case report epidural bleeding after acl reconstruction ... · epidural bleeding after acl...
TRANSCRIPT
Case report
Open Access
Epidural bleeding after ACL reconstruction under regionalanaesthesia: a case reportNikolaos T Roidis*, Lazaros A Poultsides, Nikolaos E Gougoulias,Paraskevi D Liakou, Theofilos S Karachalios and Konstantinos N Malizos
Address: Department of Orthopaedics and Trauma Surgery, University of Thessaly, Larissa, Hellenic Republic
Email: NR* - [email protected]; LP - [email protected]; NG - [email protected]; PL - [email protected]; TK - [email protected];KM - [email protected]
*Corresponding author
Published: 26 May 2009 Received: 21 March 2009Accepted: 8 April 2009
Cases Journal 2009, 2:6732 doi: 10.1186/1757-1626-2-6732
This article is available from: http://casesjournal.com/casesjournal/article/view/6732
© 2009 Roidis et al; licensee Cases Network Ltd.This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0),which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Introduction: Epidural bleeding as a complication of catheterization or epidural catheter removal isoften associated with perioperative thromboprophylaxis especially in adult reconstructive surgery.
Case presentation: We report on a case of a 19 years old male athlete that underwent anteriorcruciate ligament reconstruction, receiving low molecular weight heparin for thromboprophylaxisand developed an epidural hematoma and subsequent cauda equina syndrome two days after removalof the epidural catheter. An urgent magnetic resonance imaging scan revealed an epidural hematomafrom the level of L3 to L4. Emergent decompression and hematoma evacuation resulted in patient’ssignificant neurological improvement immediately postoperatively.
Conclusion: A high index of clinical suspicion and surgical intervention are necessary to preventsuch potentially disabling complications especially after procedures on a day-case basis and earlypatient’s discharge.
IntroductionSpinal epidural haematoma formation as a consequenceof epidural catheterization is a rare (e.g. between 1:150000and 1:190000) but devastating complication [1] and maylead to permanent paraplegia if hematoma evacuation isnot performed early after symptom onset [2]. We report ona case of a young male athlete that underwent ACLreconstruction, receiving LMWH for thromboprophylaxisand developed an epidural hematoma and subsequentcauda equina syndrome two days after removal of theepidural catheter.
