carl h. june, md -...
TRANSCRIPT

Adoptive cellular therapies
Carl H. June, MDRichard W. Vague Professor in ImmunotherapyDepartment of Pathology and Laboratory Medicine Director, Center for Cellular Immunotherapies Director, Parker Institute for Cancer ImmunotherapyUniversity of Pennsylvania Perelman School of MedicinePhiladelphia, PA
IMMUNOTHERAPY: TRANSFORMATION OF THERAPIES FOR BLOOD CANCER
Disclosures§ I disclose the following relationships
§ Novartis: Grants/Research Support§ Novartis: Royalty Recipient§ Tmunity: stockholder
§ I will discuss investigational use in my presentation:§ CTL019, CART-BCMA
2

IMMUNOTHERAPY: TRANSFORMATION OF THERAPIES FOR BLOOD CANCER
Goals
§ The purpose of this presentation is to§ Provide update on states of adoptive cell therapy
§ After this session, learners should be better able to§ Understand toxicities from CD19 directed CAR T cells§ Manage cytokine release syndrome§ Awareness of need for immunoglobulin replacement therapy in
patients with persistent B cell aplasias
3

Deep Pipeline of Cancer Immunotherapies
(multiple)
Nature Reviews Drug Discovery (2016) doi:10.1038/nrd.2015.35
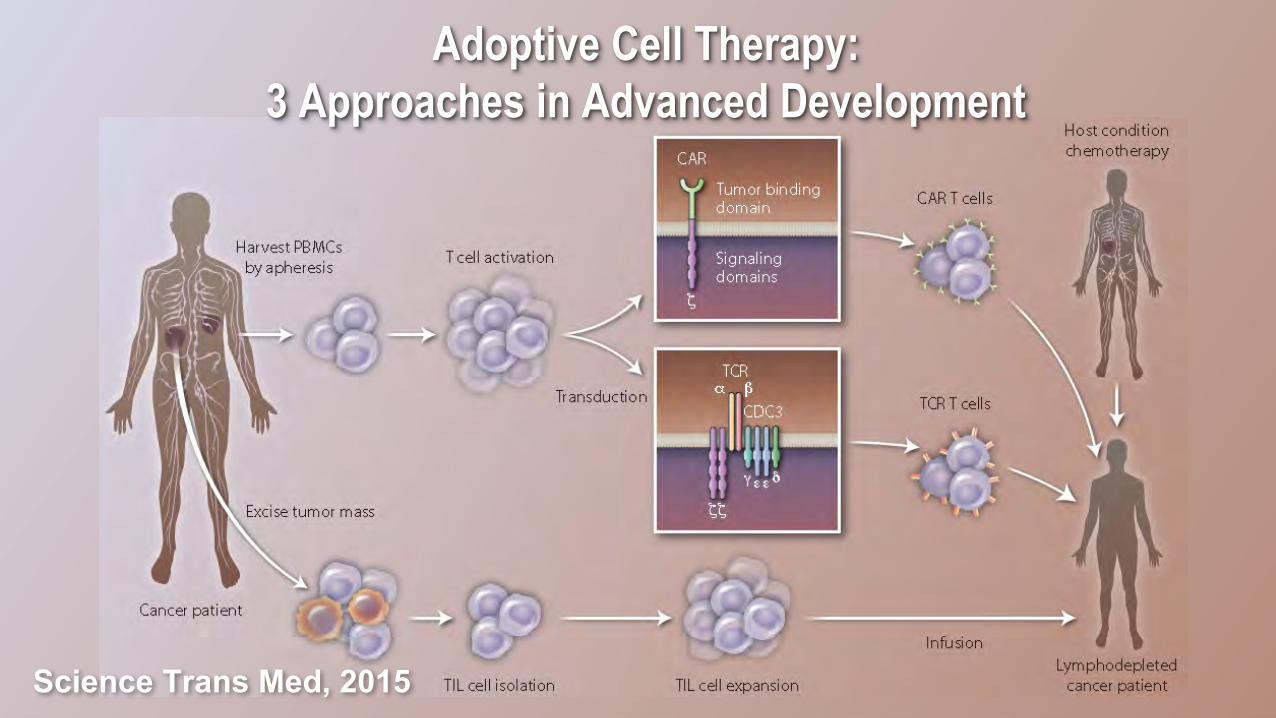
Adoptive Cell Therapy: 3 Approaches in Advanced Development
Science Trans Med, 2015

