case #2 biologics and pregnancy. history of present illness 26 f with crohn’s disease developed...
TRANSCRIPT
Case #2 Biologics and Pregnancy
History of Present Illness
• 26 F with Crohn’s disease• Developed persistent diarrhea in 2008
– colonoscopy demonstrated Crohn's disease primarily involving terminal ileum but also some active colitis in the sigmoid colon.
– Failed 5-ASA and immunomodulators. – Developed perianal abscess progressing to fistula in 2009,
requiring surgery. – Started on infliximab in 2009 but this was complicated by
anaphylaxis• Began adalimumab in 2010 and was doing well• Became pregnant in 2011 while on adalimumab
Discussion
• When is a good time to get pregnant after a flare?
• Now that she is pregnant, what would you do with her anti-TNF agent?– Continue– Continue with immunomodulator– Stop– Switch
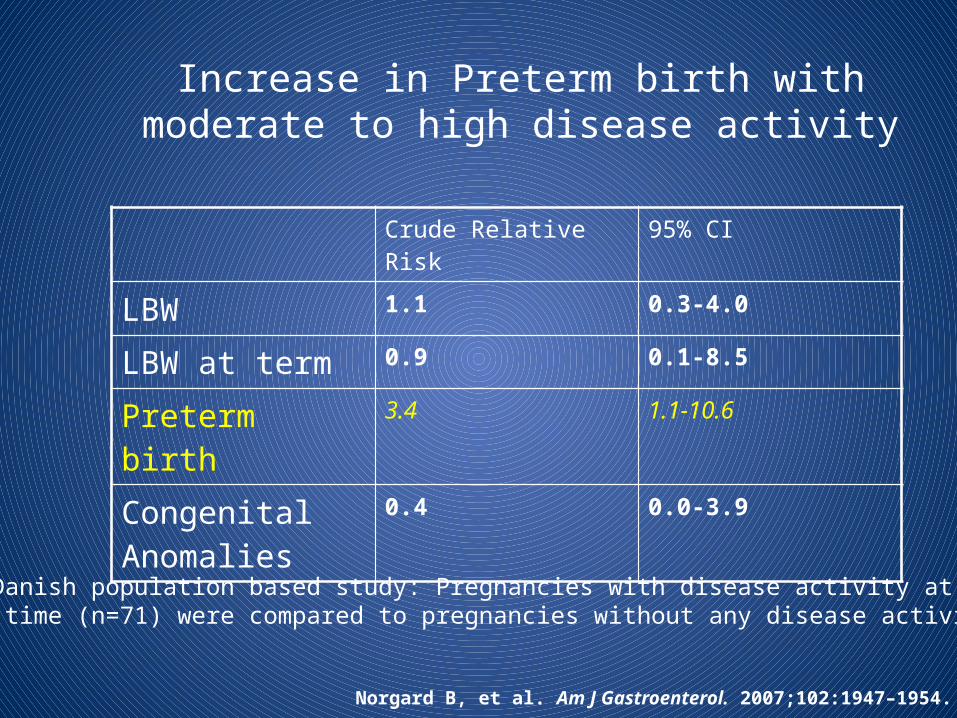
Increase in Preterm birth with moderate to high disease activity
Crude Relative Risk 95% CI
LBW 1.1 0.3-4.0
LBW at term 0.9 0.1-8.5
Preterm birth 3.4 1.1-10.6
Congenital Anomalies
0.4 0.0-3.9
Norgard B, et al. Am J Gastroenterol. 2007;102:1947–1954.
Danish population based study: Pregnancies with disease activity at any time (n=71) were compared to pregnancies without any disease activity (n=86)

• 571 IBD pregnancies in Spain (53% CD; 21% active disease during pregnancy)
• 253 pregnancies in patients exposed to IM (187) or anti-TNF (66) during/within 6 months of pregnancy– 74% IM monotherapy; 11% anti-TNF agent; 15% combination therapy
Azathioprine safety: Spanish cohort
Exposed (253)
Unexposed (318) P
Crohn’s Disease 73% 37% < 0.001
IBD Surgery 37% 6% <0.001
History: Tobacco Use 21% 13% 0.01
Active IBD 27% 19% 0.015
Exposed (253)
Unexposed (318)
Any complication 25% 32%
Spontaneous Abortion 9% 12%
Preterm Delivery 5% 9%
Low Birth Weight 5% 9%
ICU Admission 2% 3%
Malformations 1% 0.4%
All P-values NS
Casanova MJ, et al. Am J Gastroenterol. 2013 Mar;108(3):433-40
ICU, intensive care unit
Conclusion:•There was no increased risk of poor pregnancy outcomes in Spanish IBD patients on immunosuppressant therapy•Thiopurines only predictor of favorable GPO OR 1.67, 1.03-2.7
• 30 patients on azathioprine (28 patients, median dose 1.93 mg/kg) or 6-MP (two patients, doses 1.32 and 0.94 mg/kg)
• During pregnancy, median 6-TGN decreased over time (p=0.001). while 6-MMP increased, without causing maternal myelotoxicity or hepatotoxicity.
