case study i. patient identification ii. · 2018-01-28 · case study i. patient identification ......
TRANSCRIPT
Kim-Ashleigh Mostert
1
Case Study
I. Patient Identification
Mr. S was a 70 year old Caucasian male referred to the outpatient nutrition oncology
clinic. He required diet education for newly diagnosed stage IIIB non-small cell lung cancer
(T4N3MX). Mr. S passed away February 21, 2017.
II. Social History
A veteran and retired contractor, Mr. S was service connected and received social
security. Though divorced and living alone, he often had a friend staying with him to help work
on his house renovations. Mr. S wished to complete his home renovations in order to pass it on to
his only child, his daughter, and her two children. Mr. S also had a sister who is a retired RN.
Besides spending time with his two dogs and his rabbit, Mr. S. was very active in his local
Alcoholics Anonymous (AA) group. Mr. S’s main hobby was taking archaeology classes and
volunteering with an archaeological firm.
III. Medical History
Mr. S’s medical history included a diagnosis of Stage IIIB non-small lung cancer
(NSCLC) (T4N3MX) that progressed to metastatic adenocarcinoma of the lungs and impacted
the adrenal glands, spleen and the spine. He also developed Chronic Obstructive Pulmonary
Disease (COPD) secondary to his lung cancer. Mr. S also had Type II Diabetes that was
diagnosed in 2001, but he had no unusual complications associated with this disease. In 2016,
Mr. S had a cholecystectomy due to chronic pain and nausea, and to decrease the risk of
Kim-Ashleigh Mostert
2
infection, inflammation and further complications. Mr. S was an alcoholic, but had been in
remission for almost 40 years. He also had a history of smoking but quit in 1990. Mr. S had
PTSD, anxiety, depression, and was bipolar. He attempted suicide twice--once in 1979, right
before he stopped drinking, and a second time in 1986.
Mr. S’s most recent admission was February 10, 2017 when he presented to the
Emergency Department (ED) with cancer-associated back pain and shortness of breath. He had
been experiencing back pain, and was taking an oral medication, oxycodone, at home to control
this pain. His pain became uncontrollable when he ran out of oxycodone, and he was forced to
come to the ED. After admission, an examination by his medical team revealed that the cancer
had progressed to the adrenal glands, spine and spleen (metastatic adenocarcinoma of the lungs).
Further work-up revealed an acute pulmonary embolism, likely the cause of Mr. S’s shortness of
breath. A medical plan was established to treat the pulmonary embolism with anticoagulants, as
bleeding was not an increased risk based on his blood chemistry labs.
During admission, Mr. S’s back pain not well controlled with oral medications, so the
medical team advanced him to a patient-controlled analgesia (PCA) pump. Mr. S experienced
increasing discomfort with constipation, likely as a result of his pain management regimen. Mr.
S was then transferred to palliative care for pain and constipation management, with a plan to
discharge him home to receive outpatient radiation treatment for continued pain management.
While on the palliative care unit, pain control was inconsistent, so morphine was used at higher
doses to make Mr. S comfortable. Over the following five days, Mr. S’s level of alertness
diminished, his respirations became irregular and his treatment plan was adjusted as needed with
the goal of comfort. Mr. S died within 10 days of admission to the hospital.
Kim-Ashleigh Mostert
3
IV. Primary Disease Process
A. Explanation of disease
Cancer is a group of neoplastic diseases characterized by uncontrollable growth and
spread of abnormal cells, which, left untreated, may result in death. There are over 100 different
types of cancer.1 Lung cancer, specifically, is the uncontrolled growth of abnormal cells in one or
both lungs. These cells do not carry out the normal functions of lung cells and do not develop
into normal lung tissue but rather form tumors and interfere with the lung’s function of
producing oxygen for the body.2 Lung cancers are categorized as either small cell lung cancer
(SCLC) or non-small cell lung cancer (NSCLC). Most lung cancer patients have NSCLC. There
are then further subtypes of NSCLC based on the type of cell the cancer forms. Adenocarcinoma
forms in mucus-secreting glands throughout the body and squamous cell carcinoma starts in
early flat cells that line the inner airways of the lungs. Early stages of lung cancer are often
asymptomatic and therefore harder to detect, while late stages are often inoperable. As a result,
lung cancer is often not curable.3
NSCLC is graded and staged in order to adequately determine appropriate treatment and
prognosis. Tumors are graded on a scale assessing the tumor’s appearance and behavior when
viewed under a microscope. Low-grade tumors, grades one and two, are considered well
differentiated, which means the tumor cells look and behavior similarly to normal cells. High-
grade tumors, grades three and four, are poorly differentiated, or the cells are abnormal looking.