Other Investigational Adoptive Cellular Therapies in Hematologic Malignancies*
Agent Sponsor Phase Cancer Type Trial ID
KTE-C19 Kite2 NHL ZUMA-1
1/2 ALL ZUMA-3
JCAR014
Juno
1/2 CLL, ALL, NHL NCT01865617
JCAR015 2 ALL ROCKET
JTCR016 1/2 AML NCT01640301
NY-ESO TCR Adaptimmune 1/2 MM NCT01352286
BB2121 Bluebird Bio 1 MM NCT02658929
*Clinicaltrials.gov
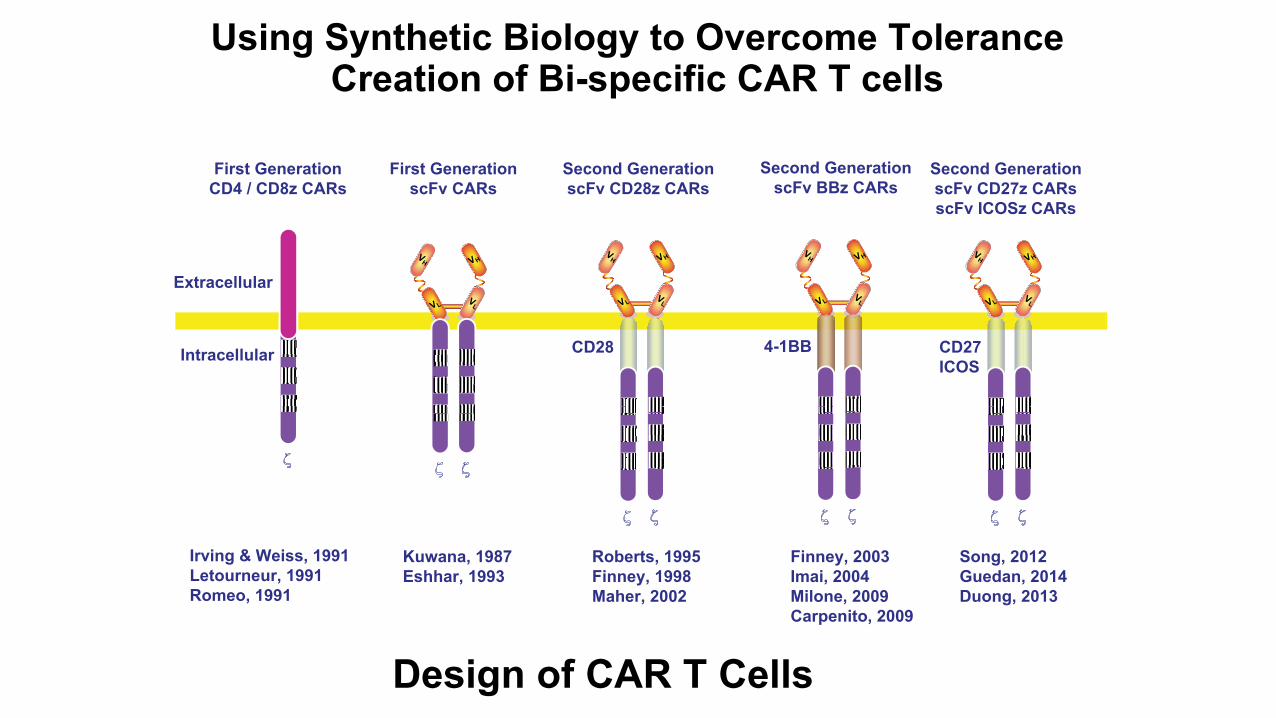
Design of CAR T Cells
Using Synthetic Biology to Overcome ToleranceCreation of Bi-specific CAR T cells
Extracellular
Intracellular
First GenerationCD4 / CD8z CARs
VH
VLV
L
VHVH
VLV
L
VH
First GenerationscFv CARs
VH
VLV
L
VHVH
VLV
L
VH
Second GenerationscFv BBz CARs
4-1BB
Finney, 2003Imai, 2004Milone, 2009Carpenito, 2009
CD28
VH
VLV
L
VHVH
VLV
L
VH
Second GenerationscFv CD28z CARs
Roberts, 1995Finney, 1998Maher, 2002
CD27ICOS
VH
VLV
L
VHVH
VLV
L
VH
Second GenerationscFv CD27z CARsscFv ICOSz CARs
Song, 2012Guedan, 2014Duong, 2013
Kuwana, 1987Eshhar, 1993
Irving & Weiss, 1991Letourneur, 1991Romeo, 1991
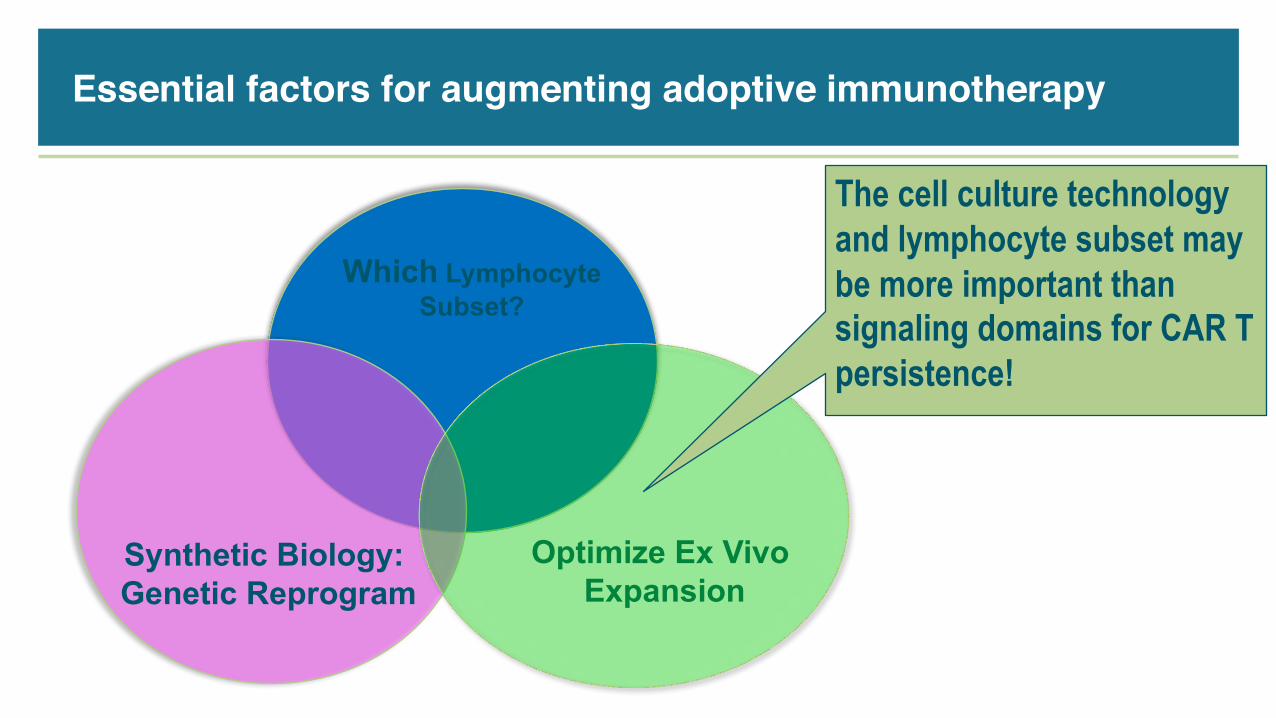
Essential factors for augmenting adoptive immunotherapy
Which LymphocyteSubset?
Optimize Ex Vivo Expansion
Synthetic Biology: Genetic Reprogram
The cell culture technology and lymphocyte subset may be more important than signaling domains for CAR T persistence!

