case presentation 洪小妹 7-year-old female date of first visit: 97/10-gu clinic 義大醫院...
TRANSCRIPT

Case Presentation
洪小妹 7-year-old femaleDate of first visit: 97/10-GU clinic
義大醫院 吳展耀醫師

Chief Complaint:
Referred from local clinic due to proteinuria and hematuria

Past History&Family History
Denied systemic disease and hospitalization history
Denied family history of renal disease Vaccine history: as schedule

Physical Examination General appearance: easy-looking Body weight: 28.7kg Vital signs: BP: 91/66mmHg, HEENT: not anemic conjunctiva, no puffy eyelid Chest: clear B.S no retraction Heart: RHB, no murmur Abdomen: soft, no hepatomegaly Ext: no pitting edema Skin: no rash, no mottled skin Joint: no swelling, no limitation of motion

Lab. Exams(98-01-03)
Urinalysis: RBC 50-100/HPF, Pro 3+, ob 4+
WBC: 8480, Hgb: 14.1, MCV 84.8, Plt: 355k
Cr: 0.7, GOT/GPT: 57/39, Alb:3.5 , Na/k:136/4.3, Ca:9.2 TG/Chol: 69/173, Glu 92
C3 99.2 (90-180), C4 19.6 (10-40), IgA 68.2 ANA: homogenous (40x) Anti-ds DNA: negative
24 hours urine CCR: 64.4 ml/min 24 hours urine daily protein: 1234.2 mg/day
Enalapril (5mg) ½ #qd

98.1.30 Urinalysis: RBC 10-25/HPF, OB 2+, Pro+ Daily urine protein 300mg/day
98.2.23 Urinalysis RBC 10-25/HPF, Pro 2+
98.3.5 Urinalysis RBC 25-50/HPF, Pro – Cr 0.6 mg/dl 24hrs urine protein 175.5mg/day

kidney biopsy (98.3.6)
Light microscopy:
I.Glomerulus number: 3Diffuse global glomerular capillary wall thickening, moderate, with subepithelial deposits and spike and focal chain-like formation of glomerular basement membrane. Focal segmental sclerosis in one glomerulus is also present.
II.Tubulointerstitium:
Unremarkable III.Blood vessel:
Unremarkable

Diffuse global glomerular capillary wall thickening


spike and focal chain-like formation of glomerular basement membrane

Immunofluorescence microscopy
Glomerular number: 4IgG+++, IgM+, C1q+, C3+/-, polyclonal kappa++ and lambda++ deposit along glomerular capillary wall, diffuse global, granular pattern
Negative for IgA

C1q IgG
IgM
Electron microscopy
No glomerulus in this part of specimen
Tubulointerstitium is unremarkable

