castration-resistant prostate cancer: are we done with hormone therapy?
DESCRIPTION
The clinical data from abiraterone acetate and enzalutamide confirm continued androgen receptor (AR) addiction in a significant proportion of castration-resistant prostate cancers (CRPC). Abiraterone acetate is a specific inhibitor of CYP17A1 and results in significant suppression of serum androgenic steroids and estrogen. Enzalutamide is a potent AR antagonist. Both agents improve the survival of CRPC patients. However patients invariably progress, often with a rise in PSA suggesting resumption of transcription of hormone-regulated genes. If abiraterone or enzalutamide-resistant cancers remain addicted to steroid receptor signaling, including but not exclusive to AR, how does reactivation occur? Or if cancers lose this addiction, do the same hormone-regulated oncogenic mechanisms continue to drive the disease? The future development of therapeutics for CRPC should be informed by an understanding of the mechanisms underlying disease progression following treatment with these novel agents. Tumor responses are being observed with sequential targeting of AR or steroidogenesis after abiraterone or enzalutamide but preliminary reports suggest lower response rates. This highlights the requirement for patient selection for future successful Phase III trials. Our experience with obtaining CRPC tumor biopsies and using them for molecular characterization will be discussed together with data obtained from circulating biomarkers including circulating tumor cells and circulating plasma nucleic acids.TRANSCRIPT

Are We Done with Hormone Therapy?
Gerhardt A6ard MD MRCP PhD Cancer Research UK Clinician ScienAst The InsAtute of Cancer Research and
the Royal Marsden NHS FoundaAon Trust

Financial disclosure
• Abiraterone was developed at The InsAtute of Cancer Research and is licensed to Cougar Biotechnology/J&J. The ICR also has a commercial interest in the development of inhibitors of PI3K, AKT and HSP90.
• I am included in The ICR co-‐inventors’ reward scheme of abiraterone.
• I receive research funding from Astra Zeneca and Genentech.
• I have received honoraria, lecture fees and travel support from Sanofi, Janssen, Veridex, Ipsen, NovarAs, Millenium PharmaceuAcals, Ventana/Roche.
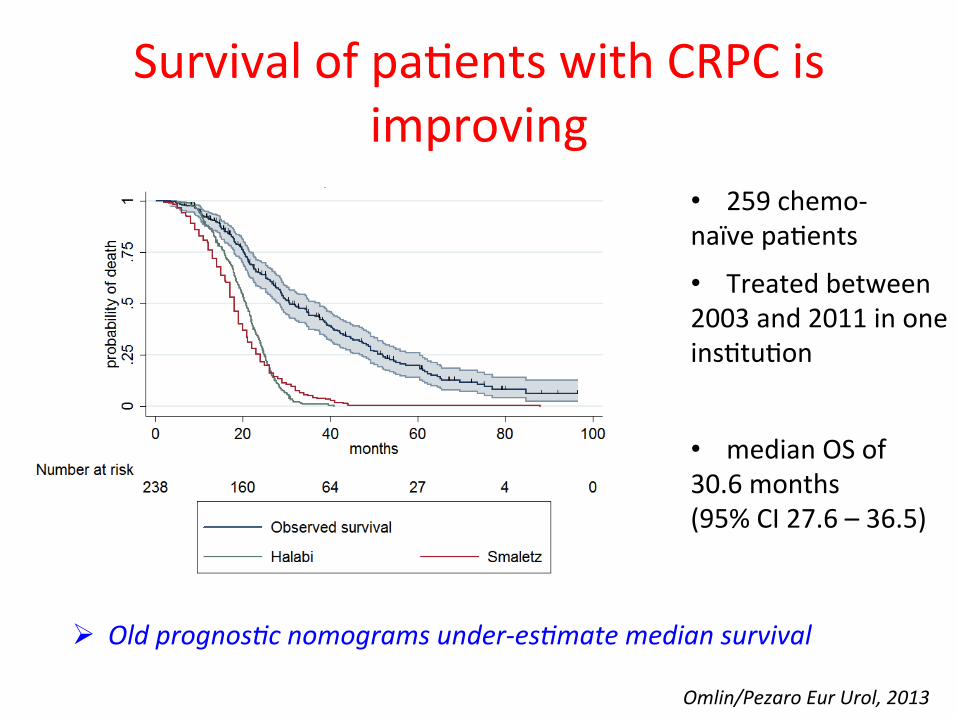
Survival of paAents with CRPC is improving
Omlin/Pezaro Eur Urol, 2013
• 259 chemo-‐ naïve paAents
• median OS of 30.6 months (95% CI 27.6 – 36.5)
• Treated between 2003 and 2011 in one insAtuAon
Ø Old prognos:c nomograms under-‐es:mate median survival
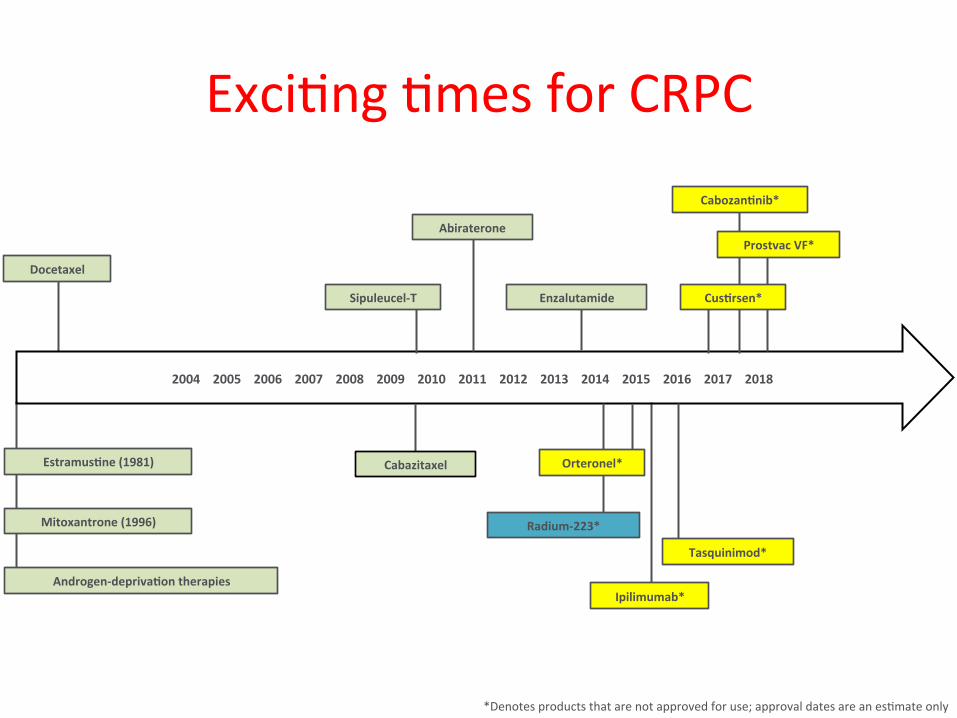
ExciAng Ames for CRPC
*Denotes products that are not approved for use; approval dates are an esAmate only
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Abiraterone
Cabazitaxel
Sipuleucel-‐T
Docetaxel
Mitoxantrone (1996)
Androgen-‐deprivaFon therapies
EstramusFne (1981)
Enzalutamide
CabozanFnib*
Prostvac VF*
Ipilimumab*
Tasquinimod*
CusFrsen*
Radium-‐223*
Orteronel*
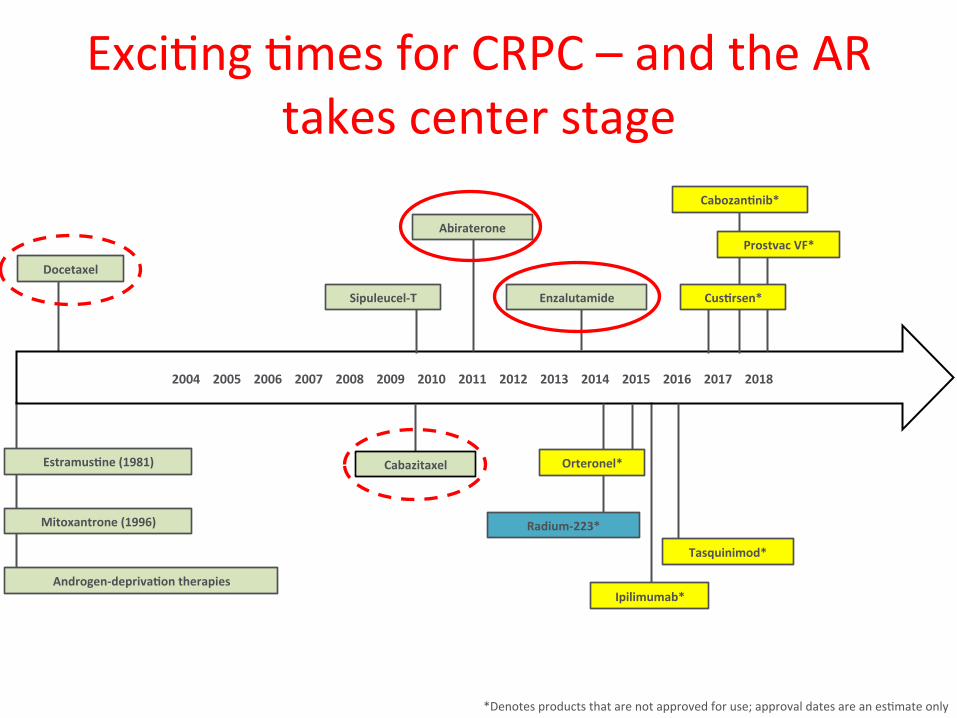
ExciAng Ames for CRPC – and the AR takes center stage
*Denotes products that are not approved for use; approval dates are an esAmate only
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Abiraterone
Cabazitaxel
Sipuleucel-‐T
Docetaxel
Mitoxantrone (1996)
Androgen-‐deprivaFon therapies
EstramusFne (1981)
Enzalutamide
CabozanFnib*
Prostvac VF*
Ipilimumab*
Tasquinimod*
CusFrsen*
Radium-‐223*
Orteronel*
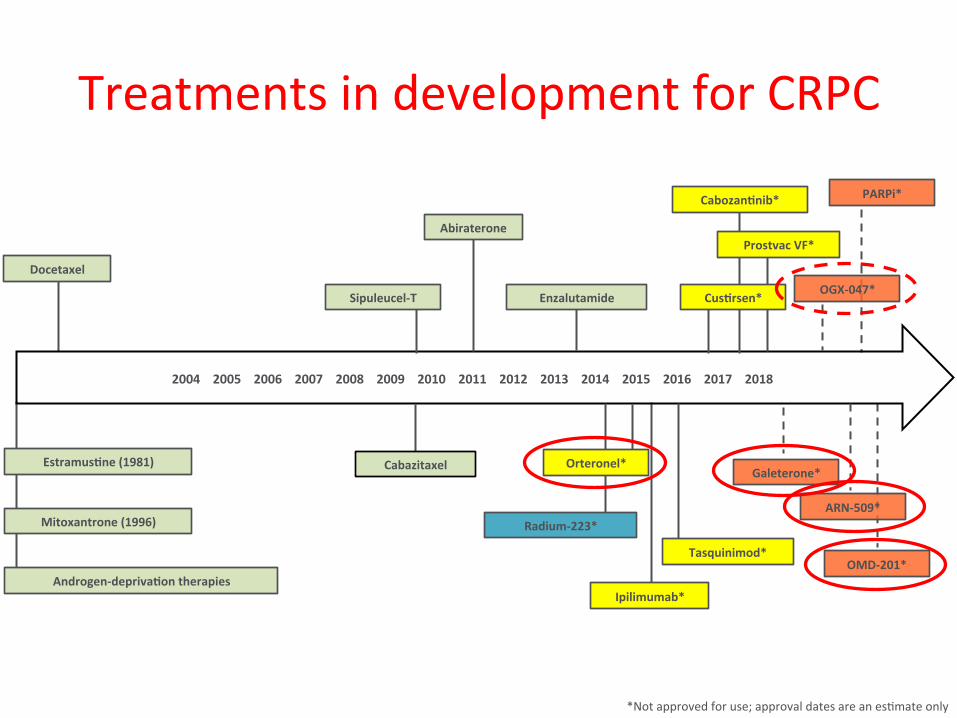
Treatments in development for CRPC
*Not approved for use; approval dates are an esAmate only
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Abiraterone
Cabazitaxel
Sipuleucel-‐T
Docetaxel
Mitoxantrone (1996)
Androgen-‐deprivaFon therapies
EstramusFne (1981)
CabozanFnib*
Prostvac VF*
Ipilimumab*
Tasquinimod*
CusFrsen*
Radium-‐223*
Orteronel* Galeterone*
ARN-‐509*
OGX-‐047*
OMD-‐201*
PARPi*
Enzalutamide
Challenges we face as physicians treaAng CRPC
• Is there a role for sequencing 2nd and 3rd generaAon AR targeAng drugs?