• After delivery, both 6-TGN and 6-MMP levels returned to preconception baseline levels.
Jharap B et al Gut 2013 Feb 19. [Epub ahead of print
Thiopurines and fetal anemia; Should we test newborns?

• Fetal 6-TGN concentrations correlated positively with maternal 6-TGN levels (p<0.0001). (n=25)
• Median 6TGN infant: mother = 42:92 pmol/8x108
• No 6-MMP was detected in the newborns except 1
• Pancytopenia and high alk phos (severe pre-eclampsia)
• 63% had anemia at birth: (n=16)
• Median Hb 9.25 mmol/l [8.25-9.60]
• 6-TGN 230 vs 90 in infants with anemia
• Congenital Anomalies: 2/31 (6.5%)
• clubfoot, ptosis
Jharap B et al Gut 2013 Feb 19. [Epub ahead of print)
Thiopurines and fetal anemia; Should we test newborns?

Adverse Pregnancy Outcomes: The Piano Study
Group A (aza)RR (CI)
Group B (bio) Group AB (combo)
Any Complication 1.2 (0.8-1.8) 1.2 (0.8-1.7) 1.7 (1.0-2.8)
Spontaneous Abortion 0.5 (0.2-1.5) 1.3 (0.6-2.9) 1.4 (0.5-4.1)
Preterm Birth 1.0 (0.6-1.8) 0.8 (0.5-1.3) 2.4 (1.3-4.3)
Low Birth Weight 0.7 (0.4-1.6) 1.2 (0.6-2.1) 1.5 (0.7-3.3)
IUGR 0.8 (0.2-2.8) 1.0 (0.3-2.8) 0.5 (0.1-3.9)
Cesarean section 1.0 (0.7-1.4) 1.4 (1.0-1.9) 1.3 (0.8-2.0)
NICU 1.1 (0.6-1.8) 1.2 (0.7-1.9) 1.3 (0.7-2.5)
Congenital Anom 0.8 (0.4-1.7) 0.9 (0.4-1.7) 0.9 (0.3-2.5)
* P <0.05Adjusted for none/mild vs. mod/severe disease activity
Biologics: Placental Transfer
• Infliximab: – Study of 10 mothers on IFX– In all cases, infant and cord IFX level were greater than mother.
6 months to clear• Adalimumab
– Study of 10 mothers on ADA– In all cases, infant and cord ADA level was greater than mother.
Up to 4 months to clear– ¾ pts who stopped ADA 35 days prior to delivery had a flare
• Certolizumab– Study of 10 mothers– In all cases, infant and cord levels were less than 2 mcg/ml even
if mom dosed the week of delivery
Mahadevan Clin Gastroenterol Hepatol. 2013 Mar
Placental Transfer• 28 live births (17 IFX, 11 ADA)
– Mean GA 39 [32-42]– Pts with active disease continued tx (5)– 10 pts on thiopurines, continued through pregnancy
• IFX: 12/17 d/c week 18-27 – Mean cord level 6.4 + 1.6 µg/ml (2.8 vs. 10 p=0.02 if >10 weeks)– 14 restarted (week 8-27 postpartum)– 1 allergic rxn, 2 changed to ADA: 3/12 (25%)
• ADA: All 11 pts stopped week 22– Mean cord level 1.7 + 0.4 µg/ml – 2/11 relapsed – [18%] (CS wk 30; C section week 37)– all resumed therapy f/u 9 mos
• 22 % (5/23) had a flare or need to change therapy postpartum.– Account for preterm birth, continuing thiopurines, presence of detectable levels even
when discontinued <30 weeks.