Case presentationA 19 years old Caucasian male (soccer player) presentedwith an anterior cruciate ligament (ACL) rupture of hisright knee two months ago. He was admitted in ourDepartment for an arthroscopic ACL reconstruction. Hismedical history was unremarkable (young athlete) and hereported no medication intake. Preoperative examinationdid not reveal any disorders and the values of PT(Prothrombin time), aPTT (activated Partial Thrombo-plastin time), INR and platelet count were normal. Anepidural catheter was inserted prior to the operation to
Page 1 of 6(page number not for citation purposes)
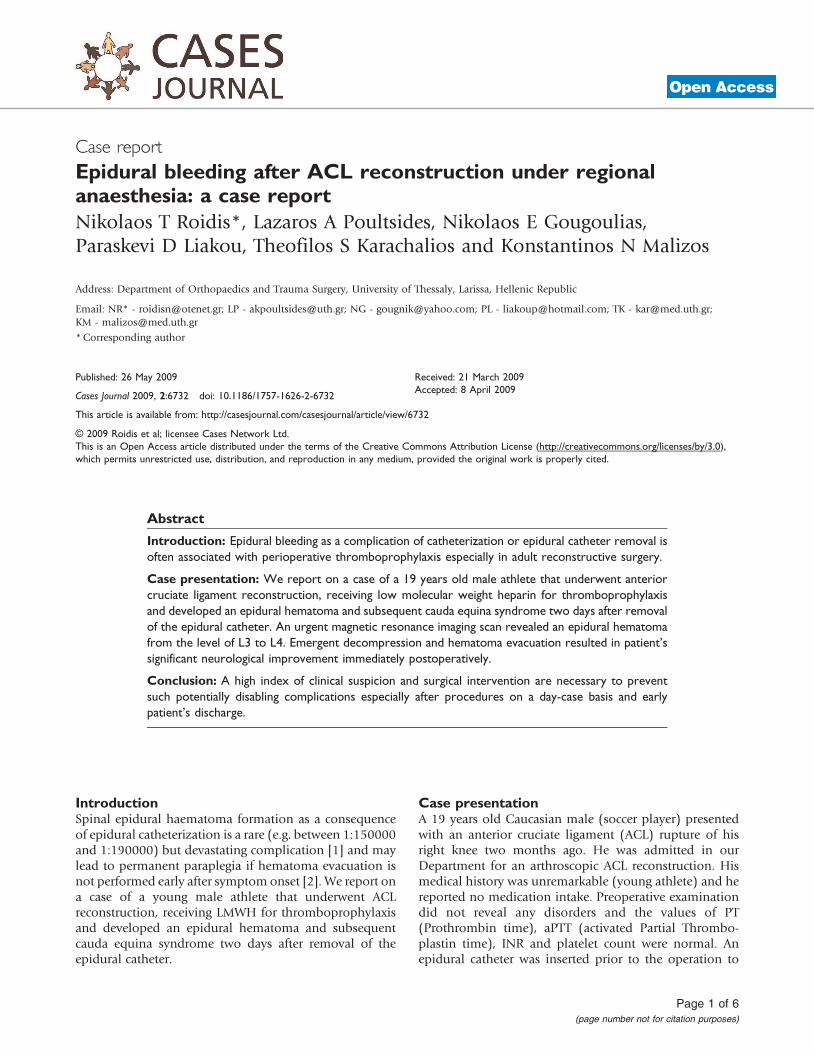
provide analgesia postoperatively. Its insertion was quickand easy without any complications as described by theanesthesiologists in charge. The operation was completeduneventfully (75 minutes), regarding both intraoperativeanesthesia and the surgery (hamstrings autografts, Endo-button CL, Smith & Nephew, Memphis, Tennessee, USA)and the patient was transferred to the recovery room(Figure 1). During his staying in the recovery room(approximately one hour), he remained hemodynamicallystable without any complaints, regaining gradually hismuscle strength and sensitivity, and then was transferredto the ward. Anticoagulative treatment started six hourafter the end of the operation as in all patients withreconstructive knee surgery and consisted of administra-tion of low molecular weight heparin (LMWH) (Tinza-parine Sodium 4500- anti-Factor Xa IU once daily). Bloodloss was not significant and the drain was removed the firstpostoperative day. Analgesia was provided through theepidural catheter for 48 hours andmobilization started thesecond postoperative day. The epidural catheter was
removed the second postoperative day, 12 hours afterthe administration of the anticoagulative injection and12 hours before the next dose, and the patient was placedon oral analgesics when it was needed. The day of surgeryand the first postoperative day he reported a minor loss ofsensitivity and numbness in both lower extremities whichimproved till the second postoperative day. At this point,neurological status was normal andmobilization (walkingwith canes with the knee in an extension brace) continuedwithout any adverse events. The third postoperative day,after the regular morning visit, the patient was dischargedbeing able to ambulate independently without any aid.On the afternoon, he reported moderate loss of sensitivity,perianal and perigenital numbness and muscle weaknessin his lower extremities, and low back pain, whichimproved after the administration of one dose of500 mg of paracetamol. The fourth postoperative day thepatient reported muscle weakness in all muscles of hislower extremities and deteriorating loss of sensitivity(from level L1 to S5) which made his mobilization
Figure 1. MRI view shows the raptured ACL. Post-op x-rays of the final result.
