case scenarios in pediatric hiv: choose your own adventure!
DESCRIPTION
Case Scenarios in Pediatric HIV: Choose Your Own Adventure!. Sabreen Akhter, DO. Case 1. - PowerPoint PPT PresentationTRANSCRIPT

Case Scenarios in Pediatric HIV:
Choose Your Own Adventure!
Case Scenarios in Pediatric HIV:
Choose Your Own Adventure!
Sabreen Akhter, DOSabreen Akhter, DO
Case 1Case 1You are seeing a 1 week old infant, born to an HIV+ mother who is not on ARVs, and who did not receive prenatal care or PMTCT during her home birth. You are trying to counsel the mother on feeding her baby. You will try to get her hooked into treatment for her HIV, and she thinks she may be able to procure clean drinking water for her child, but you are not sure of either. You tell her to:
Option 1:ExclusivelyBreast Feed
Option 2:Exclusively
Formula Feed
Option 3: Do a
combination of both

Option 1: Exclusive Breast Feeding
Option 1: Exclusive Breast Feeding
WHO statement: “Infant feeding practices recommended to mothers known to be HIV-infected should support the greatest likelihood of HIV-free survival of their children and not harm the health of mothers. To achieve this, prioritization of prevention of HIV transmission needs to be balanced with meeting the nutritional requirements and protection of infants against non-HIV morbidity and mortality.”
In other words: Breast feed if you’ve got to!
Exclusive Breast Feeding: Depends on the ScenarioExclusive Breast Feeding: Depends on the Scenario
Risk of contracting HIV through your mother during birth process: 30% (most of which is pre-partum)
Risk of contracting HIV through breast milk with subsequent feeding: 5-20%
If breast feeding is stopped, it should be done gradually over one month
It’s cost effective!: various models and studies done in HIV endemic regions have shown repeatedly the cost benefit and the morbidity/mortality benefit to exclusive breast feeding over FF in areas with no secure access to clean water
Option 2: Exclusive Formula Feeding
Option 2: Exclusive Formula Feeding
We know it’s the safest method when: environmental and social circumstances are Acceptable, Feasible, Affordable, Sustainable, Safe for, and Supportive of, replacement feeding
... that doesn’t often happen
Promoting exclusive formula feeding: compromises free choice; targets beneficiaries erroneously; creates a false perception of endorsement by health workers; compromises breastfeeding; results in disclosure of HIV status; ignores hidden costs of preparation of formula; increases mixed breastfeeding; and may require organization and management of programs that are complicated and costly

Option 3:Combination of Both
Option 3:Combination of Both
Breastfed infants who also received solids were significantly more likely to acquire infection than were exclusively breastfed children, as were infants who at 12 weeks received both breastmilk and formula milk
In a systematic review of the effect of different infant feeding practices in the absence of ARVs, decreased HIV transmission in the first six months of infant life was associated with exclusive breastfeeding (EBF) compared to mixed feeding
Hypothesis: exclusive breastfeeding preserves integrity of intestinal mucosa, promotes better breast health; large and complex proteins may facilitate ease of GI tract viral entry

Beyond 6 months...Beyond 6 months...HIV-free survival of HIV exposed infants who breastfed beyond six months of age was better than, or not statistically different from, infants who were started on replacement feeds
Infants given replacement feeds after a period of breastfeeding also suffered increased serious infections, including diarrhea and pneumonia, growth faltering and death

Case 2Case 2You need to decide whether to start ARV therapy on the same one month old before you. Mom has tested positive for HIV and has not been on treatment before, during, or after birth. There is no HIV DNA PCR test available at this time, and the HIV Ab test may come back positive due to maternal antibodies. You decide to:
Option 1:Defer
treatment until the child can be definitely
tested for HIV (with HIV Ab testing at 15-18 months)
Option 2:Test for HIV Ab,
and, if +, initiate
treatment regardless of confirmatory testing at this
time
Option 3:Test for HIV Ab, but, if +, defer treatment until child develops
an AIDS defining illness/severe HIV disease
Option 1: Defer Treatment
Option 1: Defer Treatment
50% of infants infected with HIV will die before their 2nd birthday if not on ARV prophylaxis-- the vast majority of those in the 1st year of life
Recent studies demonstrated that more than 80% of infected infants become eligible to start ART before six months of age when using the 2006 clinical and/or immunological criteria for the initiation of treatment

