cardiology abim review. mksap topics nelle –coronary artery disease –valvular heart disease...
TRANSCRIPT

Cardiology ABIM Review
MKSAP Topics
• Nelle– Coronary artery
disease– Valvular heart disease– Pregnancy– Peripheral arterial
disease
• Dylan– Arrhythmias– Heart failure– Pericardial disease– Aortic disease– Myocardial disease
Arrhythmias
Atrial Fibrillation
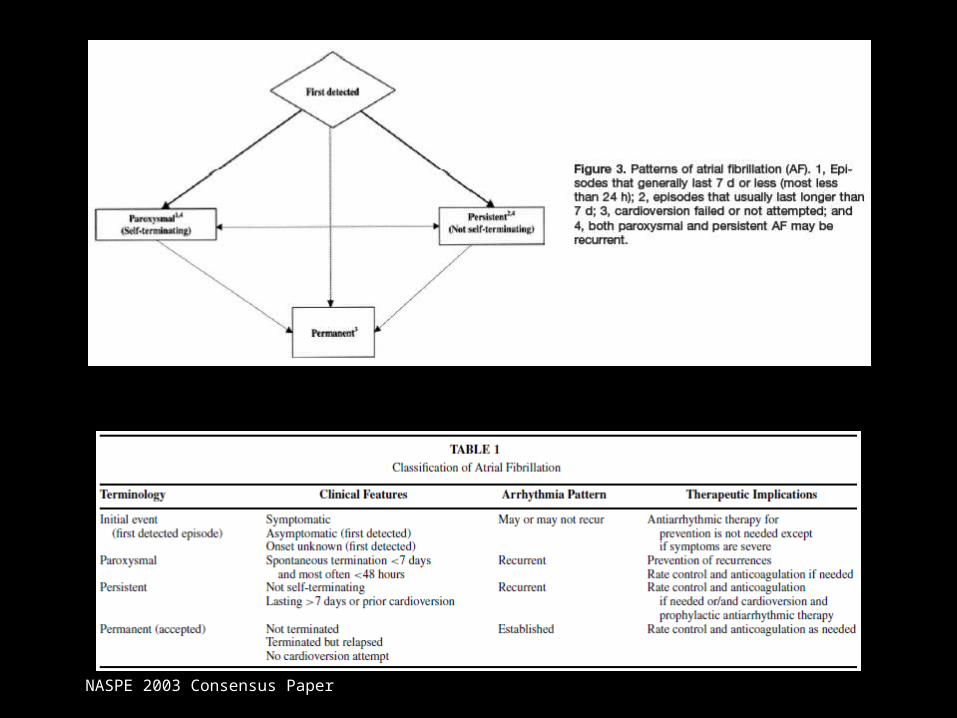
NASPE 2003 Consensus Paper
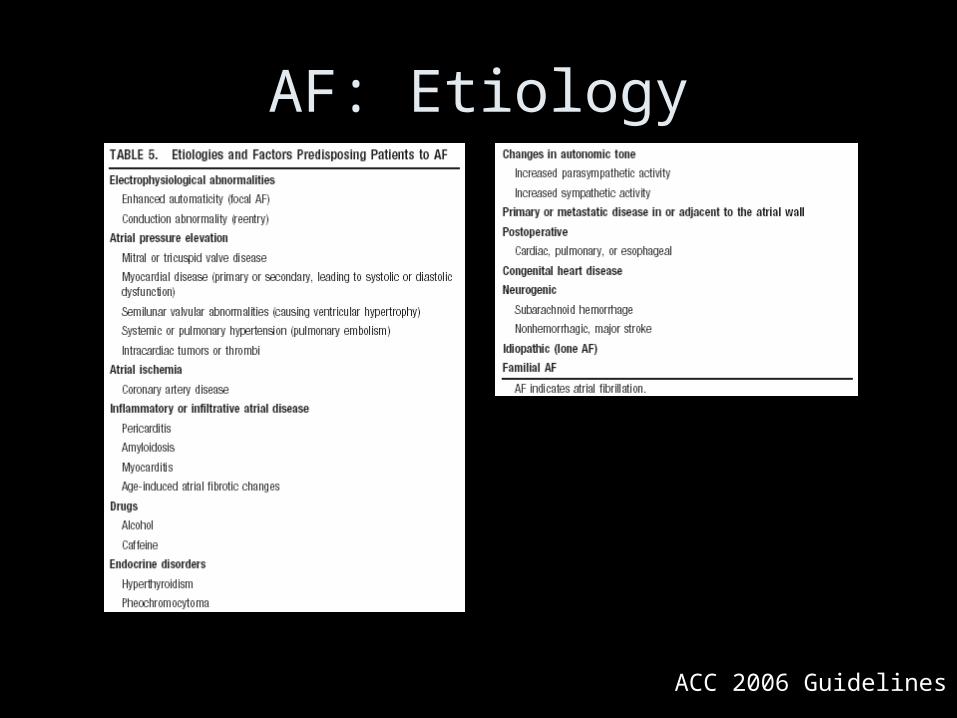
AF: Etiology
ACC 2006 Guidelines
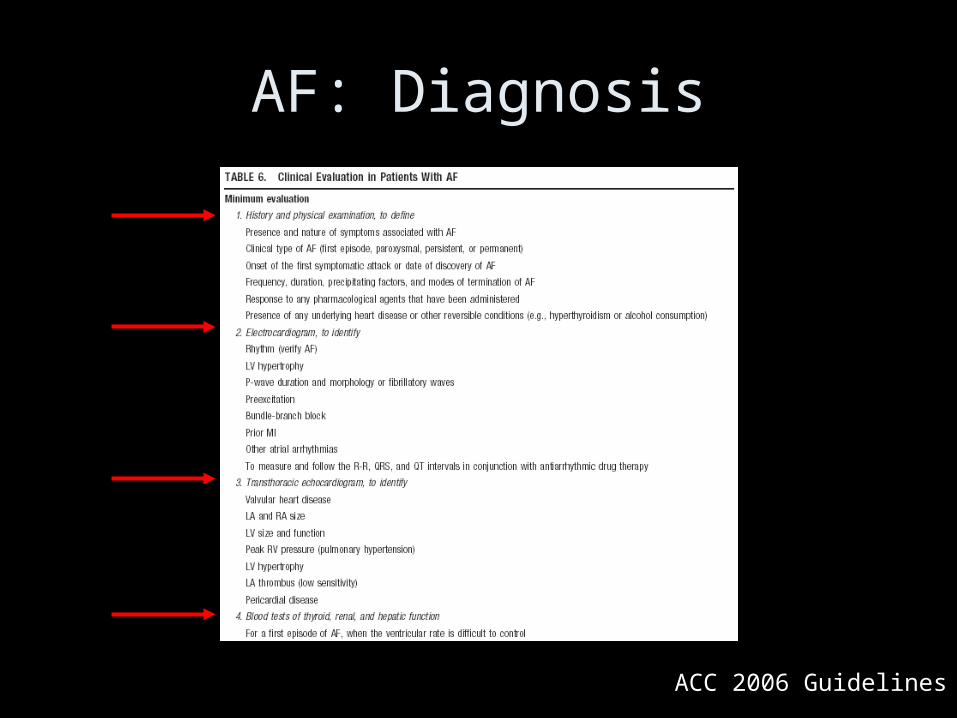
AF: Diagnosis
ACC 2006 Guidelines
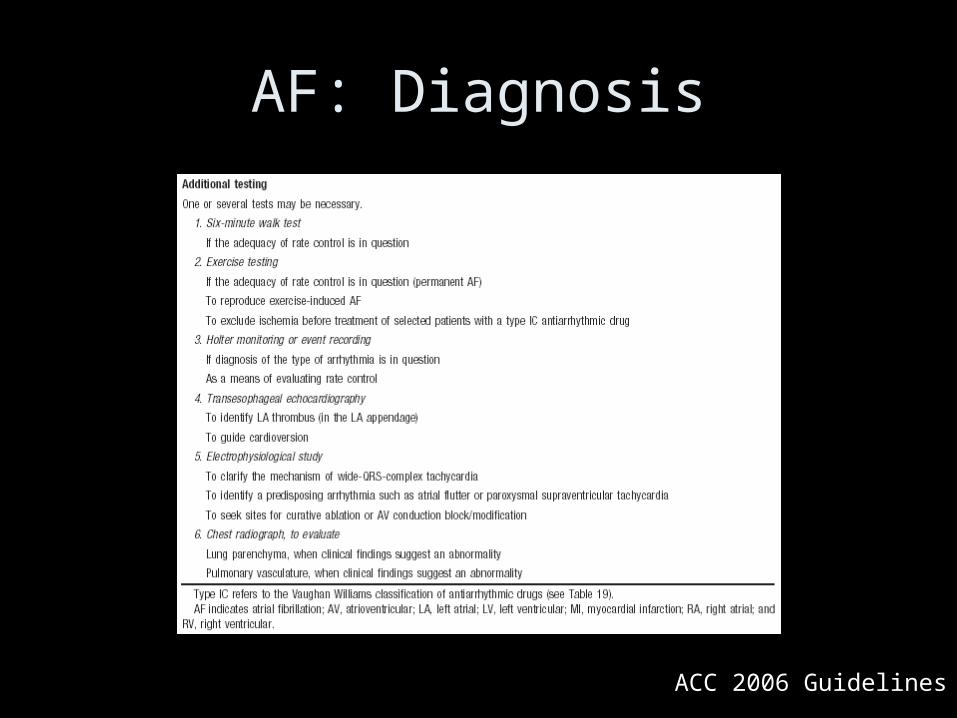
AF: Diagnosis
ACC 2006 Guidelines
ACC 2006 Guidelines
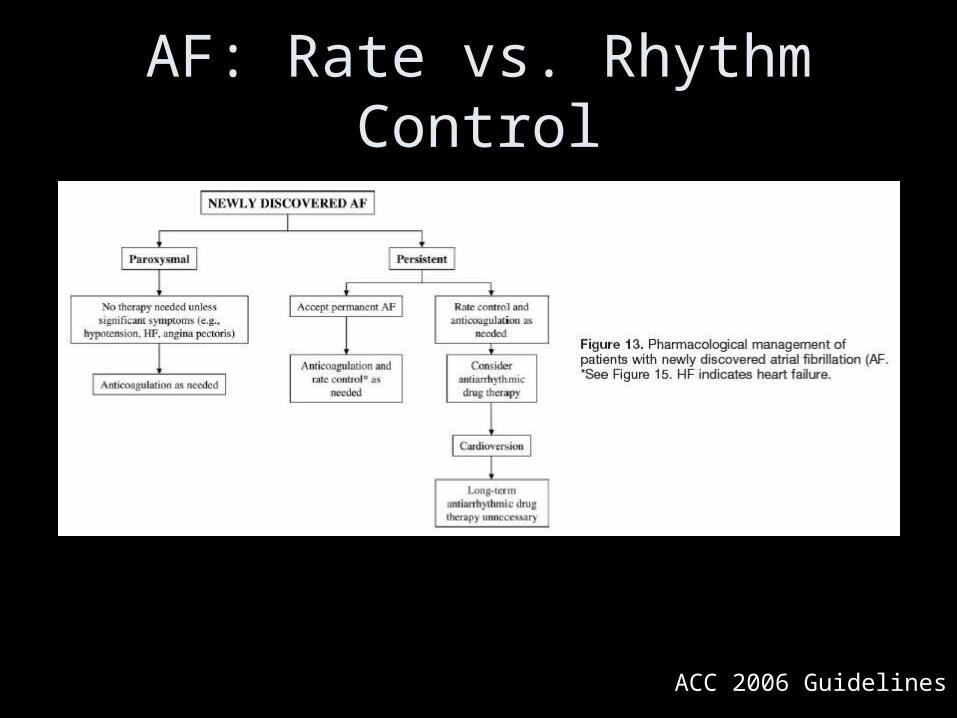
AF: Rate vs. Rhythm Control

ACC 2006 Guidelines
AF: Rate vs. Rhythm Control
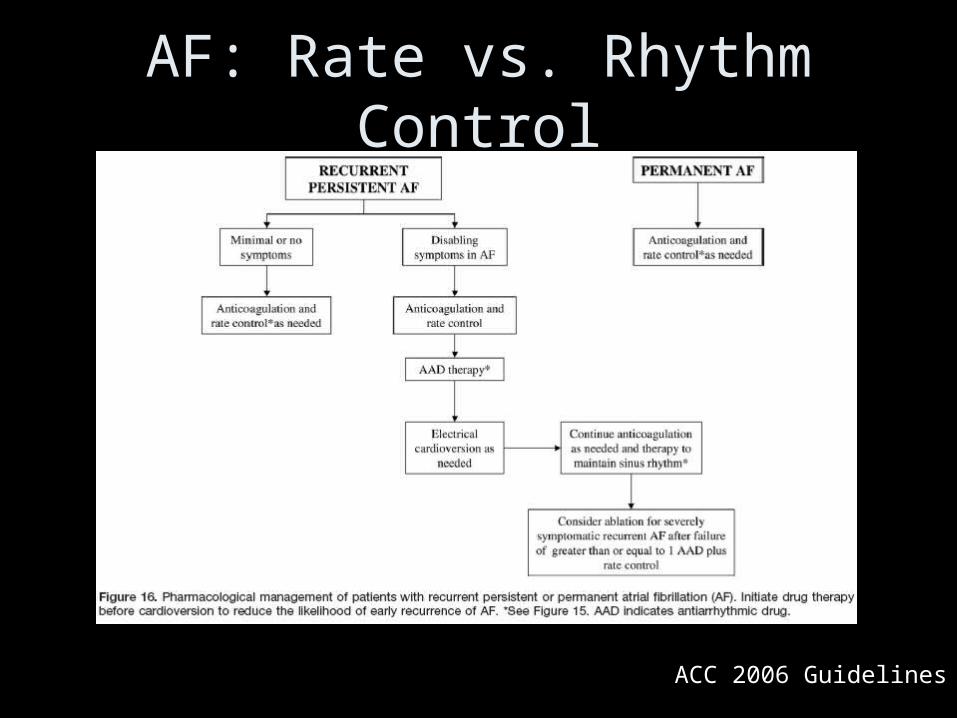
ACC 2006 Guidelines
AF: Rate vs. Rhythm Control

ACC 2006 Guidelines
AF: Rate vs. Rhythm Control

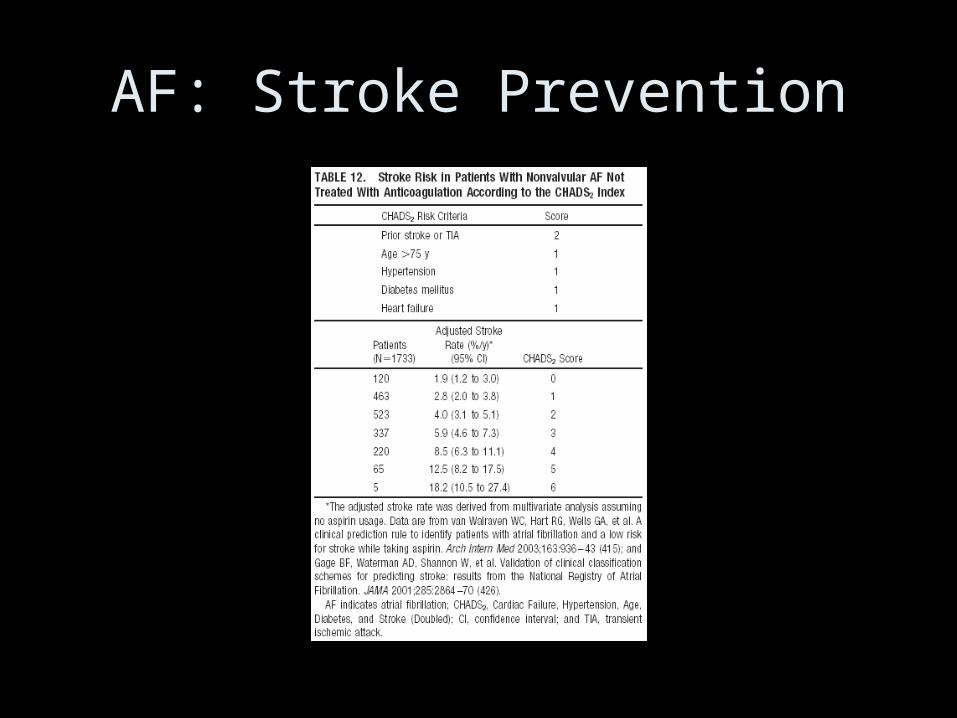
