cas 2013 – abstracts supplement supplément des résumés ... poster 8.pdf · cas 2013 –...
TRANSCRIPT
CAS 2013 – Abstracts supplement Supplément des résumés 2013 de la SCA Updated June 18, 2013
11
POSTER DISCUSSION 8 Pain: Acute – Basic & Clinical and Pain: Clinical & Chronic Chair: Dr Timur Ozelsel, Department of Anesthesiology and Pain Medicine, University of Alberta, Edmonton, AB Monday June 24 10:15 – 12:00 Chinook 1
DISCUSSION DES AFFICHES 8 Douleur aiguë, notions de base et cliniques; douleur chronique – clinique Président : Dr Timur Ozelsel, Département d’anesthésiologie et de médecine de la douleur, Université de l’Alberta, Edmonton, AB Lundi 24 juin 10 h 15 à 12 h Chinook 1
1589910 - EFFECTS OF SEASONAL VARIATIONS IN TESTOSTERONE AND CORTISOL ON PAIN RESPONSES UNDER RESTING AND STRESS CONDITIONS Presenter: Jae Chan Choi, Department of Anesthesiology and Pain Medicine, Brain Research Group, Yonsei University Wonju College of Medicine, Wonju, Kwangwon-Do, Korea, Republic of. 1623101 - META-ANALYSIS: EPIDURAL OPIOIDS FOR POSTOPERATIVE ANALGESIA Presenter: Matthew Chong, Michael G. DeGroote School of Medicine, McMaster University, Hamilton, ON Co-authors: Nayer Youssef, David Orlov, Tristan Alie, Toni Tidy, James E Paul 1636976 - OUTCOMES OF A GROUP PAIN SELF-MANAGEMENT PROGRAM 2007-2011 Presenter: Alexander Clark, Department of Anesthesia, Pain Management and Perioperative Medicine, Dalhousie University, Halifax, NS Co-authors: Douglas Cane, Mary E Lynch, Darlene Davis 1650609 - PREGABALIN FOR ACUTE POSTOPERATIVE PAIN- A SYSTEMATIC REVIEW AND META- ANALYSIS OF RANDOMIZED CONTROLLED TRIALS. Presenter: Naveen Eipe, The Ottawa Hospital, Ottawa, ON Co-authors: John Penning, Mohammed Ansari, Fatemeh Yazdi, Lucy Turner 1650616 - UNILATERAL EPIDURAL BLOCK IN LOWER LIMB VASCULAR SURGERY PATIENTS - MYTH OR REALITY? Presenter: Naveen Eipe, The Ottawa Hospital, Ottawa, ON Co-authors: Ali Faris, Qutaiba A Tawfic, John Penning 1651482 - DETERMINING AN INFUSION REGIMEN FOR INTRAVENOUS LIDOCAINE INFUSION Presenter: James Khan, Anesthesia, University of Toronto, Toronto, ON Co-authors: Maaz Yousuf, Naveed Siddiqui 1651993 - MULTIMODAL ANALGESIA WITH LIDOCAINE FOR ACUTE PAIN- A RETROSPECTIVE STUDY Presenter: Qutaiba Tawfic, The Ottawa Hospital, Ottawa, ON Co-authors: Naveen Eipe, John Penning 1652580 - A META-ANALYSIS ON THE CLINICAL EFFECTIVENESS OF SUPERFICIAL CERVICAL PLEXUS BLOCKS AFTER THYROID SURGERY Presenter: Katsushi Doi, Anesthesiology, Hamada Medical Center, Hamada, Shimane, Japan Co-authors: Hiroshi Hoshijima, Norifumi Kuratani, Yasue Kashiwagi 1652827 - FIVE YEARS OF PERI-OPERATIVE OPIOID USE AT A TERTIARY CARE CENTRE Presenter: Peter MacDougall, Anesthesiology, Pain Management and Peri-operative Medicine, Dalhousie University, Halifax, NS Co-authors: Paul Brousseau, Andrew D Milne 1653043 - KETAMINE PLUS MORPHINE FOR PATIENT CONTROLLED ANALGESIA: A META-ANALYSIS Presenter: Janet Martin, EPiCOR Group, MEDICI Centre, Department of Anesthesia & Perioperative Medicine, University of Western Ontario, London, ON Co-authors: Li Wang, Bradley Johnston, Alka Kaushal, Davy C Cheng

1589910- EFFECTS OF SEASONAL VARIATIONS IN TESTOSTERONE AND CORTISOL ON PAIN RESPONSES UNDER RESTING AND STRESS CONDITIONS
Jae Chan Choi1
1. Department of Anesthesiology and Pain Medicine, Brain Research Group, Yonsei University Wonju College of Medicine, Wonju, Kwangwon-Do, Korea, Republic of
Introduction: Pain experiments were conducted during the spring and summer to investigate whether seasonal variations in testosterone and cortisol affect pain responses to pressure under resting and stress conditions.
