case report paraplegia after intercostal neurolysis … · note: the needle tip is seen near the...
TRANSCRIPT

© 2014 Gollapalli and Muppuri. This work is published by Dove Medical Press Limited, and licensed under Creative Commons Attribution – Non Commercial (unported, v3.0) License. The full terms of the License are available at http://creativecommons.org/licenses/by-nc/3.0/. Non-commercial uses of the work are permitted without any further
permission from Dove Medical Press Limited, provided the work is properly attributed. Permissions beyond the scope of the License are administered by Dove Medical Press Limited. Information on how to request permission may be found at: http://www.dovepress.com/permissions.php
Journal of Pain Research 2014:7 665–668
Journal of Pain Research Dovepress
submit your manuscript | www.dovepress.com
Dovepress 665
C A S E R E P O RT
open access to scientific and medical research
Open Access Full Text Article
http://dx.doi.org/10.2147/JPR.S63570
Paraplegia after intercostal neurolysis with phenol
Lakshman GollapalliRudramanaidu MuppuriDepartment of Anesthesiology and Pain Medicine, Wayne State University/Detroit Medical Center, Detroit, MI, USA
Correspondence: Lakshman Gollapalli Department of Anesthesiology, Wayne State University/Detroit Medical Center, 3990 John R Road, Detroit, MI 48201, USA Tel +1 313 745 7233 Email [email protected]; [email protected]
Abstract: In patients with advanced stages of cancer, severe pain is commonly encountered
and is very difficult to treat. It affects the quality of life of the patient and the families involved.
Pain can be managed using analgesics and adjuvant therapy. However, studies have shown that
at least 10%–15% of patients fail to control pain adequately and will experience severe pain.
We discuss the case of a 66-year-old female with metastatic adenoid cystic carcinoma of the left
submandibular gland and developed paraplegia following intercostal neurolysis with phenol.
After a successful diagnostic T6 to T12 intercostal nerve block, the patient was scheduled for
an intercostal neurolytic block. We injected 2 mL of 10% aqueous phenol at each level on the
left from the T6 to T12 ribs. One hour after the procedure, the patient developed bilateral lower
extremity weakness with difficulty moving. A physical examination showed the absence of
sensation to pinpricks and vibration from T10 to S5 and an absence of anal sphincter tone and
sensation. Magnetic resonance images of the thoracic and lumbar spine showed leptomeningeal
metastatic disease and myelitis. We postulate that the paraplegia could be from phenol diffusing
along either the spinal nerves or the paravertebral venous plexus into the subarachnoid space.
This case report points to the risks involved with phenol neurolysis close to the spine, and we
propose alternative methods to minimize neurological complications.
Keywords: intercostal neurolysis, pain, phenol, paraplegia
IntroductionSevere pain is a frequently encountered symptom that affects the quality of life for
advanced cancer patients. It has been estimated that 60%–90% of all patients dying
of cancer will experience pain in the terminal phase of their disease.1–3 Pain can be
managed using analgesics and adjuvant therapy titrated according to the World Health
Organization’s analgesic ladder.4
When pain is resistant to standard therapy or when severe side effects of analgesics
occur, alternative analgesic techniques should be considered. These include regional
nerve blocks, intrathecal analgesic delivery methods, spinal cord stimulation, neu-
rolytic blocks, and vertebroplasty.5 Injections of neurolytic agents to destroy nerves
and interrupt pain pathways have been used for many years.6 In terminally ill cancer
patients, phenol has been administered using the intrathecal or epidural routes for the
blockade of sympathetic ganglia (celiac, superior hypogastric, ganglion impar, and
so on).7 Current knowledge and techniques allow these procedures to be performed
safely and expeditiously, even though the risk–benefit ratio associated with neurolysis
techniques is narrow. The use of phenol for neuroablation for chronic malignant pain
is widely accepted, especially when the life expectancy is low. We discuss a case of
Journal of Pain Research 2014:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
666
Gollapalli and Muppuri
paraplegia followed by phenol intercostal neurolysis for
intractable intercostal neuralgia.
Materials and methodsA 66-year-old Caucasian female was diagnosed with
adenoid cystic carcinoma of the left submandibular gland
in 1997. She had a left radical neck dissection, radiation,
and chemotherapy. In 2005, the patient was diagnosed with
extensive metastases to the pleura, lungs, breast, spleen,
retroperitoneum, and bones. Since 2005, she had multiple
thoracenteses and radiation therapy. The patient complained
of lancinating pain in the left side of the chest, was unrespon-
sive to medical therapy, and was referred to the pain clinic
for interventional management by the oncology care team.
