caries prevention
TRANSCRIPT

Dr.MadhuBillaII MDS
CARIES PREVENTION
Dr.Madhu Billa2nd year PG
SIBAR Institute Of Dental Sciences

CONTENTS• Introduction• Need for prevention• Aims of prevention• Levels of prevention• Methods to control carieso Nutritional o Chemicalo Mechanical
• Pit and fissure sealants• Caries vaccines• Lasers in caries prevention• Conclusion

• Dental caries is an irreversible microbial disease of the calcified tissues of the teeth, characterized by demineralization of the inorganic portion and destruction of the organic substance of the tooth , which often leads to cavitation” (Shafers)
• Prevention refers to act of stopping something from happening or arising (Oxford Dictionary)

• Primary goal of caries prevention program should be to reduce the number of cariogenic bacteria.

AIMS OF PREVENTION
• Limiting pathogen growth and metabolism
• Limitation of caries activity
• Early detection of incipient caries
• Identification of high risk patients
Essentials of Preventive and Community dentistry. Soben Peter. 2nd edition
NEED FOR PREVENTION• caries may cause severe pain• Symptomatic treatment is intensive• Caries Results in dysfunctional speech• Compromises nutrition• The cost of treatment is high
Essentials of Preventive and Community dentistry. Soben Peter. 2nd edition
LEVELS OF PREVENTION• There are three levels of prevention of dental caries.
1. Primary prevention – is defined as “actions taken prior to the onset of the disease, which
removes the possibility that the disease will ever occur.”
2. Secondary prevention - is defined as “actions which halt the progress of a disease at its incipient
stage and prevents complications.”
3. Tertiary prevention- is defined as
“ all measures available to reduce or limit impairments &
disabilities, minimizing suffering caused by existing
departures from good health & to promote the patients
adjustments to the irremediable condition.”
Essentials of Preventive and Community dentistry. Soben Peter. 2nd edition

PREVENTIVE SERVICES
HEALTH PROMOTION SPECIFIC PROMOTION
EARLY DIAGNOSIS AND PROMPT TREATMENT
DISABILITY LIMITATION
REHABILITATION
CARE TO BE TAKEN BY THE PATIENT
Diet planning
Demand for preventive services
Periodic visits to the dental office
Appropriate use of fluorides
Ingestion of fluoridated water
Use of fluoridated dentifrice
Oral hygiene practices
Self examination and referral
Utilization of dental services
Utilization of dental services
Utilization of dental services
SERVICES PROVIDED BY THE DENTAL PROFESSIONAL
Patient education
Plaque control program
Diet counseling
Recall and reinforcement
Caries activity tests
Topical application of fluorides
Topical fluoride supplements/rinses
Pit and fissure sealants
Complete examination
Prompt treatment of incipient lesions
Preventive resin restorations
Simple restorative procedures
Pulp capping
Complete restorative dentistry
Pulpotomy
RCT
Extraction
Fixed and removal prothodontics
Minor tooth movements
Implants
LEVELS OF PREVENTION PRIMARY PREVENTION
SECONDARY PREVENTION TERTIARY PREVENTION
LEVELS OF PREVENTION
Methods Of Caries Prevention
1.Nutritional measures.
2.Chemical measures.
3.Mechanical measures.

NUTRITIONAL MEASURES
• Nutrition: The sum processes concerned in the growth, maintenance and repair of living body as a whole or its constituent parts. (Oxford Dental Dictionary)
• Science of food and its relationships to health. It is concerned primarily with the part played by the nutrients in body growth, development and maintenance. (WHO 1971)
• "Diet refers to the customary allowance of food and drink taken by any person from day to day.
• Thus, the diet may exert an effect on caries locally in the mouth by reacting with the enamel surface and by serving as a substrate for cariogenic microorganisms."
(Newbrun, E. Cariology. Third ed. 1989).
Effect Of Nutrition On Dental Caries• Systemic effect:
- Depends on their content of nutrients and includes their influence on general health, growth and development ability of the tissues to repair and resistance to diseases.
• Local effect:
- Consists of what food can do to the tissues or their environment because of their presence in such an environment .
- It result from the interaction between food residues and oral bacteria leading to plaque formation.
- Their metabolites in turn effect the soft and hard oral tissues
DIETARY ANALYSIS
Objectives of a dietary analysis includes-
oTo obtain an overall picture of the types of food in the patient diet, food preference and quantity of food eaten.
oCorrection of diet imbalances that could effect the patient's general health & also reflected in his oral health.
oModification of dietary habits, particularly the ingestion of sucrose containing foods in forms, amounts and circumstances that promote caries formation.

• To record for study and future comparison of the types and frequency of use of potential cariogenic food.
• To provide a basis for making individual recommendation for changes in diet, important to the health of the oral mucosa and the prevention of dental caries.

Diet analysis program consists of:
• The interview, where diet diary forms are introduced with a brief discussion of the purpose of diet counseling.
• A 24 hour diet record is prepared to get an idea of food being consumed.
• A six days diet diary is advised to be prepared by the patient.

Diet diary of the patient for a week

• Sugar factors are isolated.
• Patient is educated about the role of sugar in the decay process & the consumption of acceptable substitutes .
• Practical limitations to immediate success are recognized.
• Provision for a continuous positive reinforcement are planned.
Continuous production of acid by plaque bacteria and
Insufficient time for the saliva to neutralize the acid.
Persistent acidic environment favoring the
development of dental caries.
Consequences of frequent snacking

First appointment: In a 15 to 20 minutes appointment the diet diary
forms are introduced with a brief discussion of the purpose of diet
counseling. Patient is explained –
1.That we are looking for possible dietary causes of the caries to
reduce the risk of future caries by dietary means.
2.What beneficial outcome could be available for him in better oral
health and possibly improved health in general.
DIETARY COUNSELLING

PATIENT EDUCATION:• The cariogenic potential of a patient's diet is evaluated by
determining the total number of exposures to sucrose-containing foods during 6 consecutive days.
• Exposure is defined as eating the food at one time and is not related to the amount of food sucrose ingested.
• Total time of exposure to acid = (total exposure X 20minutes)
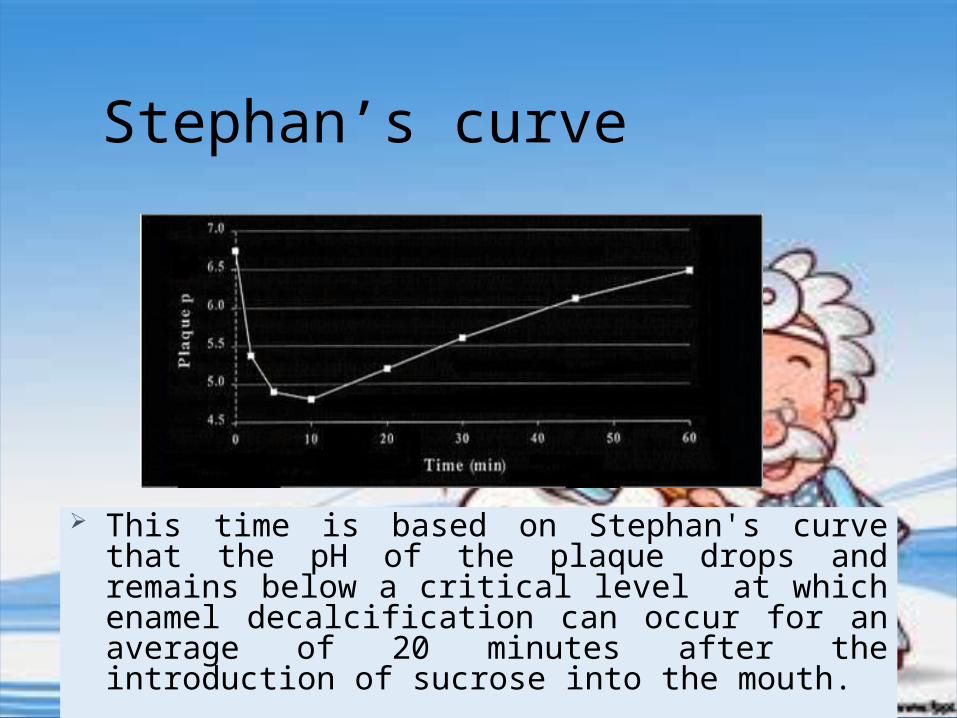
Stephan’s curve
This time is based on Stephan's curve that the pH of the plaque drops and remains below a critical level at which enamel decalcification can occur for an average of 20 minutes after the introduction of sucrose into the mouth.

Dietary Changes
o From the summary of exposures to fermentable carbohydrates the dietary changes that are better for dental health are determined.
o Substitutes should be reasonable, which are acceptable to the dentists in terms of lesser cariogenicitv as well as to the patient as far as taste and preferences are concerned.
o Substitution can be : - Use sugared food during meal time . - Food consumption followed by appropriate oral hygiene
measures.

• To reduce the frequency of snacks, sufficient amount of food
should be taken during breakfast, lunch and dinner at regular
intervals.
• If hungry in between meals, healthy snacking is advised.
• Sweets or beverages - eat or drink them right after meal.
• To quench thirst - plain water is preferred to sweet beverages.

