case 1 21 year old male office worker gp referral, “ibs not responding to rx 3 month history of...
TRANSCRIPT

Case 1
• 21 year old male office worker
• GP referral, “IBS not responding to Rx
• 3 month history of abdominal discomfort, worse after eating, can keep him awake
• Wight loss of ½ stone
• Intermittent loose motions
Case 1
• Average build
• Slightly pale
• Abdomen not distended
• Mild tenderness in lower half
• No mass palpable
• Anus normal ,∑ - normal rectal mucosa

Case 1
• How would you investigate him?

Case 1Case 1

Case 1
• What is the diagnosis?
–Confirmatory investigations?
• How would you manage the patient?

Case 2
• 30 year old anaesthetic registrar
• Presented as emergency:
–acute abdominal pain and vomiting
• 3 month history of abdominal discomfort
• Wight loss of ½ stone
• Loose motions

Case 2
• Unwell
• Fever 380 c
• Distended abdomen
Tender,guarding

Case 2• AXR
Case 2
• Laparotomy
• Small bowel obstruction
• Adhesions right iliac fossa to
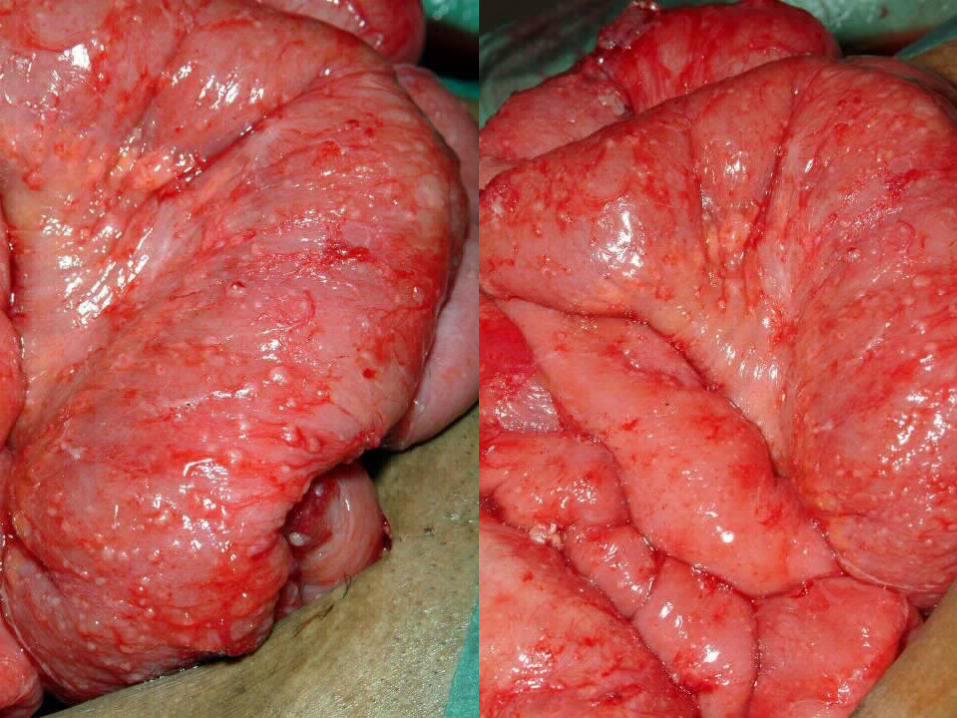
• Inflamed appendix and ileocaecal area
• What operation?

Case 2
• Laparotomy
• Small bowel obstruction
• Adhesions right iliac fossa to
• Inflamed appendix and ileocaecal area
• Appendicectomy performed (non specific acute inflammation)

Case 2
• Next 4 months continued abdominal pain
• Diarrhoea persists
• Further weight loss
• Frightened to eat
• What investigations?

Case 2
• What is the diagnosis?
• What management?
• Medical?
• Surgical?

Case 3
• 18 year old trainee chef
• Feels tired
• 6 month history of abdominal pain and diarrhoea
• Bowels opened up to 6 times per day
• Mucus in stool
• Occasional blood with motion

