Ca2+ chan-nels (p. 190). which are clustered in groups of fourcalled "tetrads" (Fig. 9-9). These voltage-gated channelsplaya pivotal role in coupling electrical excitation tocontraction because they function as the voltage sensorin EC coupling. Electron microscopy reveals a checker-board pattern of projections arising from the T -tubulemembrane and extending toward the cisternae of the SR;these projections probably represent the cytoplasmic faceof these L-type Ca2+ channels. Each of the four voltage-gated Ca2+ channels in a tetrad is in fact a heteropenta-
Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9 241
SA tenninal cisterna
meric protein (see Fig. 7-128). Each of the four Ca2+channels is also called a DHP receptor, because it isinhibited by a class of antihypenensive drugs known asdihydropyridines. Depolarization of the T -tubule mem-brane evokes conformational changes in each of the fourL-type CaH channels and has two effects. First, the con-formational changes allow CaH to enter through the fourchannel pores. Second, and much more important, theconformational changes in the four L-type CaH channelsinduce a conformational change in each of the four sub-units of another channel-the Ca2+-release channel-that is located in the SR membrane.
The CaH-release channel (Table 6-2, #18) has ahomotetrameric structure quite different from that of theL-type CaH channel that constitutes the voltage sensor.The CaH -release channel in the SR is also known as theryanodine receptor because it is inhibited by a class ofdrugs that include the plant alkaloids ryanodine and caf-feine. CaH -release channels cluster in the ponion of theSR membrane that faces the T tubules. Each of the foursubunits of these channels has a large extension-alsoknown as a "foot." These feet project as a regular arrayinto the cytosol. The foot of each of the four CaH -release

242 9 I Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
channel subunits is complementary to the cytoplasmicprojection of one of the four l-type Ca2+ channels in atetrad on the T tubule (see Fig. 9-9). The close physicalproximity of these two proteins, as well as the ability ofboth DHP and ryanodine to block muscle contraction,suggests that interaction between these two different Ca2+channels underlies EC coupling. The precise mechanismof interaction between these proteins is not yet fully un-derstood, although we know that it is not electrical inas-much as ion conductance of the Ca2+ -release channel isnot strongly voltage dependent. A large cytoplasmic pro-jection on the Ql subunit of the l-type CaH channelappears to be necessary for interaction between the twoCaH channels on opposing T -tubule and SR membranes.Thus, it is possible that direct mechanical coupling existsbetween this projection and the Ca2+ -release channel.
As the l-type CaH channel on the T -tubule membranemechanically opens the CaH -release channel in the SR,CaH sequestered in the SR rapidly leaves via the Ca2+-release channel. The resultant rapid increase in [CaHI,activates troponin C, thus initiating cross-bridge cyclingas described earlier. The entire process, extending fromdepolarization of the T -tubule membrane to the initiationof cross-bridge cycling, is termed excitation-contractioncoupling.
Although we have stressed activation of the CaH -re-lease channel in the SR by mechanical coupling between itand the l-type CaH channel in the T -tubule membrane,local elevations in [CaHL can also activate the CaH-re-lease channel in skeletal muscle. When the l-type Ca2+channel opens during depolarization, it allows an influxof CaH that locally increases [Ca2+li' This mechaniSm ofactivating the CaH -release channel in the SR is known asCa2+-induced Ca2+ release (ClCR). Although l-typeCa2+ channels allow [Ca2+1i to rise during action poten-tials in skeletal muscle, ClCR is not necessary for contrac-tion. Indeed, skeletal muscle contraction persists evenwhen CaH is absent from the extracellular fluid. How-ever, as we will see later, ClCR plays a critical role in ECcoupling in cardiac muscle.
In Cardiac Muscle, Ca2+ Entry Through L- TypeCa2+ Channels Is Amplified By Ca2+-lnducedCa2+ Release from the SarcoplasmicReticulumWhereas EC coupling in skeletal muscle does not requireCa2+ influx through l-type Ca2+ channels, cardiac con-traction has an absolute requirement for CaH influ~through these channels during the action potential. Be-cause the T-tubule lumen is an extension of the extracel-lular space, it facilitates the diffusion of Ca2+ from bulkextracellular fluid to the site of the l-type Ca2+ channelson the T -tubule membrane. Thus, the CaH can simulta-neously reach superficial and deep regions of the muscle.The increase in [Ca2+1i resulting from Ca2+ influx alone isnot, however, sufficient to initiate contraction. Rather, theincrease in [CaHli that is produced by the l-type Ca2+channels is greatly amplified by ClCR from the SR via theCaH -release channels. Indeed, because the CaH -releasechannels remain open for a longer period than do l-type
Ca2+ channels, the contribution of CICR to the rise in[Ca2+)t is greater than the flux contributed by the l-typeCa2+ channels of the T tubules.
It appears that each l-type Ca2+ channel controls onlyone SR Ca2+ -release channel. The close physical proximityof l-type Ca2+ channels of the T -tubule membrane andthe Ca2+ -release channel in the SR at the triad junctionsallows for this tight local control. Although Ca2+ diffusesin the cytosol away from its SR release site, Ca2+ releaseat one site does not appear to be able to induce Ca2+release from a neighboring SR Ca2+ -release channel. Thus,Ca2+ release events are not propagated along the myocyte.In fact. the SR Ca2+ -release channel does not appear torespond to generalized increases in cytoplasmic [Ca2+)jOGeneralized cardiac muscle contractions occur as a resultof the spatial and temporal summation of individual CICRevents.