RECALL VISITS• During the next months at regular intervals, the dentist
should evaluate the patient's progress and provide psychological reinforcement.
• Evaluations are made by means of: -The patient' s response to questionnaires. -New diet diaries.
Reinforcement is provided by-• praising the patient's efforts• improvements made in the diet as well as in the test results
and the absence of new caries lesions.
Emphasis should be placed on-• making the patient fully aware of the benefits derived from
the program • benefits are the product of the patient's own efforts.

SUGAR SUBSTITUTES
• Are less cariogenic or non-cariogenic. • Sweeteners stimulate the flow of saliva • Have a smaller role or no effect on bacterial glycolysis. • Plaque ph raises with sweeteners, it mobilizes the
calcium and phosphates for remineralization of the tooth surface
• In children consuming sucrose containing snacks more frequently, it is ideal to replace the sucrose by sugar substitutes.

Sweeteners are of two types:
(I) Non-caloric Sweeteners
(Ii) Caloric Sweeteners.

NON CALORIC SWEETNERS
• Provide no energy but provide intense sweet taste.
• Are not metabolized to acids.
• Disadv:
Instability and lack of volume.
• Ex - saccharin and aspartate.

CALORIC SWEETNERS
• Include 1. Sugars—e.g. fructose, glucose, lactose. 2. Sugar alcohols —e.g. lycasin, sorbitol, Xylitol
• Used in- sugar free chewing gums, medicines, food products, and toothpaste.
• xylitol is the most popular and widely used at present.

Sugar Alcohols
Xylitol. ois non-acidogenic. ois a sugar alcohol having an acceptable sweetening taste. o approved as a sweetener in more than 45 countries.oused mainly in chewing gums, ice creams, jams, cookies and
soft drinks.
Xylitol:C5

• Allows remineralization of initial enamel lesions. (Turku study).
• Incorporated in chewing-gum, its action is increased due to the stimulation of salivary secretion.
• Synergic action with fluoride. o Disadvantages- - Toxicity studies have shown it
increases urinary bladder calculi formation, epithelial hyperplasia & neoplasia of the bladder.
- laxative effect at high conc.

2. Sorbitol
• Is a low cariogenic sugar substitute used mainly as sweetener in chewing gums, soft drinks, cookies and jams.
• Not as sweet as sucrose.• Sweets made of it cannot be stored for long.

3. Coupling sugar. • Are very effective sugar substitutes and anticariogenic &
exactly resembles sucrose• Widely used in a variety of snacks. • Disadv- is too expensive.
4. Saccharin.• Is non-caloric, and less cariogenic.• Leaves some bitter aftertaste. • Is highly intense sweetener
CHEMICAL METHODS
Chemical methods1) Substances which alter the surface of tooth structure a. Fluoride. b. Iodides. c. Bis-biguanides. d. Silver nitrate. e. Zinc chloride and potassium ferrocyanide.
2) Substances which interfere with carbohydrate degradation through enzymatic reaction/alterations
a. Vitamin K. b. Sarcoside.

3)Substance which interfere with bacterial growth and metabolism
a.Urea and ammonium compounds b. Chlorophyll c.Nitrofurans

Substances which alter the surface of tooth structure
Iodine:• Miller (1980) reported the intraoral use of iodine
solution as an antibacterial mouth rinse.• Bactericidal effectiveness is not time dependent i.e. it kills
microorganisms immediately once contact with the organisms is established.
• Disadv:- -Metallic taste. -Tendency to stain silicate or composite restoration. -Allergic potential.

• Commercially available forms -a) Chlorhexidine
b) Alexidine
• They are effective antiplaque agents and thus potential anticaries agents.
• Topical antiseptics characterized by molecular structure having both hydrophobic and hydrophilic constituents and possess a net positive charge at physiologic pH.
Bis-biguanides:
Mode of action:• Ionic adsorption of negatively charged bacterial surface• Interaction with and damage to permeability barrier of
cytoplasmic membrane• Penetration into cells and subsequent penetration of
cytoplasmic constituents and culmination in membrane leakage and cell death.
Disadv• Bitter taste• Brownish discoloration of soft & hard tissue.• Painful desquamation of mucosa.
Silver Nitrate:
• It was used clinically for many years to prevent or arrest dental caries.
• Earlier workers believed that silver 'plugged' the enamel, either the organic invasion pathways such as the enamel lamellae or the inorganic pathways, combining with the soluble inorganic portion of enamel to form less soluble combination.
• But studies by Klein & Knutson indicated it had no significant difference in the appearance of new lesion.

• Gottleib proposed they act by effectively impregnating the enamel and seal off caries invasion pathways.
• But clinical results did not substantiate the theories proposed.
Zinc Chloride and Potassium Ferrocyanide

Substances Which Interfere With Carbohydrate Degradation Through Enzymatic Reaction/Alterations
Vitamin K- • 2-methyl-1,4-naphthoquinone was suggested by Fosdick as
a anticaries agent.• Invitro studies have found it prevents acid formation in
incubated mixtures of glucose & saliva.

Substance which interfere with bacterial growth and metabolism
1.Urea & ammonia compounds-
-Decrease oral bacteria count & increase the salivary pH to over 8 for more than an hour after an quinine-ammonia mouthwash. (Wach et al)
-Urea upon degradation by urease yields ammonia which neutralizes acids & interferes with bacterial growth. (Stephan et al)
- Though some studies have shown some reduction in dental caries but magnitude of reduction has not been so great that their widespread use can be advocated.
Chlorophyll:
• Bacteriostatic against lactobacilli, streptococci & micrococci. (Griffith et al).
• Sodium copper chlorophyllin prevents or reduces pH fall of in carbohydrate- saliva mixtures in vivo. (Shaffer et al).
• Short term clinical studies have suggested their use in reducing mouth odors & allaying gingivitis but anticariogenic properties are still inconclusive.

Nitrofurans
o Are derivatives of furfural. o exert a bacteriostatic and bactericidal action in many Gram
positive and Gram negative organisms.o Even in low concentrations, acid production in saliva from
caries active persons was prevented. (Driezen et al 1951) o Data from studies, indicate that they significantly reduces
dental caries experience and that this substance may have potential use as an anticariogenic agent.

ANTIBIOTICS
1. PENICILLIN :
• Tested as an anticariogenic compound, becauseof its antibiotic property.
• Reduction from an average of 72000 colony count to an average of 300 was found after use of the dentifrice containing 1000 units of Penicillin per gram, for 5 weeks.
• However the wisdom of using this material for such a purpose has been further questioned because of the possibility of development of penicillin resistant pathogenic microorganisms and sensitization, as well as development of allergic reactions.

PROBIOTICS
• Probiotics (derived from the Greek pro bios, for life) are defined by the World Health Organization as live microorganisms which when administered in adequate amounts confer a health benefit on the host
• Probiotics are nonmodified human isolates from healthy individuals and most of them belong to the lactobacilli and bifidobacteria groups which are naturally present in the intestinal flora
Treatment Protocols: NonfluorideManagement ofthe Caries Disease Process and Available Diagnostics (DCNA2009)
MECHANISM OF ACTION
1. Probiotic bacteria compete for nutrients and binding sites in the biofilm.2. When attached, probiotic bacteria can produce bacteriocins (eg, hydrogen peroxide and reuterin) that hamper and inhibit growth of a variety of bacteria.3. Probiotic bacteria stimulate the specific and nonspecific immune response through activation of T cells and production of cytokines that mediates the inflammatoryprocess.
Treatment Protocols: NonfluorideManagement ofthe Caries Disease Process and Available Diagnostics (DCNA2009)

2. ERYTHOMYCIN
• 35% decrease in plaque formation after a seven day test period of rinsing, then swallowing the agent 4 times a day (LOBENE et al). Was found with erythromycin
• Disadvantage : causes diarrhea as a side effect.
3. KANAMYCIN
-reduces plaque weight & improves oral health if applied topically.-Reduces S.mutans & S.sanguis population

4. TETRACYCLINE
• decrease plaque scores when used as an 0.5 per cent mouthwash three times a day for five days in place of mechanical oral hygiene (Loe et al).
5 Vancomycin
• Temporarily suppress streptococcus mutans when applied to the teeth of children as a 15 percent gel on five successive days.
• Diminution in s. mutans was found following testing with 1 percent vancomycin paste.
• Statistically significant reduction in dental caries experience
in fissures but not on smooth surfaces in the experimental groups (depaola et al).