Page 2 of 6(page number not for citation purposes)
Cases Journal 2009, 2:6732 http://casesjournal.com/casesjournal/article/view/6732

difficult. He was admitted again in our department;neurologic evaluation revealed at this point muscleweakness in all muscle groups of the lower extremities.According to British Medical Research Council (MRC)scale (Medical Research Council) [3] muscle strength wasrated as 3 for iliopsoas, 3 for quadriceps, 3 for hamstrings,3 for anterior and 3 for the posterior tibial muscles. Thepatient remained hospitalized, his neurological statusworsened rather than improving and the fifth post-operative day, a dose of IV cortisone was administered(30 mg/kg MPS). An epidural hematoma was suspectedand the administration of low molecular weight heparinceased; an urgent MRI scan was ordered which revealed anepidural hematoma from the level of L3 to L4 (Figure 2).Prothrombin time (PT), activated partial thromoblastintime (aPTT) and INR continued to be normal. Immedi-ately, the patient was prepared emergently for theoperating room (fifth postoperative day). It is worthmentioning that during patient’s preparation in theoperating room, just prior to the administration of
anaesthesia, a new clinical evaluation showed againworsening of the muscle weakness. In more details,muscle strength was rated as 2 according to MRC scale inall muscle groups: 2 (iliopsoas, quadriceps, hamstrings) or2 (anterior and posterior tibial muscles). The patient hadalso lost control of the sphincters, was almost paraplegic,unable even to move legs in bed with significant loss ofsensation all over his lower extremities and in perianal andgenitary region (cauda equine establishment).
