case report: anesthetic challenges in patient with known ... · case report: anesthetic challenges...
TRANSCRIPT

Case Report: Anesthetic challenges in patient with known inter-atrial shunt undergoing re-do sternotomy for CABG and MVR
Rowena Lui, M.D., Aymen Alian, M.D. Department of Anesthesiology, Yale University School of Medicine, New Haven, CT
Background (cont.)
References
79-‐year-‐old male with PMHx coronary artery disease, severe mitral regurgitaCon, s/p thymectomy with radiaCon to chest presented for redo sternotomy for CABG and MVR. • Pre-‐op CT chest was concerning for adhesions between mediasCnal structures and posterior table of the sternum. Intra-‐operaCve echo was posiCve for severe mitral regurgitaCon and leM-‐to-‐right inter-‐atrial shunt.
• Upon chest dissecCon, a copious amount of blood was encountered along with a decrease in blood pressure. Emergent right fem-‐fem bypass was iniCated to decompress the right heart and chest dissecCon was completed. Once the chest was open, laceraCon of the right ventricle was discovered.
• During TEE examinaCon to check venous cannula posiCon, numerous air bubbles were detected on both sides of the heart and in the aorta. Surgeon was noCfied, and due to concern for air emboli stroke, paCent was placed in Trendelenberg posiCon, cooled to 20°C, his head was packed in ice, and corCcosteroids were administered
• The right ventricle was repaired with a pericardial patch and planned procedure was aborted.
• PaCent followed post-‐op, was AAOx3 without any focal neurological deficits and normal mini-‐mental state examinaCon
Case: This was a case complicated by many issues. The paCent unfortunately had previous thoracic surgery causing significant scarring and adhesions between mediasCnal structures, and radiaCon therapy resulCng in severe radiaCon-‐induced vasculiCs. This caused the iniCal chest dissecCon to be challenging requiring a sagiYal saw, which resulted in damage to the right ventricle. The damaged right ventricle likely caused entrained air, which involved the leM heart through his inter-‐atrial shunt aMer bypass was iniCated. With the large amount of air in his leM heart, the paCent was at a high risk for an air embolic stroke. Fortunately the paCent did not suffer any neurologic sequelae. There are several case reports of paCents on bypass who did have an air embolic event with subsequent CT findings and neurologic deficits. In all of the cases, the paCents were given steroids and placed under deep hypothermic circulatory arrest. In one case, the paCent was placed in a hyperbaric oxygen chamber and improved over the course of a few days. Another report menConed placing the paCent in a barbiturate coma to further decrease cerebral metabolic funcCon; however, this paCent did not improve. But these examples can certainly be taken into consideraCon for our paCent, had he had neurologic deficits. Conclusions: 1. Recognize the risks of re-‐opening a sternotomy incision complicated
by prior radiaCon therapy 2. Interpret the finding of intra-‐cardiac air in the leM heart and realize
the associated risks 3. Demonstrate knowledge of how to minimize damage from possible
cerebral ischemia intra-‐operaCvely
1. Van der Zee, M; Koene, B; Mariani, M. Fatal air embolism during cardiopulmonary bypass: analysis of an incident and prevenCon measures. InteracCve Cardiovascular and Thoracic Surgery. 2014, 1–3
2. Tian, DH et al. A meta-‐analysis of deep hypothermic circulatory arrest alone versus with adjuncCve selecCve antegrade cerebral perfusion. Ann Cardiothorac Surg. 2013, May;2(3):261-‐70
3. Moon RE. Bubbles in the brain: what to do for arterial gas embolism? Crit Care Med 2005;33:909-‐910 4. Shrinivas VG, Sankarkumar R, Rupa S. Retrograde cerebral perfusion for treatment of air embolism aMer valve surgery.
Asian Cardiovasc Thorac Ann 2004;12:81-‐82.
Figure 2: Mid esophageal 4-‐chamber view. Air visible in the leM atrium and right atrium
Figure 3: Mid-‐esophageal 4-‐chamber view with air in the LA and LV
Background
Discussion
Arterial air embolism during cardiac surgery is a complicaCon requiring expediCous acCon before significant cerebral damage occurs. The most likely causes of an embolic event include a reversed vent line, ruptured arterial tubing, introducCon of air during administraCon of cardioplegia, inadequate removal of air from the arterial circuit, and a defect in the oxygenator (1). Outside the context of cardiac surgery, arterial air embolism can also be caused by venous gas entering the arterial circulaCon via a right-‐to-‐leM shunt (e.g. a patent foramen ovale or an atrial septal defect).
