case report- hemoptysis
TRANSCRIPT

CasePresentation
內科intern吳易儒

Basic data
Name: 廖OO
Age: 47y/o
Gender: Male
Admission: 6.17/2014Education: Junior high school
Occupation:包工程水電行
Chart number: 41840334

Chief complaint
Hemoptysis for 2 days

Present illness
● This 47 y/o male with history of liver cirrhosis and HBV infection was admitted to our ER due to hemoptysis for 2 days.
● As the statement of him, he has followed up his liver disease in our OPD. But he lost followed up since 2011.

● Half a year ago, he would have been choked sometimes while drinking water. Bleeding after taking food and dysphagia were mentioned, too.
● About 2 weeks ago, a left submandibular mass was noted by him. Also, he complained about tarry stool.

Present illness
● nausea(-)● vomiting (-)● dizziness (-)● nosebleed(-)● dyspnea(-)● chest tightness(-)
● fever(-)● cold sweating(-)● abdominal pain(-)● cough(-)● dysuria(-)● anti-coagulant use
(-)
● He suffered from hemoptysis since 2 days ago. Therefore, he went to our ER.

Past medical history
Hospitalization: 2010.3.3 -3.152011.5.6 -5.142011.8.27 -9.5 GI bleeding-> Esophageal Varices s/p EVL

Personal history
Allergy: noneAlcohol: heavy drinkiner(維士比)Betal nut: yesCigarette: 0.5ppd for 20 yearsTravel history: deniedFamily history: Father had DM type II

Physical examinationGCS: E4M6V5 T/P/R: 37.7/104/25 BP: 101/68HEENTEyes-Conjunctiva: pale
-Cornea:yellowNeck-General:left neck big mass

Physical examination-Carotid pulses:regular , normal amplitude,
no bruits. -Jugular vein:no engorgement
Chest and Lungs-Inspection:normal thoracic cage, normal
expansion, no spider nevi.-Palpation:equal tactile fremitus.-Percussion:resonance to both lung field -Auscultation:clear
Physical examination
Heart-Inspection/palpation:PMI over the L't 5th
ICS mid-clavicular line, no LV heaves.-Auscultation:regular rhythm, normal S1,
loud S2, no S3, S4 or opening snap.
Abdomen-Inspection:no scars,no spider nevi, RUQ
superficial vein engorgement.

Physical examination
-Auscultation:normoactive bowel sounds , no bruits.
-Percussion:no shifting dullness . tympanic percussion
-Palpation:no tenderness ,no Murphy's sign, soft, no muscle guarding,no rebound tenderness, no mass.no hepatomegaly ,no splenomegaly
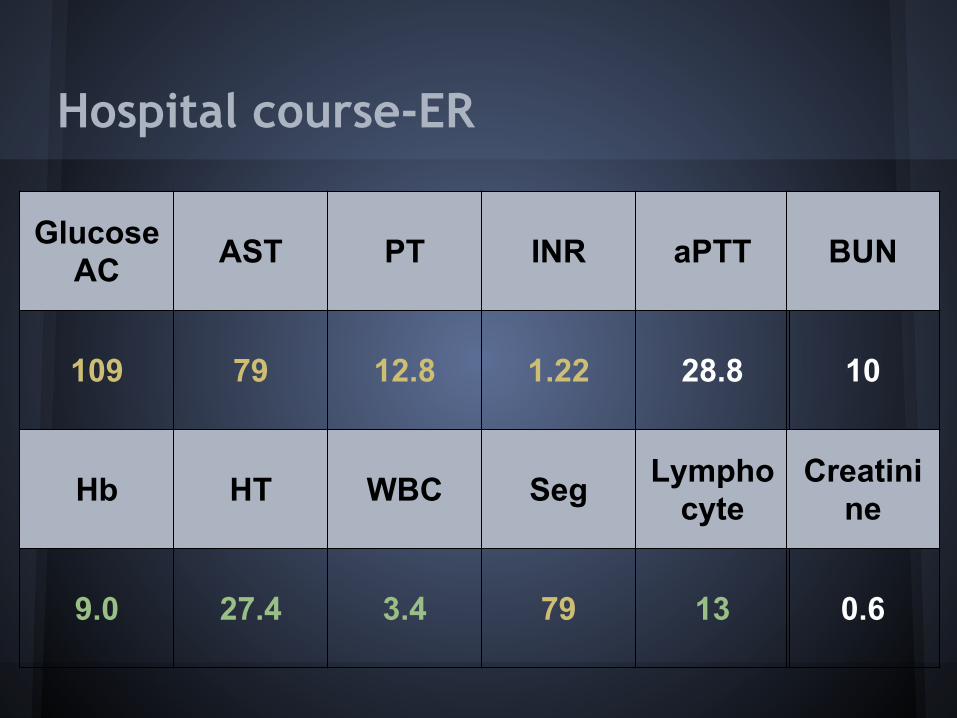
Hospital course-ER
Glucose AC AST PT INR aPTT
109 79 12.8 1.22 28.8
Hb HT WBC Seg Lymphocyte
9.0 27.4 3.4 79 13
BUN
10
Creatinine
0.6