These types of tumors tend to grow and spread rapidly.4
The tumor, node, metastasis (TNM) system is used to then stage NSCLC. For example,
T4N3MX; the T describes the primary tumor. The higher the number after the T, the larger the
tumor or the more it has grown into nearby tissues. N refers to the number of nearby lymph

Kim-Ashleigh Mostert
4
nodes that have been infected with cancer cells. M describes if the cancer has metastasized, or
spread to other parts of the body. M1 means the cancer has spread to other parts of the body, M0
means the cancer has not spread to other parts of the body. MX means metastasis cannot be
measured.5
B. Etiology and occurrence
Lung cancer is the leading cause of death from cancer for males and females worldwide.
While the exact cause of each case of lung cancer is unknown, there are many known risk
factors. The primary risk factor for developing lung cancer is tobacco use, mainly from
cigarettes.6 Smoking cessation reduces cancer risk; however, former smokers are still at
increased risk of developing cancer compared to people who have never smoked.3 For non-
smokers, exposure to radon, secondhand smoke and air pollution are common risk factors.
Exposure to asbestos, diesel exhaust and other chemicals can also cause lung cancer. Lung
cancer in non-smokers is often different from lung cancer due to smoking. This cancer tends to
occur at younger ages and this population often have certain gene changes that are different from
people who developed cancer from smoking. Cancer can be caused by DNA changes that alter
how genes control cell life cycles. DNA mutations that increase the risk for developing certain
cancers can be inherited. For example, some people inherit a reduced ability to break down or get
rid of certain cancer-causing agents in the body. Other people inherit a poor DNA repair
mechanism and, as a result, are more likely to experience DNA changes. These types of inherited
mutations could increase risk for lung cancer.7

Kim-Ashleigh Mostert
5
C. Symptoms
Lung cancer is often asymptomatic until it has advanced. Commons lung cancer
symptoms include chronic cough that may progressively get worse, coughing up blood or
phlegm, chest pain that is worse with deep breathing, coughing or laughing, hoarseness, weight
loss and/or loss of appetite, shortness of breath, fatigue, and recurrent infection, such as
bronchitis or pneumonia, and wheezing.1
Lung cancer that has spread to other organs can cause symptoms associated with the area
of the body impacted. For example, bone pain may occur if the cancer has spread to the back or
hips, nervous system changes can occur if cancer is present in the brain or spinal cord, and
yellowing of the skin occurs from cancer impacting the liver.
Specific types of lung cancers have a group of specific symptoms, called syndromes.
Horner’s syndrome occurs when the cancer is located at the top part of the lungs and impacts
certain nerves to the eyes and face. As a result, drooping or eyelid weakness can manifest, a
smaller pupil may develop in the same eye, and/or reduced or loss of sweating on one side of the
face can also occur. Superior vena cava (SVC) syndrome is when the tumor presses on the SVC
and causes the blood to back up in the veins. This leads to swelling in the face, neck, arms and
chest. It can also cause headaches, dizziness and changes in consciousness. Paraneoplastic
syndrome occurs when the cancer creates a hormone-like substance that enters the bloodstream
and acts on other organs and tissues.8 It is important to note that many lung cancer symptoms can
be, and often are, caused by something else, thereby making lung cancer very difficult to identify
early.
