cbt for post traumatic stress disorder (ptsd) leslie sokol, ph.d
TRANSCRIPT

CBT
For
Post Traumatic Stress Disorder
(PTSD)
Leslie Sokol, Ph.D.
PTSD
About 5.2 million adults have PTSD during a given year. This is a small portion of people who have experienced trauma.
Up to 60% of the U.S. population is exposed to at least one traumatic event in their lifetime.

PTSD
Lifetime prevalence of PTSD in U.S. if approximately 8%
For veterans of the Iraq and Afghanistan wars, PTSD prevalence rate is estimated to be 11-20%
Women are twice as likely to develop PTSD than men Note: women are more likely to report and
mostly interpersonal trauma (rape/abuse)

PTSD is associated with higher odds for:
School dropout Teenage childbearing Marital instability Unemployment Suicide attempts Substance abuse Inpatient hospitalization

Type of Trauma War trauma Domestic violence Rape Motor vehicle accident Witnessing a murder or other violent act Industrial accident Childhood abuse Natural disasters Traumatic grief Severe medical illness (HIV, Cancer)
DSM-5 Diagnostic Criteria Released May 2013 Includes changes to diagnostic criteria
for PTSD and Acute Stress Disorder Criteria was revised to take into account
data from scientific research and clinical experience
NIH may reject the DSM 5 and use the RDOC tool instead

Major Revisions PTSD (as well as Acute Stress Disorder)
were moved from class of anxiety disorders to a new class: “TRAUMA and STRESSOR –RELATED DISORDERS
All of the conditions in this classification require exposure to a traumatic or stressful event

Other changes
Symptoms were revised to clarify symptom expression
Criterion A2 (requiring fear, helplessness or horror happen right after the trauma) was removed in DSM-5. Research suggested that Criterion A2 did not improve diagnostic accuracy

Criterion A: Stressor (1 required)
The person was exposed to: death, threatened death, actual or threatened serious injury, or actual or threatened sexual violence, as follows:
1. Direct exposure
2. Witnessing, in person

3. Indirectly, by learning that a close relative or close friend was exposed to trauma. (If death must be violent or accidental)
4. Repeated or extreme indirect exposure to aversive details of the event, usually in the course of professional duties. Does not include exposure through media, tv, movies.

There a more opportunities to fit the criteria so the concern is the diagnosis is being watered down. However, the problem must be debilitating to fit the criteria.

Criterion B: Intrusion (1 required)
1. Recurrent, involuntary and intrusive memories.
2. Traumatic nightmares
3. Dissociative reactions
4. Intense prolonged distress after exposure to reminders,
5. Marked physiologic reactivity

Key Alterations
Note: mostly DSM-IV and 5 are same Now 4 clusters instead of 3
Intrusion, avoidance, negative alterations in cognitions and mood, and alternations in arousal and reactivity
Criterion C: avoidance and numbing is now 2 criteria
Criteria C (avoidance) Criteria D (negative alternations in cognitions and mood)
Criterion C: Avoidance(1 required)
Persistent effortful avoidance of trauma-related stimuli:
1. Thoughts and feelings
2. External reminders (people, places, conversations, activities, situations, etc.)
NOTE avoidance makes patients very difficult to treat.

new symptoms addedCriteria D is a new
cluster Criteria D: ( negative alternations in cognitions and mood) 2 required
1. Inability to recall key features of event
2. Persistent negative beliefs about oneself
3. Persistent distorted blame (self or others) New symptom
4. Persistent negative emotions New Symptom

Criterion D. Continued
5. Markedly diminished activities
6. Feeling alienated from others
7. Constricted affect

Criterion E: alterations in arousal and reactivity (2
required)1. Irritable or aggressive behavior
2. Self-destructive or reckless behavior
3. Hypervigilance
4. Exaggerated startle response
5. Concentration problems
6. Sleep disturbance
Note if sleep is the predominant symptom in the first 30 days, high predictor (80%) convert to PTSD

Criterion F: durationPersistence of symptoms (in Criteria B, C, D and E) for more than one month.

Criterion G: functional significanceSignificant symptom-related distress or functional impairment (e.g., social, occupational).

Criterion H: exclusionDisturbance is not due to medication, substance use, or other illness.

Clinical Subtype AddedSpecify if:
With dissociative symptoms (depersonalization or derealization)This subtype is applicable to individuals who
meet the criteria for PTSD and experience additional depersonalization and derealization symptoms
1.Depersonalization: experience of being an outside observer of or detached from oneself (e.g., feeling as if "this is not happening to me" or one were in a dream).
2.Derealization: experience of unreality, distance, or distortion (e.g., "things are not real").

Specify if: With delayed expression.Full diagnosis is not met until at least 6 months after the trauma(s), although onset of symptoms may occur immediately.

Children ages 6 and younger
Separate diagnostic Criteria

Prevalence Lower in DSM 5
Revision of Criterion A1 narrowed qualifying traumatic events Unexpected death of family or friend due to
natural causes is no longer included
Splitting Criterion C in two required at least one avoidance symptom

Pre-Traumatic Risk Factors
Gender: Women are at twice the risk. Age: Higher risk under age 25. Childhood trauma and/or adversity. Prior psychiatric disorder (including a pre-
disposed “ability” to dissociate under duress).
Additional adverse life events. Poor physical health; money problems. Family history of trauma (e.g., 2nd
generation Holocaust survivor); psychiatric disorders.
25

Post-Traumatic Risk Factors
Poor social support. Development of Acute Stress Disorder?
(This is the subject of current research). Dissociation at (or just after) the time of
the trauma (also under investigation). Note: Early dissociative responses have
been linked to persistent PTSD only in non-sexual assault victims.
26

Overlap between PTSD and other disorders
Many people with PTSD are misdiagnosed because their presentation overlaps with other disorders (e.g. GAD, OCD, specific phobia, substance abuse, borderline personality disorder)
Can have both PTSD and one or more of the above disorders
PTSD treatment has been shown to diminish symptoms of other disorders along with PTSD

Overlap between PTSD and other disorders
One could have trauma-related difficulties without having full-blown PTSD
Hallmark of PTSD is: a constellation of symptoms grouped into four general clusters: intrusion, avoidance, alterations in cognitions and mood, and alterations in arousal and reactivity.
May oscillate continuously between the four or tend to be mostly “stuck” on one.

Typical Characteristics of PTSD (1)
Re-experiencing (“Reliving”)
Intrusive recollections and flashbacks. Unwanted. Sudden, unexpected, startling. Can interfere with normal ideation.
Traumatic nightmares.
29

Typical Characteristics of PTSD (2)
Avoidance Avoiding thoughts, feelings, activities,
places, and people related to the traumatic event.
“Psychogenic amnesia” for the traumatic event. Physiological reactions may still occur. Vague sense of terror and doom may still occur.
Suppression of feelings. Goal: self-protection. “Side-effect”: Joy, humor, and love are muted.
30

Typical Characteristics of PTSD (3)
Hyperarousal Excessive physiological reactions.
Exaggerated startle reactions. Poor concentration.
Insomnia. Irritability.
31

Typical Characteristics of PTSD (4) The duration of the disturbance
(including symptoms of re-experiencing, avoiding, and hyperarousal) is more than one month.
The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning.
32

Alternative View of PTSD
PTSD can also be conceptualized as a “normal” reaction to abnormal circumstances, extending in time and scope beyond its usefulness.
33

Cognitive Model of PTSD
Nature of Trauma Memory
Matching Triggers
Current ThreatIntrusions, Arousal and Emotions
Negative Appraisals
Strategies Intended to Control Threat/Symptoms

Cognitive Model of PTSD: Key Factors (1)
PTSD becomes persistent when individuals process trauma in a way that leads to a sense of serious, current threat.
The above involves excessively negative appraisals of the trauma and its sequelae.
PTSD involves poor autobiographical recall, poor elaboration, and poor contextualization, but strong associations and perceptual priming.
35

Cognitive Model of PTSD: Key Factors (2)
Generalization of subjective sense of threat leads to hyperarousal, hypervigilance, and exhaustion.
The person’s own physiology becomes a source of fear.
Therapeutic changes in the above are hampered by the patient’s avoidance.
36

Cognitive Model of PTSD: Key Factors (3)
Poor recall for positive memories (especially evident in persons with Acute Stress Disorder).
Impaired ability to draw upon past experiences in order to problem-solve current difficulties.
37