Methods: Forty-six healthy males were recruited from a medical college. Local Ethics Committee approval was obtained. The same pain experiments were conducted twice, once during rest two days before stress exposure and once during stress. Stress was induced by having the participating medical students perform anesthetic technique tests. A 12-cm-wide mercury sphygmomanometer cuff was placed tightly around the wrist. The cuff was inflated to a pressure of 300 mmHg in a step-by-step fashion until the participant first reported pain. The pain threshold was defined as the lowest pressure at which the participants reported pain. After the pain threshold was reached, the pressure was increased to 300 mmHg and held for 15 sec and participants were then asked to rate their degree of pain. Salivary testosterone and cortisol levels, pain thresholds, pain ratings, anxiety ratings, blood pressure, and heart rate were measured under resting and stress conditions in the spring and summer. Ratings were assessed using the Numerical Rating Scale (NRS) ranging from 0 to 100 (0 = no pain and anxiety; 100 = maximum imaginable pain and anxiety). Data were collected from 46 participants during the spring (n=25) or summer (n=21).
Results: Testosterone levels and pain thresholds were significantly lower for all participants (n=46) under stress than at rest, while cortisol levels, pain ratings, anxiety ratings, systolic blood pressure and heart rate were significantly higher under stress than at rest. In the 25 participants sampled during the spring, testosterone levels were significantly higher at rest than under stress (p = 0.005), but there was no significant difference in cortisol levels at rest vs. under stress (p = 0.689). Pain and anxiety ratings and pain thresholds did not vary significantly by season. In the 21 participants sampled during the summer, there was no significant difference in testosterone levels at rest and under stress (p = 0.428), but cortisol levels were significantly higher under stress than at rest (p = 0.006). As mentioned above, pain and anxiety ratings and pain thresholds did not vary significantly by season.
Discussion: The results of this study indicate that seasonal variations in testosterone and cortisol levels under stress and at rest may affect pain responses, and these variations should be taken into account in future studies investigating responses to pain stimuli. These results also suggest that acute clinical pain, similar to the pressure pain used in the present study, may be relieved when a participant is under stress in the spring by preventing a decrease of testosterone and in the summer by preventing large increases of cortisol.
1623101 - META-ANALYSIS: EPIDURAL OPIOIDS FOR POSTOPERATIVE ANALGESIA
Nayer Youssef1, David Orlov
1, Tristan Alie
1, Matthew Chong
2, Toni Tidy
1, James E. Paul
1
1. Department of Anesthesia, McMaster University, Hamilton, ON, Canada
2. Michael G. DeGroote School of Medicine, McMaster University, Hamilton, ON, Canada
Introduction: Epidural opioids are widely used for the facilitation of central neuraxial blockade and
postoperative analgesia. Despite this, the optimal opioid with the least side effects and best analgesia
remains controversial.
Methods: We conducted a meta-analysis of RCTs that compared at least two continuous epidural
infusions for acute postoperative analgesia over at least 24h. Visual-analogue scale (VAS) pain scores
were the primary outcome. Secondary outcomes included opioid side effects, such as pruritus, post-
operative nausea and vomiting (PONV), respiratory depression, hypotension, sedation, and total opioid
consumption.
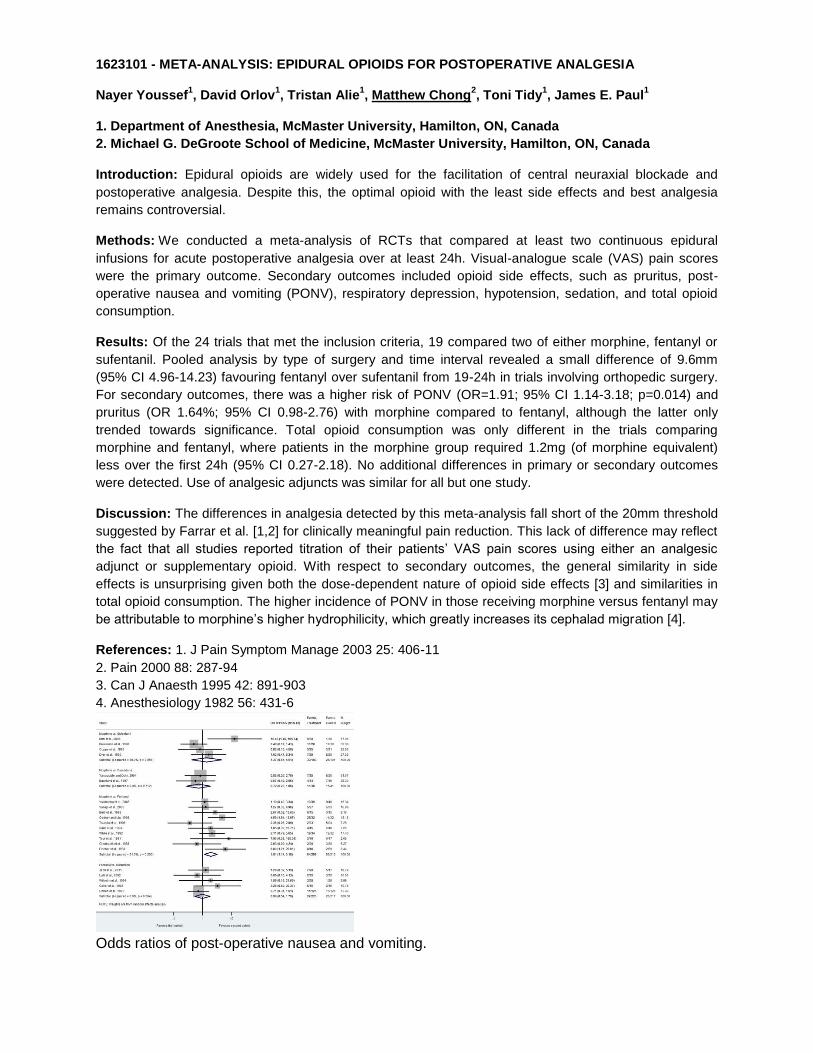
Results: Of the 24 trials that met the inclusion criteria, 19 compared two of either morphine, fentanyl or
sufentanil. Pooled analysis by type of surgery and time interval revealed a small difference of 9.6mm
(95% CI 4.96-14.23) favouring fentanyl over sufentanil from 19-24h in trials involving orthopedic surgery.
