cases from the clinic
TRANSCRIPT
The UC San Diego AntiViral Research Center sponsors weekly presentations by infectious disease clinicians, physicians and researchers. The goal of these presentations is to provide the most current research, clinical practices and trends in HIV, HBV, HCV, TB and other infectious diseases of global significance. The slides from the AIDS Clinical Rounds presentation that you are about to view are intended for the educational purposes of our audience. They may not be used for other purposes without the presenter’s express permission.
AIDS CLINICAL ROUNDS
Cases%from%the%Clinic%
Darcy%Wooten,%MD,%MS%Health%Sciences%Assistant%Clinical%Professor%
Owen%Clinic%Infec<ous%Diseases%Hospital%Medicine%
%
Financial%disclosures:%None%%Conflicts%of%interest:%None%

HPI%36%yo%man%with%no%PMH%
• %2%weeks%prior,%presented%to%public%health%with%urethral%discharge%%
• %Diagnosed%with%nonJgonococcal%urethri<s%(by%a%“urine%test,”%denied%having%throat/rectal%tes<ng)%and%new%HIV%
• %Treated%with%azithromycin%1g%PO%x1%dose%
• %Referred%to%Owen%Clinic%for%further%care%
• %1%week%prior%to%his%Owen%Clinic%appointment,%reJpresented%to%public%health%with%ongoing%urethral%discharge%and%treated%with%7%days%of%doxycycline%100mg%bid%
Owen%Clinic%Visit%(#1)%At%his%first%Owen%Clinic%visit%(2%weeks%a[er%his%ini<al%symptoms):%
• %Unchanged%urethral%discharge%(thin,%watery,%morning)%
• %Mild%urinary%urgency,%but%NO:%dysuria,%burning,%frequency,%hesitancy,%dribbling,%hematuria%
• %No%tes<cular%pain%or%swelling,%genital%ulcers,%rectal/perirectal%pain,%pelvic%floor%pain,%inguinal%pain%
• %No%abdominal%pain,%nausea,%vomi<ng,%diarrhea,%cons<pa<on,%back%pain,%rash,%eye%symptoms,%or%joint%pain%
• %No%fevers,%chills,%sweats%%
Addi<onal%History%Social%History:%• %%No%tobacco%
• %6%glasses%wine/week%
• %MJ%q%2%weeks;%IN%cocaine%x1,%ecstasy%x2,%no%other%drugs,%no%IVDU%
• %Born%in%San%Diego,%lives%alone%
• %Works%in%So[ware%R&D%
• %No%travel%or%pets%%%
PMH:%• %Per%HPI%
Meds:%• %Azithro%+%Doxy%per%HPI%• %100%%adherent%
%All:%• %NKDA%%%Family%History:%• %Hypertension%

Sexual%History%%• %Sex%with%men%(inser<ve%and%recep<ve%oral%and%anal%sex)%%• %Used%condoms%with%anal%sex,%but%only%during%ejacula<on%%• %No%associated%alcohol%and%substance%use%during%sex%%• %3%partners%in%the%past%3%months%%• %~10J15%life<me%partners,%unknown%HIV/STI%status%of%partners%%• %No%history%of%symptoma<c%STIs%%
• %No%new%partners%since%HIV%diagnosis%
Exam%Normal%vitals%%HEENT:%Sclera%anicteric%and%not%injected,%OP%clear%without%erythema%or%exudates,%no%thrush,%no%LAD%%Cardiac,%Pulm:%Normal%%Abdomen:%So[,%NT,%ND,%+BS,%no%HSM,%no%CVA%tenderness%%GU:%Circumcised,%no%penile%lesions/ulcer,%normal%meatus%without%discharge,%normal%testes,%normal%perirectal%exam,%DRE%normal%without%tenderness,%and%mild,%nonJtender,%mobile%inguinal%LAD%%Skin:%No%rash%%Neuro:%Normal%%
Owen%Clinic:%Plan%• %Ordered%a%UA,%urine%culture,%urine/throat/rectal%GC/CT%PCR,%and%syphilis%EIA%
• %Requested%outside%records%
• %“ReJtreated”%with%Ce[riaxone%250mg%IM%x1%+%Azithro%1g%PO%x1%
• %Ini<al%“HIV%labs”%(CD4,%viral%load,%genotype,%CBC,%CMP,%lipids,%hepa<<s%serologies,%QFN,%HLA%B5701)%
• %Discussed%ARV%op<ons%
• %Follow%up%in%2%weeks%to%start%ART%and%reassess%symptoms%
2%Weeks%Later…%• %Returns%for%follow%up%with%no%change%in%urethral%discharge%• %Improved%for%~1J2%days%a[er%an<bio<cs%but%then%returned%to%baseline%symptoms%
• %No%new%symptoms%or%exam%findings%• %No%new%sexual%partners%since%HIV%diagnosis%
2%Weeks%Later…%• %Returns%for%follow%up%with%no%change%in%urethral%discharge%• %Improved%for%~1J2%days%a[er%an<bio<cs%but%then%returned%to%baseline%symptoms%
%• %No%new%symptoms%or%exam%findings%• %No%new%sexual%partners%since%HIV%diagnosis%
• %WBC:%5.1% % % % %CD4:%375%(29%) %HIV%VL:%10K,%WT%• %Hgb:%15.5% % % % %GC/CT%PCR%x3:%Neg%• %Plt:%196 % % % % %UA:%Normal,%UCx:%Neg%
• %Chem%panel:%Normal% %Hep%A+B:%Immune,%HCV%Ab:%Neg%• %LFTs:%Normal% % % %Syphilis%EIA:%Neg%%%%%%%QFN:%Neg%
Audience%Response%Ques<on%What%would%your%next%steps%in%management%be%for%this%young,%HIV+%man%with%ongoing%urethri<s%despite%mul<ple%rounds%of%an<bio<c%therapy?%%A. Repeat%treatment%with%ce[riaxone%and%azithromycin%B. Repeat%treatment%with%azithromycin%1g%PO%x1%C. Repeat%treatment%with%azithromycin%1.5g%PO%over%5%days%
(500mg%on%day%1%!%250mg%daily%on%days%2J5)%D. Repeat%treatment%with%moxifloxacin%for%7J14%days%E. Admit%to%the%hospital%and%retreat%with%broadJspectrum%IV%
an<bio<cs%%%%
Owen%Clinic%Visit%(#2)%• %Sent%urine%for%Urogenital%Ureaplasma%and%Mycoplasma%spp.%PCR%(sendout%to%ARUP)%
• %Treated%with%Moxifloxacin%400mg%PO%daily%x7%days%
• %Started%Stribild%
• %1%week%later:%symptoms%resolved%with%Moxifloxacin%
%
4%Weeks%Later…%%• %ARUP%report:%
• %Ureaplasma-parvum%PCR:%Not%detected%• %Ureaplasma-urealy0cum-PCR:%Not%detected%• %Mycoplasma-hominis-PCR:%Not%detected%• %Mycoplasma-genitalium-PCR:%Detected%
Mycoplasma-genitalium:%%Emerging%Pathogen%