Heightened Appraisal of Threat
Sense of serious, current threat. External threat (e.g., the world is a
dangerous place). Internal threat (e.g., “I am not capable of
protecting myself.” “I’ll never get over this.” “I’m dead inside.” “I am permanently damaged”).
Thought suppression makes it worse.
38

Acute Stress Disorder
Appeared in the DSM-IV in order…
To recognize the significant levels of distress experienced in the initial month following a traumatic experience.
To foster early identification of those trauma survivors in greatest distress.
39

Acute Stress Disorder: Caveats (1)
Clinicians should exercise caution in making the diagnosis of ASD shortly after a trauma, because the observed distress may simply reflect a transient response.
40

Acute Stress Disorder: Caveats (2)
The notion of treating all people who are symptomatic in the acute trauma phase is unjustified because of evidence that most of these people recover without formal intervention. This is why mandatory treatment is problematic.
41

Acute Stress Disorder: Caveats (3)
Bear in mind that some of the apparent psychological symptoms seen in patients after they have experienced trauma may in fact be medical symptoms, such as a reaction to morphine, the after-effects of head trauma, and other such conditions.
42

When to Intervene?
Early interventions (e.g. debriefing) – evidence not supportive and may be harmful (e.g. Ehlers, Clark et al, 2003)
A role for care and support in first days and weeks, and ‘watchful waiting’
Intervene when problem shows signs of being chronic and not resolving itself (three months?)
Critical Incident Stress Debriefing
Actually found to be associated with a higher incidence of PTSD
Different from Brief CBT for Acute Stress Disorder which is associated with positive outcomes

Treatment of PTSD
Psychotherapy – particularly CBT with trauma exposures
Only effective treatment to date.
Psychopharm – prazosin (for nightmares),
SSRIs (probably), atypical antipychotics
No medication is endorsed as effective for treating symptoms of PTSD

Elements of Cognitive-Behavioral Therapies for PTSD Psychoeducation Relaxation Training Exposure to anxiety-provoking situations Cognitive restructuring Behavioral experiments
The Key elements for PTSD thus far appear to be exposure and cognitive restructuring

There are several cognitive-behavioral therapies for PTSD Prolonged Exposure Therapy (PE) Cognitive Processing Therapy (CPT) Stress Inoculation Training (SIT) Cognitive Therapy (CT) Eye Movement Desensitization and
Reprocessing (EMDR)

A word or two about EMDR
No evidence that eye movements reduce anxiety EMDR just as effective without eye movements Treatment effects no larger than exposure alone General consensus among Behaviorist is that the eye
movements and tapping are inert additions to otherwise effective treatments

Treatment for PTSD

Sample Treatment Goals

Prolonged Exposure TheapyBased on:
Foa, E.B. Hembree, E. A., & Rothbaum, B.O. (2007) Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences. New York: Oxford University Press.

PE
Based on 20 yrs of controlled studies International Consensus Group on
Depression and Anxiety selected exposure therapy as treatment for PTSD
“Model Program” by SAMHSA (substance abuse and mental health administration)
PE therapy effective in treatment of PTSD and comorbid symptoms
Appropriate for use across cultural groups
Effective in treating victims from a wide range of traumas
Effective in treating individuals who have multiple traumas and patients who have complex PTSD
Progress maintained at follow-up (6 months or 1 year)

Prolonged Exposure Therapy: Main Components
1. Education about PTSD and trauma
2. Repeated reliving of trauma memories through imagination
3. Repeated in-vivo exposure to avoided situations

Prolonged Exposure Therapy 10=12 weekly or twice=weekly sessions Sessions are generally 90 minutes Therapy may take fewer or more than
10 sessions depending on number of traumas and severity
Sessions are audio-taped

Providing patients a rationale It is difficult for clients to give up
avoidance and a good rationale helps PE focuses on addressing trauma
related fears and symptoms Sometimes memories get easier but
mostly trauma memories and symptoms stay the same or get worse usually because of avoidance

Prolonging Trauma Memories:
How Patients Avoid Pushing away memories, thoughts, and feelings
Avoiding situations, places, or people The presence of unhelpful beliefs such
as: “The world is dangerous” “ I can’t trust anyone” “I can’t get over this”

Why avoidance is a problem
When you avoid, you are giving yourself the opportunity to work through the memory or to think about it in a more helpful way. It never gets better.
Helpful to find out how each individual patient’s avoidance behaviors
Helpful if patients can recall a time they overcame something they were avoidant of.

2 Main procedures Imaginal Exposure: repeatedly reliving
the traumatic event using imagination. Confronting the memories allows for processing of experiences and allows for modifying unhelpful cognitions.
In-Vivo Exposure: Repeatedly approaching trauma related situations out in real-life (usually for homework and in between sessions)Target trauma-related situations that are safe, modifies cognitions about danger.

PE has seven components1. History, including most significant
trauma(s)
2. Psychoeducation
3. Formal assessment of PTSD severity
4. Relaxation training
5. Exposure hierarchy
6. In vivo exposures
7. Narrative exposures

Contraindications for PE
If trauma just happened-exact amount of time varies (Foa recommends 3 months) PE has been shown to be equally effective with old and new trauma even decades past
Imminent threat of suicide or serious self-harm
Psychosis Traumatic Brain injury (TBI)
Contraindications Continued Still has a relationship with assailant Severe dissociation Current substance abuse with no
motivation to stop (abstinence is not required but guidelines)
Inadequate memory of the trauma

Under Engagement
Patient is “going through the motions” Little emotion Tell client what you observe Label it as PTSD avoidance Explore perceived consequences Help patient use their senses to get in
better touch with the event

Over Engagement
Too close to feeling as if it is really happening (take a break and ground them, tell them they are safe, play with stress ball)
Evidence of dissociating Regressive behaviors Physical movements that “replay”event Uncontrollable sobbing
Address Over Engagement
Can modify procedures to decrease engagement
Past tense Eyes open Write it out Take a time out More therapist involvement Grounding techniques

Session 1-12
Breathing re-training Exposure Hierarchy- things not doing
and afraid of (sitting in restaurant with back to door, talking to friend)
Face feared situations for 20 minutes (regardless of whether SUDS decrease/used to be 50%)
By session 3, narrative of trauma-no cognitive work, restructure later
TIPS Avoid cognitive work during the
exposure to the narrative-make sure anxiety is not too high (person nauseas, urge to urinate, defecate, dissociating, confused, tunnel vision (sessions 4-9+)
Make narrative exposure intense, use first person, close eyes, focus on “hot spots”, avoid analyzing
Over time narratives are shorter focusing on hot spots

Continue narrative exposure in session and listening to session (narrative) at home
Continue in vivo exposures outside of session using breathing exercise
Cognitive restructuring is done just like CPT and CT (in repeated exposure to narrative see how their reactions change, situations unrelated to trauma are no longer trigger, separate present from past, mastery of memories)

Individualizing treament
PE is a manualized treatment but not “cookie cutter”
Homework is specifically tailored for each patient’s unique avoidance behaviors
Patients therapy and life goals should be elicited and re-iterate how PE is helping to achieve those

Comorbidity
80% of PTSD patients also suffer from depression, another anxiety disorder, or a substance sue disorder
May have a personality disorder Medical conditions can complicate
PTSD and can even be the index trauma (HIV, Cancer)

Can still do PE with these groups May have to be more flexible with
treatment Address substance use or health issues
as needed Important to still focus on trauma as
main focus of treatment

Cognitive Processing Therapy Process the trauma through writing out
details and reading repeatedly Systematically challenges unhelpful
“rules” related to self, others, world Addresses topics such as safety, trust,
intimacy, and power and control 17 sessions https://cpt.musc.edu

Cognitive Processing Therapy Strong Research Support Focuses on distorted thinking about the trauma Contains an exposure component (written narrative) Can easily be done in group formats Manual freely available online(http://cptforptsd.com/cpt-resources/) Goals of treatment
To Recognize and modify old thoughts and feelings that may be unhelpful
To accept the reality of the event To change beliefs enough to accept it with going overboard To feel your emotions about the event

Cognitive Processing Therapy Recommended for more complex PTSD Focuses on cognitive distortions made
during attempts to accommodate the traumaAssimilation: altering information coming in
to fit with prior beliefsOver-accommodation: altering beliefs about
the world to the extreme in order to feel safer and in more control

Goal
Accommodation – altering your beliefs about the world enough to incorporate the new information but in a balanced and functional manner. Bad things happen, but this is not the defining order of the world in general.