• Is there a role for combinaAons of AR targeAng drugs?
• How do we select paAents for one drug versus another?
• Which drug/class of agents do we prioriAse for combinaAon studies?
A@ard and de Bono, Clin Cancer Res, 2011
Ø A significant number of paAents with castraAon-‐resistant prostate cancer have disease that remains driven by ligand acAvaAon of the androgen receptor
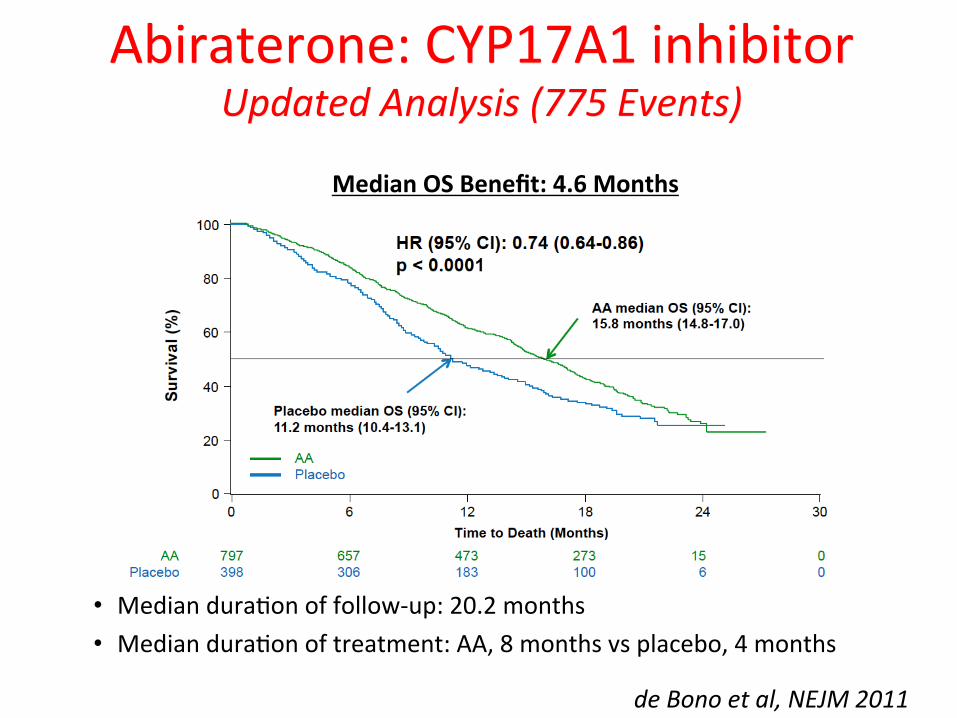
Abiraterone: CYP17A1 inhibitor Updated Analysis (775 Events)
• Median duraAon of follow-‐up: 20.2 months • Median duraAon of treatment: AA, 8 months vs placebo, 4 months
Median OS Benefit: 4.6 Months
de Bono et al, NEJM 2011
Ø Abiraterone inhibits adrenal CYP17A1 and causes significant suppression of serum androgens and estrogens
Ø Tumor CYP17A1-‐dependent synthesis of steroidogenic ligands has been demonstrated in preclinical models but remains unproven in paAents (albeit supported by strong circumstanAal data)
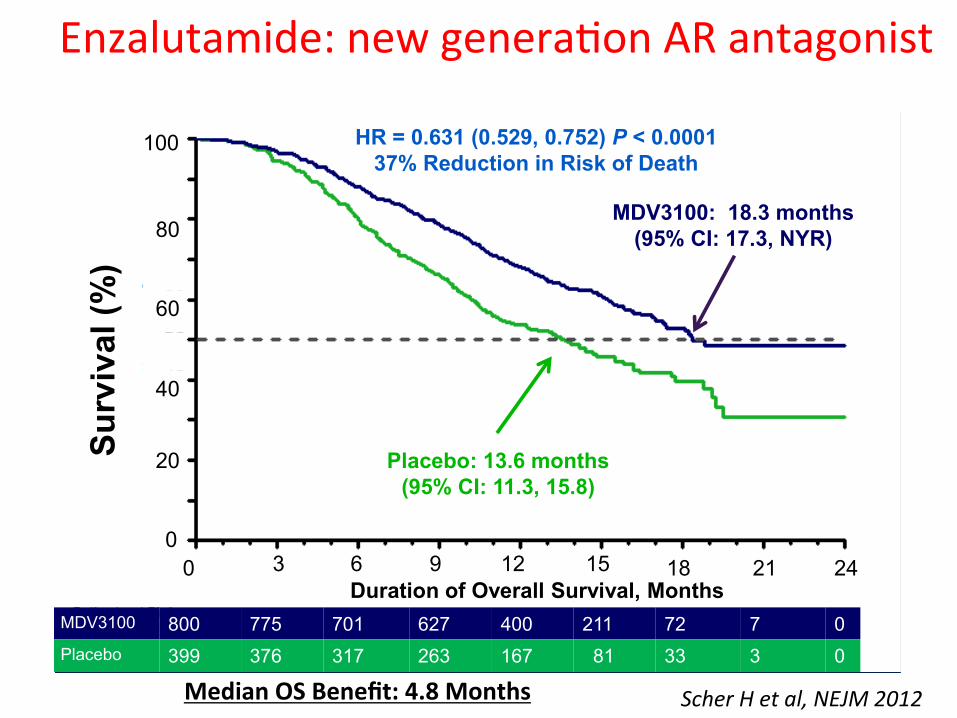
Enzalutamide: new generaAon AR antagonist
Scher H et al, NEJM 2012 1
Surv
ival
(%)
100
80
60
MDV3100 800 775 701 627 400 211 72 7 0Placebo 399 376 317 263 167 81 33 3 0
MDV3100: 18.3 months (95% CI: 17.3, NYR)
Placebo: 13.6 months (95% CI: 11.3, 15.8)
HR = 0.631 (0.529, 0.752) P < 0.000137% Reduction in Risk of Death
40
20
00 3 6 9
Duration of Overall Survival, Months12 15 18 21 24
Median OS Benefit: 4.8 Months
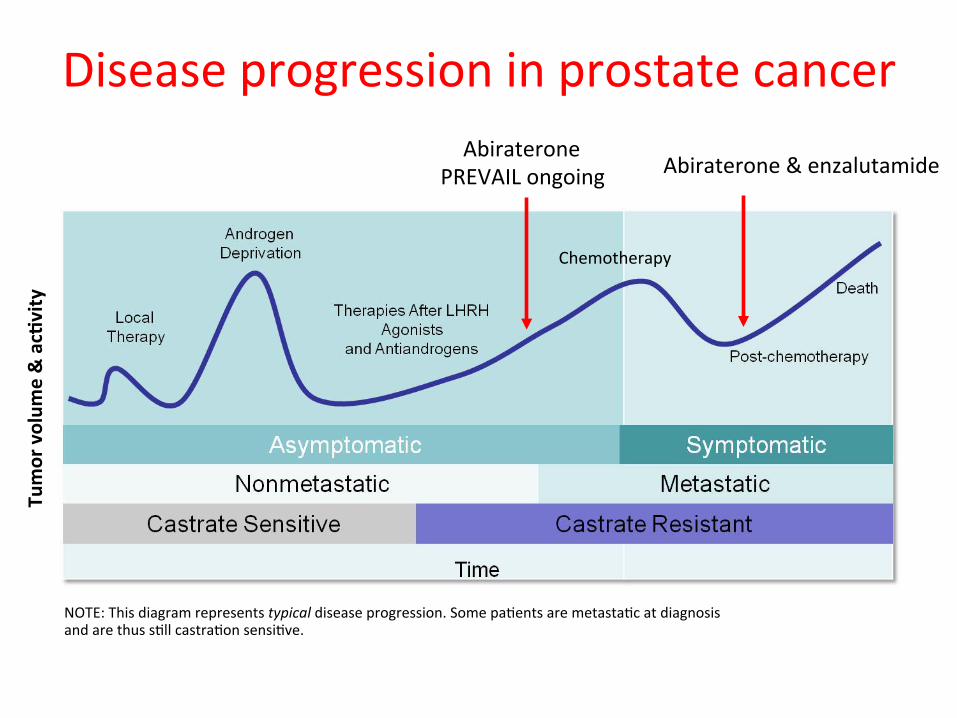
Disease progression in prostate cancer
Chemotherapy
Tumor volum
e & acFvity
NOTE: This diagram represents typical disease progression. Some paAents are metastaAc at diagnosis and are thus sAll castraAon sensiAve.