Patients with lung cancer often suffer for a variety of symptoms that impact nutritional
status. The most common symptoms include dyspnea, coughing, hemoptysis, pain, fatigue,
Kim-Ashleigh Mostert
6
anorexia, and esophagitis. Patients with lung cancer often suffer from involuntary weight loss at
time of diagnosis, as well as throughout treatment. Weight loss can be due to inadequate intake
because many patients experience anorexia, but some patients have increased energy needs,
which can also lead to involuntary weight loss. The presence of dyspnea can have an impact on
patient’s ability to eat due to the associated fatigue.3 Once again, these symptoms can be caused
by something besides lung cancer and cannot be used alone to identify or diagnose cancer.
D. Lab abnormalities
Laboratory tests can be the examination of a sample of blood, urine, or other bodily fluid,
or tissue to obtain information about a person’s health. They are often used in conjunction to
learn more about a specific condition prior to diagnosis. Blood tests are studied in all cancer
types and while they are not used to diagnose lung cancer, they are important to monitor for
abnormalities. Complete blood count (CBC) determines if the blood has normal amount and
ratio of blood cells. For example, low red blood count can indicate anemia, low blood platelets
could indicate bleeding troubles or low white blood cells could show an increased risk of
infection. Chemotherapy treatments impacts blood cell formation so these tests will be repeated
regularly. Blood chemistry tests measure the amounts of certain substances that are released into
the blood by organs and tissue. These tests can help highlight abnormalities in certain organs,
indicating possible spread of the cancer or side effects of treatments. For example, cancer in the
bones may alter calcium and alkaline phosphatase levels.9 In the possibility of lung cancer, a
sputum cytology or sputum culture can also be collected to test for the presence of abnormal
cells.10
Kim-Ashleigh Mostert
7
E. Usual nutrition interventions and medical treatments for primary disease process
even if not offered/available at the VA
Computerized Tomography (CT) scan, or some kind of imaging scan, is ordered as the
first step in diagnosis. No one scan can diagnosis NSCLC, though, so the scan is used in
conjunction with blood tests, physical exam and a biopsy to form a diagnosis.11 Other scans,
such as an MRI, are used to determine if the cancer has spread to other parts of the body, such as
the brain or bone.
Following diagnosis, the usual medical treatment for NSCLC takes into account the stage
of the cancer, possible side effects and the patient’s preference. Stage IIIB lung cancers cannot
be completely removed surgically; therefore medical teams often recommend chemotherapy in
combination with high-dose radiation, assuming the patient is in fairly good health. This
combination therapy is used aggressively to control the tumor locally and increase survival time.
If a patient is in poor health, then radiation is often used by itself and, less commonly,
chemotherapy may be used by itself. When chemotherapy is initiated, a combination drug
mixture, such as Carboplatin with Paclitaxel is often used. Research supports the combination of
chemotherapy drugs because it has been shown to have the best outcomes and longer survival
rates, although also greater toxicity and thus many side effects.12 Chemotherapy agents are
designed to kill cancer cells, but many chemotherapy drugs are indiscriminate and many also
damage normal cells, often those in the bone marrow, esophagus, stomach and intestines.
Common side effects such as loss of appetite, nausea and diarrhea are the result of this damage.1
If the cancer continues to progress and metastasize, typical treatments to follow would be for
radiation by itself for palliative purposes.
Kim-Ashleigh Mostert
8
One usual nutrition, and overall lifestyle, intervention for NSCLC is smoking cessation.
Even once a patient has cancer, it is important to stop smoking because smoking can decrease the
effectiveness of treatment and make side effects worse. Studies show that smoking cessation
leads to a better prognosis and overall improved quality of life.13 Research indicates that poor
nutrition status is associated with higher rates of hospital admissions, readmissions, increased
length of hospital stay, and lower quality of life and mortality. Poor nutrition status is also
associated with decreased tolerance of treatments, such as radiation and chemotherapy.14
Many nutrition interventions are aimed at ensuring adequate intake of nutrients. Diet and
meal plans are often liberalized to encourage patients to consume adequate protein and calories
in order to prevent unintentional weight loss and promote maintenance of lean body mass.