ENT consultation 6/16 12:22ENT finding: Lt neck level II mass 2x2 cm, firm, non-movableLt parapharyngeal wall tumor with ulceration, no active bleedingA: oropharyngeal tumor r/o EV or GI bleeding Liver cirrhosisP: please trerat medical problem as your expertise 1. arrange PES 2. arrange neck CT or MRI with /without contrast including hypopharynx 3. ENT OPD f/u for further evaluation






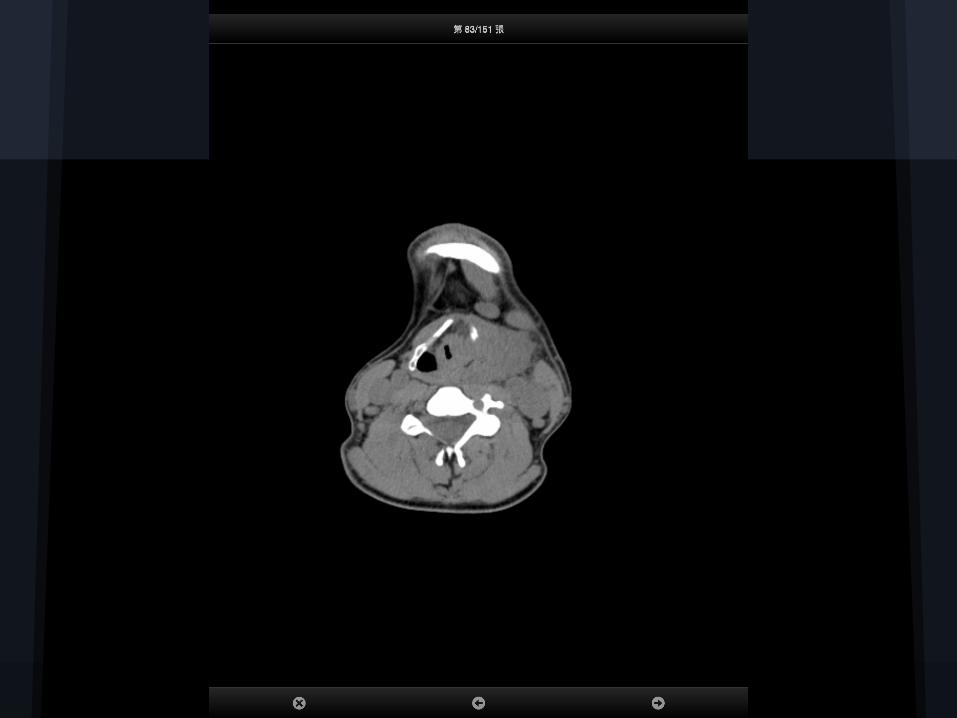
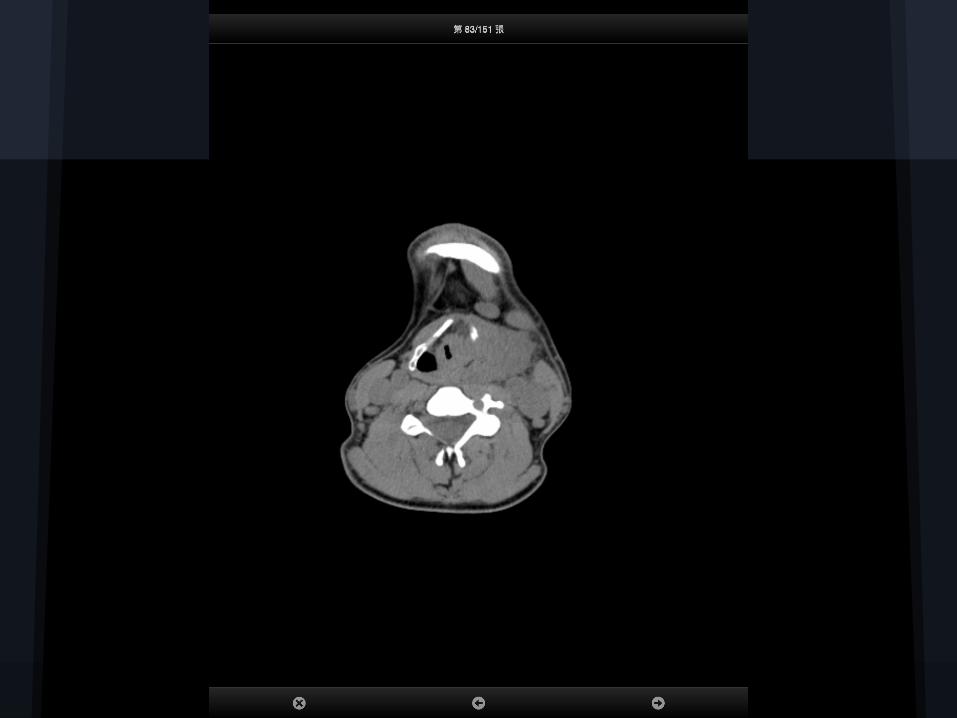