Abiraterone & enzalutamide Abiraterone
PREVAIL ongoing
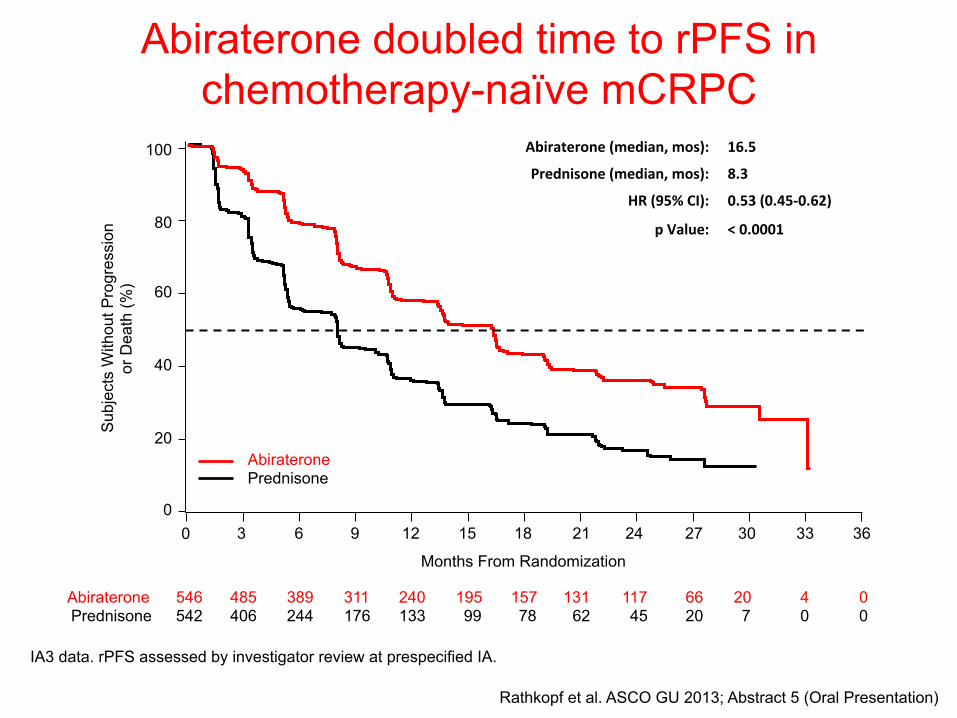
Abiraterone doubled time to rPFS in chemotherapy-naïve mCRPC
IA3 data. rPFS assessed by investigator review at prespecified IA.
100
80
60
40
20
0 0
Sub
ject
s W
ithou
t Pro
gres
sion
or
Dea
th (%
)
6 12 18 30 36 24
546 542
389 244
240 133
157 78
20 7
0 0
Abiraterone Prednisone
117 45
Months From Randomization
Abiraterone Prednisone
Abiraterone (median, mos): 16.5
Prednisone (median, mos): 8.3
HR (95% CI): 0.53 (0.45-‐0.62)
p Value: < 0.0001
15 9 3 21 27 33
485 406
311 176
195 99
131 62
66 20
4 0
Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)
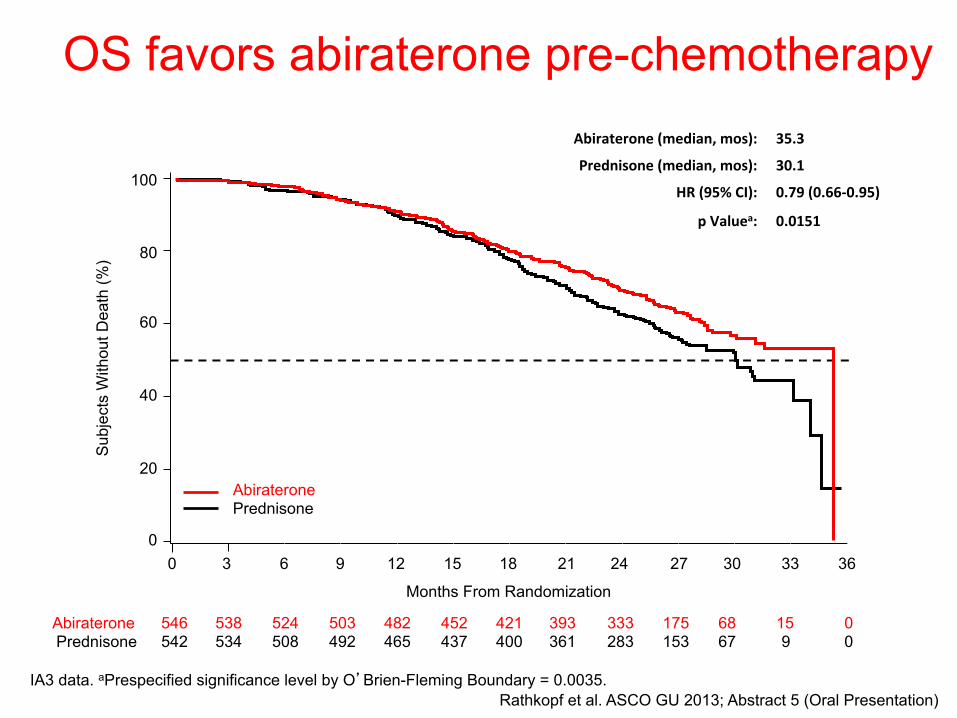
OS favors abiraterone pre-chemotherapy
IA3 data. aPrespecified significance level by O’Brien-Fleming Boundary = 0.0035.
100
80
60
40
20
0
Sub
ject
s W
ithou
t Dea
th (%
)
6 12 18 30 36 24
546 542
524 508
482 465
421 400
68 67
0 0
Abiraterone Prednisone
333 283
Months From Randomization
Abiraterone Prednisone
Abiraterone (median, mos): 35.3
Prednisone (median, mos): 30.1
HR (95% CI): 0.79 (0.66-‐0.95)
p Valuea: 0.0151
15 9 3 21 27 33
538 534
503 492
452 437
393 361
175 153
15 9
Rathkopf et al. ASCO GU 2013; Abstract 5 (Oral Presentation)
0
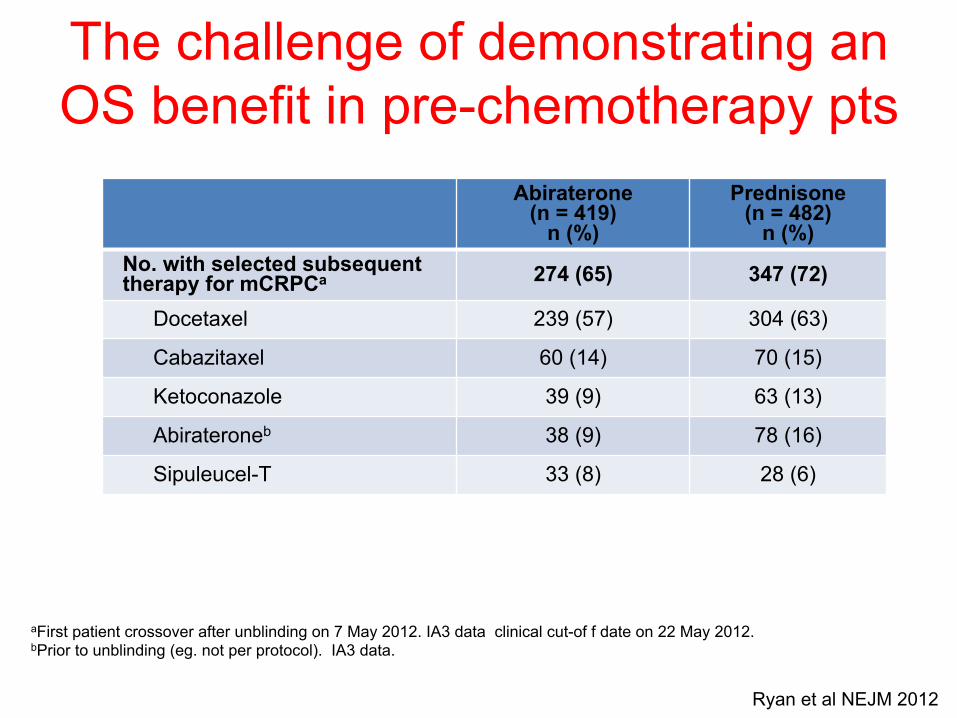
The challenge of demonstrating an OS benefit in pre-chemotherapy pts
aFirst patient crossover after unblinding on 7 May 2012. IA3 data clinical cut-of f date on 22 May 2012. bPrior to unblinding (eg. not per protocol). IA3 data.
Abiraterone (n = 419)
n (%)
Prednisone (n = 482)
n (%) No. with selected subsequent therapy for mCRPCa 274 (65) 347 (72)
Docetaxel 239 (57) 304 (63)
Cabazitaxel 60 (14) 70 (15)
Ketoconazole 39 (9) 63 (13)
Abirateroneb 38 (9) 78 (16)
Sipuleucel-T 33 (8) 28 (6)
Ryan et al NEJM 2012
Ø However, although >90% of paAents respond to castraAon, the response rate to subsequent AR targeAng is up to 50-‐60%

PSA declines with abiraterone (or enzalutamide)
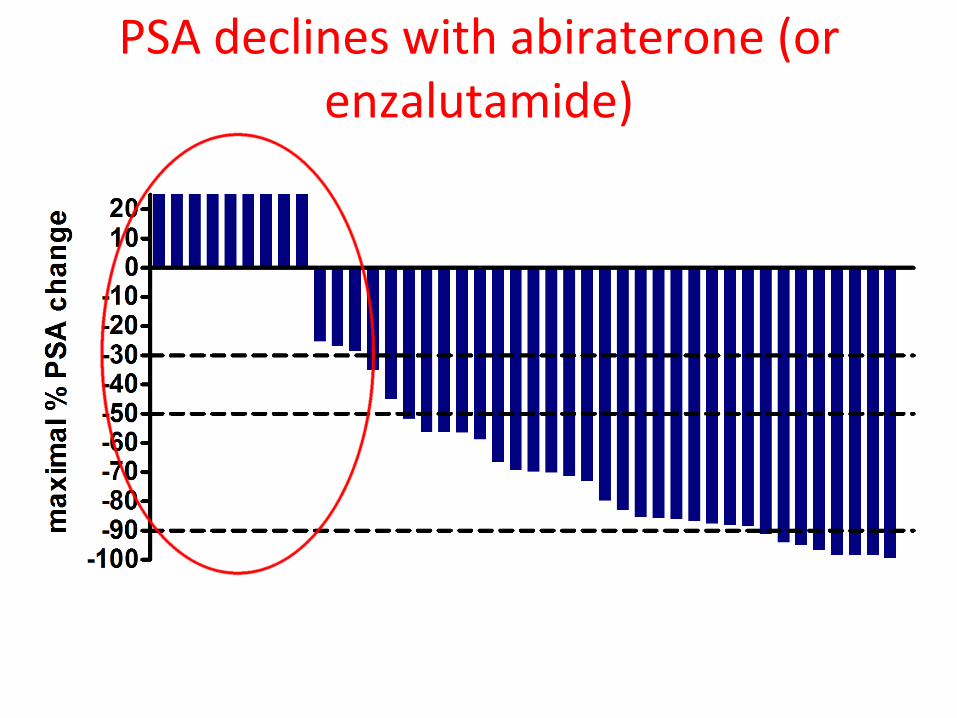
PSA declines with abiraterone (or enzalutamide)

What is the evidence to support conAnued targeAng of the AR?