Consequently, an emergent decompression through rightfenestration at the level of the hematoma was performed(L3 and L4 vertebrae) without disturbing the facets and thevertebral canal was explored. An extensive clot, which wascompressing the dura and its contents had been formed.The hematoma was meticulously evacuated. No bleedingvessels were identified. The wound was closed withoutfusion of the spine. A bolus dose of methylo-prednizolone(1000 mgr of Solumedrol in one hour) was administeredto the patient in the recovery room.
Figure 2. MRI scans show the epidural hematoma at the level of L3-L4.
Page 3 of 6(page number not for citation purposes)
Cases Journal 2009, 2:6732 http://casesjournal.com/casesjournal/article/view/6732
In the ward, the patient presented significant improve-ment; he could mobilize his legs without pain and his lossof sensation and numbness were improving continuously.He remained in bed for two days and he was regularlyevaluated neurologically. The first day after decompres-sion the patient showed significant neurological improve-ment with increased muscle strength. Improvementcontinued and at day 2 post-decompression the patientcould move his legs freely in bed and consequently wasmobilized. At day 3 postoperatively he could stand aloneand make a few steps with a walker without anycomplaints; his recovery was complete. It is worthmentioning that genitary loss of sensation was the last todisappear. According to MRC scale at day 3 musclestrength was rated as normal for all muscle groups ofboth lower extremities. The patient was discharged fromhospital at day 5 post-fenestration and was re-evaluated1 week later (day 12 after fenestration). He presentedwithout any neurologic deficit at all and range of motion
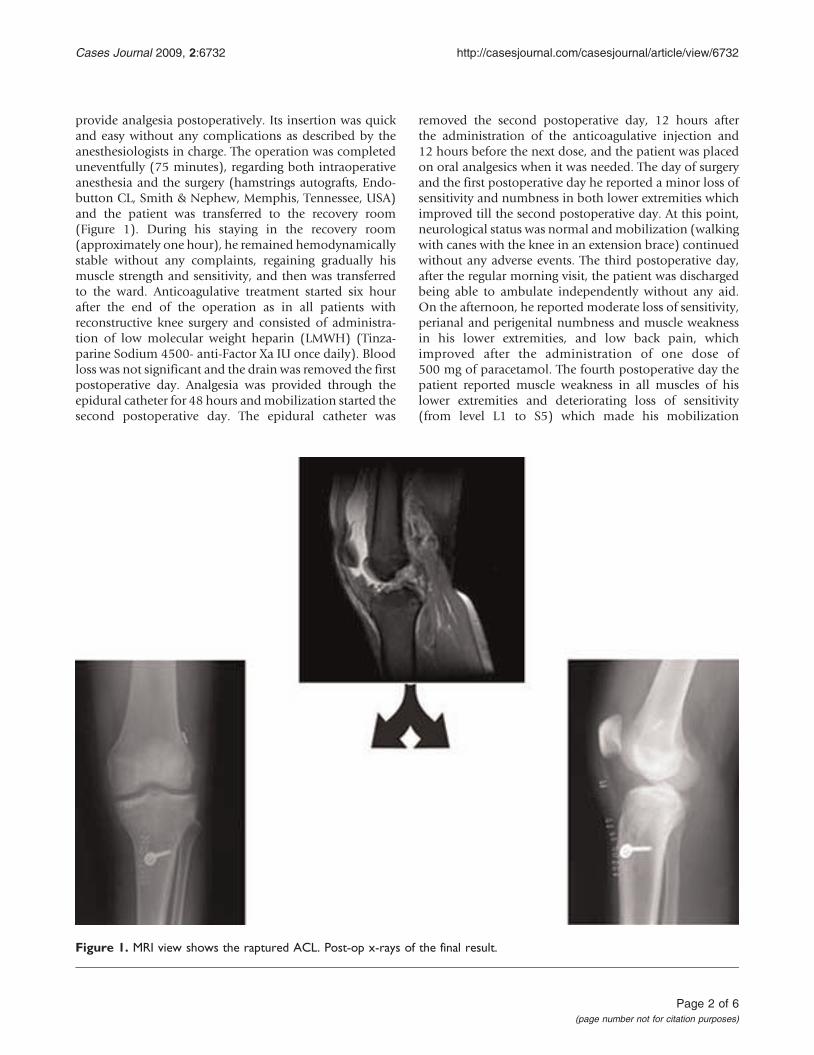
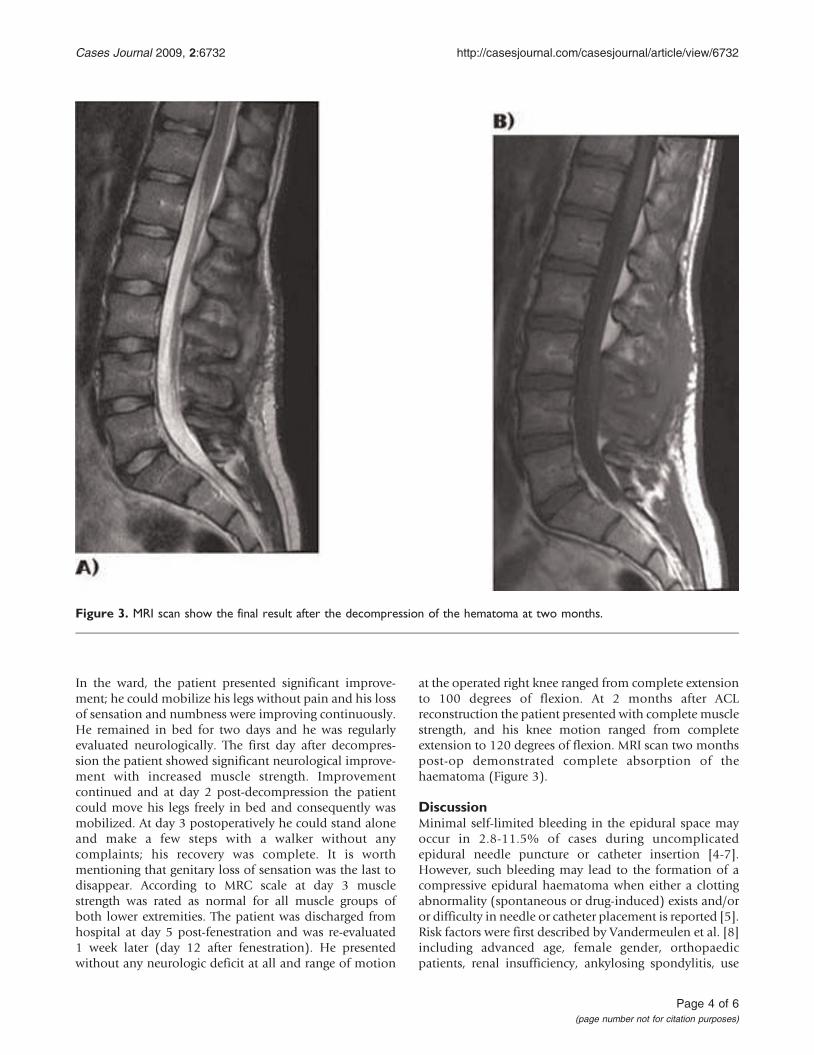
at the operated right knee ranged from complete extensionto 100 degrees of flexion. At 2 months after ACLreconstruction the patient presented with complete musclestrength, and his knee motion ranged from completeextension to 120 degrees of flexion. MRI scan two monthspost-op demonstrated complete absorption of thehaematoma (Figure 3).