EX: Car Jacking Assimilation: my fault for being in bad
neighborhood, bad things don’t happen to good people who are smart.
Over-Accommodation: you can’t trust men, it’s kill or be killed in my neighborhood

Goal: Accommodation “The carjacking was a tragedy, but I am
grateful to have survived. It wasn’t my fault. It’s not likely to ever happen again.”
OR In the case of a rape, “The rape was a
tragedy, but it wasn’t my husband that raped me. He loves me and we can enjoy sex with each other because it’s safe and loving.”

CPT
The theory behind CPT is that the patient with PTSD has been unable to cognitively accommodate the trauma in a healthy way. Accommodation (and therefore recovery from trauma) requires tolerating and processing complex and conflicting thoughts and intense emotions.

Instead, the person with PTSD engaged in assimilation or over-accommodation of the trauma, but assimilation and over-accommodation generally result in persistent, negative views of the world, the future, or oneself. The assimilated or over-accommodated thoughts create “stuck points” that prevent recovery from PTSD.

CPT: Socratic dialogue Clarifying by asking for more information Probing assumptions Probing reasons and evidence Questioning viewpoints and
perspectives Analyzing implications of beliefs Questions about questions (redirecting
questions asked by the patient back on to the patient)

Key
Don’t argue with the patient. Collaborate. If the patient isn’t ready to examine a particular belief, note it, move on, and come back to it later.

Cognitive Processing Therapy 12 weekly or twice-weekly sessions 60-90 minute sessions Initially focuses on identifying and
evaluating assimilation errors, then on identifying and evaluating over-accommodation errors. (guilt and blame first, external blame second)
Done in individual or group sessions
NOTE
PE does not work in groups and data actually can make people worse (retraumatized)
CP works in groups – especially in VA where people have been through similar traumas-vets trust another vet

CPT Session by SessionSession 1: Introduction and EducationSession 2: The Meaning of the EventSession 2a: Traumatic Bereavement (Optional Session)Session 3: Identification of Thoughts and FeelingsSession 4: Remembering the Traumatic EventSession 5: Identification of Stuck PointsSession 6: Challenging QuestionsSession 7: Patterns of Problematic ThinkingSession 8: Safety IssuesSession 9: Trust IssuesSession 10: Power/Control IssuesSession 11: Esteem IssuesSession 12: Intimacy Issues and Meaning of the Event
Impact statement
One page Handwritten Why person thinks trauma happened to
him How the trauma changed the person’s
view of the world, future, other people and himself

Session 2
Read impact statement Socialize them to cognitive model Document stuck points ABC worksheet – activating event,
belief, consequences (are my thoughts in B realistic and what can I tell myself in the future on such occasions)
ABC worksheets
A-My platoon sergeant wouldn’t let me help the wounded Iraqi child.
B-Leaders are always insensitive jerks who don’t understand what it’s like on the ground. I am weak because I did not disobey orders.
C-Feel sad. Don’t trust authority. Can’t be around own kids without feeling guilty thinking about wounded Iraqi kids.

Reframe
Leader’s are not all insensitive Leader’s are human do make mistakes Not Weak to struggle with complex
issues. If I disobeyed orders and someone in
platoon got hurt, I would have felt horrible.
Leader was looking out for us.

Session 3 Trauma account Handwritten Several pages in length (Barad 35pgs) Full account of trauma and thoughts and
feeling experienced Want them to experience emotions but
not be overwhelmed, take breaks if need to
Read account daily after completing it Do ABC worksheets

Session 4 Read Trauma account out loud Allow affective displays Encourage them to describe the thoughts
and feelings they experienced during the trauma –add in-add how feeling now in parentheses. At the time I felt scarred and sad (but right now I am angry)
Note stuck pointsPlaces the patient stops writing or glossed over,
self-blame, judging the situation in hindsight.

Session 5-7
Evaluate the stuck points in and out of session using the evaluating questions worksheet.

Evaluating Questions WorksheetBelief:____________1. What is the evidence for and against
this idea?2. Is your belief a habit or based on facts?3. Are your interpretations of the situation
too far removed from reality to be accurate?
4. Are you thinking in all or nothing terms?5. Are you using words or phrases that
are extreme or exaggerated?

6. Are you taking the situation out of context and only focusing on one aspect of the event?
7. Is the source of information reliable?
8. Are you confusing a low probability with a high probability?
9. Are your judgments based on feelings rather than facts?
10. Are you focused on irrelevant factors?
Session7-11
Keep reading the trauma account and work on one theme:
1. Safety
2. Trust
3. Power/control
4. Esteem
5. Intimacy

Patient thinks about how they viewed themselves and others (in terms of each theme) before the trauma, and how these views changed after the trauma
Use worksheet to evaluated beliefs related to theme (homework and in office)

Session 12
Review Evaluating Belief worksheets on themes
Review the new impact statement wrote for homework (why thinks trauma happened and how changed view) and compare with original impact statement
Review skills

References US National Center for PTSD –
www.ptsd.va.gov APA Treatment Guidelines for PTSD –
www.psychiatryonline.com/praGuide/praGuideTopic_11.aspx
Rothbaum, BO, Foa EB, Hembree EA. Reclaiming Your Life From a Traumatic Experience: Workbook. Oxford University Press, 2007.
Medical University of South Caralina, navy Medicine. CPTWeb: A web-based learning course for Cognitive Processing Therapy. https://cpt.musc.edu/index

Research Ehlers, A.& Clark, DM. (2000) A cognitive model of
PTSD. Behaviour Research and Therapy 38 Ehlers et al, (2003) A RCT of CT, a self-help booklet,
and repeated assessments as early interventions for PTSD
Ehlers et al (2005) CT for PTSD: Development and evaluation. Behaviour Research and Therapy, 43
Ehlers et al (in prep) A RCT of intensive and weekly cognitive therapy versus emotion focussed supportive therapy
Gillespie et al (2002). Community based CT in the treatment of PTSD following the Omagh bomb. Behaviour Research and Therapy, 40
Duffy et al (2007) PTSD in the context of terrorism and other civil conflict in Northern Ireland: RCT. British Medical Journal, 334

A BRIEF LOOK AT CPTThis CBT treatment lines up really well with the Mind over Mood Curriculum

CPT Session by Session Session 1 - Introduction and Education: Symptoms of PTSD;
explanation of symptoms (cognitive theory); description of therapy. Practice assignment: Write Impact Statement.
Session 2 - The Meaning of the Event*: Patient reads Impact Statement. Therapist and patient discuss meaning of trauma. Begin to identify stuck points and problematic areas. Review symptoms of PTSD and theory. Introduction of A-B-C Worksheets with explanation of relationship between thoughts, feelings, and behavior. Practice assignment: Complete 1 A-B-C sheet each day, including at least one on the worst trauma.
Session 3 - Identification of Thoughts and Feelings: Review A-B-C practice assignment. Discuss stuck points with a focus on assimilation. Review the event with regard to any acceptance or self-blame issues. Begin Socratic questioning regarding stuck points. Practice assignment: Reassign A-B-C Worksheets. Assign written trauma account.




CPT Session by Session Session 4 - Remembering Traumatic Events: Have patient read
full trauma account aloud with affective expression. Identify stuck points. Start to help patient challenge self-blame or assimilation with Socratic questions. Explain difference between responsibility and blame. Practice assignment: Rewrite trauma account, read full written trauma account on a daily basis, complete A-B-C sheets daily.
Session 5 - Identification of Stuck Points: Have patient read second written trauma account aloud. Identify differences between first and second account. Help patient challenge self-blame or assimilation with Socratic questions. Introduce Challenging Questions Worksheet to help patient challenge stuck points. Practice assignment: Challenge one stuck point per day using the Challenging Questions Worksheet, continue to work on trauma account if not finished, read trauma account daily.


CPT Session by Session Session 6: Challenging Questions - Review practice assignment. Review
Challenging Questions Worksheet. Continue cognitive therapy regarding stuck points. Introduce Patterns of Problematic Thinking Worksheet. Teach patient to use the new worksheet to challenge his cognitions regarding the trauma(s). Practice assignment: Identify stuck points and complete Patterns of Problematic Thinking worksheets for each. Look for patterns in thinking. Continue to read trauma account if still having strong emotions about it.
Session 7 - Patterns of Problematic Thinking: Review Patterns of Problematic Thinking Worksheets to address trauma-related stuck points. Introduce Challenging Beliefs Worksheet with a trauma example. Introduce Safety Module. Discuss how previous beliefs regarding safety might have been disrupted or seemingly confirmed by the index event. Use Challenging Beliefs Worksheet to challenge safety beliefs. Practice assignment: Daily identification of stuck points, including one on safety using the Challenging Beliefs Worksheet. Read Safety Module. Continue to read trauma account if still having strong emotions about it.