For secondary outcomes, there was a higher risk of PONV (OR=1.91; 95% CI 1.14-3.18; p=0.014) and
pruritus (OR 1.64%; 95% CI 0.98-2.76) with morphine compared to fentanyl, although the latter only
trended towards significance. Total opioid consumption was only different in the trials comparing
morphine and fentanyl, where patients in the morphine group required 1.2mg (of morphine equivalent)
less over the first 24h (95% CI 0.27-2.18). No additional differences in primary or secondary outcomes
were detected. Use of analgesic adjuncts was similar for all but one study.
Discussion: The differences in analgesia detected by this meta-analysis fall short of the 20mm threshold
suggested by Farrar et al. [1,2] for clinically meaningful pain reduction. This lack of difference may reflect
the fact that all studies reported titration of their patients’ VAS pain scores using either an analgesic
adjunct or supplementary opioid. With respect to secondary outcomes, the general similarity in side
effects is unsurprising given both the dose-dependent nature of opioid side effects [3] and similarities in
total opioid consumption. The higher incidence of PONV in those receiving morphine versus fentanyl may
be attributable to morphine’s higher hydrophilicity, which greatly increases its cephalad migration [4].
References: 1. J Pain Symptom Manage 2003 25: 406-11
2. Pain 2000 88: 287-94
3. Can J Anaesth 1995 42: 891-903
4. Anesthesiology 1982 56: 431-6
Odds ratios of post-operative nausea and vomiting.

1636976 - OUTCOMES OF A GROUP PAIN SELF-MANAGEMENT PROGRAM 2007-2011
Alexander J. Clark1, Douglas Cane
2, Mary E. Lynch
1, Darlene Davis
2
1. Department of Anesthesia, Pain Management and Perioperative Medicine, Dalhousie University, Halifax, NS, Canada 2. Pain Services, Capital Health, Halifax, NS, Canada
Introduction: Individuals who attend our interdisciplinary led group Pain Self-Management Program (12-3 hr sessions) and Follow-up Program (3-3 hr sessions) complete a comprehensive assessment at the start/end of the program and at follow-up as part of a structured program evaluation. The goals of the program are to: promote active coping strategies, decrease psychological distress, develop an ongoing exercise plan, increase satisfaction with performance of daily activities, adopt a more self-reliant approach to pain management and provide specific strategies to manage pain. The purpose of the evaluation is to assess changes in pain experience, affect, general functioning, beliefs about pain, and activity patterns.
Methods: Our Ethics Committee does not require approval of this evaluation (QA program). Individuals with chronic pain completed measures of activity patterns, pain intensity, affect, perceived disability, pain control, and acceptance of pain before and after a group pain management program. Average treatment effect size (the difference between pre- and post-treatment/follow-up scores divided by the standard deviation of the pre-treatment scores) is used to describe outcomes.
Results: 521 individuals with chronic pain attended the program from 2007-2011. 85% completed the program and attended 10.4/12 sessions. Average age was 49.5 yrs and 64% were women. Median time since onset of pain was 7.1 yrs (range 1-53 yrs). 53% reported multi-site pain, 18% - back pain and 8% - neck and head pain. Complete data sets were available for 307 individuals pre- and post-treatment and 114 individuals pre-treatment and post follow-up. By convention treatment effect sizes of .20-.50 are described as small, .50-.80 as moderate, and >.80 as large. Effect sizes are presented such that larger numbers indicate greater improvement. The table details the treatment effects sizes for the measures used.