In Smooth Muscle, Both Extracellular andIntracellular Ca2+ Activate Contraction
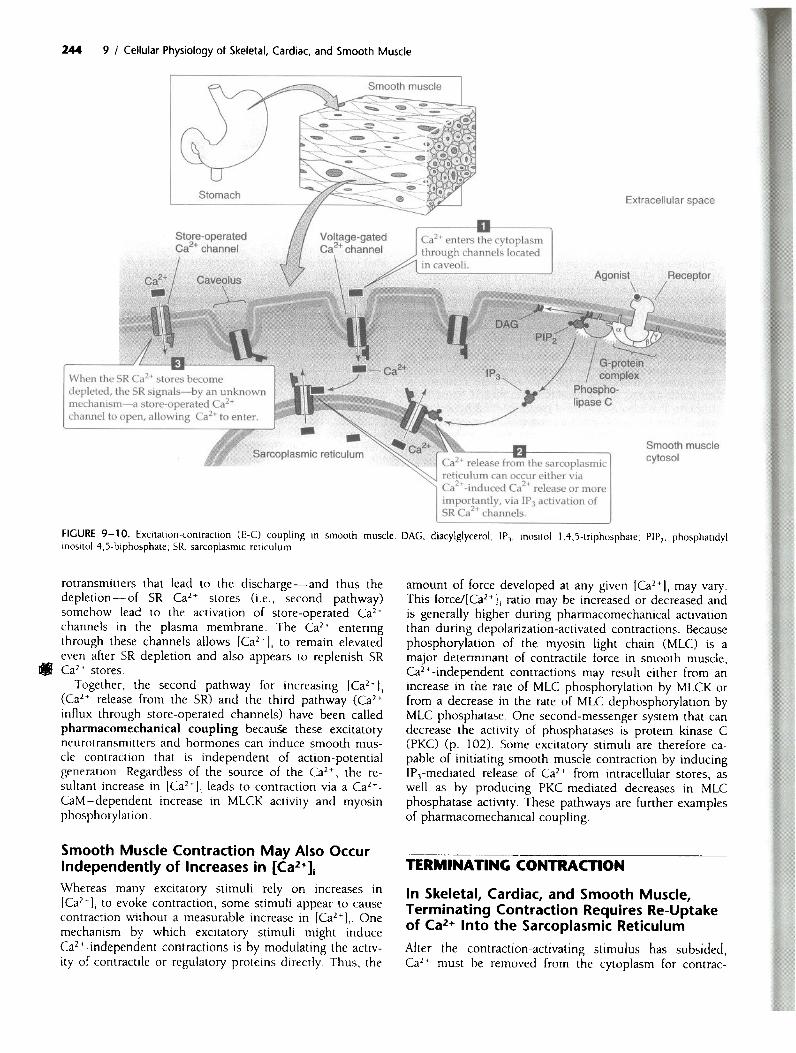
In smooth muscle cells, three major pathways-whichare not mutually exclusive-can lead to the increase in[CaH)j that triggers contraction: (1) CaH entry throughvoltage-gated channels in response to cell depolarization,(2) CaH release from the SR, and (3) CaH entry throughvoltage-independent channels.
Cr+ ENTRY THROUGH VOLTAGE-CiA TED CHANNELS. As
noted earlier, smooth muscle cells respond to stimulationwith graded depolarizations or action potentials. In eithercase, depolarization may produce an influx of Ca2+through voltage-gated L-type Ca2+ channels (Fig. 9-10).
Cr+ RELEASE FROM THE SR. This Ca2+ release may occurby either of two mechanisms: CICR or IPrmediated Ca2+release. As we have already seen, CICR plays a key role inEC coupling in cardiac muscle, where the L-type Ca2+channels are highly ordered and in close proximity to theCa2+ -release channels in the SR. Thus, Ca2+ influxthrough L-type Ca2+ channels can trigger ClCR. Insmooth muscle. the relationship betWeen the plasmamembrane and the SR is not as regularly organized as itis in striated muscle. Nevenheless. electron-dense cou-plings have been observed bridging the 8- to 10-nm gapbetWeen the cell membranes and elements of the SR insmooth muscle. Although ClCR occurs in smooth musclecells under some conditions. it requires [Ca2+]j levels thatare higher than those that typically occur under physio-logical conditions. and its role remains unclear.
A more imponant mechanism for Ca2+ release from theSR of smooth muscle is the IP) pathway. The existence ofthis pathway is supponed by the observation that someextracellular agonists can elicit smooth muscle contractionwith minimal depolarization and negligible Ca2+ influx.Funhermore, even for agonists such as serotonin or nor-epinephrine. which activate a Ca2+-influx pathway, theobserved increase in [Ca2+L is out of proponion to thatexpected from Ca2+ influx alone. Thus, another pathwaymust exist for increasing [Ca2+]j. Some agonists causesmooth muscle contraction by triggering the productionof IP) (p. 100). which binds to a specific receptor on the

MALIGNANT HYPERTHERMIA
Malignant hyperthermia (MH) is a genetic disorder affect- lows a mendelian autosomal-dominant pattem. Cloninging between 1 in 10,000 and 1 in 50,000 individuals. of the gene (RyRl) encoding the Ca2+-release channelAffected individuals are at risk for a potentially life-threat- (ryanodine receptor) allowed genetic linkage analysis toening syndrome when exposed to any of the various demonstrate that human MH is closely linked in someinhalation anesthetic agents, particularly halothane. Ad- families to the RyRl gene on chromosome 19. In swine,ministration of succinylcholine can also trigger or exag- MH results from a single amino-acid substitution in RyRlgerate MH. This drug is a short-acting inotropic (nico- (Cys for Arg at position 614). An analogous substitutiontinic) acetylcholine-receptor antagonist that acts by first is present in some human kindreds as well. This substitu-opening the acetylcholine receptor channel and then tion increases the probability that the Ca2+-release chan-blocking it, thereby resulting in a burst of muscle activity, nel will be open. In other families, MH has been associ-followed by paralysis. Onset of the syndrome in the set- ated with other genetic abnormalities in the RyRl gene.ting of the operating room is typified by the develop- In still others, MH does not appear to be geneticallyment of tachypnea (rapid breathing), low plasma [02], linked to the RyRl gene. It is possible that defects inhigh plasma [CO21, tachycardia (rapid heart rate), and other steps along the excitation-contraction cascade canhyperthermia (rising body temperature), as well as rigidity, result in abnormal regulation of muscle contraction andsweating, and dramatic swings in blood pressure. The the MH phenotype. For example, when under anesthesia,patient's temperature may rise as rapidly as 1°C every 5 patients with some forms of muscular dystrophy mayminutes. The onset of MH is usually during anesthesia, have metabolic crises that resemble MH.but it can occur up to several hours later. If untreated, MH also occurs in domestic livestock. The incidence ofthe patient will develop respiratory and lactic acidosis, MH is particularly high In swine, where episodes are trig-muscular rigidity, and a breakdown of muscle tissue that gered by a variety of physical and environmental stressesleads to the release of K+ and thus profound hyperkale- (porcine stress syndrome). MH in animals has significantmia. These episodes reflect a progressively severe hyper- economic importance in view of the potential loss frommetabolic state in the muscle tissues. Fortunately, our fatal episodes and the devaluation of meat as a result ofevolving understanding of the physiology of MH has led muscle destruction during non-fatal episodes.to the development of a therapeutic regimen that has In humans, a condition similar to MH may occur ingreatly improved the once-dismal prognosis. patients treated with neuroleptic agents such as the phe-
The major features of the syndrome-hyperthermia, nothiazines or haloperidol. It is called the neuroleptic mo-muscular rigidity, and an increased metabolic rate-led lignant syndrome and appears to result from abnormallyearly investigators to suggest that MH was a disease of high neuronal input to the muscle cells.abnormal regulation of muscle contraction. According to Therapy for MH now involves administration of thethis hypothesis, uncontrolled muscle contraction-some- drug dantrolene, cessation of anesthesia, and aggressivehow triggered by the administration of halothane and efforts aimed at cooling the body. 08ntrolene is ansuccinylcholine-causes excessive adenosine triphosphate effective therapeutic agent because it blocks excitation-(ATP) hydrolysis to provide energy for contraction. The contraction coupling between T tubules and the SR, thusincreased rate of ATP hydrolysis leads to an increased interrupting the otherwise uncontrolled progression ofmetabolic rate as muscle tries to replenish and sustain its muscular contractions. The drug can be given acutely inATP stores. Hyperthermia develops because of the heat an effort to abort an ongoing attack or, in a personliberated by the hydrolysis of ATP. known to be at risk, it can be given before the initiation
Further support for this hypothesis came from the ob- of anesthesia in order to prevent onset of the syndrome.servation that more tension developed in muscle fibers Therapy also includes intravenous hydration and the judi-obtained by biopsy from susceptible individuals than in cious use of diuretics to keep the urine flowing. The latterfibers from normal individuals when the fibers were ex- lessens damage to the kidneys from the release of break-posed to halothane. 'In muscle fibers from both humans down products, such as myoglobin from the damagedand a strain of swine susceptible to MH, Ca2+-induced muscles. Sodium bicarbonate is given to counter the lac-Ca2+ release from the sarcoplasmic reticulum (SR) is en- tic acidosis, and patients may be mechanically hyperven-hanced when compar'ed with fibers from unaffected sub- tilated to blow off the excess CO2,jects. Furthermore, caffeine, which causes the Ca2+-re- Despite the intensive protocol just outlined, MH is stilllease channels to open, induced greater contractions in associated with high mortality. The relatives of a patientfibers from susceptible subjects. Taken together, these with a documented history of one episode of MH shouldobservations suggested the possibility that MH results be carefully screened to see whether they, too, carry thefrom an abnormality in the Ca2+-release channel in the inherited trait; many of the affected relatives may demon-SR membrane. strate baseline elevations in muscle enzyme levels in their
In both humans and animals, inheritance of MH fol- blood (e.g., an increase in creatine kinase levels).
