caring for seriously ill people
TRANSCRIPT

1
Caring for Seriously Ill People
Kyle P. Edmonds, MD
Assistant Clinical ProfessorDoris A. Howell Palliative Care ServiceDirector, SOMI 421, Subinternship in Palliative Medicine
Medicine 401UCSD School of Medicine

2
Free-range
Millennial
Zone
Caring for Seriously Ill People
#HPM #MedEd with @kpedmonds
From @UCSDPalliative @UCSDHealth

3
4
Specialist Palliative Care
• A team that can help your patients and families manage the pain, symptoms, and stress of serious illness.
• Available at any age and at any stage in a serious illness and can be provided along with curative treatment.
• Expert communication for challenging situations.
• Partnering with you for better outcomes by helping your patients tolerate curative treatment.

5
Generalist / Specialist Palliative Care
Hospice
•Symptom management•Whole person plan of care•No relation to prognosis•Not a philosophy of care
•Funding mechanism•Strictly <6mo prognosis•Home-based•Teaches caregivers

6
Forget the line in the sand
Time
Palliative
Care
Routine Medical Care:
antibiotics, dialysis, chemotherapy, surgery
“Dying”?
“Nothing more to do”?
“Pt / family request”?
“Really sick”?
“Really, really sick”?

7
Time
General OR Specialty Palliative
Care
Routine Medical Care
The Course of Illness

8
General OR Specialty Palliative
Care
Routine Medical Care
Hospice Bereavement
Decision
Maker
Goals of
Care
Nausea
Mgmt
Psychosocial
Needs
Care
coordination
Prognostication
Bowel
Obstruction
Mgmt
Legacy
Work
Family
Meetings
Hospice
Education
POLST
Spiritual
SupportMgmt: Vomiting,
Pain, Ascites,
Delirium,
Anxiety
Care
Transitions
1
2 3
4
5
7
6
Equipment
Teaching
Medications
Home Aides
Volunteers
Prognosis
Symptoms
24/7 Access
Preparing
Children
Support
Groups
Counseling
Resources
Dx
Death
Adapted from Landzaat, 2013.
The Course of Illness

9
Routine Medical Care
Generalist Palliative Care
Specialist Palliative Care
•Fluids•Antibiotics•Etc.
•ACP/GoC•opioids•Ondansetron•Routine MDM •Complex pain
•High dose opioids•Limit setting•Hope & Prognostication•Complex MDM

10
Palliative principles are appropriate for all patients with serious illness
Principle

11
Hospice
• Historical evolution
• US Medicare Hospice Benefit
• ~40% of all deaths
• Median enrollment 18.5 days
• 34.5% of patients die within 7 days
NHPCO. 2014.

12
The Many Meanings of “Hospice”
• A system of reimbursement
• An organization or program
• A place
• An approach to or philosophy of care

13
Choosing Hospice
• Prognosis < 6 months according to two providers
• Elect to use hospice benefit
• Consent to treatment
• Maybe forego some dz-directed therapies
• Can sign on & off at will
Table adapted from NHPCO. 2014.
Location of Death 2013
Place of residence 66.6%
Private residence 41.7%
Nursing home 17.9%
Residential facility 7%
Hospice inpt facility 26.4%
Acute care hospital 7%

14
Structure of Hospice
• Capitated, per diem payment
• Medicare/Medicaid
• Private insurance
• Charity• Out of pocket
• Levels of care
• Routine care
• General inpatient care
• Continuous care
• Respite care

15
What Patients & Families Get
• Interdisciplinary care
• Chaplaincy, nursing, medical social services, counseling, volunteers
• Primary care physician
• Hospice medical director
• Medical equipment, supplies
• Medications and therapies related to the terminal diagnosis
• Bereavement counseling

16
Hospice is an underutilized way to deliver patient-centered & family oriented care
Principle
17
Assessing Symptoms
• 58yo mother of three with metastatic colorectal CA
• Admitted with recurrent SBO (being medically managed), nausea and pain out of control