Discussion: Overall, significant but small, treatment effects were observed in all domains at the end of a pain self-management program and at follow-up 3 months later. The largest changes were noted with respect to beliefs about pain and patterns of activity. The present results provide support for both the immediate and longer-term efficacy of interdisciplinary pain self-management programs.
Pre- vs. Post-Group Treatment Effect
Size Pre- vs. Follow-up Treatment Effect
Size
Pain Intensity
PPI-L .32 .26
PPI-W .39 .02
Affect
BDI .36 .41
STAI-T .28 .20
General Functioning
PDI .23 .29
SF-P .19 .22
SF-M .32 .14
Beliefs about Pain
PCS .35 .58
TSK .45 .43
SOPA-C .65 .45
CPAQ .35 .45
Patterns of Activity
POAMP-A .17 .17

POAMP-O .39 .40
POAMP-P .32 .54
Abbreviations: PPI-L/W – Present Pain Intensity – Least/Worse
BDI – Beck Depression Inventory STAI-T – State-Trait Anxiety Inventory – Trait
PDI – Pain Disability Index SF-P/M – SF-36
Physical/Mental Functioning PCS – Pain Catastrophizing Scale
TSK – Tampa Scale of Kinesiophobia SOPA-C – Survey of Pain Attitudes – Pain Control CPAQ – Chronic Pain Acceptance Questionnaire
POAMP-A/O/P – Patterns of Activity Measures – Avoidance/Overdoing/Pacing

1650609 - PREGABALIN FOR ACUTE POSTOPERATIVE PAIN- A SYSTEMATIC REVIEW AND META- ANALYSIS OF RANDOMIZED CONTROLLED TRIALS
Naveen Eipe1, John Penning
1, Mohammed Ansari
2, Fatemeh Yazdi
2, Lucy Turner
2
1. The Ottawa Hospital, Ottawa, ON, Canada 2. Knowledge Synthesis Group, Centre for Practice-Changing Research, Ottawa Hospital Research Institute, Ottawa, ON, Canada
Introduction: The objective of this systematic review and meta- analysis was to update the assessment of the effects of pregabalin on postoperative pain, analgesic consumption, and adverse events in comparison with placebo in adults undergoing surgery and further investigate the heterogeneity in findings across subgroups of surgical pain models.
Methods: We prospectively registered our systematic review (PROSPERO registration number CRD42012002078) and published an a priori peer-reviewed detailed protocol to which our research conduct has been adherent [1]. In July 2012, we completed the search of MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials as described in the published protocol[2].
Results: A total of 1140 citations were retrieved. After full text screening, 32 RCTs (total n=2781; Pregablin n=1568, control n=1213) were included for both quantitative and qualitative analysis. Due to inconsistency in how outcomes were measured and reported, we report results by dose and time point. Ten studies assessing 501 patients compared placebo with patients receiving pregabalin at 24 hours and showed a reduction in average total analgesic consumption (RoM 0.77; 95% CI:0.66 – 0.88; ), postoperative pain at 300mg at 24 hours for VRS-in movement (MD -0.02; 95% CI:-0.23to 0.19; P 0.86) and decreased nausea and vomiting (RR = 0.83; 95% CI:[0.71, 0.96]; P 0.01). No significant reduction in pain scores at any time point or dose range was observed. Nausea and vomiting was significantly reduced in patients receiving pregabalin- 32 studies were pooled at the highest dosage and maximum time point reported this.
Discussion: This meta-analysis revealed a lower risk for postoperative analgesic consumption and nausea/ vomiting with perioperative pregabalin use in comparison with placebo in adults undergoing surgery; however, the influence of pregabalin on measurements of postoperative pain is less clear. Clinical and methodological heterogeneity was very prominent for all meta-analyses. It appears that use of pregabalin in minor surgical procedures exposes these patients to increased risk of adverse events. Further clinical trials in these less painful models should be discouraged [3]. Overall, improvements in acute pain management with pregabalin are seen in certain patients undergoing some surgeries; further studies should be directed towards identifying these patients and standardising the ways in which outcomes for these trials are reported.
References: 1. Systematic Reviews 2012; 1:40. 2. Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series, Wiley Online Library. 2008; 243-96. 3. Pain Res Manag 2011; 16:353–6.
1650616 - UNILATERAL EPIDURAL BLOCK IN LOWER LIMB VASCULAR SURGERY PATIENTS - MYTH OR REALITY?
Ali Faris1, Qutaiba A. Tawfic
1, Naveen Eipe
1, John Penning
1
1. The Ottawa Hospital, Ottawa, ON, Canada
Introduction: Epidural anesthesia/analgesia is a frequently used for lower limb vascular surgeries. Unilateral epidural block is one of the major drawbacks that can affect the usefulness of postoperative epidural analgesia when it relates to the non-operative side [1,2]. The purpose of this study is to identify the incidence of postoperative failure of epidural analgesia in patients who underwent lower limb vascular surgeries. Furthermore, we aim to recognize the contribution of unilateral epidural block to this problem.