AF: Stroke Prevention
AF: Stroke Prevention
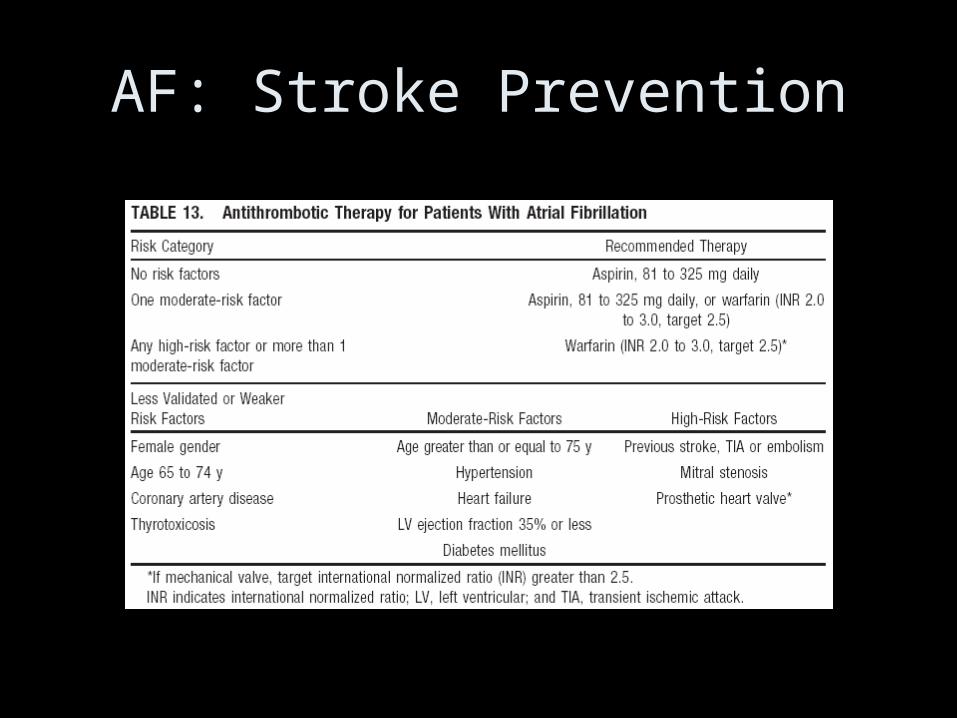
AF: Stroke Prevention
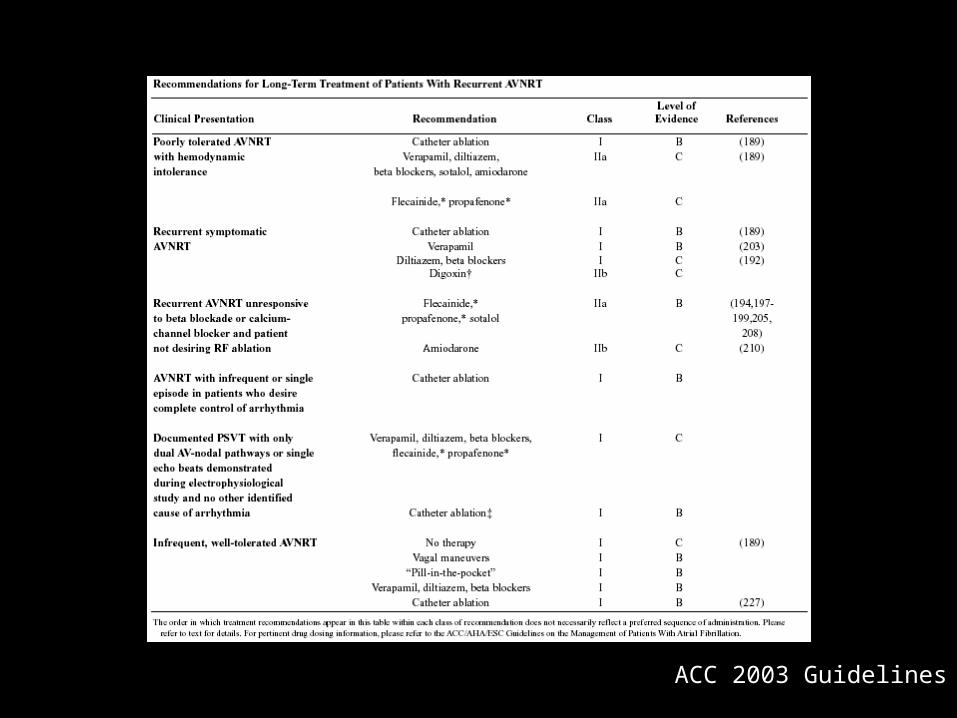
Supraventricular Tachycardias
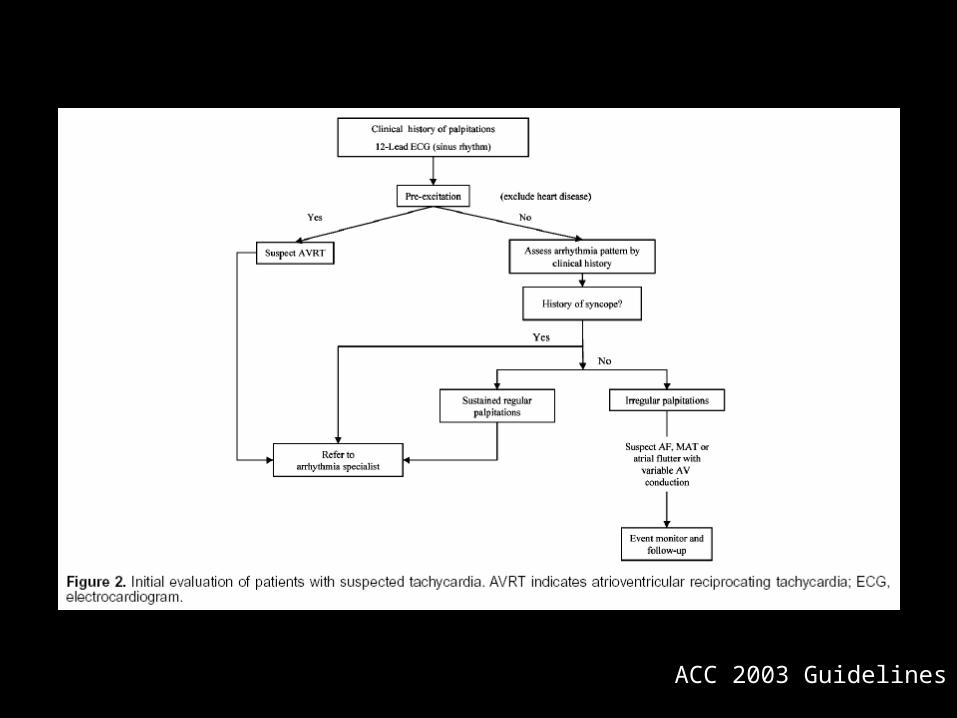
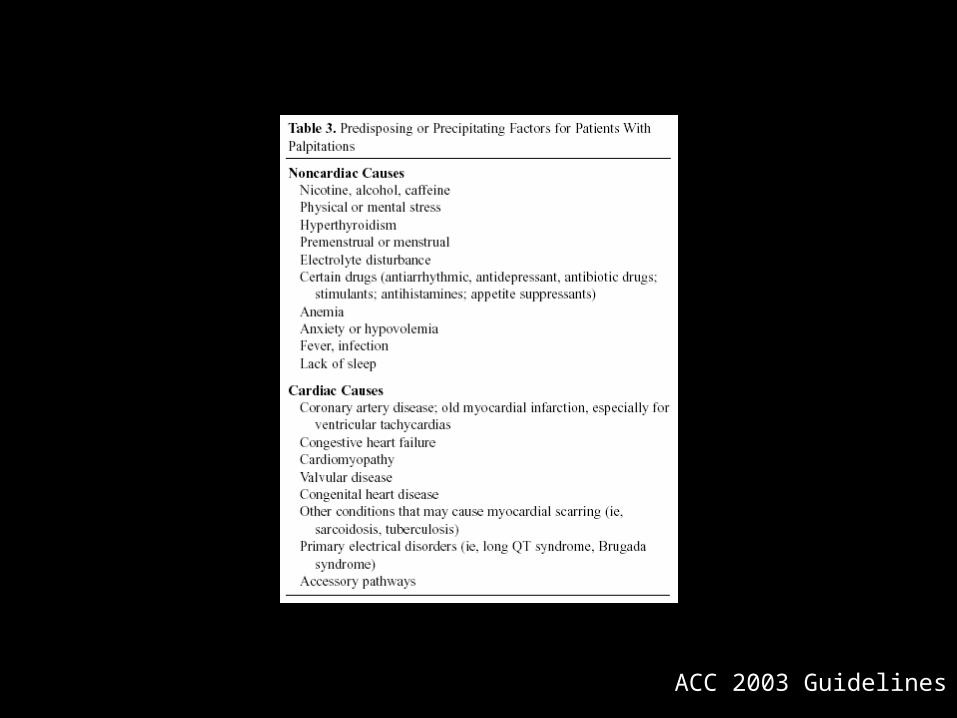
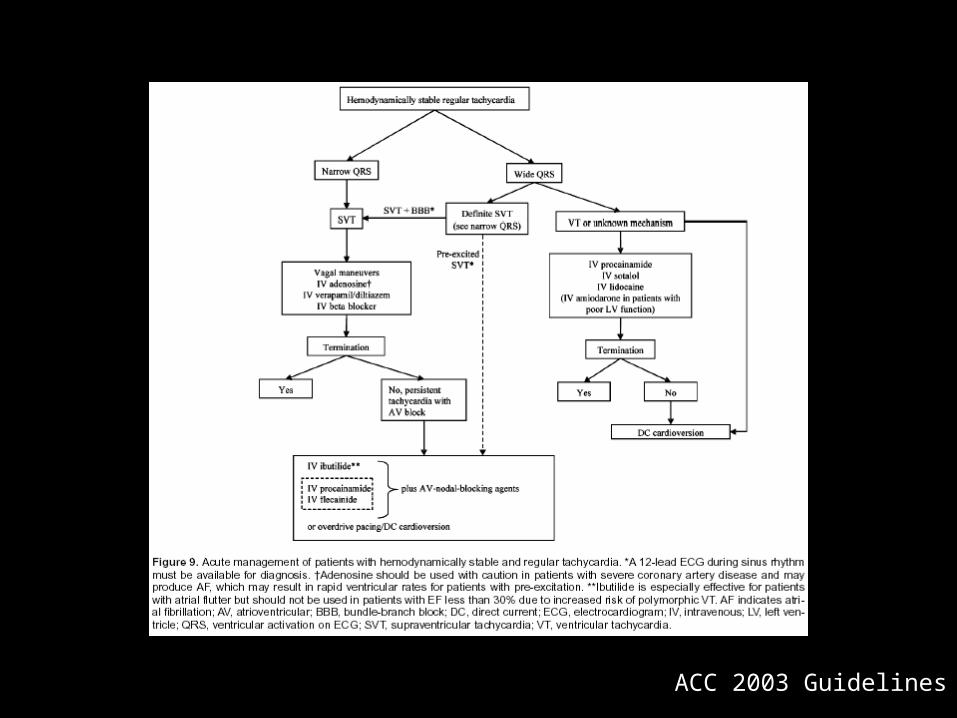
ACC 2003 Guidelines
ACC 2003 Guidelines
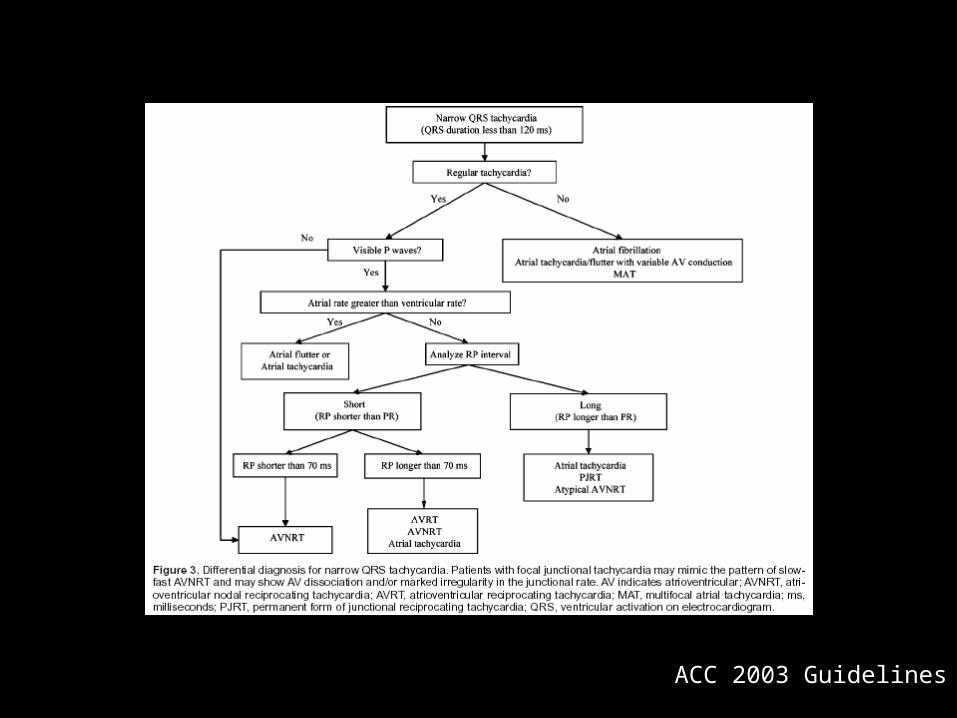
ACC 2003 Guidelines
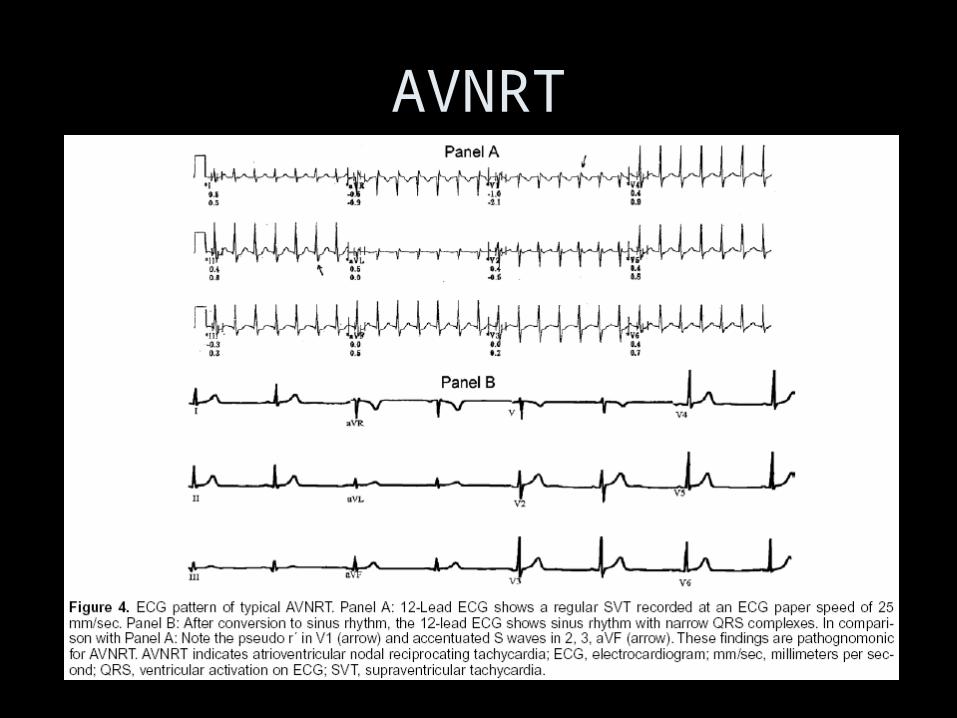
AVNRT
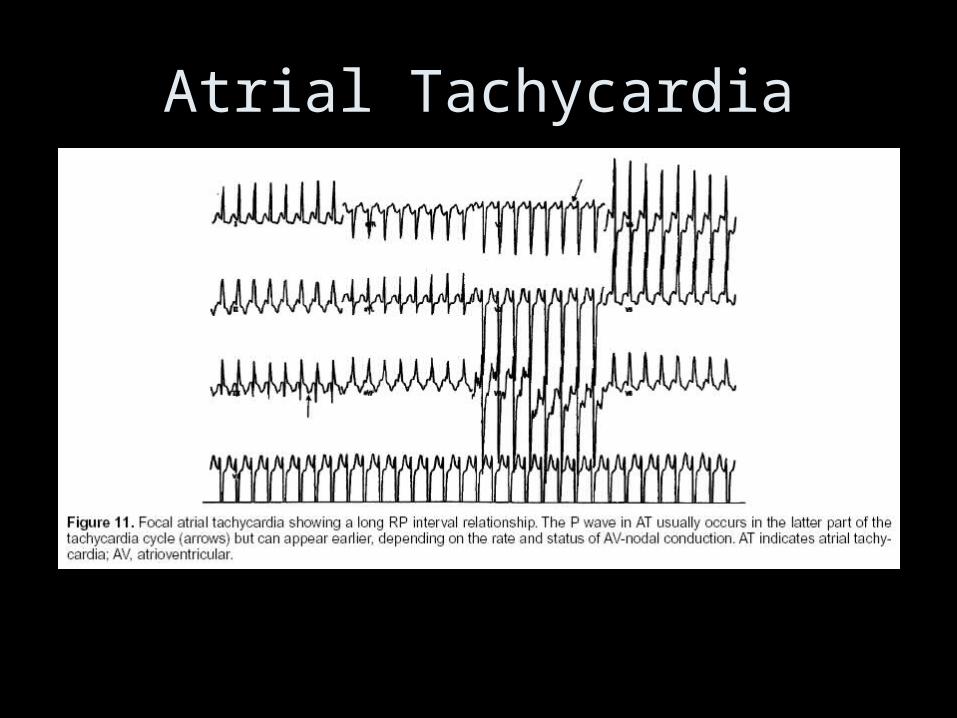
Atrial Tachycardia
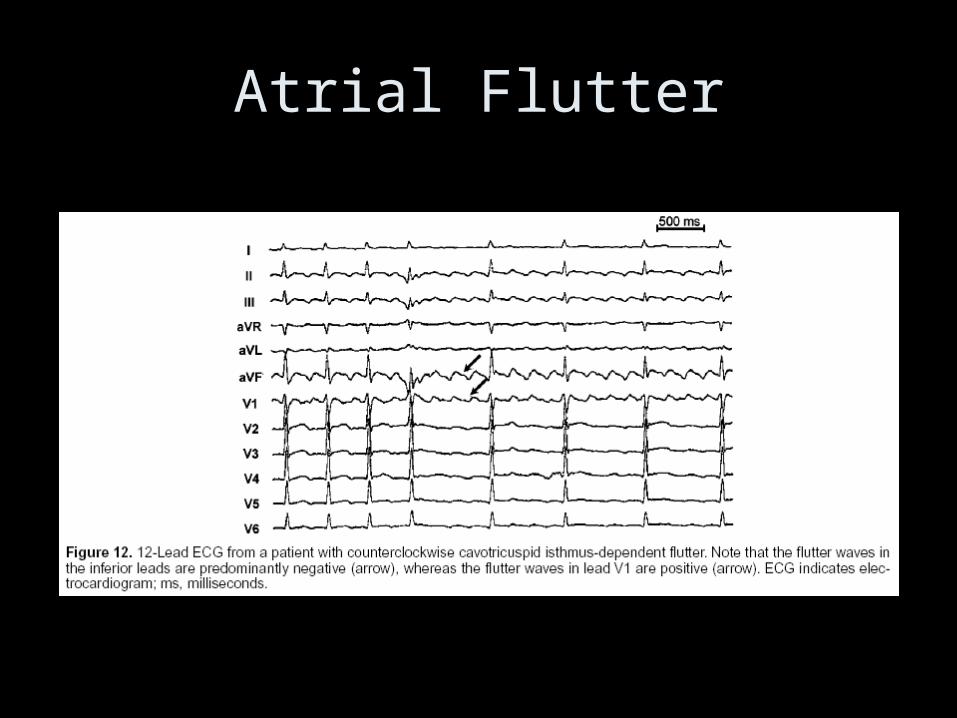
Atrial Flutter
ACC 2003 Guidelines
ACC 2003 Guidelines
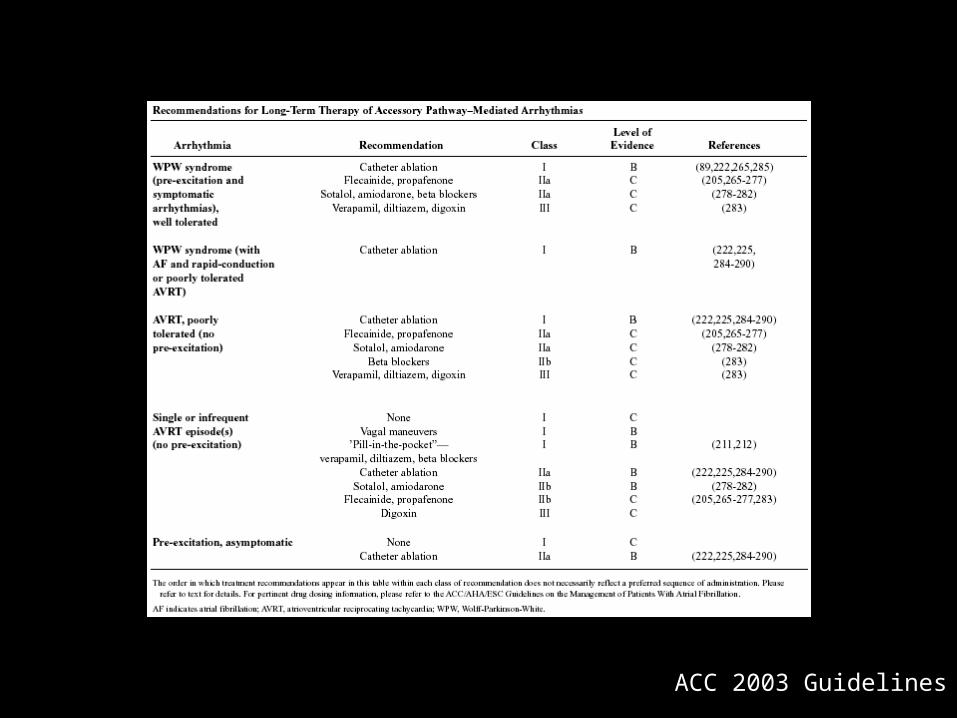
ACC 2003 Guidelines
Ventricular Arrhythmias

Epidemiology of VA & SCD
Classification of Ventricular Arrhythmia by Electrocardiography
•Nonsustained ventricular tachycardia (VT)♥ Monomorphic♥ Polymorphic
•Sustained VT♥ Monomorphic♥ Polymorphic
•Bundle-branch re-entrant tachycardia•Bidirectional VT•Torsades de pointes•Ventricular flutter•Ventricular fibrillation