Medical causes of chest pain were ruled out before diagnostic
intercostal nerve blocks were scheduled. She had no signifi-
cant medical problems other than constipation from opioids,
and she had a 20 pack-year smoking history.
The patient was brought to the operating room and was
placed in a prone position. Standard American Society of
Anesthesiologists monitoring was applied, and the patient
received anesthesia with an intravenous midazolam, fentanyl,
and propofol infusion. The patient’s back was prepared and
draped in a sterile fashion. We had decided to proceed with
an intercostal neurolytic block when the patient reported
60%–70% pain relief for about 6–8 hours with a diagnostic
T6 to T12 intercostal nerve block. The left T6 to T12 ribs were
identified 6–7 cm from the midline and marked. The inferior
approach was used to insert a 1.5-inch, 25 gauge needle into
the inferior border of each rib; the needle was advanced until
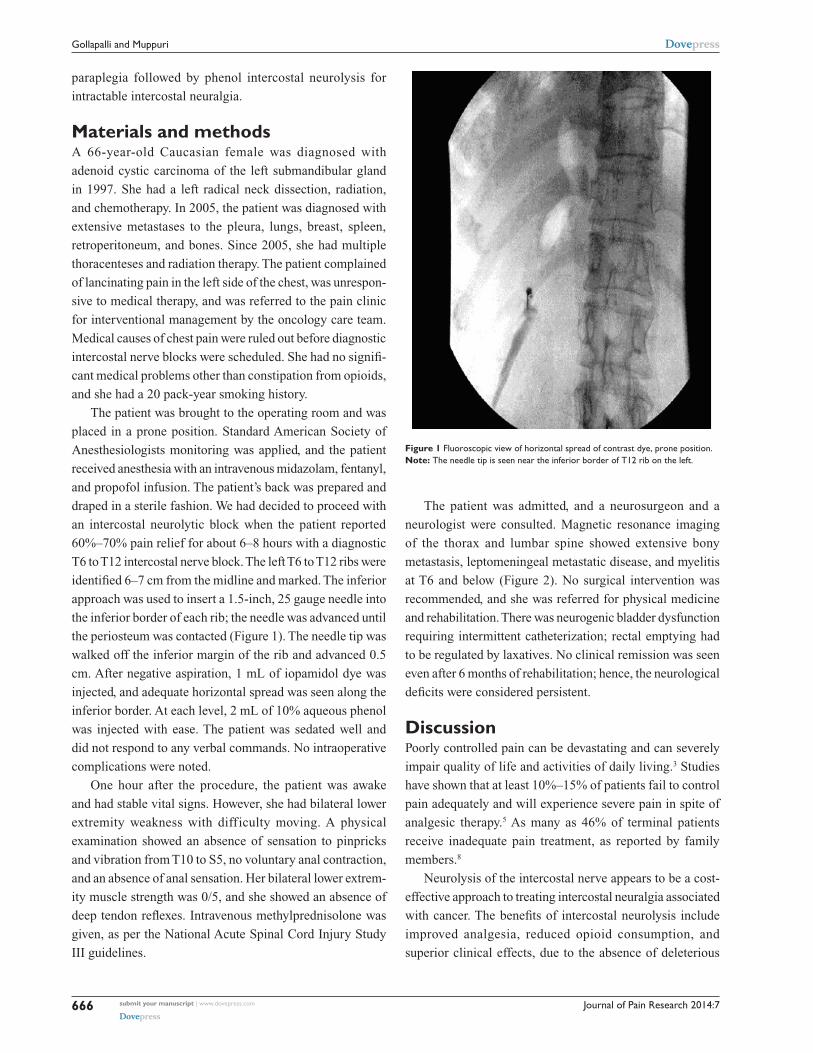
the periosteum was contacted (Figure 1). The needle tip was
walked off the inferior margin of the rib and advanced 0.5
cm. After negative aspiration, 1 mL of iopamidol dye was
injected, and adequate horizontal spread was seen along the
inferior border. At each level, 2 mL of 10% aqueous phenol
was injected with ease. The patient was sedated well and
did not respond to any verbal commands. No intraoperative
complications were noted.
