case report an uncommon indication of lower inclined · pdf filean uncommon indication of...
TRANSCRIPT

24Journal of Dental Research and Scientific Development | 2014 | Vol 1 | Issue 1
An uncommon indication of lower inclined plane
Ruchi Thakur, Anand L Shigli1, Gagan Thakur2
AbstractA cemented lower inclined acrylic plane is a well known treatment modality for anterior dental crossbite involving one or more teeth. This technique has the possibility of opening the bite if worn for more than three weeks. It can be used in cases when upper incisors are in crossbite with considerable amount of vertical overbite. This case presents a similar situation in a fourteen year old boy who was to receive porcelain fused to metal crowns for upper incisors but due to inability of patient to turn up for consecutive appointments, supraeruption of lower incisors occurred leading to an edge to edge bite. A lower inclined plane aided in labializing the upper incisors in three to four weeks’ time where the force was transmitted through the customised metal posts.
the bite if worn for more than 3 weeks.[2] It can be used in cases when upper incisors are in crossbite with considerable amount of vertical overbite.[3] The aim is to gradually tip the affected upper tooth or teeth labially to a point where a desirable overbite relationship exists.[4] And, hence, relapse is usually prevented by the posttreatment achieved normal overjet/overbite.[5]
Case Report
A 14‑year‑old male patient reported to the department of pedodontics and preventive dentistry whose clinical examination revealed that the patient had Ellis and Davey’s class III fracture with 11 and 21. As indicated by the nonvitality of the pulp, root canal treatment was done for 11 and 21. Compromised remaining tooth structure dictated a need for reinforcement using a customised post and core for both incisors. Crown preparation to receive porcelain fused to metal crowns owing to the esthetic requirement was done for both incisors and elastomeric impression was made to duplicate the postspace adequately on the cast.
Polycarbonate crowns were given as temporary crowns to the patient for both incisors and the patient was asked to report back after 4 days which would be required for fabrication of custom
Correspondence to: Dr. Ruchi Thakur, Dental Avenue, C–16, Vidya Nagar, Hoshangabad Road, Bhopal ‑ 462 026, Madhya Pradesh, India. E‑mail: [email protected]
Introduction
The word eruption is derived from the Latin word “Erumpere” meaning “to break out.” It usually means occlusal movement of the tooth from the position where it develops in the bone to its functional position in the occlusal plane. This eruptive movement begins as the root formation starts. Appearance after emergence of the tooth through the gingiva is considered the first clinical sign of eruption. Following emergence, the teeth erupt at a maximum rate to reach the occlusal plane. They then continue to erupt at a slower rate to keep pace with jaw growth and occlusal wear. Posteruptive tooth movements are those that maintain the position of the erupted tooth, while the jaw grows and makes up for occlusal and proximal wear. This compensating for occlusal and proximal wear continues throughout life by axial and mesial migration, respectively. Even after eruption of the tooth, the forces causing this tooth eruption are still available to bring about sufficient axial movement of the tooth to compensate for occlusal wear. It occurs most actively between the ages of 14 and 18 and is associated with condylar growth.[1]
A cemented lower inclined acrylic plane is a well‑known treatment modality for anterior dental crossbite involving one or more teeth. This technique has the possibility of opening
Key words: Inclined plane, post and core, supraeruption
Case Report
Departments of Pedodontics and Preventive Dentistry, and 2Oral and Maxillofacial Surgery, Peoples College of Dental Sciences and Research Centre, Bhopal, Madhya Pradesh, 1Department of Pedodontics and Preventive Dentistry, Bharati Vidyapeeth Deemed University Dental College, Sangli, Maharashtra, India
Access this article online
Website: www.iadrsd.orgQuick response code

25
Thakur, et al.: Uncommon indication of lower inclined plane
Journal of Dental Research and Scientific Development | 2014 | Vol 1 | Issue 1
when one or more teeth are abnormally malposed either labially or lingually in relation to opposing teeth. Before using an inclined plane, it is imperative to differentiate between a dental and skeletal crossbite.[2,6‑8] Dental crossbite involves only tipping of one or more teeth.[6] When there are two or more teeth involved in crossbite, then the jaw relation should be checked both in centric occlusion and in edge to edge relationship.[9,10] If patient is able to bite in an edge to edge relation, it means the anomaly is dentoalveolar in nature. Adequate and correct case selection is very important for using this appliance, as it majorly is responsible for the success of the treatment. Lee[2] stated that case selection and treatment decision should depend on sufficient overbite to hold the tooth in position following correction, adequate space in the arch to reposition the tooth and a class I molar relation.