Option 2: Initiate treatment
Option 2: Initiate treatment
Almost right...
CDC recommendations: start prophylaxis with 6 weeks of AZT as soon as possible after birth for all HIV exposed neonates
Infants born to HIV-infected women who have not received antepartum ARV drugs should receive prophylaxis with a combination ARV drug regimen, begun as soon after birth as possible (AI). RCTs have shown that a 2 drug regimen of zidovudine given for 6 weeks combined with three doses of nevirapine in the first week of life (at birth, 48 hours later, and 96 hours after the second dose) is ideal
But that’s under ideal circumstances...

Barriers to ARV UseBarriers to ARV UseAntenatal and Peripartum period:
antenatal care attendance is low, particularly in rural areas
too few pregnant women have access to HIV testing
access to optimal ARV prophylaxis or therapy is insufficient
alternatives to breast-feeding are uncommon.
In its 2010 progress report, the WHO indicated that only one quarter of pregnant women had received an HIV test, and among those identified as HIV-infected, only half received any antiretroviral prophylaxis during pregnancy or at delivery.

Barriers to ARV UseBarriers to ARV UseAvailability, cost, ease of administration
US market demand has declined dramatically
Pharmaceutical companies have invested little in ensuring the safety and efficacy of antiretroviral use in children or in developing child-appropriate drug formulations
2010 the Drugs for Neglected Diseases initiative (DNDi): consensus around the need to develop an improved first-line regimen for infants. The ideal formulation: palatable, heat-stable, easily dispersible, administered once daily or less, carries minimal risk for the development of resistance, and be suitable for infants and young children (<2 months to 3 years of age), with minimum requirements for weight adjustments.
Drugs must be compatible with tuberculosis drugs and, especially, affordable
Option 3: Test For HIV Ab Now, but if
Positive, Defer Treatment Until
Child Develops AIDS Defining
Illness/Severe HIV OR Definitive Testing
Can Be Done
Option 3: Test For HIV Ab Now, but if
Positive, Defer Treatment Until
Child Develops AIDS Defining
Illness/Severe HIV OR Definitive Testing
Can Be Done
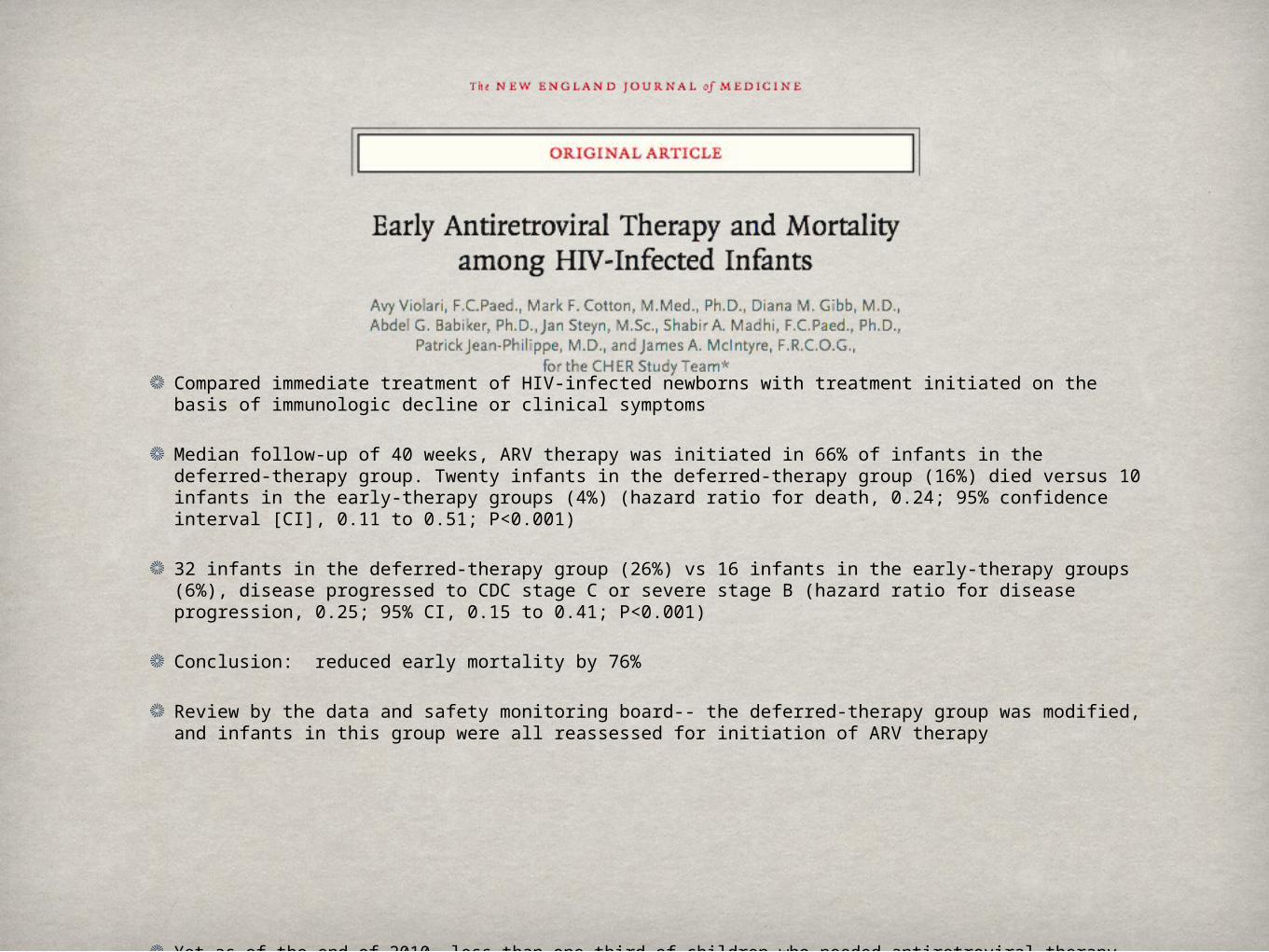