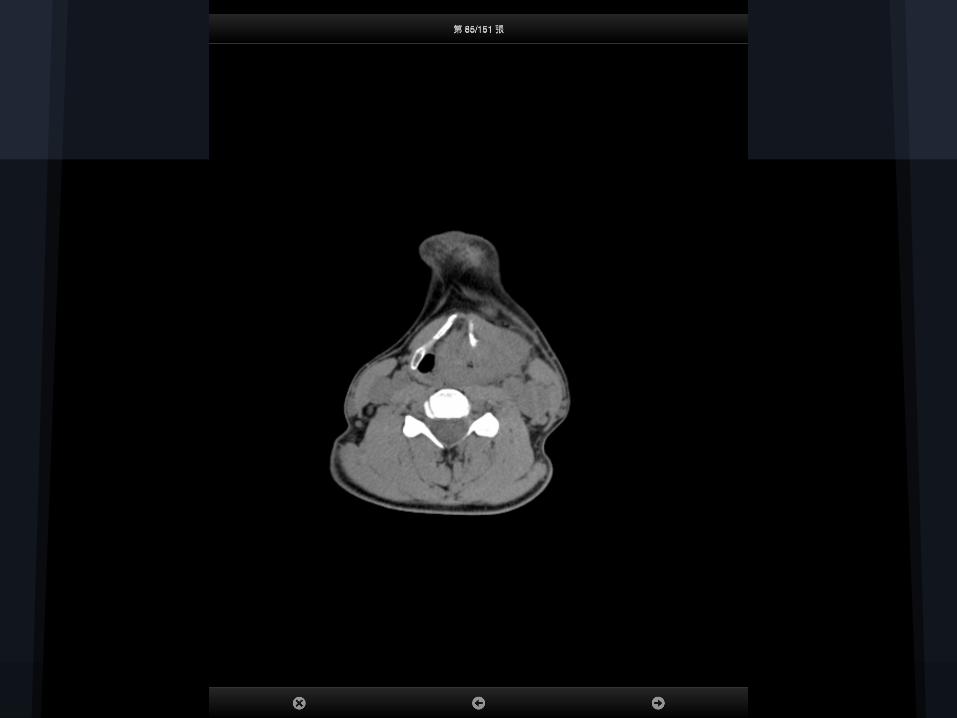




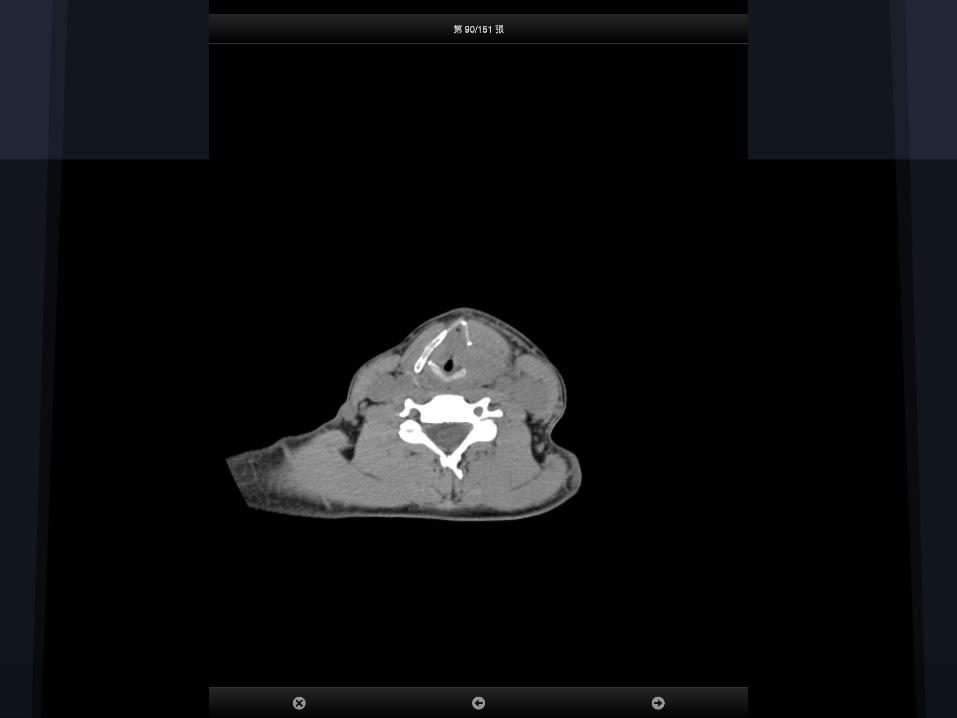


CT report
● Evidence of bulky tumor involving left lateral oropharyngeal, hypopharyngeal and laryngeal walls. The origin is hard to defined.
● Enlarged lymph nodes are noted at submental area, left lateral retrophryngeal space and along left internal jugular chain, level II

Gastroscopy 2014/06/16 14:36:42