CPT Session by Session Session 8 - Safety Issues: Review Challenging Beliefs
Worksheets and help patient to challenge problematic beliefs they were unable to complete successfully on their own. Introduce Trust Module. Pick out any stuck points on self-trust or other-trust. Practice assignment: Read Trust Module and complete at least one Challenging Beliefs Worksheet on trust. Continue to challenge stuck points on a daily basis using Challenging Beliefs Worksheets. Continue reading trauma account if still having strong emotions about it.
Session 9 - Trust Issues: Review Challenging Beliefs Worksheets. Introduce module on Power/Control. Discuss how prior beliefs were affected by the trauma. Practice assignment: Read Power/Control Module and complete at least one Challenging Beliefs Worksheet on Power/Control issues. Continue to challenge stuck points on a daily basis using Challenging Beliefs Worksheets. Continue to read trauma account if still having strong emotions about it.

CPT Session by Session Session 10 - Power/Control Issues: Review Challenging Beliefs
Worksheets. Introduce module on Esteem (self-esteem and regard for others). Practice assignment: Read module and complete Challenging Beliefs Worksheets on esteem, as well as assignments regarding giving and receiving compliments and doing nice things for self. Continue to challenge stuck points on a daily basis using Challenging Beliefs Worksheets. Continue to read trauma account if still having strong emotions about it.
Session 11 - Esteem Issues: Review Challenging Beliefs Worksheets. Discuss reactions to two behavioral assignments – giving and receiving compliments and engaging in a pleasant activity. Introduce final module on Intimacy. Practice assignment: Continue giving and receiving compliments, read Intimacy Module and complete Challenging Beliefs Worksheets on stuck points regarding intimacy. Continue to read trauma account if still having strong emotions about it. Final assignment: Write final Impact Statement.

CPT Session by Session Session 12 - Intimacy Issues and Meaning of the Event: Go
over the Challenging Beliefs Worksheets. Have patient read the final Impact Statement. Therapist reads the first Impact Statement and then compares the differences. Discuss any intimacy stuck points. Review the entire therapy and identify any remaining issues the patient may need to continue to work on. Encourage the patient to continue with behavioral assignments regarding compliments and doing nice things for self. Remind patient that he is taking over as therapist now and should continue to use skills he has learned.
A modified protocol (CPT-C) is available for individual who refuse to write the trauma narrative

CBT
For
ANGER

STEPS
112
1. A should rule is broken
(Perceived wrong)
Examples:
“People should listen to me, and they don’t.”
“I should have total control over this situation, and I don’t.”

113
2. Meaning: What hurts or scares you the most? (Hurt or Fear?) Feeling Diminished? Victimized?
(Categorical thinking, recalled grievances through selective attention)

114
Examples:
“They are diminishing me.”
“People are rude and insensitive, they don’t care.”
“I’ll be made the victim.”
“He’s going to leave me.”

115
3. Hot Thoughts/Ruminations on Grievances(Anger driven thoughts)
Examples:“How dare he?”
“How stupid can she be?”
“Poor me, they are always blaming me.”

116
4. Anger (Arousal/Anxiety)
Physical/emotional symptoms
Examples:
Muscles tension
Anxiety

117
5. Moral Disengagement: Permission-giving beliefs
(Mobilize for action)
Examples:“He deserves it.”
“I just want them to hurt the way I have been hurt.”

118
6. Extort validation: Passive Aggression/Aggression/Violence
(Strike) (Dysfunctional Behaviors)
Examples:
Acts aggressively and ignores the rights of other people
Violence

119
7. Resentment, Guilt, Shame
(Outcome)
Examples:
Views every anger episode as a self-perpetuating failure, as a set back
Views anger as proof of being helpless, powerless, weak

120
Each step represents a point of intervention or choice point
One can choose to intervene at each step, cool down and break the pattern
OR
Continue down the destructive path

121
1. A SHOULD RULE IS BROKEN.
ACCEPT REALITY (THAT YOU HAVE 0% CONTROL OVER OTHER PEOPLE’S BEHAVIOR AND 100% CONTROL OVER YOUR CHOICES)CHOOSE A DIRECTION BASED ON YOUR VALUES: SHOULD RULES OFTEN REFLECT DEEPER VALUES AND PRINCIPLES. TAKE CONSTRUCTIVE ACTION IN THAT DIRECTION.
STEP INTERVENTION

122
INTERVENTION
Facts are that people don’t listen, they do get in our way, and we cannot control their behavior. We can learn to accept the circumstance as given, accept them as reality.
Ask yourself:
Intervention
• What do I want in the long run? • What constructive steps can I take in that
direction?
When people do ignore my wishes and intrude, I can tell myself I wish it were different but accept the reality.

What Should Rule Was Broken?Example:
Bill is at his friend’s house cleaning and another friend shows up to use the computer.
Bill thinks, “He should know not to come in while I am cleaning.” “ Doesn’t he see my car and realize I am here?” “ He should be more considerate.”

Response to Broken ShouldExample:
“ I have 100% control over me and 0% control over the rest of the world. If would be nice if the world followed my rules but I cannot demand they see the world I do.”
“My expectations and rules are not the same as his and I have to accept people are always going to break my rules since they are not their rules, too.”

126
STEP
2. Meaning: What hurts or scares you the most? (Hurt or Fear?)
Feeling Diminished? Victimized?

127
Toll: What’s the effect of my thinking?
What are the costs/benefits of thinking this way?
INTERVENTION
128
INTERVENTION
Ask “What really hurts here?” Maybe they are trying to help me, not control me. Maybe I can see myself not as a victim but a person getting assistance. It’s not helping me to think about it this way, its possible they would act that way no matter who it was.

Ask, what does it mean to me or about me that they did not meet my expectation?
129
Example:
“The audacity!” “Am I supposed to accommodate him, this is so inconsiderate.” “My time does not matter.” The world revolves around him.” “I have no control.” “I’m powerless.”

Examine the thoughts.Is the meaning true or just an emotional perception?
130
Example:
Alternative View: Consider this a nervous guy who was driven by anxiety and agitation to get on the computer and not driven by his brain. He is an impaired person who is just trying to cope with his problems. He did not intentionally set out to inconvenience me. I could be sympathetic and be gracious or I could assertively ask him to come back later.

Feeling Subside
131
Example:
Feelings of being annoyed, angry and pissed-off subside.

132
STEP
3. Hot thoughts/Ruminations on Grievances
INTERVENTION
Answer them with cooling responses.
Practice using role plays.

133
Examples:
“How dare he.”
“How stupid can she be.”
“Poor me, they are always blaming me.”

134
INTERVENTION
Find more level headed thoughts, like
“I think he is trying to help me.”
“She’s human.”
“I guess I did make a mistake, or I did overreact.”

New Conclusion
135
Example: The guy did not use the computer to intentionally annoy me, he just did not think and instead was just trying to cope with his anxiety.

136
STEP
4. Anger (Arousal/Anxiety)
Physical/emotional symptoms

137
Examples:
Muscles tension
Anxiety

138
INTERVENTION
Learn and practice different form of relaxation therapy (progressive relaxation, visualization, music).
Learn to relax muscles and focus attention away from anger inducing stimuli.
See the anger as energy for constructive action.
Remind oneself that just as Martin Luther King was angry at racism and Mother Theresa was angry at poverty, I can turn anger into positive action.

139
STEP
5. Moral Disengagement: Permission-giving beliefs
(Mobilize for action)

140
INTERVENTION
Reconnect with morals and values: “Do unto others as you would have them do unto you.” Respond to the ways you rationalize or minimize aggression.

141
Examples:“I just want them to hurt the way I have been
hurt.”
“I have to teach them a lesson.”
“I am not going to let them have one up on me.”
“This is the only way I can get my point across.”
“He deserves it.”

142
INTERVENTION
Examine the beliefs that turn anger into dysfunctional action. Help them recognize these ideas are con artistry. They con the person into throwing aside their morals and engaging in threats, sarcasm, demands and blame. Have them remind themselves of the cost of such strategies, and the benefits of remaining calm and fair.