Cumulative Patient Safety: Exposure to Genetically Modified T cellsUniversity of Pennsylvania (as of May 2016)
Pharmacovigilance
Trial EngineeredTCell #PatientsInfused Safety(Patient-Years)CD4zCAR(HIV) RetroviralCAR 44 745.6SangamoZFNCCR5(HIV) Ad5/35zincfingernuclease 12 65.0SB-728mRCCR5ZFN CCR5ZFN 7 3.1MAZ-Takara(HIV) RetroviralMazF 10 14.1VirxSysVRX496(HIV) LentiviralantisenseHIVenv 20 186.9Adaptimmune(HIV) LentiviralgagTCR 2 9.1AdaptimmuneNY-ESO-1 LentiviralNY-ESO1TCR 21 79.3NovartisCTL019(tisagenlecleucel-T) Lentiviral19:BBzCAR 224 335.5UPCC19214CART-MESO-19 CART-MESO-19 3 2.1UPCC31213 CART-MESO 15 16.6
Total 368 1457

CART19 (tisagenlecleucel-T ): Overview
Patient DonatesCells
Genetic engineeringExpand T cells
T cell transfusion
Porter, 2011Grupp, 2013Maude, 2014Garfall, 2015
July 31, 20101st CART19 Infusion
SyntheticBiology
PediatricOncology:
ALL
Adult Oncology:ALL, CLL, DLBCL,
MCL, Myeloma
CVPF
Cytokine Release Syndrome
4

