cardiovascular system - medical nutrition therapy portfolio · nutrition therapy intervention...
TRANSCRIPT

Cardiovascular System
KNH 406

Cardiovascular Disease
Leading cause of death in U.S.
70 million Americans
$400 billion in direct and indirect costs
Rate has dropped 40% in past 30 years

© 2007 Thomson - Wadsworth

Cardiovascular System
Anatomy & Physiology
Regulates blood flow to tissues
Retrieves waste products
Thermoregulation
Gas exchange
Closed loop of blood vessels

Hypertension
Chronic elevation in blood pressure
> 140/90 mmHg
“Silent killer”
Increases risk for CHF, kidney failure, MI, stroke,
aneurysms, vision problems

© 2007 Thomson - Wadsworth

Hypertension
Etiology
Primary or essential – idiopathic
Secondary – result of another chronic condition
Lifestyle factors – smoking, exercise, diet
Sodium intake
Inflammatory response

Hypertension
Pathophysiology
Excessive secretion of vasopressin & angiotensin II
Smoking
Renal disease
Adrenal disorders
Neurological disease

Hypertension
Treatment
Reduce risk of CD and renal disease
Lower BP to < 140/90
Through:
Weight reduction, physical activity, nutrition therapy,
pharmacological intervention
Medication

Hypertension
Nutrition Therapy
DASH – Dietary Approaches to Stop Hypertension
Decrease sodium, saturated fat, alcohol
Increase calcium, potassium, fiber
Lifestyle modifications
Weight loss

© 2007 Thomson - Wadsworth

Hypertension
Nutrition Therapy
Sodium restriction controversial
“salt sensitive” or “salt resistance”
Limit processed & cured foods, no added salt during
preparation and cooking
Limit to 2400 mg/day

© 2007 Thomson - Wadsworth

© 2007 Thomson - Wadsworth

Hypertension
Nutrition Therapy
Alcohol in moderation
Potassium, calcium, and magnesium inversely related to BP
from food intake vs. supplements

Hypertension
Nutrition Therapy
DASH
Comprehensive dietary method
Variety of foods – high fruit & vegetable intake

Hypertension
Nutrition Therapy
Physical activity
At least 30 minutes per day
Smoking
Cessation - single most important factor

Hypertension
Nutrition Therapy Prescription
Weight reduction
Assess dietary intake
Meet DASH dietary goals
Tailor exercise goals

Atherosclerosis
Thickening of the blood vessel walls caused
by presence of plaque (AS)
Arteriosclerosis… includes loss of vascular
elasticity
Results in restriction of blood flow
Myocardial infarction (MI)
Cerebrovascular incident (stroke)
Peripheral vascular disease (PVD)
CAD and CHF


Atherosclerosis
Etiology - risk factors; additive effect
Family history
Age and sex
Obesity
Dyslipidemia
Hypertension



© 2007 Thomson - Wadsworth

Atherosclerosis
Etiology - risk factors cont.
Physical inactivity
Atherogenic diet
Diabetes mellitus
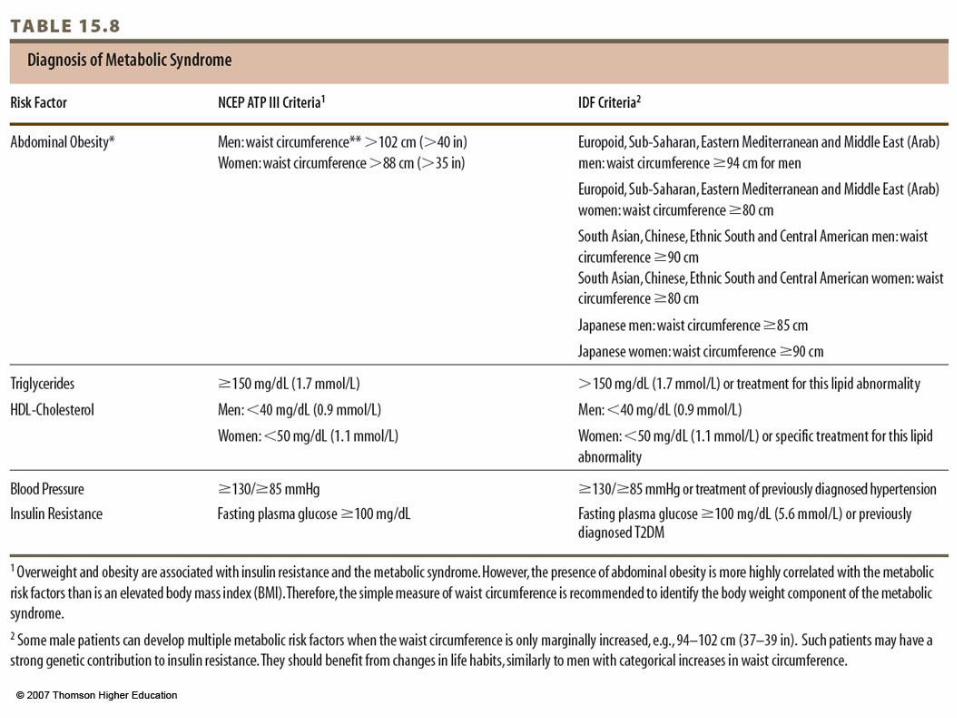
Impaired fasting glucose/ metabolic syndrome
Cigarette smoke
© 2007 Thomson - Wadsworth


