case discussion pompe disease 2003. 06. 30
DESCRIPTION
Case Discussion Pompe Disease 2003. 06. 30. Ri 許哲偉 Ri 李秉學. Brief History. This is a 1-year-old boy, G1P1, GA 39+5 wk, NSD, BBW 3178 gm. When he was 2 months old in Sep., 2002, he had cough, rhinorrhea, decreased appetite and activity, and he was admitted to 中國 hospital. - PowerPoint PPT PresentationTRANSCRIPT
Case DiscussionCase Discussion
Pompe DiseasePompe Disease
2003. 06. 30.2003. 06. 30.
Ri Ri 許哲偉許哲偉Ri Ri 李秉學李秉學
Brief HistoryBrief History
This is a 1-year-old boy, G1P1, GA 39+5 This is a 1-year-old boy, G1P1, GA 39+5 wk, NSD, BBW 3178 gm.wk, NSD, BBW 3178 gm.
When he was 2 months old in Sep., 2002, When he was 2 months old in Sep., 2002, he had cough, rhinorrhea, decreased appehe had cough, rhinorrhea, decreased appetite and activity, and he was admitted to tite and activity, and he was admitted to 中國 中國 hospital. hospital.
Cardiomegaly and hypotonia were noted aCardiomegaly and hypotonia were noted and Pompe’s disease was suspected. nd Pompe’s disease was suspected.
Brief HistoryBrief History
9/19/2002, in NTU, liver enzyme, cardiac e9/19/2002, in NTU, liver enzyme, cardiac enzyme, LDH level all increased.nzyme, LDH level all increased.
Echo: hypertrophic cardiomyopathyEcho: hypertrophic cardiomyopathy 、、 momoderate LVOT obstruction, severe MR, mild derate LVOT obstruction, severe MR, mild TR, PFO. TR, PFO.
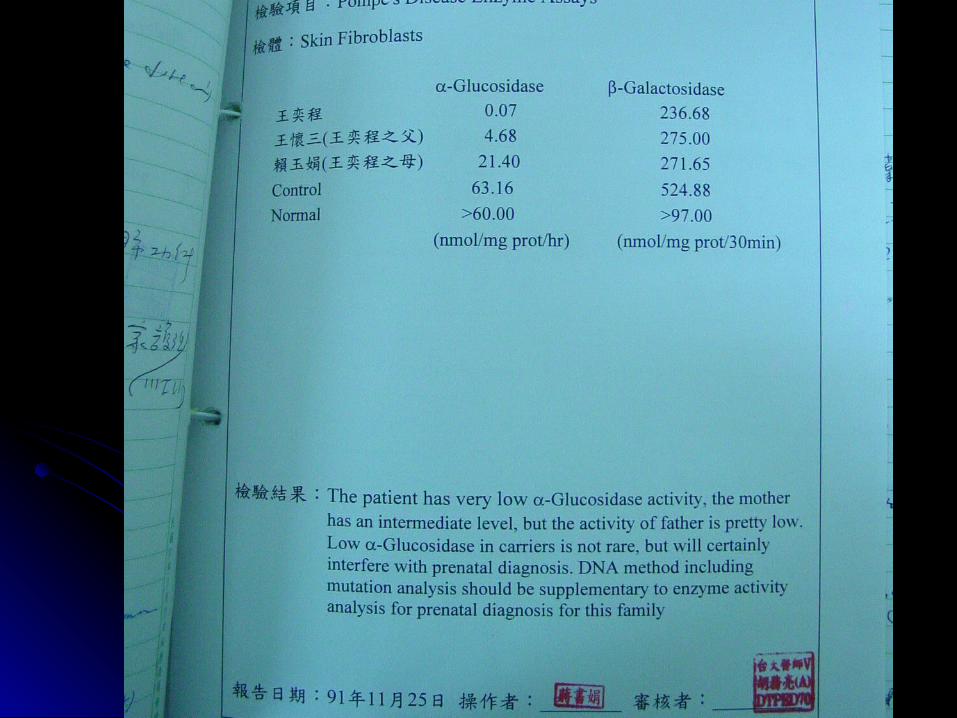
Enzyme assays of lymphocyte, skin fibroblEnzyme assays of lymphocyte, skin fibroblast and urine revealed prominent decreasast and urine revealed prominent decreased ed αα- glucosidase level.- glucosidase level.