Methods: REB approval was obtained to do this retrospective study. Definition of unilateral epidural analgesia and the criteria of failure of post-operative epidural analgesia were identified a priori. Patients who had epidural catheter placement for unilateral lower limb vascular surgeries between January 1, 2008 and July 1, 2011 were included in this study. The required cohort of patients was obtained from the Operating Room (OR) census and charts were accessed from the medical records. Data from anesthesia charts, acute pain service order sheets and follow up charts were reviewed and collected.
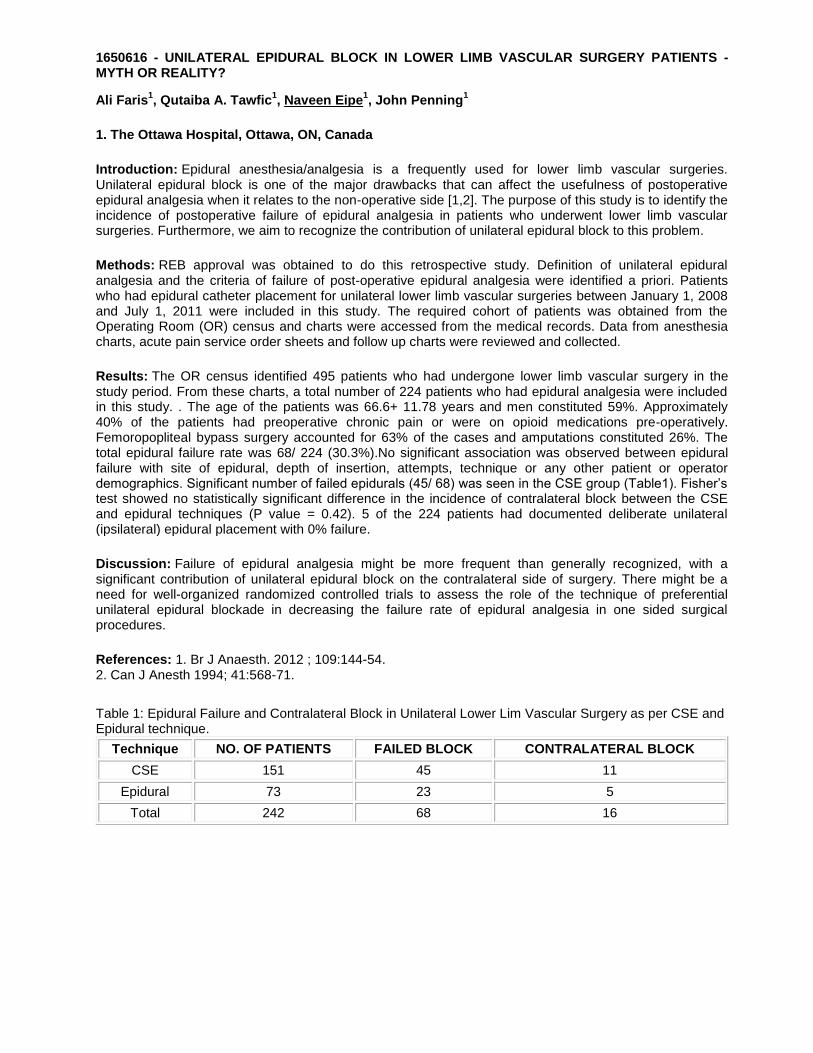
Results: The OR census identified 495 patients who had undergone lower limb vascular surgery in the study period. From these charts, a total number of 224 patients who had epidural analgesia were included in this study. . The age of the patients was 66.6+ 11.78 years and men constituted 59%. Approximately 40% of the patients had preoperative chronic pain or were on opioid medications pre-operatively. Femoropopliteal bypass surgery accounted for 63% of the cases and amputations constituted 26%. The total epidural failure rate was 68/ 224 (30.3%).No significant association was observed between epidural failure with site of epidural, depth of insertion, attempts, technique or any other patient or operator demographics. Significant number of failed epidurals (45/ 68) was seen in the CSE group (Table1). Fisher’s test showed no statistically significant difference in the incidence of contralateral block between the CSE and epidural techniques (P value = 0.42). 5 of the 224 patients had documented deliberate unilateral (ipsilateral) epidural placement with 0% failure.
Discussion: Failure of epidural analgesia might be more frequent than generally recognized, with a significant contribution of unilateral epidural block on the contralateral side of surgery. There might be a need for well-organized randomized controlled trials to assess the role of the technique of preferential unilateral epidural blockade in decreasing the failure rate of epidural analgesia in one sided surgical procedures.
References: 1. Br J Anaesth. 2012 ; 109:144-54. 2. Can J Anesth 1994; 41:568-71.
Table 1: Epidural Failure and Contralateral Block in Unilateral Lower Lim Vascular Surgery as per CSE and Epidural technique.
