cases of poisoning - reported by physicians 2004
TRANSCRIPT

INF
OR
MA
TIO
N
2004
Cases of PoisoningReported by Physicians

Cases of Poisoning Reported by Physicians in 2004Published by: BfR Press and Public Relations OfficeEditors: Poison and Product Documentation Centre at the BfRNo of copies printed: 1000Typesetting and printing: Werbedruck Schreckhase, www.schreckhase.dePrinted on chlorine-free paper
ISBN 3-938163-08-9ISSN 1435-4047
Cases of Poisoning Reported by Physicians
Cases of Poisoning Reported by Physicians2004
Poison and Product Documentation Centre at the Federal Institute for Risk Assessment 11th Report (2004)
A. Hahn, H. Michalak, K. Begemann, K. Preußner, A. Engler

Cases of Poisoning Reported by Physicians
2

Table of Contents
1 Introduction 51.1 Legal basis and activities of the Centre 51.2 Processing of reports received 51.3 Product data bank (poison information data bank) 71.3.1 Figures 71.3.2 Collaboration between the BfR, industry and reporting Poison Control Centres 7
2 Case reports by physicians 92.1 Evaluation of reports 92.2 Reports on cases of poisoning in 2004 92.2.1 Origin 92.2.2 Spectrum of cases reported 92.2.3 Causes of poisoning 102.2.4 Age structure and sex distribution 112.2.5 Degree of severity of health impairment 112.2.6 Outcome of illnesses 122.3 The product information system, PRINS 132.3.1 Rapid communications 142.3.2 Summary reports 15
3 Selected toxicological problems 183.1 Risk of aspiration carried by petroleum distillates and paraffins 183.1.1 Reports in the ESPED study, state as of 31 December 2004 183.1.2 Measures to be taken 183.1.3 Overall evaluations of liquids involving aspiration risks 193.2 Health impairments caused by toner 203.3 Case reports 223.3.1 Cases of poisoning by paraffins 223.3.1.1 Liquid products for grill lighting 223.3.1.2 Garden torch 233.3.1.3 Oil lamp 233.3.2 Food supplements 253.3.2.1 Maca powder 253.3.2.2 Atractylosides 273.3.2.3 Ephedra alkaloids 293.3.3 Foods 303.3.3.1 Butterfish/Escolar 303.3.3.2 Shiitake mushroom 313.3.4 Welding fumes 333.3.5 Internal combustion engines 34
3

3.3.6 Sewage collector tank 353.3.7 Battery acid 383.3.8 Glow sticks 403.3.9 Multiple chemicals 413.3.10 Henna tattoos 433.3.11 Plants – Colchicum autumnale 443.3.12 Animals – Vipera berus 46
4 Annex 494.1 Overview of reported cases of poisoning in the period of
1 January–31 December 2004 494.2 Notification form 544.3 List of Poison Control Centres 554.4 Press releases on toxicological problems issued by the BfR in 2004 57
Cases of Poisoning Reported by Physicians
4

1 Introduction
1.1 Legal basis and activities of the CentreWith the Chemicals Act (ChemG), legislation inthe Federal Republic of Germany laid the foun-dation "to protect humans and the environmentfrom harmful effects of dangerous substancesand preparations, particularly to make them rec-ognizable, to avert and to prevent the develop-ment of such effects" (according to §1).
For a realistic assessment of risks for humanhealth, importance has been increasingly as-cribed to the knowledge of data on human toxi-cology that can be obtained from the evaluationof cases of poisoning in humans. This is whylegislation has introduced compulsory notifica-tion of poisonings by attending physicians from1 August 1990, by the first amendment to theChemG (§16e).
A physician who is consulted for treatment orevaluation of sequelae of diseases caused bychemical substances or products is obliged tosubmit essential data on poisonings to the Poi-son and Product Documentation Centre at theFederal Institute for Risk Assessment (BfR).
According to the Chemicals Act, illnesses orsuspected poisonings associated with the fol-lowing substances are notifiable:� Chemical substances and products used in
the household, e.g. detergents and cleansingagents, hobby and DIY articles;
� Cosmetics;� Pest control products;� Plant protection products;� Wood preservatives;� Chemicals used at the workplace;� Harmful chemical substances in the environ-
ment and� Plants/animals.
Within the meaning of the Chemicals Act, theterm of poisoning designates all cases in which
health impairment has occurred, as well as sus-pected cases of poisoning. Under the Act, alsothe Poison Information and Treatment Centres(Poison Control Centres, PCC) were subjectedto compulsory reporting of their knowledge (ofgeneral importance) gained in the context oftheir activities.
1.2 Processing of reports receivedReports received on health impairment associ-ated with chemicals are subjected to an assess-ment procedure resulting in the rating of a pos-sible causal relationship between the toxicantand the manifestations observed, as well as oth-er conclusions. Such relationship may be classi-fied as "possible", "probable", "confirmed","none" or "cannot be assessed". The rules ap-plied in the assessment of individual caseshave been described in detail in the previousannual reports.
Differentiated analyses and evaluation of thedata on cases form the basis for the estimationof toxic risks in humans. For these purposes,the data on cases in humans are continuouslydocumented as case data sets and case re-ports. Information on identified risks is passedon to ministries, manufacturers and industrialassociations in the form of rapid communica-tions or annual summarizing reports by meansof the product information system PRINS (seeChapter 2.3). At the same time, the responsiblemanufacturers or distributors are requested tosubmit information on the measures envisagedby them to improve product safety.
The BfR publishes annual reports on the knowl-edge gained from the cases of poisoning re-ported by physicians. These publications areavailable on request in writing at the Presses-telle of the Federal Institute for Risk Assess-ment, Thielallee 88-92, D-14195 Berlin, Ger-many. In part, they have also been published as
5

electronic documents on the internet(ww.bfr.bund.de).
A graphical representation of these tasks andprocedures is shown in Fig. 1.
Cases of Poisoning Reported by Physicians
6
Notificationsphysicians§ 16e para 2
Human data
InformationPoison Control Centres
§ 16e para 3
Casedata bank
Productdata bank
Assessment of individual case
AnalysisRisk identification
aimed at scientific
information
Statistical analysesCase reportsPress release
Rapid communications
to manufacturers/distributorsministeries
industrial association
Criteriumsevere
health impairments
Summarizing reports
annually to manufacturers/distributors
Criteriumnon-severe
health impairments
Measures for risk minimization
Risk communication
aimed atrisk management
Notificationsindustrie
§ 16e para 1Dangerous
products/biocides
Cosmetics Regulations § 5dCosmetics
Voluntary notifications
Fig. 1: Terms of reference of the Poison and Product Documentation Centre

1.3 Product data bank (poison informationdata bank)
1.3.1 FiguresAt he end of 2004, 185 487 documents on indi-vidual products had been recorded in the poi-son information data bank maintained by theBfR, which can be accessed by the Poison Con-trol Centres in Germany thus supporting theiractivities in providing consultation and treatmentin cases of poisoning. The structure of the databank and the different types of product datasets have been described in detail in previousreports. The number of reports on products re-ceived by the Centre for Recording of Poison-ings at the BfR increased by 23 458 documentsin 2004 (Fig. 2).
1.3.2 Collaboration between the BfR, indus-try and reporting Poison Control CentresMore than 90 % of product data on cosmeticsreceived by the BfR are submitted by manufac-turers and distributors in electronic form, whilethe major part of reports made on a voluntarybasis, reports on dangerous preparations andbiocidal products is still submitted on paperforms.
Until the end of the year, 1 699 product formula-tions were received by the BfR through the elec-tronic information procedure (EMIL) elaboratedin cooperation with the Poison Control Centresand the German Cosmetics, Toiletries, Per-fumes, and Detergents Association (Industrie-verband Körperpflege und Waschmittel e.V. –
7
Fig. 2: Notifications on products received since 1997 and transmission of information to the German Poison Control Centres
32,297
11,2200
20000
40000
60000
80000
100000
120000
140000
160000
180000
200000
1996 1997 1998 1999 2000 2001 2002 2003 2004
Notifications
185,487
141,970
Cosmetics
Products, voluntary
Products, legal (§16e)+biocides
Total

Cases of Poisoning Reported by Physicians
8
Fig. 3: Notifications under §16e para 1 of the Chemicals Act: legal products and biocidal products
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
1997 1998 1999 2000 2001 2002 2003 2004
Dangerous preparations6,316
Biocides4,904
Notifications
Pro
du
ct n
oti
fica
tio
ns
IKW), which is guided by the notification proce-dure for cosmetics. The data were transmittedby diskette and e-mail. The envisaged end pointof electronic data transmission is online datarecording and data transmission in the frame-work of a central poison information data bank.
Of the dangerous preparations and biocidalproducts notifiable under §16e para 1 of theChemicals Act, 11 220 data sets have been dis-tributed by transmission to the Poison ControlCentres so far (Fig. 3).
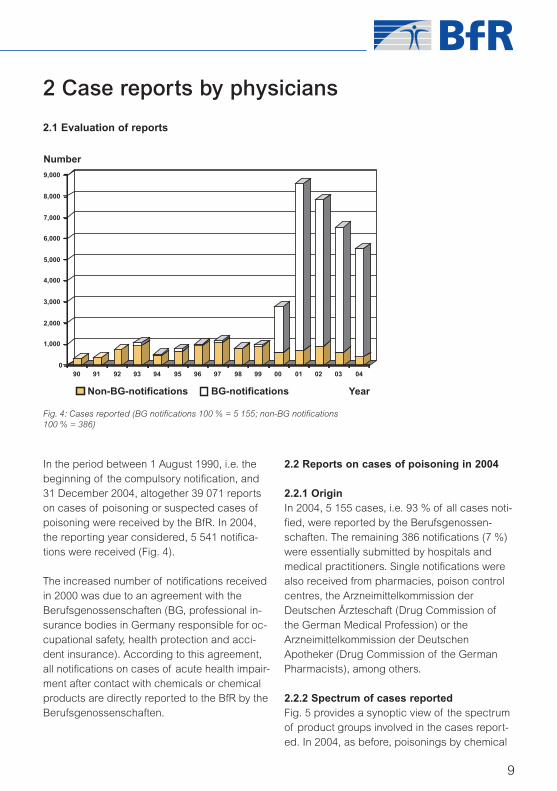
In the period between 1 August 1990, i.e. thebeginning of the compulsory notification, and31 December 2004, altogether 39 071 reportson cases of poisoning or suspected cases ofpoisoning were received by the BfR. In 2004,the reporting year considered, 5 541 notifica-tions were received (Fig. 4).
The increased number of notifications receivedin 2000 was due to an agreement with theBerufsgenossenschaften (BG, professional in-surance bodies in Germany responsible for oc-cupational safety, health protection and acci-dent insurance). According to this agreement,all notifications on cases of acute health impair-ment after contact with chemicals or chemicalproducts are directly reported to the BfR by theBerufsgenossenschaften.
2.1 Evaluation of reports
2.2 Reports on cases of poisoning in 2004
2.2.1 OriginIn 2004, 5 155 cases, i.e. 93 % of all cases noti-fied, were reported by the Berufsgenossen-schaften. The remaining 386 notifications (7 %)were essentially submitted by hospitals andmedical practitioners. Single notifications werealso received from pharmacies, poison controlcentres, the Arzneimittelkommission derDeutschen Ärzteschaft (Drug Commission ofthe German Medical Profession) or theArzneimittelkommission der DeutschenApotheker (Drug Commission of the GermanPharmacists), among others.
2.2.2 Spectrum of cases reportedFig. 5 provides a synoptic view of the spectrumof product groups involved in the cases report-ed. In 2004, as before, poisonings by chemical
9
2 Case reports by physicians
Fig. 4: Cases reported (BG notifications 100 % = 5 155; non-BG notifications 100 % = 386)
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
90 91 92 93 94 95 96 97 98 99 00 01 02 03 04
Non-BG-notifications BG-notifications Year
Number

products and primary substances have re-mained in top position among the total of casesreported by the Berufsgenossenschaften. Allother product groups play a minor role withshares of less than 2 % each.
As expected, the spectrum of substances andproducts involved in poisonings is somewhatdifferent in the reports received from hospitalsand those received from medical practitioners.Also among these, notifications related to chem-ical products ranked first in the reporting year.They are followed, at a clear distance, by theprimary substances that are likewise subject tocompulsory notification. Next in the ranking are
health complaints caused by foods, beveragesand medicinal products that were reported al-though these are not subject to compulsory no-tification.
For a detailed list of toxicants in tabular formsee Annex. In this table, the cases reported in2004 have been classified by product applica-tion groups (assignment of toxicants accordingto their intended use).
2.2.3 Causes of poisoningThe Berufsgenossenschaften almost exclusivelyreported cases of exposure to poisons in thecontext of occupational accidents (ca. 96 % of
Cases of Poisoning Reported by Physicians
10
0
10
20
30
40
50
60%
BG notifications Non-BG notifications
Chem. P
roduct
s
Primar
y su
bstan
ces
Foods an
d bev
erag
es
Med
icin
al p
roduct
s
Indust
rial a
ccid
ents
Other
s*
* Others: Cosmetics/personal hygiene products,pesticides, agrochemicals, plants, fungi, ani-mals, veterinary medicines, weapons, others
BG notifi cations(100 % = 5 155 notifi cations)
Non-BG notifi cations(100 % = 386 notifi cations)
Chemical products 55.7 % (2 872 cases) 40.7 % (157 cases)
Primary substances 37.6 % (1 936 cases) 12.7 % (49 cases)
Foods and beverages 0.7 % (36 cases) 13.2 % (51 cases)
Medicinal products 1.6 % (22 cases) 12.2 % (47 cases)
Industrial accidents 0.4 % (20 cases) 10.4 % (40 cases)Others 5.4 % (285 cases) 14.5 % (56 cases)
Table 1: Spectrum of notifications (repeat listing of cases possible)
Fig. 5: Spectrum of cases reported (BG notifications 100 % = 5 155;non-BG notifications 100 % = 386)