18
Pt/Fam
Disease Mgmt
Physical
Psych
SocialSpiritual
Practical
End of Life Worries
Whole-person Assessment…
19
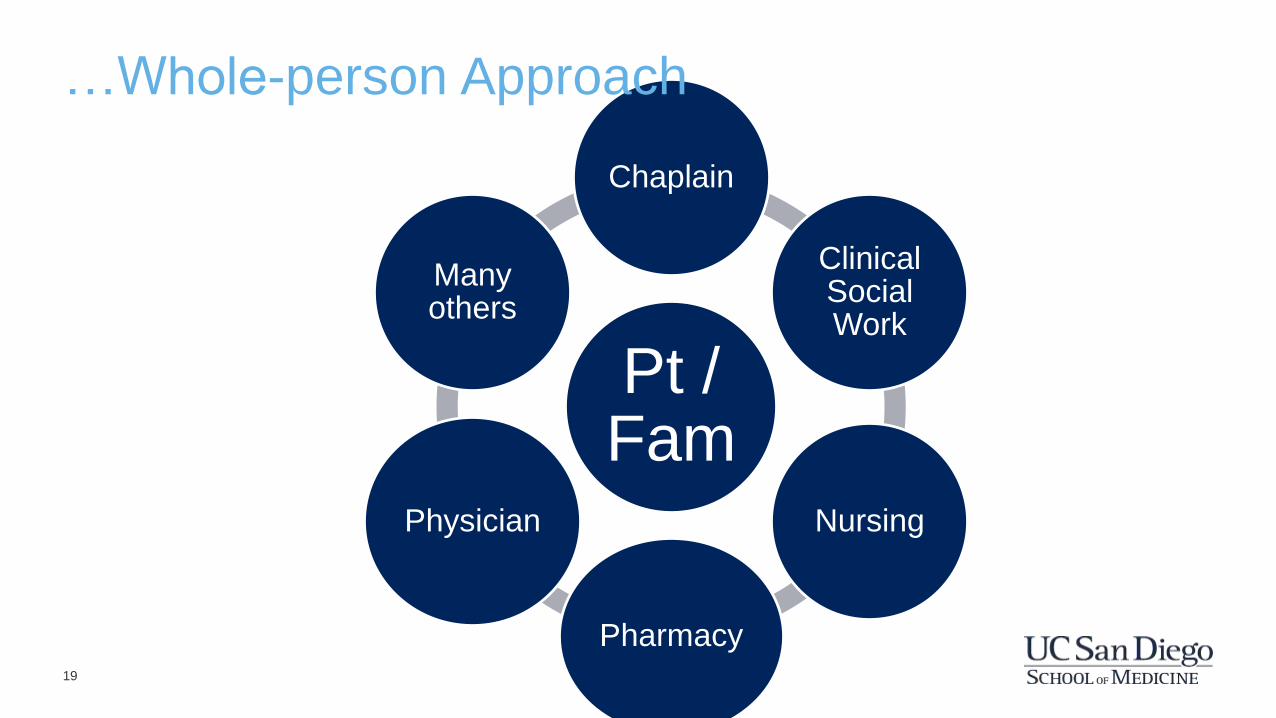
Pt / Fam
Chaplain
Clinical Social Work
Nursing
Pharmacy
Physician
Many others
…Whole-person Approach

20
Symptoms exist in the context of a person’s life
Principle

21
Managing Symptoms
• 58yo mother of three with metastatic colorectal CA
• Admitted with recurrent SBO (being medically managed) and pain out of control
• On PRN hydrocodone/APAP at home• Nausea has resolved since NGT placed

22
• Constant
• Constant + Acute
• Intermittentacute
Symptom Time Course

23
For constant symptoms, treat with constant (scheduled) meds
Principle

24
For acute symptoms, treat with frequent, fast-acting (PRN) meds
Principle

25
Example: Pain
• 58yo mother of three with metastatic colorectal CA
• Admitted with recurrent SBO (being medically managed) and pain out of control
• On PRN hydrocodone/APAP at home• You want to start morphine…