FLUORIDES
• Ranks 13th among the elements in the order of their abundance.
• Most electronegative element
Highly reactive

FORMS OF FLUORIDE
• Inorganic Fluoride a.Ionic Fluoride b.Nonionic Fluoride
• Organic Fluoride

ANTICARIES MECHANISM OF FLUORIDES
Anticaries mechanism can be broadly grouped into
1.Increased enamel resistance
2.Increased rate of maturation
3.Remineralization of incipient lesion
4.Antimicrobial activity
FLUORIDE DELIVERY METHODS
MAIN FLUORIDE DELIVERY SYSTEMS
• SYSTEMIC
• TOPICAL

SYSTEMIC FLUORIDES
• WATER FLUORIDATION
• SALT FLUORIDATION
• MILK FLUORIDATIONS
• FLUORIDE SUPPLEMENTS
TOPICAL FLUORIDES
Agents • SODIUM
FLUORIDE
• STANNOUS FLUORIDE
• ACIDULATED PHOSPHATE FLUORIDE
• FLUORIDE
VARNISH
• FLUORIDE DENTIFRICES
• FLUORIDE MOUTH RINSE
Forms


WATER FLUORIDATION
Water fluoridation is defined as controlled adjustment of the concentration of fluoride in a communal water supply so as to achieve maximum caries reduction and a clinically insignificant level of fluorosis (SOBEN PETER)
Water fluoridation is one of the most effective, practical, and economical public health measure for prevention of dental caries.
• Reduction in prevalence of dental caries in primary teeth range from 40%-50% permanent teeth was between 50%-60%

FLUORIDE COMPOUNDS USED IN WATER FLUORIDATION
• Fluorspar• Sodium fluoride• Silicofluorides• Sodium silicofluoride• Hydroflurosilicic acid• Ammonium silicofluoride
BENEFITS OF WATER FLUORIDATION
• Reduction in caries rate by 50%-70%
• 75% reduction in first permanent molar loss
• There is a reduction in progression and development of dental caries in fluoridated area
• Reduction in the number of surface attacked by dental caries
• Prevents malocclusion due to prevention of early loss of contact points due to proximal caries

LIMITATIONS
• Can be implemented only in areas which have central pipe water system
• It interferes with personal choice
• Initial cost for installing fluoridation plant is high
DEFLUORIDATION
• Defluoridation is downward adjustment of fluoride ion concentration in a public drinking water supply so that the level of fluoride is maintained at the normal physiological limit of 1 ppm to prevent dental caries with minimum possibility of causing dental flourosis.
• Methods of defluoridation a. based on ion exchange or adsorption b. based on addition of chemicals to water

• Based on ion exchange materials used include synthetic tricalcium phosphate,
hydroxyapatite, magnesia, activated alumina, activated carbon.
• Based on addition of chemicals materials used includes lime either alone or with
magnesium salts or aluminium salts.

NALGONDA TECHNIQUE
• Was developed by NEERI• It is a simple and economical process• Highly effective for removal of fluoride from 1.5-2mg F- /l to
desired level• Method could be used for defluoridation of domestic and
community water supply• Uses readily available chemicals – sodium aluminate or lime,
bleaching powder and filter alum
SALT FLUORIDATION
• As a dietary vehicle for ensuring adequate ingestion of fluoride domestic salt comes second
• Was introduced by Wespi in Switzerland in 1955
• Most popular in Spain, Hungary and Columbia
• Recommended concentration is 250µg of fluoride/g salt

Advantages
• Economical• Practical• Caries reduction about 40 %
Disadvantages
• Consumption of salt till 4-5 yrs after birth is negligible, hence no benefit for younger children.
• Not useful in case of medically compromised patients (hypertension and renal failure)
MILK FLUORIDATION
• It is the addition of a measured quantity of fluoride to bottled milk packet
• Mainly recommended for growing children
• Substantial caries reduction noticed when milk consumption begins before the eruption of permanent teeth
• Rationale for adding fluoride to milk is that this procedure targets fluoride directly to children
Concentration• 2.2mg of NaF added to 1/4litre of milk
• Later milk bottles of 250 ml, containing 0.625mg of fluoride was introduced
Caries reduction is about 60%
Limitations
• Since children from lower socioeconomic groups tend to drink less amount of milk or no milk at all, hence they would be benefited least.
• Any benefits cease, as an individual grows older and if he or she drinks less milk.
• Expensive.• Parent co-operation is important.

School water fluoridation
o Recommended -for communities with no central water supply or fluoride deficient water supply.
o Reduces dental caries by 40%.o Primary effects are systemic but also has a topical effects. o Caries reduction –57% in teeth erupted after exposure to school water
fluoridation. 31% if the teeth have already erupted.oFor maximum benefit, children should attend the school
regularly and stay their till they complete the higher secondary school.
• Recommended conc.- 4.5 ppm.

Reasons for recommending high conc. :
1. Students receive only small part of the daily intake of water when they are in school.
2. Students may not attend the school throughout the year.
3. Frequency of drinking water in school by children is variable.
4. Children attend the school only for a few hours.

Advantages1) Target population—school children.2) Caries experience is high during the developmental
period (among children).3) Quite economical Disadvantages4) Need for cooperation from school authorities.5) All children may not attend the school all days.
FLUORIDE SUPPLEMENTS
• When community water fluoridation is not feasible or where there is political opposition preventing its implementation, fluoride supplements offer an alternate source of systemic fluoride
• Can be given in the form of fluoride tablets, fluoride drops and lozenges
• The cariostatic effect ranges from 30 to 70% depending-on
dosage and degree of compliance.
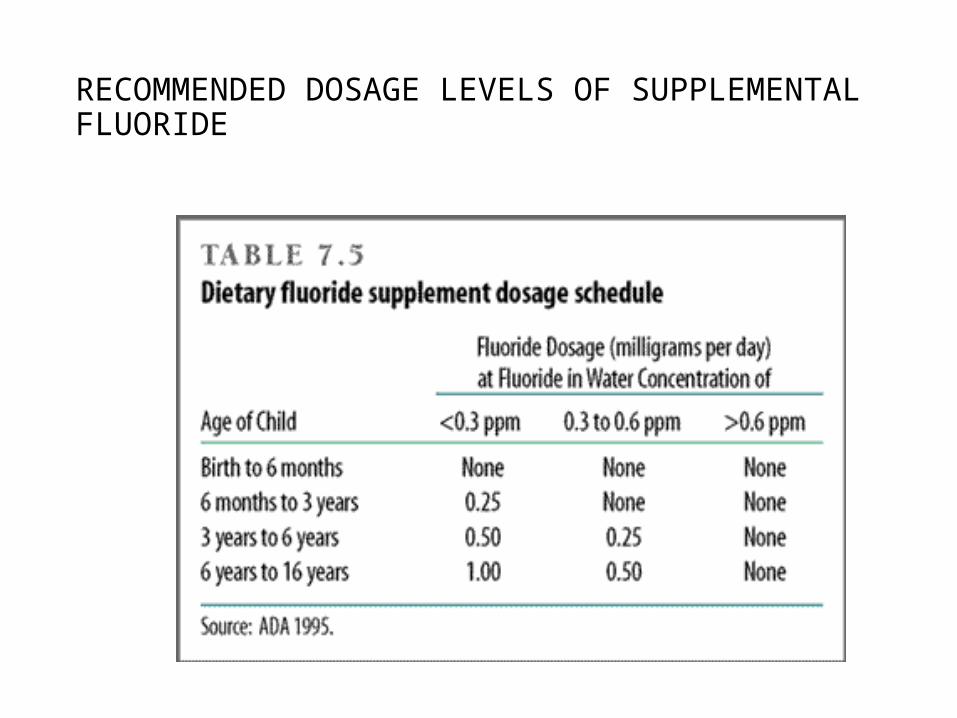
RECOMMENDED DOSAGE LEVELS OF SUPPLEMENTAL FLUORIDE

TOPICAL FLUORIDES
Topical fluoride therapy refers to the use of systems containing relatively large conc. of fluoride applied locally or topically to the erupted tooth surfaces to prevent formation of dental caries
The various topical fluorides used are
• Sodium fluoride• Stannous fluoride• Acidulated phosphate fluoride• Fluoride varnish

SODIUM FLUORIDE
• developed by Knutson so technique of use also called Knutson’s technique
• Conc: 2% of NaF• pH :7• Prepared by dissolving 2gm of NaF in 100 ml of
distilled water• A full series of 4 treatments recommended at the ages
of 3, 7, 10, 13years, coinciding with the eruption of different groups of primary and permanent teeth
Method of application
• Oral prophylaxis is done in first visit.• Each quadrant is isolated• 2% NaF is then applied to the tooth surface with cotton
applicators and kept wet for about 4 minutes. The procedure is repeated for the remaining quadrants.
• After the treatment, the patient is instructed to avoid eating, drinking or rinsing for 30 minutes. This is to prolong the availability of "F" ion to react with tooth surface.
• 2nd, 3rd and 4th applications are given at weekly intervals

Mechanism of action
Ca10(PO4)6(OH)+F 10 CaF2+6PO4 +20H-
As a result of this reaction, the principal compound formed is CaF2 and this is due to high concentration of "F" (9000 ppm) in 2% NaF.
This results in the phenomenon called "choking off phenomenon“ — once a thick layer of CaF2 forms, it interferes with further uptake of "F-" ions'.
Hence, NaF is applied once left to dry for 4 minutes. Later CaF2 dissolves slowly in oral fluids and CaF2 breaks
down into Ca+ and ion. This fluoride is in free ionic form. CaF => Ca++ + F-
This " F- " is highly reactive and reacts with HA to form fluoridated hydroxyapatite.
Disadvantages
• The patient must make 4 visits to the dentist within a relatively short time (weekly intervals for four weeks).
• The expected caries reduction is not satisfactory (20-25%)

STANNOUS FLUORIDE
• Developed by Muhler• Annual or biannual application• pH is 2.4-2.8.• Available in gel and solution forms • It has to be freshly prepared before use each time as has a
very short shelf-life • It is chemically highly unstable. • Prepared by dissolving 0.8 gm or 1 gm of SnF2 powder is in
10 ml of distilled water to get 8% or 10%

Mechanism of Action
Ca10(PO4)6(OH)2 + 19SnF2 10CaF2 + 6Sn3F3P04 + SnO.H2O
• Compared with that of NaF, the reaction of SnF2 with enamel is unique in that both the cations (stannous) and anions (fluoride) react chemically with enamel components.• Formations of stannous fluorophosphates, prevent at least
temporarily the phosphate loss which is typical of NaF applications.• The CaF2 so formed, further reacts with Hydroxyapatite forms fluoridated Hydroxy Apatite (FHA).• The tin hydroxy phosphate gets dissolved in oral fluids and is responsible for metallic taste.• The Sn3F3P04 makes the tooth structure more stable and less
susceptible to acid dissolution
Advantages
•Applied every 6 or 12 months.
•Very potent and effective topical fluoride preparation
•Very useful for spot application among patients with nursing bottle caries and rampant caries.
•Stable stannous fluoride gel is available and is the recommended and ideal preparation in case radiation caries (cervical) among patients undergoing radiation therapy for head and neck cancers.
•Expected caries reduction is 25-35%.