One hour after the procedure, the patient was awake
and had stable vital signs. However, she had bilateral lower
extremity weakness with difficulty moving. A physical
examination showed an absence of sensation to pinpricks
and vibration from T10 to S5, no voluntary anal contraction,
and an absence of anal sensation. Her bilateral lower extrem-
ity muscle strength was 0/5, and she showed an absence of
deep tendon reflexes. Intravenous methylprednisolone was
given, as per the National Acute Spinal Cord Injury Study
III guidelines.
The patient was admitted, and a neurosurgeon and a
neurologist were consulted. Magnetic resonance imaging
of the thorax and lumbar spine showed extensive bony
metastasis, leptomeningeal metastatic disease, and myelitis
at T6 and below (Figure 2). No surgical intervention was
recommended, and she was referred for physical medicine
and rehabilitation. There was neurogenic bladder dysfunction
requiring intermittent catheterization; rectal emptying had
to be regulated by laxatives. No clinical remission was seen
even after 6 months of rehabilitation; hence, the neurological
deficits were considered persistent.
DiscussionPoorly controlled pain can be devastating and can severely
impair quality of life and activities of daily living.3 Studies
have shown that at least 10%–15% of patients fail to control
pain adequately and will experience severe pain in spite of
analgesic therapy.5 As many as 46% of terminal patients
receive inadequate pain treatment, as reported by family
members.8
Neurolysis of the intercostal nerve appears to be a cost-
effective approach to treating intercostal neuralgia associated
with cancer. The benefits of intercostal neurolysis include
improved analgesia, reduced opioid consumption, and
superior clinical effects, due to the absence of deleterious
Figure 1 Fluoroscopic view of horizontal spread of contrast dye, prone position.Note: The needle tip is seen near the inferior border of T12 rib on the left.

Journal of Pain Research 2014:7 submit your manuscript | www.dovepress.com
Dovepress
Dovepress
667
Paraplegia after intercostal neurolysis
properties of high-dose chronic opioid therapy. Pain practitio-
ners have been performing these blocks as a part of adjuvant
therapy for the optimal treatment of cancer pain.
Phenol, also known as carbolic acid and as hydroxy-
benzene, was introduced in the 1950s.9 It is a colorless,
crystalline substance that has a characteristic odor and is
soluble in water and organic solvents. It has been in use
for neuroablation in chronic cancer pain for a long time.
However, because of the complications that phenol causes,
its use for chemical neurolysis for chronic noncancer pain
is less common. When injected near motor nerves, phenol
can produce flaccid paralysis and might also cause systemic
complications, such as nausea and vomiting, central nervous
system stimulation, cardiovascular depression, and cardiac
arrhythmias.10 Phenol can diffuse from the paravertebral gut-
ter through the intervertebral foramina toward the epidural
space, and then to the cerebrospinal fluid to cause persistent
paraplegia.11
Invasive use of phenol has been shown to cause irre-
versible neural tissue damage, and several complications
have been reported.10,12 There was one case report in which
a patient had persistent paraplegia following an intercostal
block with a 7.5% aqueous phenol solution.11
In our case, the patient could have developed
paraplegia from the diffusion of the phenol along the
spinal nerves or the paravertebral venous plexus into the
subarachnoid space. It is unlikely to be intravascular,
since the symptoms presented about an hour after the
procedure. There is a possibility that rapid infusion of
the drug could have forced the solution to diffuse faster
into the spinal space, even though only 2 mL of phenol
had been used. Paraplegia could also occur from verte-
bral or lymph node metastases or though direct extension
from adjacent primary tumors, such as lung carcinoma,
or through leptomeninges, thereby damaging the motor
and sensory roots in leptomeningeal metastatic disease.
The phenol intrathecal elimination half-life is 8 minutes,
as revealed from the Renografin® solution in monkeys.7
Slow diffusion of phenol through the leptomeninges
at multiple levels leads to neurological damage. Deep
sedation masked the immediate effects of neurological
damage in our case. Leptomeningeal carcinomatosis that
involves the spinal nerves often has a nodular appearance
in which tumor foci appear as a string of beads throughout
the cauda equina and extend out of the nerves into the
neural foramina. Along the spinal cord, a leptomeningeal
tumor typically presents as a thin coating along the pia
mater, although nodularity and diffuse involvement of the
arachnoid space also can occur.