CTL019 Phase I Trial for r/r CLL: 5 yr follow upSummary of patient baseline characteristics
N= 14 patients, protocol 04409 (NCT01029366)
§ Overall response rate: 57%
§ CR 4/14 (28%)
§ PR 4/14 (28%)
§ NR 6/14 (43%)
Characteristics Statistics, N(%)N 14Age at infusion in years
Mean (SD)Median (range)
66.9 (8.1)66 (51-78)
GenderMaleFemale
12 (85%)2 (14%)
Number of prior therapiesMean (SD)Median (range)
5.3 (2.8)5 (1-11)
P53 or 17p deletionNoYes
8 (57%)6 (43%)
IGHV mutationNo YesUnknown
9 (64%)4 (29%)1 (7%) Porter et al, Science Trans Med 2015
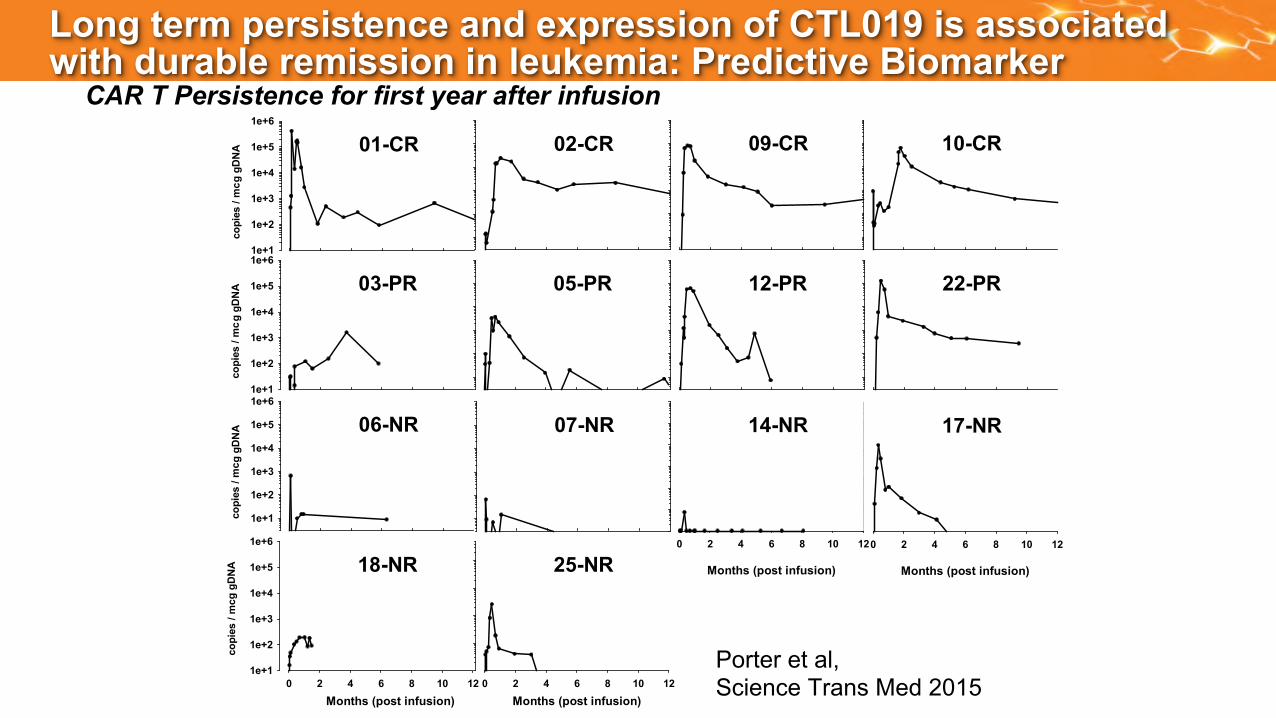
Long term persistence and expression of CTL019 is associated with durable remission in leukemia: Predictive Biomarker
CAR T Persistence for first year after infusion
copi
es /
mcg
gDNA
1e+1
1e+2
1e+3
1e+4
1e+5
1e+6
01-CR
ggD
NA
1e+1
1e+2
1e+3
1e+4
1e+5
1e+6
03-PR
ggD
NA
1e+1
1e+2
1e+3
1e+4
1e+5
1e+6
06-NR 07-NR
05-PR
Months (post infusion)0 2 4 6 8 10 12
25-NR
10 120 2 4 6 8
ggD
NA
1e+1
1e+2
1e+3
1e+4
1e+5
1e+6
18-NR
Months (post infusion)
02-CR 09-CR 10-CR
12-PR 22-PR
Months (post infusion)
0 2 4 6 8 10 12
17-NR
Months (post infusion)
0 2 4 6 8 10 12
14-NR
copi
es /
mc
copi
es /
mc
copi
es /
mc
Porter et al, Science Trans Med 2015