Technique NO. OF PATIENTS FAILED BLOCK CONTRALATERAL BLOCK
CSE 151 45 11
Epidural 73 23 5
Total 242 68 16

1651482 - DETERMINING AN INFUSION REGIMEN FOR INTRAVENOUS LIDOCAINE INFUSION
James Khan1, Maaz Yousuf
1, Naveed Siddiqui
1
1. Anesthesia, University of Toronto, Toronto, ON, Canada
Introduction: Numerous studies have indicated that intravenous lidocaine infusions (IVLI) during bowel surgeries can significantly reduce postoperative pain, nausea and vomiting, and time to hospital discharge1. IVLI have also been included in enhanced-recovery protocols where thoracic epidurals are either contraindicated or refused2. Since no standardized IVLI regimen exists, there has been reluctance to adopt this practice due to confusion about dosing and duration of infusion extending beyond PACU to less monitored setting of hospital wards. Using a quantitative review of the literature, we investigate a possible dosing regimen and evaluate whether an early or late infusion stop time yields comparable outcomes after bowel surgery.
Methods: A systematic search was conducted using Ovid, Embase, CINAHL, and Cochrane CENTRAL databases. All randomized controlled trials (RCTs) were included and studies were selected for intravenous lidocaine infusion in bowel surgery while under general anesthesia. Studies were divided by infusion stop time: 1) within 60 min postoperative and 2) beyond 60 min postoperatively. Hospital length of stay, postoperative pain scores, opioid use, nausea and vomiting, and complications were collected and compared between the two groups. Data on lidocaine bolus and infusion dosing used in the studies were collected.
Results: A total of seven randomized controlled trials were found. All studies used a lidocaine bolus with induction, 6 of the studies used a dose of 1.5mg/kg. Five studies used a weight-based infusion ranging from 1.5 – 3.0 mg/kg/hr (mean ± SD: 2 ± 0.61). Three studies (160 patients) stopped their IVLI prior to 60 min postoperatively, and 4 studies (202 patients) continued beyond 60 minutes, with one study extending up to 5 days postoperatively. Weighted effect sizes were calculated for hospital length of stay, postoperative pain scores, opioid use, nausea and vomiting, and complications and there were no differences between the two groups. No case of local anesthetic toxicity was reported in any study.
Discussion: Intravenous lidocaine infusions are a useful adjunct during bowel surgery when a thoracic epidural is contraindicated or refused. The literature suggests a dosing regimen of a lidocaine bolus dose of 1.5mg/kg with induction and an infusion rate at 2mg/kg/hr. There are no additional advantages of extending an intravenous lidocaine infusion beyond 60 minutes postoperatively. These results may help in simplifying the strategies and reducing barriers for the perioperative use of lidocaine infusion.
References: 1. Brit J Surg 2007 95: 1331 – 1338 2. Anesthesiology 2007 106: 11-18

1651993 - MULTIMODAL ANALGESIA WITH LIDOCAINE FOR ACUTE PAIN- A RETROSPECTIVE STUDY
Qutaiba A. Tawfic1, Naveen Eipe
1, John Penning
1
1. The Ottawa Hospital, Ottawa, ON, Canada
Introduction: Lidocaine is an amide local anesthetic with a significant analgesic, anti-hyperalgesic and anti-inflammatory properties when used intravenously. In 2009, the Acute Pain Service of a tertiary level university hospital implemented a protocol for the use of lidocaine infusions for perioperative pain management. The aim of this study was to review this use of intravenous lidocaine over a three year period.
Methods: After approval from Research and Ethics Board, this retrospective study was completed. A list of patients for whom lidocaine was dispensed from the pharmacy was obtained from September 2009 to August 2012. This inpatient study included only those patients who received lidocaine infusion for pain. Patients receiving lidocaine only as a bolus, for other indications and in the ICU while on ventilatory or inotropic support were excluded. The data from anesthesia charts, acute pain service order sheets, pain assessments and acute pain medications administration records were reviewed. Indications, demographics, impact and side- effects for the patients receiving lidocaine were collected.
Results: In the study period, 169 patients were identified as having received lidocaine. After exclusions, 102 patients were included in this study. The patients were 52% male with mean age 53 years (±36). The mean weight was 75 kg (range 40-80 kg) .The indications for intravenous lidocaine were laparotomy (49%),spine surgery (16.7%), polytrauma (12.7%), amputations (6.9%), hysterectomy (5.9%), orthopedics (3.4%) and others (4.9%). History of chronic pain was present in 50%, while only 35.3% of whole patients were chronic opioid users. Bolus dose was used 95% of our patients, with a mean dose of 1.34 mg/Kg (range 0.75- 2.5). The infusion dose was ranging between 0.5-2 mg/kg/hour. Lidocaine infusion was started as a part of intraoperative care and continued postoperatively in 61 patients (60%). Regarding the other 41 patients (40%), it was started as adjuvant after failure of the initial plan in controlling pain. Table 1 is showing the duration of lidocaine infusion. Mild side effects and/or signs of toxicity were reported in 10 patients (9.8%) and the infusion was stopped for 8 of them. No serious side effects or toxicity was reported.