cases). The remaining 4 % of cases referred toaccidents that occurred during the common useof a product or the cause of the accident wasunknown.
Also among the reports submitted by hospitalsand medical practitioners, accidents were thepredominant cause of poisoning (58 %) fol-lowed by exposure during common use (25 %).Suicidal action was reported in no more than1.8 % of cases. In the remaining cases, thecause has been unknown.
On principle, acute poisoning takes a dominat-ing position among the reports (Table 2). This isdue to the fact that the agreement on the trans-mission of reports on cases of poisoning by theBerufsgenossenschaften expressly provides forthe submission of reports on acute cases ofpoisoning only.
2.2.4 Age structure and sex distributionIn 2004, the share of poisonings in adultsamong the total of cases reported was 96.8 %.
The cases submitted by the Berufsgenossen-schaften were exclusively those involving adults.The share of cases in adults predominated alsoamong the reports received from hospitals andmedical practitioners while the share of childreninvolved was 43 % (Table 3).
2.2.5 Degree of severity of health impairmentAlso in 2004, the majority of cases reported re-ferred to minor health impairment only, bothamong the cases reported by the Berufs-genossenschaften and among those reportedby hospitals and medical practitioners. Moder-ate and severe health impairment is more oftenreported by medical practitioners or physiciansworking in hospitals because they also receivereports on suicide attempts (Table 5).
11
Table 2: Duration of exposure
BG notifi cations(100 % = 5 155 notifi cations)
Non-BG notifi cations(100 % = 386 notifi cations)
Acute 99.9 % (5 149 cases) 83.2 % (321 cases)
Chronic 0.1 % (4 cases) 15.8 % (61 cases)Unknown 0 % (2 cases) 1 % (4 cases)
BG notifi cations(100 % = 5 155 notifi cations)
Non-BG notifi cations(100 % = 386 notifi cations)
Children 0 % (0 cases) 43.1 % (166 cases)
Adults 100 % (5 154 cases) 55.4 % (214 cases)Unknown 0 % (1 case) 1.5 % (6 cases)
BG notifi cations(100 % = 5 155 notifi cations)
Non-BG notifi cations(100 % = 386 notifi cations)
Male 62.3 % (3 211 cases) 44 % (170 cases)
Female 22.0 % (1 134 cases) 44.3 % (171 cases)Unknown 15.7 % (810 cases) 11.7 % (45 cases)
Table 3: Age groups
Table 4: Sex distribution
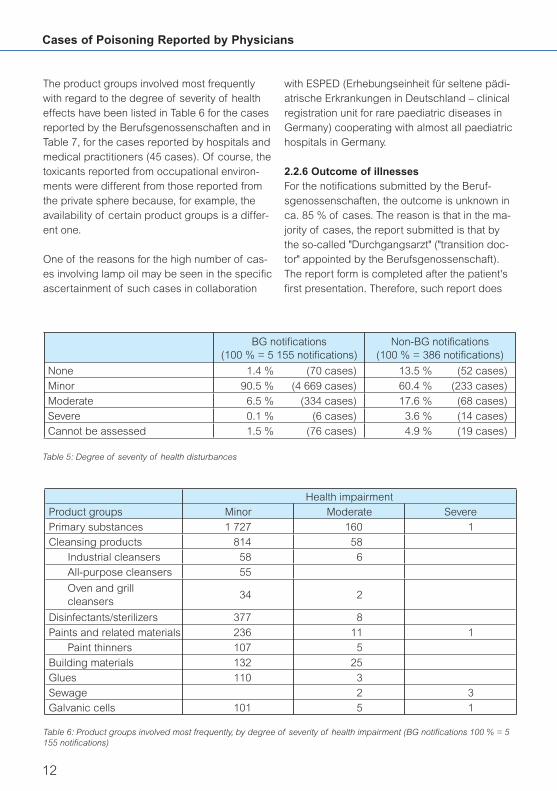
The product groups involved most frequentlywith regard to the degree of severity of healtheffects have been listed in Table 6 for the casesreported by the Berufsgenossenschaften and inTable 7, for the cases reported by hospitals andmedical practitioners (45 cases). Of course, thetoxicants reported from occupational environ-ments were different from those reported fromthe private sphere because, for example, theavailability of certain product groups is a differ-ent one.
One of the reasons for the high number of cas-es involving lamp oil may be seen in the specificascertainment of such cases in collaboration
with ESPED (Erhebungseinheit für seltene pädi-atrische Erkrankungen in Deutschland – clinicalregistration unit for rare paediatric diseases inGermany) cooperating with almost all paediatrichospitals in Germany.
2.2.6 Outcome of illnesses For the notifications submitted by the Beruf-sgenossenschaften, the outcome is unknown inca. 85 % of cases. The reason is that in the ma-jority of cases, the report submitted is that bythe so-called "Durchgangsarzt" ("transition doc-tor" appointed by the Berufsgenossenschaft).The report form is completed after the patient'sfirst presentation. Therefore, such report does
Cases of Poisoning Reported by Physicians
12
Health impairmentProduct groups Minor Moderate Severe
Primary substances 1 727 160 1
Cleansing products 814 58
Industrial cleansers 58 6
All-purpose cleansers 55
Oven and grill cleansers
34 2
Disinfectants/sterilizers 377 8
Paints and related materials 236 11 1
Paint thinners 107 5
Building materials 132 25
Glues 110 3
Sewage 2 3Galvanic cells 101 5 1
Table 6: Product groups involved most frequently, by degree of severity of health impairment (BG notifications 100 % = 5155 notifications)
Table 5: Degree of severity of health disturbances
BG notifi cations(100 % = 5 155 notifi cations)
Non-BG notifi cations(100 % = 386 notifi cations)
None 1.4 % (70 cases) 13.5 % (52 cases)
Minor 90.5 % (4 669 cases) 60.4 % (233 cases)
Moderate 6.5 % (334 cases) 17.6 % (68 cases)
Severe 0.1 % (6 cases) 3.6 % (14 cases)
Cannot be assessed 1.5 % (76 cases) 4.9 % (19 cases)

not contain any information on the course of thepatient’s illness. In selected cases, enquirieswere made to obtain information on the courseof the disease. In the majority of cases onwhich information was available, patients hadrecovered completely.
Of the notifications submitted by hospitals andmedical practitioners, patients recovered com-pletely in 254 cases (67 %). In 118 cases (31 %), the outcome was unknown; in nine cas-es (2 %), late damage could not be excluded orpartial recovery was reported.
Altogether seven deaths were reported in 2004,two of these by the Berufsgenossenschaftenand five, by hospitals and medical practitioners.
The fatal two cases reported from workplaceswere poisonings by gases such as hydrogensulfide from an industrial sewage collection tank(cf. Chapter 3.3.6).
In the preceding year, regrettably also twodeaths were reported that referred to childrenwho had accidentally ingested paraffin-contain-ing colourless lamp oil (cf. Chapter 3.3.1).
In addition, two deaths were reported that hadbeen due to consumption of leaves of
colchicum being mistaken for those of bear'sgarlic (cf. Chapter 3.3.11) and one suicide in-volving the pesticide, parathion.
2.3 The product information system, PRINSThe notifications by physicians in cases of poi-soning legally required under the Chemicals Act(§16e para 2) are regularly evaluated to protectconsumers from health risks posed by chemi-cals and chemical products. Since 1994, the re-porting physicians, the responsible ministriesand the scientific community have been in-formed by annual reports on analyses of thesenotifications and the corresponding results. Inthe context of these notifications, the term, poi-soning is used to designate any health impair-ment associated with chemicals, including forexample also allergies.
Since 1998, manufacturers and distributors ofchemical products such as household chemi-cals, hobby articles, cosmetics, plant protectionand pest control products and correspondingproducts for commercial use have been in-formed about reports received by the BfR oncases of health impairment associated withtheir products.
13
Table 7: Product groups involved most frequently, by degree of severity of health impairment (Non-BG notifications 100 %= 386 notifications)
Health impairmentProduct groups Minor Moderate Severe
Industrial accidents 40
Foods and beverages 34 8 4
Food supplements 25 4 3
Lamp oil 24 24 3
Primary substances 31 15 2
Cleansing products 14 2
Cosmetic creams/ lotion 10 1Fire lighting products 1 5 2

2.3.1 Rapid communicationsIf reports on severe health risks (except thoserelated to suicide attempts) are received by theBfR, it will provide for immediate information ofthe manufacturer/distributor of the chemicalproduct involved as well as the competent in-dustrial association/federal trade associationand the responsible ministries, the Federal Min-istry of Consumer Protection, Food and Agricul-ture, the Federal Ministry for the Environment,Nature Conservation and Nuclear Safety, andthe Federal Ministry of Health and Social Secu-rity as well as the Federal Office for ConsumerProtection and Food Safety.
Between 1 January 1998 and 31 December2004, altogether 21 rapid communications wereprepared and communicated. A synoptic viewof these is given in Table 8. For explanationswith regard to individual cases until 2003, refer-ence is made to the 2002 and 2003 Annual Re-ports. In the reporting year of 2004, two rapidcommunications were distributed. The casesconcerned were two fatal ones in children asso-ciated with the ingestion of colourless paraffinsfrom a garden torch and an oil lamp. The casereports are described in detail in Chapters3.3.1.2. and 3.3.1.3.
Cases of Poisoning Reported by Physicians
14
Year Product Toxicologically relevant substance
Person exposed
Outcome Proposal by BfR (P) and results (R)
1998 Impregnating agent
Fluorinated hydrocarbons
Adult Death P: Warnings for asthmaticsR: Accepted
1998 Disinfectant Quaternary ammonium compounds (surfactants)
Elderly adult Death P: Information, labelling „corrosive“R: Accepted
1999 Toilet drain cleanser
Sodium hydroxide Adult Caustic burns None
1999 Solvent Petrol Adult Pulmonary oedema
None
1999 Depilatory cream Thioglycolic acid Adult Scars None
1999 Disinfectant Quaternary ammonium compounds (surfactants)
Elderly adult Death P: Information, labelling
1999 Industrial cleanser
Sodium hydroxide Young child Caustic burns P: Information
1999 Medicinal product Dimenhydrinate Infant Death P: Warnings
2000 Cream bath product
Surfactants Elderly adult Death P: Information
2000 Lamp oil Paraffi ns Young child Severe pneumonia
P: Partial banR: Accepted, paraffi n substitute
2001 Disinfectant Alkylamine (surfactant)
Elderly adult Death P: Information

2.3.2 Summary reportsNotifications referring to non-severe health im-pairment caused by chemical products in occu-pational or private environments are transmittedto the manufacturers/distributors in the firstquarter of each new year in a summarized form.As requested by manufacturers, alsosuicides/suicide attempts have been included inthe summary notifications since 2003 irrespec-tive of the degree of severity of poisoning.Thus, manufacturers and distributors gainknowledge on possible risks involved in the han-dling of their products, which enables them toexercise responsible care with regard to theirproducts. If they find the information provided tobe insufficient, additional information can beobtained from the BfR. Much use has beenmade of this opportunity. The information pro-
vided for the manufacturer is a contribution toincrease product safety and thus, to improveconsumer protection. There has been great in-terest in such information. For example, acci-dent analyses have revealed that eye injuriescaused by chemical products have frequentlyoccurred in spite of wearing safety goggles.The safety data sheet should therefore point out"closely fitting safety goggles".
Summary reports for the year 2004 referred to303 products and were formally transmitted to148 manufacturers. The table below (Table 9)provides a synoptic view of product applicationgroups (minimum three listings) of the 2004summary reports. Strikingly high numbers havebeen recorded for cleansing products (90) anddisinfectants (61).
15
Table 8: Rapid communications 1 January 1998 – 31 December 2004
Year Product Toxicologically relevant substance
Person exposed
Outcome Proposal by BfR (P) and results (R)
2001 Tea (biodrug) Atropa belladonna Adolescent Respiratory insuffi ciency
P: Information
2002 Lavatory cleaner Surfactant Elderly adult Caustic burns P: Information
2002 Mild detergent Surfactant Elderly adult Death P: Information
2003 Cleansing product
Surfactant Elderly adult Respiratory insuffi ciency
P: Information
2003 Food supplement Proteins Adult Severe allergy P: Information
2003 Fumigant Sulfuryl difl uoride Adult Death P: Information
2003 Drain cleanser Potassium hydroxide solution
Child Severe caustic burns
P: Information
2003 Disinfectant Peracetic acid Adult Respiratory insuffi ciency
P: Information
2004 Garden torch Paraffi ns, colourless
Infant Respiratory insuffi ciency, death
P: Information, additional EU ban on colourless / unscented paraffi nsR: Accepted
2004
Oil lamp Paraffi ns, colourless
Infant Respiratory insuffi ciency, death
P: Information, additional EU ban on colourless/unscented paraffi nsR: Accepted

Cases of Poisoning Reported by Physicians
16
First level Second level Third levelAgrochemicals 7
Chemical products 254 Building materials, auxiliary products
4
Building materials 6
Fuels, liquid 14 Lamp oil 14
Offi ce materials, chemical
13
Disinfectants/sterilizers 61
Glass-working, auxiliary products
3
Glues 3
Metallurgy, auxiliary products
3
Cleansing products 90 Descaling products 3
Dishwasher detergents
4
Dishwasher cleansers 3
Industrial cleansers 9
Milking machine cleansers
11
Lavatory cleansers 13
Detergents, auxiliary products
4
Water treatment products
3
Cosmetics/personal hygiene products
18 Skin care products 15 Creams 10
Pesticides 24 Fungicides 4
Herbicides 7Insecticides 9
Table 9: Product groups in 2004 summary reports
Table 10 shows the number of moderate healthdisturbances associated with the productgroups in 2004. The remaining product groupswere involved in minor health impairment.The BfR also performs cumulative data analyses
of case reports. If trends become apparent, themanufacturers of the products confirmed are in-formed. In turn, manufacturers are requested bythe BfR to communicate comparable data andtrends that may serve to improve product safety.

17
First level Second level Third levelAgrochemicals 1
Chemical products 36 Paints and related materials
1
Building materials 1
Fuels, liquid 7 Lamp oil 7
Offi ce materials, chemical
4
Disinfectants/sterilizers 3
Galvanizing agents, auxiliary products
2
Glass-working, auxiliary products
1
Coolants 1
Metallurgy, auxiliary products
2
Cleaning products 10 Floor polishes 1
Industrial cleaners 1
Milking machine cleaners
2
Furniture polishers 1
Cosmetics/personal hygiene products
2 Hair care products 1 Dyes/colorants 1
Skin care products 1 Creams 1Pesticides 2 Insecticides 2 Phosphoric esters 1
Table 10: Product groups associated with moderate health disturbances of summary reports in 2004

3.1 Risk of aspiration carried by petroleumdistillates and paraffinsAs repeatedly reported earlier, liquid fuels con-taining paraffins and petroleum distillates thatare used in ornamental oil lamps, garden torch-es, for grill lighting and fire-breathing, carry ahigh potential risk. Very low quantities, often on-ly a little sip, may result in severe chemicalpneumonia. In Germany, already five deaths ininfants and young children have been recordedsince 1990. In the reporting year of 2004, twoinfants died of the consequences of aspirationof colourless paraffin-containing lamp oils (seealso case reports).
In addition to the regular documentation of cas-es under §16e of the Chemicals Act , the BfRhas recorded cases of poisoning involving lampoils in collaboration with the clinical registrationunit for rare paediatric diseases in Germany(ESPED) and almost all German paediatric hos-pitals since 1 March 2000. A detailed report onthe first part of the study (ESPED I: 1 March2000–28 February 2003) was published in theannual report "Cases of Poisoning Reported byPhysicians in 2003". Since lamp oil substitutes(rape seed methyl ester, high-viscosity mineraloils and paraffins) are being placed on the mar-ket, the study will be continued until 31 Decem-ber 2006.
The ESPED study "Lamp oil poisoning in Ger-many" has proved to be a reliable instrument ofpostmarketing control. It has reliably describedthe introduction of substitute substances andthe residual risks posed by lamp oils for infantsand young children. The figures documented sofar demonstrate that the frequency of lamp oilaccidents requiring inpatient treatment has con-tinued to be on a decrease in Germany. The banon coloured and scented lamp oils containingparaffins or kerosene that was introduced inGermany on 1 January 1999, the placing on the
market of substitutes and the warning to con-sumers issued by the most different institutionsand the media appears to have taken effect. Acomparable trend has also been recorded bythe German Poison Control Centres. In 2004, asalready in the reporting period of 2003, no sin-gle case of health impairment due to the newsubstitutes was documented, neither at the BfRnor at the German Poison Control Centres.
3.1.1 Reports in the ESPED study, state as of31 December 2004Between 1 March 2000 and 31 December 2004,the BfR received 616 case reports from ESPEDwith a total number of 458 questionnaires beingreturned (67 %). 411 of these cases could bevalidated as lamp oil ingestion with a 40 % rateof pneumonia (in 165 infants and young chil-dren). In the majority of cases (61 %), pneumo-nia was caused by lamp oils containing paraf-fins or petroleum distillates that were either oldproducts (i.e. coloured or scented productssold before the ban) or uncoloured and un-scented products not subject to the ban sofar. Observations made by different partieshave indicated that the uncoloured and un-scented products containing paraffins/petrole-um distillates that are not subject to the ban aremore aggressively advertised and sold with in-creasing market shares by wholesalers and re-tailers. A possible reason is that these productsare a good fuel for garden torches and for light-ing of charcoal (products for grill lighting).
3.1.2 Measures to be takenAlarmed by the two tragic deaths in 2004 thatwere caused by products containing paraffinsand petroleum distillates (lamp oil in one caseand liquid fuel for garden torches in the other),the Federal Institute for Risk Assessment andthe Ministry for the Environment, Nature Conser-vation and Nuclear Safety have again (as al-ready in 1993/1996) demanded a ban on all
Cases of Poisoning Reported by Physicians
18
3 Selected toxicological problems

products of such type on the EU level. At pres-ent, a risk survey is performed by the EU in allits member states in order to achieve an appro-priate decision. Until such a decision isachieved, it is of utmost importance to keenlyprotect children and to draw attention to substi-tute fuels (e.g. on a rape oil basis). In October2002, an EU standard for the design of child-proof oil lamps took effect (EN 14059: Decora-tive oil lamps – Safety requirements and testmethods), which, however, has not yet been tak-en up by the German industry in spite of per-sisting accidents. Also the results of the ESPEDstudy have suggested that the passive protec-tion of children can be improved essentially, giv-en the fact that children have very frequently in-gested the toxicant from non-childproof oillamps. When grilling is performed in the pres-ence of children, paraffin-/kerosene-containingliquid products for grill lighting should not beused. The BfR has pointed out this special riskin press releases.
3.1.3 Overall evaluations of liquids involvingaspiration risksEvaluations of all notifications received by theBfR of cases associated with liquids involvingaspiration risks such as lamp oils, liquid prod-ucts for grill lighting and fire eating/breathing aswell as case reports of the ESPED study haveshown a decreasing tendency. In these evalua-tions, the essential share in the figures is repre-sented by the ESPED study data (ca. 85 %).The total number of cases recorded at the BfRhas distinctly decreased, while the share ofcases of aspiration pneumonia has shown aslight decrease. This tendency becomes evi-dent even if these figures refer to those casesonly where knowledge of the formulation of theproduct involved has suggested the ingestion ofparaffin-containing liquids (Fig. 6). Thus, the re-sults of the ESPED study and notifications un-der §16e have demonstrated the fact of a de-creasing total number of ingestion of liquids in-volving aspiration risks in Germany.
19
Fig. 6: Frequency of notifications under §16e Chemicals Act of cases involving paraffin-containing products from 1 Janu-ary 2000 – 31 December 2004 (linear trend, the figure for 2000 with regard to ESPED cases was obtained by linear ex-trapolation since the study started on 1 March 2000)
76
5763
38 3936
16 20
26
23
0
10
20
30
40
50
60
70
80
90
100
2000 2001 2002 2003 2004
All notifications (paraffin-containing products) of these pneumonia Year
Cases