● Active bleeding in the left epiglottis. ● Suggest ENT for hemostasis and intubation
as needed for high risk of suffocation.


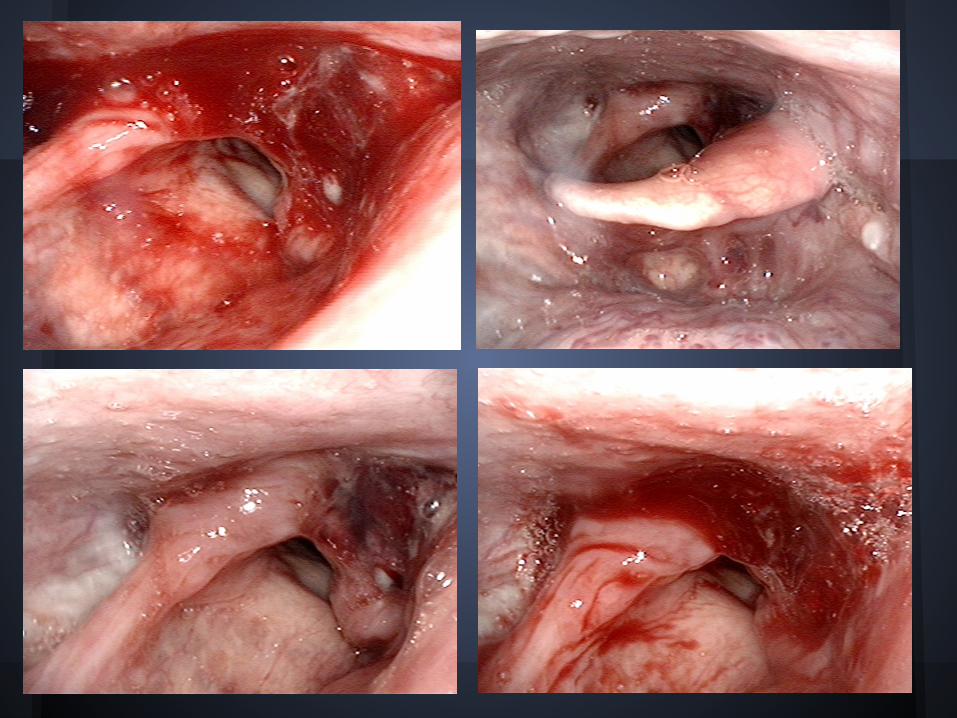
Laryngeal scope 2014/06/16 18:08:55
Left hypopharyngeal ca with ulceration and blood clot, no active bleeding Left vocal palsy Airway compromise【Diagnosis】 Left hypopharyngeal ca Suspected GI bleeding【Comment】 Protect airway Embolization if needed