143
STEP
6. Extort validation: Passive Aggression/Aggression/Violence
(Strike) (Dysfunctional Behaviors)

144
INTERVENTION
Time outEmpathyAssertiveness (Being Fair to yourself and fair to
others):
DEALDescribe the situation – just the factsExpress feelings – without blameAsk for changes in the relationship – no
demandsList the benefits of those changes

INTERVENTION
145
Put yourself in the other person’s shoes and empathize. Imagine what they are thinking and feeling and work to understand their perspective.

Action or No Action
146
Cleaning Example:
Confronting this guy would have probably resulted in a man crying. It could have snow balled and my anger would have gotten the best of me. The better choice was to leave the computer room not cleaned and left the house as soon as possible.
KEY: Take Appropriate Action.

STEP
147
7. Resentment, Guilt, Shame
(Outcome)

INTERVENTION
148
Relapse prevention: Turn guilt or resentment into constructive action. Break episode into points of intervention. Review what you can do at each step.

EXAMPLES
149
• Views every anger episode as a self-perpetuating failure, as a set back
• Views anger as proof of being helpless, powerless, weak

INTERVENTION
150
Reduce resentment and guilt.
Learn to see each episode as a success, so long as you are examining the triggering should statements, the angering beliefs, the automatic thoughts, the anger arousal, the permission giving beliefs, and the strategies you engage in.
The episodes can be fewer and further between and less intense.

Strategies Stop Take a Breath Observe Pull Back (get some
perspective) Practice what works

Coping CardPatient with chronic anger
Anger comes from your should rule being broken.
“She should not have done what she did!”HURT comes from me believing it was because I wasn’t good enough, special enough, or valued enough.

Coping CardRECOVERY come from:
1. Accepting you cannot control the world. You cannot make what happened not happen. You can wish it but not demand it. Accept that it did happen.
Coping Card
2. To help you accept remind yourself that the marriage had problems and at that time the circumstances presented themselves to make what happened happen. BUT, it never happened again and it will never happen again.
This woman loves you and is committed to you!
The goal is not to forget but to Accept!

Situation
155
Husband leaves a pile of dirty clothing sitting on floor.

Thinks
156
Why do you have to leave a pile of dirty clothing on the floor?
I told you explicitly not to do this.
He should put his clothing in the laundry.

157
You do it purposely to get me upset.
You’re trying to push my buttons.
You don’t care about me.

Feels
158
Angry
Frustrated
Hurt

Alternative Response
159
He does care. He calls me during the day. He asks about my day and is genuinely interested. He talks to me. We are good friends. We are lovers.
It is not that he doesn’t care, he is not purposely trying to hurt me. It is just the way he is. Born slob. He has been a slob his whole life.

Alternative Response Cont.
160
This is the negative side of who he is, but the positive side is a lot longer. He is smart, kind, a good friend, responsible, reliable, attractive and my good friend and lover.
He is not going to change so there is no benefit in shouting and demanding he do so.

Alternative Response Cont.
161
I am the one suffering. he just laughs it off.
Instead of shouting and demanding he should do what I want, I can wish it, desire it, or prefer it and maybe even let him know in these words.

Conclude
162
I can accept his mess if I remind myself this is about him not about me. He is not purposely trying to hurt me, he cares about me too much. He is not going to change but his strengths outweigh such an unimportant deficit.

Coping Cards
163
Step 1
Anger comes from broken should rules, identify the should rule that has been broken .
Step 2
Recognize the world does not operate on imperatives: should, ought, have to, must.
164
Step 3
Replace the imperative with a preference: wish, like, prefer, it would nice.
Step 4
What does it mean to you that your should rule was broken? What does it mean about you or what does it mean about them?
Look for the Hurt or Fear under the anger and the thoughts that drive those feelings.

165
Step 5
Examine the validity of the thoughts that are connected to the hurt or fear.
Step 6
Recognize the answer is not in changing others but in changing how you think, taking appropriate action, and modifying your external circumstances if that is what is necessary.

HOMEWORK
166
Look for the should.
Replace the should with prefer.
Look for the thoughts connected to hurt or fear.
Evaluate your thoughts.
Take appropriate action.

Trigger: 2 year old son is being difficult
167
Should Rules:
He should be cooperative.
He should be patient.
He should be satisfied.
Should Rules for all of his kids:
They should be able to self-entertain.
They should be able to play nicely.
They should be less crazy, be calm, be patient.

Ask is that Demand valid?
168
These are not valid demands. The kids are young and they cannot control their impulses. My kids have learning issues and that makes it even harder for them. Their 2 and 4 year old brains are not fully developed, give them time. It is difficult if not impossible for most 2 and 4 year olds to have patience. Patience is even more compromised when disability makes things frustrated. Even adults have difficulty with this.

Replace the Should
169
It would be nice if my kids…
I would prefer if the kids…
I would like…
It would be better if…
Remember, replace the should, must, ought, have to or anger and frustration will remain.

Trigger: Daughter is not practicing the Piano
170
“ For all we spent, she should be practicing!”
SHOULD RULE is broken.
But, it is reasonable to expect her to practice since she wanted to do this.
Acknowledge the frustration.
BUT, Demanding her cooperation is not an answer.

171
You cannot force her to practice. In the short-run you may be able to, but in the long run, it is up to her. Since you cannot effectively force her, you can only help convince her to choose to practice. She has to choose to make it happen.
You can remind her. You can encourage her. You can help her see the advantages and sell it. You can set rules and impose consequences.
Tolerate sharing the power.
Feeling Frustrated and Angryand Starts Yelling
172
Look out for the escalation of upset.
Your gut warns you.
Stop the aggressive yelling before it escalates.
Force yourself to communicate in a soft, slow voice. (This will have a natural calming effect and the facts will be heard and not your yells.)
Yelling leads to more upset and forces people to defend themselves and be less likely to hear you.

Be Assertive
173
Use a soft voice.
Engage them by asking questions that lead them to see your point. Don’t ask why questions, but rather questions that help them see practicing will get them closer to their goals.
Recognize that demands makes us more powerless even though we do it to try and get more power.

174
State the facts.
Let them know how it made you feel.
Let them know what you wish for or would like.
Ask what they want and hear them.
Compromise.

Venting
Research dating back to at least the 80s has shown that venting is generally not helpful and tends to increase anger

Insomnia

Sleep Hygiene Keep bed for sleep and sex. Don't use it for watching television, using computer etc.
Get the TV out of the bedroom Get some regular exercise during the day. Try some regular swimming or walking.
Avoid exercise late in the evening. Cut down on caffeine (tea, coffee, some soft drinks) in the evening. Try a milky drink
instead. Don’t drink a lot of alcohol. It may help you fall asleep, but you will almost certainly
wake up during the night. Don’t eat or drink a lot late at night. Try to have your evening meal early rather than
late. If you’ve had a bad night, resist the temptation to sleep the next day – it will make it
harder to get off to sleep the following night. If something is troubling you and there is nothing you can do about it right away, try
writing it down before going to bed and then tell yourself to deal with it tomorrow. If you can’t sleep, don’t lie there worrying about it. Get up and do something you find
relaxing. After a while you should feel tired enough to go to bed again. Avoid clock watching when in bed

CBT
For
Psychosis
Highlights

Evidence for CBT for Schizophrenia Improvements in positive symptoms Improvements in negative symptoms Improvements in ability to cope with
voices At follow-up may demonstrate increased
improvement

Focus in Patients’ Assets From Aaron T. Beck, M.D.
Patients have healthy, accessible attitudes that can be tapped to neutralize or moderate disturbing symptoms
Through self-reflection and correction of distressing beliefs, they can modify neurocircuitry (neuro-plasticity)
The symptoms can be understood in terms of universal psychological problems
Even patients with severe deficits can benefit from psychotherapy

Problems Exacerbated By IllnessFrom Aaron T. Beck, M.D. Estrangement/Stigmatization Withdrawal Anxiety Hopelessness Depression Suicidal Passivity
Cognitive Therapy Approach For all presenting problems-
Thinking influences emotion and behavior○ Interpretation of experience key
Beliefs are possibilities, hypotheses, not facts
Approach can be applied to beliefs associated with hallucinations and delusions

Strategies/Principles
Forming working relationship Provide structure Guided discovery Collaborative empiricism Improve reality testing Case formulation Normalizing rationale Activate questionable mode
From Aaron T. Beck, M.D.