Causes%of%nonJgonococcal%urethri<s%%• %NonJgonococcal%urethri<s%(NGU)%• -Chlamydia-trachoma0s%(25%%of%cases)-
• %Mycoplasma-genitalium%(30%%of%cases)-
• %Trichomonas-vaginalis%(10J25%%of%cases)%
• -Ureaplasma-urealy0cum%(controversial)%
• -HSV-
%
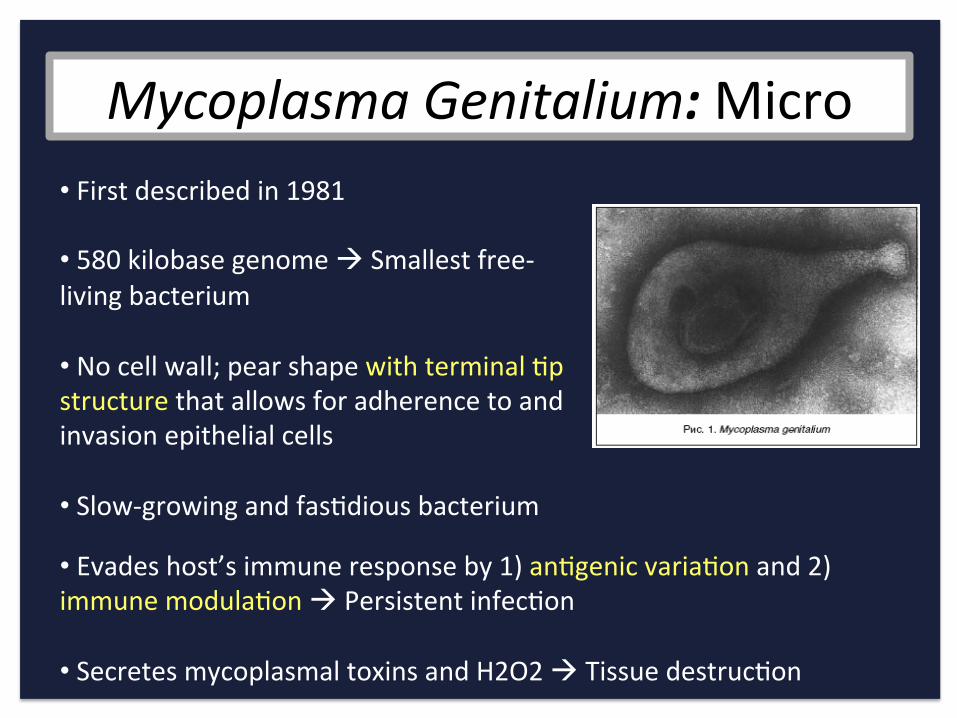
Mycoplasma-Genitalium:"Micro-• %First%described%in%1981%
• %580%kilobase%genome%!%Smallest%freeJliving%bacterium%
• %No%cell%wall;%pear%shape%with%terminal%<p%structure%that%allows%for%adherence%to%and%invasion%epithelial%cells%
• %SlowJgrowing%and%fas<dious%bacterium%%• %Evades%host’s%immune%response%by%1)%an<genic%varia<on%and%2)%immune%modula<on%!%Persistent%infec<on%
• %Secretes%mycoplasmal%toxins%and%H2O2%!%Tissue%destruc<on%
Mycoplasma-Genitalium:%Epi-• %Risk%Factors:%
• %Higher%number%of%sex%partners%• %Younger%age%during%first%intercourse%• %Partner%with%ac<ve%STI%symptoms%• %CoJinfec<on%with%other%STIs%• %Smoking%• %HIV%coJinfec<on%%%%• %Strongest%associa<on%with%nonJgonococcal%urethri<s%in%men%• %Weaker%associa<on%with%cervici<s%and%PID%(conflic<ng%studies)%
Mycoplasma-Genitalium:%Dx-%• %Consider%in%cases%of%NGU%or%cases%of%persistent%urethri<s%despite%therapy%%• %No%FDAJcleared%tests%(NAAT%as%a%sendout%is%available)%
• %NAATs%target%78%bp%region%of%the%adhesion%protein%and%a%517%bp%region%of%the%16S%rRNA%• %Op<mal%specimen%is%unclear%(first%void%urine%in%men,%vaginal%specimen%in%women)%
%