HighResponseRateinRefractory ALL
Youngadult/pediatricphase1:
• 93%CR(57/60pts)
• 22%earlyBcellrecovery(<6months)
• 15%CD19+relapse
DurationofBCellAplasiaisaPredictiveBiomarkerinALL
Mechanisms of Resistance to CD19 CAR T cells
§ Loss of CAR T engraftmentØ Immunogenicity of CAR transgeneØ Exhaustion of CAR T cellsØ Manifest by loss of B cell aplasia
§ Target lossØ CD19 escape Ø Observed in ALL but not CLLØ Prevented by combinatorial targeting?
§ CAR B Cells

Mechanism of resistance in ALL: CD19 escape
Grupp,etal.NEJM2013.Sotilloetal. CancerDiscovery 2015
By flow cytometry, the CD19escape variants lack the epitope recognized by theCAR T cell
PREDICTED PROTEIN PRODUCTS FOR ISOFORMS• CD19 escape is a
combination ofmutations andshifts in splic ingthat favor retainingsome CD19 protein
• DNA mutations canbe subclona l, andmay include splicefactors sites
CART19 Toxicities - I
16
§ B cell aplasiaØ observed in all responding patients to dateØ long-lived plasma cells may survive
Ø managed with IVIG replacement therapy
§ Tumor lysis syndrome (TLS)Ø may be delayed for 20 to 50 days post infusion
§ Macrophage activation syndrome (HLH / MAS)Ø elevated serum ferritin (>500,000 ng/ml), CRP, D-dimer, IL-6, IFN-gamma
§ Cerebral edema: JCAR15 ?

A B
DC
Anti-Streptococcus pneumoniae IgG
0
20
40
60
80
100200250
10
0 90 180
UPCC04409-2UPCC04409-3UPCC04409-5UPCC04409-26UPCC04409-27UPCC04409-31
Day post-CTL019
mg/
L
Anti-Tetanus Toxoid IgG
0
1
2
3
4
0.010 90 180
UPCC04409-2UPCC04409-3UPCC04409-5UPCC04409-26UPCC04409-27UPCC04409-31
Day post-CTL019
mg/
L
Anti-Measles IgG
0 90 180120
UPCC04409-2UPCC04409-3UPCC04409-5UPCC04409-26UPCC04409-27UPCC04409-31
1000
2000
3000
Day post-CTL019
mIU
/mL
Anti-HSV1/2 IgA
0 100 200 300 4000
50
100
150 UPCC04409-27UPCC04409-31CHP959-107CHP959-115CHP959-125
CHP959-115IVIg Monthly
CHP959-107IVIg Monthly
Day pre/post-CTL019
U/m
l
30
CART19 Toxicities – IICD19 Independent Long-lived Plasma Cells
• Patients with persistent B cell aplasia
• Antigen-specific antibody titers at baseline and after CTL019 infusion
• Adults may not require IVIG?
VG Bhoj et al, Blood 2016

CART19 Toxicities - III
18
§ Cytokine release syndrome (CRS)Ø Reversible, on-target toxicityØ Severity related to tumor burden: Treat MRD as outpatient?Ø Cytokine blockade: Therapeutic tocilizumab or pre-emptive tocilizumabØ Role for Jakinibs: RuxolitinibØ Source of IL-6