184184
Specific Tasks in CBT for Psychosis1. Establish therapeutic alliance2. Assess & Formulate problems3. Construct a ‘problem list’4. Explore catastrophic (non psychotic) beliefs
about symptoms & experiences (normalising).
5. Explore patient’s problems – including positive symptoms.
6. Evaluate ‘problematic’ beliefs – develop ‘benign’ alternatives, look for evidence for/against the alternatives, behavioral expts.
7. Schema Level Work

185185
Engaging and Rapport Building Empathy, warmth, unconditional acceptance and
respect
Genuineness
Find a balance between non-confrontation and non-collusion
If patient insists s/he is right then need to agree to differ
If emotional climate become too intense then tactical withdrawal is advised

Purpose of CBT for Psychosis Decrease distress
If patient reports no distress:○ Try to understand why○ Respect his or her wishes
It’s not the symptom that is the problem, it is the emotional behavioral consequences
Patient may have other issues to bring forthCan do therapy without tackling delusions
and hallucinations

Cognitive Model of SchizophreniaBizarre Beliefs Information-processing biases contribute
to development Overestimate coincidences, “jump to
conclusions”, engage in self-serving biases, or threat-related stimuli biases
Maintained by recruiting supporting evidence and ignoring or minimizing disconfirming evidence

Therapeutic ProcessAssessment
Engagement
Trace origins of beliefs/hallucination
Elicit beliefs about the mechanisms underlying delusions/hallucinations
Reattribute hallucinations and discuss content
Normalize symptoms and discuss alternative mechanisms
Inference chain resistant delusions
Specific techniques for negative symptoms, etc.

Hallucinations

190190
The Cognitive Model
EventEvent THOUGHTTHOUGHT FeelingsFeelings
BehaviourBehaviour
PhysiologyPhysiology

191191
EventEvent
Hearing Hearing Voices that no Voices that no
one else one else claims to hearclaims to hear
ThoughtsThoughts
I’m going madI’m going mad
I’ve got I’ve got schizophreniaschizophrenia
I’ll lose my jobI’ll lose my job
People will be People will be frightened of mefrightened of me
My life is ruinedMy life is ruined
I’m going to be I’m going to be locked awaylocked away
AffectAffect
FearFear
DespairDespair
HopelessHopeless

192192
Triggers and Maintenance
Stressful Life Events
Psychotic Episode
Catastrophic Interpretation of
EventsIncreased Arousal
193193
EventEvent
Hearing Hearing Voices that no Voices that no
one else one else claims to hearclaims to hear
ThoughtsThoughts
This is a reaction to This is a reaction to all the stress I’ve all the stress I’ve
been underbeen under
If I take my If I take my medication or get medication or get the stress under the stress under
control then these control then these symptoms should symptoms should
go awaygo away
I can get my life I can get my life under control againunder control again
AffectAffect
ReliefRelief
HopeHope

194194
Cognitive Biases in Patients with Delusions
Use less information and more likely to jump to conclusions
More likely to look for confirmatory data Less likely to have alternative beliefs
available. Theory of mind deficits – less likely to be
able to determine others’ intentions and feelings.

195195
The Cognitive Model
EventEvent THOUGHTTHOUGHT FeelingsFeelings
BehaviourBehaviour
PhysiologyPhysiology

196196
Cognitive Model of Delusions
A B C
ActivatingEvent:
Anomalous Anomalous ExperienceExperience
Belief
DelusionDelusion
Consequences:AffectBehaviourPhysiology

Cognitive Assessment of DelusionsDelusionDelusion Situation/Situation/
AntecedentAntecedentBeliefBelief Emotional/Emotional/
Behavior Behavior ConsequencesConsequences
ParanoidParanoid People heard People heard speaking speaking outside houseoutside house
““they’ve come they’ve come to harm me”to harm me”
Fear/ Escape Fear/ Escape househouse
Though Though broadcastbroadcast
Hears man ask Hears man ask for bus ticket for bus ticket just as he was just as he was thinking “I need thinking “I need a ticket”a ticket”
My thoughts are My thoughts are being passed to being passed to othersothers
Fear/EscapeFear/Escape
ReferenceReference Plane passes Plane passes overheadoverhead
WW III is WW III is startingstarting
Anxiety/Anxiety/
HelplessnessHelplessness
SomaticSomatic Develops skin Develops skin rashrash
I’ve got AIDSI’ve got AIDS Terror/Terror/
HopelessnessHopelessness

CBT Techniques for Delusions
Peripheral questioning Socratic questioning Graded reality testing Tackling emotional/behavioural
investment Inference chaining and schema level
work Maintaining a collaborative set

Focus on Specific Beliefs Related to:
Voice’s identity
Purpose of voices
Perceived power/omnipotence
Perceived consequences of obedience/disobedience

200200
Exploring BeliefsExplore beliefs using a gentle non-interrogative Socratic
style.
Is there some truth in the ‘delusional’ belief? Be aware of your own cognitive biases - don’t jump to conclusions but take comments at face value.
Even if belief isn’t factually true it is very real to the patient as is the associated affect.
Don’t try to do too much but keep the flow of discussion going
Aim for sessions to be positive, even enjoyable, experiences as far as its reasonable to do so.

Origins of Beliefs
How did he/she come to this belief? What was happening at that time? Stress? Personal History? Why that conclusion?

Understanding Beliefs
Give context to beliefs An attempt to make sense of an unusual
or confusion circumstance? Jumped to conclusions? Need for closure?

Mechanisms
What evidence have they collected that that this is the case?
What evidence have they seen that this may not be the case?

204204
Weakening Delusional Beliefs What makes person think this? May need to review evidence for belief and not
belief itself○ E.g “the car did a U-turn – it must have been following me”○ Are there any other reasons for cars to do U-turns?
Generation of Alternatives○ Consider impact of beliefs on self esteem, mood etc. ○ Consequences of alternative being true?
Identify other sources of self esteem if belief weakened

Verbal challenge
Generating AlternativesRecognizing other possibilitiesDirect confrontation avoidedColumbo, not Dirty HarryCollaborative, not forceful style
○ “What are some other possibilities?”○ “Hypothetically . . .”○ IF someone told you _____, what would you
say?”

Components of Verbal Challenge Inconsistencies pointed out (gently) Alternative explanation discussed
Ideally from client, can be offered by therapist
Which explanation most likely, given evidence

Thought RecordExample of patient with Paranoid Schizophrenia
EventEvent Automatic Automatic ThoughtsThoughts
Realistic Realistic ThoughtsThoughts
Seeing a red Seeing a red carcar
They are trying to They are trying to tell me somethingtell me something
They want me to do They want me to do somethingsomething
They can control meThey can control me
There are lots of There are lots of red carsred cars
Color of car Color of car doesn’t doesn’t determine who determine who is insideis inside
My illness makes My illness makes me overreact to me overreact to a situationa situation
“I didn’t really look at it as accepting, but that’s probably what it was—accepting. And I suppose once you accept it, it’s easier for you to look at ways of coping. Because when you’re fighting it, you’re just scared.”
--Quote from a participant in person-based cognitive therapy (PBCT) for distressing voices; Goodliffe et al., 2010

CBT for Schizophrenia:Treatment Considerations
Standard treatment always includes psychotropic medication and case management.
CBTp for Sz would be in addition to standard treatment.
Risk for suicide and self-harm is high and is harder to detect; careful, direct, and frequent monitoring is important.
The focus of CBTp is in helping individuals cope with and manage (versus “cure”) schizophrenia.

CBT for Schizophrenia:Clinical Strategies
Engagement and establishment of a therapeutic relationship
Importance of establishing rapport is heightened at beginning of treatment when clients may be particularly paranoid, etc.
Assessment and CBT case formulation including an understanding of client’s beliefs regarding their psychotic symptoms
Intervention Strategies

CBT for Schizophrenia:Highlighted Intervention Strategies
Attention Switching It is not the goal, nor is it necessary, to eliminate
delusions/hallucinations, just attend less or respond differently to them.
Reattribution “It may seem like a real voice, but it is [or could be] my own
thoughts.” Awareness training
Decentered awareness; ACCEPT experiences without having to react to them.
Attend to (be mindful of) form and characteristics of thoughts and perceptions versus the content.
Goal: increase the client’s scientific curiosity into their symptoms and sx patterns.

CBT for Schizophrenia:Highlighted Intervention Strategies
Behavior change is probably the best way to produce cognitive change. Behavioral experiments and reality testing. Clients may tend toward biased interpretation and confirming
beliefs; therapist can help by [gently] suggesting alternative interpretations.
Enhancing self-efficacy in client’s ability to cope Self-efficacy can be the highest when the client is experiencing
delusions, hallucinations or other symptoms. (The good news in the bad news.)
Again, the goal does not have to be “getting rid” of symptoms.

