case studies in luminal gastroenterology adam harris consultant gastroenterologist the spire...
TRANSCRIPT

Case Studies in Luminal Gastroenterology
Adam Harris
Consultant Gastroenterologist
The Spire Tunbridge Wells Hospital

Luminal Gastroenterology
Learning objectives:
1. Avoiding foregut complications of NSAIDs
2. Understanding new dietary option in IBS
3. Understanding latest drug treatments in constipation

Case Study 1
87 yr old woman with OA, nocturnal joint pains, angina & bleeding DU 1999
Needs pain relief – what do you recommend?

NSAIDs & Bleeding ulcers
• PMH of ulcer bleeding who use NSAIDs are at highest risk (20%) of re-bleeding
• Use NSAID plus standard dose PPI
• Despite this 4-8% will re-bleed in 6 months
Chan et al. New Engl J Med 2002; 347:2104-10.

NSAIDs
High Risk of Complications• PMH PUD or bleed • >65 yrs • Longterm use; high dose • More than one NSAID• Co-prescribed steroids, clopidogrel or
warfarin• Serious co-morbidities

Risk of gastro-duodenal ulcer
Placebo + Aspirin
Naproxen +Aspirin
Celecoxib +Aspirin
8% 27% 19%

NSAIDs & PPIs
4 points to remember:1. PPIs decrease risk of NSAID-associated GU &
DU cf placebo2. PPIs equally effective whether non-selective
NSAIDs or COX-2 inhibitors3. PPI co-therapy is effective in healing &
preventing recurrent ulcers with long term NSAIDs
4. PPIs decrease risk of NSAID-associated bleeding

Aspirin 4 points to remember:
1. Aspirin increases risk of UGIB 4 fold
2. Aspirin + other NSAID increases risk 8 fold
3. No difference in RR with EC or “junior”
4. Eradication of H pylori decreases risk of ulcer
Lai et al. New Engl J Med 2002; 346: 2033-38
McQuaid KR, Laine L. Am J Med 2006; 119: 624-38
Arora G et al. Clin Gastro Hepatol 2009; 7: 725-35

Case Study 2 24 yr old female with 1-2 year of recurrent low abdominal pain, bloating & intermittent watery diarrhoea
Unemployed & lives alone
Normal examination
Blood tests, urine & stool culture normal
Faecal calprotectin <50

Low FODMAP diet
• Fermentable, Oligo-, Di-, Mono-saccharides and Polyols
• Comprise fructose, lactose, fructans, galactans & polyols
• Low FODMAP diet developed at Monash University in Melbourne, Australia

FODMAPs in diet
• Fructose eg fruits, honey, corn syrup• Lactose eg diary• Fructans eg wheat, onion, garlic• Galactans eg beans, lentils, legumes• Polyols eg sorbitol, avocado, apricots, plums

Low FODMAP
• FODMAP CHO trigger changes in fluid content & bacterial fermentation in bowel leading to symptoms in susceptible individuals
• Follow low FODMAP diet to eliminate fermentable carbohydrates; trained dietician required.
• Eliminate from diet for trial period then re-introduce each FODMAP carbohydrate gradually & record symptoms
• Reported (by enthusiasts) that up to 70% of patients report improvement in symptoms

Case Study 3
28 yr old woman with 5 yr history of constipation (BO 2 x/wk) with straining & passage of hard stool; bloating & low abdo discomfort
No incontinence. No neurological illness.
Examination & blood tests normal.
Tried fibre, lactulose, Movicol, Senna, bisacodyl with limited or no benefit.

Differential Diagnosis?