Disadvantages
•Chemically more unstable (cannot be storedhence, requires instant preparation just prior to the application (takes more chair side time).•Pigmentation of teeth after application of SnF2 and brown discoloration can occur on demineralised enamel and anterior restorations.•Metallic taste (astringent taste)—children do not like the taste.•When brought in contact with gingiva, during application it causes blanching and burning sensation due to astringent property.•It is not economical.

ACIDULATED PHOSPHATE FLUORIDE (APF)
• APF was introduced by Brudevold and co-workers.
• Developed in an effort to achieve greater amounts of fluoridated hydroxyapatite and lesser amounts of calcium fluoride formation.
• Composition: 1.23% of NaF buffered to a pH of 3-4 in phosphoric acid.
• Prepared by dissolving 2gm of NaF in 100ml of 0.1 M phosphoric acid. To this 50% HF is added to adjust pH at 3 and F- conc to 1.23%
• Semiannual or annual application.

Mechanism of action
Ca10(P04)6 + NaF CaHP04.2H20
CaHP04.2H20 + F- Ca5 (P04)3F + HP04
When APF is applied on the teeth, initially leads to dehydration and shrinkage in the volume of HA crystals and formation of dicalcium phosphate di hydrate (DCPD). This DCPD is highly reactive with "F" and leads to the formation of Fluorapatite "FA"

Advantages
• Semiannual or annual application.• Chemically stable and can be stored for ready use.• Does not produce staining of enamel.• Available in different flavours.• Expected caries reduction is about 30 to 40% (better than
NaF and SnF2).• Can be recommended for home use by self-application.


FLUORIDE VARNISH
• Fluoride has been incorporated in varnishes since they have the ability to adhere to enamel for long period, and it is hypothesized that it will slowly release fluoride to the teeth.
• The retentive and possible slow release of fluoride from these products
-increase the exposure time of the fluoride by several days, without increasing chairside time,
- allow fluoride to be more permanently bound to the teeth.

INDICATIONS:
- Exposed roots and root caries
- Erupting teeth
- White spot lesions
- Margins of restorations
- Carious anterior tooth in young children

Types:
• Duraphat: 22.6 mg F/ml. 5% NaF in Colophonium base—available in 10 mltube.
1% difluorisilane in polyurethane base (1 mg/ml)• Fluorprotector pH lower than Duraphat and is available in box with 20 vials—each
vial contains 0.4 ml of solution.• Duraflour : 22.6 mg/ml. 5% NaF in.alcoholic suspension of natural resins. Addition of
sweetening agent—xylitol.• Cavity shield: 5% NaF in resinous base.
Technique
Oral prophylaxis.
Isolation –•of quadrant using cotton rolls. •set in the presence of moisture, so meticulous drying of teeth is not critical.
Application-• using disposable brush or cotton applicator. •The entire surface of the teeth must be treated.• Avoid getting varnish on the soft tissue. Sets in few seconds leaving a fluoride rich layer adjacent to the tooth surface.

• The entire process takes 3-4 minutes.
• Duraphat and Duraflour set to a yellowish-brown layer causing a temporary change in tooth colour.
• Parents and patients should be instructed that this discolouration is temporary and will vanish once toothbrushing is commenced.
• Patient should avoid brushing for the rest of the day

FLUORIDE DENTIFRICES
• Considered as a major reason for decline in dental caries in many parts of the world
• Most widely used method of topical application of fluoride• Most widely used fluoride in dentifrices is sodium
monofluorophosphate• Mechanism of action: Dentifrices serve as a constant source
of supply of fluoride in the oral environment hence accelerate the remineralisation process.

FLUORIDE MOUTHRINSES
• Found to be an effective tool in prevention of dental caries in areas where water fluoridation is not possible/not been implemented
• DosageOnce daily-0.02%of NaF 0.05% of NaFOnce weekly-0.2%NaF 0.5% of NaF

Indications• Caries prone children over the age of 6 yrs• Patients with orthodontic appliance• Patients with erosions and root caries• Patients with dentine hypersensitivity
Contraindications• Children under 6 yrs of age who are not capable of rinsing
adequately (when reflex control of swallowing absent)

Fluorosis
• Fluorosis is a disease caused by deposition of fluorides in the hard and soft tissues of the body.
• It is not merely caused by excess intake of fluoride but there are many other attributes and variables which determine the onset of fluorosis in human population.
• Characterized by discoloration of teeth and skeletal crippling disorders.

DENTAL FLUOROSIS
• occurs by excessive intake of fluoride during tooth development.• Once the crowns of the teeth are formed no further fluorosis can
be induced by additional intake of fluoride• Occurs symmetrically within the dental arches.• Clinical features are characterized by lusterless opaque white
patches in enamel which may become mottled, striated and/or pitted

Fluorosis in India
• Rajasthan and Gujarat in North India and Andhra in South India are worst affected.
• Throughout India fluorosis is essentially Hydrofluorosis except in parts of Gujarat and U.P. where industrial fluorosis is also seen.
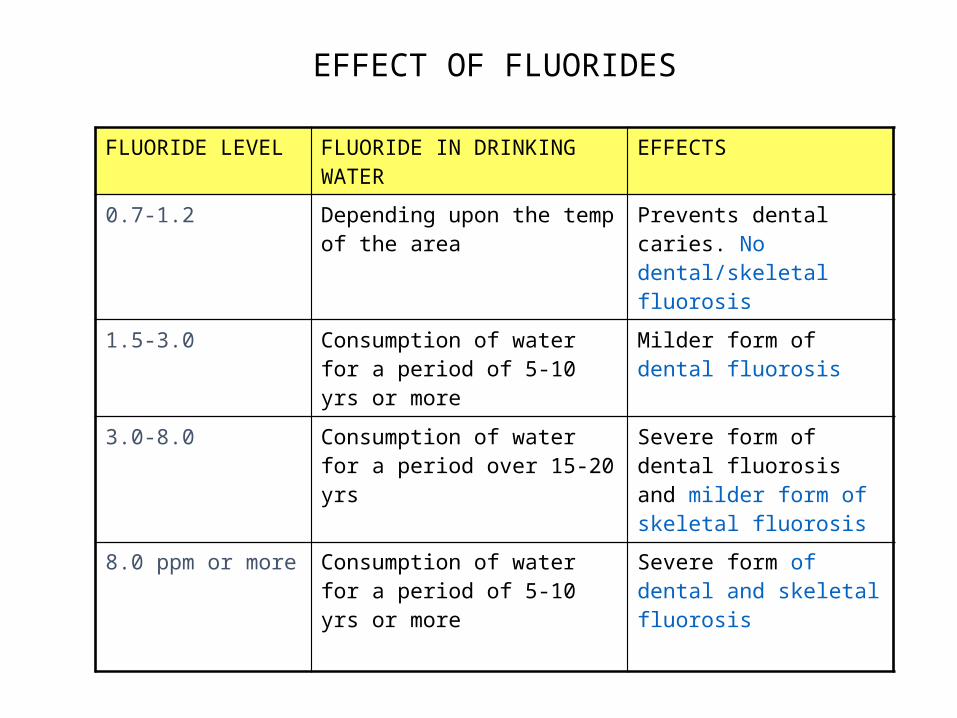
FLUORIDE LEVEL FLUORIDE IN DRINKING WATER
EFFECTS
0.7-1.2 Depending upon the temp of the area
Prevents dental caries. No dental/skeletal fluorosis
1.5-3.0 Consumption of water for a period of 5-10 yrs or more
Milder form of dental fluorosis
3.0-8.0 Consumption of water for a period over 15-20 yrs
Severe form of dental fluorosis and milder form of skeletal fluorosis
8.0 ppm or more Consumption of water for a period of 5-10 yrs or more
Severe form of dental and skeletal fluorosis
EFFECT OF FLUORIDES

