care around birth - rmncha.inrmncha.in/wp-content/uploads/publications_img/1502707675.pdf · deaths...
TRANSCRIPT
A successful journey towards respectful and quality maternal and newborn care services.
Care around BIRTH
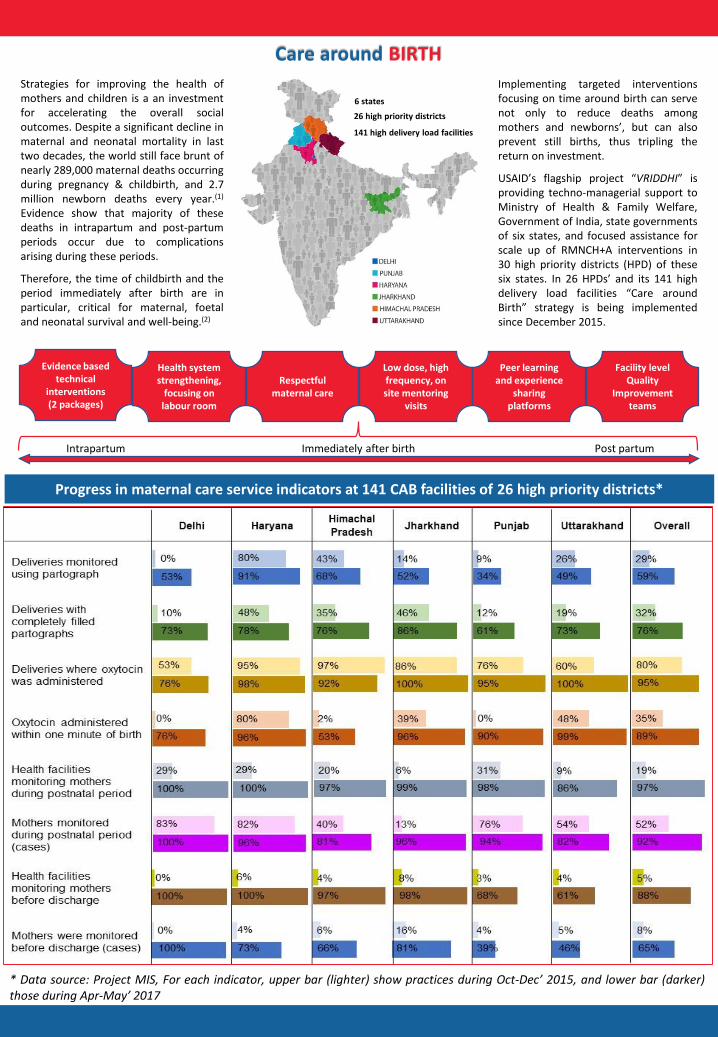
Progress in maternal care service indicators at 141 CAB facilities of 26 high priority districts*
* Data source: Project MIS, For each indicator, upper bar (lighter) show practices during Oct-Dec’ 2015, and lower bar (darker)those during Apr-May’ 2017
Strategies for improving the health ofmothers and children is a an investmentfor accelerating the overall socialoutcomes. Despite a significant decline inmaternal and neonatal mortality in lasttwo decades, the world still face brunt ofnearly 289,000 maternal deaths occurringduring pregnancy & childbirth, and 2.7million newborn deaths every year.(1)
Evidence show that majority of thesedeaths in intrapartum and post-partumperiods occur due to complicationsarising during these periods.
Therefore, the time of childbirth and theperiod immediately after birth are inparticular, critical for maternal, foetaland neonatal survival and well-being.(2)
Implementing targeted interventionsfocusing on time around birth can servenot only to reduce deaths amongmothers and newborns’, but can alsoprevent still births, thus tripling thereturn on investment.
USAID’s flagship project “VRIDDHI” isproviding techno-managerial support toMinistry of Health & Family Welfare,Government of India, state governmentsof six states, and focused assistance forscale up of RMNCH+A interventions in30 high priority districts (HPD) of thesesix states. In 26 HPDs’ and its 141 highdelivery load facilities “Care aroundBirth” strategy is being implementedsince December 2015.