Case 3
• Pale, clinically anaemic
• Tall and thin
• Abdomen soft, mild tenderness in left iliac fossa
• No mass palpable
• Anus – small tags only
• Rectal mucosa “normal” – slightly red
Case 3
• Hb – 10.6
• Platelets – 635
• WCC – 8.9
• CRP – 87
• Barium enema
Case 3
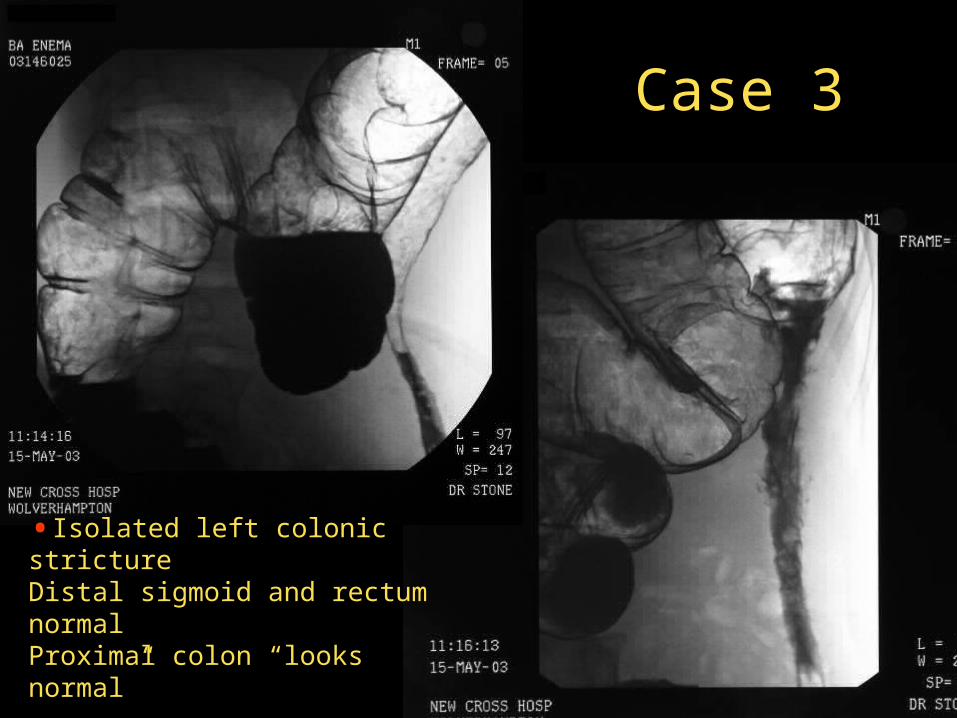
•Isolated left colonic strictureDistal sigmoid and rectum normalProximal colon “looks normal”

Case 3
• How would you manage this patient?
Case 3
• What operation would you perform?
Case 3
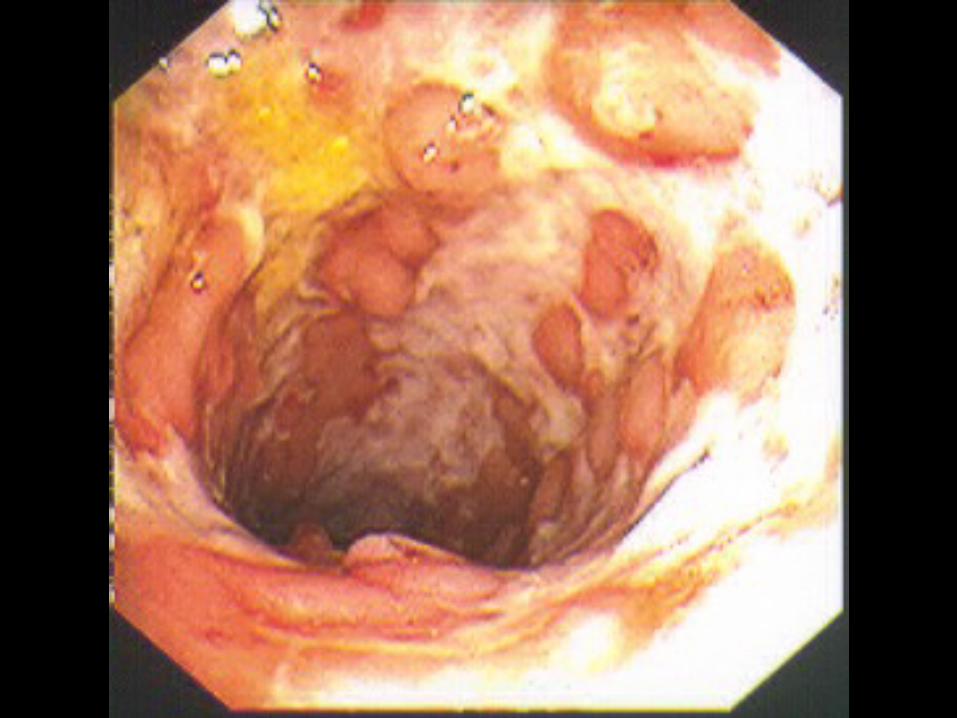
• Represents January 2006
• Acute anal abscess
• Large tags
• Abscess partially draining from 2 sites
• EUA
• Chronic fistulous abscess posteriorly
• Ulcerated anal canal
• Active rectal inflammation
Case 3
Case 3
• How would you manage this patient now?
Case 4
• 56 year old female
• Previous resection for ileo-colic Crohn’s disease
• Previous anal abscess x 2
• Now presents with increasing anal and labial pain
• Miserable


Case 4
• How would you manage this patient
–Further investigations
–Treatment