Patient in such cases should have a normal skeletal pattern with crossbite only in the axial inclination of the affected teeth,[8] such an appliance uses natural forces to bring about rapid correction of anterior cross bites.[12] According to Proffit et al.,[11] correction of anterior dental crossbite is preceded by opening of enough space, then repositioning the displaced tooth or teeth across the occlusion into proper position. Since there was no crossbite present clinically and our intention was to only labialise the maxillary central incisors, lower inclined plane was opted for. The movement of teeth occurs as a result of force imparted on the inclined plane by the muscle responsible for elevation of mandible, that is, closing muscles of the jaw. While fabrication it should be borne in mind that the acrylic base of the inclined plane is wide enough. Also for better retention of the appliance, it is advisable to incorporate teeth with different axial inclination like incisors and canines and also premolars sometimes. The lower inclined plane covers the lower incisors and bears an inclination of about 45° to the occlusal plane. When the patient closes the jaw upper incisors come in contact with the inclined plane and the pressure is so directed and distributed that it is imparted in two directions. One that proclines the upper incisors and the other that intrudes the upper incisors. Any increase in the steepness of the plane of the appliance shall result in pushing the upper incisors further labially. Regular examination of the patient at weeks’ interval is critically essential so as to reach a timely decision to remove the appliance in cases of prolonged treatment time.
Newton’s third law of motion states that every action has an equal and opposite reaction. The pressure through the appliance is directed to reposition (tip) upper incisors labially but similarly another equal and opposite pressure directs (tips) mandibular teeth slightly in the lingual direction.[13] This treatment modality is advantageous as patient cooperation does not have a huge role to play because the appliance is cemented. Entire procedure works out to be cost‑effective as it is done in less number of patient visits and without involving any fixed orthodontic procedure. However, there are certainly a few disadvantages of this appliance like reduced
made post and coping. But unfortunately the patient neither turned up for his appointment scheduled for custom made metal post and coping trial nor in near future. However, the patient reported back after 3 months and gave history of having dislodged his temporary crowns within 1 week of placement. This could lead to mesial drifting of adjacent teeth due to missing proximal contacts, supraeruption of opposing incisors, and an unesthetic appearance. When examined clinically, it was observed that an edge to edge bite was established between the prepared maxillary incisor crowns and lower incisors which suggested that lower incisors had supraerupted. However, there was no midline shift or drifting, infact the teeth appeared absolutely asymptomatic and sound enough to receive the metal coping‑post unit. Radiographic examination also did not reveal any changes in the Periodontal ligament and/or alveolar bone. Finishing of the previously done crown preparation and necessary alterations were carried out to accommodate the earlier fabricated customized metal post and coping for both 11 and 21 [Figure 1a]. During coping trial, it was observed that supraeruption of lower incisors established an edge to edge bite without any space to accommodate the copings. It was also clear from the clinical pictures that after cementation of post and coping units there existed an unacceptable premature contact in the upper and lower anterior teeth leading to an open bite in the posterior teeth [Figure 1b].