Because the brain receives about 20% of cardiac output, an arterial air embolism can cause major cerebral injury; direct occlusion can cause sudden ischemia, clinically manifesCng as a stroke (altered mental status, loss of consciousness, focal neurologic deficits), which is difficult to assess in the semng of general anesthesia. Thus, it is important to have a high index of suspicion and take appropriate acCon. The literature menCons several measures to treat an air embolic stroke (or at least miCgate the cerebral damage it may cause) which include: placing the paCent in steep Trendelenberg posiCon, iniCaCng deep hypothermic circulatory arrest, administering corCcosteroids, retrograde brain perfusion, and administraCon of hyperbaric oxygen. Trendelenberg posiConing and hyperbaric oxygen aims to reduce the amount and volume of the actual air bubbles while the other treatments are targeted to brain funcCon (2, 3). Hypothermic circulaCon lowers cerebral metabolic rate and corCcosteroids serve to minimize inflammaCon and edema. Retrograde cerebral perfusion is not in common use, but is an established technique during aorCc surgery along with deep hypothermic circulatory arrest for cerebral protecCon (2, 4).
Figure 2:
Figure 1: Mid esophageal bicaval view with shunt visible between RA and LA
LA
RA
shunt LA LA
LV RA
Abstract
Effect of changes in tidal volume on plethysmographic variability in pediatric patients Rowena Lui, M.D., Aymen Alian, M.D.
Department of Anesthesiology, Yale University School of Medicine, New Haven, CT
IntroducCon Results
References
The pulse oximeter is widely used as a standard for intra-‐operaCve monitoring of oxygenaCon during anesthesia. Studies have looked into expanding its uClity by using the respiratory induced variaCon of the photoplethysmography (PPG) waveform as a dynamic index of preload (1,2). It has also been shown that shown that different respiratory paYerns can affect the waveform variability. In adults, a Cdal volume of at least 8cc/kg is necessary to cause significant circulatory changes (4). Reviews of studies done in children have been equivocal with regard to the use of respiratory-‐induced PPG variaCon to predict preload condiCons (5). None of the studies standardized the venClator semngs used. AddiConally, compared to adults, children have higher chest wall compliance and more compliant arterial vasculature. The aim of this study is to invesCgate whether or not pediatric paCents require higher than 8cc/kg Cdal volume to induce respiratory induced variaCons due to their physiology.
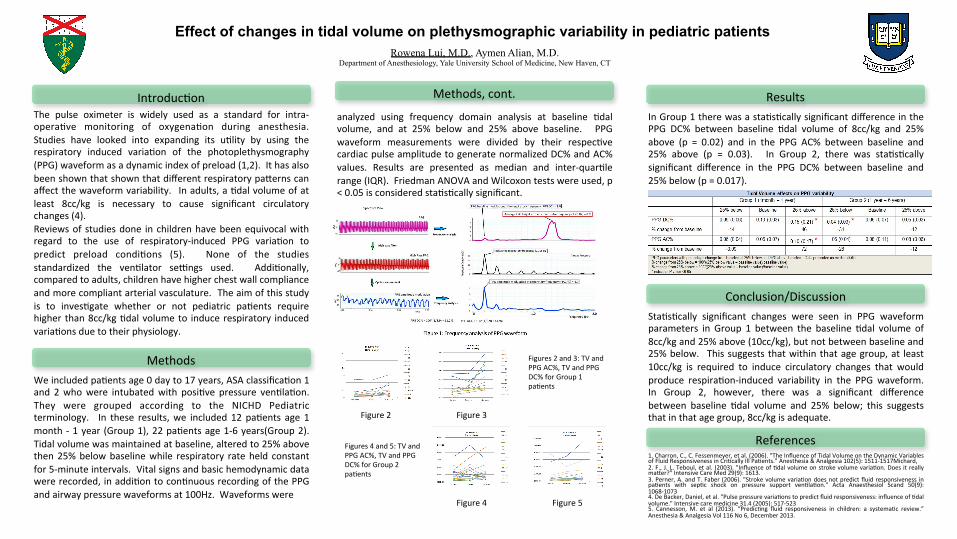
StaCsCcally significant changes were seen in PPG waveform parameters in Group 1 between the baseline Cdal volume of 8cc/kg and 25% above (10cc/kg), but not between baseline and 25% below. This suggests that within that age group, at least 10cc/kg is required to induce circulatory changes that would produce respiraCon-‐induced variability in the PPG waveform. In Group 2, however, there was a significant difference between baseline Cdal volume and 25% below; this suggests that in that age group, 8cc/kg is adequate.