membrane of the smooth muscle SR (p. 100). This IP3receptor is itself a ligand-gated Ca2+ channel. Thus, areceptor in the plasma membrane can indirectly induceCa2+ release from the SR and hence contraction.
Cr+ fNTRY THROUGH VOLTAGE. INDEPENDENT CHAN-NW. In smooth muscle it is possible that extracellular
Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9 243
ligands may trigger the influx of CaH through eitherligand-gated channels (p. 170) or channels that are acti-vated via G-protein-coupled receptors. Nevenheless, it isnot clear to what extent, if any, these types of CaHchannels contribute to [CaH)i increases in smooth mus-cle. However, another c~ of channel$-5torc-operatec1CaH channels-appears to play an imponant role. Neu-
244 9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
FIGURE 9- 1 O. ExcilJllion-contraclion (E-C) coupling in smooth muscle.inositol f,5-biphosphate; SR, sarcoplasmic reliculum.
rotransmitters that lead to the discharge-and thus thedepletion-of SR Ca2+ stores (Le., second pathway)somehow lead to the activation of store-operated Ca2+channels in the plasma membrane. The Ca2+ enteringthrough these channels allows (Ca2+]j to remain elevatedeven after SR depletion and also appears to replenish SR. Ca2+ stores.
Together, the second pathway for increasing (Ca2+]j(Ca2+ release from the SR) and the third pathway (Ca2+influx through store-operated channels) have been calledphannacomechanical coupling becau~ these excitatoryneurotransmitters and hormones can induce smooth mus-cle contraction that is independent of action-potentialgeneration. Regardless of the source of the Ca2+, the re-sultant increase in (Ca2+L leads to contraction via a Ca2+-CaM-dependent increase in MLCK activity and myosinphosphorylation.
Smooth Muscle Contraction May Also OccurIndependently of Increases in [Ca2+]1Whereas many excitatory stimuli rely on increases in[Ca2+Ji to evoke contraction, some stimuli appear to causecontraction without a measurable increase in [Ca2+J.> Onemechanism by which excitatory stimuli might induceCaH -independent contractions is by modulating the activ-ity of contractile or regulatory proteins directly> Thus, the
Extracellular space
cytosol
DAG, diacylglycerol; IP), inositol l,o4,S-triphosphate; PIP» phosphatidyl
amount of force developed at any given [Ca2+]j may vary.This force/[Ca2+); ratio may be increased or decreased andis generally higher during pharmacomechanical activationthan during depolarization-activated contractions. Becausephosphorylation of the myosin light chain (MLC) is amajor determinant of contractile force in smooth muscle,Ca2+ -independent contractions may result either from anincrease in the rate of MLC phosphorylation by MLCK orfrom a decrease in the rate of MLC dephosphorylation byMLC phosphatase. One second-messenger system that candecrease the activity of phosphatases is protein kinase C(PKC) (p. 102). Some excitatory stimuli are therefore ca-pable of initiating smooth muscle contraction by inducingIP)-mediated release of Ca2+ from intracellular stores, aswell as by producing PKC-mediated decreases in MLCphosphatase activity. These pathways are further examplesof pharmacomechanical coupling.
TERMINA TINCi CONTRACTION
In Skeletal, Cardiac, and Smooth Muscle,Terminating Contraction Requires Re-Uptakeof Ca2+ Into the Sarcoplasmic Reticulum
After the contraction-activating stimulus has subsided,CaH must be removed from the cytoplasm for contrac-

cr+.
~
FIGURE 9- 11. Mechanisms of CaH removal from the cytoplasm.
tion to cease and for relaxation to occur. CaH may beextruded across the cell membrane or sequestered withinintracellular compartments (Fig. 9-11).
The cell may extrude CaH using either an Na-Ca ex-changer (NCX. p. 68) or a CaH pump at the plasmamembrane (PMCA. p. 64). Extrusion across the cell mem-brane. however. would eventually deplete the cell of Ca2+and is therefore a minor mechanism for CaH removalfrom the cytoplasm. Instead, Ca2+ re-uptake into the SRis the most important mechanism by whichthe cell returns [Ca2+)1 to resting levels. CaH re-uptakeby the SR is mediated by a SERCA-type CaH pump(p. 64). .
It is possible that the rate of CaH re-uptake into theSR may be regulated by modulating the activity of the SRCa2+ pump. For example. in cardiac muscle. SR Ca2+-pump activity is inhibited by the regulatory protein phos-pholamban. When phospholamban is phosphorylated bycyclic adenosine monophosphate (cAMP)-dependent pro-tein kinase (PKA). its ability to inhibit the SR CaH pumpis lost. Thus, activators of PKA. such as the neurotrans-mitter epinephrine. may enhance the rate of cardiac my-ocyte relaxation (p. 525).