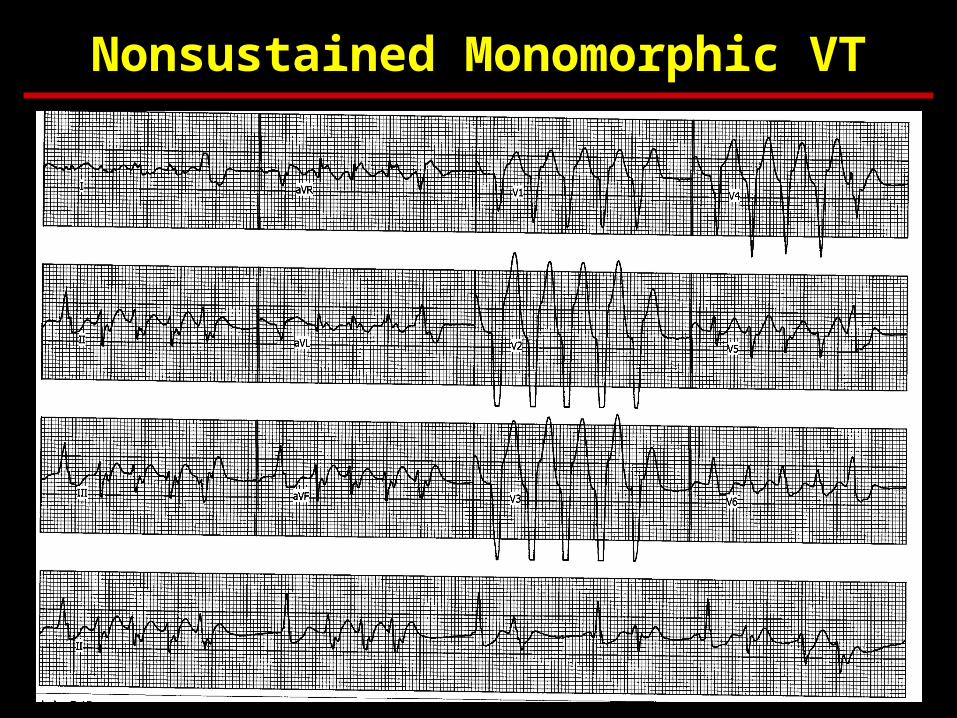
Nonsustained Monomorphic VT
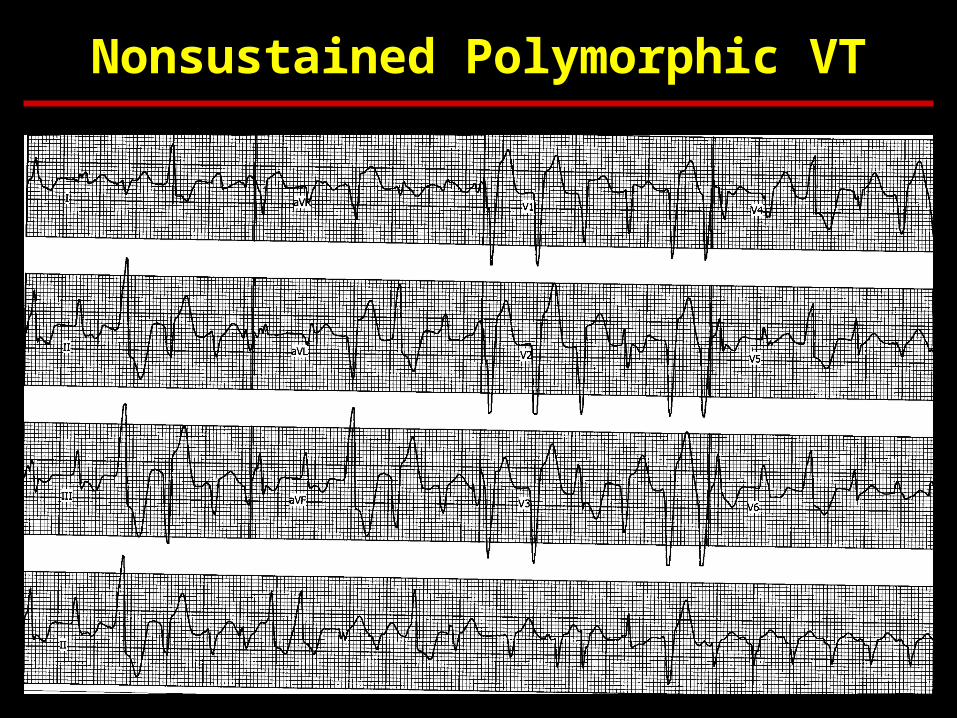
Nonsustained Polymorphic VT
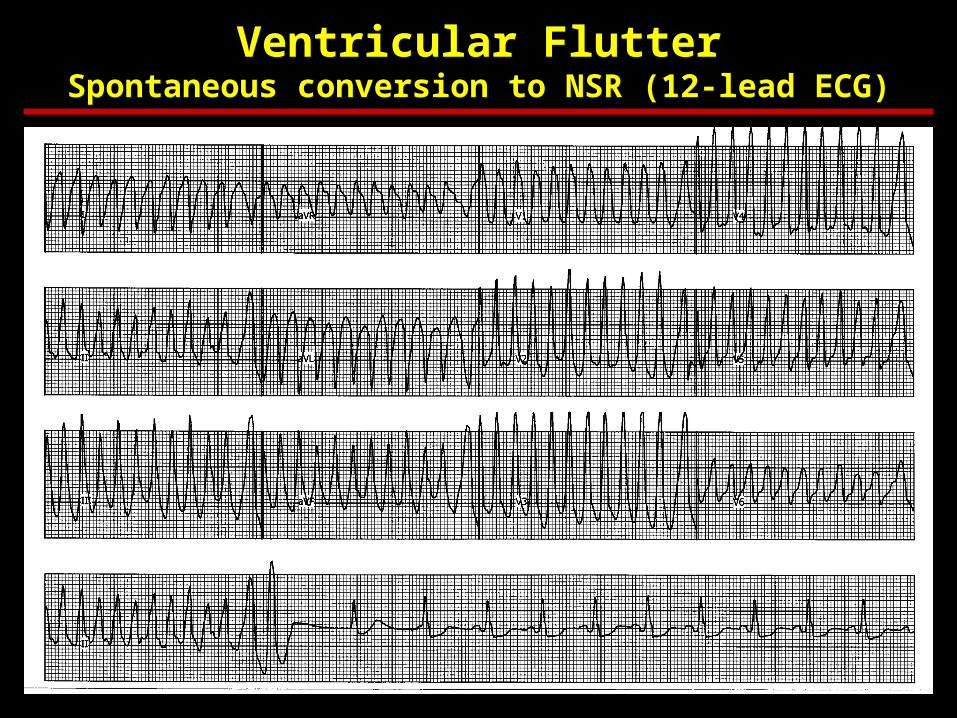
Ventricular FlutterSpontaneous conversion to NSR (12-lead ECG)
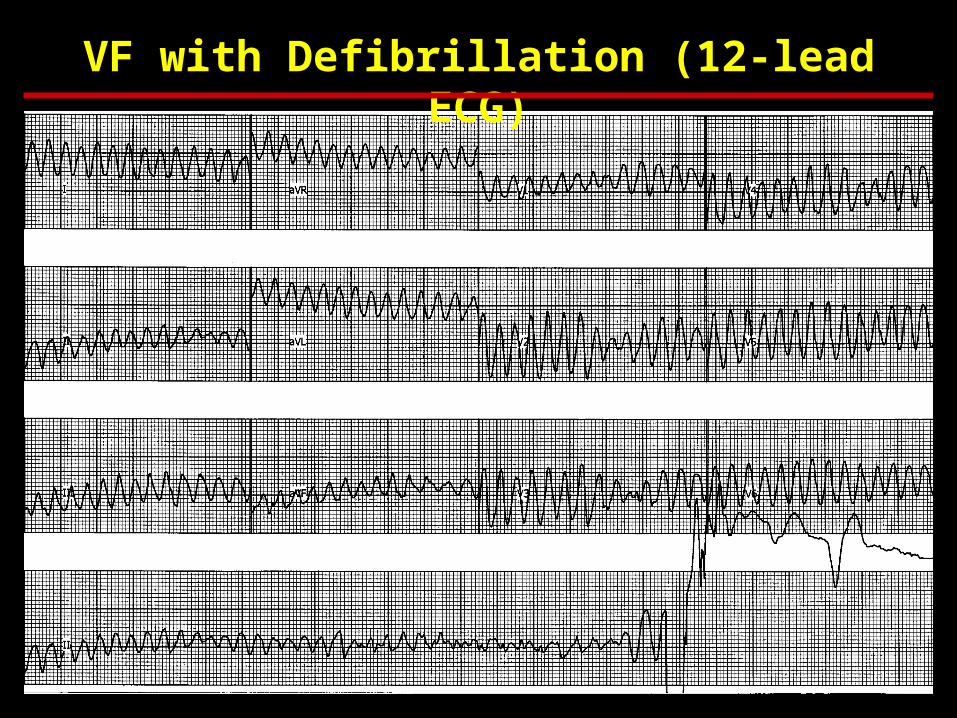
VF with Defibrillation (12-lead ECG)
Epidemiology of VA & SCD
Classification of Ventricular Arrhythmia by Clinical Presentation
•Hemodynamically stable ♥ Asymptomatic ♥ Minimal symptoms, e.g., palpitations•Hemodynamically unstable
♥ Presyncope♥ Syncope♥ Sudden cardiac death♥ Sudden cardiac arrest
Epidemiology of VA & SCD
Classification of Ventricular Arrhythmia by Disease Entity•Chronic coronary heart disease
•Heart failure•Congenital heart disease•Neurological disorders•Structurally normal hearts•Sudden infant death syndrome•Cardiomyopathies
♥ Dilated cardiomyopathy♥ Hypertrophic cardiomyopathy♥ Arrhythmogenic right ventricular (RV) cardiomyopathy