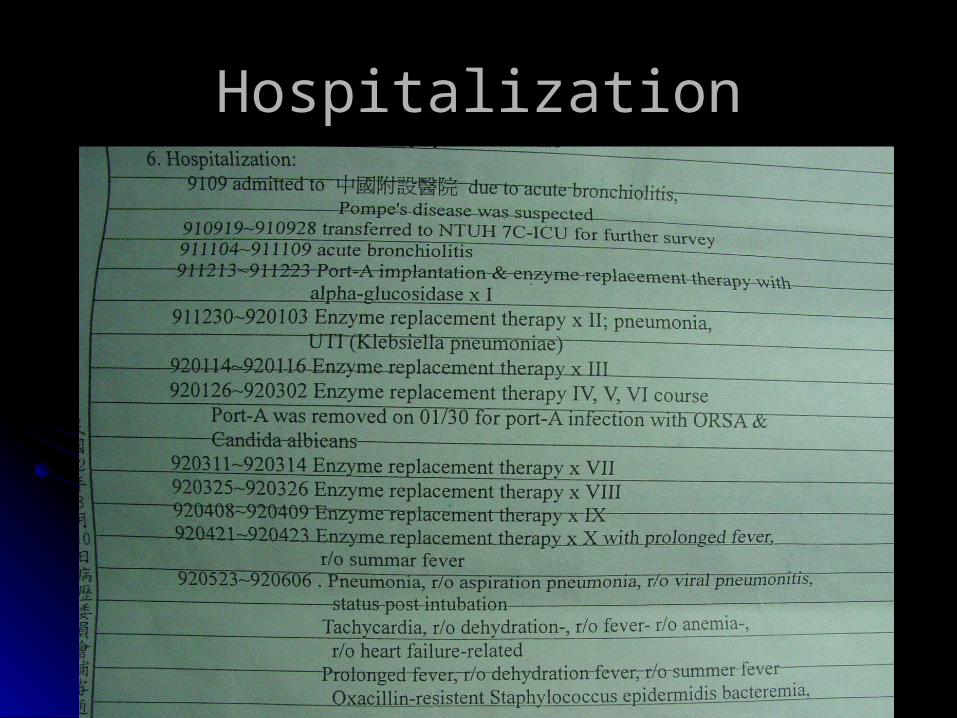
HospitalizationHospitalization
Chief ComplaintChief Complaint
AcrocyanosisAcrocyanosis 、、 chillschills 、、 tachypneatachypnea 、、 decdecreased urine outputreased urine output 、、 dry lips were also ndry lips were also noted.oted.
Low grade fever with productive cough for Low grade fever with productive cough for 3 wks.3 wks.
Present IllnessPresent Illness
High fever (40 ) with tachycardia for 2 days.℃High fever (40 ) with tachycardia for 2 days.℃
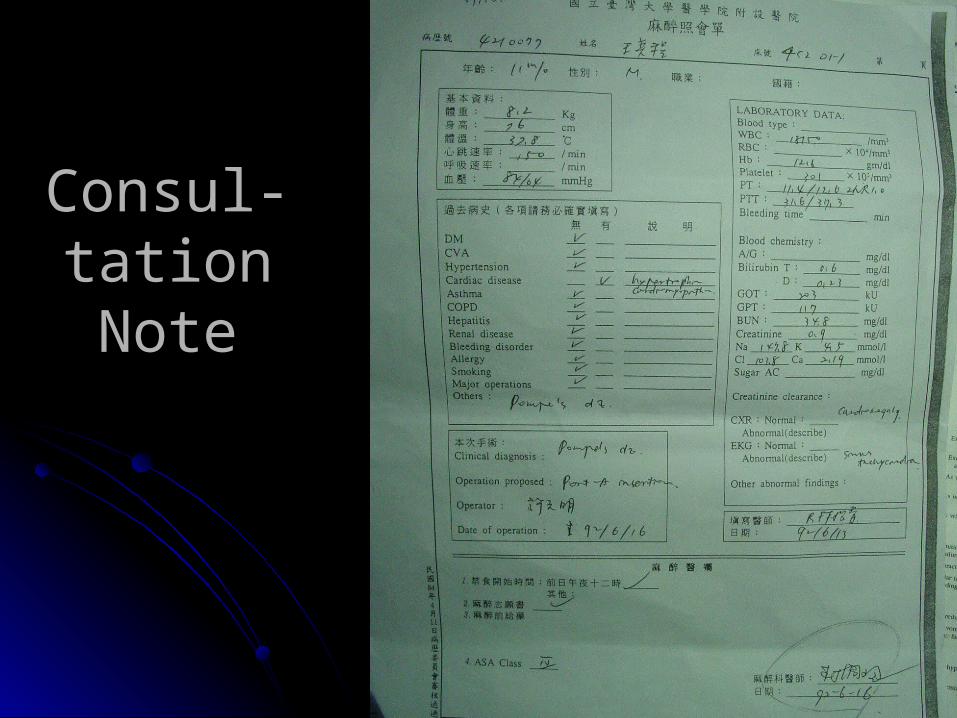
Consul-taConsul-tation Notetion Note

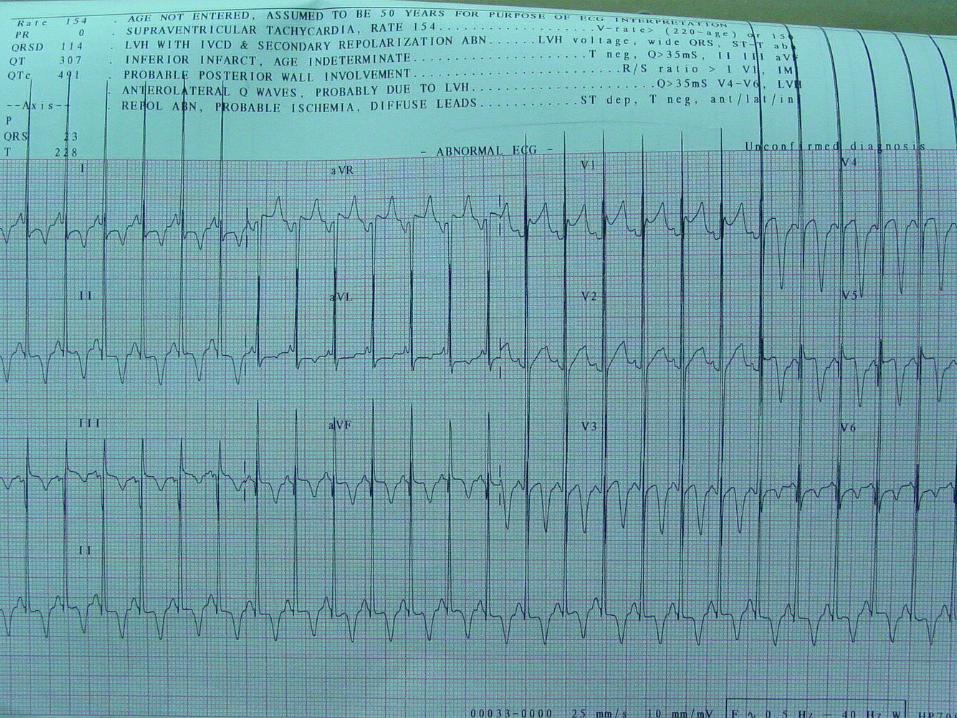
Anesthetic Anesthetic RecordRecord
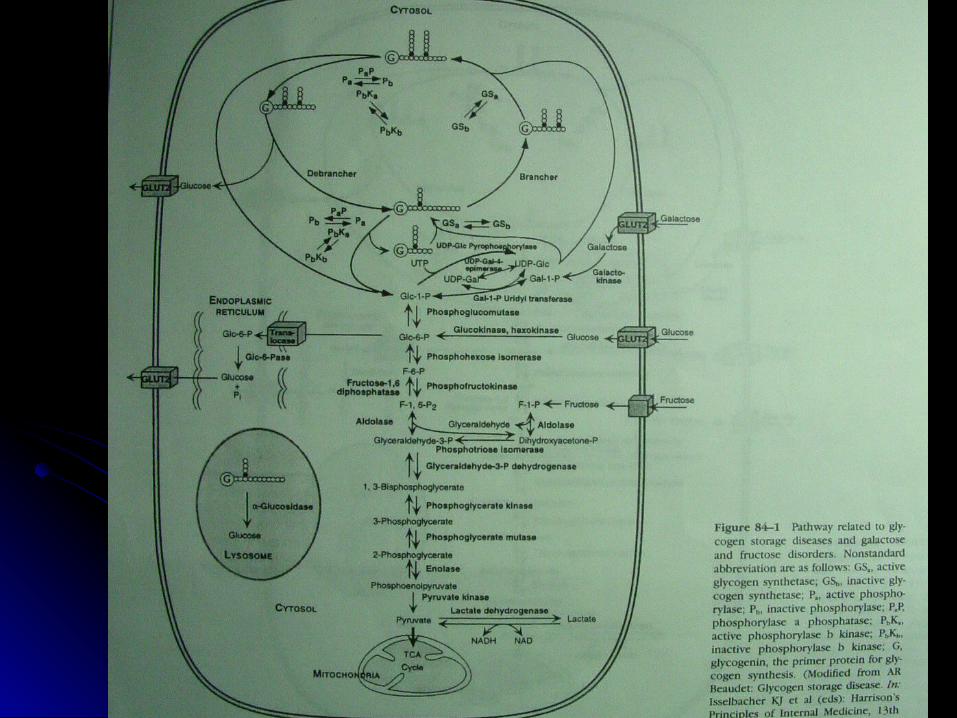
Glycogen Storage DiseaseGlycogen Storage Disease
and Pompe Disease and Pompe Disease
Glycogen Storage DiseaseGlycogen Storage Disease
Inherited disorders affecting glycogen metInherited disorders affecting glycogen metabolism.abolism.
Virtually all enzymes involved in its syntheVirtually all enzymes involved in its synthesis, degradation, and regulation cause sosis, degradation, and regulation cause some type of GSD.me type of GSD.