Weight loss of as little as 6% predicts a reduced response to treatments, reduced survival and
reduced quality of life.1 Nutritional interventions for lung cancer must be individualized to the
therapy and specific side effects a patient is experiencing. General principles to help patients
management nutritional impact symptoms often include encouraging or setting up small,
frequent meals, and easy to swallow and chew foods. Oral supplements that are nutrient-dense
may be used to maximize calorie and protein intake as liquid nutrition is often better tolerated
than solids. Encouraging physical activity such as walking can help improve appetite and
maintain muscle mass.3 Malnutrition or severe dysphagia, often caused by radiation to the chest
and neck or a side effect of chemotherapy, often leads to the need for enteral nutrition to provide
adequate nutrition or supplement feedings. This form of nutrition therapy it used to once again
ensure patients receive adequate protein and calories, as well as to correct for any occurring
deficiencies.
Kim-Ashleigh Mostert
9
F. Usual prognosis
The TNM staging system used to stage patients with NSCLC is the factor that has the
greatest impact on prognosis. Other factors include weight loss, reduced appetite and overall
poor performance status. Survival decreases progressively with more advanced disease stages
and stage IIIB NSCLC has about a 5-10% five year survival rate.15
G. Current and past research studies related to primary disease process
The best opportunity to fight lung cancer is to prevent its formation. As smoking
continues to be the leading cause of lung cancer, research is ongoing to help find new ways to
help people quit smoking and to convince people to never start smoking. Researchers are also
looking at ways that medications and food can provide protection against the development of
lung cancer, but studies have yet to show definitive risk reduction via specific foods or
medications.
Other research studies are related to advancing the treatments for lung cancer. DNA
sequencing methods are being developed to help create gene mutation profiles of solid tumors,
like lung cancer. These tests are then being used to help chose the best treatments. As researchers
learn more about the specific actions of cancers cells that control growth, targeted therapy drugs
are being tested to determine if this type of treatment helps people with cancer live long or
relieve symptoms for increased comfort. Immune treatments are also being studied and
developed further to more efficiently aid the body’s immune system in fighting the cancer.16

Kim-Ashleigh Mostert
10
V. Nutritional Assessment
A. Anthropometric measurements
Anthropometric measurements necessary to assess Mr. S include height, which was 5ft
10in and weight. At time of diagnosis, Mr. S weighed 205lb (BMI 26), which was about his
usual body weight. Excess weight in lung cancer patients is associated with longer survival rates
because lung cancer patients often have decreased weight right before or right after diagnosis.1 In
a four month period, right after diagnosis, Mr. S. lost 12lbs, which was 6% of his body weight. In
total, from diagnosis to his last admission to the hospital, Mr. S lost 21lbs (Figure 1). Weight and
height are important measurements to track because unintended weight loss, at any BMI, has
been shown to be correlated with decreased survival.3
B. Biochemical data, medical tests, and procedures
Mr. S initially presented to the hospital, in October of 2016, with long-term cold and flu
symptoms of chest and sinus congestion, and a productive cough of clear sputum for one month.
Figure 1

Kim-Ashleigh Mostert
11
He was diagnosed with pneumonia. Following treatment for pneumonia, Mr. S’s symptoms were
not improving so a CT scan was conducted. The CT scan of the lungs revealed a right lung mass
(5.0 cm) in the right middle lobe concerning for malignancy with associated mediastinal
lymphadenopathy (LAD). The scan also showed another 7.2mm solid nodule and a 1.8cm
ground glass nodule, both in the right lower lobe (RLL). Overall these finding were concerning
for primary lung cancer. Following these results, Mr. S underwent an endobronchial ultrasound
(EBUS) with biopsy of an enlarged lower paratracheal (4R) lymph node. Mr. S’s case was
discussed at the tumor board meeting and his cancer was staged. A brain MRI was needed to
check for metastasis and complete the staging of the cancer. The results were then discussed with
Mr. S, and oncology and radiation teams were consulted to discuss treatment. Mr. S’s treatment
team encouraged aggressive treatment in hope to provide further quality time but his cancer was
advanced and full recovery was not expected.