VA: Diagnosis
• Chemistry panel• Resting ECG• Ambulatory ECG
– Holter monitor, event monitor, or ILR
• Stress testing– Exercise or pharmacologic– ECG, echoc, or SPECT MPI
• Left ventricular function & imaging– TTE, LHC, CCT, or CMR
• Electrophysiologic testing
• Antiarrhythmic Drugs
• ♥ Beta Blockers: Effectively suppress ventricular ectopic beats & arrhythmias; reduce incidence of SCD
• ♥ Amiodarone: No definite survival benefit; some studies have shown reduction in SCD in patients with LV dysfunction especially when given in conjunction with BB. Has complex drug interactions and many adverse side effects (pulmonary, hepatic, thyroid, cutaneous)
• ♥ Sotalol: Suppresses ventricular arrhythmias; is more pro-arrhythmic than amiodarone, no survival benefit clearly shown
• ♥ Conclusions: Antiarrhythmic drugs (except for BB) should not be used as primary therapy of VA and the prevention of SCD
Therapies for VA
Non-antiarrhythmic Drugs
♥ Electrolytes: magnesium and potassium administration can favorably influence the electrical substrate involved in VA; are especially useful in setting of hypomagnesemia and hypokalemia
♥ ACE inhibitors, angiotensin receptor blockers and aldosterone blockers can improve the myocardial substrate through reverse remodeling and thus reduce incidence of SCD
♥ Antithrombotic and antiplatelet agents: may reduce SCD by reducing coronary thrombosis
♥ Statins: have been shown to reduce life-threatening VA in high-risk patients with electrical instability
♥ n-3 Fatty acids: have anti-arrhythmic properties, but conflicting data exist for the prevention of SCD
Therapies for VA
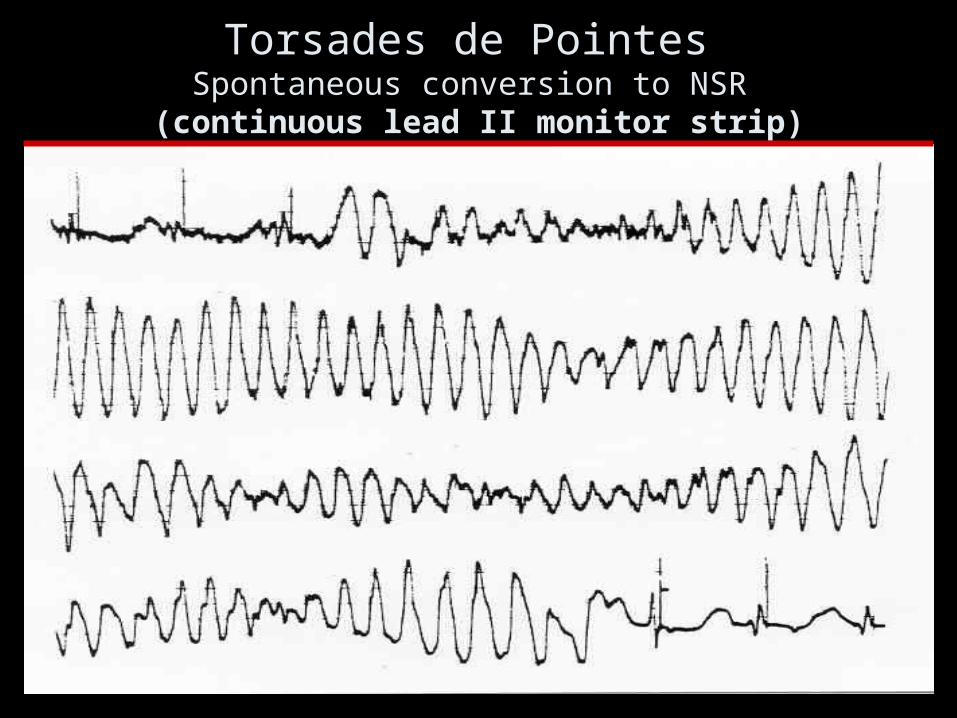
Torsades de Pointes Spontaneous conversion to NSR
(continuous lead II monitor strip)
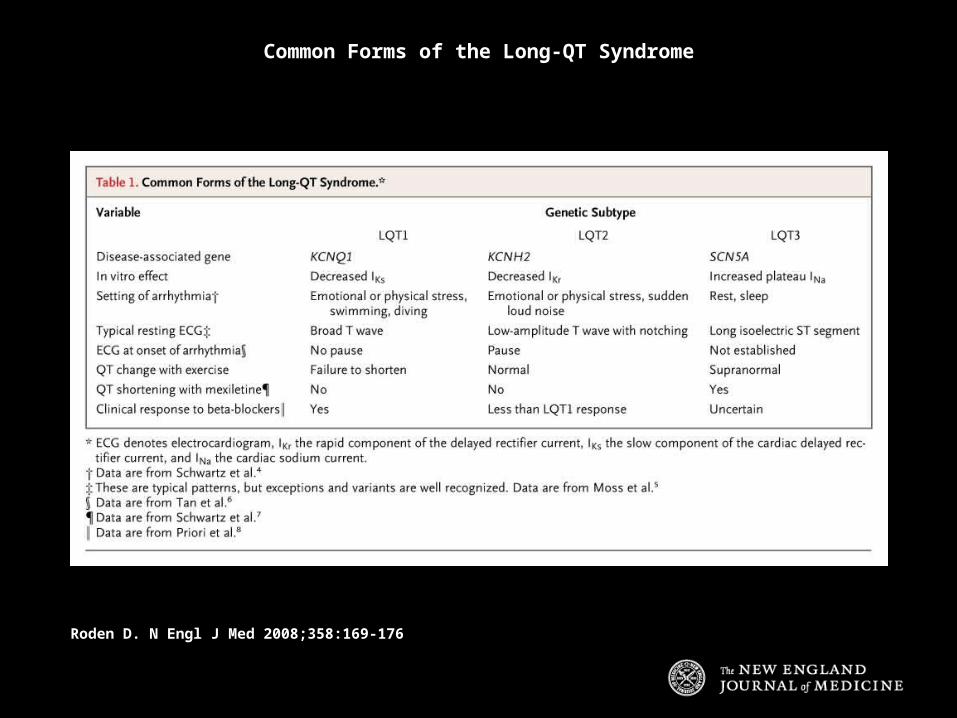
Common Forms of the Long-QT Syndrome
Roden D. N Engl J Med 2008;358:169-176
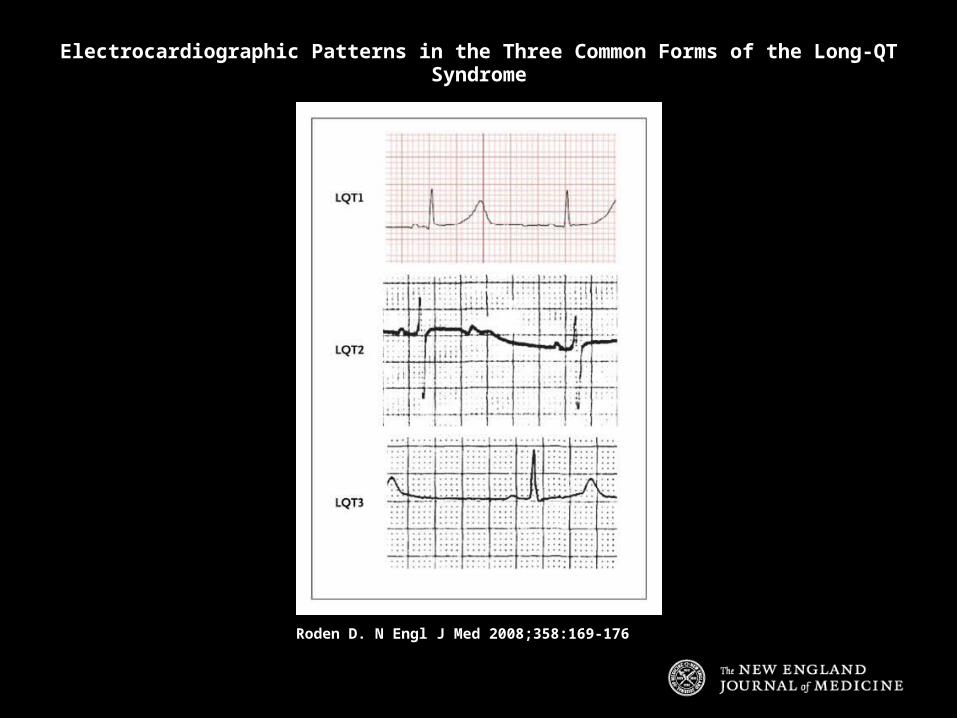