• Hypothesis 1: AR/steroid receptor signaling remains important in a significant proporAon of paAents progressing on abi/enza
• PSA rising at progression in a significant number of paAents Ø Is this AR driven?
• Responses with repeated targeAng of AR • AR shows conAnued nuclear expression in a proporAon of paAents

Combined Image
DAPI AR Pan-‐CK
Ki-‐67 CD45
Nuclear expression of AR in a paAent progressing on abiraterone
Combined
TargeAng the AR in abi/enza resistant CRPC
• Hypothesis 2: CYP17A1 inhibiAon without concomitant exogenous glucocorAcoids will improve efficacy in addiAon to reducing toxicity

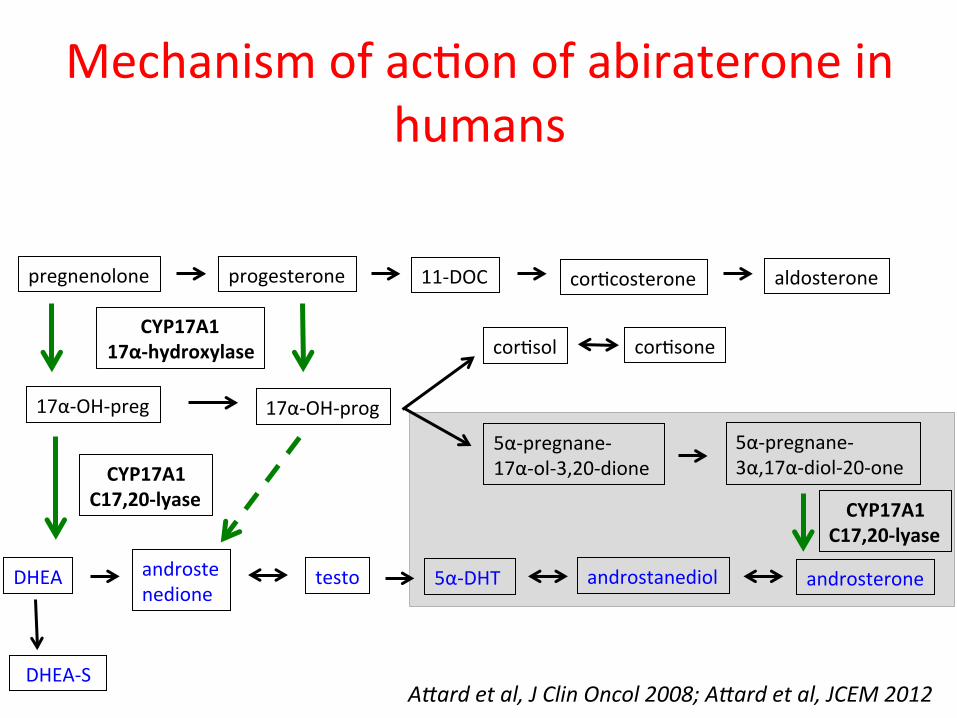
Mechanism of acAon of abiraterone in humans
pregnenolone progesterone 11-‐DOC corAcosterone aldosterone
17α-‐OH-‐preg 17α-‐OH-‐prog
corAsol corAsone
5α-‐pregnane-‐ 17α-‐ol-‐3,20-‐dione
5α-‐pregnane-‐ 3α,17α-‐diol-‐20-‐one
DHEA
DHEA-‐S
androstenedione
testo 5α-‐DHT androstanediol androsterone
CYP17A1 17α-‐hydroxylase
CYP17A1 C17,20-‐lyase CYP17A1
C17,20-‐lyase
A@ard et al, J Clin Oncol 2008; A@ard et al, JCEM 2012
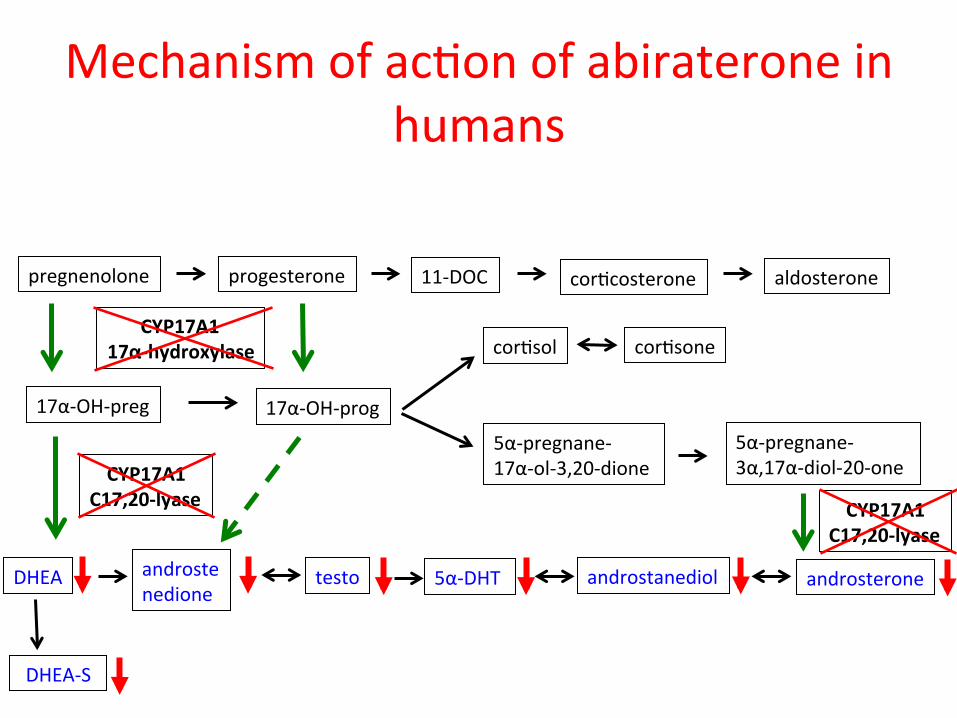
Mechanism of acAon of abiraterone in humans
pregnenolone progesterone 11-‐DOC corAcosterone aldosterone
17α-‐OH-‐preg 17α-‐OH-‐prog
corAsol corAsone
5α-‐pregnane-‐ 17α-‐ol-‐3,20-‐dione
5α-‐pregnane-‐ 3α,17α-‐diol-‐20-‐one
DHEA
DHEA-‐S
androstenedione
testo 5α-‐DHT androstanediol androsterone
CYP17A1 17α-‐hydroxylase
CYP17A1 C17,20-‐lyase CYP17A1
C17,20-‐lyase
A@ard et al, J Clin Oncol 2008; A@ard et al, JCEM 2012
Mechanism of acAon of abiraterone in humans
pregnenolone progesterone 11-‐DOC corAcosterone aldosterone
17α-‐OH-‐preg 17α-‐OH-‐prog
corAsol corAsone
5α-‐pregnane-‐ 17α-‐ol-‐3,20-‐dione
5α-‐pregnane-‐ 3α,17α-‐diol-‐20-‐one
DHEA
DHEA-‐S
androstenedione
testo 5α-‐DHT androstanediol androsterone
CYP17A1 17α-‐hydroxylase
CYP17A1 C17,20-‐lyase CYP17A1
C17,20-‐lyase
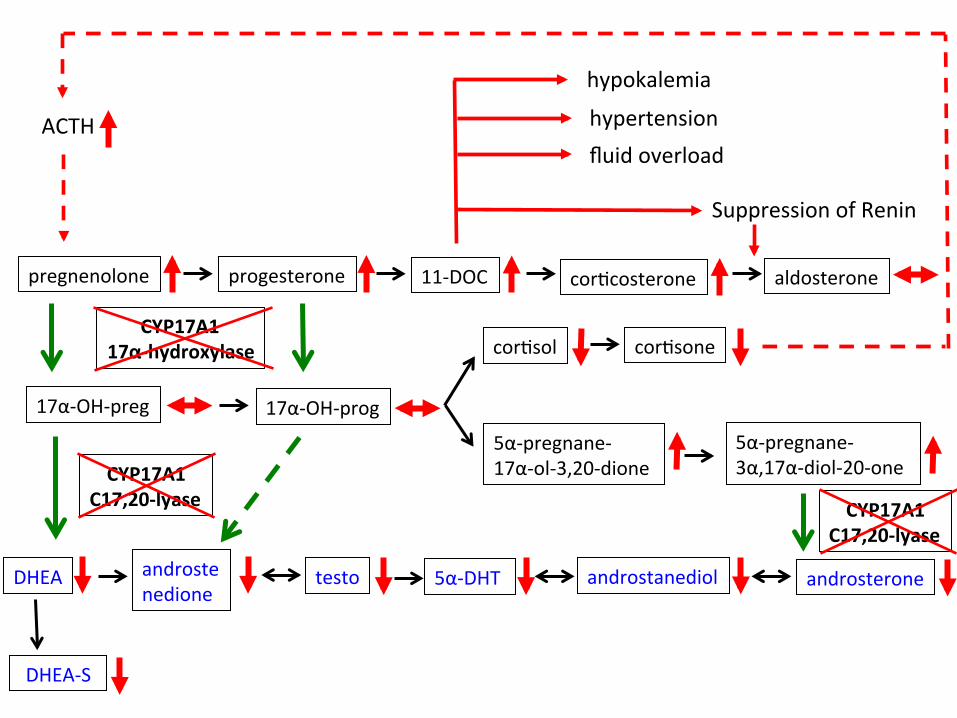
pregnenolone progesterone 11-‐DOC corAcosterone aldosterone
17α-‐OH-‐preg 17α-‐OH-‐prog
corAsol corAsone
5α-‐pregnane-‐ 17α-‐ol-‐3,20-‐dione
5α-‐pregnane-‐ 3α,17α-‐diol-‐20-‐one
DHEA
DHEA-‐S
androstenedione
testo 5α-‐DHT androstanediol androsterone
CYP17A1 17α-‐hydroxylase
CYP17A1 C17,20-‐lyase CYP17A1
C17,20-‐lyase
ACTH
hypokalemia
hypertension fluid overload
Suppression of Renin
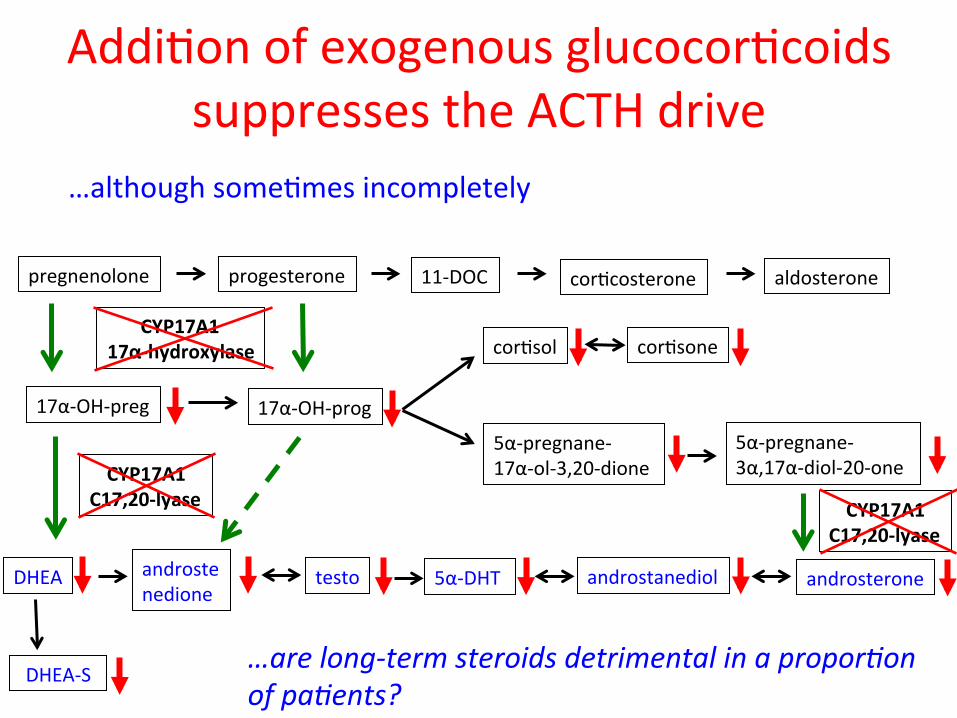
AddiAon of exogenous glucocorAcoids suppresses the ACTH drive
pregnenolone progesterone 11-‐DOC corAcosterone aldosterone
17α-‐OH-‐preg 17α-‐OH-‐prog
corAsol corAsone
5α-‐pregnane-‐ 17α-‐ol-‐3,20-‐dione
5α-‐pregnane-‐ 3α,17α-‐diol-‐20-‐one
DHEA
DHEA-‐S
androstenedione
testo 5α-‐DHT androstanediol androsterone
CYP17A1 17α-‐hydroxylase
CYP17A1 C17,20-‐lyase CYP17A1
C17,20-‐lyase
…although someAmes incompletely
…are long-‐term steroids detrimental in a propor:on of pa:ents?