DiscussionMinimal self-limited bleeding in the epidural space mayoccur in 2.8-11.5% of cases during uncomplicatedepidural needle puncture or catheter insertion [4-7].However, such bleeding may lead to the formation of acompressive epidural haematoma when either a clottingabnormality (spontaneous or drug-induced) exists and/oror difficulty in needle or catheter placement is reported [5].Risk factors were first described by Vandermeulen et al. [8]including advanced age, female gender, orthopaedicpatients, renal insufficiency, ankylosing spondylitis, use
Figure 3. MRI scan show the final result after the decompression of the hematoma at two months.
Page 4 of 6(page number not for citation purposes)
Cases Journal 2009, 2:6732 http://casesjournal.com/casesjournal/article/view/6732

of anticoagulants and coagulopathy, difficult catheterinsertion and catheter removal. Epidural venous plexihave been suggested as the source of haemorrhage, asepidural veins are more susceptible to rupture afteractivities that transiently raise venous pressure such asmild exercise, coughing, straining, or other vasalvamanoeuvres [9]. Case series from the last few yearsindicate that spinal epidural haematoma is more commonthan previously estimated, with a prevalence from1:100000 in obstetric patients to as high as 1:3600 infemale orthopaedic patients [6,10]. Epidural bleeding as acomplication of catheterization is often associated withthe use of perioperative thromboprophylaxis [5,8,10-16].Guidelines regarding safe time intervals for epiduralcatheterization and catheter removal, adopted by manycountries, do exist; however they are not evidence basedand rely mainly on published reports regarding relevantrisks and on drugs pharmacokinetics [12,13]. LMWHadministration to prevent deep vein thrombosis has beenimplicated in the USA for the high-incidence of bleedingafter central neural blockade, since the introduction ofenoxaparin use in 1993. However similar complicationrates in Europe were not observed probably due to thedifferent dosage regimes used in the two continents [17].As the plasma half-life of LMWH is 4-6 h, 10-12 h is nowthe recommended safe time interval following LMWHprophylaxis for placement of a central neuraxis or removalof an epidural catheter [5]. Although standard doseLMWHs are associated with a predictable anticoagulanteffect considering that the anti-Xa activity after a singlebolus of 40 mg enoxaparine for example has nearlyreturned to baseline after 12 h in patients with normalrenal function [18], the risk of unexpected bleeding cannotbe excluded [12,19]. It is important to mention thatdespite existing awareness in a review of 613 cases withspinal haematoma, no clear aetiologic factors wereconfirmed in about 1/3 of patients [19].