Schizophrenia:Diagnostic Criteria
Positive Symptoms: excess or distortion of normal functioning (e.g., hallucinations, delusions)
Negative Symptoms: decrease in or loss of normal functioning (e.g., restricted affect, alogia, avolition)
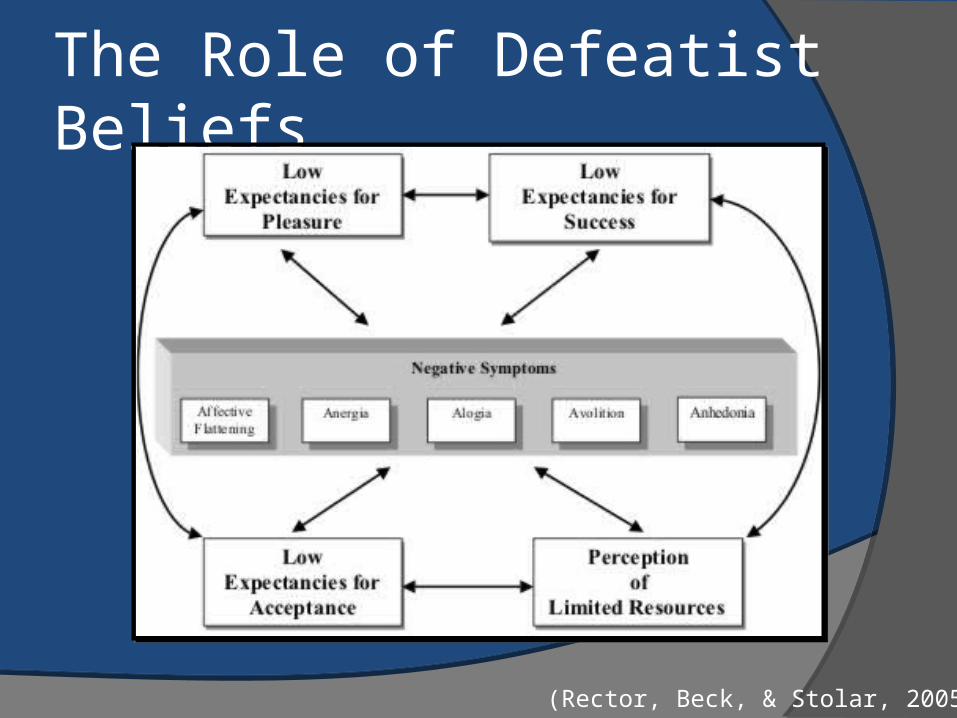
The Role of Defeatist Beliefs
(Rector, Beck, & Stolar, 2005)

Negative Expectancy Appraisalsnegative symptoms
Low self-efficacy (success)
Low satisfaction (pleasure)
Low acceptance
Low available resources
Affective flattening
If I show my feelings, others will see my inadequacy.
I don’t feel the way I used to.
My face appears stiff and contorted to others.
I don’t have the ability to express my feelings.
Alogia I’m not going to find the right words to express myself.
I take so long to get my point across that it’s boring.
I’m going to sound weird, stupid, or strange.
It takes too much effort to talk.
Avolition Why bother, I’m just going to fail.
It’s more trouble than it’s worth.
It’s best not to get involved.
It takes too much effort to try.
(Rector, Beck, & Stolar, 2005)

Core Elements
Therapeutic alliance a priority Collaborative approach in exploring
symptoms Acceptance of patient’s subjective
experience Symptoms not directly confronted Try to reduce distress related to
symptoms Reduce stigma related to illness
Overall purpose of CBT for Hallucination and Delusions
To reduce distress and disability
(Reducing delusions and hallucination is simply a means to that end)

Useful Texts
Beck, A.T., Rector, N.A., Stolar, N., Grant, P. Schizophrenia: Cognitive theory, research and therapy (2008). New York: Guilford

Useful TextsKingdon, D. and Turkington, D. (1994).Cognitive behavioural therapy of
schizophrenia. New York: Guilford.
Fowler, D., Garety, P., and Kuipers, E. (1995). Cognitive behaviour for psychosis: Theory and practice. New York: Wiley.
Chadwick, P.D.J., Birchwood, M., and Trower, P. (1996). Cognitive therapy for delusions, voices, and paranoia, New York: Wiley.

Working with Difficult Clients

What are your automatic thoughts about working with people who have a personality disorder?
Awareness

We’re looking at the contingencies that maintain a behavior set
We’re looking at cognitive distortions that maintain a behavior set
We’re maintaining an empirical mindset We’re utilizing experiments to test assumptions and
beliefs We’re valuing skill generalization, and using logs
and homework to track “real world” behavior change
Same Principles Apply

Describe the patient in behavioral terms What is their learning history? How did these behaviors develop? What is the function of these behaviors? How are they maintained by the environment? What cognitive distortions are present? How did they develop? How are they maintained? / How are they not disconfirmed? How will these thoughts and behaviors interact with treatment?
Conceptualizing

Avoidance Paradigm
(Lynch & Cheavens, 2007)

Enduring maladaptive patterns of behavior Exhibited across many contexts These patterns develop early, are inflexible and are
associated with significant distress or disability
What’s the theme? Pervasiveness
This is something we are likely to see “in the room with us”
Key Diagnostic Terms
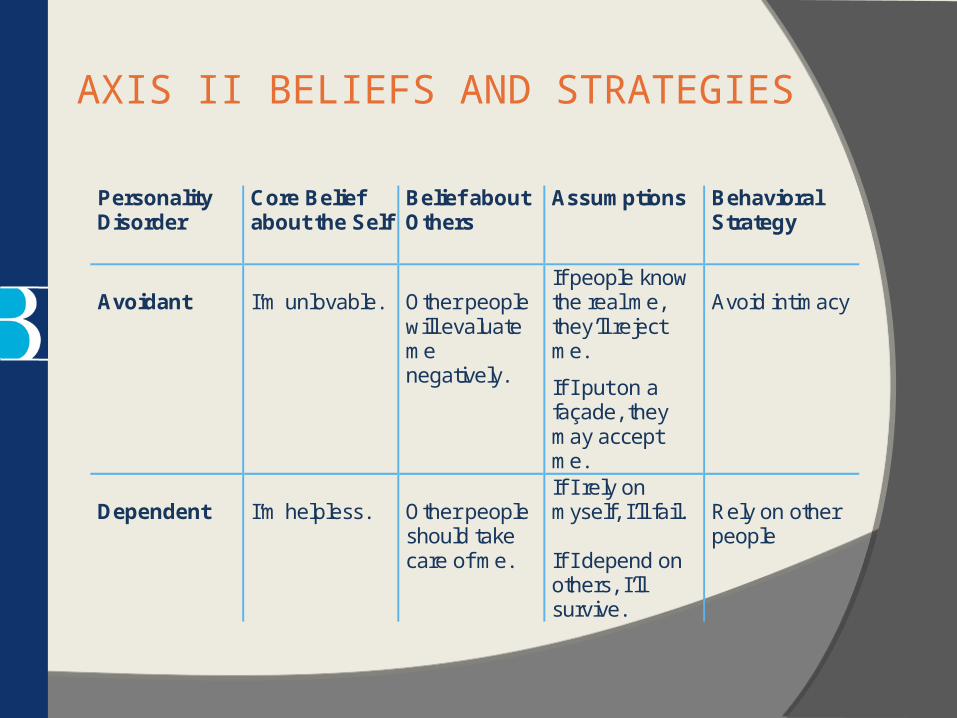
AXIS II BELIEFS AND STRATEGIES
Personality Disorder
Core Belief about the Self
Belief about Others
Assumptions Behavioral Strategy
Avoidant
I’m unlovable.
Other people will evaluate me negatively.
If people know the real me, they’ll reject me.
If I put on a façade, they may accept me.
Avoid intimacy
Dependent
I’m helpless.
Other people should take care of me.
If I rely on myself, I’ll fail. If I depend on others, I’ll survive.
Rely on other people