CART19: ALL Patient #1
Day (post infusions)
0 5 10 15 20 25 30
Seru
m C
ytok
ine
(fold
cha
nge
from
bas
elin
e)
10-1
100
101
102
103
IL-2 IL-6 IFN-g IL-2Ra TNF-a
CHP #100
Grupp et al NEJM 2013 May 2016
April 2012
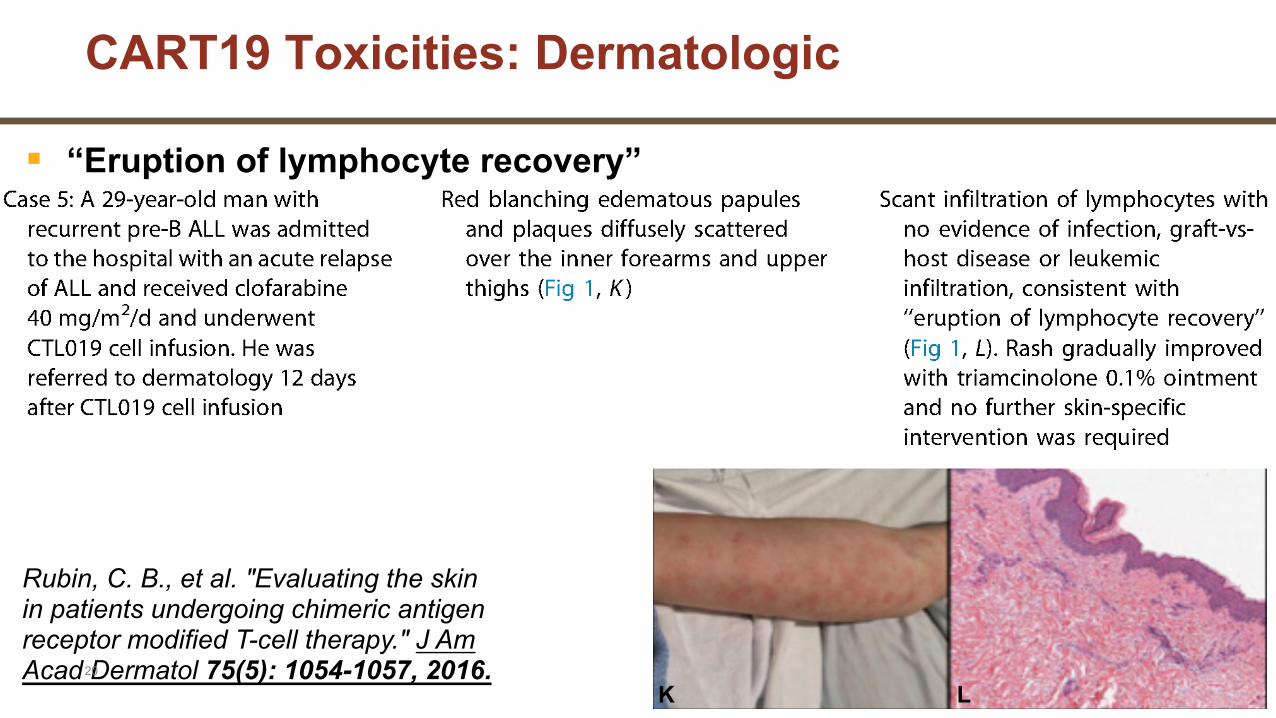
CART19 Toxicities: Dermatologic
Rubin, C. B., et al. "Evaluating the skin in patients undergoing chimeric antigen receptor modified T-cell therapy." J Am Acad Dermatol 75(5): 1054-1057, 2016.20
§ “Eruption of lymphocyte recovery”