These are some alternative methods to minimize the
neurological complications with intercostal neurolysis in
leptomeningeal metastatic disease:
1. Especially for the blockade of peripheral nerves near the
spine, lipid phenol should be used instead of aqueous
solutions, because diffusion and unwanted damage can-
not be excluded reliably.11 (The use of phenol solutions
in water may result in 50 times higher toxicity than that
of lipid phenol.)13
2. For leptomeningeal metastatic disease, radiofrequency
neuroablation is an alternative treatment method to
phenol for intercostal neurolysis, which is used in the
treatment of the most common chronic nonmalignant
pain syndromes.14
3. Intercostal neurolysis should be performed at the midaxil-
lary line,15,16 far from the costovertebral joint.
4. Mild sedation with patient communication during the
intercostal neurolysis procedure minimizes the chance
of developing permanent neurological damage.
Figure 2 Magnetic resonance images of the thoracic spine, sagittal view, different sections, showing the thoracic body involvement.Note: Extensive metastatic disease of the vertebral body can be seen.

Journal of Pain Research
Publish your work in this journal
Submit your manuscript here: http://www.dovepress.com/journal-of-pain-research-journal
The Journal of Pain Research is an international, peer-reviewed, open access, online journal that welcomes laboratory and clinical findings in the fields of pain research and the prevention and management of pain. Original research, reviews, symposium reports, hypoth-esis formation and commentaries are all considered for publication.
The manuscript management system is completely online and includes a very quick and fair peer-review system, which is all easy to use. Visit http://www.dovepress.com/testimonials.php to read real quotes from published authors.
Journal of Pain Research 2014:7submit your manuscript | www.dovepress.com
Dovepress
Dovepress
Dovepress
668
Gollapalli and Muppuri
ConclusionThis case highlights the risk associated with aqueous phenol
application in the vicinity of the spinal cord for leptomenin-
geal metastatic disease. We recommend that patient selection
prior to the interventional pain treatment is very important.
We also recommend that alternative methods be used for
intercostal neurolysis in leptomeningeal metastatic disease
patients whenever possible.
DisclosureThe authors report no conflicts of interest in this work.
References1. Keefe FJ, Abernethy AP, C Campbell L. Psychological approaches to
understanding and treating disease-related pain. Annu Rev Psychol. 2005;56:601–630.
2. Portenoy RK. Cancer pain. Epidemiology and syndromes. Cancer. 1989;63(Suppl 11):2298–2307.
3. Christo PJ, Mazloomdoost D. Cancer pain and analgesia. Ann N Y Acad Sci. 2008;1138:278–298.
4. Cancer pain relief and palliative care. Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1990;804:1–75.
5. Sloan PA. The evolving role of interventional pain management in oncology. J Support Oncol. 2004; 2(6):491–500, 503.
6. Maher RM. Intrathecal chlorocresol in the treatment of pain in cancer. Lancet. 1963;281(7288):965–967.
7. Concilus RR, Sehlhorst CS, Denson DD, Katz J, Gregg RV. Dural transfer of phenol following epidural injection in cynomologus monkeys [abstract]. Anesthesiology. 1988;69(3A):A399.
8. Tolle SW, Tilden VP, Rosenfeld AG, Hickman SE. Family reports of barriers to optimal care of the dying. Nurs Res. 2000;49(6):310–317.
9. Patt RB. Cancer Pain. Philadelphia, PA: Lippincott Williams & Wilkins; 1993.
10. Superville-Sovak B, Rasminsky M, Finlayson MH. Complications of phenol neurolysis. Arch Neurol. 1975;32(4):226–228.
11. Kowalewski R, Schurch B, Hodler J, Borgeat A. Persistent paraplegia after an aqueous 7.5% phenol solution to the anterior motor root for intercostal neurolysis: a case report. Arch Phys Med Rehabil. 2002; 83(2):283–285.
12. Galizia EJ, Lahiri SK. Paraplegia following coeliac plexus block with phenol. Case report. Br J Anaesth. 1974;46(7):539–540.
13. Cain HD. Subarachnoid phenol block in the treatment of pain and spasticity. Paraplegia. 1965;3(2):152–160.
14. Van Zundert J, Raj P, Erdine S, van Kleef M. Application of radiof-requency treatment in practical pain management: state of the art. Pain Pract. 2002;2(3):269–278.
15. Scott DB. Techniques of Regional Anesthesia. 2nd ed. Norwalk, CT: Appleton and Lange; 1995.
16. Kreuscher H. Regionale Schmerztherapie. In: Niesel HC, editor. Regionalana¨sthesie, Lokalana¨sthesie, Regionale Schmerztherapie. Stuttgart, Germany: Georg Thieme; 1994:709–761.