Obsessive Compulsive
My world can go out of control.
Other people can be irresponsible.
If I’m not totally responsible, my world will fall apart.
If I impose rigid rules and structure, things will turn out okay.
Control others rigidly
Paranoid
I’m vulnerable.
Other people are malicious.
If I trust other people, they will harm me,
If I am on my guard, I can protect myself.
Be overly suspicious
Antisocial
I’m vulnerable.
Other people are potentially exploitative.
If I don’t act first, I can be hurt.
If I can exploit first, I can be on top.
Exploit others
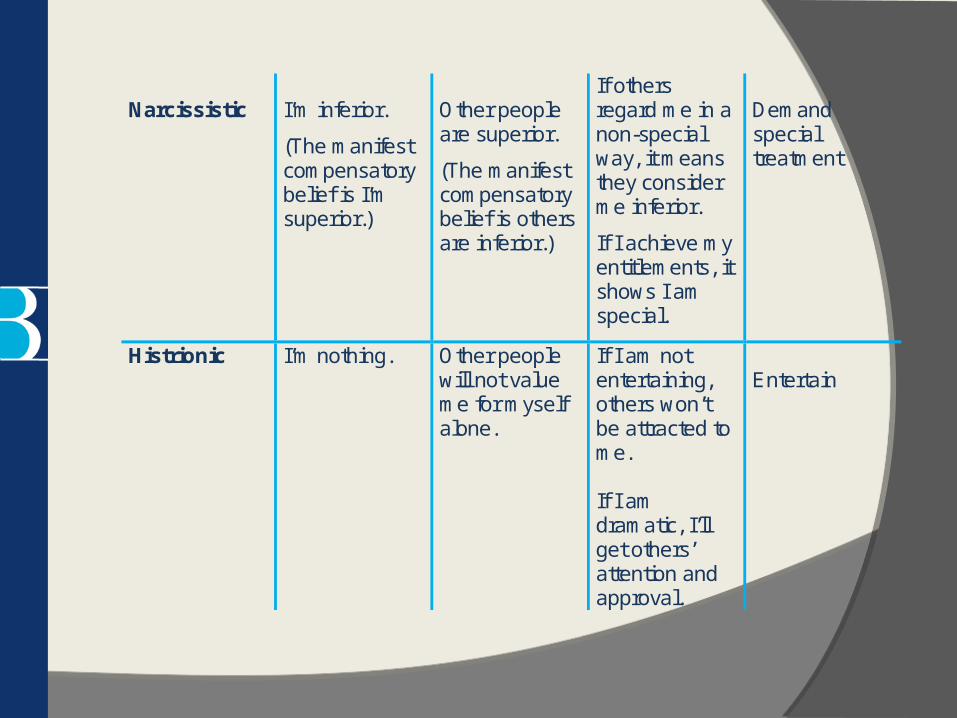
Narcissistic
I’m inferior.
(The manifest compensatory belief is I’m superior.)
Other people are superior.
(The manifest compensatory belief is others are inferior.)
If others regard me in a non-special way, it means they consider me inferior.
If I achieve my entitlements, it shows I am special.
Demand special treatment
Histrionic I’m nothing. Other people will not value me for myself alone.
If I am not entertaining, others won’t be attracted to me. If I am dramatic, I’ll get others’ attention and approval.
Entertain

Schizoid I’m a social misfit.
Other people have nothing to offer me.
If I keep my distance from others, I’ll make out better. If I try to have relationships, they won’t work out.
Distance self from others
Schizotypal I am defective.
Other people are threatening.
If I sense that others are feeling negatively toward me, it must be true. If I’m wary of others, I can divine their true intentions.
Assume hidden motives
Borderline Personality Disorder
I’m defective. I’m helpless. I’m vulnerable. I’m bad.
Other people will abandon me. People can’t be trusted.
If I depend on myself, I won’t survive. If I trust others, they’ll abandon me. If I depend on others, I’ll survive but ultimately be abandoned.
Vacillate in extremes of behavior

TYPICAL OVERDEVELOPED and UNDERDEVELOPED STRATEGIES
Personality Disorder Overdeveloped Strategy
Underdeveloped Strategy
Obsessive- Compulsive
Control Responsibility Systematization
Spontaneity Impulsivity
Dependent Help-Seeking Clinging
Self-sufficiency Mobility
Passive-Aggressive Autonomy Resistance Passivity Sabotage
Intimacy Assertiveness Activity Cooperativeness

Personality Disorder Overdeveloped Strategy
Underdeveloped Strategy
Paranoid Vigilance Mistrust
Serenity Trust
Narcissistic Self-aggrandizement Competitiveness
Sharing Empathy Encouragement
Antisocial Attacking Deprive others Exploit
Empathy Reciprocity Social sensitivity
Schizoid Autonomy Withdrawal
Intimacy Reciprocity
Avoidant Avoidance Inhibition
Self-assertion Gregariousness
Histrionic Exhibitionism Expressiveness Impressionistic
Self-discipline Control Systematization
Adapted from Beck, A.T. Freeman, A. & Associates, Cognitive Therapy of Personality Disorders, 2004

When Client (and Therapist) Behaviors Interfere with Treatment
What things do your clients do that make it difficult to work with them?
Anyone brave enough to talk about things that they do that impacts treatment?For some this can be avoidance of the real
issues

Emotions too high or too low New learning is
not occurring when emotions are extremely high
Hard to do good work without accessing emotions
Want to shoot for a moderate level of emotion

Ever feel like this?

Basic Strategy for Working with TIBs1. Call it out
2. Highlight how behavior is not serving their goals and how it affects your relationship
It’s probably related to problems outside of session
3. Get buy-in to work on it by relating in session problematic behaviors to out of session problematic behaviors
4. Get explicit permission to target it
5. Make TIB a focus of treatment

Saying I don’t know a lot
Differential: Hypotheses They don’t actually know (how they’re
feeling) They don’t want to talk about it They are afraid of how they’ll feel if they
talk about what your asking Other ideas?

Other Common TIBs
Missing sessions Consistently not doing the homework Being Hostile towards the therapist Constantly being in crisis Too Much Talking about Peripheral
Issues

INTERRUPTINGWhat are your beliefs about interrupting a patient?

• Most of the clients we work with live extremely stressful, painful, and chaotic lives
• While we certainly want to be emphatic and validating
• The most compassionate thing we The most compassionate thing we can do is work with them to build a can do is work with them to build a better lifebetter life
• This invariably includes: interrupting people, sticking to an agenda, and making goals
SOOTHING VS. THERAPEUTIC

Dissociation: Strategy Grounding Grounding is a set of simple strategies
to detach from emotional pain (for example, drug cravings, self-harm impulses, anger, sadness). Distraction works by focusing outward on the external world-- rather than inward toward the self. You can also think of it as “distraction,” “centering,” “a safe place,” “looking outward,” or “healthy detachment.”

Mental Grounding Describe your environment in detail using all your senses.
For example, “The walls are white, there are five pink chairs, there is a wooden bookshelf against the wall...” Describe objects, sounds, textures, colors, smells, shapes, numbers, and temperature. You can do this anywhere.
Play a “categories” game with yourself. Try to think of “types of dogs”, “jazz musicians”, “states that begin with ‘A’”, “cars”, “TV shows”, “writers”, “sports”, “songs”, “European cities.”
Say a safety statement. “My name is ____; I am safe right now. I am in the present, not the past. I am located in _____; the date is _____.”
Read something, saying each word to yourself. Or read each letter backwards so that you focus on the letters and not on the meaning of words.

Physical Grounding
Grab tightly onto your chair as hard as you can. Touch various objects around you: a pen, keys, your clothing, the
table, the walls. Notice textures, colors, materials, weight, temperature. Compare objects you touch: Is one colder? Lighter?
Dig your heels into the floor-- literally “grounding” them! Notice the tension centered in your heels as you do this. Remind yourself that you are connected to the ground.
Carry a grounding object in your pocket-- a small object (a small rock, clay, ring, piece of cloth or yarn) that you can touch whenever you feel triggered.
Walk slowly, noticing each footstep, saying “left” “right” with each step.
Focus on your breathing, noticing each inhale and exhale. Repeat a pleasant word

Soothing Grounding Think of favorites. Think of your favorite color, animal,
season, food, time of day, TV show. Picture people you care about (e.g., your children; and
look at photographs of them). Remember the words to an inspiring song, quotation, or
poem that makes you feel better (e.g., the Serenity Prayer).
Remember a safe place. Describe a place that you find very soothing (perhaps the beach or mountains, or a favorite room); focus on everything about that place-- the sounds, colors, shapes, objects, textures.
Say a coping statement. “I can handle this”, “This feeling will pass.”

Practice Conceptualizing
Forming a compassionate conceptualizationIdentifying the contingenciesIndividualized treatment plan
Role-plays
Yes, let’s do this
Does anyone have a difficult client?
LET’S PRACTICE

Your Homework:
Watch a YouTube video of a good CBT session

Questions & Answers