Zelinkova Clin Gastroenterol Hepatol. 2013 Mar
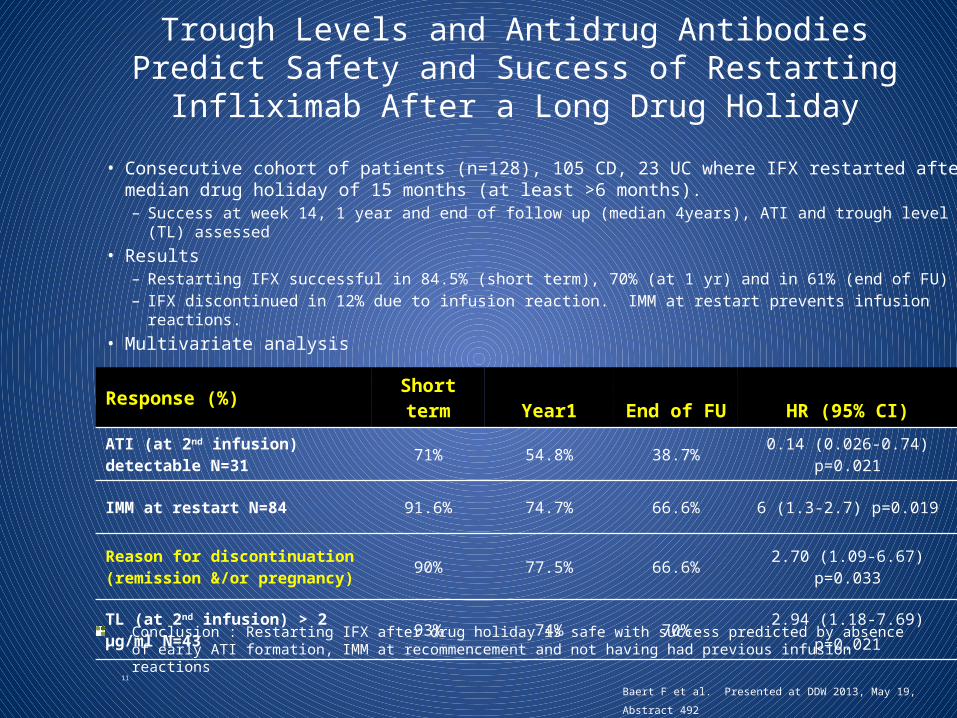
• Consecutive cohort of patients (n=128), 105 CD, 23 UC where IFX restarted after median drug holiday of 15 months (at least >6 months).
– Success at week 14, 1 year and end of follow up (median 4years), ATI and trough level (TL) assessed• Results
– Restarting IFX successful in 84.5% (short term), 70% (at 1 yr) and in 61% (end of FU)– IFX discontinued in 12% due to infusion reaction. IMM at restart prevents infusion reactions.
• Multivariate analysis
11
Trough Levels and Antidrug Antibodies Predict Safety and Success of Restarting Infliximab After a Long Drug Holiday
Response (%) Short term Year1 End of FU HR (95% CI)
ATI (at 2nd infusion) detectable N=31 71% 54.8% 38.7% 0.14 (0.026-0.74) p=0.021
IMM at restart N=84 91.6% 74.7% 66.6% 6 (1.3-2.7) p=0.019
Reason for discontinuation (remission &/or pregnancy) 90% 77.5% 66.6% 2.70 (1.09-6.67) p=0.033
TL (at 2nd infusion) > 2 μg/ml N=43 93% 74% 70% 2.94 (1.18-7.69) p=0.021
Baert F et al. Presented at DDW 2013, May 19, Abstract 492
Conclusion : Restarting IFX after drug holiday is safe with success predicted by absence of early ATI formation, IMM at recommencement and not having had previous infusion reactions

• Her adalimumab was stopped in the first trimester (4/11)
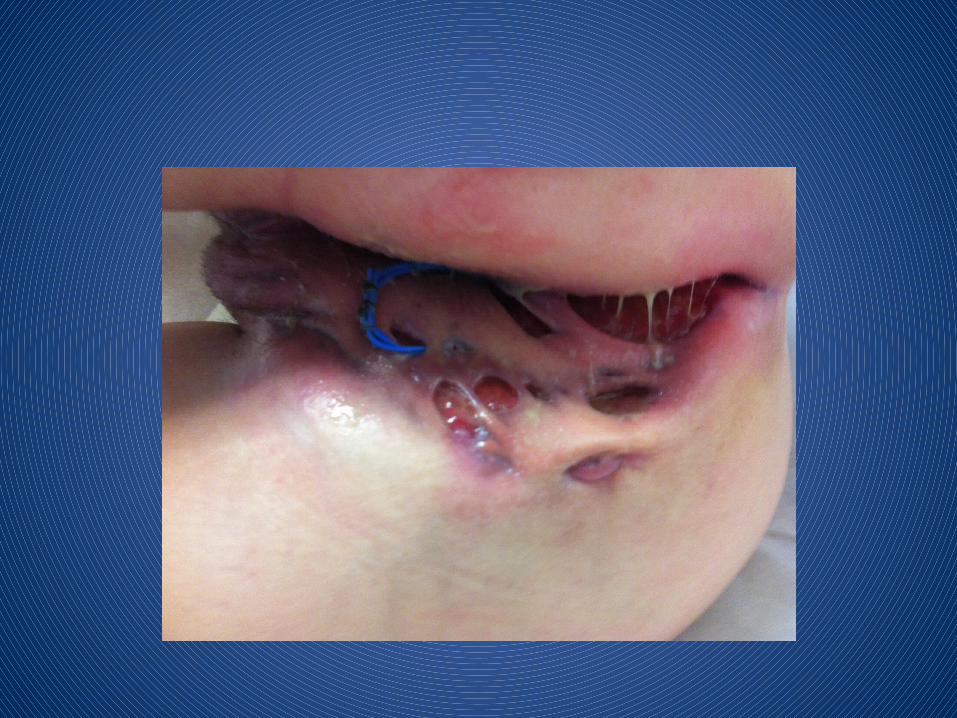
• She began developing perianal disease which progressed throughout pregnancy– No therapy was given initially due to concern for