Hospital course-ER ABG 60% PEEP 5
pH PaCO2 PaO2
7.553 28.3 178.8
SaO2
99.4%
HCO3 BE
24.3 3.1

Tentative diagnosis
● •Suspect left hypophargeal cancer with ulceration and active bleeding s/p endotracheal intubation for protect airway
● Anemia, related tumor bleeding● EV s/p ligation without active bleeding● Liver cirrhosis, child A● History of gastric ulcer

MICU Hospital course
● NG irrigation● Blood transfusion on 6/17-> Hb rise from 7.7 to 9.7● NPO● CVP for nutrition
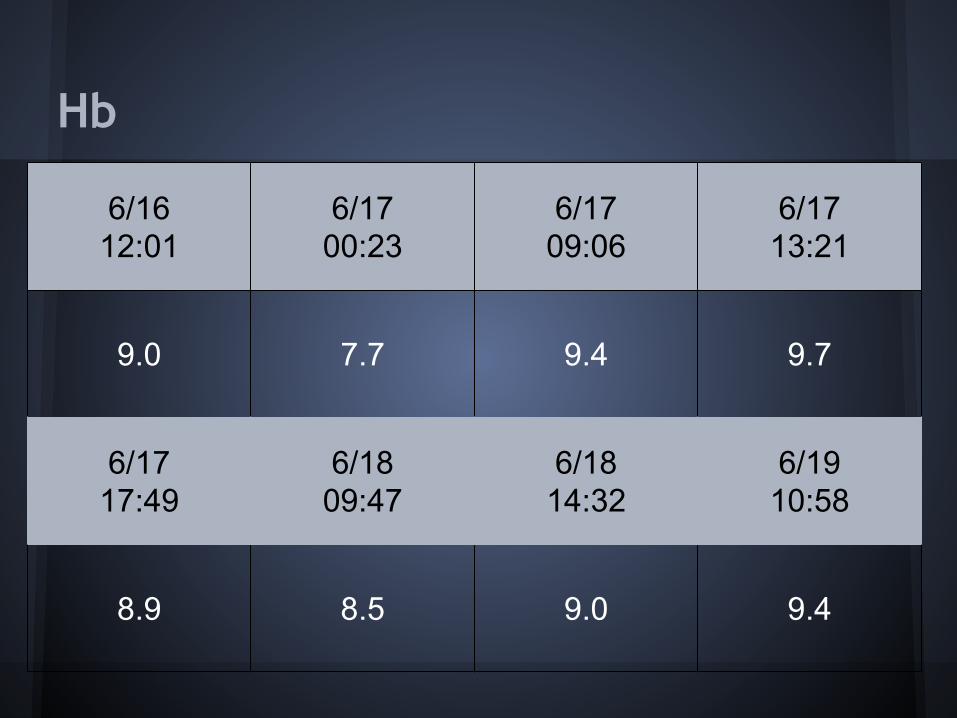
Hb
6/1612:01
6/17 00:23
6/1709:06
6/1713:21
9.0 7.7 9.4 9.7
6/1717:49
6/1809:47
6/1814:32
6/1910:58
8.9 8.5 9.0 9.4

Gastroscopy 6/17 21:23pm
ESOPHAGUS1.One protruding mass with blood coating and friable
mucosal change at the left side of epiglottis are noted. Mild oozing is found. One pseudo-tract is noted below the right side of pyriform sinus (located upper of the esophageal opening).
2.Two varices (2F1, Cb, Li, RCS(-)) and one fibrotic ring are noted at the EC junction.STOMACH
1.Superficial Gastritis 2.Ulcer

Hb
6/1612:01
6/17 00:23
6/1709:06
6/1713:21
9.0 7.7 9.4 9.7
6/1717:49
6/1809:47
6/1814:32
6/1910:58
8.9 8.5 9.0 9.4