VT-‐464: can complete & irreversible C17,20-‐lyase inhibiAon be achieved
without corAsol suppression?
Compound Human CYP17 Lyase IC50 (mM)
Human CYP17 Hydroxylase
IC50 (mM)
Human CYP17 Lyase/Hydroxylase
Selectivity
VT-464 0.069 0.670 9.7
Abiraterone 0.015 0.0025 0.17
0
10
20
30
Abiraterone VT-‐464 Vehicle
ng/m
l
Pregnenolone
0 5 10
ng/m
l
DeoxycorFcosterone
0
10
20
30
40
Abiraterone VT-‐464 Vehicle
ng/m
l
Progesterone
0
200
400
Abiraterone VT-‐464 Vehicle
ng/m
l
CorFcosterone
Eisner et al, ENDO 2012
VT-‐464 is almost 60-‐fold more lyase-‐selecAve than abiraterone.
VT-‐464: can complete & irreversible C17,20-‐lyase inhibiAon be achieved
without corAsol suppression? Phase 1/2 study underway in chemotherapy-‐naïve CRPC paAents: • Exogeneous glucocorAcoids not required to date • Dose-‐related decreases in androgens observed with no
impact on corAsol, pregnenolone, progesterone or corAcosterone levels
• PSA responses observed in current dose cohort (one confirmed response @ 12 weeks with 92% decrease from baseline)
• Safety and tolerability acceptable to date
A6ard, PCF Annual retreat Oct 2012, Oral PresentaAon Royal Marsden/University of Athens/St Gallen
TargeAng the AR in abi/enza resistant CRPC
• Hypothesis 3: LBD targeAng using structurally different AR antagonists/ with funcAonally disAnct properAes (AR degradaAon?)/ lower drug brain levels will prove effecAve
• (or new AR targe:ng drugs can be posi:oned differently)
• ARN-‐509
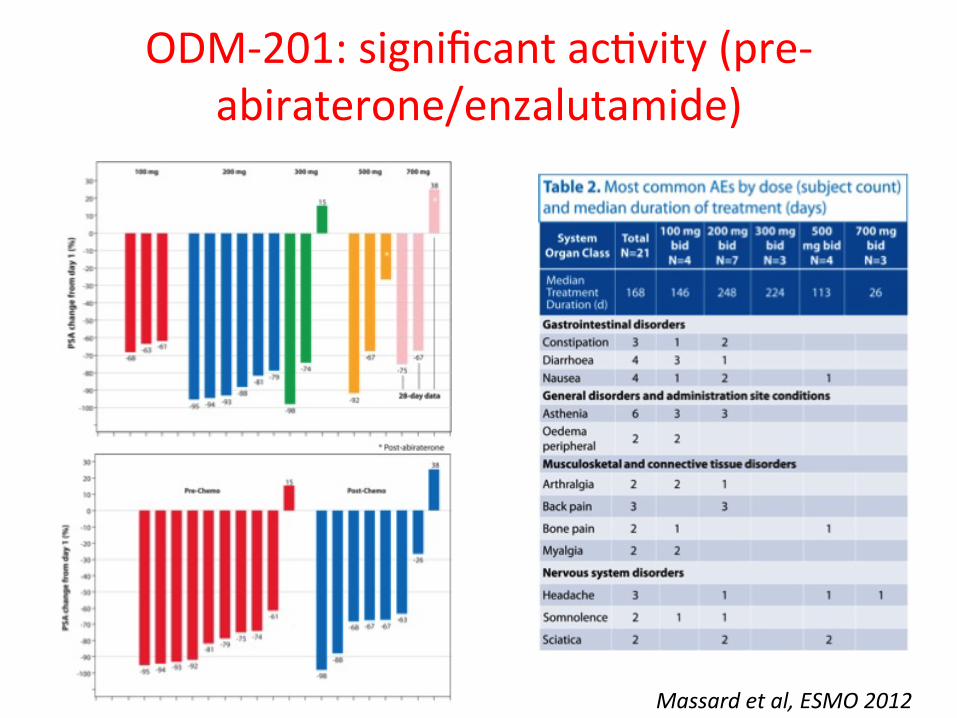
ODM-‐201: significant acAvity (pre-‐abiraterone/enzalutamide)
Massard et al, ESMO 2012
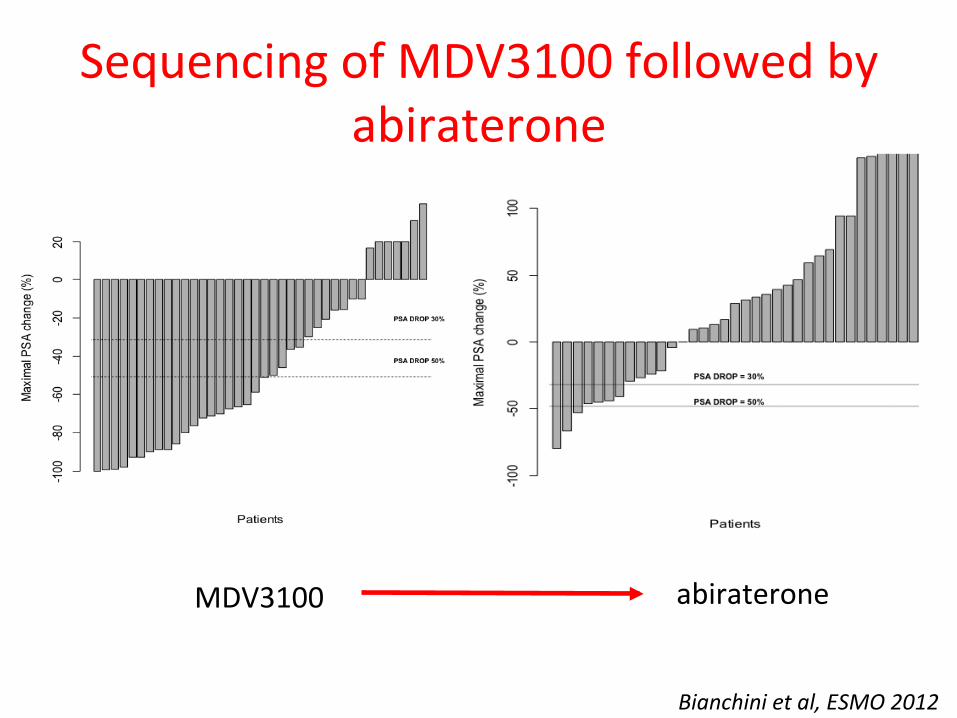
Sequencing of MDV3100 followed by abiraterone
MDV3100 abiraterone
Bianchini et al, ESMO 2012
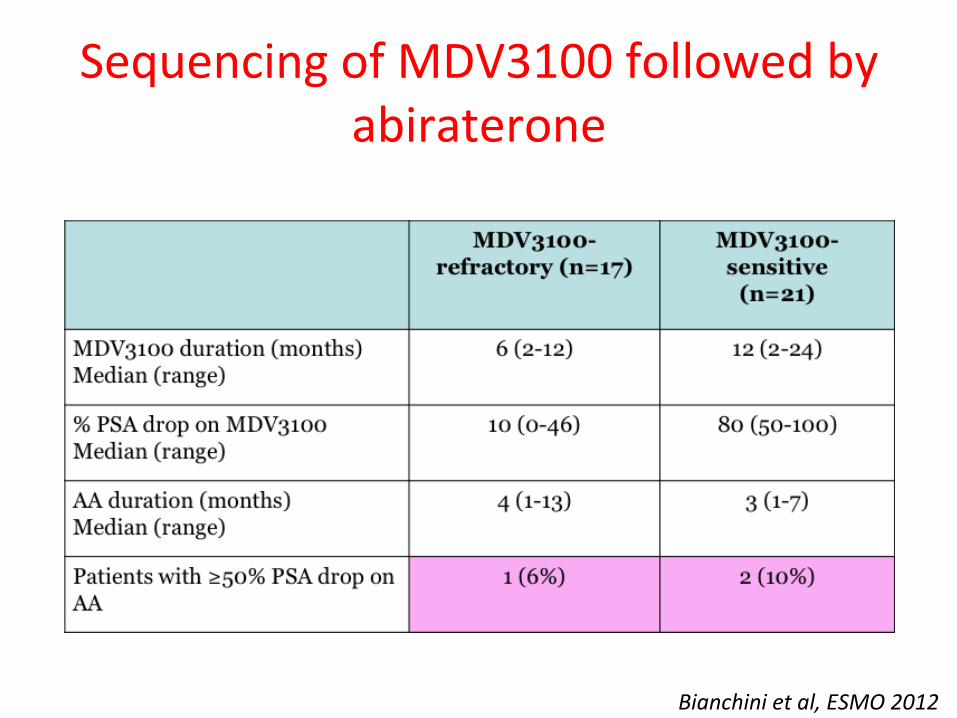
Sequencing of MDV3100 followed by abiraterone
Bianchini et al, ESMO 2012
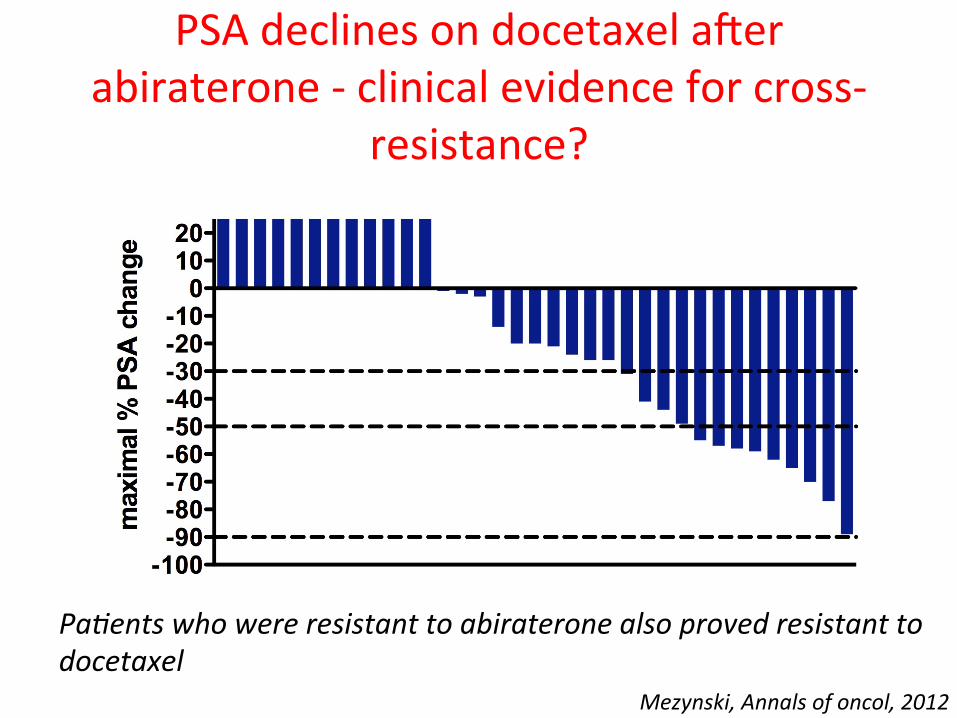
PSA declines on docetaxel aver abiraterone -‐ clinical evidence for cross-‐
resistance?