Mycoplasma-Genitalium:%Tx-Doxycycline%%Azithromycin%%Moxifloxacin%

Mycoplasma-Genitalium:%Tx-Doxycycline%• %In-vitro-data%suggests%M.-genitalium-would%be%suscep<ble%
• %Controlled%clinical%trials%show%efficacy%ranging%between%22J45%%
• %Discrepancy%is%unclear%
• %Not%recommended%for%therapy%

Mycoplasma-Genitalium:%Tx-Azithromycin%• %Good%in-vitro-ac<vity%
• %Efficacy%of%Azithromycin%1g%dose%appears%to%be%declining%• %87%%cure%rates%prior%to%2005%vs%71%%a[er%2005%• %85%%cure%rates%prior%to%2009%vs%67%%a[er%2009%
• %Explana<ons:%• %Increase%in%AzithroJresistance%• %Organism%load%

Mycoplasma-Genitalium:%Tx-
Would%an%extended%dose%of%azithromycin%be%more%efficacious%and/or%lead%to%less%resistance?%
%1g%vs%1.5%g%(500mg%x1%+%250mg%x4)%
%%
• %Controlled%trial%1g%vs%1.5g,%efficacy%was%85%%vs%95%%• %Pa<ent%treated%with%1.5g%dose%had%previously%failed%treatment%with%doxy%
Mycoplasma-Genitalium:%Tx-Moxifloxacin%%• %Cipro,%Levo,%and%Ofloxacin%all%have%poor%in-vitro-ac<vity%against%M.-genitalium-as%well%as%poor%clinical%efficacy%
• %Ini<al%cure%rates%with%moxifloxacin%amongst%pa<ents%with%prior%treatment%failure%were%as%high%as%100%%
• %In%Asia,%treatment%failure%is%as%high%as%15J30%%and%is%associated%with%FQ%resistance%
Take%Home%Points%• %Think%about%Mycoplasma-genitalium,%especially%in%pa<ents%with%persistent%urethri<s%
• %ARUP%has%a%panel%which%tests%for:%%
%• %Order%as%“Urine%Lab%Misc.”%and%type%in%“Urogenital%Ureaplasma%and%Mycoplasma%spp.%PCR”%%
• %Treatment%is%challenging%because%of%resistance%• %Azithro%1.5g%or%Moxifloxacin%
%
Ureaplasma-parvum%PCR%Ureaplasma-urealy0cum-PC%Mycoplasma-hominis-PCR%Mycoplasma-genitalium-PCR%

HPI%CC:%Rash%%HPI:%• %31%yo%woman%with%newly%diagnosed%HIV%(CD4%385,%VL%4.5%million)%and%drugJresistant%TB%in%November,%2014%at%Sharp.%%%• %Miliary%pulmonary%disease,%+pleural%effusion,%bone%marrow%biopsy%with%nonJcasea<ng%granulomas.%%
• %11/26/14:%Sputum%AFB%smear%neg,%Cx:%+MTB,%+MTD%PCR%• %11/26/14:%Pleural%fluid%AFB%Smear%neg,%Cx:%+MTB,%+MTD%PCR%• %12/6/14:%Sputum%AFB%smear%neg,%Cx:%+MTB%• %12/7/14:%Sputum%AFB%smear%neg,%Cx:%+MTB%• %Low%level%resistance%to%INH%and%Ethionamide%%
• %Rifabu<n,%Ethambutol,%Pyrazinamide%12/6%–%12/24%