Methods
Conclusion/Discussion
We included paCents age 0 day to 17 years, ASA classificaCon 1 and 2 who were intubated with posiCve pressure venClaCon. They were grouped according to the NICHD Pediatric terminology. In these results, we included 12 paCents age 1 month -‐ 1 year (Group 1), 22 paCents age 1-‐6 years(Group 2). Tidal volume was maintained at baseline, altered to 25% above then 25% below baseline while respiratory rate held constant for 5-‐minute intervals. Vital signs and basic hemodynamic data were recorded, in addiCon to conCnuous recording of the PPG and airway pressure waveforms at 100Hz. Waveforms were
In Group 1 there was a staCsCcally significant difference in the PPG DC% between baseline Cdal volume of 8cc/kg and 25% above (p = 0.02) and in the PPG AC% between baseline and 25% above (p = 0.03). In Group 2, there was staCsCcally significant difference in the PPG DC% between baseline and 25% below (p = 0.017).
Figure 2 Figure 3
Figure 4 Figure 5
analyzed using frequency domain analysis at baseline Cdal volume, and at 25% below and 25% above baseline. PPG waveform measurements were divided by their respecCve cardiac pulse amplitude to generate normalized DC% and AC% values. Results are presented as median and inter-‐quarCle range (IQR). Friedman ANOVA and Wilcoxon tests were used, p < 0.05 is considered staCsCcally significant.
Methods, cont.
1. Charron, C., C. Fessenmeyer, et al. (2006). "The Influence of Tidal Volume on the Dynamic Variables of Fluid Responsiveness in CriCcally Ill PaCents." Anesthesia & Analgesia 102(5): 1511-‐1517Michard, 2. F., J. L. Teboul, et al. (2003). "Influence of Cdal volume on stroke volume variaCon. Does it really maYer?" Intensive Care Med 29(9): 1613. 3. Perner, A. and T. Faber (2006). "Stroke volume variaCon does not predict fluid responsiveness in paCents with sepCc shock on pressure support venClaCon." Acta Anaesthesiol Scand 50(9): 1068-‐1073 4. De Backer, Daniel, et al. "Pulse pressure variaCons to predict fluid responsiveness: influence of Cdal volume." Intensive care medicine 31.4 (2005): 517-‐523 5. Cannesson, M. et al (2013). “PredicCng fluid responsiveness in children: a systemaCc review.” Anesthesia & Analgesia Vol 116 No 6, December 2013.
Figures 2 and 3: TV and PPG AC%, TV and PPG DC% for Group 1 paCents
Figures 4 and 5: TV and PPG AC%, TV and PPG DC% for Group 2 paCents
Effect of changes in respiratory rate on plethysmographic variability in pediatric patients Rowena Lui, M.D., Aymen Alian, M.D.
Department of Anesthesiology, Yale University School of Medicine, New Haven, CT
IntroducCon
Results References
The pulse oximeter is widely used as a standard for intra-‐operaCve monitoring of oxygenaCon during anesthesia. Studies have looked into expanding its uClity by using the respiratory induced variaCon of the photoplethysmography (PPG) waveform as a dynamic index of preload. It has been shown in several meta-‐analyses and systemic reviews of adult studies and some animal studies that these indices have excellent predicCve value of preload condiCons. AddiConally, there have been studies showing that different respiratory paYerns can affect the variaCon. In studies involving adult paCents, high respiratory rates have been shown to abolish the variaCons in some dynamic indices of preload. Reviews of studies done in children have been equivocal with regard to the use of respiratory-‐induced PPG variaCon to predict preload condiCons. None of the studies standardized the venClator semngs that were used. AddiConally, compared to adults, children have higher chest wall compliance, and more compliant arterial vasculature. The aim of this study is to invesCgate whether or not changes n respiratory rate have an effect on the PPG waveform variability.