pregnancy– She developed large draining skin defects
throughout her perineum, perivaginal area, perianal area, sacrum, inner thighs, and umbilicus.
Discussion
• What type of diagnostic tests would you do in this pregnant patient now in her second trimester?– Labs? Stool tests?– Imaging?– Endoscopy?
• How do you manage surgical needs in the pregnant patient?
• Would you start anti-TNF denovo in pregnancy? In third trimester?
• She underwent urgent surgery + seton placements in July 2011, September 2011, and multiple times in 2012 as well
• She underwent cesarean section 11/11• She was not started on therapy despite
ongoing perianal disease until 3/2012 when she presented to our office


• What medication would you offer her at this point (anaphylaxis to infliximab; off adalimumab for 7 months)
• What concerns do you have about lactation and azathioprine/anti-TNF therapy?
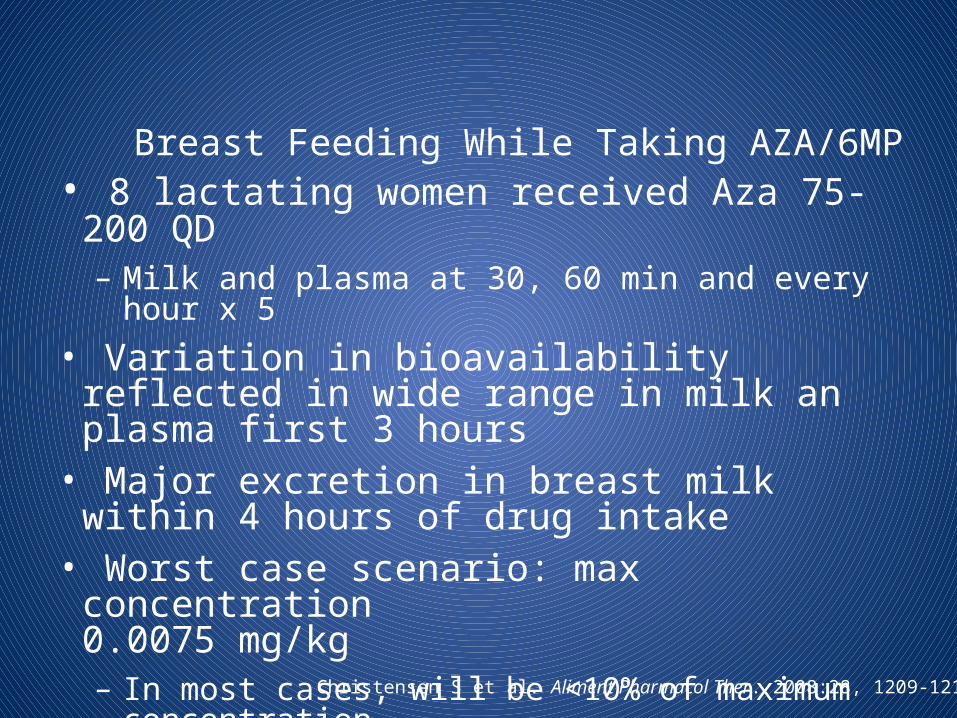
Breast Feeding While Taking AZA/6MP• 8 lactating women received Aza 75-200 QD
– Milk and plasma at 30, 60 min and every hour x 5• Variation in bioavailability reflected in wide range in
milk an plasma first 3 hours• Major excretion in breast milk within 4 hours of drug
intake• Worst case scenario: max concentration
0.0075 mg/kg– In most cases, will be <10% of maximum concentration
Christensen S et al. Aliment Pharmacol Ther. 2008:28, 1209-1213.