HPI%(cont.)%%• %Absconded%on%12/24/14%
• %%Found%crossing%the%border%from%Mexico%in%June,%2015%
• %%Admiwed%to%Sharp%and%reJstarted%on%Rifabu<n,%Ethambutol,%and%Pyrazinamide%
• %Repeat%sputum%AFB%smears%neg,%cultures%were%posi<ve%for%MTB%%
HPI%(cont.)%%• %Drug%Suscep<bility%Report%(BACTEC%MGIT%960)%• %Isoniazid%0.1%ug/mL:%Resistant%• %Isoniazid%0.4%ug/mL:%Sensi<ve%• %Pyrazinamide%100%ug/mL:%Sensi<ve%• %Ethambutol%5%ug/mL:%Sensi<ve%• %Ethionamide%5.0%ug/mL:%Resistant%• %Capreomycin%3.0%ug/mL:%Sensi<ve%• %Amikacin%1.5%ug/mL:%Sensi<ve%• %Moxifloxacin%0.25%ug/mL:%Sensi<ve%
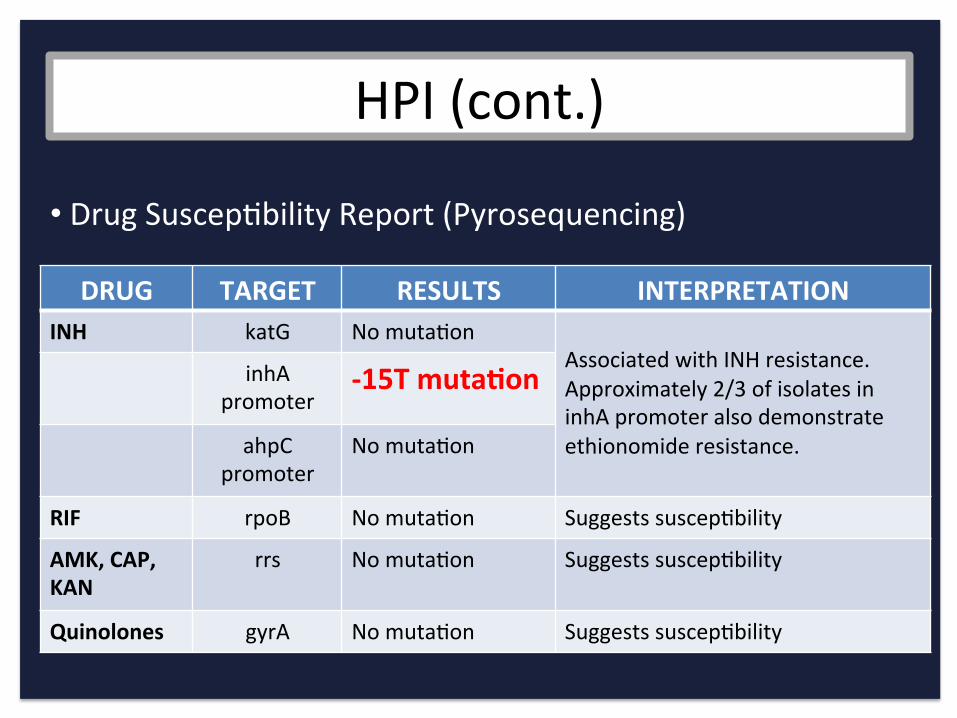
HPI%(cont.)%%• %Drug%Suscep<bility%Report%(Pyrosequencing)%
DRUG% TARGET% RESULTS% INTERPRETATION%INH% katG% No%muta<on% %
Associated%with%INH%resistance.%%Approximately%2/3%of%isolates%in%inhA%promoter%also%demonstrate%ethionomide%resistance.%
inhA%promoter%
015T%muta7on%
ahpC%promoter%
No%muta<on%
RIF% rpoB% No%muta<on% Suggests%suscep<bility%
AMK,%CAP,%KAN%
rrs% No%muta<on% Suggests%suscep<bility%
Quinolones% gyrA% No%muta<on% Suggests%suscep<bility%%
INH%Resistance%%• %Mechanism%of%INH%vs.%TB%
• %Inhibits%mycolic%acid%synthesis%• %INH%is%ac<vated%by%mycobacterial%catalase%and%then%binds%to%inhA%protein%(involved%in%the%synthesis%of%mycolic%acid)%!%Inhibi<on%of%cell%wall%synthesis%%
• %Muta<ons%in%the%katG%and/or%inhA%genes%account%for%85J90%%of%INH%resistance%
• %Low%level%resistance%=%MIC%>0.1%but%%<1.0%ug/mL%(point%muta<ons)%• %High%level%resistance%=%MIC%>1.0%ug/mL%(major%dele<ons)%
• %7J11%%of%pa<ents%with%TB%in%the%U.S.%have%INH%resistance%
• %Ethionamide%is%an%isonico<nic%acid%deriva<ve%(similar%to%INH)%• %Muta<ons%in%the%inhA%gene%are%also%associated%with%ethionamide%resistance,%but%not%muta<ons%in%the%katG%gene%
HPI%(cont.)%• 3%weeks%into%therapy%she%developed%a%rash%and%her%TB%therapy%was%
stopped.%
• TB%therapy%reJintroduced%one%drug%at%a%<me;%developed%a%rash%with%rifabu<n%
%• TB%therapy%stopped%again%%• Desensi<za<on%to%rifabu<n%%• TB%therapy%reJini<ated%and%developed%a%rash%to%rifabu<n%again%%• TB%therapy%change%to%rifampin/EMB/PZA%without%development%of%
rash%
HPI%(cont.)%• Rifampin/EMB/PZA%con<nued%for%4%weeks%without%
development%of%rash%• Efavirnez/Truvada%started%• Discharged%to%SNF%
• 2%weeks%later,%presents%to%Owen%Clinic%with%4%days%of:%• Diffuse,%pruri<c,%and%burning%rash%on%bilateral%upper%extremi<es,%
then%lower%extremi<es,%then%torso%and%back%• Started%a%red%papules%that%then%coalesced%into%plaques%• Bilateral%lower%extremity%edema%(painful)%• Large,%tender,%right%cervical%lymph%node%• Fevers%to%102,%tachycardic%to%130%
%

PMH%
• %HIV%(CD4%351,%VL%10%million,%treatmentJnaïve)%• %Disseminated,%drugJresistant%TB%• %Syphilis%(late%latent,%RPR%1:4,%never%treated)%• %Genital%HSV%• %Schizophrenia/ADHD/Bipolar%disorder/Developmental%delay%• %Tobacco%use%• %Methamphetamine%use%• %Severe%calorie%and%protein%malnutri<on%• %s/p%2%CJsec<ons%%

MEDS%• Efavirenz%800mg%daily%(stopped%2%days%ago)%• Truvada%1%tab%daily%(stopped%2%days%ago)%
• Rifampin%600mg%daily%(stopped%2%days%ago)%• Ethambutol%800mg%daily%(stopped%2%days%ago)%• Pyrazinamide%1000mg%daily%(stopped%2%days%ago)%
• Ce<rizine%10mg%daily%• Hydroxyzine%0.25mg%q%6%
• Olanzapine%5mg%q%am,%10mg%q%pm%
• Nysta<n%S+S%
• Tylenol,%Norco,%Zofran,%Nico<ne%patch,%Metoprolol,%Levothyroxine,%Ferrous%sulfate%
%