Final Diagnosis
Diffuse membranous glomerulopathy, stage 2-3

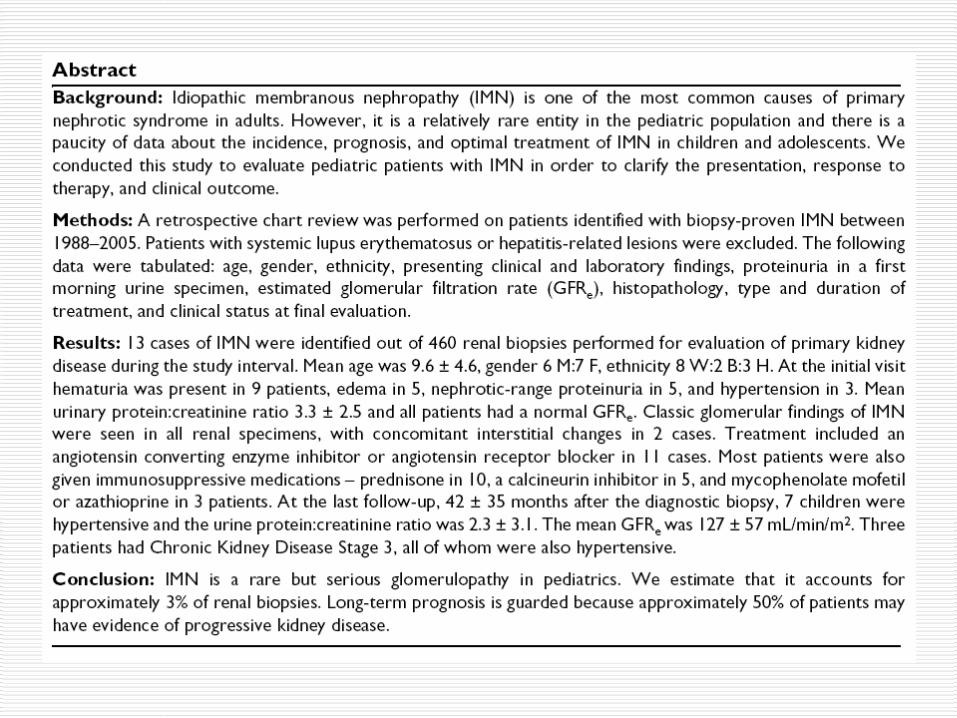
Causes and classificationPrimary/idiopathic 85% of MGN cases are classified as primary membranous glomerulonephritis.
Secondary autoimmune conditions (e.g., systemic lupus erythematosus) infections (e.g., syphilis, malaria, hepatitis B) drugs (e.g., captopril, NSAIDs, gold, mercury, penicillamine, nonsteroidal
anti-inflammatory agents, probenecid). tumors (in particular, chronic lymphocytic leukemia, carcinoma of the lung
and colon, and melanoma)

Pathology
Stage I
By light microscopy glomeruli appear normal, although the capillary lumen is mildly dilated and a stiffness of the capillary wall can be detected.
Finely granular or pseudo-linear IgG deposits are present all along the glomerular capillary wall.
By electron microscopy, small electron-dense subepithelial deposits with segmental distribution can be observed. Focal foot process effacement is a constant feature.

Stage II This stage is characterized by glomerular enlargement and diffuse thickening of
the capillary wall. Mesangial expansion and proliferation are usually absent.
The typical feature of membranous glomerulonephritis is best highlighted by silver staining: argyrophilic extensions of the glomerular basement membrane (spikes) look black,
Some cases of Stage II MGN show focal and segmental sclerotic lesions, indistinguishable from idiopathic focal segmental glomerulosclerosis. According to some authors, the cases with these superimposed lesions present a worse outcome compared to those with pure membranous GN.

Stage III Diffuse immune deposits and a more severe thickening of the basement
membrane are detectable by light microscopy. Huge and diffuse granular deposits are present all along the glomerular
basement membrane.
Stage IV A further thickening of the glomerular basement membrane together with
segmental or global glomerulosclerosis are detectable by light microscopy

Treatment Treatment of secondary membranous nephropathy is guided by the
treatment of the original disease.
For treatment of idiopathic membranous nephropathy
Immunosuppressive therapy Corticosteroids: They have been tried with mixed results, with one study
showing prevention of progression to renal failure without improvement in proteinuria.
Chlorambucil Cyclosporine Tacrolimus Cyclophosphamide Mycophenolate mofetil

a six-month course of methylprednisolone and chlorambucil can bring about sustained remission of the nephrotic syndrome and help to preserve renal function in patients with idiopathic membranous nephropathy.

a six-month therapy with methylprednisolone and chlorambucil increases the probability of remission of proteinuria and protects from renal function deterioration even in the long-term. This treatment may avoid dialysis or death within 10 years to about one third of nephrotic patients with membranous nephropathy.

Methylprednisolone /Chlorambucil1. treated /untreated patients , renal survival rate 92%/60%2. MTP/Chlorambucil V.S. MTP alone, remission of NS 64% V.S. 38%3. equivalent results between MTP/C and MTP/cyclophosphamide 4. cyclosporine in reducing proteinuria, relapse when cyclosporine stopped





-Remission was complete in 75% of the patients and partial in 17%. -One patient (8%) with chronic kidney disease (stage 2) -Complete remission was significantly associated with the absence of chronic histological changes (p = 0.03).-Children with NS and/or NRP associated with MGN appear to have a good prognosis when treated with a combination of corticosteroids and cyclophosphamide.