The severe health impairments caused bycolourless lamp oils and liquid products for grilllighting and fire eating/breathing have shownthat the protection of the population, particularlyof infants and young children, has to be furtherimproved. Appropriate measures on an EU levelare expected to be initiated in 2005.
3.2 Health impairments caused by tonerSingle reports on health impairments caused bytoners were received from the field of occupa-tional medicine. They primarily referred to healthcomplaints involving the mucosal membranessuch as rhinitis, eye and throat irritation andasthma-like cough. One of these cases was de-scribed in the annual report "Cases of Poison-ing Reported by Physicians in 2002" by the Fed-eral Institute for Risk Assessment and informa-tion provided for physicians on the manifesta-tions and relationships observed.
Until the end of 2004, physicians and Berufs-genossenschaften reported to the BfR 48 casesinvolving toners (reporting year 2000: 1 case;2001: 5 cases; 2002: 11 cases; 2003: 5 cases;2004: 26 cases). 15 cases were reported byphysicians working in hospitals, nine by medicalpractitioners and two, by Poison Control Centres(three by others). 19 reports were received fromBerufsgenossenschaften. The persons involvedwere exclusively adults (24 females, 21 males,three cases unknown). Most of the exposures(46) occurred at the workplace, only two ofthem in the private sphere. In most cases, theexposure was chronic (26), but also acute cas-es occurred (20, in two cases unknown). Theroute of exposure occurring most frequentlywas inhalation (42), but also exposure throughthe skin (10) and the eyes (2) and one case ofingestion were reported (repeated listing possi-ble). The health impairments experienced bythe persons affected were predominantly classi-fied as "minor" (28). "Moderate" health impair-ments were observed in 15 cases, no impair-ment in three cases. In two cases, the health im-pairment could not be assessed on the basis of
the data available. The health impairments ob-served referred mainly to the respiratory tractincluding cough (20), rhinitis (16), bronchitis(13), but also dyspnoea (12) and bronchial asth-ma (9). Also eye irritation, headache and aller-gies (9) were reported.
The Interessengemeinschaft der Ton-ergeschädigten (ITG, a self-help group of per-sons affected by health damage due to toners)has stated the number of persons affected tobe at least 700. This was reported on a hearingof the ITG performed at the BfR on 1 September2004. Printing and copying processes are com-plex physical and chemical processes associat-ed with the liberation and emission into the in-door air of volatile organic compounds of differ-ent chemical groups, microparticles from tonersand papers and gases. As a result, users oflaser printers and copying machines are ex-posed to a higher or lower degree to a numberof substances, among these also substancesinvolving health hazards. For the evaluation ofpossible health damage caused by toners, theBfR has been collaborating with other federal in-stitutions, such as the Federal Institute for Occu-pational Safety and Health (BAuA/FIOSH), theFederal Institute for Materials Research andTesting (BAM) and the Federal EnvironmentalAgency (UBA) all of which have already dealtwith the problem in the context of scientifictasks and studies. A BfR pilot study on healthrisks posed by toners is envisaged.
The case report below demonstrates how diffi-cult an evaluation of symptoms associated withexposure to toner dusts may be.
Case reportHealth impairment after contact with tonerin a patient suffering from atopic diathesisA 42-year-old female patient had been suffer-ing from cough and sudden dyspnoea since1985. Having moved into a newly furnishedoffice in 1989, she began to suffer increas-
Cases of Poisoning Reported by Physicians
20

ingly from breathing difficulty at her work-place. The patient attributed her complaints tothe impact of dust emitted by copying ma-chines and printers. She was examined andher medical condition assessed, with a tenta-tive diagnosis of obstructive disease of therespiratory tract. There was no sufficient evi-dence to incriminate the patient's occupationas the cause of her breathing difficulties.
Manifestations/courseThe case history revealed certain indicationsof frequent respiratory tract complaints at theworkplace.
When packaging deep-frozen products in thespring of 1985, the patient experienced forthe first time cough and an oppressive feelingwhen breathing. These manifestations abatedin her private home. This was followed bymanifestations such as a runny nose, sneez-ing and irritation of the conjunctivae of theeyes. Later, she also developed manifesta-tions on her hands, particularly after exposureto dust emitted during reconstruction work inher office. Reportedly, she developed 'influen-za-like' complaints particularly when workingat copying machines or laser printers. Duringweekends and holidays, her condition im-proved clearly. Asthma-like complaints requir-ing increased administration of medicinesand allergic rhinoconjunctivitis were stated.However, examinations performed to deter-mine exposure at the workplace did not re-veal any clear evidence of an occupationalcause of the patient's bronchial asthma. Vari-ous occupational provocation tests were car-ried out on the basis of the patient's assump-tions about substances that might have trig-gered the complaints. After working at acopying machine, inhalation of dust broughtalong from her workplace as well as afterstaying in an archive of medical files, the pa-tient developed breathing difficulties compa-
rable to those experienced at her workplace.However, measuring techniques were unableto unequivocally detect any reaction of therespiratory tract in these provocation tests. Itwas assumed that the patient's complaintsmight have to be attributed to a sick buildingsyndrome. It was stated that no risk of atrend-setting deterioration of the disease wasseen as that could be associated with a con-tinuation of her previous occupation. The lastexpert opinion of 1996 concluded that thepatient was suffering from a rhinopathy due tohouse dust mites which had been partlycaused by exposure to such mites. In thiscontext, the exposure to house dust mites inthe patient's home was considered as less in-tensive than that at the workplace becausethe patient had taken measures to control theinfestation by house dust mites in her privatehome. However, no sufficient evidence wasfound that would have permitted to attributethe bronchial disease of the patient to anti-genic influences at the workplace or to the in-criminated action of dusts emitted by copyingmachines and printers. Great importance wasattributed to the patient's high cigarette con-sumption as a cause of the persistence ofher chronic bronchial asthma. Furthermore, asensitisation to cat epithelium was found toplay an additional role in the unspecific in-crease of responsiveness of the bronchialsystem.
NotesIn the case described, a subjective health im-pairment was experienced at the workplace bythe patient who had been suffering from an un-derlying allergic disease. Nevertheless, no evi-dence of a workplace-associated cause lead-ing to occupational disease was found by exam-inations performed with regard to dust exposureat the workplace.
21

3.3 Case reports
3.3.1 Cases of poisoning by paraffins
3.3.1.1 Liquid products for grill lighting
Respiratory insufficiency in a young childafter ingestion of a liquid product for grilllighting A two-year old boy drank and aspirated anunknown quantity of a liquid product for grilllighting. As a consequence, artificial respira-tion had to be performed. In the furthercourse, the patient developed subglotticgranulomas, in addition to pneumonia. Hewas referred to inpatient treatment, whichlasted for almost three weeks and resulted incomplete recovery.
Manifestations/courseAfter ingestion, the child showed signs of res-piratory insufficiency. Since primary oxygensupply was insufficient as a therapy, the boyhad to be intubated and respirated.On admission to hospital, the little patient wasanalgosedated and kept under mechanicalventilation applied equally on both sides ofthe chest. Auscultation revealed crepitationover the lung fields. Other organ findingswere normal. Pneumonia, which could alsobe verified radiologically, receded slowly sothat respiration could be withdrawn from day4 and extubation performed on day 6. In thefurther course, a marked inspiratory stridorwas found to be present. Bronchoscopy wastherefore performed on day 10, which re-vealed subglottic granulomas. The patient re-mained under intubation and artificial respira-tion. Three days later, bronchoscopy was re-peated under laser conditions at an ENT hos-pital. Except for a moderate mucosal swelling,other manifestations were not found to per-sist. After cortisone administration andsuprarenin inhalation, extubation could beperformed three hours later. Stridor was no
longer found to be present. A secondary in-fection with Haemophilus influenzae detectedin the tracheal secretion was treated with an-tibiotics. After 18 days, the patient had com-pletely recovered and was discharged.
NotesThe detailed composition of the liquid involvedwas not available. In most cases, the only rele-vant components contained in liquid productsfor grill lighting are hydrocarbons such aspetrol, paraffin oil, isoparaffins, kerosene and,less often, also isopropanol. Investigations intoeleven product formulations performed at theFederal Institute for Risk Assessment (BfR) re-vealed as ingredients: lamp oils in six, kerosenein three and petrol in two products. The twoproducts containing petrol, however, had beenavailable on the market only until 2001.
Ingestion of petrol or kerosene is mostly fol-lowed by the typical foetor ex ore since thesesubstances are largely excreted through therespiratory tract. In the case described above,such typical smell was not described, however,the authors of the report may just have failed todo so. The hydrocarbons concerned have chainlengths between C9 and C15 and involve a highrisk of aspiration because of their physico-chemical properties such as low viscosity, lowsurface tension and low vapour pressure. Theyreadily pass the epiglottis by creeping and thusmay cause severe chemical pneumonitis. Aspi-ration of amounts as low as < 1 mL may inducepneumonia in humans. The cardinal sign is aninitial and often persistent cough. In addition,vomiting may occur. This may be followed bydyspnoea and/or tachypnoea, cyanosis andless frequently, by somnolence. In cases of pul-monary manifestations, pneumonitis may devel-op in ca. 25-50 % of cases. However, also in theevent of an initial absence of manifestations,pneumonitis may develop in 10-20 % of cases.Death due to progressive pulmonary oedema is
Cases of Poisoning Reported by Physicians
22

also possible. Less often, pneumatoceles havebeen observed. In cases of ingestion of>1mL/kg b.w. or suspected aspiration it is al-ways recommended to seek medical advice in ahospital. In all patients suffering from initial man-ifestations, clinical and/or radiological examina-tions are required to exclude pneumonia. X-rayexamination should be performed two hours af-ter ingestion but not earlier. Clinically asympto-matic patients with pathological X-ray findingsshould undergo clinical observation for 6-12hours. The aspiration problem associated withlamp oils for use in ornamental lamps, liquid fu-els used by fire breathers and also liquids forgrill lighting has already been comprehensivelydealt with by the Federal Health Office (BGA),the Federal Institute for Health Protection ofConsumers and Veterinary Medicine (BgVV)and their successor institution, the Federal Insti-tute for Risk Assessment (BfR).
Evaluation of the case described:In the case described above, a causal relation-ship between the ingestion and the manifesta-tions observed has been rated as probable onthe basis of the information given on the tempo-ral relationship and in the absence of othercauses, for the severe health impairment suf-fered by the patient.
3.3.1.2 Garden torch
3.3.1.3 Oil lamp
Severe health impairment with lethal out-come in two infants after ingestion ofcolourless and unscented lamp oils con-taining paraffin In the context of notifications of cases of poi-soning under § 16e para 2 of the GermanChemicals Act, two severe cases of healthimpairment with a lethal outcome were report-ed to the Federal Institute for Risk Assess-ment (BfR). The notifications referred to a girlaged 13 months (date of accident 16 May
2004) and a boy aged one year and eightmonths. In both cases, the substances in-volved were colourless and odourless lampoils on a paraffin basis. Both children diedfrom the sequelae of lamp oil aspiration, inspite of intensive medical treatment.
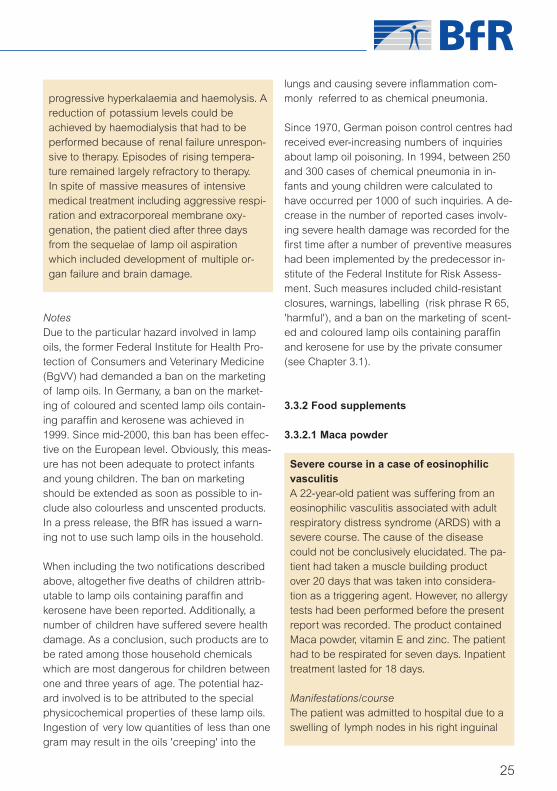
Case No 1: Garden torchWhen playing in the garden, a girl aged 13months drank an unidentified quantity of clearand odourless lamp oil contained in a gardentorch. The manufacturer of the product hasremained unknown so far. According to analy-
23
Fig. 7: Garden torch
ses performed, the product involved consist-ed of paraffins (long-chain alkanes, fractionsC9 - C14) and was labelled with R 65 under theGerman Regulations on Dangerous Sub-stances and Materials (Gefahrstoffverord-nung – GefStoffV).
Manifestations/courseThe child was reported to have coughed,retched and vomited several times immedi-ately after ingestion. After an emergencyphysician had referred her to a hospital which

took place without delay, the little patient'scondition deteriorated dramatically, as seenby signs of respiratory insufficiency, increaseof heart rate and cyanosis. She was artificial-ly respirated and transferred to the paediatricintensive care unit of a large hospital. On ar-rival, a decompensated respiratory acidosiswith a pH of 7.2 was already found to bepresent. Chest X-ray revealed extended ac-cumulation of fluid in both lungs, with pleuraleffusion right in the sense of an extendedchemical pneumonia. In the further course,the clinical picture showed a pronouncedacute respiratory distress syndrome (ARDS)which developed shortly afterwards. In spiteof massive measures of intensive medicalcare, no oxygen saturation could be achievedeven at the highest ventilation pressure avail-able. After a sudden decrease of the heartrate followed by cardiac arrest, cardiac mas-sage, intratracheal administration of threedoses of adrenaline and defibrillation re-mained unsuccessful. The child died after ca.twelve hours from the sequelae of lamp oilaspiration, having developed a severe pneu-monia and destruction of lung tissue, whichwere confirmed histologically.
Evaluation of the case described:Based on the information received on thetemporal relationship between ingestion andmanifestations, a causal relationship is proba-ble.
Case No 2: Oil lampA boy aged 20 months drank an unknownamount of a colourless and unscented paraf-fin-containing oil from a lamp (a heavy glassbottle equipped with a metal ring that report-edly had held a wick). However, it has alsobeen considered as possible that the boy hadonly sucked from the wick because the latterwas found beside the bottle. The lamp hadbeen placed on the terrace. The manufactur-
er of the product was known. Also in thiscase, the substance involved consisted ofparaffins both according to the product labelsubmitted and the analyses performed.
Cases of Poisoning Reported by Physicians
24
Fig. 8: Oil lamp
Manifestations/courseThe child was reported to have coughed im-mediately and vomited later on. After admis-sion to the nearest hospital, the boy was intu-bated and respirated while developing an in-creasing clouding of consciousness. Due tocardiac arrest, cardiopulmonary resuscitation(by mechanical measures and medication)over a short period became necessary andas a result, temporary haemodynamic stabi-lization was achieved. When respiratory insuf-ficiency continued to deteriorate, the boy wastransferred by helicopter to a university hospi-tal. In spite of aggressive respiration and re-peated catecholamine administration, a respi-ratory and haemodynamic stabilization couldnot be achieved again when the patient de-veloped right ventricular failure. A thoracicECCPAD implantation was performed (extra-corporeal membrane oxygenation). In the fur-ther course, the patient became anuretic. Un-der conditions of a considerable generalizedmetabolic disturbance, the patient developed
progressive hyperkalaemia and haemolysis. Areduction of potassium levels could beachieved by haemodialysis that had to beperformed because of renal failure unrespon-sive to therapy. Episodes of rising tempera-ture remained largely refractory to therapy.In spite of massive measures of intensivemedical treatment including aggressive respi-ration and extracorporeal membrane oxy-genation, the patient died after three daysfrom the sequelae of lamp oil aspirationwhich included development of multiple or-gan failure and brain damage.
NotesDue to the particular hazard involved in lampoils, the former Federal Institute for Health Pro-tection of Consumers and Veterinary Medicine(BgVV) had demanded a ban on the marketingof lamp oils. In Germany, a ban on the market-ing of coloured and scented lamp oils contain-ing paraffin and kerosene was achieved in1999. Since mid-2000, this ban has been effec-tive on the European level. Obviously, this meas-ure has not been adequate to protect infantsand young children. The ban on marketingshould be extended as soon as possible to in-clude also colourless and unscented products.In a press release, the BfR has issued a warn-ing not to use such lamp oils in the household.
When including the two notifications describedabove, altogether five deaths of children attrib-utable to lamp oils containing paraffin andkerosene have been reported. Additionally, anumber of children have suffered severe healthdamage. As a conclusion, such products are tobe rated among those household chemicalswhich are most dangerous for children betweenone and three years of age. The potential haz-ard involved is to be attributed to the specialphysicochemical properties of these lamp oils.Ingestion of very low quantities of less than onegram may result in the oils 'creeping' into the
lungs and causing severe inflammation com-monly referred to as chemical pneumonia.
Since 1970, German poison control centres hadreceived ever-increasing numbers of inquiriesabout lamp oil poisoning. In 1994, between 250and 300 cases of chemical pneumonia in in-fants and young children were calculated tohave occurred per 1000 of such inquiries. A de-crease in the number of reported cases involv-ing severe health damage was recorded for thefirst time after a number of preventive measureshad been implemented by the predecessor in-stitute of the Federal Institute for Risk Assess-ment. Such measures included child-resistantclosures, warnings, labelling (risk phrase R 65,'harmful'), and a ban on the marketing of scent-ed and coloured lamp oils containing paraffinand kerosene for use by the private consumer(see Chapter 3.1).
3.3.2 Food supplements
3.3.2.1 Maca powder
Severe course in a case of eosinophilicvasculitisA 22-year-old patient was suffering from aneosinophilic vasculitis associated with adultrespiratory distress syndrome (ARDS) with asevere course. The cause of the diseasecould not be conclusively elucidated. The pa-tient had taken a muscle building productover 20 days that was taken into considera-tion as a triggering agent. However, no allergytests had been performed before the presentreport was recorded. The product containedMaca powder, vitamin E and zinc. The patienthad to be respirated for seven days. Inpatienttreatment lasted for 18 days.
Manifestations/courseThe patient was admitted to hospital due to aswelling of lymph nodes in his right inguinal
25