SR CaH_pump activity is also inhibited by high [CaH)within the SR lumen. This inhibition of SR Ca2+-pumpactivity is delayed by CaH -binding proteins within the SRlumen. These Ca2+-binding proteins buffer the [CaH) in-crease in the SR during Ca2+ re-uptake and thus mark-edly increase the CaH capacity of the SR. The principalCa2+ -binding protein in skeletal muscle, calsequestrin, isalso present in airdiac and some smooth muscle. Calre-
245Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9
ticulin is a ubiquitous Ca2+ -binding protein that is foundin panicularly high concentrations within the SR ofsmooth muscle. These proteins have a tremendous capac-ity to bind Ca2+, with up to 50 binding sites per proteinmolecule.
Ca2+ -binding proteins are not located diffusely withinthe SR. Rather, calsequestrin is highly localized to theregion of the SR immediately beneath the triad junction.Calsequestrin appears to bind directly at the triad, whereit forms a complex with the Ca2+ -release channel andwith two other triad proteins, junctin and triadin. Here,calsequestrin is poised not only to aid muscle relaxationby buffering Ca2+ within the SR lumen but also to unloadits Ca2+ in the vicinity of the Ca2+ -release channel andthus facilitate EC coupling. It has been hypothesized thatEC coupling promotes Ca2+ release from calsequestrin,making Ca2+ available for exit from the SR.
In Smooth Muscle, TerminatingContraction Also RequiresDephosphorylation of theMyosin light ChainBecause Ca2+ triggers smooth muscle contraction by in-ducing phosphorylation of the myosin regulatory lightchain. merely restoring [CaHJ; to its low resting valuemay not allow muscle relaxation. Rather, relaxation ofsmooth muscle requires MLC dephosphorylation, which isaccomplished by myosin light chain phosphatase. Thisphosphatase is a heterotrimer consisting of subunits withmolecular masses of 130, 20, and 37 kDa. The 130-kDasubunit confers specificity by binding to myosin, whereasthe 37 -kDa protein is the catalytic subunit responsible forthe dephosphorylating activity. .
REGULATING MUSCLE CONTRACTION
Muscle Contractions Produce Force and/orShortening and, in the Extreme, Can BeStudied Under Either Isometric or IsotonicConditionsThe total force generated by a muscle is the sum of theforces generated by many independently cycling actin-myosin cross-bridges. The number of simultaneously cy-cling cross-bridges depends substantially on the initiallength of the muscle fiber and on the pattern or fre-quency of muscle-cell stimulation. When muscle is stimu-lated to contract, it exerts a force tending to pull theattachment points at either end toward each other.This force is referred to as the tension developed by themuscle.
Two mechanical-and artificial-arrangements can beused to study muscle contraction. In one, the attachmentpoints are immobile, thereby fixing the muscle lrngth.Here, stimulation causes an increase in tension, but noshortening. Because these contractions occur at constantlength, they are referred to as isometric contractions(Fig. 9-1lA). In the second arrangement, one of the twoattachment points is mobile, and a force-or load-

9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle246
B ISOTONIC
Velocity
FIGURE 9-12. Isometric and isotonic conuaction. A. Experimental preparation for studying muscle contraction under isometric conditions. B,Experimental preparation for studying muscle contraction under isotonic conditions. C. The "passive" curve represents the tension that is measured atvarious muscle lengths prior to muscle contraction. The "Iola!" curve represents the tension that is measured at various muscle lengths during musclecontraction. D. The "active" tension is the difference between the "total" and the "passive" tensions in C. E, Each of the three blue curves shows that thevelocity of muscle shortening is faster if the muscle lifts a lighter weight-it is easier to lift a feather (left side of each curvel1ow load) than to lift abarbell (right side of each curvelhigh load). The three blue curves also show that, for any given velocity of shortening, a longer muscle can develop agreater tension than can a shorter muscle.
C LENGTH-TENSION DIAGRAM (ISOMETRIC)
100
75
50
25
0
100
75
50
25
0
T enaion
70 85 100 115Length
130 145
D "ACTIVE" LENGTH-TENSIONDIAGRAM (ISOMETRIC)
Activetension
70 85 130 145100 115Length
E LOAD-VELOCITY DIAGRAM (ISOTONIC)
Velocity of isotonic contraction at 3different initial resting lengths;
Velocity ofshortening
Load (tension)

tends to pull this mobile point away from the fixed one.Here, stimulation causes shonening, provided that thetension developed by the muscle is greater than the op-posing load. Because these shonenings occur at constantload, they are referred to as isotonic contractions (seeFig. 9-128). Both isometric and isotonic contractions canbe examined at different initial muscle lengths. Moreover,they can be measured during individual muscle twitchesthat are evoked by single muscle action potentials, as wellas during other patterns of stimulation.
Muscle Length Influences TensionDevelopment By Determining the Degree ofOverlap Between Actin and Myosin FilamentsThe isometric force of contractions depends on the initiallength of the muscle fiber. Unstimulated muscle may beelongated somewhat by applying tension and stretching it.The tension measured before muscle contraction is re-ferred to as passive tension (see Fig. 9-12C). Becausemuscle gets stiffer as it is distended, it takes increasingamounts of "passive" tension to progressively elongate themuscle cell. If at any fixed length (Lo., isometric condi-tions) the muscle is stimulated to contract, an additionalactive tension develops because of cross-bridge cycling.The total measured tension is thus the sum of the passiveand active tension. This incremental or active tension-the difference between total tension and passive ten-sion-is quite small when the muscle is less than ap-proximately 70% of its normal resting length (see Fig. 9-12D). As muscle length increases toward its normallength, active tension increases. Active tension is maximalat a length-usually called ~-that is near the normalmuscle length. Active tension decreases with furtherlengthening; thus, active tension is again small when themuscle is stretched beyond 150% of its normal restinglength. Although the relationship between muscle lengthand tension has been best characterized for skeletal mus-cle, the tension of cardiac and smooth muscle also ap-pears to depend on length in a similar manner.
247Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle / 9
This length-tension relationship is a direct result of theanatomy of the thick and thin filaments within individualsarcomeres (see Fig. 9-12D). As muscle length increases,the ends of the actin filaments arising from neighboring Zdisks are pulled away from each other. When length isincreased beyond 150% of its resting sarcomere length,the ends of the actin filaments are pulled beyond theends of the myosin filaments. Under this condition, nointeraction occurs between actin and myosin filamentsand hence no development of active tension. As musclelength shonens from this point, actin and myosin fila-ments begin to overlap and tension can develop; theamount of tension developed corresponds to the degreeof overlap between the actin and the myosin filaments. Asthe muscle shonens fuMer, opposing actin filamentsslide over one another and the ends of the myosin fila-ments and-with extreme degrees of shonening-even-tually butt up against the opposing Z disks. Under theseconditions, the spatial relationship between actin and my-osin is distoned and active tension falls. The maximaldegree of overlap between actin and myosin fila-ments, and hence maximal active tension, corresponds toa sarcomere length that is near its normal resting
length.