Compared immediate treatment of HIV-infected newborns with treatment initiated on the basis of immunologic decline or clinical symptoms
Median follow-up of 40 weeks, ARV therapy was initiated in 66% of infants in the deferred-therapy group. Twenty infants in the deferred-therapy group (16%) died versus 10 infants in the early-therapy groups (4%) (hazard ratio for death, 0.24; 95% confidence interval [CI], 0.11 to 0.51; P<0.001)
32 infants in the deferred-therapy group (26%) vs 16 infants in the early-therapy groups (6%), disease progressed to CDC stage C or severe stage B (hazard ratio for disease progression, 0.25; 95% CI, 0.15 to 0.41; P<0.001)
Conclusion: reduced early mortality by 76%
Review by the data and safety monitoring board-- the deferred-therapy group was modified, and infants in this group were all reassessed for initiation of ARV therapy
Yet as of the end of 2010, less than one third of children who needed antiretroviral therapy were receiving it. Without treatment, one third of children born with HIV die before their first birthday; 50% die before they turn two.
TestingTestingHigh income countries use HIV DNA or RNA polymerase in the newborn period-- most children have a diagnosis by 6 weeks of age
Low income countries still rely in HIV Ab tests, which require waiting till the child is 15-18 months to be sure that maternal Abs are not longer present
Future: real time dried blood spot tests on filter paper sent to remote labs
WHO Recommendations
WHO RecommendationsHIV serologic assays should be done as soon as possible
<18 months for screening; >18 months for diagnosis
HIV virologic assays should be done ASAP, especially in infants < 18 months
In infants with positive virologic test, start treatment right away
Initiate ARV in all HIV infected infants in the first year of life, regardless of clinical staging or CD4 count
Initiate ART for any child less than 18 months of age who has been given a presumptive clinical diagnosis of HIV infection
What to StartWhat to StartFor infants not exposed to ARVs, start ART with nevirapine (NVP) + 2 nucleoside reverse transcriptase inhibitors (NRTIs)
For infants exposed to maternal or infant NVP or other NNRTIs used for maternal treatment or PMTCT, start ART with lopinavir/ritonavir (LPV/r) + 2 NRTIs
For infants whose exposure to ARVs is unknown, start ART with NVP + 2 NRTIs