Mezynski, Annals of oncol, 2012
Pa:ents who were resistant to abiraterone also proved resistant to docetaxel
TargeAng the AR in abi/enza resistant CRPC
• Hypothesis 4: Re-‐acAvaAon of AR occurs through LBD-‐independent mechanisms – Repeated LBD targeAng will prove ineffecAve in the majority of paAents
• Do AR splice variants cause resistance?
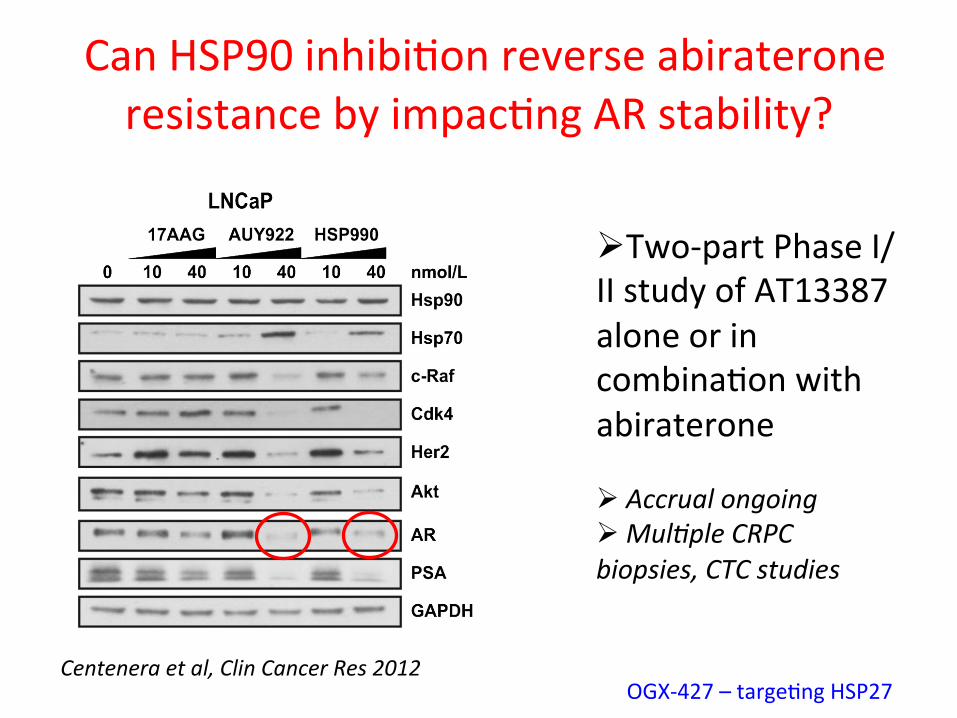
Can HSP90 inhibiAon reverse abiraterone resistance by impacAng AR stability?
Centenera et al, Clin Cancer Res 2012
Ø Two-‐part Phase I/II study of AT13387 alone or in combinaAon with abiraterone Ø Accrual ongoing Ø Mul:ple CRPC biopsies, CTC studies
OGX-‐427 – targeAng HSP27
TargeAng the AR in abi/enza resistant CRPC
Ø Hypothesis 5: EvaluaAon of an unselected
paAent populaAon will be unsuccessful
Ø AcAvity in treatment-‐naïve CRPC but can a survival advantage be achieved post abi/enza?

AR-‐independent disease progression • 75 year old previously progressed on castraAon, bicalutamide, dexamethasone – Started abiraterone and prednisone in Jan 2010 – Baseline PSA 50ng/dl – Good PSA response (nadir: 6.7, July 2010)
March 2011 June 1 Sep 15 Nov 8 Dec 10 11 18 18 11
Biopsied x2
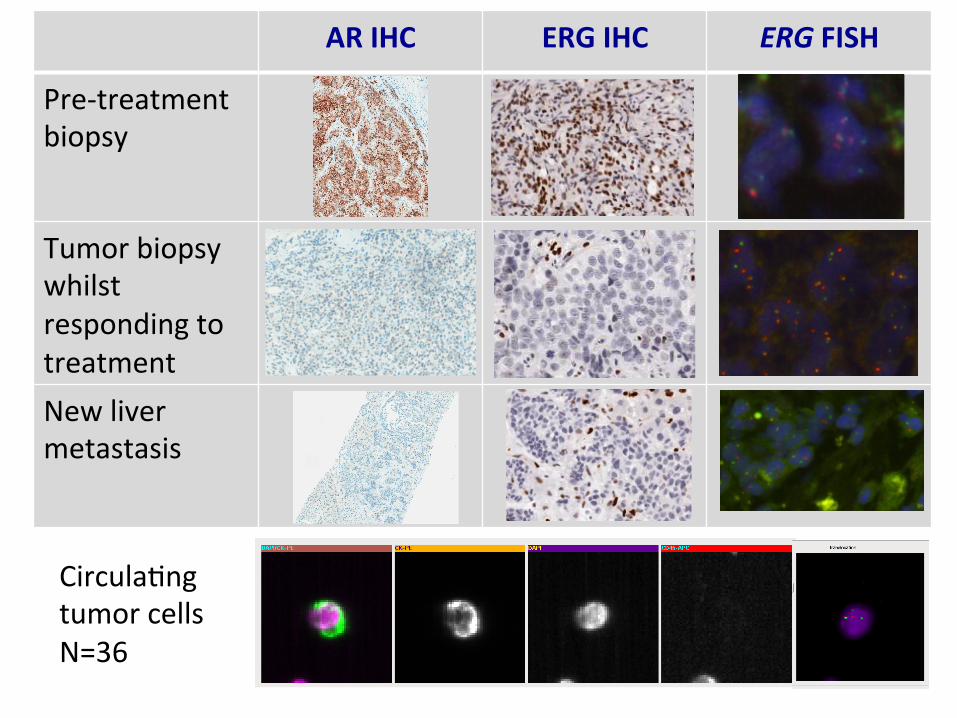
AR IHC ERG IHC ERG FISH
Pre-‐treatment biopsy
Tumor biopsy whilst responding to treatment New liver metastasis
CirculaAng tumor cells N=36
How can we select paAents?