Addi<onal%History%
SH:%• ½%ppd%tobacco%• No%alcohol%• Methamphetamine%use%• WSM,%likely%contracted%HIV%through%exJboyfriend%• Previously%worked%as%a%pros<tute%in%TJ%• Originally%from%Texas%
FH:%• Unknown%
Allergies:%• Bactrim%!%Rash%• Rifabu<n%!%Rash%

Exam%%VS:%100.3 %%93/52 % %111 % %19 % %97%%RA%%%GEN:%Cachec<c,%mildly%ill%appearing%HEENT:%Sclera%anicteric,%injected%L%conjunc<va,%PERRL,%MMM,%no%thrush%NODES:%Firm,%tender%3x3%cm%supraclavicular%lymph%node%CHEST:%CTAB%HEART:%Tachy%but%regular,%no%murmurs%ABDOMEN:%So[,%tender%to%palpa<on%in%RUQ%with%hepatomegaly%and%splenomegaly,%no%R/G%EXT:%1+%edema%in%bilateral%lower%extremi<es%SKIN:%Diffuse%blanching,%erythematous%papular%confluent%rash%on%bilateral%UE,%LE,%torso,%worse%on%the%le[%v%right%sparing%face,%palms,%and%soles%NEURO:%A+Ox3,%CN%intact,%normal%gait%
%




Audience%Response%Ques<on%In%this%young%woman%with%HIV%and%drugJresistant%TB,%with%a%history%of%rash%to%Bactrim%and%Rifabu<n,%a%history%of%syphilis,%and%recently%on%Rifampin/Ethambutol/Pyrazinamide%x7%weeks%and%efavirenz/tenofovir/emtrici<bine%x%2%weeks,%which%of%the%following%is%the%MOST%likely%cause%of%her%rash?%%A. Rifampin%B. Ethambutol%C. Pyrazinamide%D. Efavirnez%E. Olanzapine%F. Undiagnosed%vasculi<s%G. Syphilis%(it’s%always%syphilis)%

Clinical%Course%%• %Admiwed%to%the%hospital%
• %All%TB%and%HIV%meds%held%
• %Labs%and%imaging%
• %Dermatology%consult%

Labs%%• %WBC:%4.1%(65%%segs/%25%%lymphs/%7%%%mono/%4%%eos)%• %Hgb:%9.6%• %Plt:%199%
• %Cr:%0.44 % %LDH:%159%
• %LFTs:%Normal%(0.21%/%19%/%17%/%117)%
• %UA:%>50%WBCs,%+LE,%neg%Ni,%2+%protein%
• %Syphilis%EIA+,%RPR%1:4%
• %Hep%A,%B,%C:%Neg%
Labs%%• %Blood%cultures:%Neg%
• %AFB%blood%culture:%NGTD%
• %Sputum%AFB%smear/Cx%x3:%Neg/NGTD%
• %Sputum%MTD%PCR:%Neg%
• %Stool%AFB%smear/Cx:%NGTD%%• %Serum%CrAg:%Neg,%Serum%Cocci:%Neg,%Urine%Histo%Ag:%Neg%
• %uCG/CT:%Neg%

CT%Neck%
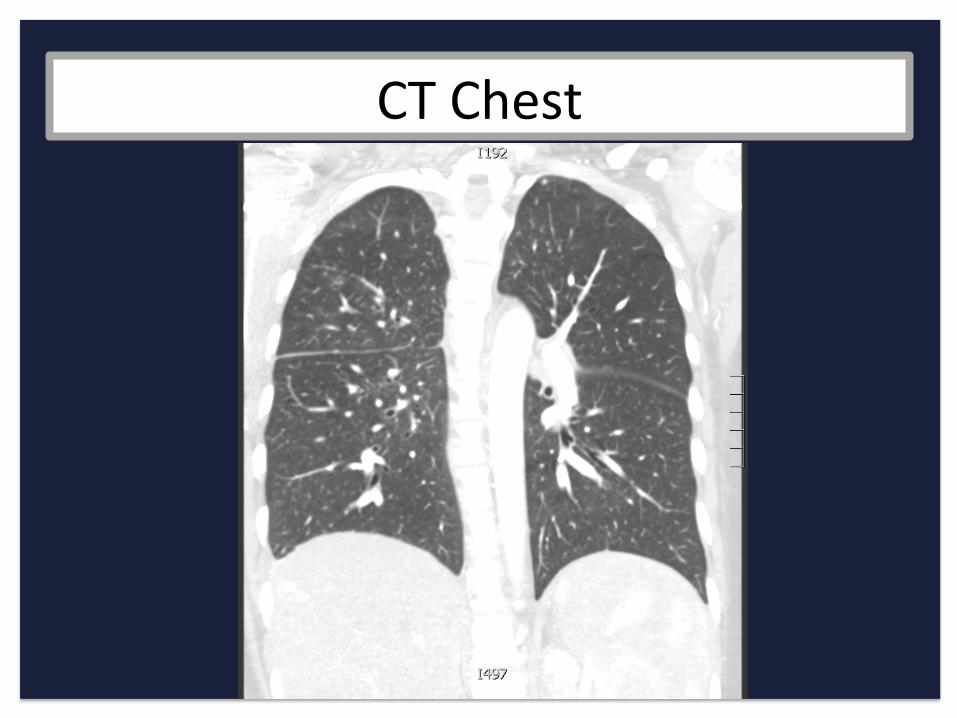
CT%Chest%

CT%Abdomen/Pelvis%
Dermatology%Consult%%• %Exanthematous%drug%reac<on%
• %Not%clinically%consistent%with%DRESS%or%SJS/TEN%
• %No%biopsy%
Clinical%Course%%• %Rash%resolved%a[er%several%days%off%all%TB%and%HIV%meds%
• %FNA%of%cervical%lymph%node:%• %Path:%Necro<zing%granulomatous%inflamma<on%• %Unable%to%perform%GMS%and%AFB%stains%• %Micro:%AFB%smear%and%culture%nega<ve%
• %Plan%was%made%to%reJintroduce%TB%medica<ons%in%a%stepwise%fashion%and%hold%ARVs%un<l%she%was%able%to%tolerate%2%weeks%of%TB%therapy%