Mr. S and his medical team decided to use aggressive means to try to control his lung
cancer. He was scheduled for weekly chemotherapy sessions of Carboplatin 2 + Paclitaxel 45 in
combination with daily radiation treatments for two months. Despite treatments, Mr. S’s cancer
metastasized and the plan became for him to have palliative radiation treatments for pain relief.
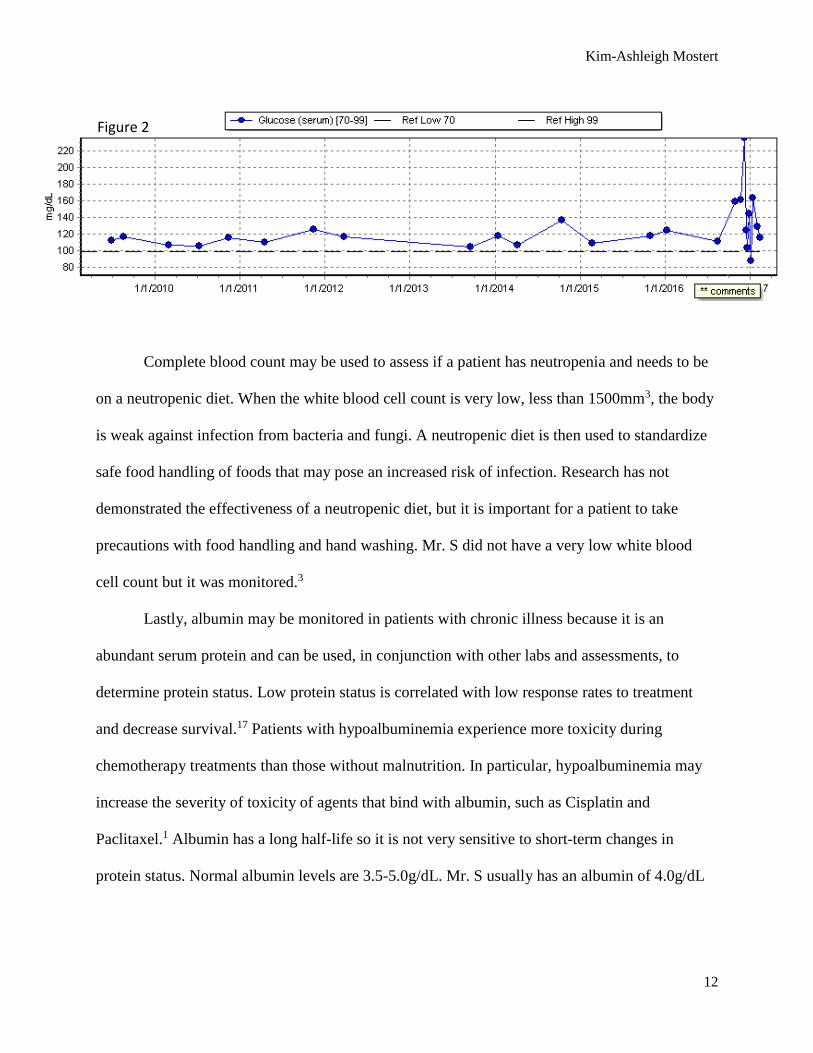
In regards to nutrition labs, Mr. S’s fasting glucose was monitored because he had
diabetes and it was important to establish his base level prior to activation of cancer therapy, as
glucose levels often become elevated with pain, fatigue and overall stress of an illness.
Typically, controlled blood glucose levels are between 70-180mg/dL. As shown in Figure 2, over
the years Mr. S had a very steady blood glucose, which became elevated with his illness at the
end of 2016.