© 2007 Thomson - Wadsworth

© 2007 Thomson - Wadsworth

Atherosclerosis
Nutrition Therapy
Therapeutic Lifestyle Changes (TLC) developed as
component of ATP-III
Modifications in fat, cholesterol
Rich in fruits, vegetables, grains, fiber
Limit sodium to 2400 mg
Include stanol esters
See Table 15.11 for summary, complete guidelines in Appendix
E9

© 2007 Thomson - Wadsworth

Atherosclerosis
Nutrition Therapy - Fat Modifications
Total fat 25-35% of calories
Very-low-fat diets
Saturated fat < 7% of calories
Avoid trans fats
Increase intake of monounsaturated fats &
Polyunsaturated omega-6 fatty acids
Increase intake of omega-3 essential fatty acids
Limit dietary cholesterol < 200 mg daily

© 2007 Thomson - Wadsworth

Atherosclerosis
Nutrition Therapy - Other
Increase sources of soluble fiber
Increase intake of plant sterols
Weight loss – BMI 18.5-24.9
Regular physical activity

Atherosclerosis
Nutrition Therapy Prescription
Assessment of dietary fat intake, saturated fat intake
MEDFICTS assessment tool
Dietary CAGE questions – Table 15.12
REAP –Table 15.13
Target weight calculated
Prioritize nutrition problems
Multiple planned visits with R.D.


Ischemic Heart Disease
Inadequate blood supply to the heart (a.k.a. CAD)
Occlusion caused by AS - may be asymptomatic
Angina – chest pain
Can precipitate MI causing necrosis of tissue

Ischemic Heart Disease
Etiology
Acute coronary syndrome – acute MI or unstable angina
Plaque erosions, rupture of plaque forming thrombus,
vasoconstriction
Traditional risk factors for AS apply to IHD
C-reactive protein (CRP) good predictor

Ischemic Heart Disease
Pathophysiology
MI or angina initiated by:
Sudden blockage
Hemorrhage
Arterial spasm
Increase in myocardial oxygen demand
All related to occlusion of the lumen by AS
Soft lipid more likely to cause MI
Ischemic Heart Disease
Nutrition Therapy
Post MI
Decrease oral intake
Clear liquids, no caffeine
Progress to soft, more frequent meals
Individualized – use TLC recommendations

Peripheral Arterial Disease
Occlusion of blood flow in non-coronary arteries (lower extremities)
Pathophysiology similar to AS and IHD
Eventually suffer from denervation of affected muscle
Can cause ulceration; commonly foot or toes

Peripheral Arterial Disease
Clinical manifestations/diagnosis
Intermittent claudication – cramp-like pain with activity
Ankle Brachial Index (ABI)
Treadmill test
Major risk for amputation

Heart Failure
Impairment of the ventricles’ capacity to eject or fill
with blood
Underlying cause – structural or functional
End-stage CVD

Heart Failure
Etiology/pathophysiology
Stages of heart failure – see Table 15.15
Primary cause – IHD, htn., dilated cardiomyopathy, valvular disease
Begins with heart injury or LVH
BP changes
Heart becomes weak and dilated
Progressive