Case 3Case 3The mother you have been speaking with is wondering about vaccines for her child if he turns out to be infected with HIV. You tell her:
Option 1: Even if he is HIV+, the child can
get all the vaccines that he normally would have
Option 2: If he is HIV+, he can get some of the vaccines that he normally would
have
Option 3: If he is HIV+, his
immune system is not functioning
properly, and vaccination will
not work effectively, so he should get no vaccines
until his immune status has improved

Option 3: Delay Vaccination Until His Immune System is
Better
Option 3: Delay Vaccination Until His Immune System is
BetterActually, the opposite... don’t wait!
For a neonate with a relatively healthy mother, he probably does not have advanced HIV yet
Advanced HIV infections can result in a blunted immune response to immunization, but this response does depend on how affected the immune system is at the time of vaccine receipt
Therefore, it is important to immunize HIV-infected children as quickly as possible so that they can mount protective responses prior to the failing of their immune system

Advanced HIV-- When to Wait
Advanced HIV-- When to Wait
Delay post-reconstitution immunizations for at least 3 months to maximize the immune response to vaccines for:
Infants/children with CD4+ < 15% or an absolute CD4+ lymphocyte count that is lower than normal for age, those with a history of an AIDS-defining illness, or those with clinical manifestations of symptomatic HIV to have severe immunosuppression
Patients with CD4+ lymphocyte counts from 15% to 25% or those patients older than 6 years with counts of 200-500 are considered to have limited immune deficits--> go ahead with immunizations