Kim-Ashleigh Mostert
12
Complete blood count may be used to assess if a patient has neutropenia and needs to be
on a neutropenic diet. When the white blood cell count is very low, less than 1500mm3, the body
is weak against infection from bacteria and fungi. A neutropenic diet is then used to standardize
safe food handling of foods that may pose an increased risk of infection. Research has not
demonstrated the effectiveness of a neutropenic diet, but it is important for a patient to take
precautions with food handling and hand washing. Mr. S did not have a very low white blood
cell count but it was monitored.3
Lastly, albumin may be monitored in patients with chronic illness because it is an
abundant serum protein and can be used, in conjunction with other labs and assessments, to
determine protein status. Low protein status is correlated with low response rates to treatment
and decrease survival.17 Patients with hypoalbuminemia experience more toxicity during
chemotherapy treatments than those without malnutrition. In particular, hypoalbuminemia may
increase the severity of toxicity of agents that bind with albumin, such as Cisplatin and
Paclitaxel.1 Albumin has a long half-life so it is not very sensitive to short-term changes in
protein status. Normal albumin levels are 3.5-5.0g/dL. Mr. S usually has an albumin of 4.0g/dL
Figure 2
Kim-Ashleigh Mostert
13
but this decreased to 2.7g/dL after diagnosis. With treatments and nutritional interventions it
went back up to 3.1g/dL but decreased prior to readmission to the hospital in February.
C. Nutrition-focused physical findings
First assessment of Mr. S showed he was overweight, but as he lost weight it was apparent
that he was experiencing muscle wasting despite a normal BMI. At initial assessment Mr. S had
full, well-defined temples and his clavicles were not prominent. Two months later, his temples
were slightly depressed and his clavicle bones became visible as the pectoral muscles
diminished. Muscle wasting contributes to fatigue, weakness, respiratory complications and
reduced performance and quality of life.3
Research shows that about 50% of lung cancer patients develop COPD, which is associated
with additional weight and muscle mass loss. Patients with COPD also have a change in muscle
fiber that makes them more susceptible to fatigue.1 As a result of his wasting and development of
COPD, it was not surprising that Mr. S complained of fatigue and the inability to continue his
usual level of activity, sometimes not even spending time out of bed or off the couch.
Mr. S was also experiencing swallowing difficulties due to esophageal pain caused by the
high-dose radiation treatments. This, along with decreased appetite and nausea, contributed to
overall decreased food intake.
D. Food/nutrition-related history
Mr. S’s usual daily intake included two meals, usually skipping breakfast or lunch. In the
first nutrition appointment, Mr. S learned about the importance of adequate intake of protein and
energy. He was encouraged to eat easy-to-swallow foods such as yogurts and smoothies and
Kim-Ashleigh Mostert
14
consume small, frequent meals to help with fatigue and loss of appetite. He was also started on a
low-carbohydrate supplement shake to drink if he was unable to eat a full meal. Lastly, Mr. S
was educated on the importance of hydration.
On Mr. S’s admission to the hospital in February, he reported his portions used to be large
but decreased, as appetite declined, to less than 50% of what he used to eat. He was still trying to
drink the supplemental drinks but other food was unappealing and he did not have the energy to
consume full meal trays. Mr. S worked hard to comply with fluid intake to stay hydrated.
Prior to the start of treatments, Mr. S was very active, spending time walking his dogs and
working on his house. As he became more fatigued and lost muscle mass, Mr. S was unable to
maintain his level of physical activity. Mr. S also experienced shortness of breath and increased
pain associated with his cancer progression, and this also contributed to his lack of physical
activity.
E. Medications
The use of medications is a significant component in medical therapy for treating and
managing many diseases; therefore it is important to note the medications with nutritional
implications. One past medications Mr. S was taking included Metformin for diabetes. Other
medications with food-drug interactions included Lisinopril, Simvastatin, Sildenafil, and
Tamsulosin.
Mr. S also took a variety of medications to help with the side effects of his cancer treatments
and to try to increase his nutritional status and quality of life. Those medications included
Ondansetron and Prochlorperazine for nausea and vomiting; CPD-Stomatitis mixture to help
relieve pain from stomatitis; and Megestrol, which is an appetite stimulant.
Kim-Ashleigh Mostert
15
F. Estimation of protein and energy requirements. Include which calculations were
used for Kcals/Protein/Fluids.