© 2007 Thomson - Wadsworth
© 2007 Thomson - Wadsworth

© 2007 Thomson - Wadsworth

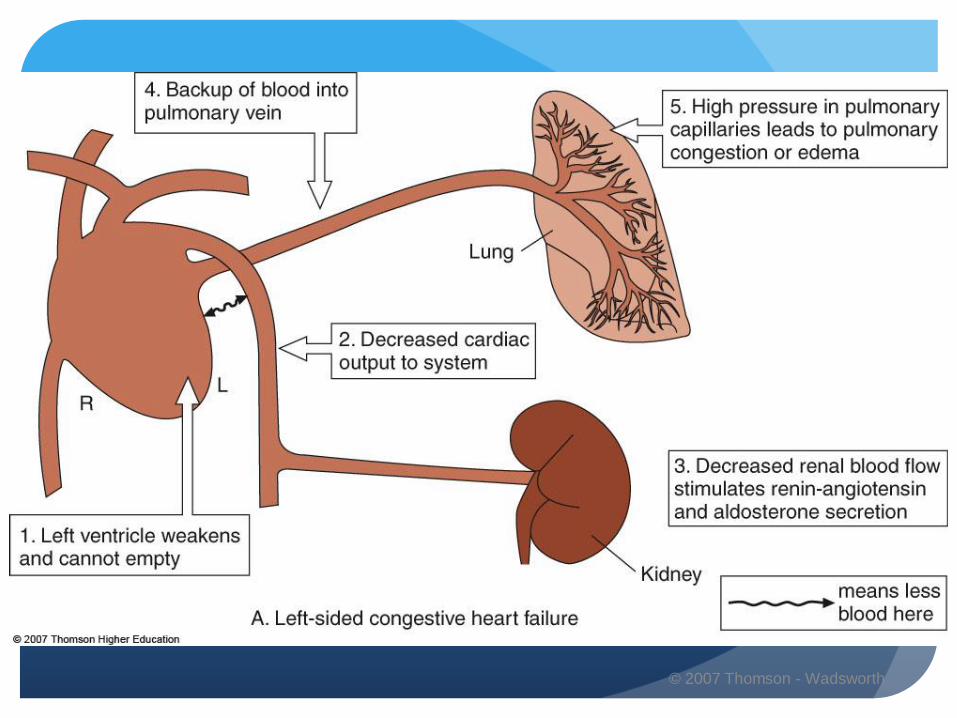
Heart Failure
Clinical manifestations
Decreased blood flow and oxygen
Dyspnea, fatigue, weakness, exercise intolerance, poor
adaptation to cold
Orthopenea - if left-sided failure
Fluid retention, pulmonary congestion, edema, hepatomegaly,
splenomegaly, ascites - if right-sided failure

Heart Failure
Treatment
Treat underlying cause
Control symptoms
BP control
Prevent continued damage
Medications
Prevention of respiratory infections
Exercise
Nutrition therapy

Heart Failure
Nutrition Therapy Implications
Increased workload/difficulty eating
Cardiac cachexia – malnutrition/ wasting, fatigue, anorexia
L-carnitine, CoQ10, creatine, thiamin, taurine

Heart Failure
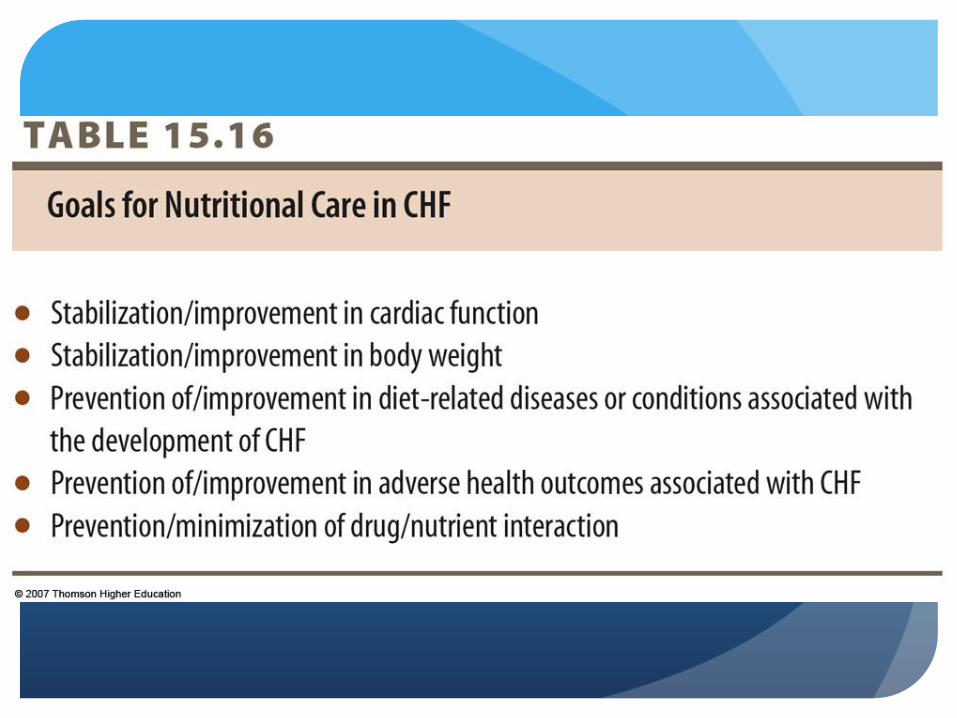
Nutrition Therapy Intervention
Control signs and symptoms
Promote overall nutritional status rehabilitation – see Table 15.16
Sodium and fluid restriction
2000 mg Na
Fluid 1 mL/kcal or 35 mL/kg
Correction of deficiencies
Increase nutrient density
Enhance oral intake

Heart Failure
Nutrition Therapy
Assess drug-nutrient interactions
Losses of water-soluble vitamins
Supplementation may be warranted
Consider arginine, carnitine and taurine in dietary regimen