Electrocardiographic Patterns in the Three Common Forms of the Long-QT Syndrome
Roden D. N Engl J Med 2008;358:169-176
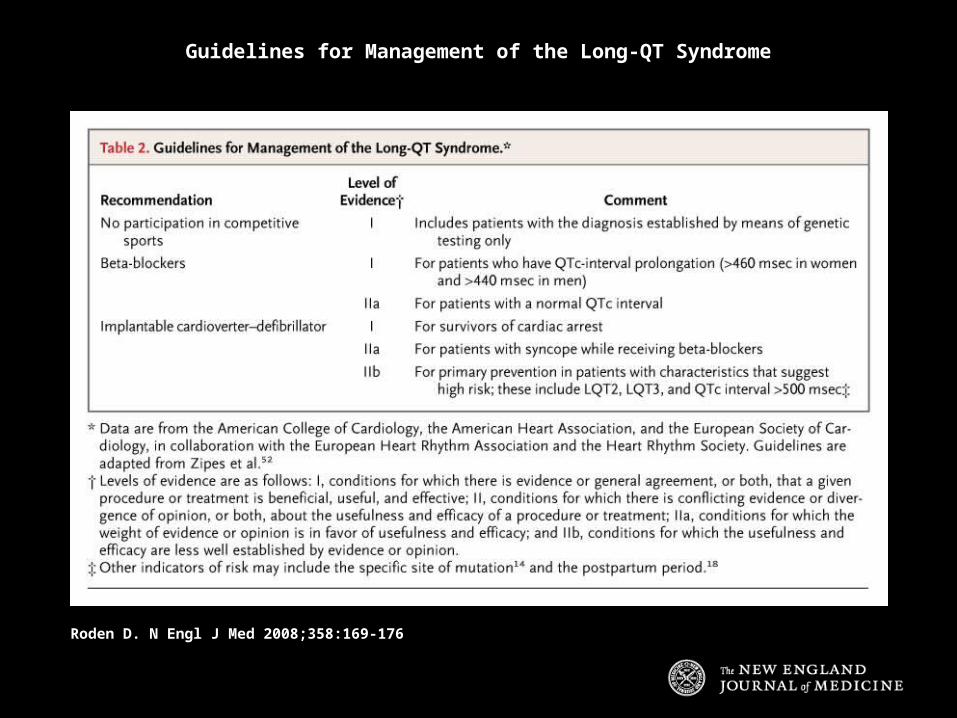
Guidelines for Management of the Long-QT Syndrome
Roden D. N Engl J Med 2008;358:169-176
Roden D. N Engl J Med 2004;350:1013-1022
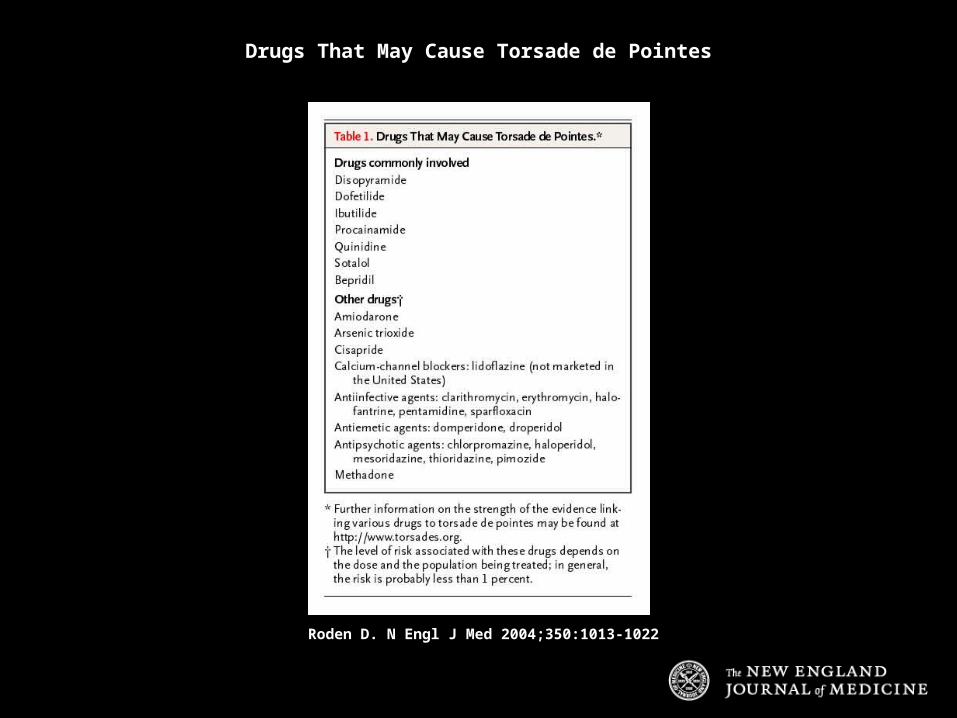
Drugs That May Cause Torsade de Pointes
Roden D. N Engl J Med 2004;350:1013-1022
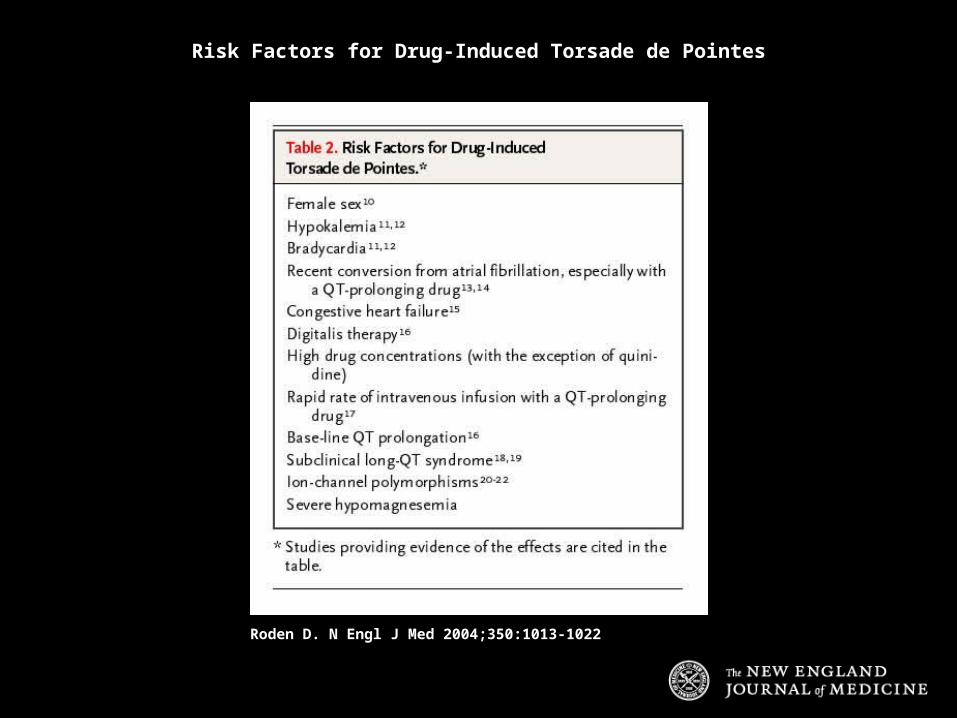
Risk Factors for Drug-Induced Torsade de Pointes
Syncope

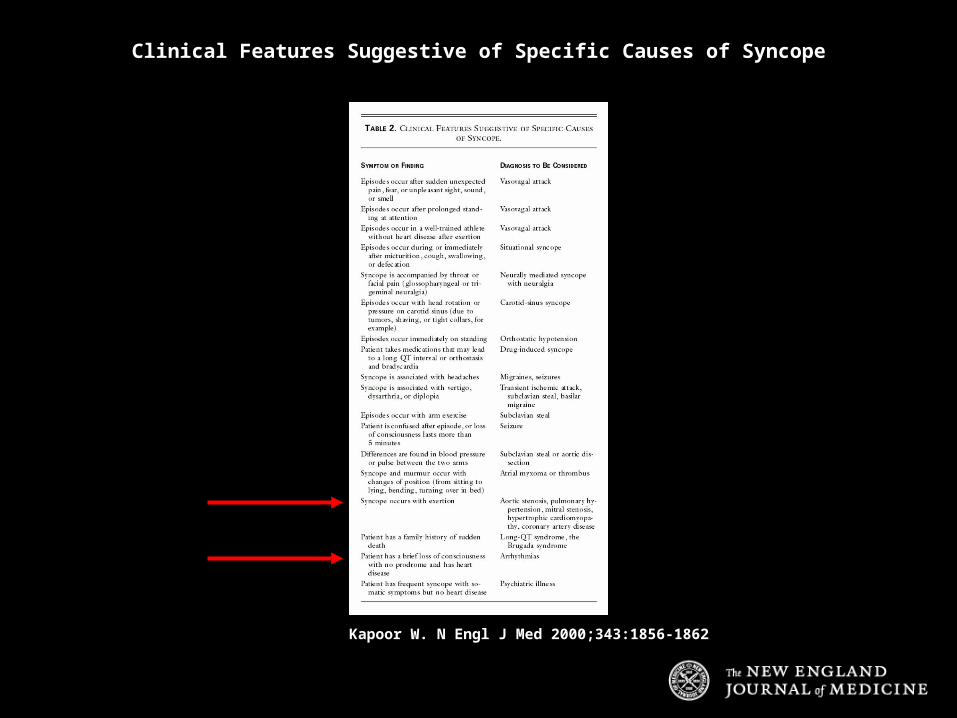
Kapoor W. N Engl J Med 2000;343:1856-1862
Causes of Syncope
Kapoor W. N Engl J Med 2000;343:1856-1862
Clinical Features Suggestive of Specific Causes of Syncope
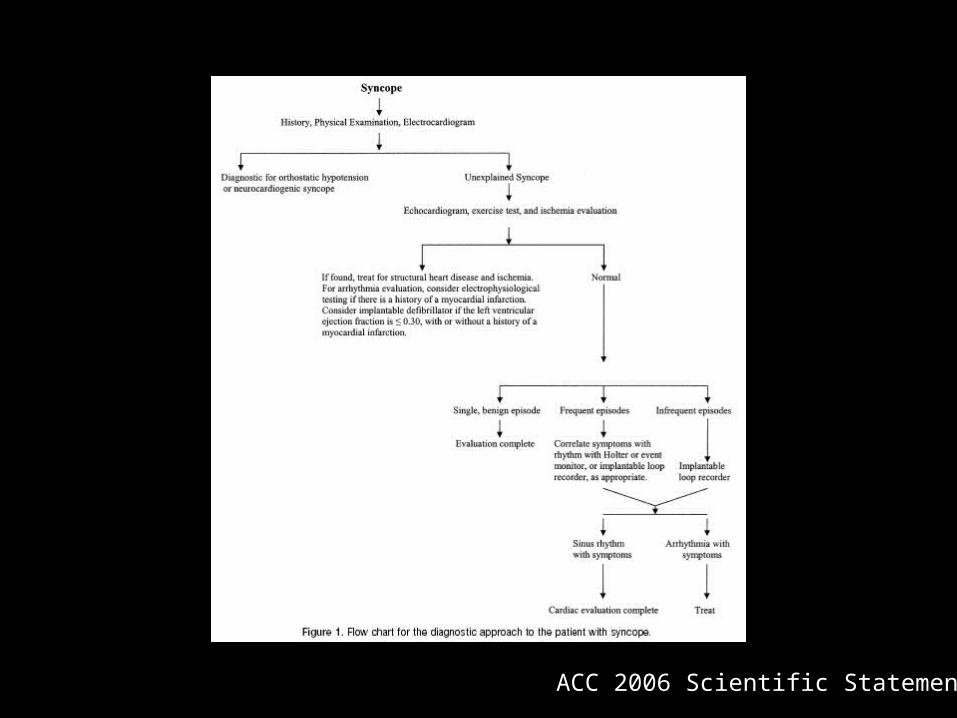
ACC 2006 Scientific Statement
Bradyarrhythmias
Mangrum J and DiMarco J. N Engl J Med 2000;342:703-709
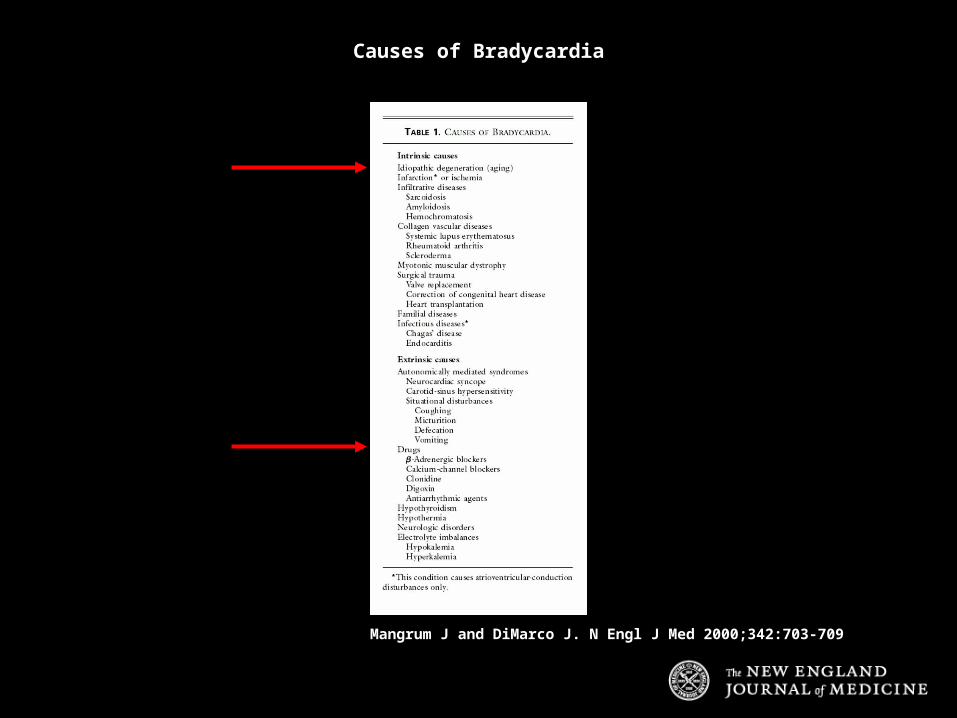
Causes of Bradycardia

Mangrum J and DiMarco J. N Engl J Med 2000;342:703-709