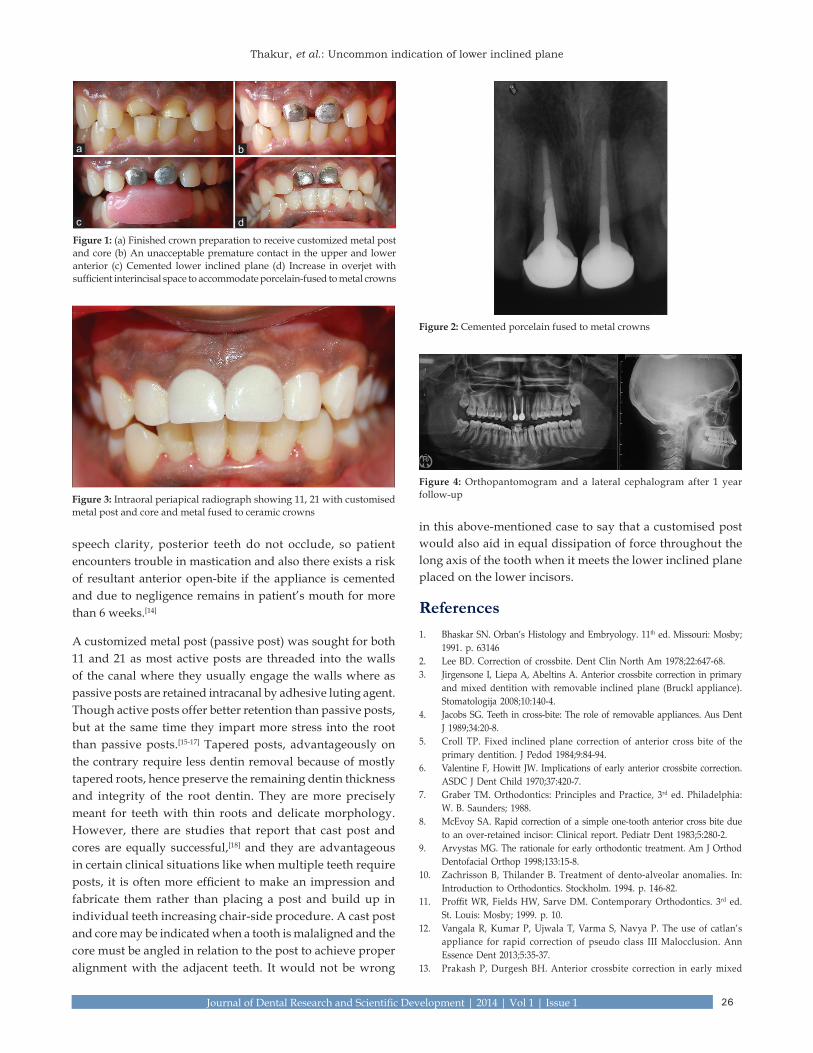
A wide range of treatment modalities for the same was considered. Creating an ample amount of space for adjustment of the porcelain fused to metal crowns could be brought about by two ways‑Either intrusion of supraerupted lower incisors or by supraeruption of posteriors by giving an anterior bite plane. Bringing about intrusion of lower incisors would be a very time‑taking procedure, so it was not considered. Bite opening by giving an anterior bite plane was also ruled out as the patient had a long and narrow face type. Bite opening in such a scenario would not be advisable as it would impart a further elongated and an unacceptable appearance to the face. Therefore, the treatment decided was to place an inclined plane on lower incisors, which would redirect the upper central incisors to a more labial position thereby increasing the overjet. Post and coping as a single unit was cemented on both 11 and 21, which provided a firm surface to contact the inclined plane [Figure 1c]. Increase in overjet was achieved in 3 to 4 weeks’ time [Figure 1d]. This provided space for the placement of porcelain fused to metal crowns for 11 and 21 as seen clinically and radiographically [Figures 2 and 3]. Patient was followed‑up regularly for any alterations in occlusion or relapse of overjet achieved. Orthopantomogram and a lateral cephalogram after 1 year follow‑up reveal no such occlusal changes [Figure 4].
Discussion
Inclined plane is one of the treatment modalities for correction of anterior crossbite. Graber[7] has defined crossbite as a condition
26
Thakur, et al.: Uncommon indication of lower inclined plane
Journal of Dental Research and Scientific Development | 2014 | Vol 1 | Issue 1
speech clarity, posterior teeth do not occlude, so patient encounters trouble in mastication and also there exists a risk of resultant anterior open‑bite if the appliance is cemented and due to negligence remains in patient’s mouth for more than 6 weeks.[14]
A customized metal post (passive post) was sought for both 11 and 21 as most active posts are threaded into the walls of the canal where they usually engage the walls where as passive posts are retained intracanal by adhesive luting agent. Though active posts offer better retention than passive posts, but at the same time they impart more stress into the root than passive posts.[15‑17] Tapered posts, advantageously on the contrary require less dentin removal because of mostly tapered roots, hence preserve the remaining dentin thickness and integrity of the root dentin. They are more precisely meant for teeth with thin roots and delicate morphology. However, there are studies that report that cast post and cores are equally successful,[18] and they are advantageous in certain clinical situations like when multiple teeth require posts, it is often more efficient to make an impression and fabricate them rather than placing a post and build up in individual teeth increasing chair‑side procedure. A cast post and core may be indicated when a tooth is malaligned and the core must be angled in relation to the post to achieve proper alignment with the adjacent teeth. It would not be wrong
in this above‑mentioned case to say that a customised post would also aid in equal dissipation of force throughout the long axis of the tooth when it meets the lower inclined plane placed on the lower incisors.
References1. Bhaskar SN. Orban’s Histology and Embryology. 11th ed. Missouri: Mosby;
1991. p. 631462. Lee BD. Correction of crossbite. Dent Clin North Am 1978;22:647‑68.3. Jirgensone I, Liepa A, Abeltins A. Anterior crossbite correction in primary
and mixed dentition with removable inclined plane (Bruckl appliance). Stomatologija 2008;10:140‑4.