DEANS FLOUROSIS INDEX(1938)
DEANS SCORE
CRITERIA
0 Normal enamel
0.5 Questionable mottling :normal translucency is varied by a few white flecks
1 Very mild mottling :small opaque paper white areas are scattered over the teeth ,involving less that 25% of surface
2 Mild mottling: white opaque areas are extensive ,but do not extend more than 50% of surface
3 Moderate mottling: all enamel surfaces are effected and those subjected to attrition show wear. Brown stains are a frequent disfiguring feature
4 Severe mottling: all enamel are affected and hypoplasia is so marked that tooth form may be altered. Major diagnostic feature is discrete or confluent pitting

Mild Dental fluorosis Moderate Dental fluorosis
Severe Dental fluorosis

FLUORIDE TOXICITY
• Fluoride is often called as a double edged sword -inadequate intake is associated with dental caries; excessive intake leads to dental ,skeletal fluorosis which has no cure.
• Toxic effects of fluoride can be classified as a. Acute
b. Chronic

ACUTE TOXICITY
• Results from rapid excessive ingestion of fluoride at one time
• Speed and severity of the response depends on the amount of fluoride ingested and the weight and age of the individual
• Could be fatal if not treated within 2-4 hrs

• Certainly Lethal Dose (CLD) is 32 to 64mg of fluoride per kg of body weight. i.e approx 2.5-5gm in case of children and 5-10gm one single dose in case of adults.
• Safely tolerated dose 8-16 mg of fluoride per kg of body weight.
• Acute poisoning causes death by blocking normal cellular metabolism.
• Death usually occurs due to either cardiac failure or respiratory paralysis.

Emergency treatment for fluoride over dose
Fluoride ion per mg/kg
Treatment
Less than 5.0 mg/kg
Give calcium orally(milk) to relieve GI symptoms. Observe for a few hours.Induced vomiting not necessary.
More than 5.0 mg/kg
Empty stomach by induced vomiting with emetic. For patients with depressed gag reflex caused by age(<6 months old), downs syndrome, or severe mental retardation, induced vomiting is contraindicated and endotracheal intubations should be performed before gastric lavage.Give orally soluble calcium in any form (milk ,5%calcium gluconate, or calcium lactate solution).Admit to hospital and observe for a few hours.
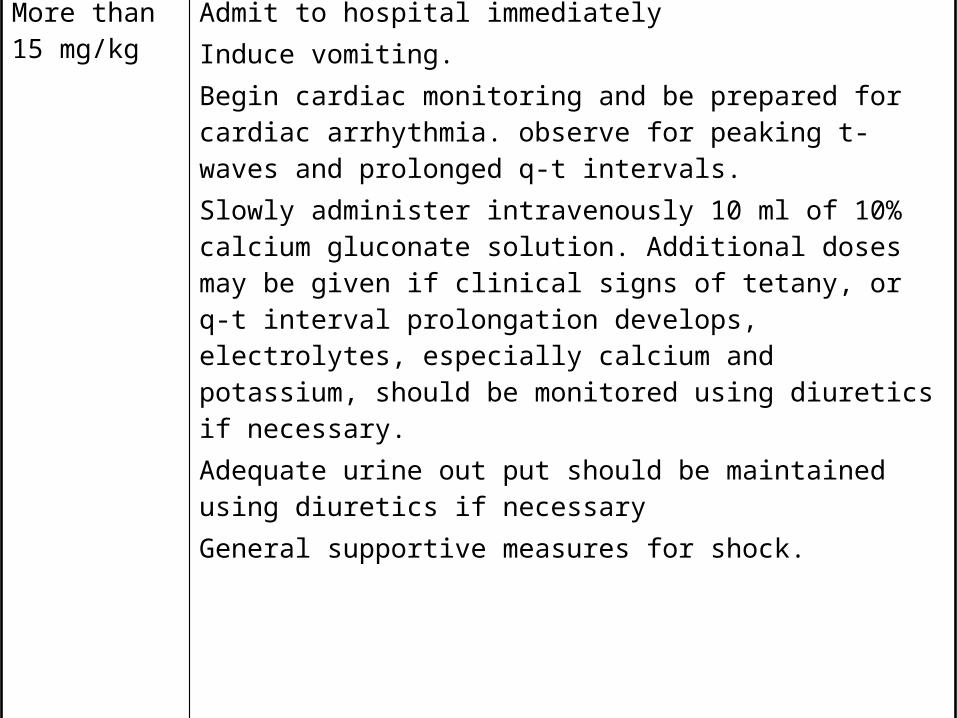
More than 15 mg/kg
Admit to hospital immediately Induce vomiting.Begin cardiac monitoring and be prepared for cardiac arrhythmia. observe for peaking t-waves and prolonged q-t intervals.Slowly administer intravenously 10 ml of 10% calcium gluconate solution. Additional doses may be given if clinical signs of tetany, or q-t interval prolongation develops, electrolytes, especially calcium and potassium, should be monitored using diuretics if necessary.Adequate urine out put should be maintained using diuretics if necessary General supportive measures for shock.
CHRONIC TOXICITY
• Results from long term ingestion of small amounts of fluoride.
• Effect of chronic fluoride toxicity- severe dental fluorosis and skeletal fluorosis.
• Fluorosis is an endemic disease in geographic areas where content of fluoride ion exceeds 2ppm.
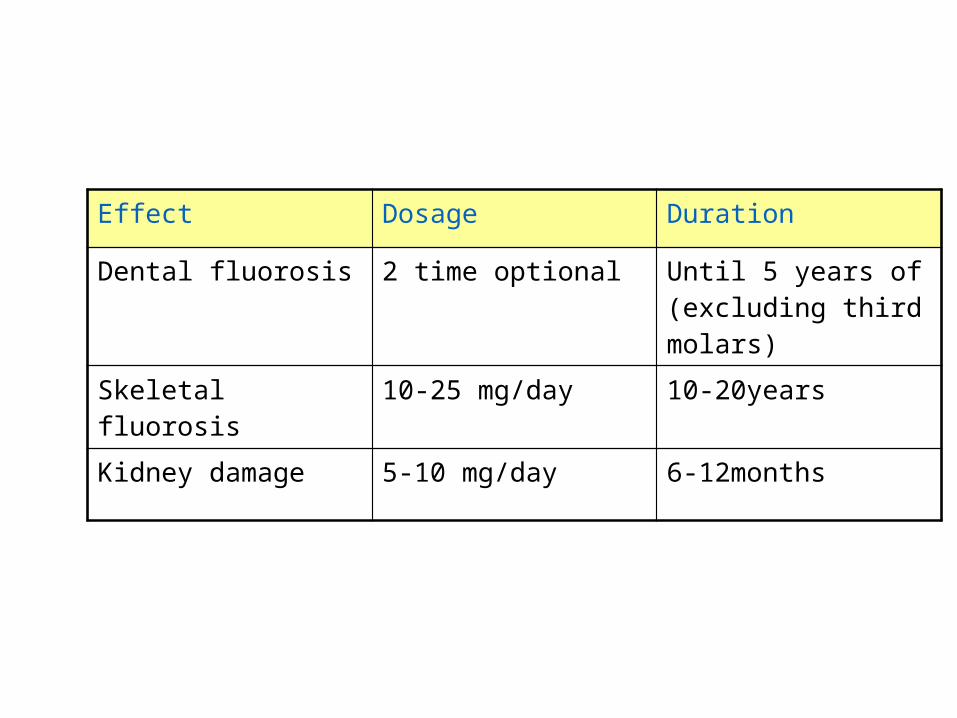
Effect Dosage Duration
Dental fluorosis 2 time optional Until 5 years of (excluding third molars)
Skeletal fluorosis 10-25 mg/day 10-20years
Kidney damage 5-10 mg/day 6-12months
TOOTHBRUSHES• The bristle toothbrush appeared about the year 1600 in China
• First patented in America in 1857
• Toothbrushes vary in size and design as well as in length, hardness, and arrangement of the bristles.
MECHANICAL METHODS

TOOTHBRUSH DIMENSIONS(ADA specifications)
Total length: 6.0-7.5 inchesLength of brushing plane: 1-1.25 inchesWidth of brushing plane: 5/16-3/8 inchFilament height: 7/16 inch
Filament diameter Soft: .007 inchMedium: .012 inchHard: .014 inch

POWER TOOTHBRUSH
•Better effectiveness in removing plaque and reducing gingivitis than manual brushes is still not proven.
• Enhance patient motivation.
• Use less brushing force.
•Head: Detachable and replaceable.
•Size: ¼ to 1/2 inch wide by ¾ inch long.
MECHANISM OF ACTION
• Mechanical contact between bristle and tooth.• Low frequency acoustic energy generating fluid movement, cleans slightly away from the bristle tips.• Vibrations interfere with bacterial adherence to oral surfaces.• Hydrodynamic shear forces disrupt plaque a short distance from the bristle tips.

Precautions• Avoid excessive force on restorations.• Avoid pressure with abrasive dentifrice on exposed cementum or dentin.
Recommendations•Encourage ones who prefer to use powered toothbrushes to do so.•Poor brushers, children .