At Higher Loads, the Velocity of ShorteningIs Lower Because More Cross-Bridges AreSimultaneously ActiveUnder isotonic conditions, the velocity of shortening de-creases as the applied load opposing contraction of themuscle fiber increases. This point is obvious; anyone canlift a single French fry much faster than a sack of pota-toes. As shown for any of the three blue curves in Figure9-12E-each of which represents a different initiallength of muscle - the relationship between velocity andload is hyperbolic. Thus, the smaller the load applied tothe muscle, the greater its velocity of shortening. Con-versely, the greater the load, the lower the velocity of
shortening.

Z48 9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
A EXPERIMENTAL PREPARATION
8 ISOTONIC30
Displacement ~~
~ . }Distance :ll1 } Force of (nm) actin moves Force 4 a 8ingIe
0 In one croa- (pH) 2 CfO8S-bridgebridge cycle 0 cycle
0.0 0.5 1.0 1.5 0.0 02 0.4 0.8TIme (see) Time (see)
FIGURE 9- 13. Microscopic measurem=rs of cross-bridgf: force and displacement A, An actin filament is attached at each end to a poIystyrcM bead.The "optical tweezers: a finely focused beam of laser ligtll, can "trap" the bead at Irs focal point and physically move it. By adjusring the laserintensity. the experimenter can alter the strength of the trap (I.e., the force with which the bead is held). In this experiment. two optical tweezers wereused to suspend the actin filament above a coverglass. AtlaCbcd to this coverslip is a silica bead. and myosin molecules are bound to the bead. B, Inan "isotonic" experiment. the force ~n the actin filamcnt and the fixed myosinIsilica bead is kept COOSWIt by using a stable laser intenSity. Theexperimenter measures, as a (unction of time, the displaccmcnt of the polystyrene bead (blue) away from the center of the trap. Thus. in one CTO55-bridge cycle. the myosin-actin interaction pulls the polystyrene bead approximately 11 nm away from the center of the trap. Co In an "Isometric'experiment. the cxperirncnter mC2$UTCS, as a funaion of time. the extra force that needs to be applied (i.e., Increase in laser intensity) to keep thepolystyrene bead (blue) at a fixed position near the center of the trap. Thus. in one cross-bridge cycle, the myosin-actin interaCtion exerts a force ofapproximately 5 pN. (Data (rom Finer ]T. Mehta AD. Spudich JA: Characterization of single actin-myosin interactions. Biophys J 68:2915-2965. 1995.)
20Displacement 1 0(nm) 0
The load (or tension)-velocity relationship is perhapsbest understood by considering the situation at maximumload for a resting muscle length (Le.. ~tric conditions).This situation is represented by the upper bl~ curve inFigure 9-12E. At any time. aU the available cross-bridgesare engaged in resisting the opposing force. None are leftover to make the muscle shonen. If the number of en-gaged cross-bridges were decreased. the muscle wouldlengthen. At a slightly smaller load but at the same iso-tonic muscle lenM. fewer cross-bridlles need to be en-gaged to resist the opposing load. -Thus. extra cross-bridges are available to ratchet the thick myosin filamentsover W thin actin filaments, but at a very low velocity.At a still lower load, even more cross-bridges are availablefor ratcheting the myosin over the actin, and the velocityincreases funher. At very low loads, it is reasonable toexpect that as the myosin filament slides along the actinfilament, only a tiny fraction of the actin monomers need
\GISSScoverslip
cC ISOMETRIC1°
L8 Force 6
(pH) ~
} Fon:e of
~
DIst8nce} actin moves
in one cross-bridge cyde
to interact with myosin heads to overcome the load. Un-der these conditions of vanishingly small loads, the speedwith which the thick and thin filaments slide over eachother is limited only by the time that it takes for theATP-consuming cross-bridge cycle to occur. With increas-ing velocity, the probability of actin-myosin interactionsdecreases. Thus, fewer cross-bridges are simultaneouslyactive at higher shonening velocities, and less tensiondevelops.
Note that the upper blue curve in Figure 9-12E appliesto a particular initial length of the muscle, that is, theresting length. We already saw in Figure 9-12C that thetotal isometric tension (Le., the maximal load that themuscle can sustain at zero velocity) increases with initialmuscle length. This principle is confirmed in Figure 9-12E: the longer the initial length, the larger the maximalload under zero-velocity conditions (i.e., (he three differ-ent intercepts with the abscissa). In contrast to this maxi-

SINGLE MUSCLE TWITCHES B TEMPORAL SUMMATION(5 Hz) (10 Hz)
rJ .f 1< 'I J J
Time TimeFrequency summation of skeletal muscle twitches.9-14.
load. which depends very much on length. maximal. is independent of length. as shown by the com-intercept of the family of curves with the ordinate.explanation for this effect-as we have already1- is that maximal velocity (at no load) depends on
.. maximal rate of cross-bridge turnover. not on the, overlap of the thin and thick filaments.
velocity-tension curve reveals an interesting rela-. between muscle power and applied load. Muscle
measurable mechanical work only when it displaces. This mechanical work (W) is the product of load
md displacement (~). Power (P) is the rate at whichis performed. or work per unit time (At):
P = W/4t = F X !1xJ4t
velocity (v) is 4x/4t, it follows that
P = F x v Equation 9-2
For a given load (F), we can calculate the power byg the velocity (v) from the uppermost of the three
load-velocity relationships in Figure 9-12E. Power isat intermediate loads (where both F and v are
rate) and falls to zero at max;imum load (where= 0) and at zero load (where F = 05.
, a Single Skeletal Muscle Fiber, the Forceloped May Be Increased By Summing
Multiple Twitches In TimeAt sufficiently low stimulation frequencies, the tensiondeveloped falls to the resting level between individualtwitches (Fig. 9-14A). Single skeletal-muscle twitches lastbetween 25 and 200 msec, depending on the type ofmuscle. Although each twitch is elicited by a single mus-cle action potential, the duration of contraction is longwhen compared with {he duration of the exciting actionpotential, which lasts only several milliseconds. Becausethe muscle twitch far exceeds the duration of the actionpotential, it is possible to initiate a second action potentialbefore a first contraction has fully subsided. When this
Cellular Physiology of Skeletal, Cardia<:, and Smooth Muscle / 9 249
c UN FUSED TETANUS D FUSED TETANUS(50 Hz)(25 Hz)
I~
situation occurs, the second action potential stimulates atwitch that is superimposed on the residual tension of thefirst twitch, thereby achieving greater isometric tensionthan the first (compare Fig. 9-14A and B). This effect isknown as summation.
If multiple action potentials occur closely enough intime, the multiple twitches can summate and thus greatlyincrease the tension developed. Summation is more effec-tive at increasing tension when the action potentials aregrouped more closely in time, as in Figure 9-14C. Inother words, tension is higher when action potentials areevoked at higher frequency. Because this type of tensionenhancement depends on the frequency of muscle stimu-lation, it is referred to as frequency summation.