region lasting for ten days. In addition, hecomplained of exhaustion, night sweat andcough. In order to exclude a malignant under-lying disease, a lymph node puncture wasperformed under spinal anaesthesia. Duringthis procedure, the patient already developedconsiderable dyspnoea associated with re-duced gas exchange and a peripheral oxy-gen saturation of 84 % when breathing indoorair. At first, therapeutic attempts includednon-invasive artificial respiration. Due to a fur-ther deterioration of the patient's condition,he was transferred to the intensive care uniton the following day. There, the striking signsof tachypnoea with respiratory rates of up to30/min and a peripheral oxygen saturation of88 % were recorded under conditions of oxy-gen supply by nasal tube. Because of a fur-ther deterioration (peripheral saturation 75%), the patient was intubated and respirated.Still, the gas exchange was found to be ex-tremely reduced. Bronchoscopy was per-formed without delay and revealed only lowamounts of a yellow-brownish secretion with-out any obstruction of the airways. The mu-cosa was found to be normal except for red-dening and petechial haemorrhages. Theclinical picture found was that of a severeARDS associated with pronounced confluentshadowing over both lungs revealed by X-rayand shadows from pleural effusions revealedby computer tomography. Based on a tenta-tive diagnosis of an infectious-septic process,a broad-spectrum antibiotic therapy was initi-ated. Nevertheless, laboratory analysis re-vealed only a moderate increase of inflamma-tory parameters and a significant increase ofeosinophils in the differential blood count(23.5 %, reference value: 2.7 %). After a sep-tic process had been excluded, a tentative di-agnosis of an allergic-immunological causewas assumed and therefore, it was decidedto perform a probatory high-dose steroid ad-ministration. Already administration of the first
dose of 500 mg of prednisolone resulted in asignificant improvement of the patient's con-dition. Gas exchange parameters improvedcontinuously, pulmonary infiltrates receded,and eosinophil levels returned to normal. Dueto the clinical picture and the findings madeby lymph node biopsy associated with anecrotizing vasculitis and considerableeosinophilia, the tentative diagnosis statedwas that of an eosinophilic vasculitis of un-clear origin. After seven days, extubation ofthe patient could be performed without anyproblems as he exhibited sufficient sponta-neous respiration and a good vigilance. Inparallel to the ARDS, the patient had devel-oped a considerable coagulation disorder as-sociated with thrombopenia, hypofibrino-genaemia and increased D-dimer levels asan expression of hyperfibrinolysis. However,there was no increased haemophilia.
Neither external nor internal medical historyrevealed any event or responsible agent thatcould be considered as a trigger for the aller-gic-immunological process observed in thepatient. The muscle building product takenbefore the onset of the disease was taken in-to consideration as a possible cause. No sim-ilar cases have become known so far.
NotesThe muscle building product contained a rootpowder from the plant, Lepidium meyenii, alsoreferred to as Maca, which is imported from Pe-ru. In addition, the preparation contains vitaminE and zinc oxide. It is sold as a vitality-enhanc-ing food supplement for health-conscious peo-ple. According to the responsible food controlauthority, it is marketable as a food.
Although closely related to the popular gardencress (Lepidium sativum), the perennial Macaplant has been almost unknown in Europe sofar. Maca was cultivated as a crop plant in Peru
Cases of Poisoning Reported by Physicians
26

in pre-Columbian times already. The edible andnutrient-containing part of the plant is the tuberhaving a size of ca. 8 cm in diameter. The softouter layers are rich in sugars. The more solidinner tissues of the tuber accumulate mainlystarch, but also valuable proteins. The contentof nutrients is even higher than that of cerealsand potatoes. The Maca tuber contains ca. 60% of carbohydrates (mainly starch, but also var-ious types of sugar), 10-13 % proteins, 8-9 %dietary fibre and 2-3 % lipids, mainly fatty acidssuch as linoleic and oleic acid. In addition, itcontains important minerals such as iron and io-dine, but also calcium and magnesium. Othersubstances contained include alkaloids, tanninsand saponins whose biological activity in hu-mans still requires further research. Owing to itsoptimal ingredients, Maca became a medicinalplant surrounded by mysticism in the Andeanregion. It was used as a holy medicinal plant al-ready by the Incas. World-wide, Maca powderhas gained increasing popularity because it issaid to enhance physical energy, enduranceand stamina in athletes, etc.
Evaluation of the case described:In the absence of results of allergy tests, a pos-sible relationship cannot be assessed at present.
3.3.2.2 Atractylosides
Intrauterine hepatic damage of unclear ori-gin after exposure to atractylosidesA female infant aged one month and 20 dayswas admitted to hospital due to an increas-ingly poor general condition. The findingsmade included an inadequate circulation dueto vitamin-K deficiency associated withcholestasis under conditions of hepatopathy.An intrauterine hepatic damage due to theadministration of plant products allegedlycontaining atractylosides was suspected.One of the products involved had been takenby the mother during the last three months ofgestation and the second one, during the lac-
tation period. Both products had been mar-keted as food supplements and were boughtin a pharmacy. The report did not contain anyinformation on why the expectant and laterbreast-feeding mother hat taken the prepara-tions concerned. One of the preparationswas labelled on the package with the warn-ing: 'Do not use during pregnancy'. In the fur-ther course, a diagnosis of progressive famil-ial intrahepatic cholestasis was established.
Manifestations/courseThe child had been suffering from congenitalicterus. One or two weeks before admittanceto hospital, she developed a haematoma onher back. Two days before admittance to hos-pital, she suffered from nose bleeding. Hergeneral state deteriorated, and on admit-tance, the child was in a deeply comatouscondition. Due to an extended epidural haem-orrhage right, the haematoma was immedi-ately subjected to a neurosurgical relievingoperation.
Laboratory analyses revealed increased GOT253 U/L (reference range in children < 1 year:< 38 U/L), GPT 335 U/L (reference range inchildren < 1 year: < 36 U/L), bilirubin 3.5mg/dL (reference range total bilirubin new-borns < 13, adults < 1.1 mg/dL), AP 2340 U/L(reference range in children < 15 years. 110-700 U/L) and a Quick's value of 80 % (refer-ence range 70-100 %). Galactosaemia, ty-rosinaemia, alpha-1-antitrypsin deficiency,neonatal haemochromatosis, Niemann-Pickdisease, Alagille syndrome and infectioushepatitis could be excluded. Hepatopathypersisted in the infant. Liver biopsy was per-formed to exclude a progressive familial intra-hepatic cholestasis. The biopsy results re-vealed a picture of chronic hepatitis associat-ed with giant cell transformation, intrahepaticbilirubinostasis as well as marked septal fi-brosis and moderately floride inflammatory
27

activity. The histological picture was compati-ble with that of a protracted neonatal hepati-tis. Similar pictures had been seen in cases offamilial neonatal hepatitis, virus infections andalso of toxic damage resulting from medicinalproducts. The eosinophilic inflammatory com-ponent could be an indication of a previousexposure to medicinal products, e.g. thepreparations taken by the mother. Metabolicdiseases such as viral infections that may al-so cause neonatal giant cell hepatitis wereexcluded by clinical examinations. By meansof differential diagnosis, the investigatorsfound that a toxic damage had to be consid-ered as the most probable cause to explainthe clinical picture presented. Nevertheless, adiagnosis of progressive familial intrahepaticcholestasis was made in the further course.
NotesThe two products involved were preparationsused in traditional Chinese medicine (TCM). InChina and Japan, there are corresponding tra-ditional plant preparations that have been usedto improve the immune system, among otherpurposes. The two food supplements were ex-amined for hepatotoxic ingredients such aspyrrolizidine alkaloids and atractylosides. Ac-cording to the labels, both preparations containthe rhizome of an Atractylodes species, amongother ingredients. Both preparations containAtractylodes macrocephala (Bai Zhu) as an in-gredient in quantities of 12.4 % and 7.6 %, re-spectively. However, it could be detected only inthe capsules taken by the mother during herpregnancy. The concentration detected in acapsule was below 10 µg.
Phytopharmaceuticals are widely used and arelargely considered as harmless by the generalpopulation. However, on the whole, there hasbeen an increasing number of reports on hepa-totoxic effects of herbal medicines ranging fromminor changes in hepatic parameters to severe
liver damage. Particularly in South Africa, therehave been severe cases of poisoning by theplant, Callilepis laureola, containing atractylo-sides. Atractylosides are diterpene glycosidesthat may cause fatal hepatic and renal necrosisin the mammalian organism and also in humans.They inhibit the oxidative phosphorylation in theliver mitochondria. Cases of acute poisoning byplants containing atractylosides in humans havebeen described and may result in acute hepaticfailure. Also cases of renal damage have beendescribed. Knowledge is scarce concerningtheir chronic toxicity. In literature, there has beenno indication so far of intrauterine hepatic dam-age in an unborn child by atractylosides. InTCM, this plant has been described as having a"calming effect on restless foetuses". Bothpreparations seem to have been composed ac-cording to ancient traditional formulations ofTCM that are not intended for dietary purposesbut primarily for the treatment of a number ofphysical complaints, general weakness and al-so for an improvement of the immune system incases of HIV infection or cancer, among otherconditions.
Preparations that are predominantly intended tocure or relieve diseases must be considered asmedicinal products and not as foods. Also ac-cording to assessments made by the food con-trol authorities and the BfR, the products con-cerned have been suspected of belonging tothe category of medicinal products.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between the mother's ex-posure and the onset of the infant's disease,and given the diagnosis of a progressive famil-ial intrahepatic cholestasis, a causal relationshipcannot be established. However, the elevatedtransaminase levels found initially are not typicalof a progressive familial intrahepatic cholesta-sis.
Cases of Poisoning Reported by Physicians
28

3.3.2.3 Ephedra alkaloids
Adverse reaction resulting from anephedra-containing productThe BfR received a report on a suspectedcase of an adverse reaction to a food supple-ment that had been submitted by a pharma-cy. A customer of the pharmacy had reportedto suffer from health complaints after takingthe preparation. Therefore, she was in doubtabout the safety of the product and contact-ed the pharmacist asking him to check thepackage. According to the letter receivedfrom the pharmacy, the product concerned isa food supplement originating from theNetherlands and containing 20 mg ephedraalkaloids. It is used for weight reduction pur-poses. The product had been unknown to theBfR. Already in 2002, a joint press releasehad been issued by the Federal Institute forHealth Protection of Consumers and Veteri-nary Medicine (BgVV) and the Federal Insti-tute for Drugs and Medical Devices (BfArM)giving a warning against an uncontrolled useof ephedra-containing products.
Manifestations/courseThe customer of the pharmacy had reportedto suffer from hot flashes, nervousness andsleep disorders after taking the preparation.She reported to simultaneously have experi-enced a euphoric effect that had been sopronounced that she found it difficult to re-frain from taking the product. The producthad also taken effect with regard to the in-tended weight reduction. However, these sideeffects and the effect of addiction raiseddoubt in her as to whether the product wassafe in terms of health.
NotesDue to the ephedra alkaloids contained in theproduct according to the information given bythe pharmacy, the product involved may have tobe considered as a medicinal product. The
herb, ephedra (Ephedra sinica) is a Chinesetherapeutic agent. It is available on the marketas a food supplement under the Chinese nameof Ma Huang. Being a natural source ofephedrine, it has pharmacological properties.Its effects include vasoconstriction, circulatorystimulation, rising blood pressure, CNS stimula-tion, strong dehydration, suppression of ap-petite and broncho-spasmolysis. Possible ad-verse reactions include dilatation of the pupils,nervousness, tremor, sweating, cardiac arrhyth-mia, hypertension and at high doses, also con-vulsive seizures and mental changes. Form andcharacter of the ephedra alkaloids naturallycontained in the plant are similar to those ofamphetamine. Therefore, products containingephedra have been classified as medicinalproducts to be sold by pharmacies only In thisway, quality, efficacy and safety of the productsmust be ensured.
Regrettably, products containing ephedra havebeen offered on the internet as food supple-ments or foods which is a practice avoiding au-thorization limitations and quality control. Theyare sold as appetite suppressant or remedy forhay fever. A study performed in the Netherlandson the quality and safety of ephedra-containingproducts revealed that in the majority of theproducts tested, the ephedra alkaloid quantitiesdetected were higher than those stated in thelabelling. Often, caffeine is added to the ingre-dients, increasing the effects of ephedra andthus the risk of harmful effects for the consumer.
In literature, there has been a great number ofreports on health impairment associated withthe use of ephedra-containing food supple-ments. After taking four tablets of a Ma Huangpreparation for alleged weight reduction, abodybuilder complained of severe pain in hisright thorax and suffered myocardial infarction.In another case, a 54-year-old female sufferedfrom hallucination associated with long-term useof food supplements containing ephedra (Clini-cal Toxicology 38 (2000) 5). Recently, it was re-
29

ported that a 22-year-old female was admittedto hospital presenting with tachycardia, nausea,tremor, abdominal pain and vomiting after hav-ing consumed a food supplement containingephedrine and caffeine. Electrocardiography re-vealed manifestations of ischaemia (ClinicalToxicology 41 (2003) 6). The Food and Drug Ad-ministration (FDA) being responsible for the ap-proval of medicinal products and food control inthe USA has announced that it will ban the saleof all products containing ephedrine alkaloids.Also in the Netherlands, the use of ephedrine inproducts other than those classified as medici-nal products has meanwhile been discontinued.
Already in 2002, the former BgVV has pointedout that such products should only be adminis-tered under control by a physician. Products forwhich a therapeutic effect is claimed in adver-tising have to be considered as medicinal prod-ucts. Therefore, such products require authori-zation by the Federal Institute for Drugs andMedical Devices (BfArM). Products lackingsuch authorization are not marketable. In con-trast, food supplements are foods of generalconsumption and must not be advertised byclaiming medicinal effects. Responsibility forsafety in terms of health rests with the manufac-turer. Due to the direct sale of ephedrine-con-taining products on the internet, a completecontrol by the national control authorities is im-possible.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between the ingestion andthe occurrence of the manifestations observed,and in the absence of other causes, a causalrelationship has to be assumed in the case de-scribed.
3.3.3 Foods
3.3.3.1 Butterfish/Escolar
Caution when consuming smoked butter-fish/escolar A female patient and her partner experiencedhealth complaints after the consumption ofsuch fish that had been bought in a freshstate, stored in the refrigerator at 4 °C and un-dergone heat treatment. Manifestations per-sisted for four days. The patient becameaware of the problem when reading com-ments on health reports from Australia pub-lished by the BfR.
Cases of Poisoning Reported by Physicians
30
Fig. 9: Butterfish/Escolar
Manifestations/courseBoth partners experienced gastrointestinalcomplaints in the form of diarrhoea that per-sisted for three to four days, with stools of oilyconsistency and dark yellow colour. After 48hours, a physician was consulted who sam-pled blood for examination and recommend-ed to drink large amounts of fluid. Since therewas no feedback from the physician consult-ed, it has been assumed that the results ofchemical examinations were not alarming. Noreport was received from the attending physi-cian.