26
Pla
sm
a C
on
cen
trati
on
0 Time
AbsorptionExcretion
First Order KineticsWhen biological effect
follows plasma concentration

27
Pla
sm
a C
on
cen
trati
on
0 Time ( hours )
Time to Maximum Concentration ( t Cmax )
20
10
1
= time it takes to get to
maximum concentration
Cmax
Morphine
PO / PR
Cmax = 1 hour

28
Pla
sma C
on
cen
trati
on
0 Time
IV
PO / PR60min
Time to Maximum Concentration ( t Cmax )10min

29
Pla
sma C
on
cen
trati
on
0 Time
Cmax
Treating Acute Pain
PO / PR
≈ 1 hr
IV
~10 min
Cmax

30
For acute pain, dose every C-max with short-acting meds
Principle

31
Goals of Care
• 58yo mother of three with metastatic colorectal CA
• Admitted with recurrent SBO (being medically managed) and pain out of control
• 3rd admission in 3 months for SBO• “I want to get back to how I was!”

32
Potential Goals of Care
Restorative or Cure
Return to Baseline
Improve Survival
Improve Function
Relieve Symptoms
Allow Natural Death
Adapted from Mulkerin, 2011.

33
Goals…How?
• Perception of patient/family
• Exploration of life before illness
• Relating patient story to medical situation
• Sources of worry for the future
• Outline the plan concretely
• Notify those who need to know
Edmonds, Ajayi, Cain, Yeung, & Thornberry. 2014.

34
Goals of care are who the patient is and what they want
Principle

35
Breaking Bad News
• 58yo mother of three with metastatic colorectal CA
• Admitted with recurrent SBO (being medically managed) and pain out of control
• PMHx of CHF
• Needs help around the house and with dressing
• Albumin 2.4 g/dL
• 3rd admission in 3 months for SBO

36
Formulating Prognosis
• ePrognosis.org
• CAPC.org/Fast-facts
Covinsky et al., 2011.

37
Use SPIKES Protocol to Break Bad News
• Setting
• Perception of patient / family
• Invitation (+ Warning Shot)
• Knowledge
• Empathize & Explore
• Strategy & Summary
Buckman et al., 2000.

38
Use a standardized approach to breaking bad news
Principle

39
• Palliative principles are appropriate for all patients with serious illness
• Hospice is an underutilized way to deliver pt-centered & family oriented care
• Symptoms exist in the context of a person’s life
• For acute symptoms, treat with frequent, fast-acting (PRN) meds
• For constant symptoms, treat with constant (scheduled) meds
• For acute pain, dose every C-max with short-acting meds
• Goals of care are who the patient is and what they want
• Use a standardized approach to breaking bad news
Principles

40
Caring for Seriously Ill People
Kyle P. Edmonds, [email protected]
Want more? Take SOMI 421, Subinternship in Palliative Medicine

41
• Baile WF, Buckman R, Lenzi R, Glober G, Beale EA & AP Kudelka. SPIKES: A six-step protocol for delivering bad news: Application to the patient with cancer. The Oncologist. 5:302-11.
• Edmonds KP, Ajayi TA, Cain J, Yeung HN & K Thornberry (2014). Establishing goals of care at any stage of illness: The PERSON mnemonic. J Pall Med. 17(10).
• Mulkerin, C.M. (2011). Palliative care consultation. In T. Altilio & S. Otis-Green (Eds.), Oxford Textbook of Palliative Social Work (pp. 43-51). New York, Ny: Oxford University Press, Inc.
• NHPCO (2014). NHPCO’s Facts & Figures: Hospice care in America. Acessed via: http://www.nhpco.org/sites/default/files/public/Statistics_Research/2014_Facts_Figures.pdf
References