Electrocardiographic Findings Associated with Sinus-Node Dysfunction
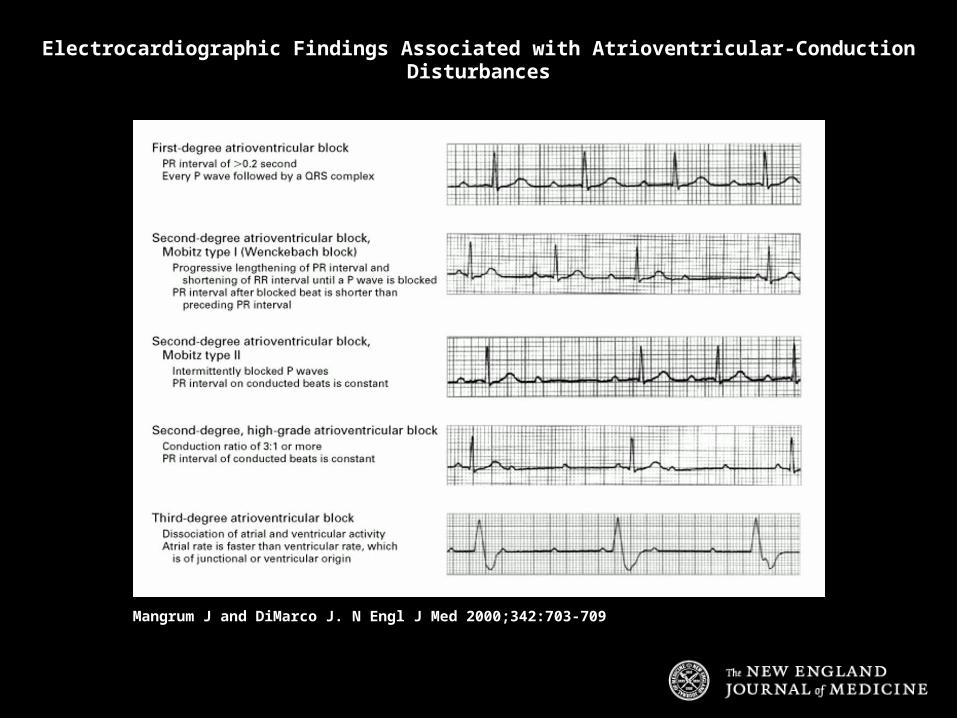
Mangrum J and DiMarco J. N Engl J Med 2000;342:703-709
Electrocardiographic Findings Associated with Atrioventricular-Conduction Disturbances
Devices
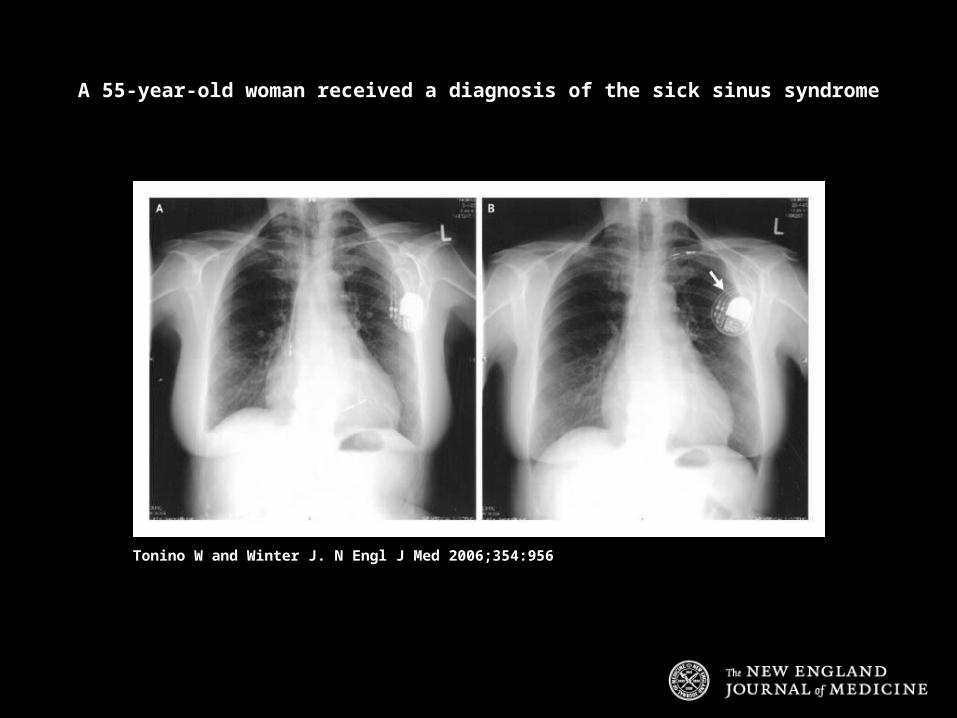
Tonino W and Winter J. N Engl J Med 2006;354:956
A 55-year-old woman received a diagnosis of the sick sinus syndrome

PPM: Indications
ACC 2008 Guidelines
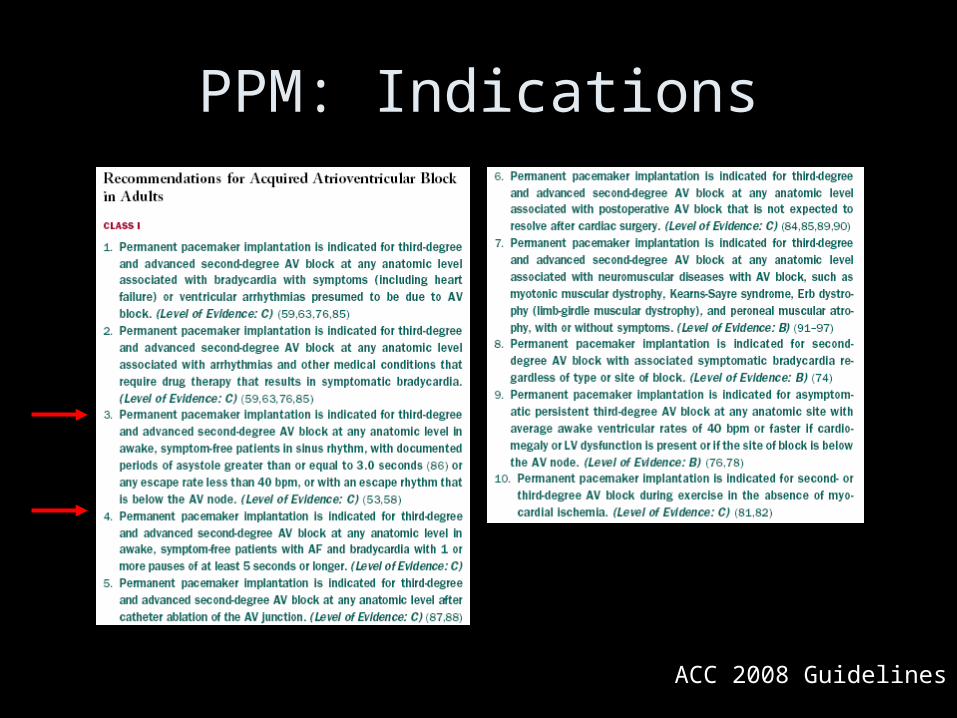
PPM: Indications
ACC 2008 Guidelines
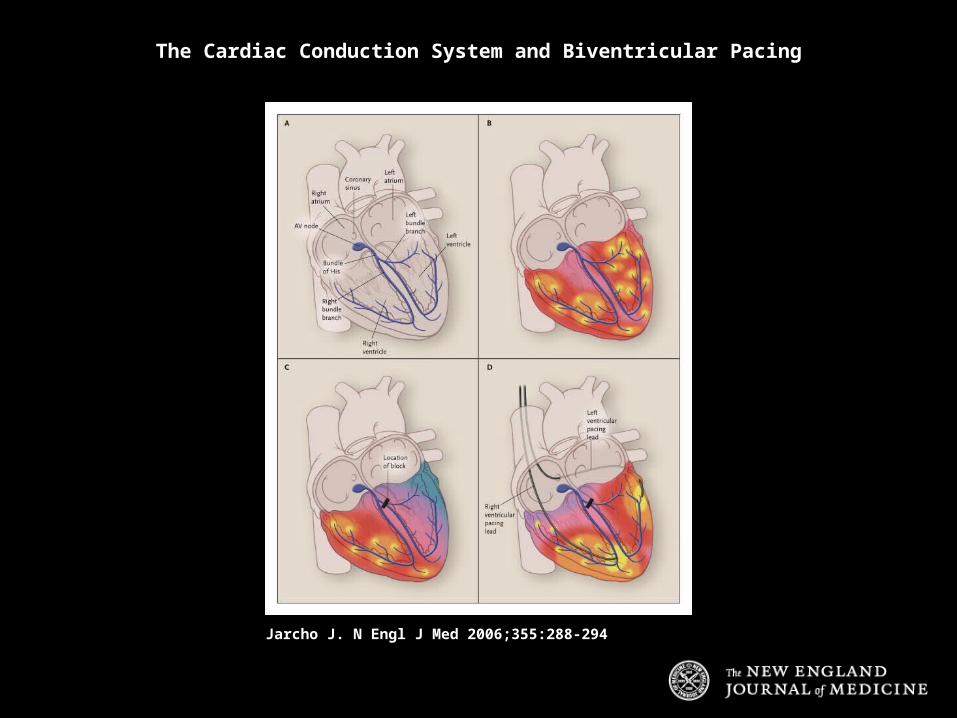
Jarcho J. N Engl J Med 2006;355:288-294
The Cardiac Conduction System and Biventricular Pacing
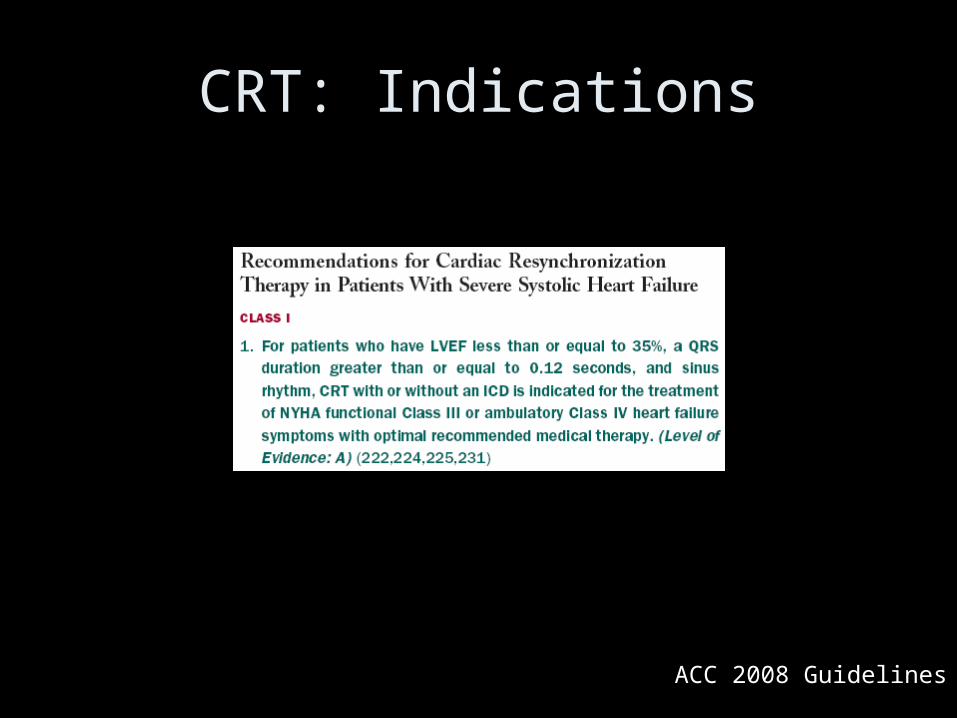
CRT: Indications
ACC 2008 Guidelines

DiMarco J. N Engl J Med 2003;349:1836-1847
Diagram of a Single-Chamber Implantable Cardioverter-Defibrillator System

ICD: Indications
ACC 2008 Guidelines
Heart Failure
ACC 2005 Guidelines
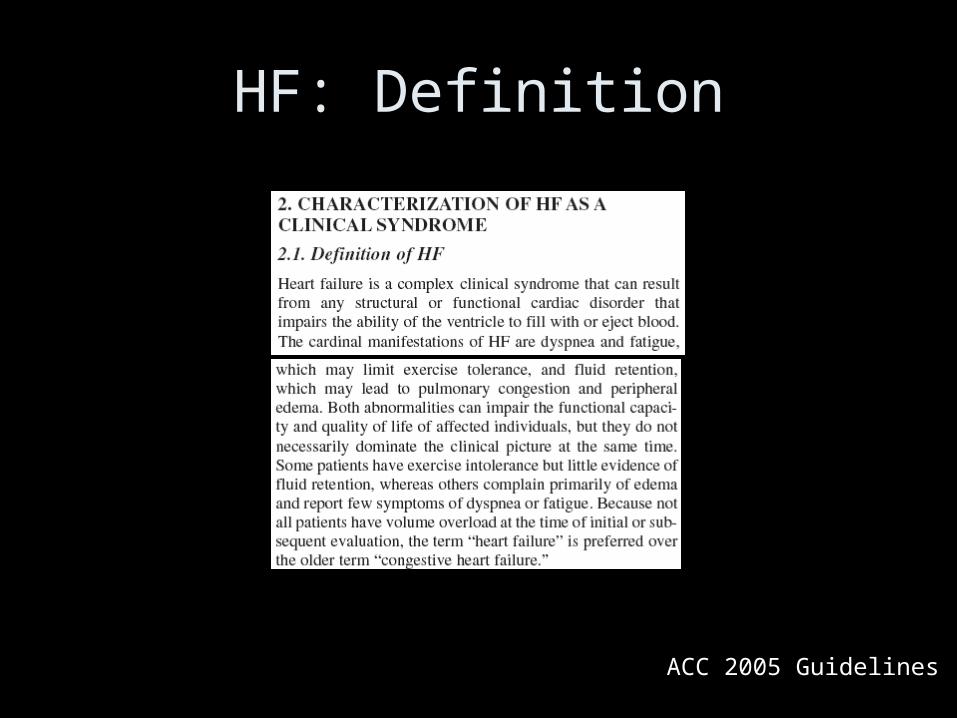