NotesIn mid-2003, Australian health authorities report-ed health complaints associated with the con-sumption of escolar, also referred to as rudder-fish. 98 cases had been recorded since 1999.In a press release, the BfR informed the publicthat in particularly sensitive persons, the con-sumption of large amounts of fish of thespecies Lepidocybium flavobrunneum (escolar)and Ruvettus pretiosus (oilfish) both belongingto the Gempylidae family (German terms: "But-terfisch" or "Buttermakrele") may cause healthimpairments such as diarrhoea, abdominalcramping, vomiting and headache and warnedthat caution be observed when eating suchproducts. Experts have assumed as a presump-tive cause the presence of poorly digestible oreven indigestible wax esters that represent 90% of the oil or fat in these two fish species. Sofar, it has remained unclear whether these waxesters are the only causes responsible for suchillnesses or whether there are other factors play-ing a role as well. Such factors could possiblyinclude certain allergenic fish proteins or bio-genic amines (histamine, among others) thatmay form in fresh fish during extended storageperiods. Another unknown factor consists in thequantity of fish that must be consumed to pro-duce such health disturbances. The Germanterms of "Butterfisch" and "Buttermakrele" arecollective terms used in the marketing of severalhigh-fat fish species caught as by-catch indeep-sea fishing. In Germany, such fish hasbeen available on the market for several years inthe form of hot smoked fish cuts referred to as"geräucherte Buttermakrele", formerly"geräucherter Butterfisch". According to a studyby the Federal Research Centre for Fisheries inHamburg, waxy esters form more than 90 % ofthe oil or fat of the smoked "Butterfisch" and"Buttermakrele" marketed in Germany. The twocases described above are the first ones report-ed in Germany.
With regard to the toxicity of fishery productsassigned to the family of Gempylidae, an expert
opinion of 30 August 2004 by the Scientific Pan-el on Contaminants in the Food Chain (CON-TAM) stated that according to the EFSA (Euro-pean Food Safety Authority), it was not possibleto establish, on the basis of case reports re-ceived, an intake level for such fish which wouldnot lead to these adverse effects. By using ap-propriate practices of preparation, such as dis-carding the oil released, the occurrence of suchsymptoms may perhaps be avoided.
Evaluation of the case described:On the basis of the information given in the twoabove cases on the temporal relationship be-tween the ingestion and the occurrence of themanifestations observed, and in the absence ofother causes, the existence of a causal relation-ship has to be assumed.
Other cases involving butterfish/escolarReports by lay persons after publication of thearticle on the internet.
Case No. 4592/04After the consumption of 350 g of fish each,both partners suffered from severe diarrhoeapersisting for five to six days. Their stools con-tained large quantities of fat excreted in theform of globules. However, this type of diar-rhoea was not associated with pain as usual.
Case No. 4593/04One day after the consumption of 300 g of fish,diarrhoea with stools of a yellow colour andwaxy-oily consistency occurred that persisteduntil the next day. There were no other healthcomplaints.
3.3.3.2 Shiitake mushroom
Shiitake dermatitis (flagellate dermatitis)A dermatological outpatient department re-ported on a patient presenting with dermalmanifestations after the ingestion of at leasttwo raw shiitake mushrooms on two consecu-
31

tive days. The patient's wife had also eatensuch mushrooms, however, without develop-ing any health complaints.
lar scales, its gills are white-brownish and itsspores colourless. It is highly valued as a fooddue to its excellent spicy taste. It has been as-cribed extensive favourable effects on health.Particularly in Chinese and Japanese cooking, ithas been a quite popular food. However, it isbeing cultivated and consumed in largeamounts also in Germany. It is the second mostpopular mushroom in the world next to the but-ton (table, white) mushroom. The beneficialproperties and effects ascribed to this "overallhealthy mushroom" include being a source ofprotein, potassium, zinc, vitamins B1, B2 and D,and more, an activator of the immune system, areducer of the cholesterol level, and havingfavourable effects on the immune system in thetreatment of cancer and AIDS. The main flavour-ing substances identified are sulfur compounds.They include lenthionine, tetrathiane and trithi-olane as well as the amino acid, eritadenine.
In a few individuals, consumption of thesemushrooms may have unpleasant conse-quences. Some hours after the meal, they willdevelop a so-called shiitake or flagellate der-matitis. The medieval penitents castigatingthemselves, also referred to as flagellants, lenttheir name to the clinical picture of the diseasebeing characterised by skin lesions which re-semble whiplashes on the trunk, the arms andlegs and on the neck. In the past, such skinmanifestations had been seen mainly after theingestion of inadequately cooked mushrooms. Itwas, therefore recommended to eat shiitakemushrooms only if they had been thoroughlycooked or fried. However, recent reports havesuggested that the type of preparation was ofno influence on the health complaints devel-oped by sensitive individuals.
The suspected cause of the intolerance reac-tion is the polysaccharide, lentinan, being a nat-ural component of the mushroom. The sub-stance appears to be heat-stable which is why itmay cause the dermatitis to develop also afterthe ingestion of well-cooked and fried mush-
Cases of Poisoning Reported by Physicians
32
Fig. 10: Shiitake mushroom
Manifestations/courseThe changes of the skin observed were de-scribed by the physician on duty as linearerythema (similar to factitious urticaria)spreading over the entire body including thehead. In addition, disseminated seropapuleswere seen. Furthermore, the patient stated tofeel weak and abnormally tired. One monthlater, he still complained of skin irritation onmechanical stimulation. Treatment includedsystemic administration of cortisone which,however, was not taken by the patient. An al-lergy test was to be performed. The result re-mains to be seen.
NotesThe shiitake mushroom (Lentinus edodes) be-longs to the family of Tricholomataceae and is asaprophytic fungus which colonises deadwood. Its cap has a diameter of up to 20 cmand is of brownish-grey colour with flat triangu-

rooms. In spite of the large quantities of shiitakemushrooms cultivated world-wide, cases of shi-itake dermatitis have been very rare in Germany.Obviously, a sensitive reaction is developed by afew individuals only while the causes have notyet been elucidated. It has been assumed thatresponsible factors may also include unknownco-factors in addition to the amount ingestedand the type of preparation. Based on the num-ber of cases described, the risk for the con-sumer seems to be low, according to the pres-ent state of knowledge.
Mainly Japanese authors have reported aboutworkers on mushroom farms who had devel-oped an allergic alveolitis after inhalation of shi-itake spores. In this context, also cases of aller-gic contact dermatitis were mentioned thatcould be diagnostically confirmed by means ofthe patch test. As a sign of the allergic reaction,the skin rash was found to be associated witheosinophilia. Flagellate dermatitis was de-scribed for the first time in 1977 by Nakamura.In 1985, he reported on 30 cases observed inJapan within a period of nine years. They re-ferred to patients presenting with severe erythe-ma and pruritus after ingestion of the mush-rooms in traditional Asian dishes. All his patientssuffered from intensely pruritic, very smallpapules appearing closely together in lines.They reported these stripes to have developedwithin one or two days after the meal containingthe mushrooms. The stripes expressing a Koeb-ner phenomenon had obviously resulted fromscratching of the skin. The manifestations dis-appeared after 20–30 days. Until 1991, Naka-mura recorded a number of additional cases.Other authors reported on 58 patients present-ing with shiitake dermatitis during the1997–2001 period. In 33 of these cases, thedisease had developed after the ingestion ofsufficiently cooked/boiled mushrooms. In Ger-many, only single cases of this disease have oc-curred after consumption of this mushroom.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between the ingestion andthe occurrence of the manifestations observed,and in the absence of other causes, a causalrelationship has been considered as probable.
3.3.4 Welding fumes
Moderate health impairment after weldingof plastic materialA 39-year-old worker reported to have weldedplastic material on two days for a period of al-together 17 hours. At his workplace, the ex-haust hood under which the work was per-formed was defective. In addition, he hadworn a defective gas mask for three hours.On the following evening, he experiencedhealth complaints that caused him to seekmedical advice in an outpatient department.
Manifestations/courseThe patient reported influenza-like symptomsin the form of arthralgia over the last 36hours. In addition, he suffered from severecough and fever. Inhalation was associatedwith marked pain, and he experienced dysp-noea and decreasing vitality. His cigaretteconsumption was stated to be ten cigarettesper day. The findings of an outpatient exami-nation performed two days later revealed thatthe patient was in a good general condition.Cardiovascular and pulmonary findings, aswell as the status of the other organs exam-ined were normal. No treatment was required,and the patient was recommended to avoidmajor physical strain and temporarily refrainfrom smoking.
NotesThe case described above was presumably dueto exposure to fumes from plastic materials re-sulting from non-compliance with occupationalsafety regulations. The manifestations describedwere largely compatible with those of polymer
33
fume fever being similar to those of metal fumefever. During the processing of plastic materials,fluorocarbons in monomer or polymer form arereleased that may cause polymer fume fever. Itis characterised by chest pain, choking fits, drycough, fever, shivers and arthralgia. In mostcases, such manifestations will disappear withinone or two days after exposure. However, alsoprotracted pneumonia associated with agoniz-ing cough, retrosternal pain and general healthimpairment may occur. Chronic health damagehas not been recorded. Exposure to fluorine gasand possibly hydrocyanic acid could not be ex-cluded. Due to the short half-life of both sub-stances, a toxicological analysis was no longerpossible after two days had passed.
Health impairment after steel welding oper-ationsDuring the welding of antimagnetic steel, aworker had inhaled chromium and nickelfumes, in spite of wearing a respirator. Thisresulted in moderate health impairment re-quiring inpatient treatment.
insufficiency. An elevated carbon monoxideHb level (CO-Hb) was found. Pulmonaryoedema could be excluded by radiologicalexamination. The patient's condition improvedrapidly under oxygen supply and inhalatoryadministration of corticoids. He could be dis-charged in a symptom-free state on the fol-lowing day.
NotesThe above case of moderate health impairmentwas possibly associated with the formation ofchromium and nickel fumes during welding op-erations. A temporary partial respiratory insuffi-ciency receded rapidly under appropriate treat-ment. Chromium and nickel fumes may cause ir-ritation of the respiratory tract after inhalationalexposure. Single cases of respiratory diseaseafter occupational exposure to chromium dustand chromium compounds have been reportedwhich were associated with functional pul-monary disorders. Inflammatory and asthma-likelung diseases were reported to have occurredafter acute inhalational exposure. A sensitisingeffect on the respiratory tract has to be as-sumed.
3.3.5 Internal combustion engines
Industrial accident associated with an in-ternal combustion engineAt his workplace, a 33-year-old patient hadcut a concrete slab in an insufficiently venti-lated room. The disk grinder used was pow-ered by an internal combustion engine. Inspite of occasional breaks, the patient hadexperienced health complaints after twohours of working. He was monitored at an in-tensive care unit for one day.
Manifestations/courseAfter having worked for approximately twohours, the patient experienced vertigo and
Cases of Poisoning Reported by Physicians
34
Fig. 11: Welding
Manifestations/courseTypical signs of inhalational poisoning weredescribed including dyspnoea at rest, verti-go, cough and two episodes of vomiting. Ablood gas analysis performed on the day ofadmission to the hospital revealed a partial
weakness. He could just leave the room be-fore his legs gave way. There was no loss ofconsciousness nor breathing difficulty. Hewas immediately subjected to intensive med-ical treatment. The carbon monoxide Hb level(CO-Hb) established on the patient's arrivalwas 29.1 %. Under high-dose oxygen supply(15 L/min), the CO-Hb decreased to 2.1 %.Since it remained unclear whether other toxicgases had also been present in the room, thepatient was monitored for another 24 hoursand administered dexamethasone. On the fol-lowing day, the patient could be dischargedin a good general condition.
NotesThe circumstances described by the patientraised doubts as to whether the required meas-ures of occupational safety had been compliedwith. Working in a poorly ventilated room withmachinery powered by an internal combustionengine involves a considerable health risk forthe operator. Possible organ damage due tooxygen deficiency may result in permanentbrain damage or even acute death from suffo-cation.
Combustion gases from internal combustion en-gines contain 4–11 % carbon monoxide. Carbonmonoxide is haemotoxic. It binds to haemoglo-bin to form carbon monoxide Hb (CO-Hb) bydisplacing the oxygen. The affinity of carbonmonoxide to haemoglobin is 300 times higherthan that of oxygen. This is the reason for thehazard posed by CO. Individuals differ consid-erably in their sensitivity to carbon monoxide inacute poisoning events. Because of their higherrespiration rate and more intense metabolism,adolescents and small and slim persons aremore at risk, as a rule, than adult and sturdypersons. Already at CO-Hb levels as low as 4 %, changes can be detected in psychomotortests. As in the case described above,headache, weakness and vertigo will as a ruleoccur, if ca. 30 % of the haemoglobin has be-come bound by carbon monoxide. Levels above
40–50 % will result in collapse and uncon-sciousness. If the respiration is deprived of75 % of the haemoglobin, the inevitable resultwill be death from suffocation. As compared toyounger individuals, CO-Hb concentrations that may lead to death become lower with in-creasing age. Carbon monoxide poisoning isparticularly often followed by late damage andsecondary diseases that may occur mainly assequelae of hypoxia experienced over a moreor less extended period. Frequent sequelae in-clude brain damage characterized by differentmanifestations because the central nervous system is highly sensitive in its response to hypoxia. Other sequelae recorded include my-ocardial necrosis and pneumonia. Also changesin the peripheral nerves or even paralysis havebeen reported. Similar to the central manifesta-tions, they are in part caused by primary vascu-lar damage.
The German MAK (maximale Arbeitsplatzkon-zentration – maximum admissible concentrationat the workplace) has been set at 30 mL/m3 (33mg/m3), and the BAT (Biologischer Arbeitsstoff-toleranzwert – biological threshold limit value),at 5 % CO-Hb in whole blood at the end of theexposure period.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between carbon monoxideinhalation and occurrence of the manifestationsobserved, and in the presence of clearly elevat-ed blood levels, a causal relationship has beenconfirmed.
3.3.6 Sewage collector tank
Serious industrial accidents in an industri-al sewage collector tankThe bottom of a sewage collector tank (depthca. 3 m, capacity 60 m3, manhole 1.50 m2) ofa plant producing leather fibre was to becleaned by means of a fire hose. For this pur-
35