Discussion: This quality assurance study reports the safety and efficacy of intravenous lidocaine by an Acute Pain Service. The use of lidocaine for acute pain outside the anesthesia and critical care environment has not been previously reported and requires further investigation.
References: 1. Can J Anaesth. 2011; 58:22-37. 2. Br J Surg. 2008 ;95:1331-8.
Table 1: The duration of lidocaine infusion for acute pain management
Duration of infusion(Days) No. Of patients %
<1 3 2.9
1 18 17.6
2 41 40.2
3 34 33.3
4 6 5.9
Total 102

1652580 - A META-ANALYSIS ON THE CLINICAL EFFECTIVENESS OF SUPERFICIAL CERVICAL PLEXUS BLOCKS AFTER THYROID SURGERY
Katsushi Doi1, Hiroshi Hoshijima
2, Norifumi Kuratani
3, Yasue Kashiwagi
1
1. Anesthesiology, Hamada Medical Center, Hamada, Shimane, Japan 2. Anesthesiology, Saitama Medical University Hospital, Moroyama, Saitama, Japan 3. Anesthesiology, International University of Health and Welfare Hospital, Nasushiobara, Tochigi, Japan
Introduction: Thyroid surgery can cause mild to moderate postoperative pain. Recently, the use of superficial cervical plexus blocks (SCPBs) as an analgesic technique for thyroid surgery has been reported. There has, however, been little information about the efficacy of SCPBs in terms of postoperative analgesia following thyroid surgery. In this study, we performed a meta-analysis of randomized controlled trials to assess the analgesic efficacy of SCPBs combined with general anesthesia (GA).
Methods: A comprehensive search of the literature was conducted to identify clinical trials comparing a placebo with SCPBs following thyroid surgery. Two reviewers independently assessed each report to confirm that all reports met our inclusion criteria. The primary outcomes were determined to be acute postoperative pain scores. Visual analogue pain scores and numerical rating scales were converted to a standardized 0-10 scale. The secondary outcomes were number of patients who needed postoperative rescue analgesics. The data from each trial were combined using the randomized-effects model to calculate the weight mean difference (WMD), pooled risk ratio (RR) and their corresponding 95% confidence intervals (CIs). Funnel plots were used to assess publication bias.
Results: Eight randomized controlled trials met our inclusion criteria. Overall, 342 patients received SCPBs and 277 received placebos. The use of SCPBs reduced pain scores at 0 hrs (WMD -1.01, 95% CI -1.84 to -0.18), 2 hrs (WMD -1.04, 95% CI -2.01 to -0.07) , 6 hrs (WMD -0.69, 95% CI -1.27 to -0.11), and 24 hrs (WMD -0.485, 95% CI -0.90 to -0.07), but did not reduce pain scores at 12 hrs, postoperatively. There was a significant difference in the number of patients who needed postoperative rescue analgesics between SCPBs and GA alone (RR, 0.54; 95% CI 0.35 to 0.84). The heterogeneity of the data was not statistically refuted. Publication bias was evident in a funnel plot.
Discussion: Although Warschkow et al reported that SCPBS has a low efficacy after performing the meta-analysis; they did not analyze the number of patients who needed postoperative rescue analgesics 1). Our analysis revealed that the use of SCPBs in addition to GA provides a better postoperative pain control compared with the use of GA alone.
References: 1) Warschkow R, et al. Thyroid 2012; 22: 44-52

1652827 - FIVE YEARS OF PERI-OPERATIVE OPIOID USE AT A TERTIARY CARE CENTRE
Peter MacDougall1, Paul Brousseau
1, Andrew D. Milne
1
1. Anesthesiology, Pain Management and Peri-operative Medicine, Dalhousie University, Halifax, NS, Canada
Introduction: Nearly every type of surgery is associated with a chronic pain state ( 1,2). The relationship between the peri-operative period and long term opioid use is not understood. A large dataset was created by combining the Anesthesia Information Management System (AIMS) and the provincial prescription monitoring program (PMP) database (3). This allows us to characterize the use of prescription opioids before and after surgery.This study outlines a review of the peri-operative opioid use of for all patients having surgery over a 5 year period at a tertiary care centre.
Methods: REB approval was obtained. The study is a retrospective review of data from a large dataset (3). Inclusion criteria were 1) One surgical procedure during the selected time period; 2) At least one opioid prescription within 6 months prior to or following the surgical procedure. Exclusion criteria were 1) Admission for surgery within six months of discharge from a previous surgery; 2) Absence of prescription for opioids. Pre-operative opioid use was classified as (i) Naive (no pre-op prescription), (ii) Acute (prescriptions for at least 75% of days for </= 3 months prior to surgery), (iii) Intermittent (prescriptions for < 75% of days for </= 3 months prior to surgery; (iv) Chronic (prescriptions for at least 75% of days for > 3 months prior to surgery. Post operative use was described as prescriptions for 75% of the time period described.