Our patient, a 19 years old young athlete, with a free pastmedical history, no indication of coagulopathy, normalrenal and liver function, no spinal pathology who under-went a typical epidural catheterization and receivedstandard dose LMWH postoperatively was exactly thepatient where this rare complication would be more thanunexpected. Furthermore, the epidural catheter wasremoved 12 hours after last dose of LMWH and12 hours before the next dose was administered. Initiallythe patient mobilized uneventfully and experiencedsymptoms of low-back pain, bladder incontinence andsensory and motor dysfunction, worsening in severity twodays later. A published case of, similarly to ours, latepresentation of epidural bleeding [16], 6 days aftercatheter removal in an 82-years old patient receivinghigh dose (0.8 mg/kg twice daily) enoxaparin, was
attributed to his altered coagulation status. In two recentreports [11,15] of epidural bleeding after catheterizationin three orthopaedic patients, the complication was aconsequence of a) preoperative anticoagulant therapy(long-standing dipyridamole [15] and warfarin [11]treatment) in patients undergoing TKA, or b) difficult(multiple punctures) catheterization [15]. In the currentlypresented case however, no clear risk factors were present,apart from orthopaedic surgical intervention and the useof LMWH. Haematoma formation was attributed to anarterial or venous injury in the vertebral canal, duringremoval of the catheter, which could not be foreseen.Thromboprophylaxis possibly played a significant role inmaintaining bleeding leading gradually to spinal cordcompression. To our knowledge, no other case of epiduralbleeding in young athletes undergoing an ACL reconstruc-tion has ever been presented.
Surgical intervention and haematoma evacuation has beenassociated with better outcome [2]. In such a case earlydiagnosis and treatment is crucial for avoidance ofpermanent neurologic deficits. High index of suspicionwith careful and repeated clinical examination is necessaryto evaluate the patient’s symptoms, especially if there isgradual worsening, whereas Magnetic Resonance Imagingis the preferred imaging modality that confirms compres-sion in the vertebral canal [20]. In our case, immediatepostoperative improvement was evident and completeneurological recovery occurred within a week. The treatingsurgeon should be however aware of the fact that completeneurological recovery is not always the outcome despiteearly surgical intervention [2].
ConclusionThe current report focuses on the relevant rarity of thepresented complication, pointing however on the impor-tance of early clinical suspicion and surgical interventionto maximize the possibility of avoiding permanentpatient’s disability. Although several risk factors havebeen proposed, the possibility of occurrence in youngathletic individuals undergoing sports medicine relatedreconstructive procedures cannot be excluded. Further-more, dealing with ACL reconstruction procedures on aday-case basis and early patient’s discharge, which iscommon practice after these procedures, might lead tonegligence in diagnosing similar conditions. Close follow-up is thus essential.
List of abbreviationsACL, Anterior cruciate ligament; LMWH, Low molecularweight heparin; PT, Prothrombine time; aPTT, activatedPartial Thromboplastin time; MRC, Medical ResearchCouncil; MRI, Magnetic resonance imaging; TKA, Totalknee arthroplasty.
Page 5 of 6(page number not for citation purposes)
Cases Journal 2009, 2:6732 http://casesjournal.com/casesjournal/article/view/6732

ConsentWritten informed consent was obtained from the patientfor publication of this case report and any accompanyingimages. A copy of the written consent is available forreview by the Editor-in-Chief of this journal.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsNR treated and operated the patient, LP, NG treated thepatient and collected the data, PL collected the data andwrote the manuscript, TK revised the manuscript, KMtreated-operated the patient and reviewed the manuscript.
References1. Wulf H: Epidural anaesthesia and spinal haematoma. Canadian
Journal of Anaesthesia 1996, 12:1260-1271.2. Lawton MT, Porter RW, Heiserman JE, Jacobowitz R, Sonntag VK,
Dickman CA: Surgical management of spinal epidural hema-toma: relationship between surgical timing and neurologicaloutcome. Journal of Neurosurgery 1995, 1:1-7.
3. Medical Research Council (MRC). Aids to the Investigation ofPeripheral Nerve Injuries. London; Her Majesty’s StationeryOffice, 1976.