Abnormal quantity and quality of glycogen.Abnormal quantity and quality of glycogen.Classified by organ involvement and clinicClassified by organ involvement and clinic
al manifestation into liver and muscle glycal manifestation into liver and muscle glycogenoses.ogenoses.
Glycogen Storage DiseaseGlycogen Storage Disease
More than 12 forms of glycogenoses.More than 12 forms of glycogenoses.1/20,000 in live births.1/20,000 in live births. Most common in childhoodMost common in childhood Deficiency of G-6-P (type I), Deficiency of G-6-P (type I), lysosomal acid lysosomal acid αα- gl- gl
ucosidase (type II)ucosidase (type II), debrancher (type III), and liv, debrancher (type III), and liver phosphorylase kinase.er phosphorylase kinase.
Most common in adulthoodMost common in adulthood Myophosphorylase deficiency (type V)Myophosphorylase deficiency (type V)
Pompe Disease (Type II)Pompe Disease (Type II)
Deficient activity of lysosomal acid Deficient activity of lysosomal acid αα-1,4 gl-1,4 glucosidase (acid maltase).ucosidase (acid maltase).
Accumulation of glycogen in lysosomes.Accumulation of glycogen in lysosomes.1/50,000 in live births without ethnic predic1/50,000 in live births without ethnic predic
tion.tion.An autosomal recessive disorder, chromosAn autosomal recessive disorder, chromos
ome 17q23.ome 17q23.
Clinical ManifestationsClinical Manifestations
Infantile formInfantile form Most severe, prominent Most severe, prominent cardiomegalycardiomegaly,, hypotonia hypotonia,,
and death prior to 2 yr of age. and death prior to 2 yr of age. ““Floppy baby,” Floppy baby,” feeding difficultiesfeeding difficulties, macroglossia, , macroglossia,
hepatomegaly, and heart failure due to hypertrophepatomegaly, and heart failure due to hypertrophic cardiomyopathy.hic cardiomyopathy.
ECG: ECG: high-voltage QRShigh-voltage QRS, shortened P-R interval., shortened P-R interval. Death results from cardiorespiratory failure or asDeath results from cardiorespiratory failure or as
piration pneumonia.piration pneumonia.