Ø Response rates to abiraterone are equivalent in PTEN loss and PTEN normal paAents
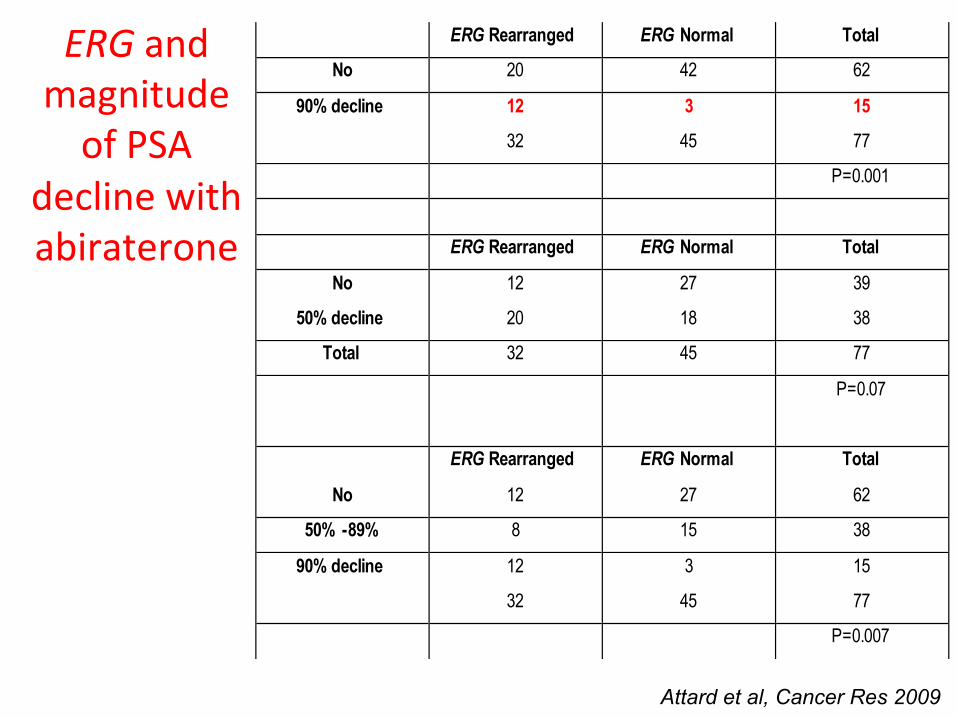
ERG Rearranged ERG Normal Total
No 20 42 62
90% decline 12 3 15
32 45 77
P=0.001
ERG Rearranged ERG Normal Total
No 12 27 39
50% decline 20 18 38
Total 32 45 77
P=0.07
ERG Rearranged ERG Normal Total
No 12 27 62
50% -89% 8 15 38
90% decline 12 3 15
32 45 77
P=0.007
ERG and magnitude of PSA
decline with abiraterone
Attard et al, Cancer Res 2009
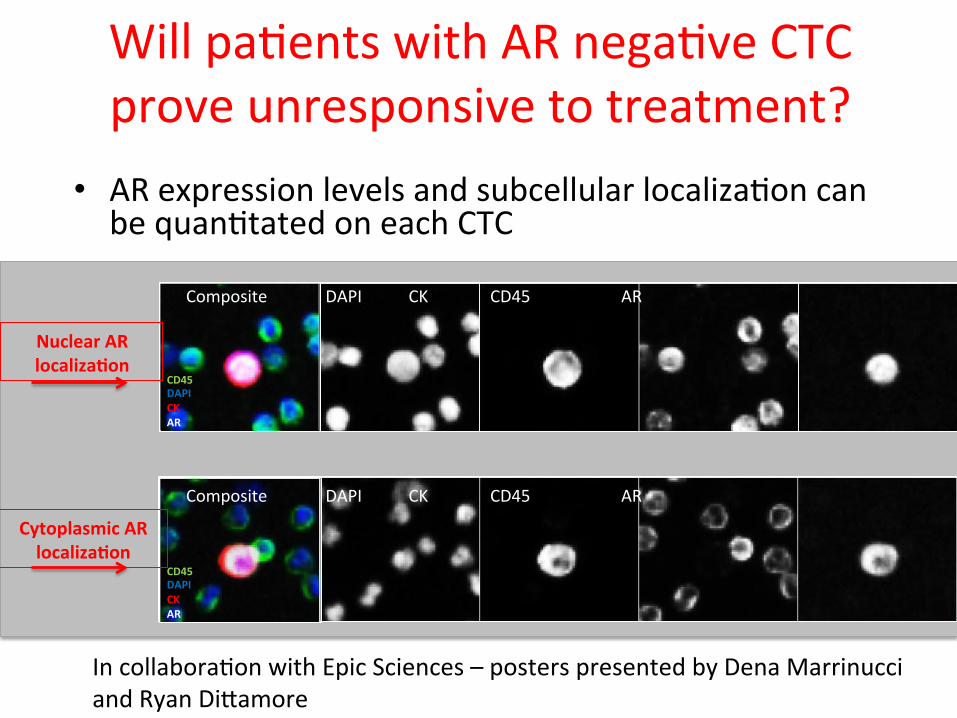
Will paAents with AR negaAve CTC prove unresponsive to treatment?
• AR expression levels and subcellular localizaAon can be quanAtated on each CTC
Composite DAPI CK CD45 AR
Composite DAPI CK CD45 AR
Nuclear AR localizaFon
Cytoplasmic AR localizaFon
CD45 DAPI CK AR
CD45 DAPI CK AR
In collaboraAon with Epic Sciences – posters presented by Dena Marrinucci and Ryan Di6amore
Hit the AR as hard as possible in AR-‐driven prostate cancer
• Hypothesis 6: Can we improve the efficacy of AR targeAng by combining CYP17A1 inhibitors with AR antagonists?
Hit the AR as hard as possible in AR-‐driven prostate cancer
• Hypothesis 6: Can we improve the efficacy of AR targeAng by combining CYP17A1 inhibitors with AR antagonists?
• Does abiraterone achieve a truly ligand free state?
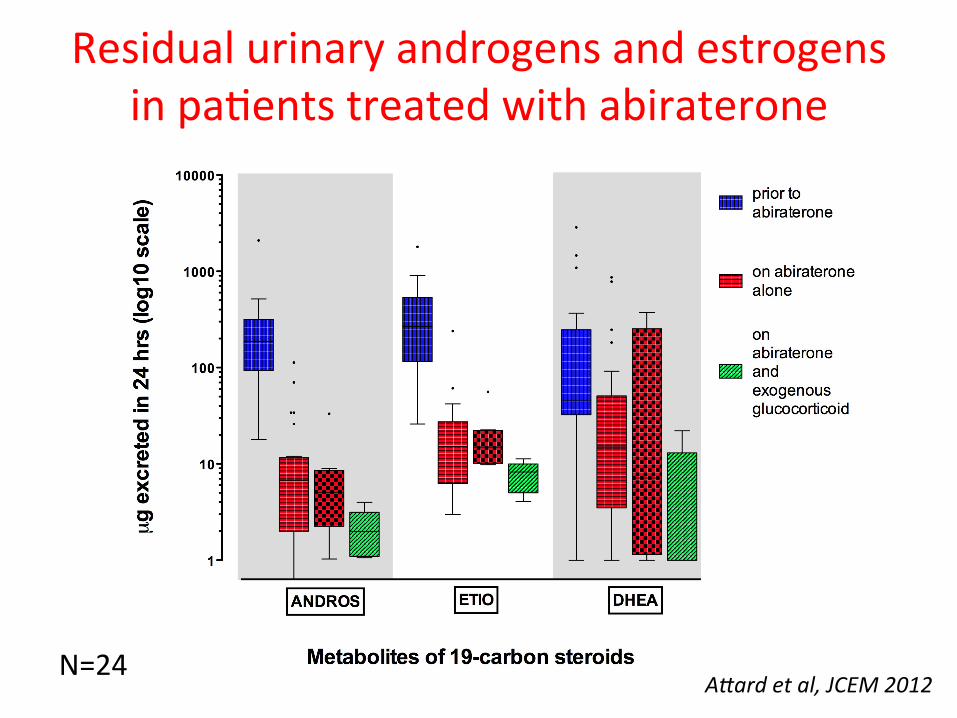
Residual urinary androgens and estrogens in paAents treated with abiraterone
A@ard et al, JCEM 2012 N=24

Can resistance occur through selecAon of AR mutaAons acAvated by exogenous glucocorAcoids given with abiraterone?
T877A L701H AR found in MDA Pca 2b cells
Richards et al, Cancer Res 2012 Zhao et al, Nature Med 2000
Ø Abiraterone is a weak AR antagonist in addiAon to a potent CYP17A1 inhibitor
Ø Uncertain relevance in paAents Ø Could explain some of the acAvity reported in preclinical models
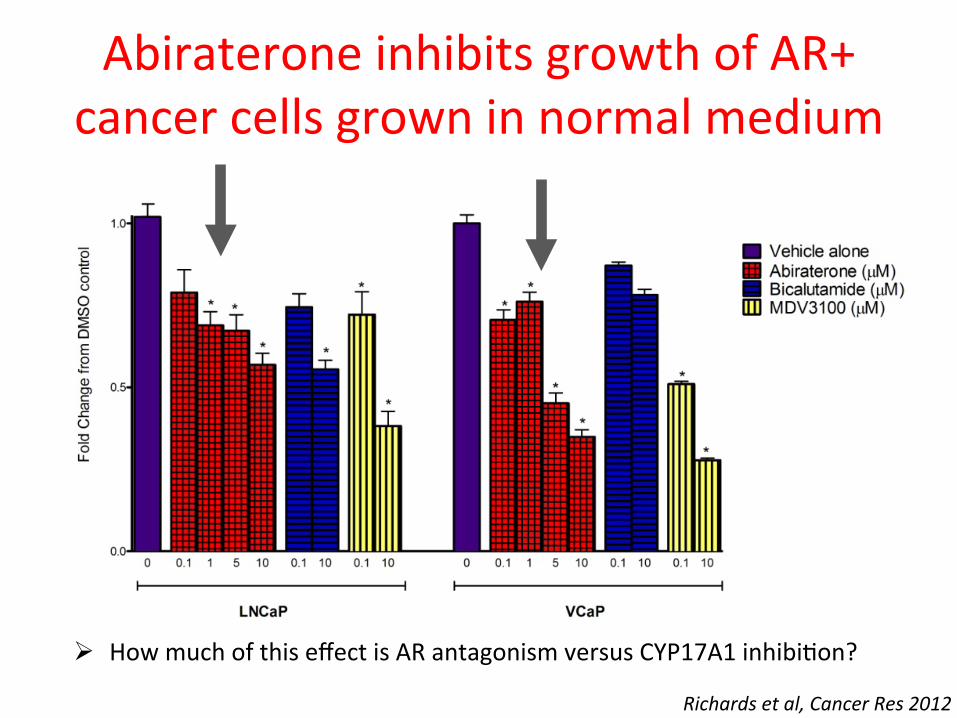
Abiraterone inhibits growth of AR+ cancer cells grown in normal medium
Ø How much of this effect is AR antagonism versus CYP17A1 inhibiAon?
Richards et al, Cancer Res 2012

Abiraterone inhibits R1881 sAmulated ARR3-‐luciferase acAvity
Ø No acAvaAon observed with previously described AR mutaAons
Ø AddiAon of an anA-‐androgen to abiraterone could reverse resistance (or increase response rate)
Ø AddiAon of an anA-‐androgen to abiraterone could reverse resistance (or increase response rate)
Ø Is there any benefit to adding a CYP17A1 inhibitor to an anA-‐androgen?