Differential Diagnosis?
• IBS-C• Idiopathic Slow Transit Constipation• Functional Outlet Obstruction

Investigation?
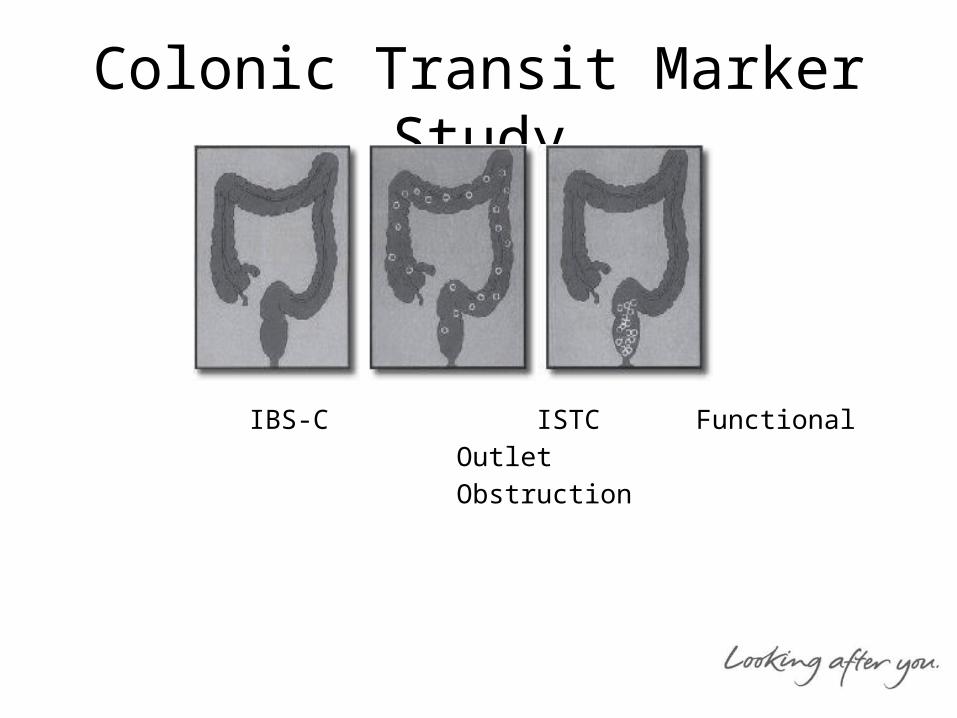
Colonic Transit Marker Study
IBS-C ISTC Functional
Outlet
Obstruction

Treatment Options
• IBS-C
linaclotide (Constella)
• ISTC
prucalopride (Resolor)
• Functional Outlet ObstructionFurther assessment; surgery; biofeedback

Prucalopride
• 5-HT4 receptor agonist with entero-colonic kinetic activity; not a laxative
• Women only• Works within 2-3 hours• ↑ spontaneous bowel movements: 67% vs
39% placebo (p<0.001)• Improves symptoms of pain, bloating,
straining & tenesmus

Prucalopride
• 2mg od for 28 days • If no response: do not continue• 1mg od: women>65 yr; liver/renal failure• AE: nausea; headache; abdo pain;
diarrhoea• Cost: 28 x 2mg ≈ £60

Linaclotide
• Guanylate cyclase-C agonist• Reduces visceral hypersensitivity, increases
intestinal secretion & accelerates transit• Treatment of moderate-severe IBS-C in adults• One capsule (290 mcg) od 30 mins before meal• Interaction: OCP, thyroxine• Adverse effect: diarrhoea (<20%)• Cost: £37.56 for 28 days

Linaclotide• 47% decrease in abdo pain over 26 weeks
(p<0.001 vs placebo)1
• 40% improvement in bloating over 26 weeks (p<0.0001 vs placebo)1
• Increase in spontaneous bowel movements from 1.7 to 5.7 weekly over 12 weeks (p<0.0001 vs placebo)2
• Improvement in QoL (p<0.01 vs placebo)
1. Quigley EM et al. Aliment Pharmacol Ther 2013; 37:49-61
2. Chey WD et al. Am J Gastroenterolo 2012; 107: 1702-12

Luminal Gastroenterology
Learning objectives:
1. Avoiding foregut complications of NSAIDs
2. Understanding new dietary option in IBS
3. Understanding latest therapies in constipation