Clinical ManifestationsClinical Manifestations
Juvenile formJuvenile formDelayed motor milestones, difficult walking,Delayed motor milestones, difficult walking,
followed by swallowing difficulties, weakn followed by swallowing difficulties, weakness of proximal muscle and respiratory mess of proximal muscle and respiratory muscle.uscle.
Death from respiratory failure before 20 yrDeath from respiratory failure before 20 yrs old.s old.
Cardiomegaly is variable, and overt cardiaCardiomegaly is variable, and overt cardiac failure.c failure.
Clinical ManifestationsClinical Manifestations
Adult formAdult form Slow progressive myopathy without cardiac involSlow progressive myopathy without cardiac invol
vement.vement. Onset between 2nd and 7th decades.Onset between 2nd and 7th decades. Proximal muscle weakness with trunk involvemeProximal muscle weakness with trunk involveme
nt. (pelvic girdle, paraspinal muscle, diaphragm nt. (pelvic girdle, paraspinal muscle, diaphragm are the most seriously affected)are the most seriously affected)
Initial symptoms: respiratory insufficiency (somnInitial symptoms: respiratory insufficiency (somnolence, morning headache, orthopnea, and exertolence, morning headache, orthopnea, and exertional dyspnea)ional dyspnea)
Laboratory FindingsLaboratory Findings
Elevated levels of serum creatine kinase, AST, aElevated levels of serum creatine kinase, AST, and LDH.nd LDH.
Muslce biopsy shows presence of vacuoles stainMuslce biopsy shows presence of vacuoles stained positive with glycogen.ed positive with glycogen.
Electron microscopy reveals glycogen accumulatElectron microscopy reveals glycogen accumulation within the membranous sac and in the cytoplion within the membranous sac and in the cytoplasm.asm.
EMG reveals myopathic features with excessive EMG reveals myopathic features with excessive electrical irritability of muscle fibers.electrical irritability of muscle fibers.
DiagnosisDiagnosis
Decreased levels of acid Decreased levels of acid αα- glucosidase a- glucosidase activity in muscle or cultured skin fibroblast.ctivity in muscle or cultured skin fibroblast.
Deficiency is more severe in the infantile fDeficiency is more severe in the infantile form.orm.
Prenatal diagnosis using amniocytes or chPrenatal diagnosis using amniocytes or chronic villi is available in the fatal infantile foronic villi is available in the fatal infantile form. rm.
Therapeutic approach to PoTherapeutic approach to Pompe diseasempe disease