Drug%Rashes%in%Pa<ents%with%HIV%• %%Adverse%drug%reac<ons%are%common%
• %Up%to%80%%of%pa<ents%experience%an%adverse%drug%reac<on%at%some%point%during%therapy%• %Immune%dysregula<on%• %Altered%drug%metabolism%• %Polypharmacy%
• %HIVJinfected%pa<ents%have%a%higher%risk%of%developing%cutaneous%reac<ons%than%the%general%popula<on%
Drug%Rashes%in%Pa<ents%with%HIV%• %%Efavirenz%
• %%Rifabu<n%
• %%Rifampin%

Efavirenz%• %%Usually%a%mild%to%moderate%maculopapular%rash;%typically%treat%through%with%topical%hydrocor<sone%and%an<histamines%
• %Can%occur%in%5J26%%of%pa<ents%(11%)%
• %Median%<me%of%onset%is%11%days;%typically%resolves%a[er%1%month%
• %Pa<ents%with%a%history%of%sulfa%rash%are%more%likely%to%develop%a%rash%to%NNRTIs%than%without%a%sulfa%allergy%
• %Severe%hypersensivity,%DRESS,%and%SJS/TEN%are%rare%but%have%been%reported%%
• %%<1%%
• %Increased%risk%of%rash%associated%with%HLAJDRB101%
Rifabu<n%and%Rifampin%• %Adverse%reac<ons%to%TB%therapy%occur%at%a%higher%frequency%amongst%HIV+%vs%HIVJ%pa<ents%%%
• %Rifabu<n%is%associated%with%rash%in%11%%of%pa<ents%
• %Rifampin%is%associated%with%rash%in%1J5%%of%pa<ents%
• %Severe%rash/hypersensi<vity%is%rare%for%rifabu<n%and%rifampin%
• %CrossJreac<vity:%Of%pa<ents%who%had%a%dermatologic%reac<on%to%rifampin,%23%%developed%a%rash%when%switched%to%rifabu<n%

Clinical%Course%%• %ReJintroduced%the%following%regimen%at%standard%doses%q2%days:%%• %Ethambutol%800mg%daily%(9/2%J%%• %PZA%30mg/kg%daily%(9/4%J%%• %Moxifloxacin%400mg%daily%(9/6%J%• %Rifampin%daily%(9/8J%%
%

Clinical%Course%%• %Tolerated%Rifampin/PZA/EMB/Moxi%for%3%days%
• %Remained%rashJfree%
• %Developed%fevers%(without%sepsis),%leukopenia,%neutropenia,%and%thrombocytopenia.%%Infec<ous%w/u%neg.%HIT%w/u%neg.%
• %RifampinJdependent%an<Jplatelet%an<body%was%sent%out%%
• %Rifampin%was%discon<nued%a[er%5%days%of%ongoing%fevers%and%cytopenias%
%
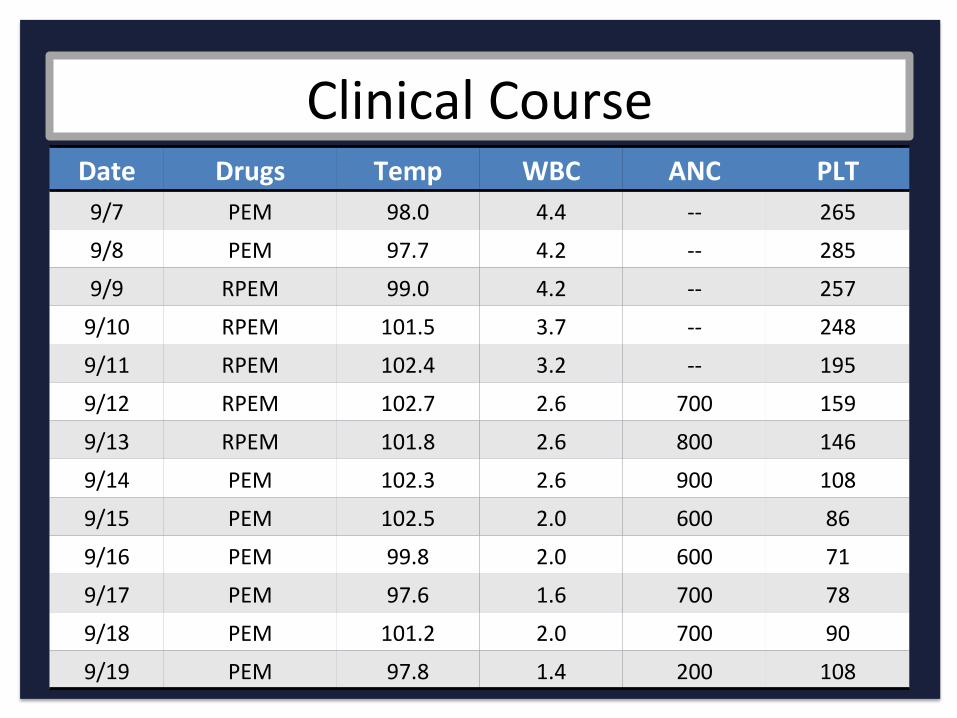
Clinical%Course%Date% Drugs% Temp% WBC% ANC% PLT%9/7% PEM% 98.0% 4.4% JJ% 265%
9/8% PEM% 97.7% 4.2% JJ% 285%
9/9% RPEM% 99.0% 4.2% JJ% 257%
9/10% RPEM% 101.5% 3.7% JJ% 248%
9/11% RPEM% 102.4% 3.2% JJ% 195%
9/12% RPEM% 102.7% 2.6% 700% 159%
9/13% RPEM% 101.8% 2.6% 800% 146%
9/14% PEM% 102.3% 2.6% 900% 108%
9/15% PEM% 102.5% 2.0% 600% 86%
9/16% PEM% 99.8% 2.0% 600% 71%
9/17% PEM% 97.6% 1.6% 700% 78%
9/18% PEM% 101.2% 2.0% 700% 90%
9/19% PEM% 97.8% 1.4% 200% 108%
Rifampin%Hypersensi<vity%Reac<on%%• %Fever,%headache,%chills,%and%bone%pain%
• %Symptoms%usually%begin%1J2%hours%a[er%medica<on%and%resolve%8J10%hours%later%
• %More%common%with%intermiwent%therapy%and%typically%develops%several%months%into%the%treatment%course%
• %%Can%be%associated%with%leukopenia,%agranulocytosis,%thrombocytopenia,%hemoly<c%anemia,%and%renal%failure%
• %ImmuneJmediated%type%III%hypersensi<vity%%
• %Fever%usually%resolves%3J5%days%a[er%discon<nua<on;%thrombocytopenia%usually%resolved%5J7%days%a[er%discon<nua<on%%
DrugJInduced%Immune%Thrombocytoepnia%with%Rifampin%• %DrugJdependent,%platelet%reac<ve%an<bodies%
• %Bind%to%platelets%or%megakaryocytes%!%cell%destruc<on%or%clearance%
• %Glycoprotein%1b/IX%has%been%iden<fied%as%the%target%for%rifampinJinduced%immune%thrombocytopenia%
• %Tes<ng%for%rifampinJdependent%an<platelet%an<bodies%can%be%done%at%the%Blood%Center%of%Wisconsin%using%flow%cytometry%
• %Sensi<vity%and%specificity%are%not%known%• %False%posi<ves%and%nega<ves%are%possible%• %Not%absolutely%necessary%to%make%the%diagnosis%
%Abciximab%
Carbamazepine%Ce[azadime%Ce[riaxone%Ep<fiba<de%Fentanyl%
%Loracarbef%Naproxen%Phenytoin%Quinidine%Quinine%Rani<dine%
%Rifabu<n%Rifampin%
Sulfamethoxazole%Suramin%
Trimethoprim%Vancomycin%