When the stimulation frequency is increased suffi-ciently, the individual twitches occur so closely togetherin time that they fuse (see Fig. 9-14D) and cause themuscle tension to remain at a steady plateau. The state inwhich the individual twitches are no longer distinguish-able from each other is referred to as tetanus. Tetanusarises when the time between successive action potentialsis insufficient to return enough CaH back to the SR tolower [Ca2+]t below a level that initiates relaxation. Infact, a sustained increase in [Ca2+]t persists until the te-tanic stimulus ceases. At stimulation frequencies abovethe fusion frequency that causes tetanus, muscle fibertension increases very little.
Equation 9-1
In a Whole Skeletal Muscle,'the ForceDeveloped May Be Increased By Summingthe Contractions of Multiple Fibers
In addition to detennining the frequency with which itstimulates a single muscle fiber, the central nervous sys-tem (CNS) can control muscle force by determining thenumber of individual muscle fibers that it stimulates at agiven time. As each additional motor-neuron cell bodywithin the spinal cord is excited, those muscle fibers thatare pan of the motor unit of that motor neuron are addedto the contracting pool of fibers (Fig. 9-15). This effect isknown as multiple-fiber summation. Generally, smallermotor neurons serve motor units consisting of fewer indi-vidual muscle fibers. Because a given excitatory stimuluswill generate a larger excitatory postsynaptic potential (p.

250 9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
A MOTOR UNIT
FIGURE 9- 15. The mOlor unil and lhe motor-neuron pooL
212) in motor neurons with smaller cell bodies, the smallmotor units are recruited even with minimal neuronalstimulation. As neuronal stimulation intensifies, largermotor neurons innervating larger motor units are alsorecruited. The progressive recruitment of first small andthen larger and larger motor units is referred to as thesize principle. The group of all motor neurons innervat-ing a single muscle is called a motor-neuron pool.
Multiple-fiber summation, sometimes referred to asspatial summation, is an imponant mechanism that al-lows the force developed by a whole muscle to be rela-tively constant in time. It is true that the CNS coulddirect the force to be relatively constant over time merelyby driving a fixed number of motor' units within themuscle to tetanus, where the force fluctuations are verysmall (see Fig. 9-14D). However, adding tetanic motorunits would increase total muscle force by rather largeindividual increments. Instead, the CNS can activate indi-vidual motor units asynchronously so that some units aredeveloping tension while others are relaxing. Thus,whole-muscle force can be relatively constant with time,even when individual fibers are not stimulated to tetanus.Smooth, non tetanic contraction is essential for fine motorcontrol.
In Cardiac Muscle, Increasing the Entry ofCa2+ Enhances the Contractile ForceWhereas frequency summation and multiple-fiber summa-tion are imponant mechanisms for regulating the strengthof skeletal-muscle contractions, these mechanisms would
not be consistent with the physiological demands of car-diac muscle. Because cardiac muscle must contract onlyonce with each heanbeat and must fully relax betweeneach contraction, frequency summation is precluded. Fur-thermore, the extensive electrical coupling between car-diac myocytes, as well as the requirement that cardiacmuscle contract homogeneously, eliminates the potentialfor multiple-fiber summation. Therefore, the strength ofcardiac muscle contraction must be regulated by modulat-ing the contractile force generated during each individualmuscle twitch. This type of regulation is an imponantpan of the adaptive response to exercise and is mediatedby norepinephrine, a neurotransmitter released by thesympathetic nervous system.
Because an increase in [Ca2 + ] j activates contraction byremoving the inhibitory influence of the regulatory pro-teins, it is reasonable to consider that contractile functionmay be regulated either by modulating the magnitude ofthe rise in [CaH I. or by altering the Ca2+ sensitivity ofthe regulatory proteins. In fact, both these mechanismsare imponant in controlling the force of cardiac musclecontraction.
In cardiac muscle, a significant proponion of the acti-vator Ca2+ enters the cell via voltage-gated CaH channelsthat open during the cardiac action potential. Most of thisCaH influx occurs via L-type Ca2+ channels. How doesnorepinephrine increase the contractile force of the hean?This hormone acts through the J3-type adrenergic receptorto increase the generation of cAMP, activate PKA (p. 97).and in turn phosphorylate the L-type Ca2+ channels,thereby increasing the passive influx of Ca2+. An in-creased [Ca2+]; leads to an increase in contractile force.The cAMP pathway also appears to increase the Ca2+sensitivity of the contractile apparatus by phosphorylatingone or more of the regulatory proteins. Thus, cAMP causesan increase in the force generated for any given [Ca2+]j'
Reciprocal control over Ca2+ entry is provided by cyclicguanosine monophosphate (cGMP)-dependent phosphor-ylation of the L-type Ca2+ channels. Acetylcholine, actingthrough muscarinic ACh receptors, raises intracellularcGMP concentrations. In turn. the cGMP-dependentphosphorylation of L-type Ca2+ channels, at sites distinctfrom those phosphorylated by the cAMP-dependent kinase.causes a decrease in Ca2+ influx during the cardiac actionpotential and thus a decrease in the force of contraction.
CaH entry may also be regulated indirectly by modu-lating other ion channels so that they either change theirCa2+ permeability or alter the duration of the action po-tential. Norepinephrine, for example, may increase theCaH permeability of voltage-gated Na+ channels. Receptortransduction mechanisms that inhibit voltage-gated K+currents may prolong the cardiac action potential andthereby increase net Ca2+ influx through L-type Ca2+channels without modulating the Ca2+ channels them-selves.
B MOTOR NEURONPOOL
In Smooth Muscle, Contractile Force IsEnhanced By Increasing the Entry of Ca2+, AsWell As By Increasing the Ca2+ Sensitivity ofthe Contractile ApparatusUnlike skeletal muscle, in which force development re-sults from the summation of individual muscle twitches,

smooth muscle cells can maintain a sustainedthat can be graded in strength over a wide
. tile force in smooth muscle largely dependsrelative balance between the phosphorylation and
.orylation of MLCs, The rate of MLC phospho-is regulated by the Ca2+-CaM complex, which in
depends on levels oj intracellular Ca2+, Smooth mus-, can regulate [Ca2+L over a wider range than
1 and cardiac muscle can for several reasons, First,smooth muscle cells do not generate action poten-Rather, their membrane potential varies slowly in
to neurotransmitters or hormones, This gradedof V m allows finer regulation of CaH influx
gh voltage-gated channels, Second, release of Ca2+intracellular stores may be modulated through neu-
'tter-induced generation of intracellular second~gers such as IP3, This modulation allows finer con-
of Ca2+ release than occurs in the SR Ca2+ releaseel by L-type Ca2+ channels in skeletal and cardiac
-Ie,second level of control over contractile force occurs
lating the Ca2+ sensitivity of proteins that regulate~tion, For example, inhibiting myosin light chain
. alters the balance between phosphorylation
dephosphorylation, in effect allowing a greater con-n at a lower [CaH];, Some neurotransmitters act by
. , the phosphatase, which appears to occur
activation of G-protein-coupled receptors. An-mechanism for governing the Ca2+ sensitivity of
that regulate contraction is alteration of the Ca2+, of the myosin light chain kinase, For example,
itself is phosphorylated at specific sites by severalkinases, including PKA, protein kinase C, and
+-CaM-dependent kinases, Phosphorylation by any ofkinases decreases the sensitivity of MLCK to activa-
by the Ca2+ -CaM complex.