Transient ViremiaTransient ViremiaTheoretical concern: Activation of the cellular immune system is important in the pathogenesis of HIV disease, and that fact has given rise to concerns that activation of the immune system through vaccinations might accelerate the progression of HIV disease through enhanced HIV replication
Studies on influenza vaccine and HIV patients have show transient viremia with influenza vaccination, but no effect on CD4 count
The benefits of appropriate vaccination generally are felt to outweigh the risks of transient viremia
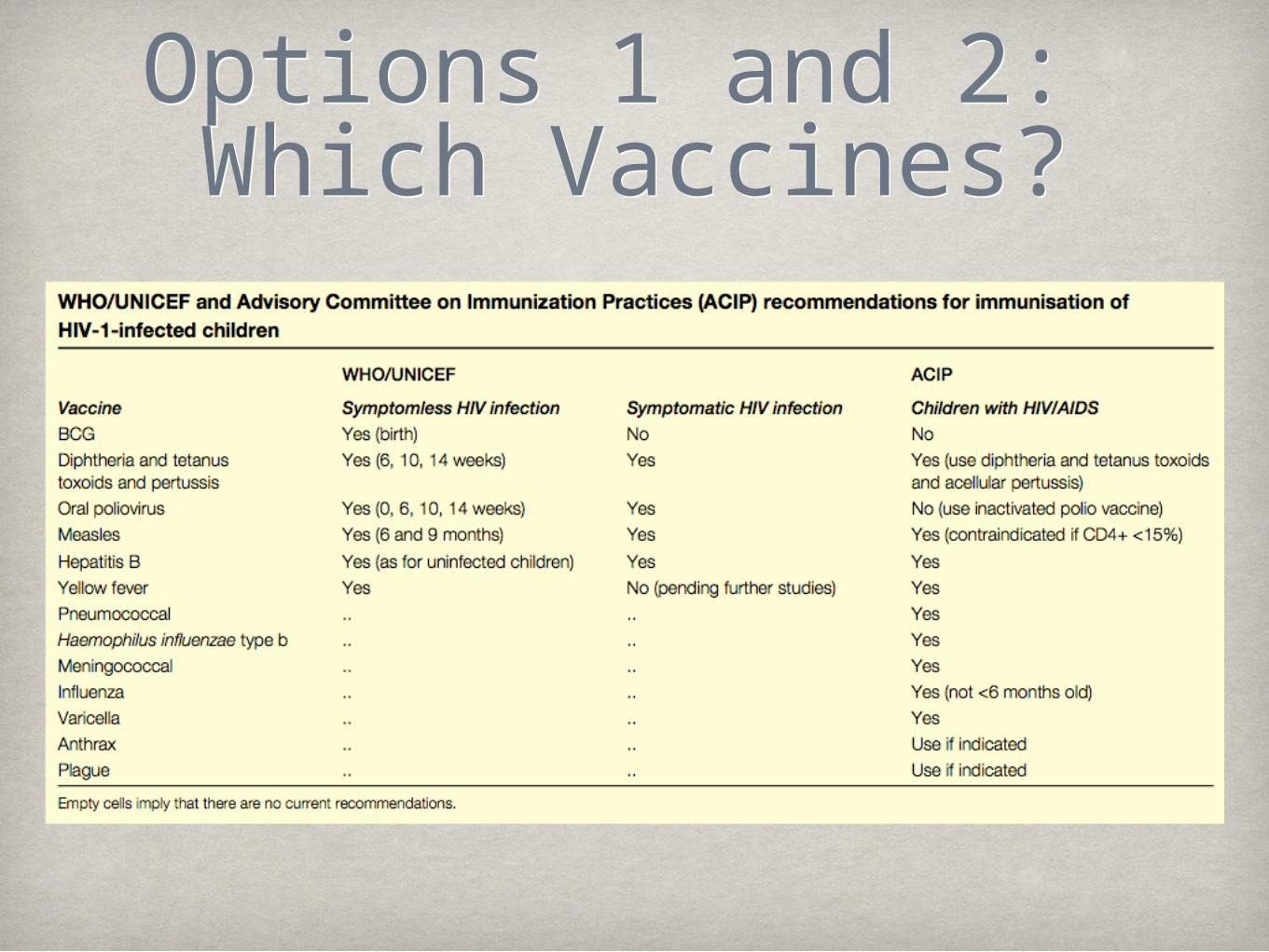
Options 1 and 2: Which Vaccines?Options 1 and 2: Which Vaccines?

In general, it is preferable to avoid live-virus vaccines if inactivated vaccine is available
Data are limited, in general, HIV-infected individuals who are well controlled on ART may receive indicated live-virus vaccines such as measles, mumps, rubella (MMR) and varicella if lacking immunity
These vaccines should be avoided in patients with severe disease
BCG should not be given to those with severe immunocompromise owing to HIV
OPV is not recommended for persons with HIV infection outside resource-limited settings if the inactivated polio vaccine (IPV) is available
Do VaccinateDo VaccinateInfants/children with HIV are more susceptible to severe, recurrent infections with vaccine-preventable pathogens, so timely vaccination is imperative
Few studies have evaluated the longevity of immunologic memory or immune protection in vaccinated children
Altogether, since the risk of disease from most vaccine-preventable diseases far outweighs the risk of vaccine-induced adverse events, the WHO currently recommends routine vaccination of HIV-1-infected children with some modification of the standard recommendations
Case 4Case 4The pregnant, HIV+ sister of the mother you have been speaking with is also present at the clinic visit. She has fallen ill with severe malaria on a few occasions before and is worried about getting malaria again while pregnant. You tell her:
Option 1:She is more
susceptible to malaria during pregnancy and especially since she is HIV+, she should receive
prophylaxis
Option 2:She has the same susceptibility to malaria as when
she was not pregnant even
though she is HIV +, and prophylaxis
medications are not safe during
pregnancy anyway
Option 3:She is most
susceptible to complications
from her malaria and HIV status
around the time of birth, so she
should only consider
prophylaxis around that time