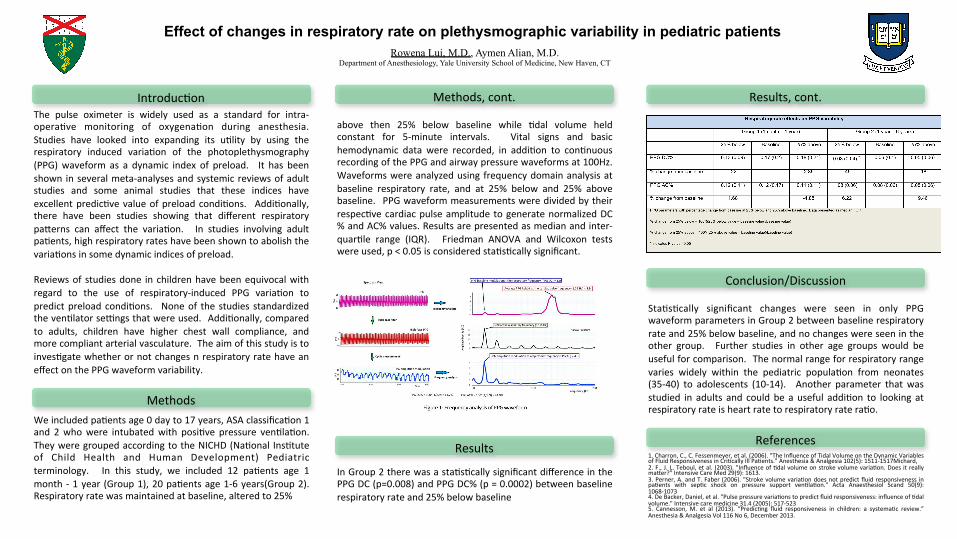
StaCsCcally significant changes were seen in only PPG waveform parameters in Group 2 between baseline respiratory rate and 25% below baseline, and no changes were seen in the other group. Further studies in other age groups would be useful for comparison. The normal range for respiratory range varies widely within the pediatric populaCon from neonates (35-‐40) to adolescents (10-‐14). Another parameter that was studied in adults and could be a useful addiCon to looking at respiratory rate is heart rate to respiratory rate raCo.
Methods
Conclusion/Discussion
In Group 2 there was a staCsCcally significant difference in the PPG DC (p=0.008) and PPG DC% (p = 0.0002) between baseline respiratory rate and 25% below baseline
above then 25% below baseline while Cdal volume held constant for 5-‐minute intervals. Vital signs and basic hemodynamic data were recorded, in addiCon to conCnuous recording of the PPG and airway pressure waveforms at 100Hz. Waveforms were analyzed using frequency domain analysis at baseline respiratory rate, and at 25% below and 25% above baseline. PPG waveform measurements were divided by their respecCve cardiac pulse amplitude to generate normalized DC% and AC% values. Results are presented as median and inter-‐quarCle range (IQR). Friedman ANOVA and Wilcoxon tests were used, p < 0.05 is considered staCsCcally significant.
Methods, cont.
1. Charron, C., C. Fessenmeyer, et al. (2006). "The Influence of Tidal Volume on the Dynamic Variables of Fluid Responsiveness in CriCcally Ill PaCents." Anesthesia & Analgesia 102(5): 1511-‐1517Michard, 2. F., J. L. Teboul, et al. (2003). "Influence of Cdal volume on stroke volume variaCon. Does it really maYer?" Intensive Care Med 29(9): 1613. 3. Perner, A. and T. Faber (2006). "Stroke volume variaCon does not predict fluid responsiveness in paCents with sepCc shock on pressure support venClaCon." Acta Anaesthesiol Scand 50(9): 1068-‐1073 4. De Backer, Daniel, et al. "Pulse pressure variaCons to predict fluid responsiveness: influence of Cdal volume." Intensive care medicine 31.4 (2005): 517-‐523 5. Cannesson, M. et al (2013). “PredicCng fluid responsiveness in children: a systemaCc review.” Anesthesia & Analgesia Vol 116 No 6, December 2013.
We included paCents age 0 day to 17 years, ASA classificaCon 1 and 2 who were intubated with posiCve pressure venClaCon. They were grouped according to the NICHD (NaConal InsCtute of Child Health and Human Development) Pediatric terminology. In this study, we included 12 paCents age 1 month -‐ 1 year (Group 1), 20 paCents age 1-‐6 years(Group 2). Respiratory rate was maintained at baseline, altered to 25%
Results, cont.