TOOTHBRUSHING METHODS
Categorized primarily a/c the pattern of motion-
• Roll -The Roll Method or Modified Stillmans Technique
• Vibratory- Charters Technique, Bass Technique
• Circular- Fones Technique • Vertical-Leonards technique• Horizontal- Scrub Technique
(CARRANZA 9TH EDITION)

-Place head of the brush parallel to the occlusal plane.-Establish a 450 angle between bristles and long axis of the head.-Place bristles in the gingival sulcus as well as partially into the embrasure.-Move back and forth with vibratory motion 20 strokes per segment. (CARRANZA 9TH EDITION)-1 to 15 secs per area. (SOBEN PETER 2ND EDITION)
ADV- Easy to master. - Concentrates cleaning in areas where plaque accumulates. -For any patient with or without periodontal involvement.
BASS TECHNIQUE

DENTAL FOLSS
• Dental floss is best indicated for plaque and debris removal from embrasure where the papilla fills the interproximal space, and the teeth are in contact
• Objectives -removes plaque and debris from interproximal embrasure and
around implants -aids in identifying overhanging restorations -may be used as a vehicle for application of chemotherapeutic
agents in interproximal and subgingival areas

Types of dental floss
• Unwaxed floss: Thinnest type. Separates during use to cover larger surface area• Waxed floss: Used in tight proximal contacts and overhanging
restorations• Dental tape: Wider and flatter than conventional floss.
• Polytetrafluoroethylene (PTFE) floss Coated with teflon material. Resistant to fraying. • Braided nylon floss, G-floss and tapered G-floss Cleaning dental implants.• Tufted floss Variable diameter.
METHOD
• Take a floss 12-18 inches long.• Wrap around the right middle finger 2-3 times and then around
left middle finger.• Fulcrum on the cheek or in the mouth.• Pass through contact using a gentle seesaw motion.• Pass floss below the gingival margin.• Wrap it tightly around the tooth in a “C” shape.• Move the floss up and down, 3 or 4 strokes.• Remove floss using a seesaw motion.

WOODEN TOOTHPICKS
Used in cases of
• Concave proximal surfaces.
• Furcation areas.
• Class II and III embrasure spaces.
• Also used to introduce fluoride and chlorhexidine into proximal areas.

Method of use
• Insert toothpick into an angled plastic holder and break off the longer end.
• Moisten the end with saliva.• Place the tip at the gingival margin, at 90o to the long axis of the
tooth and trace it around the tooth• If possible, point the tip at less than a 45 degree angle into the
sulcus, around the tooth surfaces and in root concavities.• Stop inserting once resistance is felt.• Concave proximal surfaces are cleaned using an up and down
motion.• Clean exposed furcation areas by moving the toothpick in and
out.

TYPE I embrasure
TYPE II embrasure
TYPE III embrasure
DISADVANTAGES OF TOOTHPICKS
• Causes breakdown of tooth• Causes increased interproximal spaces
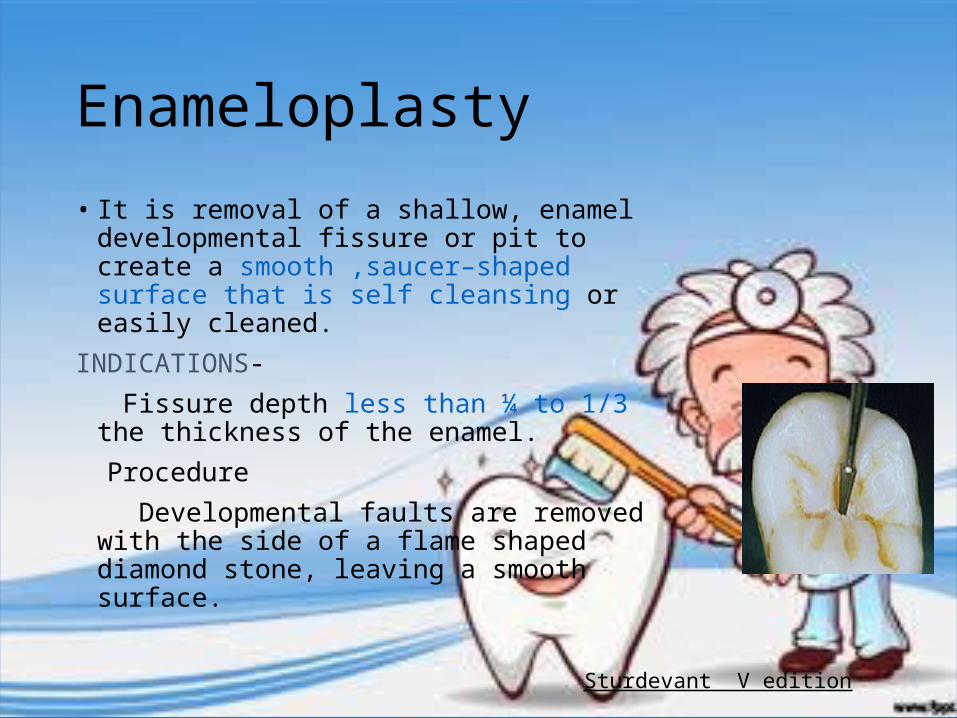
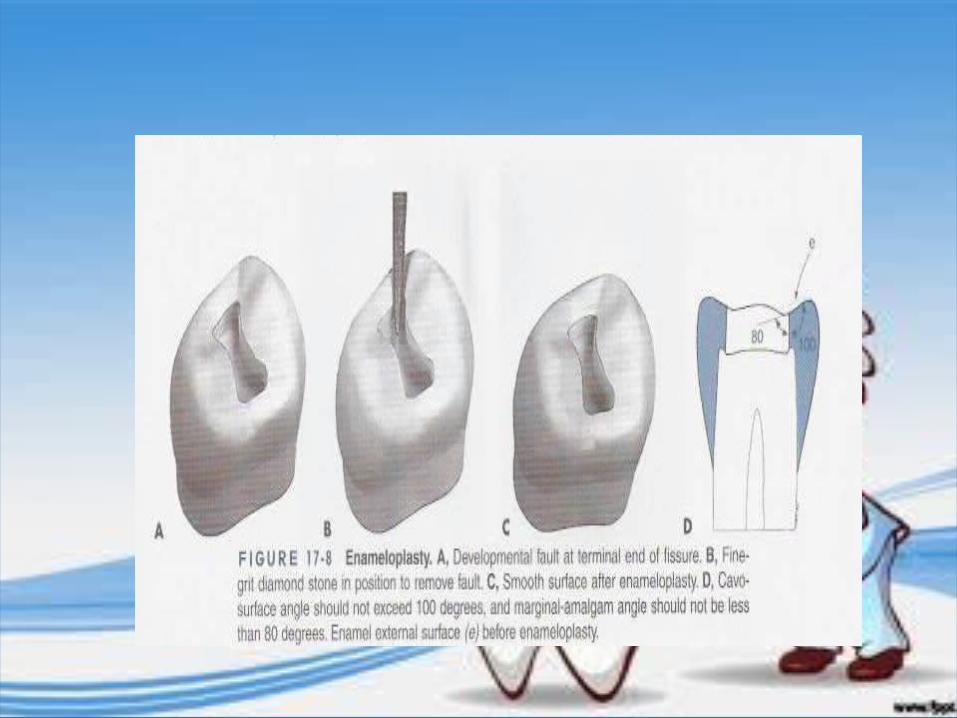
Enameloplasty• It is removal of a shallow, enamel developmental
fissure or pit to create a smooth ,saucer–shaped surface that is self cleansing or easily cleaned.
INDICATIONS- Fissure depth less than ¼ to 1/3 the thickness of
the enamel. Procedure Developmental faults are removed with the
side of a flame shaped diamond stone, leaving a smooth surface.
Sturdevant V edition

PIT AND FISSURE SEALANTS
A fissure sealant is a material applied to occlusal surfaces of the teeth in order to obliterate the occlusal fissures and remove the sheltered environment in which caries may thrive (Gordon 1962).
- Non invasive- Preventive- Seals deep narrow grooves

• Pit: It is defined as a small pinpoint depression located at the junction of developmental grooves or at terminals of those grooves. The central pit describes a landmark in the central fossae of the molars where developmental grooves join (Ash, 1993).
• Fissure: It is defined as deep clefts between adjoining cusps.. These defects occur on occlusal surfaces of the molars and premolars, with tortuous configurations that are difficult to assess from the surfaces. (Orbans, 1990)
Milestones of pit and fissure sealants
• 1895, Wilson reported the placement of a dental cement in pit & fissures to prevent caries.
• Hyatt(1923) Proposed technique called prophylactic odontotomy. Technique consisted of filling the fissures with silver or copper oxyphosphate cement as soon as the teeth erupted into the oral cavity. Later when fully erupted, preparing a small occlusal cavity and filling it with amalgam.
• Bodecker (1929) -Proposed a technique called fissure eradication. Involved mechanical eradication of fissures in order to transform deep, retentive fissures into cleansable areas

o Bunocore (1955) - Advocated the filling of pit and fissure with bonded resin.
o Mid1960's First materials used experimentally as sealants were based on cynoacrylates but they were never marketed.
o Bowen (1965) - Reported BIS-GMA material development. The basis of BIS-GMA resin is the reaction product of bisphenol A and glycidyl-methacrylate

Indications of pit & fissure sealants
• Presence of deep occlusal pit and fissures of newly erupted teeth (molars and premolars).
• Presence of lingual pits or palatal pits in relation to upper lateral incisors and molars.
• Presence of incipient lesion in the pit and fissure system.
• Children and young people with medical, physical or intellectual impairment with high caries risk.
• Children and young people with signs of higher caries activity and coming from non-fluoride area.
Contraindications
• Presence of shallow pit and fissures of molars and premolars.• An open occlusal caries lesion with extension into dentin.• Presence of large occlusal restoration.• Presence of proximal caries extending on to occlusal surface.• Partially erupted tooth where in isolation is a problem.• Uncooperative patient (getting adequate dry field is a problem).