11。。 Enzyme replacement therapyEnzyme replacement therapy
22。。 Gene therapyGene therapy
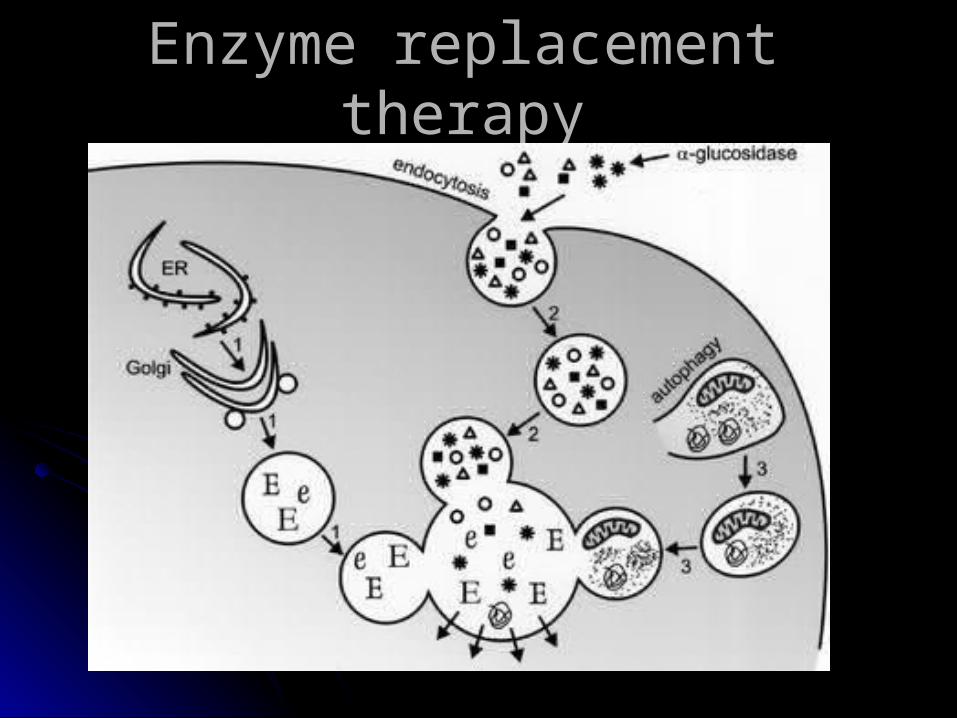
Enzyme replacement therapyEnzyme replacement therapy
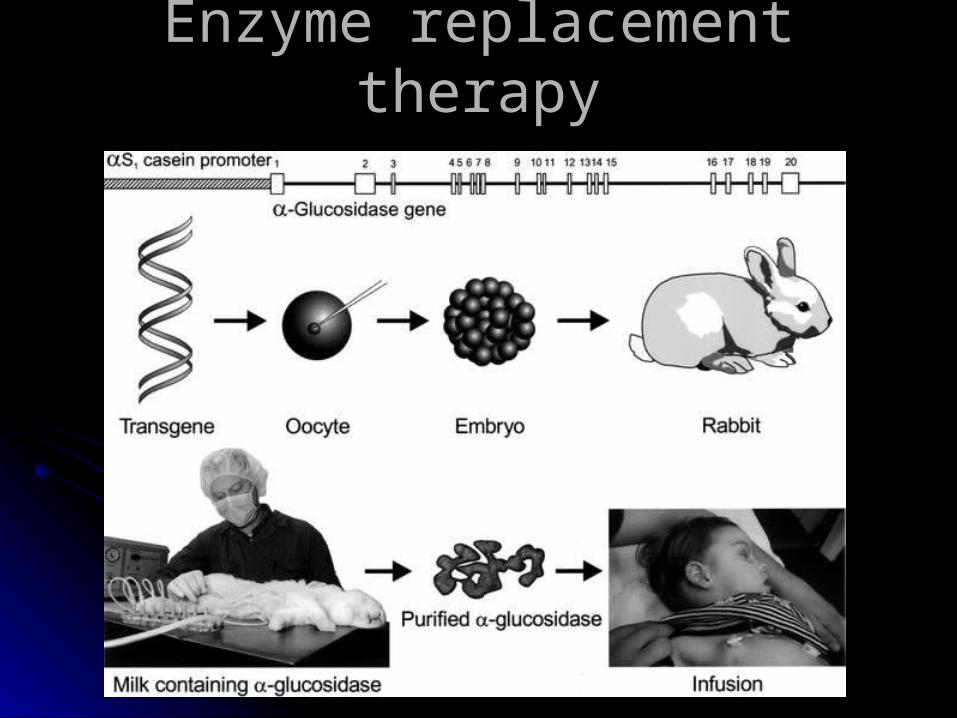
Enzyme replacement therapyEnzyme replacement therapy
Gene therapyGene therapy
Provide a permanent internal Provide a permanent internal source of enzymesource of enzyme
Gene therapyGene therapy
Still in the early stage of investigationStill in the early stage of investigationAdenovirus carrying GAA(acid alpha gluAdenovirus carrying GAA(acid alpha glu
cosidase) was examined by intramusculcosidase) was examined by intramuscular, intracardiac and intravenous adminisar, intracardiac and intravenous administrationtration
Correction of enzyme deficiency in In ViCorrection of enzyme deficiency in In Vivo experimentsvo experiments
Anesthesia and Pompe diseAnesthesia and Pompe diseasease
Major anesthetic problemsMajor anesthetic problems
The cardiomyopathyThe cardiomyopathyOxygenationOxygenationRespiratory muscle weakness and the use Respiratory muscle weakness and the use
of muscle relaxantof muscle relaxant
The cardiomyopathyThe cardiomyopathy
Massive infiltration of the ventricular walMassive infiltration of the ventricular wall may produce either a congestive or obl may produce either a congestive or obstructive cardiomyopathystructive cardiomyopathy
Avoidance of myocardial depression anAvoidance of myocardial depression and vasodilator d vasodilator
Using ketamine and sevoflurane seems Using ketamine and sevoflurane seems to be reasonableto be reasonable
OxygenationOxygenation
Some children with Pompe disease have lSome children with Pompe disease have large toungues →might cause loss of airwaarge toungues →might cause loss of airway control during anesthesiay control during anesthesia
Due to the cardiomegaly and weak respiraDue to the cardiomegaly and weak respiratory muscle, patients have increased vulnetory muscle, patients have increased vulnerability to atelectasis and aspirationrability to atelectasis and aspiration
Respiratory muscle weakness Respiratory muscle weakness and muscle relaxantsand muscle relaxants
Increased susceptibility to prolonged intubIncreased susceptibility to prolonged intubation after operation ation after operation
Succinylcholine may cause rhabdomyolysiSuccinylcholine may cause rhabdomyolysis, hyperkalemia and cardiac arrest in childs, hyperkalemia and cardiac arrest in children with undiagnosed myopathies. ren with undiagnosed myopathies.