pose, a worker wearing a gas mask enteredthe tank over a ladder and flushed the tank.The estimated outside air temperature was 28°C. Another worker stood at the entrance ofthe tank at a visible distance. Having finishedthe cleaning work after ca. 30 min, the workerwearing the gas mask climbed up the ladder.When his head was already above the level ofthe tank manhole, he took off the mask andhanded it over to his colleague responsiblefor supervision. At that moment, he fell back-wards into the sump of the tank. The workerstanding on ground level immediately soughtthe help of two colleagues, who unfortunatelyentered the tank without wearing protectivemasks and taking any protective precautions.One of them and the first worker affectedcould only be recovered dead by the firebrigade. The third worker was rescued alive.He suffered a severe brain damage. Obvious-ly, hydrogen sulfide had formed and the safe-ty precautions for working in sewage tankshad probably not been complied with. Nomeasurements were performed on the sceneneither before nor after the accident had hap-pened.
Manifestations/course1. Case No. 3951/04The deceased had cleaned the sewage tankwearing a filter mask. When he had climbedup the ladder and taken off the mask stand-ing on the last rungs, he fell backwards intothe tank for unknown reasons. He could onlybe recovered in a dead state. Post-mortemfindings indicated an acute poisoning by gas-es from the sewage tank. On post-mortem,the body surface and lung sections exhibiteda markedly putrid smell. Lung findings re-vealed oedema and tissue haemorrhage. Fur-thermore, clear signs of mucosal irritationwere found. Such findings may be explainedby an inhalation of hydrogen sulfide. Therewere no signs of drowning found neither by
post-mortem examination nor by toxicologi-cal-chemical analysis.
2. Case No. 3805/04A 51-year-old male who had tried to rescuethe first worker affected by the accident with-out taking protective measures and sufferingfrom respiratory insufficiency and acute pul-monary oedema was transported, by anemergency ambulance, to the intensive careunit of a university hospital. On admission tohospital, the patient was in an analgosedated,intubated and respirated state and his circu-lation was stable. The peripheral oxygen satu-ration level was 86 %, with an FiO2 of 1.0.The causative agent could not be identified.The cause assumed was inhalation of hydro-gen sulfide having become released in thetank. Also a formation of hydrogen cyanidecould not be excluded. Still on the day of ad-mission, the patient was subjected to bron-choscopy that revealed a massive aspirationof gastric contents. The bronchial mucosawas highly sensitive and oedematous. Thesemanifestations disappeared under antibiotictherapy and systemic and inhalatory adminis-tration of steroids as well as adrenaline in-halation. Respiration therapy which also re-quired tracheotomy could be discontinued af-ter seven days. However, the patient remainedcomatose. As a response to pain stimulus, hespontaneously opened his eyes without visualfixation and did not respond when accosted.He temporarily exhibited swallowing andchewing movements and an anisocoria rightwith persisting reaction to light. He was com-pletely paralysed (tetraplegic) and inconti-nent. The cranial computer tomography per-formed did not reveal any pathological find-ings. In the further course, the patient suf-fered from convulsive seizures that could becontrolled effectively by medication. A severecerebral psychosyndrome was diagnosed. Tooptimize nursing care, percutaneous endo-
Cases of Poisoning Reported by Physicians
36

scopic gastrostomy was performed. For fur-ther rehabilitation, the patient was transferredto a neurological rehabilitation centre. The se-vere cerebral damage will probably result inirreversible sequelae. The subsequent courseremains to be seen.
3. Case No. 3950/04The second worker who came to rescue thefirst one could only be recovered when al-ready dead.
Post-mortem findings revealed signs of acuteoxygen deficiency associated with indicationsof a possible poisoning by hydrogen sulfide.Findings included a faeces-like smell of lungsections and mucosal haemorrhage probablycaused by toxaemia. The toxicological-chemi-cal expert opinion stated that highly volatileorganic compounds were detected in thelung tissue by gas chromatography which,judged by experience, suggested a non-mas-sive inhalation of sludge digestion gases.Blood taken from the left ventricle revealed anexcess water content of 29 %.
On this basis, it had to be assumed that thedeceased had lost consciousness due to theinhalation of sewage gases and died fromdrowning. Based on toxicological-chemicalexperience, death from drowning is suggest-ed by water levels above 5 %.
NotesHydrogen sulfide is an extremely toxic irritantgas. Due to its higher density as compared toair, it accumulates on the bottom of manuretanks, well shafts and in sewer systems where itis formed in the process of anaerobic digestionof organic material. It is a colourless gas with aputrid smell (resembling that of rotten eggs)that may form explosive mixtures with oxygen.Its smell cannot be perceived at higher concen-trations because it paralyses the olfactory
nerve. It exerts a direct depressive action on thecentral nervous system and inhibits cytochromeoxidase to a higher degree than hydrogencyanide does. Due to its quick absorption afterinhalational exposure, poisoning by this gas ischaracterized by an apoplectiform course asso-ciated with a rapid onset of unconsciousness.Being a weak acid, hydrogen sulfide will alsoact as a local irritant.
In the following, H2S concentrations are listedtogether with typical cardinal signs:
37
H2S concentration
(ppm)Cardinal signs
0.025-0.13 Olfactory threshold
0.30 Clearly perceptible smell
10-100 Irritation of eyes, throat and nose
100-150 Paralysis of the olfactory nerve
>150 On inhalation for > 30 min: headache, vertigo, diarrhoea
300-500 Pulmonary oedema
500-700 Inhalation for half an hour can be lethal
>1400 Apoplectiform lethal poisoning, death after taking a few breaths
In the cases involved in the severe industrial ac-cident described above, occupational safetyrules had obviously not been complied with. In-vestigations revealed that no hazard analysis hadbeen performed. There had been neither an in-spection of the tank where the accident hap-pened nor any internal instructions for entering it.
For the inspection of such tanks, the wearing ofpersonal protective equipment and rescueequipment is required by law. For example, en-tering such a tank is only permitted for personsroped up with block-and-tackle equipment.

Therefore, rescue of persons is only permittedin cooperation with the fire brigade using appro-priate respiratory protection. A simple roping-upwith the lifeline of the rescuer is insufficient.There are also rules with regard to the wearingof respirators. Prior to entering such tanks, theambient atmosphere in the tank has to be meas-ured by means of a measuring instrument de-veloped especially for this purpose. The meas-uring result will decide on the protective meas-ures to be taken. The use of filter-type respira-tors will depend on the prevailing ambient at-mosphere while self-contained apparatus canbe used irrespective of the ambient atmos-phere. This implicates that filter respirators mustnot be used in cases of unknown ambient con-ditions or of possible detrimental changes in thecomposition of the ambient conditions. In addi-tion, the multi-gas filter mask used by the firstvictim of the accident was to be used only untilMarch 2004. It has to be concluded that the se-vere accident resulting in two deaths amongthree persons involved could have been pre-vented if the applicable rules had been com-plied with.
Evaluation of the cases described:On the basis of the information given on thetemporal relationship between the inhalationalexposure to hydrogen sulfide and the occur-rence of health impairments in the three tragiccases described, and in the absence of othercauses, a causal relationship has been consid-ered as probable.
3.3.7 Battery acid
Severe eye burns after exposure to batteryacidA 34-year-old patient was involved in an in-dustrial accident when splashes of batteryacid hit both of his eyes. The scene of the ac-cident was a storage area where probably abattery exploded. The patient suffered a se-
vere eye injury, particularly in his left eye. Herequired inpatient treatment for two weeks.The possibility of a further development of alens opacity requiring a cataract operation re-mains to be seen.
Manifestations/courseOn admission to hospital, the patient's visualacuity was severely reduced. Treatment in-cluded thorough irrigation with lactatedRinger's solution and BSS (balanced salt so-lution). X-ray findings of the orbital cavitywere normal. Corneal erosions were found inboth eyes, and hyphaema in the left eye. Thelatter was gradually absorbed except for aresidual coagulum. However, the patient de-veloped a glaucoma with an intraocular pres-sure of up to 42 mm Hg (17±3 mm Hg, on av-erage, in healthy persons, this value is ex-ceeded in persons suffering from glaucoma).To relieve the patient's condition, he wastreated by administration of acetazolamide.After two weeks, the patient was discharged.Vision of the right eye was completely re-stored, and the anterior segment found to benormal. The residual visual acuity of the lefteye was only 0.25. The conjunctiva was hy-peraemic. In addition, a loss of iris pigmentand its deposition in the anterior chamberand a sphincter lesion were found. The pupilwas misshapen. Findings also included a mi-nor corneal scar. The patient developed aslight lens opacity. Findings regarding the ac-cessible ocular fundus were normal. Thepupil response to light was only minimal. Thepatient was referred to further outpatienttreatment. To reduce the intraocular pressure,he was administered brinzolamide and locally,brimonidine and timolol eyedrops. In theevent of an increasing lens opacity, the pa-tient may require a cataract operation involv-ing the implantation of a posterior chamberlens.
Cases of Poisoning Reported by Physicians
38

NotesMotor vehicle batteries contain sulfuric acid in a32 % concentration to act as an electrolyte be-tween the positive plate consisting of lead oxideand the negative plate consisting of pure lead.In accidents, above all those involving explo-sion, the corrosive effect is decisive. Absorptionis not to be expected. With the exception of thehydrofluoric and sulfuric ones having an oxida-tive effect, acids will penetrate tissues less rap-idly than bases. The coagulation of proteinscaused by the hydrogen ions liberated will resultin a relative protection against a deep penetra-tion of acids. Minor eye injuries are associatedwith hyperaemia or chemosis of the conjunctivaand loss of the epithelium of the cornea, whilethe underlying corneal stroma remains clear.Such cases will heal within a few days withoutsequelae. Severe burns are characterized byextended and mainly deeper damage. Damagewill include large parts of the conjunctiva andthe underlying tissue. Visible blood vessels willbe thrombosed and appear in a brownish-blackcolour. The cornea becomes cloudy, and the iriswill exhibit a dirty-grey discoloration. Lensopacity (cataract) as well as protracted inflam-mation and glaucoma may occur. Eye burns arealways to be considered as emergencies. As afirst aid measure, decisive importance is attrib-uted to immediate ocular irrigation with at least1.5 L water that should be administered by ahelper because in severe cases, the person af-fected by the accident will be unable to performan effective irrigation, if any. Afterwards, the pa-tient should see a specialist. Water as an irriga-tion fluid will mostly be available in sufficientquantities. Intensive irrigation will result in the di-lution effect intended. However, water will alsoincrease the oedema and permeability of thecornea. Therefore, saline isotonic with tears orhypertonic saline should be preferably used.Lactated Ringer's solution – as was used in theabove case – is buffered and thus more effec-tive than physiological saline. BSS (balancedsalt solution) having the same osmolarity as theaqueous humour and a neutral pH is even more
suitable. It was developed especially for oph-thalmologic operations. It can prevent the devel-opment of corneal oedema and protect the en-dothelium. The subsequent procedure will de-pend on the degree of severity of the damagesuffered.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between the exposure ofthe eyes and the occurrence of the manifesta-tions observed, and in the absence of othercauses, a causal relationship has been con-firmed.
39
Health impairments due to starter batteries orautomobile accumulators/storage batteries haveaccounted for a major part of reports submittedto the BfR (n=597), particularly of those submit-ted by the professional insurance bodies (Beruf-sgenossenschaften: 590). Fortunately, the num-ber of such cases has been decreasing since2001 (2001: 176 cases, 2002: 161 cases, 2003:129 cases, 2004: 96 cases). Most often, theeyes were affected (n=452), but there were alsoreports referring to skin exposure (n=129), in-halational exposure (n=53) and ingestion (n=4).The majority of cases involved only minor health
Fig. 12: Motor vehicle battery

impairment (n=533); in 35 reports, the healthimpairment suffered was evaluated as moder-ate. 21 cases reported could not be evaluatedwith regard to the degree of severity, and in sev-en cases, no manifestations had been record-ed. The only case where a patient was affectedby a severe health impairment was the one de-scribed above. The majority of incidents in-volved unexpected gas deflagration or explo-sion of accumulators resulting in acid splashingup from accumulators causing burns, mostly inthe eyes.
With regard to the mechanism of accidents,three major types can be distinguished.1. During installation and removal of batteries,
short circuits between the accumulator bat-tery posts may be caused by conductivetools such as spanners. This may result in ex-plosion.
2. Accidents may occur when batteries arerecharged.
3. During transport, for example when carryinga battery, splashes may be released due tostumbling or if the battery is put down rough-ly.
Although most accidents of this type happenedat the workplace, the private consumer may beat risk as well. Particularly in the autumn andwinter months, many starter batteries are ex-changed in a DIY procedure. Often, people do-ing so are not aware of the risk involved. Utmostcare should be exercised when exchanging orrecharging batteries. It is recommended to fol-low all instructions given e.g. on new batteries inthe form of stickers or pictograms. It is recom-mended to always wear safety goggles and pro-tective clothing when performing such opera-tions. Regular maintenance is important. Batter-ies should be recharged only by means of ap-propriate loading devices and in well-ventilatedrooms. Sparking (e.g. from cigarettes) and openfire must be avoided at any rate. After therecharging process, the battery should be al-lowed to outgas for eight hours prior to being in-stalled (risk of formation of oxyhydrogen gas).
When connecting the battery, care must be tak-en that all current consumers in the vehiclesuch as light, radio etc. are switched off.
Already in its 2001 Annual Report, the formerFederal Institute for Health Protection of Con-sumers and Veterinary Medicine (BgVV) hasdrawn attention to the problem of health impair-ment due to starter batteries and accumulators.
3.3.8 Glow sticks
Eye injury caused by glow stickAt a company event, glow sticks were handedout to the participants. An 18-year old malemanipulated one of these sticks so that itbroke apart and splashes of the liquid con-tained hit his face and left eye. According tothe respective safety data sheet, the productcontained 8–12 % tert-butyl alcohol and 4–5
Cases of Poisoning Reported by Physicians
40
Fig. 13: Glow stick

% hydrogen peroxide (70 %). Since ocular ir-rigation could be performed already threeminutes later at the company's medical serv-ice rooms, permanent damage to the pa-tient's health was not to be expected.
Manifestations/courseThe patient complained of extremely painfulsmarting in his eye and face. His left eye andfacial area were intensely reddened, and thegreen fluorescent colorant was well visible. Athorough irrigation of the eye with Ringer'ssolution was initiated immediately. In addition,an attempt was made to remove the liquidfrom the patient's face and hair. The ophthal-mologist consulted diagnosed a chemicalburn of the conjunctiva. Permanent damagewas not to be expected since eye irrigationhad been performed early enough.
NotesBased on the report submitted by the companydoctor, attention is drawn to a number of facts inthis case.� The liquid was very difficult to remove. It
could not be removed at all from the patient'shair. The process of removal from the faceand eye, although performed by means ofthorough irrigation, took a very long time, anda quantity of 1 L of Ringer's solution had tobe used, with pain always flaring up whenthe irrigation was interrupted.
� No warning whatsoever was found on theproduct indicating that the substance contai-ned was harmful to the eyes. The safety datasheet stated merely, "moderate eye irritation".Given the experience made, the attendingphysician considered such information as akind of "understatement".
Glow sticks consist of two liquids contained in aplastic tube. By bending the sticks, the two liq-uids become mixed, thus producing a glow. Thesafety data sheet states the following informa-
tion with regard to health risks: "Direct contactwith this material may cause moderate eye irrita-tion". Enquiries made with the distributor of theproduct revealed that no similar case had be-come known so far. The distributor, who hasbeen given a detailed description of the case,will consider to provide additional warnings onthe product packaging. The result remains to beseen.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between the exposure ofthe skin and eye and the occurrence of themanifestations observed, and in the absence ofother causes, a causal relationship has beenconfirmed.
3.3.9 Multiple chemicals
Multiple chemical sensitivityA 36-year-old female biological laboratory as-sistant presented with multiple health com-plaints at an environmental health clinic. Shehad been occupationally exposed to a varietyof chemicals, particularly to solvents. After achange of her workplace, she developed ahypersensitivity to chemicals, mainly to sol-vents. At her former workplace, she hadworked mainly with acetonitrile, methanol andtoluene. The occupational safety conditionswere described as other than optimal. Ac-cording to information given by the patient,there had not been enough safety cabinets,and the rooms had been very small. Regular-ly, she had to work overtime. Since late 2002,she began to suffer from health problems thatimproved during her annual leave. Since shequitted her job in early 2004, she has foundher health to improve slowly but continuously.
Manifestations/courseThe patient complained of night sweat andsleeplessness, nausea and diarrhoea. In ad-dition, she stated to suffer from dizziness, ver-
41