Muscle Maintains High Force at Lowergy Consumption
muscle is often called upon to maintain highfor long periods. If smooth muscle consumed A TP
rates similar to striated muscle, metabolic demandsld be considerable and the muscle-,vould be prone to
-, Unlike striated muscle, however, smooth muscleable to maintain high force at a low rate of ATP
olysis. This low-energy consumptionlhigh-tensione is referred to as the latch state, The latch state in
muscle is unique because high tension can be'tained despite a decrease in the degree of muscle'ation by excitatory stimuli. As a result, force is main-
at a lower level of MLCK phosphorylation,The mechanism underlying the latch state is not en-
y known, although it appears to be due in large panchanges in the kinetics of actin-myosin cross-bridge
- . tion and detachment. These changes may be a direct
iresult of a decrease in the rate at which dephosphorylatedFross-bridges detach. Tension is directly related to the, umber of attached cross-bridges, Funhermore, the pro-
nion of myosin heads cross-bridged to actin is relatedto the ratio of attachment rates to detachment rates.
251Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle I 9
Therefore, it is reasonable to expect that a decrease in thedetachment rate would allow a greater number of cross-bridges to be maintained and would result in a lower rateof cross-bridge cycling and ATP hydrolysis. Thus, smoothmuscle appears to be able to slow down cross-bridgecycling just before detachment, a feat that can be accom-plished in skeletal muscle (see Fig. 9 - 7) only at low A TPlevels (as in rigor mortis).
DIVERSITY AMONG MUSCLES
Each muscle type (Le., skeletal, cardiac, and smooth) isdistinguishable on the basis of its unique histology, EC-coupling mechanisms, and regulation of contractile func-tion. However, even within each of the three categories,muscle in different locations must serve markedly differ-ent purposes, with different demands for strength, speed,and fatigability. This diversity is possible because of dif-ferences in the expression of specific isoforms for variouscontractile and regulatory proteins (Table 9-1).
Skeletal Muscle Is Composed of Slow-Twitchand Fast-Twitch FibersSome skeletal muscles must be resistant to fatigue and beable to maintain tension for relatively long periods, al-though they need not contract rapidly. Examples aremuscles that maintain body posture, such as the soleusmuscle of the lower pan of the leg. In contrast. somemuscles need to contract rapidly, yet infrequently. Exam-ples are the extraocular muscles. which must contractrapidly to redirect the eye as an object of visual interestmoves about.
Individual muscle fibers are classified as slow twitch(type 1) or fast twitch (type II). depending on their rate offorce development. These fiber types are also distin-guished by their histologic appearance and their ability toresist fatigue.
Slow-twitch fibers (Table 9-2) are generally thinnerand have a more dense capillary network surroundingthem. Slow-twitch fibers also appear red because of alarge amount of the oxygen-binding protein myoglobin(p. 656) within the cytoplasm. This rich capillary networktogether with myoglobin facilitates oxygen transpon tothe slow-twitch fibers, which mostly rely on oxidativemetabolism for energy. The metabolic machinery of theslow-twitch fiber also favors oxidative metabolism becauseit has low glycogen content and glycolytic-enzyme activitybut a rich mitochondrial and oxidative-enzyme content.
Fast-twitch fibers differ among themselves with re-spect to fatigability. Some fast-twitch fibers are fatigueresistant; they rely on oxidative metabolism (type IIa)and are quite similar to slow-twitch fibers with respect tomyoglobin content (indeed, they are red) and metabolicmachinery. One important difference is that fast-twitchoxidative fibers contain abundant glycogen and have agreater number of mitochondria than slow-twitch fibersdo. These features ensure adequate ATP generation tocompensate for the increased rate of ATP hydrolysis infast-twitch fibers.

9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle252
MlC-1 as, -1 bS
Present
"Fast" and "car-diac"
Myosin light chain
SR Ca ATPase SERCA2a
Other fast -twitch fibers are not capable of sufficientoxidative metabolism to sustain contraction. Because thesefibers must rely on the energy that is stored within glyco-gen (and phosphocreatine), they are more easily fatigable.Fatigable fast-twitch fibers (type lib) have fewer mito-chondria and lower concentrations of myoglobin and oxi-dative enzymes. Because of their low myoglobin content,type lIb muscle fibers are white. They are, however, richerin glycolytic enzyme activity than other fiber types are.
In reality, slow- and fast-twitch fibers represent theextremes of a continuum of muscle fiber characteristics.Moreover, each whole muscle is composed of fibers ofeach twitch type, although in any given muscle one of thefiber types predominates. The differences between fibertypes derive in large part from differences in isoformexpression of the various contractile and regulatory pro-teins (see Table 9-1).
Differences in the rate of contraction, for example, maybe directly correlated with the maximal rate of myosinATPase activity. As many as 10 different myosin heavy
TABLE 9-2
, - ~
SLOW TWITCH FAST TWITCH FAST TWITCH, . "Synonym Type I Type lIa Type lib . ~ -
Fatigue Resistant Resistant Fatigable
Color Red (myoglobin) Red (myoglobin) White (low myoglobin)
Metabolism Oxidative Oxidative Glycolytic
Mitochondria High Higher Fewer
MlC-17a, -17bMlC-1f, -3f
SERCA 1
MlC-lv, -laSERCA2a
MLC-lf, -3f
SERCA 1 SERCAla, 2b(b > > > a)
chain isoforms have been identified. Individual isoformexpression varies among muscle types and is developmen-tally regulated. At least four isoforms of the MHC proteinare expressed in skeletal muscle (MHC-I, MHC-lla, MHC-lIb, MHC-Ilx/d). For the most part, a muscle fiber typeexpresses a single MHC isoform, the ATPase activity ofwhich appears to correspond to the rate of contraction inthat fiber type. Whereas most fibers express one of theseisoforms, some fibers express a combination of two differ-ent isoforms. These hybrid cells have rates of contractionthat are intermediate between the two pure fiber types.