Mr. S’s needs for calories, protein and fluid were increased due to his disease state and the
need to limit weight and muscle loss. NSCLC patients have higher energy expenditure therefore
higher nutritional needs. It is important to monitor energy intake, especially when tube feeding a
patient, because underfeeding can lead to loss of lean body mass, immunosuppression and
increased risk of hospital acquired infections. Overfeeding, on the other hand, can lead to
respiratory failure due to increased carbon dioxide (CO2) production, alterations in hydration
status and electrolyte imbalances.1 Mr. S’s estimated energy needs were 2500-2800 calories per
day using a 30-32kcal/kg calculation. His protein needs were estimated at 105-114 grams per day
based on a 1.2-1.3g/kg calculation. Lastly his fluid needs mimic calories at 2500-2800 based on
the calculation 1ml/kcal. Energy and fluid requirements increase related to the extra effort of
breathing and loss of moisture with breathing.3 During Mr. S’s last few days in the palliative care
unit, he experienced rapid respiratory rate and likely an increase in metabolic needs and fluid
needs.
VI. Nutrition Diagnosis
Mr. S had two nutritional diagnoses at his first assessment with a dietitian. One was related to
inadequate energy intake and the second related to his nutrition-related knowledge deficit. The
nutritional diagnosis of inadequate energy intake was in conjunction with the decreased ability to
consume sufficient energy. This inadequate intake was evident in Mr. S’s dietary recall, his low
albumin levels and his decreased weight. The second nutritional diagnosis related to his lack of
Kim-Ashleigh Mostert
16
nutrition knowledge, since Mr. S had not seen a dietitian for cancer before as this was a new
diagnosis. While the knowledge-related diagnosis was resolved with education, Mr. S continued
to experience inadequate energy intake throughout his treatments, so this diagnosis was ongoing.
VII. Nutrition Intervention
Nutrition screening and early intervention is essential to reverse muscle and weight
depletion. The later nutrition care is implemented, the more difficult it is to modify a patient’s
nutritional status.1 Nutrition diagnoses related to intake takes priority because minimizing weight
loss and preserving muscle mass is so important for lung cancer patients. Nutritional
interventions related to the intake target the etiology of the diagnosis. With increased needs, the
intervention of small, frequent meals aims to help the patient eat more often to meet these needs,
without creating increased fatigue. Consuming easier to eat foods and liberalizing the diet
allowed Mr. S to eat what sounded good and foods he felt he could tolerate. Providing
supplemental shakes delivered higher energy and protein amounts in a smaller volume, making it
easier to consume and meet these increased needs. Encouraging physical activity helped Mr. S to
have an appetite to actually eat the meals to meet his elevated nutritional needs. An intervention
that was discussed with Mr. S, but not implemented, was the possibility of tube feeding to help
supplement meals because Mr. S experienced severe weight loss, loss of appetite and painful
swallowing and chewing. If Mr. S had continued to decline at the same rate, this intervention
would likely have been initiated.
Many of these interventions are aimed at the same goal because they are more likely to
produce positive results in conjunction. Providing education and multiple interventions also
helped Mr. S determine what worked for him, and at different stages of treatment, different
Kim-Ashleigh Mostert
17
interventions worked better. Mr. S played an active part in developing personal interventions that
he wanted to work on. For example, Mr. S identified that he did better consuming liquids rather
than solid foods, so healthy, high calorie smoothies were discussed, and Mr. S was provided
recipes so that he would have options when certain foods did not appeal to him.
VIII. Monitoring and Evaluation
Based on Mr. S’s rapid decline, there was little evidence that the nutritional interventions
provided additional quality time. Based on Mr. S’s reports and his slowed weight loss, the
supplemental nutrition shakes did allow him to consume more energy, and meet more of his
nutritional needs, than he would have without the supplements. Even when Mr. S was admitted
to the hospital and was refusing meal trays, he did request the supplemental shakes which shows
he enjoyed them and that they provided comfort.
IX. Summary of Patient’s Condition and Prognosis
When diagnosed with Stage IIIB NSCLC, Mr. S was informed that his prognosis was
poor but that treatment would possibly provide additional quality time. Unfortunately, despite
aggressive cancer therapies and nutritional interventions, Mr. S died just four months after he
was diagnosed, at age 70.
Kim-Ashleigh Mostert
18
X. List of References
1. Leser M, Ledesma N, Bergerson S, Trujillo E. Oncology Nutrition for Clinical Practice.
Oncology Nutrition Dietetic Practice Group of the Academy of Nutrition and Dietetics;
2013.