Results: There were 49, 463 cases with single admission within the study window. 9207 patients were prescribed opioids pre-operatively. These include Acute -676 cases, Intermittent – 7039 cases, chronic – 1492 cases. There were 40,256 naïve cases of which 23,365 cases had linked opioid prescriptions. Of the naïve cases, 17,619 cases had post-operative prescriptions. Hydromophone was the most commonly prescribed opioid. This was followed by acetaminophen/opioid combination products, morphine and oxycodone. Opioid use was dramatically reduced in the post-operative period and reached a nadir at month 2. This reduction was maintained at 6 months. The percent of patients using opioids in the post-operative period was related to the use of opioids in the preoperative period.
Discussion: Linkage of two large datasets allows elucidation of the relationship between prescribing opioids and surgery. Overall, the rate of opioid use declines significantly one month after surgery suggesting that surgery may reduce the need for opioid treatment. Rates of post – operative opioid use appears to be related to the rate of pre-operative use. Hydropmorphone is the most commonly prescribed opioid.
References: 1) Macrae WA. Chronic pain after surgery. Br J Anaesth. 2001;87(1):88. 2) Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101(1):77. 3) Gandhi N, MacDougall P, Milne AD, Brousseau P, Pellerin D, Bishop D, Whynot S. CAS 2012.

1653043 - KETAMINE PLUS MORPHINE FOR PATIENT CONTROLLED ANALGESIA: A META-ANALYSIS Janet Martin1, Li Wang1, Bradley Johnston2, Alka Kaushal2, Davy C. Cheng 1 1. EPiCOR Group, MEDICI Centre, Department of Anesthesia & Perioperative Medicine, University of Western Ontario, London, ON, Canada 2. Department of Anesthesia and Pain Medicine, The Hospital for Sick Children, Toronto, ON, Canada Introduction: Ketamine, an antagonist of the N-methyl-D-aspartate receptor, is of increasing interest in pain management, especially in sub-anesthetic doses. Objectives: To assess the efficacy and safety of ketamine plus morphine in PCA versus morphine PCA alone for acute postoperative pain in adults. Methods: Comprehensive searches of PUBMED, EMBASE, Cochrane Library, and three Chinese databases (CBM, CNKI, and WanFang) were performed up to the end of April 2012. Randomized trials (RCTs) comparing the combination of ketamine plus morphine in PCA versus morphine PCA for acute postoperative pain in adults were eligible. Outcomes of interest included pain intensity, cumulative morphine consumption, patient satisfaction, and adverse events. Two authors independently assessed risk of bias of included trials and extracted data. Meta-analysis was performed using the random effects model to calculate risk ratio (RR, 95%CI) and weighted mean differences (WMD, 95%CI). Subgroup analyses of pain score and cumulative morphine consumption were performed for: type of surgery, mode and duration of ketamine administered, use of nitrous oxide and postoperative analgesics, risk of bias, and language of publication. Meta-regression was performed to evaluate the ketamine dose-response relationship. Results: Of the 698 citations retrieved, 27 RCTs involving 1885 patients were included. Using the Cochrane Risk of Bias tool, 14/27 included studies were of high quality. Compared with morphine alone PCA, ketamine + morphine PCA significantly decreased postoperative pain intensity on visual analog scale (VAS); however, the differences were small at 6 hours (WMD -0.5 cm, 95%CI -0.8, -0.2 cm), at 12 hours (WMD -0.6 cm, 95%CI -0.8, -0.4 cm), at 24 hours (WMD -0.6 cm, 95%CI -0.7, -0.4 cm), at 48 hours (WMD -0.4, 95%CI -0.6, -0.2cm), and at 72 hours (WMD -0.7cm, 95%CI -1.1, -0.3 cm). Ketamine + morphine also reduced cumulative morphine consumption at 24 hours (WMD -9 mg, 95%CI -12, -6 mg), and at 48 hours (WMD -22 mg, 95%CI -28, -15mg). At 72 hours, the reduction was no longer significant (WMD -19 mg, 95%CI -39, +0.77) with inadequate data. Postoperative nausea and vomiting (PONV) was also significantly reduced (RR 0.73, 95%CI 0.62, 0.87). The reduction in pain intensity and in cumulative morphine consumption was not significantly associated with the pre-defined subgroup factors (interaction p > 0.05). No statistical dose-response relationship was found for any outcome (p>0.05). No significant difference was found for patient satisfaction (RR 1.5, 95%CI 0.8, 2.6). No significant difference was found in hallucination (RR 1.33, 95%CI 0.83, 2.13), vivid dreams (RR 1.24, 95%CI 0.79, 1.96), and other adverse events between groups; however, these outcomes were rarely reported in the studies. Discussion: Ketamine plus morphine in PCA reduces postoperative pain, cumulative morphine consumption, and PONV, with no reported difference in ketamine-related adverse events. However, the true incidence of adverse events remains undefined due to insufficient reporting within existing RCTs.