Audience%Response%Ques<on%Case%Summary:%31%yo%woman%with%HIV%(CD4%350),%and%disseminated,%drugJresistant%TB%(low%level%resistance%to%INH%and%resistance%to%Ethionomide)%currently%being%treated%with%EMB/PZA/Moxi%without%rifampin%because%of%presumed%associated%toxicity.%%She%has%no%respiratory%symptoms.%%What%TB%regimen%would%you%recommend%at%this%point?%%A. EMB/PZA/Moxi%for%18%(12J24)%mo%B. EMB/PZA/Moxi/INH%for%18%(12J24)%mo%C. EMB/PZA/Moxi%for%18%(12J24)%mo%+%Injectable%D. EMB/PZA/Moxi/Linezolid%for%18%(12J24%mo)%E. Awempt%reJintroduc<on%of%a%rifamycin%to%EMB/PZA/Moxi%F. Other%

Thank%you%
References%Falk%L,%Fredlund%H,%Jensen%JS.%Symptoma<c%urethri<s%is%more%prevalent%in%men%infected%with%Mycoplasma%genitalium%than%with%Chlamydia%trachoma<s.%Sex%Transm%Infect%2004;%80:289.%%Towen%PA,%Schwartz%MA,%Sjöström%KE,%et%al.%Associa<on%of%Mycoplasma%genitalium%with%nongonococcal%urethri<s%in%heterosexual%men.%J%Infect%Dis%2001;%183:269.%%TaylorJRobinson%D.%The%Harrison%Lecture.%The%history%and%role%of%Mycoplasma%genitalium%in%sexually%transmiwed%diseases.%Genitourin%Med%1995;%71:1.%%Jensen%JS,%Orsum%R,%Dohn%B,%et%al.%Mycoplasma%genitalium:%a%cause%of%male%urethri<s?%Genitourin%Med%1993;%69:265.%%TaylorJRobinson%D.%Mycoplasma%genitalium%JJ%an%upJdate.%Int%J%STD%AIDS%2002;%13:145.%%Gaydos%C,%Maldeis%NE,%Hardick%A,%et%al.%Mycoplasma%genitalium%as%a%contributor%to%the%mul<ple%e<ologies%of%cervici<s%in%women%awending%sexually%transmiwed%disease%clinics.%Sex%Transm%Dis%2009;%36:598.%Anagrius%C,%Loré%B,%Jensen%JS.%Mycoplasma%genitalium:%prevalence,%clinical%significance,%and%transmission.%Sex%Transm%Infect%2005;%81:458.%%Falk%L,%Fredlund%H,%Jensen%JS.%Signs%and%symptoms%of%urethri<s%and%cervici<s%among%women%with%or%without%Mycoplasma%genitalium%or%Chlamydia%trachoma<s%infec<on.%Sex%Transm%Infect%2005;%81:73.%%Manhart%LE,%Critchlow%CW,%Holmes%KK,%et%al.%Mucopurulent%cervici<s%and%Mycoplasma%genitalium.%J%Infect%Dis%2003;%187:650.%%Møller%BR,%TaylorJRobinson%D,%Furr%PM.%Serological%evidence%implica<ng%Mycoplasma%genitalium%in%pelvic%inflammatory%disease.%Lancet%1984;%1:1102.%%Simms%I,%Eas<ck%K,%Mallinson%H,%et%al.%Associa<ons%between%Mycoplasma%genitalium,%Chlamydia%trachoma<s,%and%pelvic%inflammatory%disease.%Sex%Transm%Infect%2003;%79:154.%