tigo, poor concentration and bad memory.She complained of panic attacks, anxietystates, tachycardia, cardiac arrhythmia, circu-latory problems, speech disorders andheadache. She reported to have frequentlydeveloped migraine after contact with chemi-cals. In indoor situations, she suffered fromrespiratory problems. In addition, she suf-fered from tinnitus and skin rash. Altogether,she reported her state of health to vary con-siderably.
Below, a report by the patient herself is cited:"Finally, I had no longer the mental capacity tooperate a technical device. My forgetfulnesscaused loss of time and an additional work-load. Another reason for quitting my job wasthat due to my dizziness, I made mistakeswhen driving. I did not want to end up stick-ing to a tree with my car. In the end, there wassimply nothing working normally with me.When I thought that all that was only due tostress, I took a time-out for myself. I startedgoing to work by bicycle as often as possible(ca. 18 km through the countryside). This re-sulted in a temporary subsiding of my symp-tomatology." Concerning her medical history,the patient reported to have undergonesubtotal thyroidectomy due to adenoma ofthe thyroid gland in 2002.
Findings of physical examinations were nor-mal as were the clinical-chemical parametersof routine laboratory analysis. A psychiatricexamination indicated the presence of an un-specific somatoform disorder and additional-ly, of dysthymia and panic disorder. Gratify-ingly, it was found that the patient obviouslyhad managed to considerably improve herstate of health by means of a number ofhealth-promoting measures taken on her owninitiative. However, the examiners consideredan extended regeneration period of severalmonths as necessary for her to completely re-
gain her health and stress tolerance. Theystated that after that period, there was a real-istic chance for her to return to work as atrained laboratory assistant. However, optimalworking conditions should be ensured if pos-sible.
NotesThe clinical picture seen is that of a so-calledmultiple chemical sensitivity (MCS). The aetiolo-gy and pathogenesis of her complaints have notyet been conclusively elucidated. MCS can bedescribed in a most appropriate way as aprocess with multifactorial causes. It is a sensi-tivity that is associated by the patients with ex-posure to chemicals and characterized by re-current manifestations in several organ systems.The symptomatology is mostly unspecific andincludes, for example, headache, vertigo, tired-ness, weakness of concentration, cardiac andcirculatory complaints, gastrointestinal com-plaints, dermal and mucosal symptoms, myalgiaand arthralgia. The symptoms are attributed toexposure to a great number of chemically unre-lated substances which likewise cannot be as-sumed to have any specific effect, e.g. on thereceptor level. There is no dose-effect relation-ship. The concentrations of the substances in-criminated have been far below those leading tohealth problems in the general population. Nei-ther clinical nor laboratory tests have shown anycorrelation with the complaints reported by thepatients, which are often experienced as veryserious and as a considerable impairment oftheir quality of life. In addition to toxicologicaltriggering factors, a variety of other factors suchas stress, electromagnetic fields and microor-ganisms may play a role in the development ofMCS. Substances stated most often by patientsaffected include solvents, dust, smoke, pesti-cides, foods and medicinal products. Thresholdvalues at which symptoms are triggered are ex-tremely low. A variety of possible causes ofMCS can be imagined: Factors that have been
Cases of Poisoning Reported by Physicians
42

discussed include an overreaction of the im-mune system, disorders of the olfactory systemor of the olfactory-limbic system. Mental mecha-nisms based on anxiety disorders play a role.On account of insufficient data available on thegenetic predisposition to develop MCS, genetictesting is not recommended.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between chronic exposureto solvents and the occurrence of manifesta-tions associated with a minor health impairment,and in the absence of other causes, a causalrelationship has to be rated as possible in thecase described. In addition to a possible trig-gering of sensitization to solvents due to long-term occupational exposure, the development ofsymptoms had been most probably also causedby psychosomatic factors. Other possible co-factors in the development of the symptomatol-ogy described are the inappropriate industrialsafety conditions and the non-optimal organiza-tion of the work resulting in regular overtimehours. In all probability, according to the as-sessment by the environmental health clinic, acombination of influencing factors had causedthe hypersensitivity and persistent complaints.
3.3.10 Henna tattoos
Allergic local reaction associated with hen-na tattooAn 18-year-old female sought medical advicefrom a general practitioner after having a tat-too made ten days earlier in Malta. No datacould be obtained on the product name orthe manufacturer. The patient was subjectedto an extended topical treatment resulting in acomplete regression of her health complaints.
Manifestations/courseThe patient presented with local erythemaand swelling of the skin in the area of the tat-too. A beginning keloid formation receded
completely on administration of a cortisoneointment.
NotesMore and more cases of contact dermatitis as-sociated with henna tattoos have been de-scribed in literature. Henna, an extract of theplant, Lawsonia, has been known for centuries inmany cultures as a means to dye hair and nailsand for decorative body painting. Also in Ger-many, wearing tattoos is very popular, particular-ly among adolescents. Henna tattoos (also re-ferred to as temporary tattoos) are not tattoos inthe proper sense because the colorant is ap-plied onto the surface of the skin. Such tech-niques are subject to the legal provisions oncosmetics under the European Cosmetics Direc-tive and the German Cosmetics Regulations.
The most frequently observed undesirable con-sequences of such tattooing include severe al-lergic reactions and inflammations. In most cas-es, the active substance, paraphenylene di-amine (PPD) is the cause of the allergic reac-tion. It is used in henna to darken its colourshade, and when making black henna tattoos, itis applied onto the skin and may penetrate intoit. It is also known as a hair dye. Persons whohave experienced sensitisation to PPD may ex-hibit allergic reactions to this substance for theirentire lifetime. Other sources of risk includecontaminants in the colour mixtures as well ascertain azo dyes that may split and form car-cinogenic aromatic amines.
While cosmetics are subject to legal regulationsstipulated by the German Foods and OtherCommodities Act, the German Cosmetics Regu-lations and the European Cosmetics Directive,tattoo dyes are still not subject to any compara-ble legal regulation. Up to the present, therehave been no legal provisions on tattoo dyes re-ferring to the degree of purity, quality and test-ing for safety in terms of health. A national regu-
43

lation is being prepared at present. Tattoos andpermanent make-up should only be performedusing colorants that comply with the require-ments of the European Cosmetics Directive andthe German Cosmetics Regulations, i.e. thathave been tested and approved for the use incosmetics. Problematic colorants containingsubstances that are hazardous due to their car-cinogenic, mutagenic or sensitising propertiesor reproductive toxicity or may form aromaticamines by splitting should be banned for suchuses. Efforts should be made to ensure an ap-propriate training and health control of personswho carry out tattooing and apply permanentmake-up. The BfR has already commented onthe health risks involved in tattoos and perma-nent make-up.
Evaluation of the case described:Based on the information given on the temporalrelationship between dermal exposure and theoccurrence of the manifestations observed, andin the absence of other causes, a causal rela-tionship has been rated as probable in the casedescribed.
3.3.11 Plants – Colchicum autumnale
Colchicum poisoning in a married coupleA 83-year-old woman and her 90-year-oldhusband were found dead in their flat. In thecouple's refrigerator, leaves of bear's garlic(Allium ursinum) and colchicum (120 and 170g, respectively) were found. When collectingthem in the vicinity of their home, the couplehad obviously accidentally mistaken thegreen leaves of colchicum for those of bear'sgarlic and had eaten both. Chemical-toxico-logical examinations revealed blood levels ofcolchicine in the lethal range.
Manifestations/courseFrom the report by the public prosecution of-fice, it was concluded that massive diarrhoeahad set in after the meal. No information was
available on other manifestations sincedeaths had probably occurred several daysago. Possibly, both partners died almost atthe same time. Inspection of the sites wheretheir bodies were found and external findingsdid not permit any conclusions as to thecause of death. From an objective point ofview, there were neither indications of vio-lence or trauma of any kind nor of a suicidalintent. Post-mortem findings included signs ofadvanced putrefaction of the bodies. Initially,the cause of death could not be clarified un-equivocally. Blood and urine as well as gastriccontents and parts of inner organs werestored and kept for further investigation.
Findings resulting from chemical-toxicologicalanalyses included: In the female corpse, thecolchicine levels detected in urine, in heartblood and in blood from the femoral vein were783, 98.3 and 78.4 ng/mL, respectively. In themale corpse, the colchicine levels detected inheart blood and blood from the femoral veinwere somewhat lower (36.6 and 22.7 ng/mL,respectively). This confirmed lethal poisoningby colchicine in both cases.
NotesThe popularity of bear's garlic tempts manypeople to pick the plant in the forest nearby.Again and again, collecting of the plant in thespring season, particularly in the month of May,has led to colchicum being mistaken for bear'sgarlic, resulting in tragic consequences. Theleaves of bear's garlic and colchicum sprout atthe same time of the year. Mistakes involving thelily of the valley (Convallaria majalis) are lessdangerous. The leaves of the three plants arequite similar in appearance. However, there aredistinguishing features that should be given at-tention. The relatively slim leaves of bear's garlichave stalks, being similar to the long and slimleaves of the lily of the valley. In contrast, theleaves of colchicum lack stalks. The smell of
Cases of Poisoning Reported by Physicians
44

bear's garlic is similar to that of garlic, butweaker, while the two other plants do not smellof garlic. But again, caution should be exer-cised when testing the smell: If bear's garlichas already been collected before, the smell ofits juice adhering to the fingers could suggest agarlic smell emanating from what is actuallycolchicum or lily of the valley.
All parts of the colchicum plant contain the cyto-toxic substance, colchicine, which is a mitoticpoison blocking cell division (capsule: 0.4–1.4%, flower: 0.8–1.8 %, leaves: < 0.2 %, bulb:0.08-0.2 %). The doses considered as potentiallylethal are 1–1.5 g seeds for children and 5 gseeds (1 g corresponds to ca. 200 seeds) or50–60 g leaves for adults. Administration ofcolchicine for medical purposes is indicated e.g.for treatment of acute attacks of gout. Accumu-lation in the leukocytes inhibits leukocyte migra-tion and thus, phagocytosis. This prevents thecrystallization of uric acid. Therapeutic doses donot result in an inhibition of mitosis. At toxic dos-es, mitosis inhibition will result in cell death andthus, multiple organ damage. Among the mostsensitive tissues are those with the highest celldivision rate such as intestinal epithelium, bonemarrow and hair follicle. Other effects includedisturbances of intracellular transport and mem-brane function resulting in an inhibition of the se-cretion of neurotransmitters, hormones, im-munoglobulins and collagen synthesis.
Toxicity is very high, with a potentially lethaldose in adults of ca. 7–8 mg (in individuals withrenal insufficiency, 3 mg only). However, alsocases of survival at higher doses have been de-scribed. In general, colchicine levels in the plas-ma of > 35 ng/mL and in urine of > 1,5 µg/mLare considered as lethal. As demonstrated bythe two cases of poisoning described above, al-so lower doses may obviously result in death.
Colchicine is readily absorbed. It is character-ized by a pronounced enterohepatic circulationand a high volume of distribution with accumu-
45
Fig. 16: Colchicum autumnale
Fig. 14: Bear's garlic
Fig. 15: Lily of the valley

lation on repeated intake. The typical clinicalpicture of poisoning is characterized by threestages:� After an initial symptom-free interval of 2-6-
14 hours, the gastrointestinal stage will bemost prominent with a sore and burning sen-sation in mouth and throat, vomiting, tenes-mus, watery and bloody diarrhoea, exsicco-sis and leukocytosis.
� Multiple organ damage will follow after 24–72hours. Manifestations will involve the nervoussystem resulting in disorientation, convulsi-ons, weakness of muscles, somnolence, so-por and coma. The cardiovascular systemwill develop hypotension, shock and arrhyth-mia. The respiratory tract will be affected,with tachypnoea, central respiratory depres-sion, respiratory arrest, pulmonary infiltrationand lung oedema. The gastrointestinal tractwill be involved with melanorrhoea and liverdysfunction. Acute renal failure may occur.The haematopoietic system will react withgranulocytopenia, thrombocytopenia andpancytopenia. The clinical picture may beco-me even more serious by metabolic disor-ders and changes of laboratory parametersassociated with metabolic acidosis, electroly-te disturbance and consumptive coagulopa-thy. This stage will persist for ca. one week. Inthe majority of cases, death occurs within 1–3 days due to toxic cardiovascular failure,acute pulmonary oedema, septicaemia orcerebral oedema.
� Patients who survive this stage will recoverfrom the seventh to tenths day onwards. Theconvalescent stage will be associated withloss of hair, mostly presenting as a completealopecia. In the course of illness, the pa-tient's condition may become affected by nu-merous other complications.
For treatment, decisive importance is attributedto primary detoxification, i.e. removal of the poi-son because there are almost no effectivemeans of secondary detoxification. So far, nocolchicine-specific Fab fragments are commer-
cially available. There have been no suggestionsof effective measures for secondary detoxifica-tion so far. This means that only symptomatictreatment can be performed.
Evaluation of the case described:In the two above cases with a tragic outcome,the relationship between ingestion of colchicumleaves and lethal outcome was confirmed bychemical-toxicological analysis.
3.3.12 Animals – Vipera berus
Poisonous snake biteDuring a holiday spent in Poland, an 8-year-old girl was bitten by a snake. When playingin the grass, the girl felt a brief and strongpain on her right hand and saw a brown-greysnake gliding away. The patient developed alife-threatening condition. She was admittedto the nearest hospital where she was admin-istered an antiserum. From there, she wastransferred to a major paediatric hospital inPoland and later, to a specialized hospital inGermany. It took one week for the child to re-cover.
Manifestations/courseWhen the mother and father had a close lookat their daughter's hand, they noticed not onlythe two punctures but also a ring formingaround the injury. They immediately went offto the hospital in the nearby town. Soon, thegirl began to suffer from strong pain, progres-sive swelling, nausea and headache. "Theswelling on her arm increased from minute tominute", reported her father. In spite of ad-ministration of an antiserum (unspecified anti-snake-bite serum), immobilization and coolingof the extremities, antibiotic shielding bymeans of amoxicillin, clavulanic acid andmetronidazole combined with antihistaminesand glucocorticoids as well as administrationof anti-tetanus prophylaxis, the patient's con-dition deteriorated. In the course of the day,
Cases of Poisoning Reported by Physicians
46

she developed persisting nausea and experi-enced repeated vomiting. The livid discol-oration and increasing swelling of her rightarm extended up to her shoulder. Findings in-cluded a slight arterial hypotension with asystolic blood pressure of 90 mmHg. Duringthe night, the patient was very restless andsuffered from states of panic. On the nextmorning, the local findings had deterioratedwith a blue-black discoloration of the patient'shand. The patient's general condition had de-teriorated to such a degree that she was al-most no longer able to sit up without support.As a consequence, she was transferred to amajor paediatric hospital in Poland. There, acentral venous catheter was attached to theleft femoral vein and the initial therapy contin-ued. On the following day, her general condi-tion stabilized and the swelling decreasedslightly. In the evening of that day, the girl wastransferred to the intensive care unit of a spe-cialized hospital in Germany by emergencyflight. There, clinical findings described thechild as being in a proper general condition,awake, responsive and cooperative. Findingsincluded a massive painful swelling and amarbled-livid discoloration of the entire rightarm and the right shoulder which had partlyextended to the right thoracic wall. The radialpulse was vigorously palpable. The status of her other organs was also found to be normal.
Laboratory examinations performed after twodays in the period of increasing swelling re-vealed thrombocytopenia of 33 000/nL (refer-ence ranges 150–350 (x103/µL), an Hb de-crease to 7.4 g/dL (reference range 12–16g/dL) without clear signs of haemolysis. Inaddition, findings included a CK increase to 3231 U/L (reference range for creatine kinase< 70 U/L) on the third day and an increase ofGPT to 162 U/L (reference range < 17 U/L).Resting electrocardiography revealed a bor-
derline PQ interval (0.17) and a QT intervalnear the normal upper limit (0.36).
The therapy which consisted of immobiliza-tion and cooling of the arm, administration ofantibiotics (for seven days) and of glucocorti-coids, as well as anaesthetic treatment by ad-ministration of metamizole and piritramidewere continued. Because of increasingswelling and extension into the shoulder andthorax regions and due to thrombocytopeniaand Hb decrease one day after admission ofthe patient to hospital, it was decided to ad-minister another dose of antiserum againstadder's poison which was well tolerated. Sub-sequently, the swelling subsided slowly, andthe livid discoloration faded. Also the labora-tory parameters returned to normal levels. Af-ter four days, the little patient was in a stablecondition and could be transferred to a pae-diatric hospital situated not far from her par-ent's place of residence. After physiothera-peutic treatment, the mobility of the little pa-tient's arm and her health were completely re-stored.
NotesThe only wildlife snakes living in Europe arethose of the family Viperidae. The respectivespecies are:
Vipera ammodytes (nosehorn viper, Westernsand viper) Vipera aspis (European asp, asp viper)Vipera berus (adder, common viper, commonadder, cross adder)Vipera lebetina (blunt-nosed viper, Levantineviper, Levant viper)Vipera latasti (Lataste's viper)Vipera ursinii (Orsini's viper, meadow viper)Vipera xanthina (Ottoman viper, coastal viper)
Based on the geographical assignment and theassignment with the help of pictures, the
47

species that had most probably been involvedin this case was the adder (Vipera berus). Acci-dents involving snake bites occur particularly of-ten between April and October. With regard tothe course of disease after snake bites, it is dif-ficult to make reliable statements because mani-festations will essentially depend on the quantityof snake poison entering the body. Since thecase described above occurred in May, thesnake had possibly accumulated a major quan-tity of poison after the hibernation period. A poi-
ing, vomiting and diarrhoea. Haemorrhages andcoagulopathy associated with bleeding andthrombosis will be the most prominent manifes-tations if vipers are involved; in the context of aconsumptive coagulopathy, the parameters ofbleeding and coagulation will exhibit pathologi-cal changes. Primarily, hypotension and shockwill result from increased capillary permeability,however, they may also result from blood lossassociated with consumptive coagulopathy.These conditions may, in turn, result in acute re-nal failure. Also damage to the heart and respi-ratory disturbances have been reported. As atherapy, the limb affected should be immobi-lized. Application of any kind of tourniquet mayresult in severe subsequent damage (necrosis)and therefore must not be performed. All othermeasures will be symptomatic. Antisera shouldbe administered in the event of a massive localreaction associated with considerable systemiceffects. The administration of antiserum in cas-es of adder bites has been questioned on thebasis of experience made in Sweden andSwitzerland. Physicians working in hospitalsconsider pre-testing to be unnecessary if theaction of the snake poison is rated as moredangerous than the risk of a possible anaphy-lactic adverse effect. Depending on the geo-graphic distribution of poisonous snakes, differ-ent types of antiserum are administered. The in-formation required has to be obtained from theresponsible regional poison control centres.
Evaluation of the case described:On the basis of the information given on thetemporal relationship between the exposure ofthe skin by bite and the occurrence of the mani-festations observed, and in the absence of oth-er causes, a causal relationship has been con-firmed. The degree of severity of the health im-pairment has been classified as moderate.
Cases of Poisoning Reported by Physicians
48
Fig. 17: Vipera berus
soning due to snake bite has to be consideredas a complex poisoning by neurotoxins andhaemotoxins, among others. In the majority ofcases, only local effects will be most prominent.Dangerous or lethal cases of poisoning havebeen observed rarely. In addition to local reac-tions such as bite marks associated with erythe-ma, oedema, pain, blue-red discoloration of theskin, haematoma, blistering, necrosis andswelling of lymph nodes, systemic reactionsmay occur. These include anxiety, dizziness, ver-tigo, headache, tachycardia, weakness, sweat-