4. Jacobs SG. Teeth in cross‑bite: The role of removable appliances. Aus Dent J 1989;34:20‑8.
5. Croll TP. Fixed inclined plane correction of anterior cross bite of the primary dentition. J Pedod 1984;9:84‑94.
6. ValentineF,Howitt JW. Implicationsofearlyanteriorcrossbite correction.ASDC J Dent Child 1970;37:420‑7.
7. Graber TM. Orthodontics: Principles and Practice, 3rd ed. Philadelphia: W.B.Saunders; 1988.
8. McEvoy SA. Rapid correction of a simple one‑tooth anterior cross bite due to an over‑retained incisor: Clinical report. Pediatr Dent 1983;5:280‑2.
9. Arvystas MG. The rationale for early orthodontic treatment. Am J Orthod Dentofacial Orthop 1998;133:15‑8.
10. Zachrisson B, Thilander B. Treatment of dento‑alveolar anomalies. In: Introduction to Orthodontics. Stockholm. 1994. p. 146‑82.
11. ProffitWR, FieldsHW, SarveDM.ContemporaryOrthodontics. 3rd ed. St. Louis: Mosby; 1999. p. 10.
12. Vangala R, Kumar P, Ujwala T, Varma S, Navya P. The use of catlan’s appliance for rapid correction of pseudo class III Malocclusion. Ann Essence Dent 2013;5:35‑37.
13. Prakash P, Durgesh BH. Anterior crossbite correction in early mixed
Figure 2: Cemented porcelain fused to metal crowns
Figure 3: Intraoral periapical radiograph showing 11, 21 with customised metal post and core and metal fused to ceramic crowns
Figure 4: Orthopantomogram and a lateral cephalogram after 1 year follow‑up
Figure 1: (a) Finished crown preparation to receive customized metal post and core (b) An unacceptable premature contact in the upper and lower anterior (c) Cemented lower inclined plane (d) Increase in overjet with sufficient interincisal space to accommodate porcelain-fused to metal crowns
dc
ba

27
Thakur, et al.: Uncommon indication of lower inclined plane
Journal of Dental Research and Scientific Development | 2014 | Vol 1 | Issue 1
dentition period using catlan’s appliance: A case report. ISRN Dent 2011;2011:298931.
14. Adams CP. The Design, Construction and Use of Removable Orthodontic Appliances. 5th ed. Bristol. 1984. p. 111‑2.
15. FeltonDA,WebbEL,KanoyvBE,Dugoni J.Threadedendodonticdowels:Effect of post design on incidence of root fracture. J Prosthet Dent 1991;65:179‑87.
16. BurnsDA, KrauseWR, DouglasHB, BurnsDR. Stress distributionsurrounding endodontic posts. J Prosthet Dent 1990;64:412‑8.
17. Standlee JP, Caputo AA. The retentive and stress distributing properties of split threaded endodontic dowels. J Prosthet Dent 1992;68:436‑42.
18. WeineFS,WaxAH,WenckusCS.Retrospective studyof tapered, smoothpost systems in place for 10 years or more. J Endod 1991;17:293‑7.
How to cite this article: Thakur R, Shigli AL, Thakur G. An uncommon indication of lower inclined plane. JDRSD 2014;1:24-7
Source of Support: Nil. Conflict of Interest: No conflict of interest.
Author Help: Online submission of the manuscripts
Articles can be submitted online from http://www.journalonweb.com. For online submission, the articles should be prepared in two files (first page file and article file). Images should be submitted separately.
1) First Page File: Prepare the title page, covering letter, acknowledgement etc. using a word processor program. All information related to your identity should
be included here. Use text/rtf/doc/pdf files. Do not zip the files.2) Article File: The main text of the article, beginning with the Abstract to References (including tables) should be in this file. Do not include any informa-
tion (such as acknowledgement, your names in page headers etc.) in this file. Use text/rtf/doc/pdf files. Do not zip the files. Limit the file size to 1 MB. Do not incorporate images in the file. If file size is large, graphs can be submitted separately as images, without their being incorporated in the article file. This will reduce the size of the file.
3) Images: Submit good quality color images. Each image should be less than 4096 kb (4 MB) in size. The size of the image can be reduced by decreas-
ing the actual height and width of the images (keep up to about 6 inches and up to about 1800 x 1200 pixels). JPEG is the most suitable file format. The image quality should be good enough to judge the scientific value of the image. For the purpose of printing, always retain a good quality, high resolution image. This high resolution image should be sent to the editorial office at the time of sending a revised article.
4) Legends: Legends for the figures/images should be included at the end of the article file.
Published by
Medknow Publications and Media Pvt. Ltd.B 9-12, Kanara Business Centre, Off Link Road, Ghatkopar (E), Mumbai – 400075, India Phone: 91-22-66491818 Website: www.medknow.com