2. What is Lung Cancer? Lung Cancer 101http://
http://www.lungcancer.org/find_information/publications/163-lung_cancer_101/265-
what_is_lung_cancer. Accessed March 4, 2017.
3. Oncology. Nutrition Care Manual.
https://www.nutritioncaremanual.org/topic.cfm?ncm_category_id=1&lv1=22938&ncm_t
oc_id=22938&ncm_heading=&. Accessed March 11,2017.
4. Grades of Non-Small Cell Lung Cancer. Candadian Cancer Society.
http://www.cancer.ca/en/cancer-information/cancer-type/lung/grading/?region=bc.
Accessed March 4, 2017.
5. Staging. National Cancer Institute. https://www.cancer.gov/about-cancer/diagnosis-
staging/staging. Accessed March 4, 2017.
6. Bala S, Gundeti S, Linda VG, Maddali LS, Digumarti RR, Uppin SG.
Clinicopathological Features and Outcomes in Adanced Nonsmall Cell Lung Cancer with
Tailored Therapy. Indian J Med Paediatric Oncology 2016;27(4)L242-250.
doi:10.4103/0971-5851.195735.
7. Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th Edition of the
AJCC Cancer Staging Manual and the Future of TNM. Ann Surg Oncol.
2010:17(6):1471-1474. doi:10.1245/s10434-101-0985-4.
Kim-Ashleigh Mostert
19
8. Signs and Symptoms of Lung Cancer. American Cancer Society.
https://www.cancer.org/cancer/lung-cancer/prevention-and-early-detection/signs-and-
symptoms.html. Accessed March 4, 2017.
9. Tests for Non-Small Cell Lung Cancer. American Cancer Society.
https://www.cancer.org/cancer/non-small-cell-lung-cancer/detection-diagnosis-
staging/how-diagnosed.html#references. Accessed March 4, 2017
10. Understanding Laboratory Tests. National Cancer Insitutute.
https://www.cancer.gov/about-cancer/diagnosis-staging/understanding-lab-tests-fact-
sheet. Accessed March 5, 2017.
11. Lung Cancer – Non-Small Cell: Diagnosis. Cancer.net. http://www.cancer.net/cancer-
types/lung-cancer-non-small-cell/diagnosis. Accessed March 5, 2017.
12. Belani CP, Choy H, Bonomi P, et al. Combined chemoradiotherapy regimens of
paclitaxel and carboplatin for locally advanced non-small-cell lung cancer: a randomized
phase II locally advanced multi-modality protocol. J Clin Oncol. 2005;23(25):5883-5891.
Doi:10.1200/JCO.2005.55.405.
13. Cataldo JK, Dubey S, Prochaska JJ. Smoking cessation: an integral part of lung cancer
treatment. Oncology. 2010;78(5-6):289-301. Doi:10.1159/000319937
14. Oncology Guidelines. EAL. http://www.andeal.org/topic.cfm?menu=5291&cat=5066.
Accessed March 18, 2017.
15. Overview of the initial evaluation, treatment and prognosis of lung cancer. UpToDate.
https://www.uptodate.com/contents/overview-of-the-initial-evaluation-treatment-and-
prognosis-of-lung-
Kim-Ashleigh Mostert
20
cancer?source=search_result&search=lung%20cancer%20prognosis&selectedTitle=1~15
0#H3. Accessed March 19, 2017.
16. What’s New in Small Cell Lung Cancer Research? https://www.cancer.org/cancer/small-
cell-lung-cancer/about/new-research.html. Accessed March 21, 2017.
17. Tanriverdi O, Avci N, Oktay E, et al. Pretreatment Serum Albumin Level is an
Independent Prognostic Factor in Patients with Stage IIIB Non-Small Cell Lung Cancer:
A Study of the Turkish Descriptive Oncological Researches Group. Asian Pac J Cancer
Prev. 2015;16(14):5971-5976. http://www.ncbi.nlm.nih.gov/pubmed/26320482.
Accessed March 20, 2017.