References%World%Health%Organiza<on%(WHO).%Laboratory%XDRJTB%defini<ons.%Geneva:%Mee<ng%of%the%global%XDR%TB%task%force%2006.%%%Velaya<%AA,%Masjedi%MR,%Farnia%P,%et%al.%Emergence%of%new%forms%of%totally%drugJresistant%tuberculosis%bacilli:%super%extensively%drugJresistant%tuberculosis%or%totally%drugJresistant%strains%in%iran.%Chest%2009;%136:420.%%%Udwadia%ZF,%Amale%RA,%Ajbani%KK,%Rodrigues%C.%Totally%drugJresistant%tuberculosis%in%India.%Clin%Infect%Dis%2012;%54:579.%%%World%Health%Organiza<on.%Global%Tuberculosis%Report%2014.%hwp://www.who.int/tb/publica<ons/global_report/en/%(Accessed%on%July%07,%2015).%%%WHO/IUATLD%Global%Project%on%An<JTuberculosis%Drug%Resistance%Surveillance.%An<Jtuberculosis%drug%resistance%in%the%world,%report%no.%4%hwp://www.who.int/tb/features_archive/drsreport_launch_26feb08/en/index.html%(Accessed%on%April%29,%2008).%%%Zignol%M,%van%Gemert%W,%Falzon%D,%et%al.%Surveillance%of%an<Jtuberculosis%drug%resistance%in%the%world:%an%updated%analysis,%2007J2010.%Bull%World%Health%Organ%2012;%90:111.%%%World%Health%Organiza<on%(WHO).%Global%tuberculosis%control:%Epidemiology,%strategy,%financing,%Geneva,%WHO%report%2009.%%%Zhao%Y,%Xu%S,%Wang%L,%et%al.%Na<onal%survey%of%drugJresistant%tuberculosis%in%China.%N%Engl%J%Med%2012;%366:2161.%%%World%Helath%Organiza<on.%Global%tuberculosis%control%2011.%WHO;%Geneva,%2011.%%%Poudel%A,%Nakajima%C,%Fukushima%Y,%et%al.%Molecular%characteriza<on%of%mul<drugJresistant%Mycobacterium%tuberculosis%isolated%in%Nepal.%An<microb%Agents%Chemother%2012;%56:2831%%%
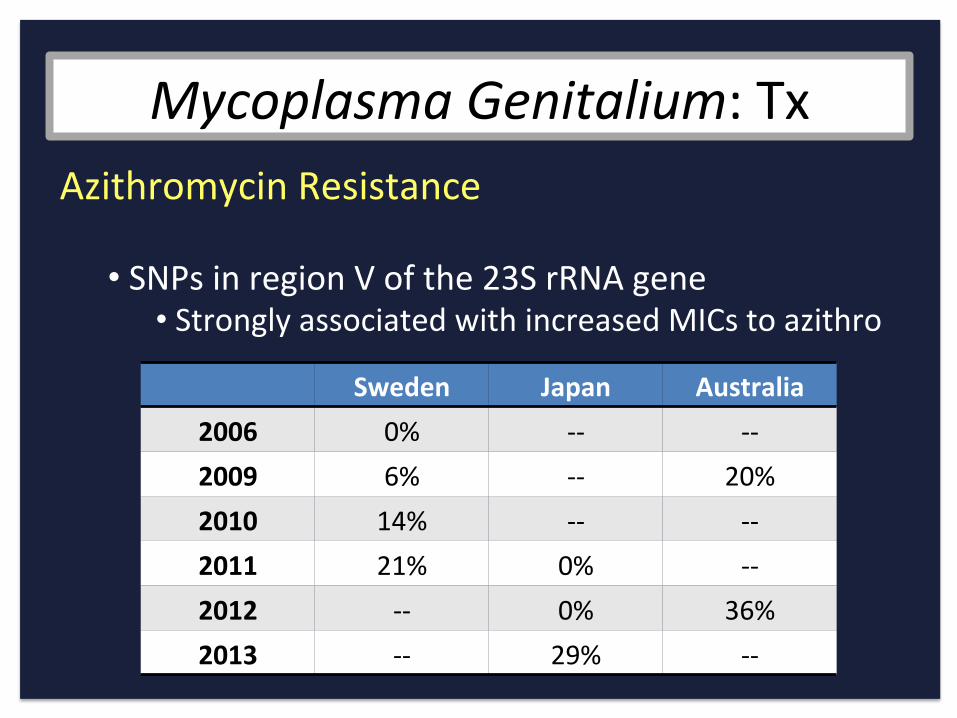
Mycoplasma-Genitalium:%Tx-Azithromycin%Resistance%%• %SNPs%in%region%V%of%the%23S%rRNA%gene%• %Strongly%associated%with%increased%MICs%to%azithro%
Sweden% Japan% Australia%2006% 0%% JJ% JJ%2009% 6%% JJ% 20%%2010% 14%% JJ% JJ%2011% 21%% 0%% JJ%2012% JJ% 0%% 36%%2013% JJ% 29%% JJ%