4.1 Overview of reported cases of poisoning in the period of 1 January–31 December 2004
49
4 Annex
Incriminated products / uses Reports, total numbersHealth impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
a-dults
Home Work Total Chil-dren
a-dults
Home Work
I. Medicinal products 129 33 96 10 85 2 2 1 1
II. Veterinary medicinal products
9 7 7
III. Chemical products 3022 100 2922 17 2904 214 34 180 2 178
Wastes, solid 36 36 36 2 2 2
Waste gases 224 1 223 1 222 8 8 8
Sewage 18 18 18 5 5 5
Paints and related materials 255 1 254 1 253 14 14 14
Paint removers / strippers 9 9 1 8
Alkyd resin paints
Emulsion paints 2 2 2 1 1 1
Artistís pai nting materials 1 1 1
Lacquers / varnishes 53 53 53 1 1 1
Parquetry sealers 1 1 1
Pigments 1 1 1
Primers 10 10 10 5
Paint thinners 114 1 113 113 5 5 5
Fire lighting products 9 9 7
Building materials, auxiliary products
26 26 26 2 2 2
Building materials 160 160 160 25 25 25
Fuels, liquid 96 56 40 40 30 26 4 4
Petrol 26 26 26 3 3 3
Ethanol for technical use 6 6 6
Lamp oil 56 56 26 26
Fuels, gaseous 2 2 2
Offi ce materials, chemical 32 32 32 8 8 8
Decoration materials
Dental materials 37 37 1 36 1 1 1
Disinfectants/sterilizers 393 393 393 8 8 8
Deodorants for technical use 5 2 3 3Diagnostics/reagents 2 2 2
Table 11: 5 530 reports vs. degree of severity of health disturbances, classified by children and adults, with the adult cas-es differentiated by exposures in the private sphere and in working environments (except for those with a degree of prob-ability of "no relationship").

Cases of Poisoning Reported by Physicians
50
Incriminated products / uses Reports, total numbers Health impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
a-dults
Home Work Total Chil-dren
a-dults
Home Work
Printing, auxiliary products 4 4 4
Insulating materials for electric equipment
De-icing products
Fire extinguishing media 21 21 21
Fire retardants
Galvanic cells 116 4 112 112 6 6 6
Dry cells 15 2 13 13 1 1 1
Button batteries 2 2
Accumulators 100 100 100 6 6
Galvanizing agents 3 3 3
Galvanizing agents, auxiliary products
3 3 3 2 2 2
Gases for technical use 2 2 2
Antifreezes 1 1 1
Glass-working, auxiliary products
3 3 3 1 1 1
Rubber, production materials 2 2 2
Semiconductors, production materials
Household auxiliary pro-ducts, chemical-technical
Hydraulic fl uids 37 37 37
Refrigerants 12 12 12 1 1 1
Ceramics, auxiliary products 2 2 2
Ceramic materials 1 1 1
Glues 121 1 120 5 115 3 3 3
Coolants 23 23 23 1 1 1
Plastics, starting materials 24 24 24 4 4 4
Plastics, formulating materials
4 4 4 2 2 2
Leather processing products 2 2 2
Luminophors 3 3 3
Solvents for technical use 65 65 1 63 2 2 2
Soldering and welding pro-ducts (except welding fumes)
6 6 6
Measuring equipment, chemical-technical
8 1 7 7
Heating meters 1 1

51
Incriminated products / uses Reports, total numbers Health impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
a-dults
Home Work Total Chil-dren
a-dults
Home Work
Mercury thermometers 1 1 1
Thermometer fl uids 4 4 4
Metallurgy, auxiliary products 30 30 1 29 4 4 1 3
Dairy, auxiliary products
Papermaking, auxiliary products
Photography, auxiliary products
5 5 5
Cleaning products 920 22 898 7 891 60 1 59 1 58
Drain cleanser 18 1 17 1 16 3 3 3
All-purpose cleaners 55 55 55
Oven and grill cleaners 36 36 36 2 2 2
Electronics cleaners
Descaling products 35 4 31 1 30
Front wall and stone cleaners
4 4 4 1 1
Stain removers 4 1 3 3 1
Floor polishes 4 1 3 3 1 1 1
Dishwashing products, manual
8 1 7 7
Dishwashing products, machine
20 3 17 17
Dishwasher cleaners 12 12 12 1 1 1
Glass cleaners 2 2 2
Industrial cleaners 65 65 65 6 6 6
Rinsing additives for dishwashers
6 6 6
Plastic cleaners 4 4 4
Lacquer cleaners
Milking machine cleaners 29 29 29 5 5 5
Metal cleaners 22 22 5 5 5
Furniture polishers 2 2 1 1
Soot removers
Lavatory cleaners 30 2 28 28
Shoe and leather cleaners 1 1 1
Carpet/upholstery cleaners
Detergents 17 2 15 15 1 1 1

Cases of Poisoning Reported by Physicians
52
Incriminated products / uses Reports, total numbers Health impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
a-dults
Home Work Total Chil-dren
a-dults
Home Work
Detergents, auxiliary products
6 1 5 2 3 1 1 1
Joke articles 1 1
Lubricants 27 27 27 2 2 2
Welding fumes 57 57 57 2 2 2
Dust-laying oils 1 1 1
Toys
Textile, auxiliary products 2 2 2
Propellants/sprays 3 3 3
Water treatment products 5 5 5
Pet shop products 1 1 1
IV. Cosmetics / personal hygiene products
75 7 68 15 52 4 4 3 1
Hair care products 21 1 20 2 18 1 1 1
Permanent wave products 7 7 7
Depilatory agents 1 1 1
Dyes / colorants 8 8 1 7 1 1 1
Conditioners 3 3 3
Hair tonics
Shampoos 1 1
Skin care products 44 4 40 10 29 2 2 1 1
Bath oils/ salts 5 1 4 4
Tanning products
Creams / ointments 14 2 12 9 3 1 1 1
Deodorants 4 4 4
Cleansers 1 1
Make-up 1 1 1
Oils
Perfumes / after shaves 2 2 2
Powders
Soaps 15 15 1 14 1 1 1
Sun blockers
Dental products 4 4 1 3
Nail care products 4 1 3 1 2 1 1 1
V. Pesticides 97 2 95 5 90 5 5 2 3
Acaricides
Fungicides 11 11 1 10 1 1 1
Herbicides 20 20 20 1 1 1Wood preservatives; 4 4 1 3 2

53
Incriminated products / uses Reports, total numbers Health impairmentmoderate/severe
First levelSecond level
Third level
Total Chil-dren
a-dults
Home Work Total Chil-dren
a-dults
Home Work
Insecticides 28 1 27 3 24 4 4 2
Carbamates 1 1 1
Chlorinated hydrocarbons 1 1 1
Phosphoric esters 6 6 2 4 3 3 2 1
Pyrethroids 2 1 1 1
Molluscicides
Repellents 1 1 1
Rodenticides 3 1 2 2
Anti-coagulants
Phosphates
Seed dressings
VI. Agrochemicals (other than pesticides)
10 22 22 2 2
Fertilizers 10 10 1 1 1
Growth regulators
VII. Substances of abuse
VIII. Plants 19 11 8 3 5 2 2 2
IX. Fungi 3 3 1 2
X. Animals 4 1 3 3 2 1 1 1
XI. Foods and beverages 86 5 78 41 36 15 1 11 8 3
Alcoholic beverages 16 16 1 15 2 2 1 1
Food additives 2 2 2
Tobacco and tobacco products
3 1 2 1
Food supplements 33 2 29 29 7 1 4 4
XII. Warfare/anti-riot agents 4 4 4
Pyrotechnic products
Tear gas 1 1 1
XIII. Miscellaneous 106 1 104 1 103 4 1 3 3
Textiles 38 38 38
Clothing 36 36 36
Furnishing fabrics 60
XIV. Basic elements 1981 3 1977 19 1955 177 2 10 164XV. Industrial accidents 60 60 60
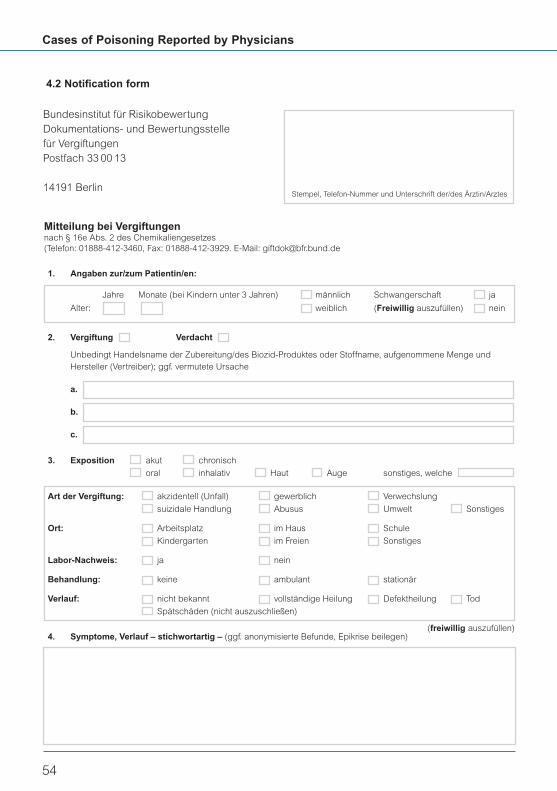
Cases of Poisoning Reported by Physicians
54
Bundesinstitut für RisikobewertungDokumentations- und Bewertungsstellefür VergiftungenPostfach 33 00 13
14191 BerlinStempel, Telefon-Nummer und Unterschrift der/des Ärztin/Arztes
Mitteilung bei Vergiftungennach § 16e Abs. 2 des Chemikaliengesetzes(Telefon: 01888-412-3460, Fax: 01888-412-3929. E-Mail: [email protected]
1. Angaben zur/zum Patientin/en:
Jahre Monate (bei Kindern unter 3 Jahren) männlich Schwangerschaft ja
Alter: weiblich (Freiwillig auszufüllen) nein
2. Vergiftung Verdacht
Unbedingt Handelsname der Zubereitung/des Biozid-Produktes oder Stoffname, aufgenommene Menge und Hersteller (Vertreiber); ggf. vermutete Ursache
a.
b.
c.
3. Exposition akut chronisch
oral inhalativ Haut Auge sonstiges, welche
Art der Vergiftung: akzidentell (Unfall) gewerblich Verwechslung
suizidale Handlung Abusus Umwelt Sonstiges
Ort: Arbeitsplatz im Haus Schule
Kindergarten im Freien Sonstiges
Labor-Nachweis: ja nein
Behandlung: keine ambulant stationär
Verlauf: nicht bekannt vollständige Heilung Defektheilung Tod
Spätschäden (nicht auszuschließen)
4. Symptome, Verlauf – stichwortartig – (ggf. anonymisierte Befunde, Epikrise beilegen)(freiwillig auszufüllen)
4.2 Notification form

55
Berlin BBGes – Giftnotruf Berlin Oranienburger D-13437 Phone: +49-30-19240
Institut für Toxikologie Str. 285 Berlin Fax: +49-0-30 68 6721
Klinische Toxikologie und [email protected]
Giftnotruf Berlin www.giftnotruf.de
Berlin Charité – Universitätsmedizin Berlin Augustenburger D-13353 Phone: +49-30-450 65 35 55
Campus Virchow Klinikum Platz 1 Berlin Fax: +49-30-450 55 3915
Klinik für Nephrologie und [email protected]
internistische Intensivmedizin, www.charite.de/rv/nephro
Giftinformation
Bonn Informationszentrale gegen Adenauerallee D-53113 Phone: +49-2 28-19240
Vergiftungen 119 Bonn Fax: +49-2 28-2 873314
Zentrum für Kinderheilkunde [email protected]
Universitätsklinikum Bonn www.meb.uni-bonn.de/
giftzentrale
Erfurt Gemeinsames Nordhäuser Str. D-99089 Phone: +49-3 61-73 0730
Giftinformationszentrum der Länder 74 Erfurt Fax: +49-3 61-7307317
Mecklenburg-Vorpommern, [email protected]
Sachsen, Sachsen-Anhalt und www.ggiz-erfurt.de
Thüringen
Freiburg Zentrum für Kinderheilkunde und Mathildenstr. 1 D-79106 Phone: +49-761-19240
Jugendmedizin Freiburg Fax: +49-761-270 44 57
Vergiftungs-Informations-Zentrale [email protected]
www.giftberatung.de
Göttingen Giftinformationszentrum-Nord der Robert Koch-Str. D-37075 Phone: +49-5 51-19240
Länder Bremen, Hamburg, 40 Göttingen Fax: +49-5 51-3 8318 81
Niedersachsen und Schleswig- [email protected]
Holstein (GIZ-Nord) www.Giz-Nord.de
Universität Göttingen –
Bereich Humanmedizin
Homburg Informations- und Beratungszentrum D-66421 Phone: +49-68 41-192 40
für Vergiftungsfälle Homburg/ +49-6841-1628314
Klinik für Kinder- und Jugendmedizin Saar Fax: +49-6841-1628438
www.uniklinikum-saarland.de/de/
einrichtungen/andere/giftzentrale
4.3 List of Poison Control Centres

Cases of Poisoning Reported by Physicians
56
Mainz Klinische Toxikologie und Langenbeckstr. D-55131 Phone: +49-6131-192 40
Beratungsstelle bei Vergiftungen der 1 Mainz +49-6131-23 24 66
Länder Rheinland-Pfalz und Hessen Fax: +49-6131-23 24 69
Universitätsklinikum +49-6131-1766 05
www.giftinfo.uni-mainz.de
München Giftnotruf München Ismaninger Str. D-81675 Phone: +49-89-192 40
Toxikologische Abteilung der II. 22 München [email protected]
Medizinischen Klinik und Poliklinik, www.toxinfo.org
rechts der Isar der Technischen
Universität München
Nürnberg Giftnotrufzentrale Nürnberg Prof.-Ernst- D-90419 Phone: +49-911-398 2665
Medizinische Klinik 2, Nathan-Str. 1 Nürnberg Phone: +49-911-398 2192
Klinikum Nürnberg muehlberg@
Lehrstuhl Innere klinikum-nuernberg.de
Medizin-Gerontologie, www.giftinformation.de
Universität Erlangen-Nürnberg Giftnotruf: +49-911-3 98 24 51
oder +49-911-3 98 26 65

57
4.4 Press releases on toxicological problemsissued by the BfR in 2004
Tattoos and permanent make-up are not without riskThe colours used for this purpose have notbeen tested03/2004, 10 April 2004
Two new child fatalities caused by lamp oils!BfR in favour of extending its ban on sale toclear and non-perfumed products07/2004, 14 July 2004
Enjoyment with unpleasant consequences
Skin reactions may occur after eating shiitakemushrooms10/2004, 19 August 2004
Exercise caution when handling ScoubidoubandsVolatile organic solvents, critical plasticisers and other problematic substances detected12/2004, 28 September 2004

Tel. +49-30 - 84 12 -0Fax +49-30 - 84 12 [email protected]
Federal Institute for Risk AssessmentThielallee 88-92D-14195 Berlinwww.bfr.bund.de