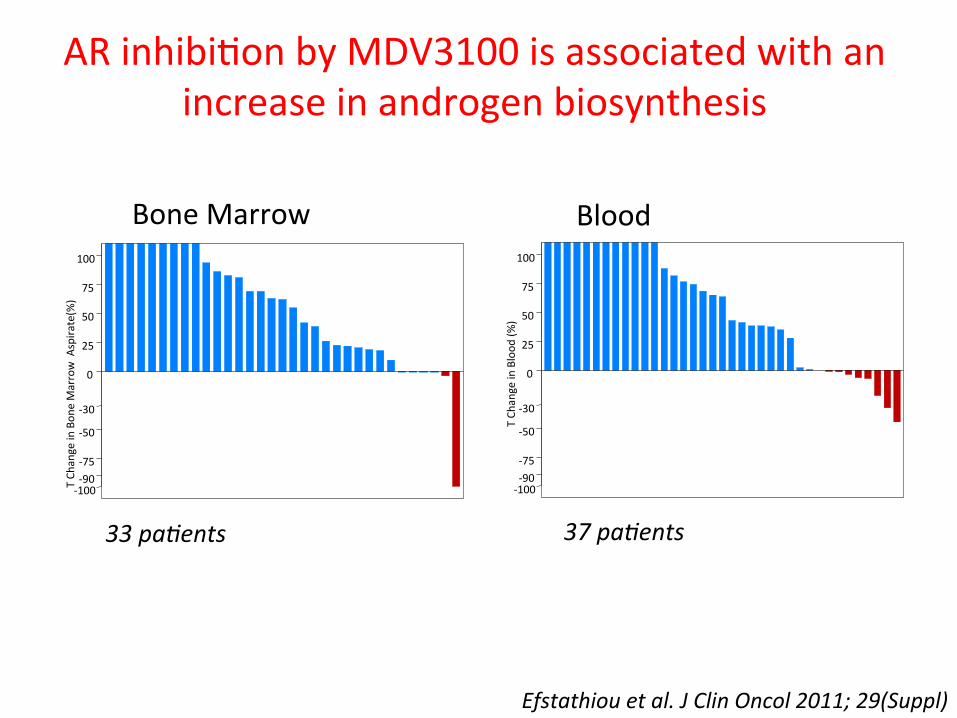
AR inhibiAon by MDV3100 is associated with an increase in androgen biosynthesis
T Ch
ange in Bon
e Marrow A
spira
te(%
)
-‐100 -‐90 -‐75 -‐50 -‐30 0 25 50 75 100
37 pa:ents 33 pa:ents T Ch
ange in Blood
(%)
-‐100 -‐90 -‐75 -‐50 -‐30 0 25 50 75 100
Efstathiou et al. J Clin Oncol 2011; 29(Suppl)
Bone Marrow Blood
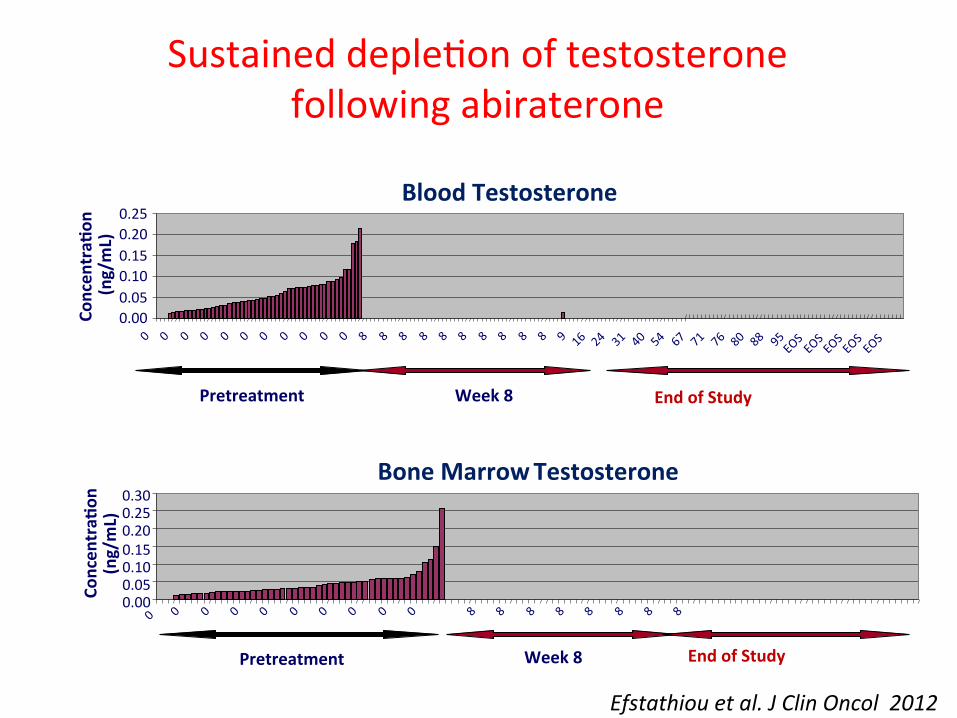
Blood Testosterone
0.00 0.05 0.10 0.15 0.20 0.25
Week 8
Concen
traF
on
(ng/mL)
Pretreatment
Bone Marrow Testosterone
0.00 0.05 0.10 0.15 0.20 0.25 0.30
Week 8
Concen
traF
on
(ng/mL)
End of Study Pretreatment
Sustained depleAon of testosterone following abiraterone
End of Study
Efstathiou et al. J Clin Oncol 2012

Increased hormone levels reduce inhibiAon of AR acAvity by MDV3100
Richards et al, Cancer Res 2012
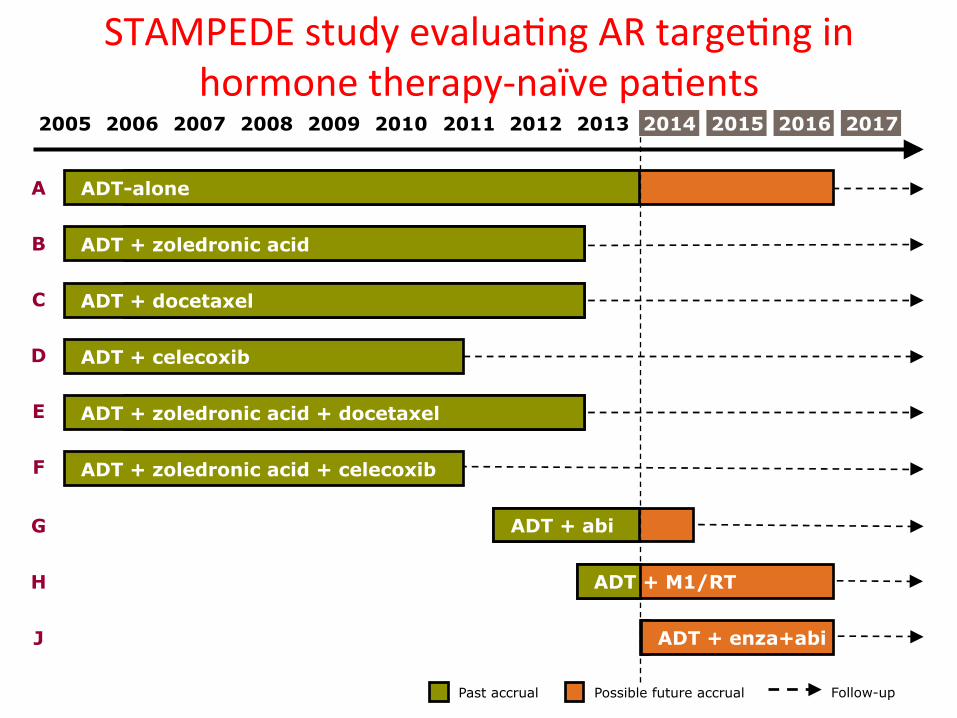
ADT + zoledronic acid + docetaxel
ADT + docetaxel
ADT-alone
ADT + zoledronic acid
ADT + celecoxib
ADT + zoledronic acid + celecoxib
STAMPEDE study evaluaAng AR targeAng in hormone therapy-‐naïve paAents
A
B
C
D
E
Past accrual Possible future accrual Follow-up
F
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
ADT + abi G
ADT + M1/RT H
ADT + enza+abi J
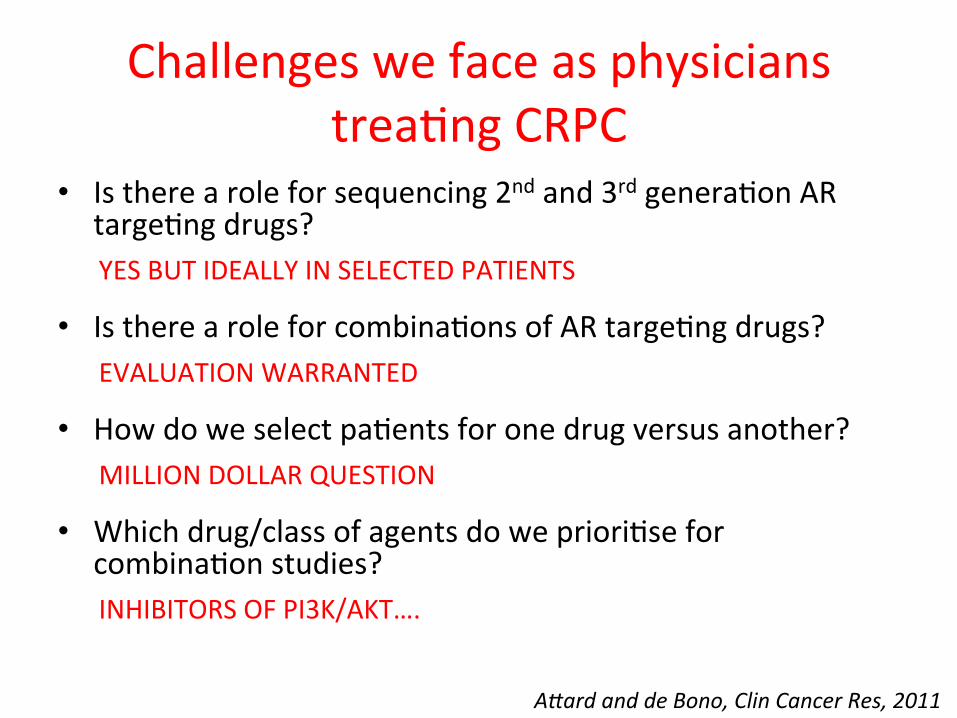
Challenges we face as physicians treaAng CRPC
• Is there a role for sequencing 2nd and 3rd generaAon AR targeAng drugs? YES BUT IDEALLY IN SELECTED PATIENTS
• Is there a role for combinaAons of AR targeAng drugs? EVALUATION WARRANTED
• How do we select paAents for one drug versus another? MILLION DOLLAR QUESTION
• Which drug/class of agents do we prioriAse for combinaAon studies? INHIBITORS OF PI3K/AKT….
A@ard and de Bono, Clin Cancer Res, 2011

Acknowledgements RMH/ICR Prostate Targeted Therapy Group Johann de Bono, Alison Reid, David Olmos Carmel Pezaro, Debbie Mukherjee, Dile6a Bianchini, Jo Hunt, Liz Sheridan Gal Maier, Bindu Baikady, Ajit Sarvadikar
The ICR Alan Ashworth, Paul Workman, Elaine Barrie
RMH Academic Urology Unit
David Dearnaley, Chris Parker
RMH Academic Biochemistry M Dowse6, L Folkerd
University of Birmingham Wiebke Arlt, Angela Taylor
The ICR Cancer Biomarkers Team Roberta Ferraldeschi, Penny Flohr, Suzanne Carreira, Juliet Richards, Ai Chiin Lim, Anna Wingate, Jane Goodall, Ruth Riisnaes, Susana Miranda, Ines Figuereido, Karolina Nowakowska, Mateus Crespo, Somi Hedayat
University of Michigan Rich Auchus
Epic Sciences
Dena Marrinucci and Ryan Di6amore
J&J/Cougar Biotechnology
Arturo Molina, Thian Kheoh
The paFents and their families