International Phase II Trial to Determine Efficacy and Safety of CTL019 in Relapsed and Refractory B-cell ALL (ELIANA)
US sites• Children’s Hospital of Philadelphia• Cincinnati Children’s Hospital• University of Wisconsin• Children’s Medical Center of
Dallas/UTSW• Children’s Mercy Kansas University• Oregon Heath & Science University• Stanford University• University of Minnesota• Children’s Hospital Los Angeles• University of Michigan• Duke University Clinicaltrials.gov NCT02435849
Protocol closed to enrollmentNovartis
Ex- US(Canada, Australia, EU, Japan)• Royal Children’s Hospital (Australia)• Hospital St. Justine (Canada)• Ghent University (Belgium)• Oslo Univ. Hospital (Norway)• Kyoto (Japan)
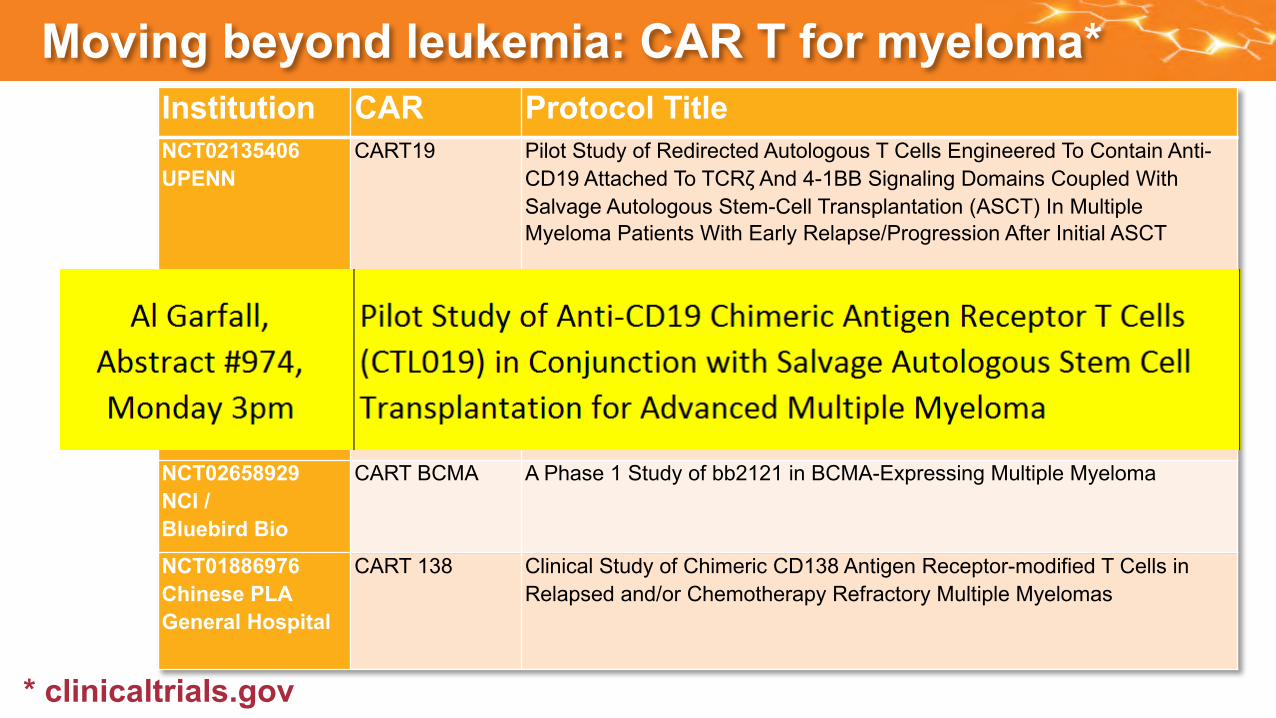
Moving beyond leukemia: CAR T for myeloma*
* clinicaltrials.gov
Institution CAR Protocol TitleNCT02135406UPENN
CART19 Pilot Study of Redirected Autologous T Cells Engineered To Contain Anti-CD19 Attached To TCRζ And 4-1BB Signaling Domains Coupled With Salvage Autologous Stem-Cell Transplantation (ASCT) In Multiple Myeloma Patients With Early Relapse/Progression After Initial ASCT
NCT02215967NCI
CART BCMA A Phase I Clinical Trial of T-Cells Targeting B-Cell Maturation Antigen for Previously Treated Multiple Myeloma
NCT02546167UPENN
CART BCMA Pilot Study of Redirected Autologous T Cells Engineered To Contain an Anti-BCMA scFv Coupled To TCRζ And 4-1BB Signaling Domains in Patients With Relapsed and/or Refractory Multiple Myeloma
NCT02658929NCI / Bluebird Bio
CART BCMA A Phase 1 Study of bb2121 in BCMA-Expressing Multiple Myeloma
NCT01886976Chinese PLA General Hospital
CART 138 Clinical Study of Chimeric CD138 Antigen Receptor-modified T Cells in Relapsed and/or Chemotherapy Refractory Multiple Myelomas
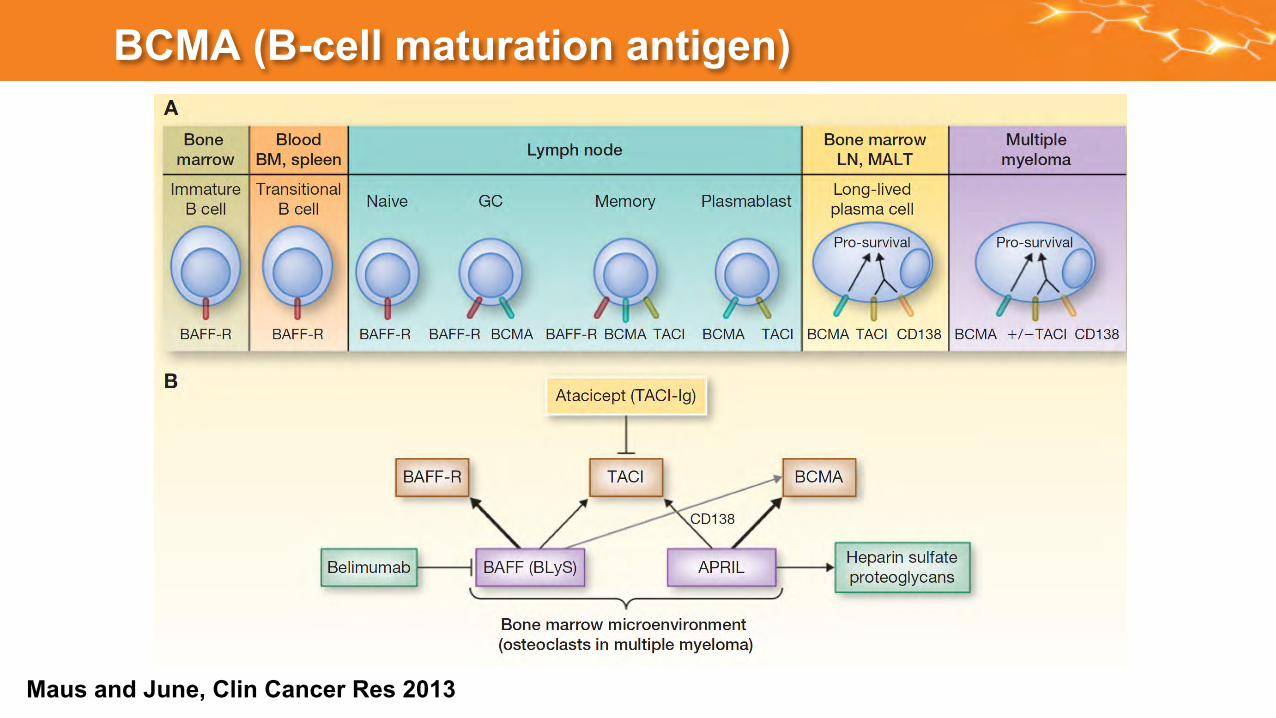
BCMA (B-cell maturation antigen)
Maus and June, Clin Cancer Res 2013