6 states
26 high priority districts
141 high delivery load facilities
Care around BIRTH
Evidence based technical
interventions (2 packages)
Health system strengthening,
focusing on labour room
Respectful maternal care
Low dose, high frequency, on site mentoring
visits
Peer learning and experience
sharing platforms
Facility level Quality
Improvement teams
Intrapartum Immediately after birth Post partum

Progress in new-born care service indicators at 141 CAB facilities of 26 high priority districts*
* Data source: Project MIS, For each indicator, upper bar (lighter) show practices during Oct-Dec’ 2015, and lower bar (darker)those during Apr-May’ 2017
Package 1 Package 2
Essential birth care and labour monitoring
Management of postpartum haemorrhage
Active management of labour (third stage)
Management of pre-eclampsia & eclampsia
Essential newborn care & resuscitation
Care of small and sick newborns
Newborn vaccination Management of pre-term labour
Postnatal monitoring & counselling at discharge
Management of maternal & newborn infection
Stepwise approach
Comprehensive baseline assessment of labour room environment,and maternal newborn practices and competencies (total 748 datapoints, 141 intervention facilities)
Roll out of first technical intervention package (Mar-Jun 2016)▪ 25 district level trainings completed▪ 1446 health providers (medical officers and nurses) trained
State level advocacy and dissemination workshops in all 6 states
Low dose high frequency mentoring visits (May 2016 onwards)▪ >1000 mentoring visits conducted at intervention facilities▪ Activities include hand holding, capacity building, collecting
MIS data, observing deliveries for practice assessment, andconducting exit interviews
Constitution of facility level Quality Improvement (QI) teams▪ 130 QI teams notified in intervention facilities▪ 763 QI team meetings conducted▪ Around 800 service providers involved in QI processes
Experience sharing platforms initiated (Oct 2016 onwards)▪ 28 district and 6 state level experience sharing meetings held
Labour room reassessment for implementation of 2nd technicalintervention package ((Mar-Jun’ 2017)
Roll out of 2nd technical intervention package (May 2017 onwards)
Technical Intervention Packages
✓ 14 evidence based interventions are being strengthenedthrough these trainings by improving knowledge and skillsof service providers.
✓ Time allocation during the training sessions comprisedmostly of practice sessions (50% time), along with plenarydiscussions (27%), presentation (7%), instructions foractivities (9%), and measurement of learning (7%).
✓ Novel approaches, like use of simulation tools (for ENCR,KMC and feeding of LBW babies) and obstetric drills (forPPH and pre eclampsia/eclampsia, were employed.
✓ 150 staff nurses from intervention facilities have beentrained at national skill labs.

DISCLAIMER: This document is made possible by the generous support of the American People through the United States Agency for International Development (USAID). The contents are the responsibility of IPE Global Limited and do not necessarily reflect the views of USAID or the United States Government.
To know more about the project and intervention, write to:
VRIDDHI: SCALING UP RMNCH+A INTERVENTIONS/USAIDIPE Global Ltd. – IPE Global House, B-84, Defence Colony, New Delhi – 110 024Email: [email protected]
Published in August, 2017
References:1. The Global Strategy for Women’s Children’s and Adolescent’s Health (2016-2030)2. Tuncalp Ӧ, Were WM, MacLennan C, Oladapo OT, Gulmezoglu AM, Bahl R, Daelmans B, Mathai M, Say L, Kristensen F, Temmerman M, Bustreo F.
Quality of care for pregnant women and newborns—the WHO vision. BJOG 2015;122:1045–1049.3. The Global Strategy for Women’s Children’s and Adolescent’s Health (2016-2030)4. A Strategic Approach to Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCH+A) in India
Posters developed on Respectful Maternity CareJob aids developed for labour rooms
Scale of success
▪ The “Care around Birth” approach synergized thematic areas and high priorityinterventions in a structured pattern. This along with system strengthening effortsand improving client experience through respectful care has resulted into an all-round improvement in the intervention facilities.
▪ Project MIS has revealed a gradual but sustained improvement in maternal andnewborn care practices across all intervention facilities.
▪ First technical package lays emphasis on strengthening the universal interventionsfor mothers and newborns, while the second phase focuses on the managementof complications. Secondly, The trainings were phased as district level trainings,followed by onsite capacity building through low dose, high frequency mentoringvisits. This phasing out of trainings resulted in improved practices, along with theenhancement of knowledge among the service providers.
▪ The Quality Improvement (QI) processes institutionalized in the facilities hasresulted in enhanced ownership and accountability. This has further facilitatedidentification of local solutions for issues identified thus ensuring sustainability.
Since the start of implementation of “Carearound Birth” approach in 141 facilities, anADDITIONAL -
▪ 30,297 women were monitored duringdelivery using partograph
▪ 106,371 women received oxytocin withinone minute of delivery
▪ 45,818 mothers were monitored duringthe post natal period
▪ 5,11,135 postnatal contacts were madewith mothers after delivery
▪ 66,205 mothers were monitored beforebeing discharged
▪ 99,040 newborns were monitored within1 hour of delivery
▪ 73,648 newborns had temperaturemonitored
▪ 84,973 newborns received Vitamin K1after birth
▪ 18,241 newborns had breastfeedinginitiated within 1 hour after birth
▪ 49,081 newborns received all 3 essentialvaccines (Hep B, OPV & BCG) beforedischarge
▪ 1,503 newborns were successfullyresuscitated out of asphyxia
▪ 59,538 newborn were monitored beforedischarge
Results and learning’s
Scale up and way forward
▪ Implement second technical intervention package and continue mentoringsupport in the 141 intervention facilities.
▪ Supporting in roll out of “Care around Birth” strategy in additional 529 L2 & l3health facilities of 26 HPDs through RMNCH+A Supportive Supervision mechanism.
▪ Supporting scale up of intervention to non high priority districts throughgovernment resources approved in the Program Implementation Plans for 2017-18for 6 states by the Ministry of Health & Family Welfare, Government of India.
▪ Gather evidence of change by collecting data on key practices and documentingqualitative improvements, disseminate learnings and evidence of impact atnational level and in other states to broaden the scope of the intervention.