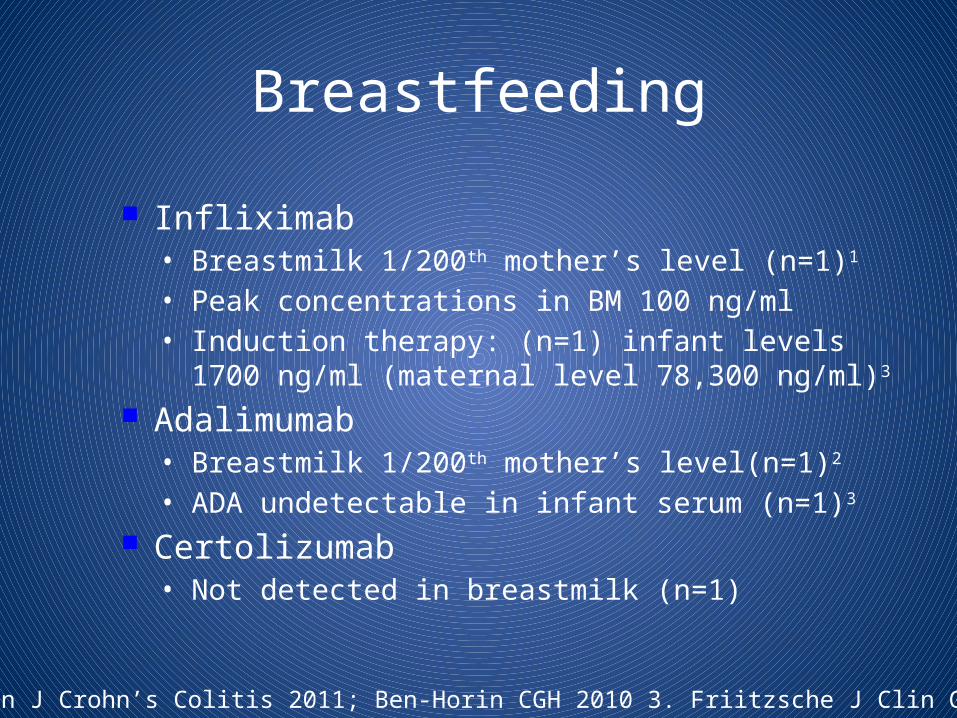
Breastfeeding
Infliximab• Breastmilk 1/200th mother’s level (n=1)1
• Peak concentrations in BM 100 ng/ml• Induction therapy: (n=1) infant levels 1700 ng/ml
(maternal level 78,300 ng/ml)3
Adalimumab• Breastmilk 1/200th mother’s level(n=1)2
• ADA undetectable in infant serum (n=1)3
Certolizumab• Not detected in breastmilk (n=1)
1. Benhorin J Crohn’s Colitis 2011; Ben-Horin CGH 2010 3. Friitzsche J Clin Gastro 2012
• She was started on certolizumab 400 mg week 0,2,4 and q 4 weeks, increased to 400 mg every 2 weeks
• She was started on azathioprine 50 mg increase to 100 mg
• She began to slowly improve
Questions for Discussion
• When (if ever) do you stop anti-TNF in pregnancy– IF you stop, what are you worried about?– Should you have azathioprine on board too
particularly if you plan to stop?• Does it matter if the patient is flaring or not?• What precautions are needed for mom and
baby?