4. Colwell CW Jr., Collis DK, Paulson R et al.: Comparison ofenoxaparin and warfarin for the prevention of venousthromboembolic disease after total hip arthroplasty. Evalua-tion during hospitalization and three months after discharge.Journal of Bone & Joint Surgery Am 1999, 7:932-940.
5. Narchi P: Spinal anaesthesia and the use of anticoagulants. BestPractice & Research Clinical Anaesthesiology 2003, 3:443-449.
6. Schroeder DR: Statistics: detecting a rare adverse drugreaction using spontaneous reports. Regional Anesthesia andPain Medicine 1998, 6(S2):183-189.
7. White RH, Romano PS, Zhou H, Rodrigo J, Bargar W: Incidence andtime course of thromboembolic outcomes following total hipor knee arthroplasty. Archives of Internal Medicine 1998,14:1525-15231.
8. Vandermeulen EP, Van AH, Vermylen J: Anticoagulants and spinal-epidural anesthesia. Anesthesia & Analgesia 1994, 6:1165-1177.
9. Adamson DC, Bulsara K, Bronec PR: Spontaneous cervicalepidural hematoma: case report and literature review. SurgicalNeurology 2004, 2:156-159.
10. Moen V, Dahlgren N, Irestedt L: Severe neurological complica-tions after central neuraxial blockades in Sweden 1990-1999.Anesthesiology 2004, 4:950-959.
11. Badenhorst CH: Epidural hematoma after epidural paincontrol and concomitant postoperative anticoagulation.Regional Anesthesia 1996, 3:272-273.
12. Gogarten W: The influence of new antithrombotic drugs onregional anesthesia. Current Opinion in Anesthesiology 2006,5:545-550.
13. Horlocker TT, Wedel DJ, Benzon H et al.: Regional anesthesia inthe anticoagulated patient: defining the risks (the secondASRA Consensus Conference on Neuraxial Anesthesia andAnticoagulation). Regional Anesthesia and Pain Medicine 2003,3:172-197.
14. Miyazaki M, Takasita M, Matsumoto H, Sonoda H, Tsumura H,Torisu T: Spinal epidural hematoma after removal of anepidural catheter: case report and review of the literature.Journal of Spinal Disorders & Techniques 2005, 6:547-551.
15. Stroud CC, Markel D, Sidhu K: Complete paraplegia as a resultof regional anesthesia. Journal of Arthroplasty 2000, 8:1064-1067.
16. Yin B, Barratt SM, Power I, Percy J: Epidural haematoma afterremoval of an epidural catheter in a patient receiving high-dose enoxaparin. British Journal of Anaesthesia 1999, 2:288-290.
17. Tryba M, Wedel DJ: Central neuraxial block and low molecularweight heparin (enoxaparine): lessons learned from different
dosage regimes in two continents. Acta AnaesthesiologicaScandinavica S1997, 111:100-104.
18. Sanderink GJ, Guimart CG, Ozoux ML, Jariwala NU, Shukla UA,Boutouyrie BX: Pharmacokinetics and pharmacodynamics ofthe prophylactic dose of enoxaparin once daily over 4 days inpatients with renal impairment. Thrombosis Research 2002,3:225-231.
19. Kreppel D, Antoniadis G, Seeling W: Spinal hematoma: aliterature survey with meta-analysis of 613 patients. Neuro-surgical Review 2003, 1:1-49.
20. Kendell J, Wildsmith JAW: Complications of central neuralblockade. Current Anaesthesia & Critical Care 1999, 3:123-129.
Page 6 of 6(page number not for citation purposes)
Cases Journal 2009, 2:6732 http://casesjournal.com/casesjournal/article/view/6732
Do you have a case to share?
Submit your case report today• Rapid peer review• Fast publication• PubMed indexing• Inclusion in Cases Database
Any patient, any case, can teach ussomething
www.casesnetwork.com