Types of fissure system
U type almost the samewidth from top to bottom(12-15%)
V type-wide at top and gradually narrowing towards the bottom.(30-35%)
IK type, extremely narrow slit with a larger space at bottom.(24-26%)
I type with a extremely narrow slit.(18-20%) Inverted Y. (5-10%)
FISSURE SYSTEM

TYPES OF PIT AND FISSURE SEALANTS
A. Generations of sealants:
i. First generation sealants- ultraviolet light cure ii. Second generation - chemically cured (autopolymerized), iii. Third generation - visible light cure. iv. Fourth generation- contain fluorides
B. Three different kinds of materials have been used as occlusal sealants:
1. Resin based sealants- -Polyurethanes -Cyanoacrylates -Bisphenol a glycidylmethacrylate(BIS-GMA) 2. Glass ionomer sealants 3. Fluoride containing sealants

C. Type of fissure sealant
1.Filled and unfilled
2.Light cured and chemically (self) cured
3.Clear and tinted
• Polyurethanes - were among the first to be commercially marketed. -but proved to be too soft and totally disintegrated in the mouth after 2
or 3 months• Cyanoacrylates - they too disintegrated after a slightly longer time. -their use has been discontinued on account of low shelf-life and high
instability.• Bisphenol a glycidyl methylaerylate (BIS-GMA) -is a mixture of Bis-GMA and methyl methacrylate. -In 1972 Nuva-Seal was the first successful commercial sealant to be
placed on the market. Since then more effective second and third-generation sealants have become available.
Resin Based Sealants• are bonded to underlying enamel by
use of acid-etch technique. • form a tight seal, which prevents
leakage of nutrients to the microflora in deeper parts of the fissure.
• may be either pure resin, composites or compomers, and their polymerisation may be initiated chemically or by lightcomparative
• In studies of longer duration(>5yrs), greater longevity was reported for the chemically cured sealants .

• Work exceptionally well, and serve their function for many years when placed properly.
• Clinical limitation difficulty of handling in a moist environment. Unless complete isolation of the tooth has been achieved, salivary
contamination will result in failure of the sealant. • Many studies have confirmed that resin-based sealants have greater
retention than glass ionomer sealants, but these studies were all conducted under conditions of good isolation and moisture control.
Glass ionomer Sealants
CLINICAL ADVANTAGES• is their ability to bond chemically to dentin and
enamel without the use of the acid-etch technique which makes them less vulnerable to moisture.
• active fluoride release into the surrounding enamel.
DISADVANTAGES• poor retention, over periods, as short as 6 to
12 months.

• However, several studies have found that GIC's exert a cariostatic effect even after they had disappeared macroscopically. This effect might be based on remnants of the cement in the fissure as well as increased levels of fluorides on the enamel surface.
• used as an alternative to resin sealants, especially where resin sealants
are contraindicated.

Clinical situations in which glass ionomer may serve as a good sealant include- treatment of children whose primary molars have deeply pitted or
fissured surfaces
isolation may be difficult
treatment of permanent first or second molars that have not fully emerged
situations where a “transitional” sealant may be considered before placement of a “permanent” resin sealant
Fluoride-releasing sealants
• Incidence and severity of secondary caries are reduced or minimized around fluoride-releasing materials .
• Fluoride uptake may provide an additional anticariogenic effect if the fluoride released from its matrix is incorporated into the adjacent enamel.
• However, further long-term clinical trials are necessary to determine that the clinical longevity of the sealant retention is not adversely affected by the presence of incorporated fluoride

CARIES VACCINE

CARIES VACCINE'Vaccine' is an immunobiological substance designed to produce
specific protection against the given disease. It stimulates the production of protective antibody and other immune mechanisms.
HISTORYoFirst developed by Williams 1944 using a homologus lactobacillus
vaccine.oBowen in 1976 demonstrated monkeys immunized by whole live
cells of S.mutans developed lesser caries.oUnderwood and Miller published in 1881 bacteria are involved in the
pathogenesis of dental caries was clearly expressed in a paper .

PROSPECTIVE FOR VACCINATION
• Which Type of S. mutans is most important? - S. mutans (containing strains of serotypes c, e, and f), and
possibly S. sobrinus (serotypes d and g) is more imp in promoting dental caries.
- The others, S. cricetus (serotype a), S. rattus (serotype b), S. ferus (serotype c) and S. macacae (serotype c) are only very rarely or never isolated from human dental plaque.
• The salivary immunoglobulin may act as a specific agglutinin interacting with the bacterial surface receptors and inhibiting colonization and subsequent caries formation.
• They inactivate surface glucosyltransferase, which would then reduce the synthesis of extra cellular glucans resulting in reducing plaque formation.
• The salivary glands produce secretory IgA antibodies by direct immunization of the gut associated lymphoid tissue, they prevent S. mutans from adhering to the enamel surface or they may prevent formation of dextran by inhibiting the activity of glucosyltransferase
MECHANIISM OF ACGTION OF CARIES VACCINE

• The gingival crevicular mechanism involves all the humoral and cellular components of the systemic immune system, which may exert its function at the tooth surface.
• After subcutaneous immunization with S. mutans, the organism is phagocytosed and undergoes antigenic processing by macrophages.
Effective molecular targets for vaccine developmentThe subcellular component which are currently being seriously proposed
as vaccines are
(a) Glucosyltransferases (GTF)
(b) Wall associated proteins.
(c) Adhesins.
(d) Glucan- binding protein.

Glucosyltransferase (GTF):-
• Group of the extracellular enzymes involved in synthesis of polymer (glucans) from sucrose.
• Genes responsible for glucan synthesis in S. mutans are gtfB, gtfC, and gtfD
• Inactivation of the gtfD gene has also resulted in a mutant with lower cariogenicity on smooth surfaces
• Passive administration of antibody to GTF in diet can also protect rats from experimental dental caries.
• Thus, presence of antibody to glucosyltransferase in oral cavity prior to infection can significantly influence the disease outcome, presumably by interference with one or more of the functional activities of the enzyme

Wall Associated Proteins
Two purified proteins from the surface of S. mutans serotype c are currently being suggested for use as dental caries vaccines-
1. Antigen I/II or B described by Lehner and his colleagues, 2. Antigen A - a small molecular weight cell wall protein
The antibody to the Wall associated proteins should prevent dental caries by blocking both the colonization of the tooth and the build-up of dental plaque by S. mutans
Expression of Streptococcus mutans Wall-Associated Protein A Gene in Chinese Hamster Ovary Cells: Prospect for a Dental Caries DNA Vaccine DCB 2001

Adhesins
• Adhesins are the receptors which allow S.mutans to bind with pellicle.
• Adhesins from two principal human pathogens, Streptococcus mutans and Streptococcus sobrinus have been purified.
• Numerous immunization approaches have shown that active immunization (with intact antigen) or passive immunization can protect subjects from dental caries

Glucan-binding Proteins (GBP)
• The ability of mutans streptococci to bind to glucan is presumed to be mediated by cell wall-associated GBP.
• S. mutans secretes at least three distinct proteins with glucan-binding activity.
• Protection can be achieved by either subcutaneous injection of GBP in the salivary gland region or by mucosal application by the intranasal route.
• Saliva samples from young children often contain IgA antibody to GBP, indicating that initial infection with S. mutans can lead to natural induction of immunity to this protein.