Differences in the rates and strength of contraction mayalso result from differences in myosin light chain isoformexpression or from isoform differences among other com-ponents of the EC coupling process. Three skeletal mus-cle isoforms have been identified. MLC-las and MLC-lbsare expressed in slow-twitch fibers, whereas MLC-lf andMLC-3f are expressed in fast-twitch fibers.
Isoform differences also exist for the SR Ca2+ pump(Le., the SERCA) , calsequestrin, the Ca2+-release channel,

C. Furthermore, some proteins, such asm, are expressed in one fiber type (slowot the other.lIarly interesting feature of muscle differenti-t fiber-type determination is not static.cise training or changes in patterns of neu-:ion, alterations in contractile and regulatorym expression may occur. For example, it isI greater proportion of fast-twitch fibers tospecific muscle with repetitive training. It isto induce cardiac-specific oofonns in skele-
..en appropriate stimulation patterns.
rties of Cardiac Cells Vary withI the Heart
il muscle consists of multiple fiber types, sort muscle. The electrophysiological and me-enies of cardiac muscle vary with their loca-II versus conducting system versus ventricle),:n among cells within one anatomic location,£erences may exist between muscle cells nearf the hean (tpicardial cdls) and those lining£ the same chambers (endocardial cells). As in:le, many of these differences reflect differ-.rm expression of the various contractile andoteins. Although some of the protein 00-sed in cardiac tissue are identical to those
Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle I 9 251
1S expressed in skeletal muscle, many of the proteins havew cardiac-specific isoforms (see Table 9-1). The MHC in
hean, for example, exists in two isoforms, a and {J,i- which may be expressed alone or in combination.c..1-ry Smooth Muscle Cells May Differ Markedlyis Among Tissues and May Adapt Theirto Properties with Time Even In a Single Tissueis When one considers that smooth muscle has a broade- range of functions, including regulating the diameter of
blood vessels, propelling food through the gastrointestinaltract, regulating the diameter of airways, and delivering anewborn infant from the uterus, it is not surprising thatsmooth muscle is a particularly diverse type of muscle. Inaddition to being distinguished as unitary or multiunit
;0 muscle (p. 231), smooth muscle in different organs di-e- verges with respect to nerve and hormonal control, elec-a- trical activity, and characteristics of contraction.~). Even among smooth muscle cells within the same sonn, of tissue, important functional differences may exist. Forar example, vascular smooth muscle cells within the walls of18 two anerioles that perfuse different organs may vary inin their contractile response to various stimuli. Differences:r- may even exist between vascular smooth muscle cells atkd two different points along one anerial pathway.0- The phenotype of smooth muscle within a given organse may change with shifting demands. The uterus, for exam-
25)

254 9 / Cellular Physiology of Skeletal, Cardiac, and Smooth Muscle
pIe, is composed of smooth muscle-the myometrium-that undergoes remarkable transformation during gesta-tion as it prepares for panurition (see Chapter 55). Inaddition to hypenrophy, greater coupling develops be-tween smooth muscle cells through the increased forma-tion of gap junctions. The cells also undergo changes intheir expression of contractile protein isoforms. Changesin the expression of ion channels and hormone receptorsfacilitate rhythmic electrical activity. This activity is coor-dinated across the myometrium by propagation of actionpotentials and increases in [CaHL through the gap junc-tions. These rhythmic, coordinated contractions developspontaneously, but they are strongly influenced by thehormone oxytocin, levels of which increase just beforeand during labor and just after panurition.
These differences in smooth muscle function amongvarious tissues or even over the lifetime of a single cellprobably reflect differences in protein composition. In-deed, in comparison to striated muscle, smooth musclecells express a wider variety of isoforms of contractile andregulatory proteins (see Table 9-1). This variety is aresult of both multiple genes and alternative splicing (p.139). This richness in diversity is likely to have imponamconsequences for smooth muscle cell function, althoughthe precise relationship between the structure and func-tion of these protein isoforms is not yet clear.
Smooth Muscle Cells Express a Wide Varietyof Neurotransmitter and Hormone ReceptorsPerhaps one of the most impressive sources of diversityamong smooth muscle relates to differences in responseto neurotransmitters, environmental factors, and circulat-ing hormones. Smooth muscle cells differ widely withrespect to the types of cell-surface receptors that mediatethe effects of these various mediators. In general, smoothmuscle cells each express a variety of such receptors, andreceptor stimulation may lead to either contraction orrelaxation. Many substances act through different receptorsubtypes in different cells, and these receptor subtypesmay act through different mechanisms. For example,whereas some neurotransmitter/hormone receptors maybe ligand-gated ion channels, others act through heterotri-
meric G proteins that either act directly on tar~ets or actthrough intracellular second messengers such -as cAMP.cGMP, or IP3 and DAG.
The list of neurotransmitters, hormones, and environ-mental factors regulating the function of vascular smoothmuscle cells alone is vast (see Chapter 22). A few of thesevasoactive substances include epinephrine, norepineph-rine, serotonin, angiotensin, vasopressin, neuropeptide Y,nitric oxide, endothelin, and oxygen. Identical stimuli,however, may result in remarkably different physiologicresponses by smooth muscle in different locations. Forexample, systemic anerial smooth muscle cells relax whenthe oxygen concentration around them decreases, whereaspulmonary anerial smooth muscle contracts when localoxygen decreases (p. 699).
See Table 9-3 for a comparison of muscle types.
REFERENCES
Books and Reviews
Farah CS, Relnacb FC: The troponln complex and regulation of musclecontraction. FASEB J 9:755- 767, 1995.
Franzini-Annstrong C. Protasi F: Ryanodine receptors of striated mus-cles: A complex channel capable of multiple interactions. Pbysiol Rev77:699-729. 1997.
Holda J. Klishin A. Sedova M, et al: Capacitative calcium entry. NewsPhysiol Sci 13:157-163, 1998.
Horowitz A. Menke CB, Lapone R. Morgan KG: Mechanisms of smoothmuscle contraction. Physiol Rev 76:967-1003. 1996.
Parekh AB, Penner R: Store depletion and calcium influx. Physiol Rev77:901-930, 1997.
Striggow F, Ehrlich BE: Ugand-gated calcium channels inside and out.CUrT Opin Cell BioI 8:'190-+95, 1996.
Journal Ankles
Cannell MB, Cheng H, Lederer W]: The control of calcium release inhean muscle. Science 268:1M5-1049, 1995.
Finer JT, Simmons RM, Spudich JA: Single myosin molecule mechanics:Piconewton forces and nanometer steps. Nature 368:113-119,1994.
Gordon AM, Huxley AF, Julian F]: The variation in isometric tensionwith sarcomere length in venebrate muscle. J Physiol 1&4:170-192,1966.
Mickelson JR. Louis CF: Malignant hyperthennia: Excitation-contractioncoupling, Ca2+ release channel. and cell Ca2+ regulation defects. Phy-sial Rev 76:537-592, 1996.