Options 1+ 2Options 1+ 2Studies suggest that dual infection with malaria and HIV leads to increased risk of adverse perinatal outcomes
One study of 2608 pregnant women, 5% of whom were HIV+, showed neonatal mortality in infants born to mothers with both placental malaria and HIV was significantly greater than with either infection alone
Co-infection with malaria and HIV: increased risk of stillbirth, preterm delivery, maternal, perinatal, and early infant death

HIV and Malaria: Associated Reductions in Mean Birth Weight
(grams) Kisumu, Kenya, 1996-99 (N=2,466)
HIV and Malaria: Associated Reductions in Mean Birth Weight
(grams) Kisumu, Kenya, 1996-99 (N=2,466)
Primi-gravidae Multi-gravidae
HIV alone 44 (-32-112) 138 (78-199)
Malaria alone 145 (82-209)* 8 (-71-88)
Dual infection 206 (115-298)* 161 (63-259)
*In Primigravidae, both malaria (RR 2.24, p=0.003) and dual infection (3.45, p<0.001) associated with significant increased relative risk of LBW (< 2,500 grams) compared with uninfected
women
Ayisi et al, AIDS, 2003
Option 3: Wait Until Delivery Time
Option 3: Wait Until Delivery Time
Malarial infection leads to a temporary increase in HIV RNA-- returns to baseline after malaria treatment
Increased viral loads at the time of delivery can increase vertical transmission
But WHO recommends prophylaxis throughout pregnancy, not just at delivery
HIV, Malaria, and Pregnancy
HIV, Malaria, and Pregnancy
Malawi study (1987-1991):
During pregnancy, malaria was more common and of higher density in HIV(+) vs. HIV(-) women
These findings were repeated in other studies and countries -Malawi (2 sites), Kenya (3), Rwanda (1)