• Challacombe et al. (1978) stated that IgG antibodies from serum reach the oral cavity through the gingival crevicular fluid.
• Seward (1971) stated that when the teeth erupted the local inflammation is common and during this time serum antibodies may stimulate opsonization and phagocytosis of bacterial cell.
Hajishengallis and Michalek- Oral Microbiol Immunol 1999
Contains structural elements of either adhesins or GTF or
GBP.
Also called attenuated
expression vectors.Helpful in targeting
vaccine to appropriate
lymphoid tissue for mucosal response.
Chemical conjugation of
functionally associated peptide components with
bacterial polyssacharides.
TYPES OF VACCINESSUB UNIT VACCINE RECOMBINANT VACCINE CONJUGATE VACCINE

-Added to the value of including multiple targets within the vaccine is that conjugation of protein with polysaccharide enhances the immunogenicity polysaccharide entity.
- Subcutaneous injection with conjugate-induced systemic IgM and IgG antibody responses to both peptide and polysaccharide, which could be boosted upon subsequent injection.
Hajishengallis and Michalek- Oral Microbiol Immunol 1999
ROUTE OF ADMINISTRATION OF VACCINE
• Both oral vaccine and passive immunization have been suggested as being possibly safer, than injected vaccine with its resultant high levels of circulating antibodies
• Subcutaneous administration of S. mutans was used successfully in monkeys and elicited predominantly serum IgG, IgM, and IgA antibodies. The antibodies find their way into the oral cavity via gingival crevicular fluid and are protective against dental caries.
ROUTES OF ADMINISTRATION:1. ORAL2. INTRA NASAL3. TONSILLAR4. MINOR SALIVARY GLAND5. RECTAL

Antibody responses
• Three main types of antibody response are:
(I) circulating antibody induced by systemic injection predominantly of IgG class) which enters the oral cavity by way of gingival crevice.
(ii) a secretory IgA Antibody which is produced by salivary glands.
(iii) local synthesis of IgG antibody in the gingiva has also been recently reported.
Hajishengallis and Michalek- Oral Microbiol Immunol 1999
Concerns regarding use of caries vaccine
o Heart cross-reactive antigens HCRA have been identified in S. mutans , which when injected in animals may damage to the heart. Streptococcus mutans antibodies, possibly reacts with, the myosin component of the heart tissues .
o The precise timing and number of injections which might ultimately be required in children has not yet been determined.
o Apart from logistic consideration of availability of patients and coordination with other vaccine programmes, fundamental details of the level and longevity of immune responses in humans are not yet known.
Nasal vaccine-newer approach• Unlike traditional vaccines, which are injected directly into the
bloodstream, the nasal spray vaccine works by way of the mucosal immune system—an antibody-producing “factory” that resides in the body’s mucosal surfaces, such as the lining of the respiratory, digestive, and urogenital tracts.
• By introducing the vaccine into the mucosal cells lining the nasal passages,( Michalek and Childers et al) hope to trigger an immune response that will spread throughout the body’s other mucosal sites, including the mouth.
Caries Vaccine
o Infants, representing the primary target population for a caries vaccine, become mucosally immunocompetent and secrete salivary immunoglobulin A antibodies during the first weeks after birth,
o Whereas mutans streptococci colonize the tooth surfaces at a discrete time period that extends around 26 months of life.
o Therefore, immunization when infants are about one year old may establish effective immunity against an ensuing colonization attempts by mutans streptococci.
Hajishengallis and Michalek-Oral Microbiol Immunol 1999

Lasers in caries prevention

Introduction
• 'Laser' is an acronym for 'light amplification by the stimulation emission of radiation'. Its theoretical basis was postulated by Albert Einstein.
• First tooth exposed to laser light was in 1960. • Laser light in dentistry is a unique, non-ionizing form of
electromagnetic radiation that can be employed as a controlled source of tissue stimulation, cutting or ablation, depending on specific parameters of wavelength, power and target tissue.

Laser use in dentistry
• Although Maiman had exposed an extracted tooth to his ruby laser in 1960, the possibilities for laser use in dentistry did not occur until 1989, with the production of the American Dental Laser for commercial use.
• This laser, using an active medium of Nd:YAG, emitted pulsed light and was developed and marketed by Dr Terry Myers, an American dentist.
• Though low-powered and due to its emission wavelength, inappropriate for use on dental hard tissue, the availability of a dedicated laser for oral use gained popularity amongst dentists.
• In 1989, experimental work by Keller and Hibst using a pulsed erbium YAG (2,940 nm) laser, demonstrated its effectiveness in cutting enamel, dentine and bone.
• This laser became commercially available in the UK in 1995 and, shortly followed by a similar Er,Cr:YSGG (erbium chromium: yttrium scandium gallium garnet) laser in 1997, amounted to a laser armamentarium that would address the surgical needs of clinical dentistry in general practice
Advantages o Appreciated by patients as they are more comfortable than drilling. o With water-cooling appears to have less side effects such as vibration,
heat, sound or iatrogenic damages of adjacent teeth.o Laser irradiation causes minimal damage to surrounding tissues,
minimal thermal changes of dental hard tissue composition, and creates favorable surface characteristics (e.g. reduced smear layer, smooth surface, and little debris).

LASERS IN CARIES PREVENTIONo Yamamoto and Oaya used as YAG laser at energy densities of 10 to 20
J/cm2 and demonstrated that the lased enamel surface was more resistant to in vitro demineralization than non lased enamel.
o Stern and Sognnaes demonstrated in vivo that enamel subjected to 10 to 15 J/cm2 showed a greater resistance to dental caries than the controls.
o Stern concluded that energy levels below 250 J/cm2 did not permanently alter the pulp but necrosis could occur when energy level, reached 1800 J/cm2 or higher.
o Lobene and Colleagues, observed that C02 laser irradiation to tooth enamel caused small amounts of hydroxyapatite to be converted to more insoluble calcium orthophosphate apatite. This paved the way for widespread use laser in prevention of caries.
LASERS IN CARIES PREVENTION
• In 1985 Terry Myers used Nd:YAG laser for debridement of incipient caries. When a topical fluoride treatment was performed after argon laser conditioning of enamel, an even more dramatic reduction in enamel acid demineralization was observed
• Studies have demonstrated the potential of laser pre-treatment of enamel or tooth roots to inhibit subsequent acid-induced dissolution or artificial caries-like challenge in the laboratory (Westerman et al, 1994).
• Nelson, 1987 demonstrated the potential caries-inhibitory effects of pulsed carbon dioxide laser irradiation of enamel at low frequencies.
• Inhibition of subsequent demineralization of enamel of up to 50% with the laser conditions they used, and reported that these effects were wavelength-dependent.

EFFECTS OF LASERS ON ENAMEL• Treatment with lasers can reduce the rate of subsurface
demineralization in enamel • It may be due to combination of reduced enamel permeability
with a reduced solubility promoted by melting, fusion, and recrystallization of enamel crystallites, which could seal the enamel surface
• Studies showed the reduction of enamel solubility could be due to changes in the ultrastructure of enamel, such as the reduction of water and carbonate contents, the increase in the hydroxyl ion contents, formation of pyrophosphates, and the decomposition of proteins

Use of individual lasers• Nd:YAG laser is indicated for use in superficial pigmented caries
removal.• Erbium family(Er:YAG , Er:YSGG) of lasers are the lasers of choice &
most efficient for enamel, dentin & caries removal.• They have shown to reduce the bacterial population & produce a
analgesic effect on the tissues.• Lasers can also be used for sealant placement- to clean,
sterilize ,clearly visualize & even etch the enamel grooves.

Different types of lasers and their wavelengths The frequent wavelengths used in studies for caries prevention are:
• Nd:YAG (λ = 1.64 µm)• Er:YAG (λ = 1.94 µm)• Er,Cr:YSGG (λ = 1.79 µm)• Argon (λ = 488–514 nm)• CO2 (λ = 9.6 and 10.6 µm)

Carbon Dioxide Lasers• The CO2 laser was demonstrated to be the most successful laser for
increasing enamel’s acid resistance due to the higher absorption in phosphate radicals of hydroxyapatite.
• Depending on the fluence applied, wavelengths of 9.3, 9.6, 10.3, and 10.6 µm promote melting of the enamel surface, which can be achieved at a temperature of 1200°C.
• The 10.6-µm laser line is the strongest one, and most of the commercially available
• The role of CO2 lasers in dental caries prevention has been explored since the 1960s, and continuous wave mode and pulsed lasers are used.
• The combination of CO2 laser irradiation with several types of fluoride application showed important results and it was suggested that laser irradiation can reduce initial enamel demineralization, inhibit subsequent lesion progression, and enhance fluoride adsorption.

Effectiveness of lasers in caries prevention• Laser treatment particularly in combination with topical fluoride
application (NaF, APF), increase resistance against caries, desensitization of hypersensitive dentine (Er:YAG) and improve marginal seal under composite resin (Nd:YAG).
• C02-laser = Caries inhibition up to 82.7%• Er:YAG-laser = Reduction in surface lesion depth (root surfaces 39%,
primary enamel surfaces 56%)• Nd:YAG-laser (with Duraphat) = Caries inhibition (pits and fissures
43%, smooth surfaces 80%).

Conclusion • Dental caries is a disease that usually can be successfully prevented or
controlled • It is an important task for the dental team to teach individuals to take
correct actions to minimize the risk for the disease.• It is also possible to identify and evaluate factors of importance for
cavity formation.• By targeted actions, such risk factors can usually be changed, resulting
in a reduced risk for caries. • In clinical practice, more emphasis is paid presently on treatment rather
than prevention. A lot of time, energy and manpower can be saved if more attention is paid to prevention.
• Research in new evidence based – methods in prevention would help us in reducing the morbidity associated with dental caries.

References• Sturdevent’s Art and Science of Operative Dentistry – 5th edition
• Cariology. Ernest Newbrun. 3rd edition
• Essentials of Preventive and Community dentistry. Soben Peter. 2nd edition
• Shafer’s textbook of oral pathology. 5th edition
• Clinical uses of fluorides. Stephen H.Y. Wei
• The biological basis of dental caries. Lewis Menakar

• Fluorides in caries prevention. J.J. Murphy.• Fluorides in dentistry. Ole Feferkov.• J Dent Research vol 77,June 1998• General dentistry March/April 2007, Vol. 55 No. 2, Page 105-111.• British dental journal volume 202 no. 1 jan 13 2007.• British dental journal volume 202 no. 8 apr 28 2007 .