Ureteroscopic removal of left ureteral litUreteroscopic removal of left ureteral lithiasis in a patient with acid maltase defihiasis in a patient with acid maltase defi
ciency diseaseciency disease ANESTH ANALG 1993;76:662-4ANESTH ANALG 1993;76:662-4
A 71-year old patient with adult type of AMD cA 71-year old patient with adult type of AMD come for removal of ureteral stoneome for removal of ureteral stone
Induction of anesthesia proceeded by propofoInduction of anesthesia proceeded by propofol(100mg, IV) ,atracurim(35mg)l(100mg, IV) ,atracurim(35mg)
Ketorolac(60mg, IM) was injectedKetorolac(60mg, IM) was injected Anesthesia was maintained by 66% nitrous oAnesthesia was maintained by 66% nitrous o
xide and IV propofol infusionxide and IV propofol infusion Neuromuscular block was reversed by neostiNeuromuscular block was reversed by neosti
gmine and glycopyrrolategmine and glycopyrrolate
Ureteroscopic removal of left ureteral litUreteroscopic removal of left ureteral lithiasis in a patient with acid maltase defihiasis in a patient with acid maltase defi
ciency diseaseciency disease ANESTH ANALG 1993;76:662-4ANESTH ANALG 1993;76:662-4
The selection of drug was based on minimizinThe selection of drug was based on minimizing post.OP drowsiness, muscle weakness, ang post.OP drowsiness, muscle weakness, and the respiratory depressant effect of anesthed the respiratory depressant effect of anestheticstics
Propofol was selected for its short recovery aPropofol was selected for its short recovery and post.operative staynd post.operative stay
Narcotics were avoided and ketorolac was usNarcotics were avoided and ketorolac was used for analgesiaed for analgesia
Depolarizing muscle relaxant was considered Depolarizing muscle relaxant was considered unsafeunsafe
Prolonged respiratory depression after anestProlonged respiratory depression after anesthesia for parathyroidectomy in patient with Jhesia for parathyroidectomy in patient with Juvenile AMD uvenile AMD Journal of Clinical Anes.,Vol.8 1996Journal of Clinical Anes.,Vol.8 1996
11 year-old boy with juvenile AMD and primar11 year-old boy with juvenile AMD and primary hyperparathyroidism undergoing parathyroiy hyperparathyroidism undergoing parathyroidectomydectomy
Anesthesia was induced by mask with enfluraAnesthesia was induced by mask with enflurane, Nne, N22O and oxygenO and oxygen
Despite of avoidance of any muscle relaxant,tDespite of avoidance of any muscle relaxant,the patient develop post.OP respiratory failure he patient develop post.OP respiratory failure and was kept intubated until the 15and was kept intubated until the 15 thth day after day after surgerysurgery
ConclusionsConclusions
Avoid cardiac depressants and Avoid cardiac depressants and vasodilatorsvasodilators
Keep PEEP and high FiOKeep PEEP and high FiO22
Close monitoring post.OP conditionClose monitoring post.OP condition
Thank you for your attentionThank you for your attention