Hypothesis: HIV infection decreases previously acquired malarial immunity, especially during first two trimesters of pregnancy
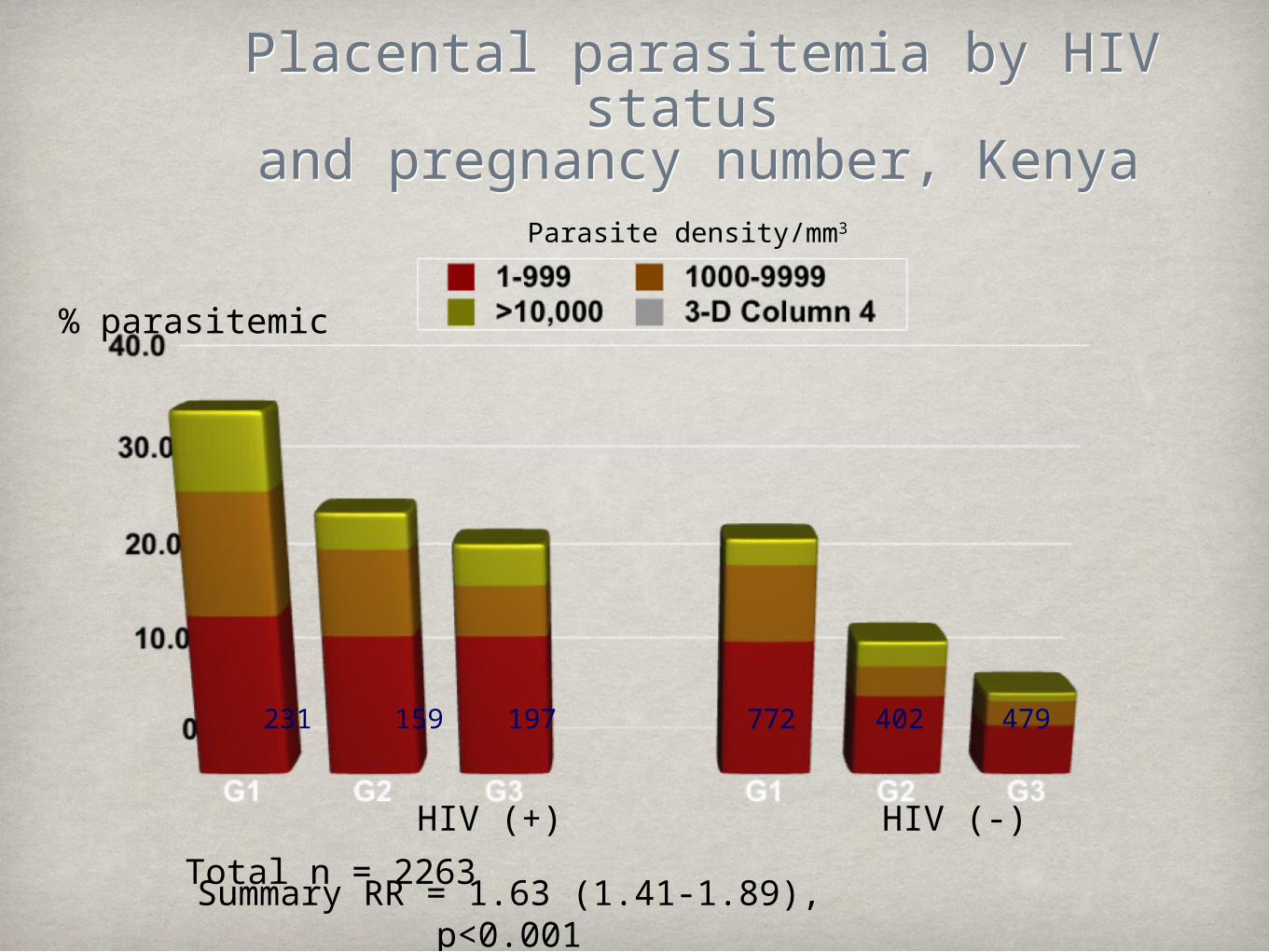
Placental parasitemia by HIV status and pregnancy number, Kenya
Placental parasitemia by HIV status and pregnancy number, Kenya
Parasite density/mm3
% parasitemic
HIV (+) HIV (-)
231 159 197 772 402 479
Total n = 2263Summary RR = 1.63 (1.41-1.89), p<0.001

WHO Recommendations:
HIV and Malaria
WHO Recommendations:
HIV and MalariaIn areas of stable malaria trasnmission: intermittent preventatie antimalarial therapy (IPT)
Most commonly: sulfadoxine-pyrimethamine at interval doses after stat of fetal movement
Studies have shown greater reduction in peripheral parasitemia and increase in mean birth weights with monthly IPT rather than the standard two-course regimen
Use of insecticide-treated bednets
Co-TrimoxazoleCo-TrimoxazoleDaily prophylaxis with Co-trimoxazole has been recommended for all HIV infected pregnant women in sub-Saharan Africa
Used to effectively treat malaria in children
Studies of non-pregnant HIV infected adults on daily co-trimoxazole have shown 70% reductions in the incidence of febrile malaria syndromes
However, risk of adverse drug reactions in HIV + persons is high
Recommendation: In HIV + pregnant women, start daily co-trimoxazole if available and indicated. If not available or not yet indicated, start IPT

Good job, Doc, you’ve answered all their questions, and they’re on their way home. But they’ll be back again soon... with more questions!