CART-BCMA Cells for Multiple Myelomaclinicaltrials.gov NCT02546167
§ Pilot, first-in-human, 3+3 dose-escalation study
§ n=12-18 rel/ref MM patients (≥ 3 priors)
§ Primary obj: Safety
VH Linker VL CD8aHinge and TM 4-1BB CD3zSignal
seq.
Anti-BCMA scFv
Adam Cohen Michael Milone

CART-BCMA Cells for Multiple MyelomaSubject #1
Interim results
§ Grade 3 CRSà responded to tocilizumab
§ Robust CART-BCMA expansion and persistence: similar to CART19
§ Ongoing sCR (6+ months)
CD8
BC
MA
-CA
R
Pre-tx Day 7
PB CART cells
Day
Seru
m M
-spi
ke
(g/d
L)
IgG
(mg/
dL)

Summary§ As few as one CD19 CAR T cell can eliminate leukemia and lymphoma
§ CAR T directed to CD19 and BCMA have potent activity in myeloma

Challenges and Opportunities: Cell Transfer § In 2017, FDA approval expected for CD19 CAR T cells for
numerous indications: =>challenging logistics of implementing personalized cellulartherapy for widespread application (lessons from Sipuleucel-T)
§Universal “3rd Party” Cells: can off the shelf cells have effects in blood cancers?
§Scale-out issues for manufacturing gene modified autologous T cells:ÞTime frame for fully automated and robotic manufacturing?

Colleagues and Patients: Thank you!PENNMedicineDavidPorterNoelleFreyLynnSchuchter
GillLabSaarGillMarcoRuellaOlgaShestova
LymphomaTeamEliseChongSunita NastaJakubSvobodaMariuszWasikDanLandsburgAnthonyMatoStephenSchuster
CenterforCellularImmunotherapiesAnneChewReginaYoungDanaHammillKatieMarcucciOmkarKawalekarAveryPoseyJohnSchollerShannonMcGettighanBiliangHuAnthonyLinMauroCastellarinGabrielaPlesa
TCellEngineeringYangbingZhaoJiangtaoRenChongyun FangXiaojunLiuShuguangJiang
MiloneLabMichaelMiloneRoddyO’ConnorSabaGhassemiSeleneNunez-Cruz
MyelomaTeamAdamCohenAlGarfallMichaelMiloneEdwardStadtmauer
CVPFBruceLevineDonSiegelSuzetteArosteguiTheresaColligonClareTaylorAnneLamontagneAlexMalykhinMattO’Rourke
PDCSJosMelenhorstSimonLaceyJosephFraietta
JohnsonLabLauraJohnsonAlexCogdillAlinaBoesteanu
CHOPStephanGruppDavidBarrettShannonMaude
NovartisUsmanAzamCelesteRichardsonJensHasskarlReshmaSinghKeithMansfieldJenniferBrogdonGlennDranoffBillSellersJayBradner