HT Albumin Total Bilirubin
Direct Bilirubin AST
29.3 2.7 2.7 1.0 72
Ammonia Glucose AC K P Ca Mg
131 120 3.3 1.6 7.7 1.3

MICU Hospital course
Chest echo: Left lung consolidationFever up to 38.2 degreeBlood culture: GPCArrange tracheotomy and biopsy to evaluate the neck mass



Medicine
● Esomeprazole for peptic ulcer● Glypressin for suspect GI bleeding● Metoclopramide for GI bleeding● Silymarin for liver cirrhosis● 6/18 T-piece ● 6/20 transfer to general ward.
Discussion

Neck mass

History taking
AGEPediatric(16-40)-inflammatory or congenitalAdult(>40)-neoplastic(tobacco/alcohol)
GROWTH PATTERNDuration-longer betterRapidly-infection/lymphomaFluctuate-viral/URI infection/congenital
SYMPTOMS Cervical meta-pain/hoarseness/dysphagia/otalgia
OTHER fever/BW loss/TOCC

Location

Physical examination
● Characteristicslocation, size, shape, consistency, tenderness, mobility, and color
● Oral Mucosa● Ear● Oropharyngeal● Skin● Cranial nerve● Thyroid gland● Abdomen
Labtory studies
● MostCBC
Infection/InflammationESR, CRP, Blood culture, EBV/CMV(adenopathy)
Specific serlogyT gondii, Bartonella, Tularemia, TB skin test
Bone marrow biopsyhematologic malignancy

Image study
● Ultrasoundguide fine needle aspiration● CTindentify primary sourcepossible vascular origin● MRIsoft tissue tissueperineural/CNS● PETdetect distant metastasisnot sensitive in neck mass

Diagnostic studies
● Fine needle aspiration(FNA)Cytology, Virus(EBV/HPV)
● Core biopsyUltrasound-guided/CT guided
● Excisional/incisional biopsyFrozen section analysis


Thanks for your attention

Hemoptysis


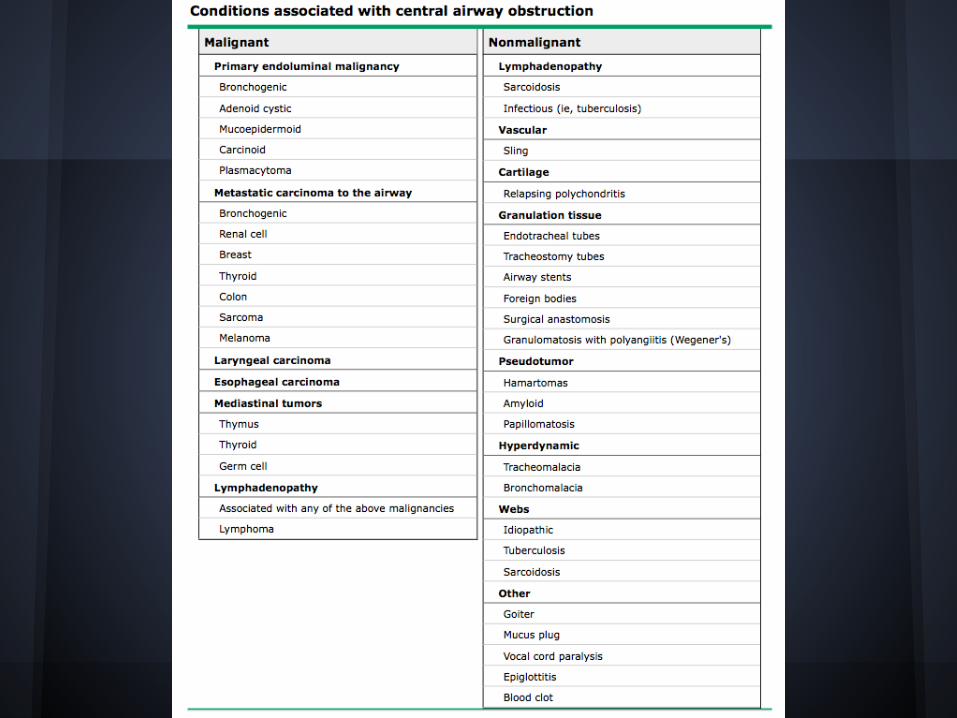
Airway obstruction