HF: Definition

ACC 2005 Guidelines
HF: Staging System
ACC 2005 Guidelines
ACC 2009 Focused Update
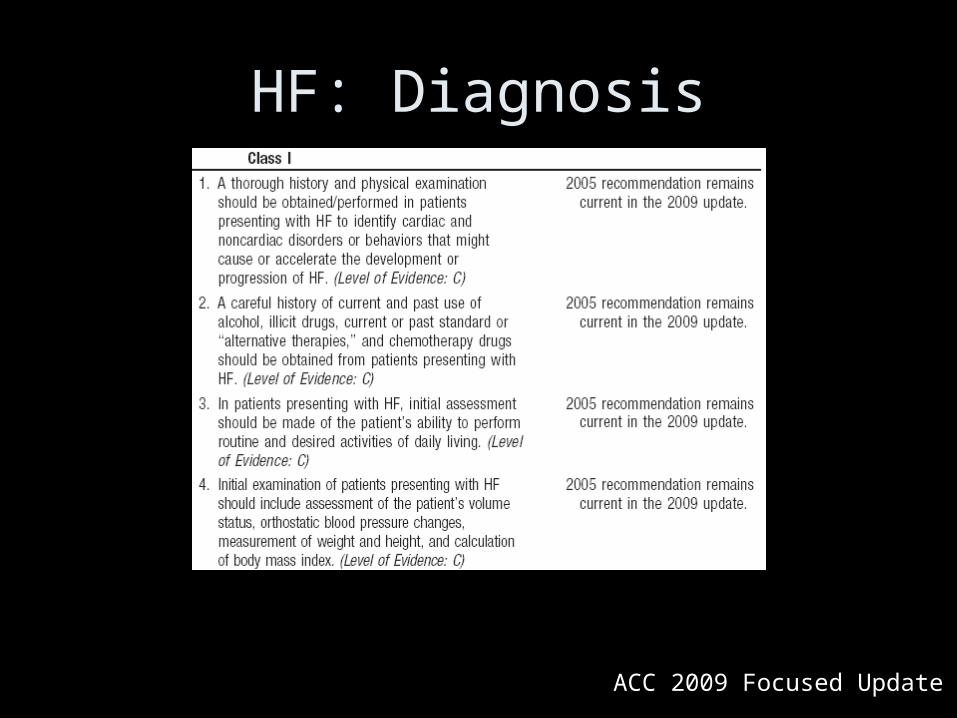
HF: Diagnosis
ACC 2009 Focused Update
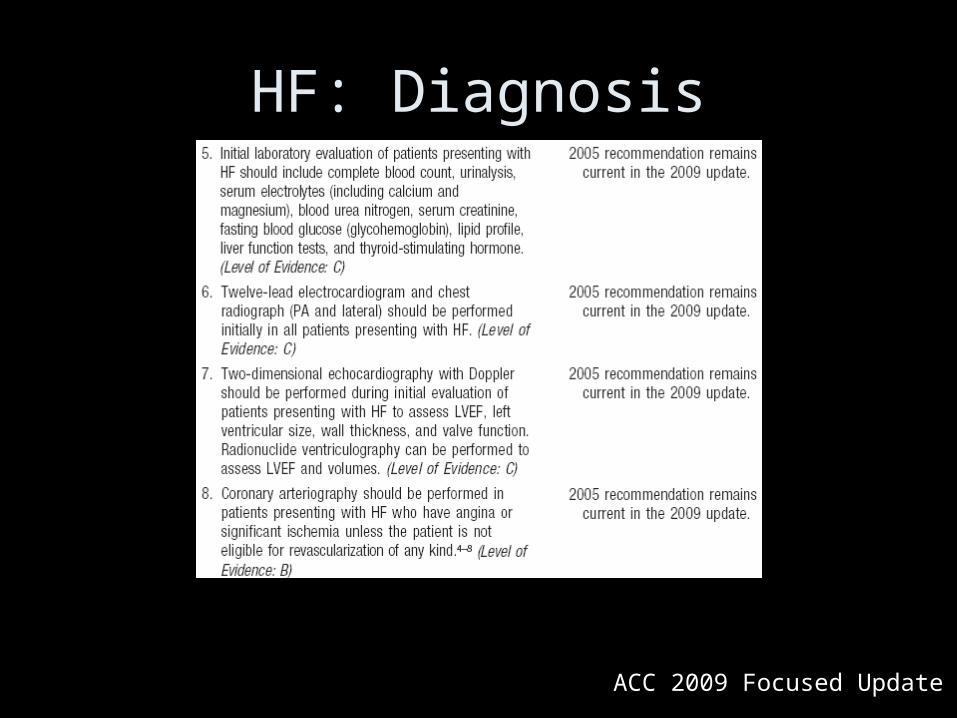
HF: Diagnosis
ACC 2005 Guidelines
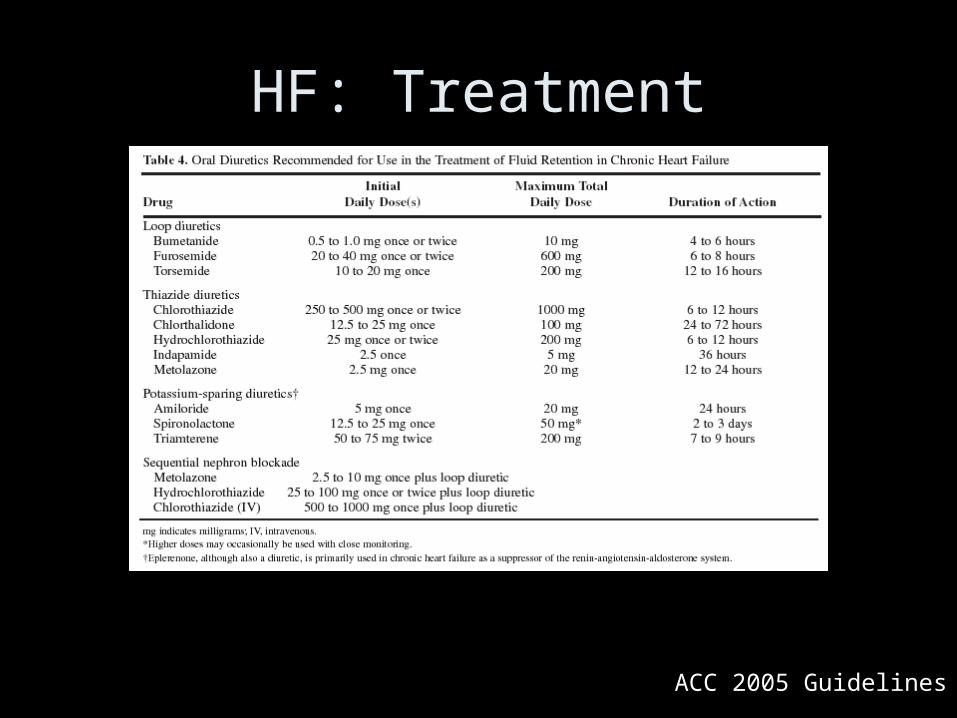
HF: Treatment

ACC 2005 Guidelines
HF: Treatment
ACC 2005 Guidelines
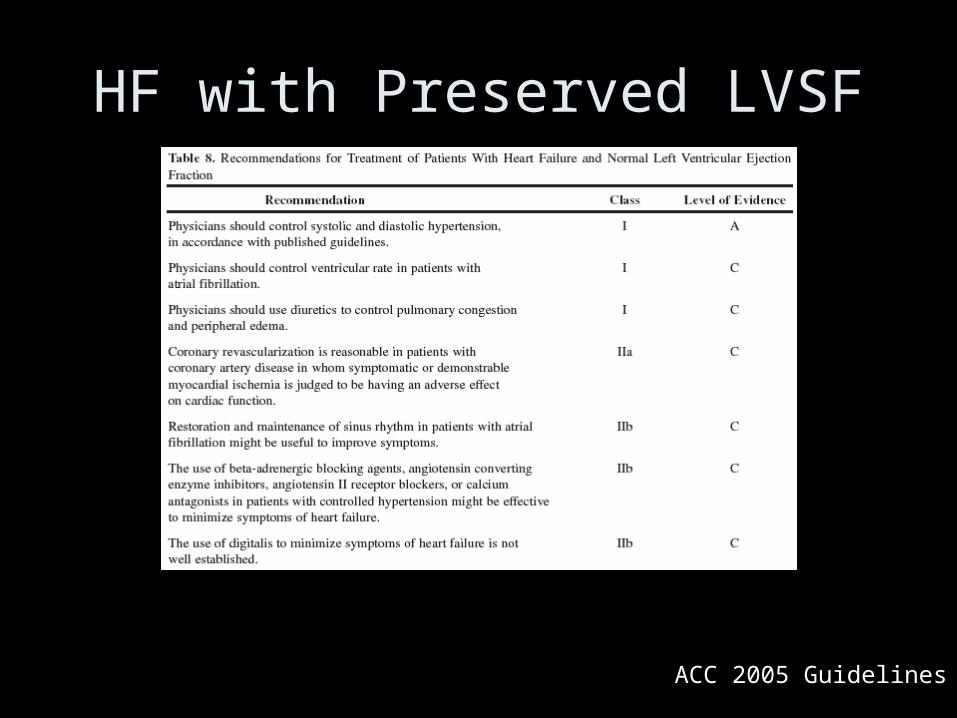
HF with Preserved LVSF
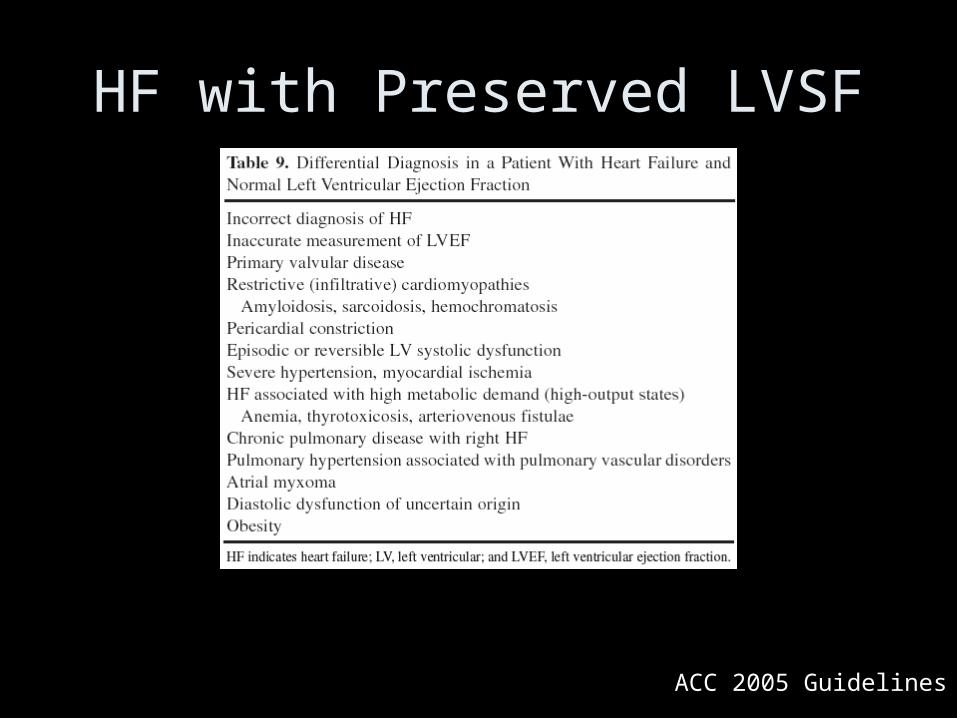
ACC 2005 Guidelines
HF with Preserved LVSF
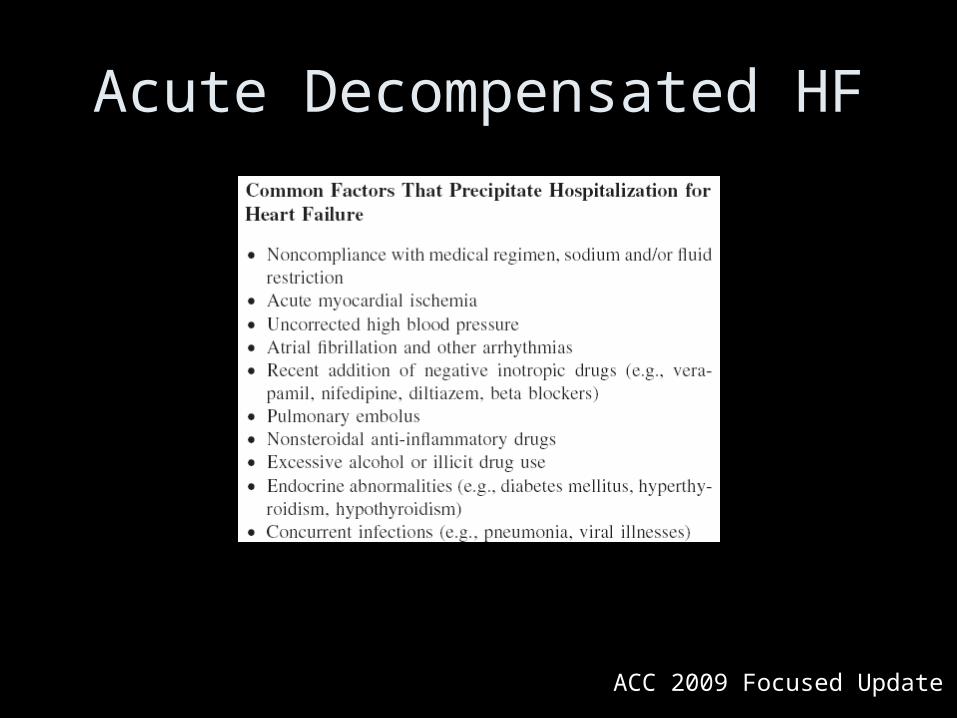
ACC 2009 Focused Update
Acute Decompensated HF
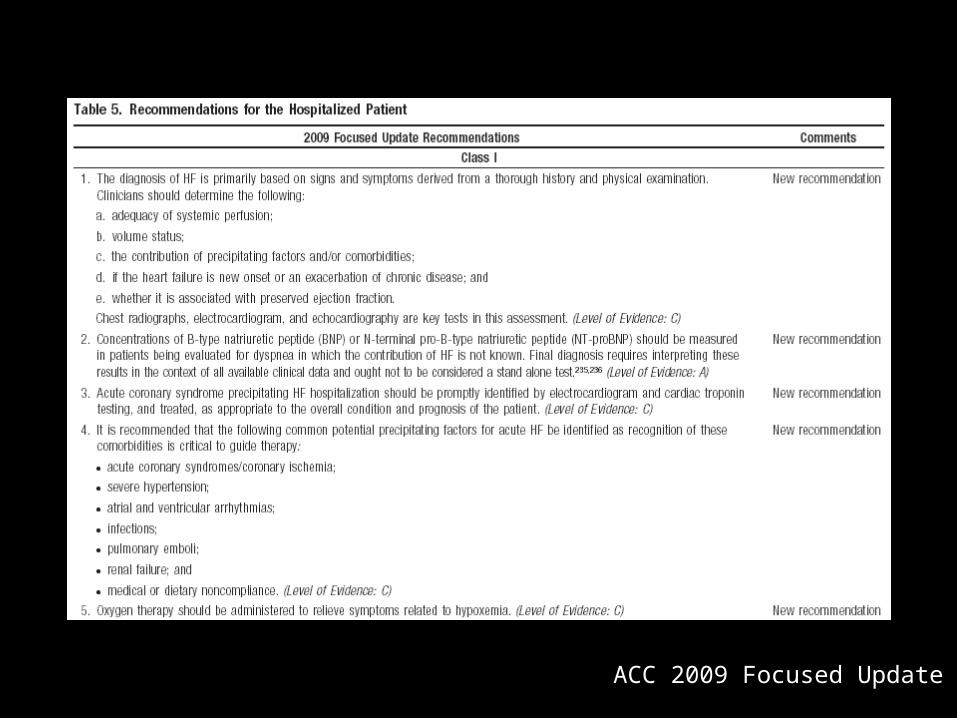
ACC 2009 Focused Update
ACC 2009 Focused Update
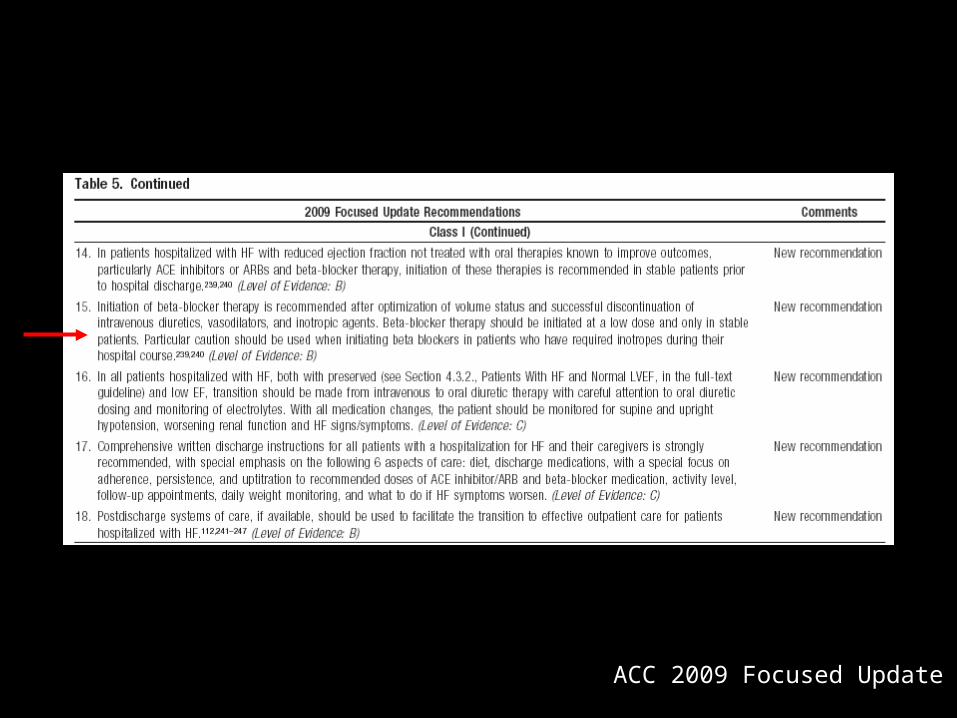
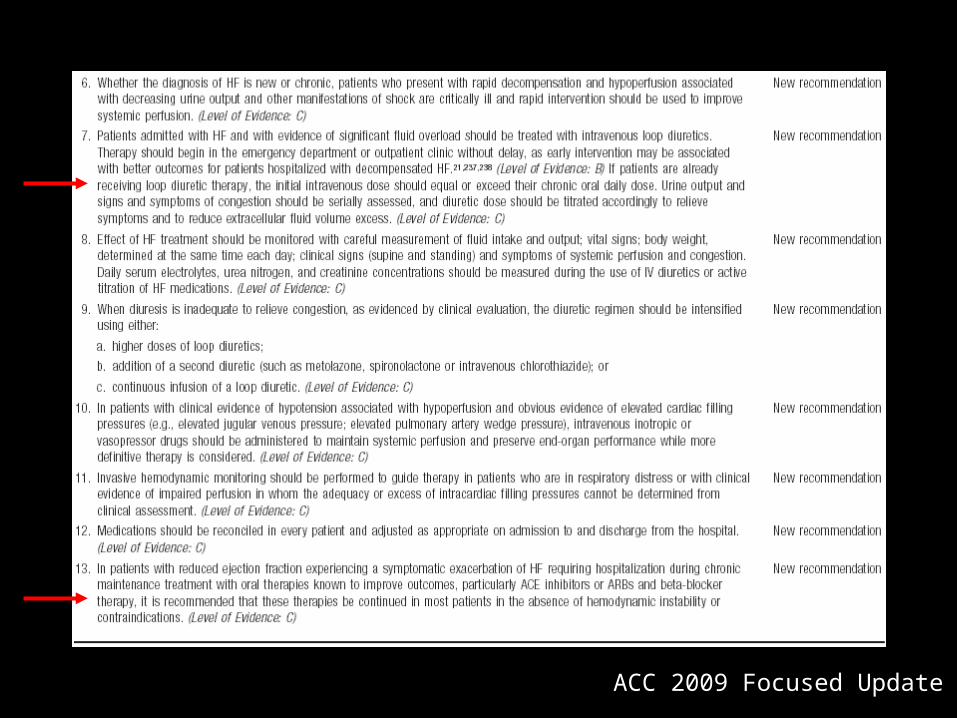
ACC 2009 Focused Update
Pericardial Disease
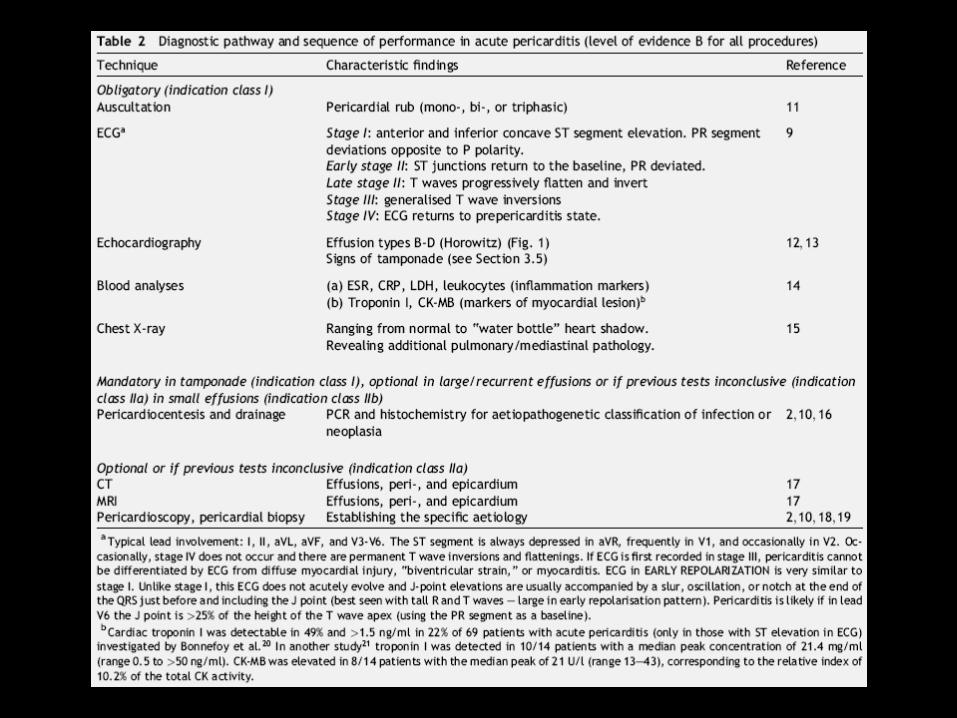
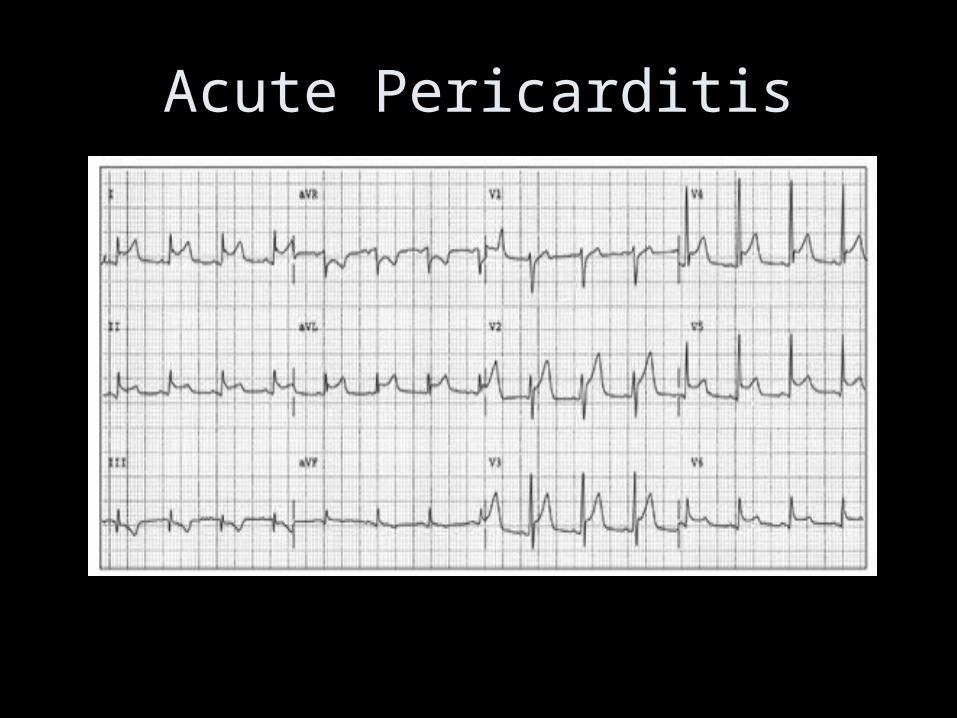
Acute Pericarditis
Lange R and Hillis L. N Engl J Med 2004;351:2195-2202
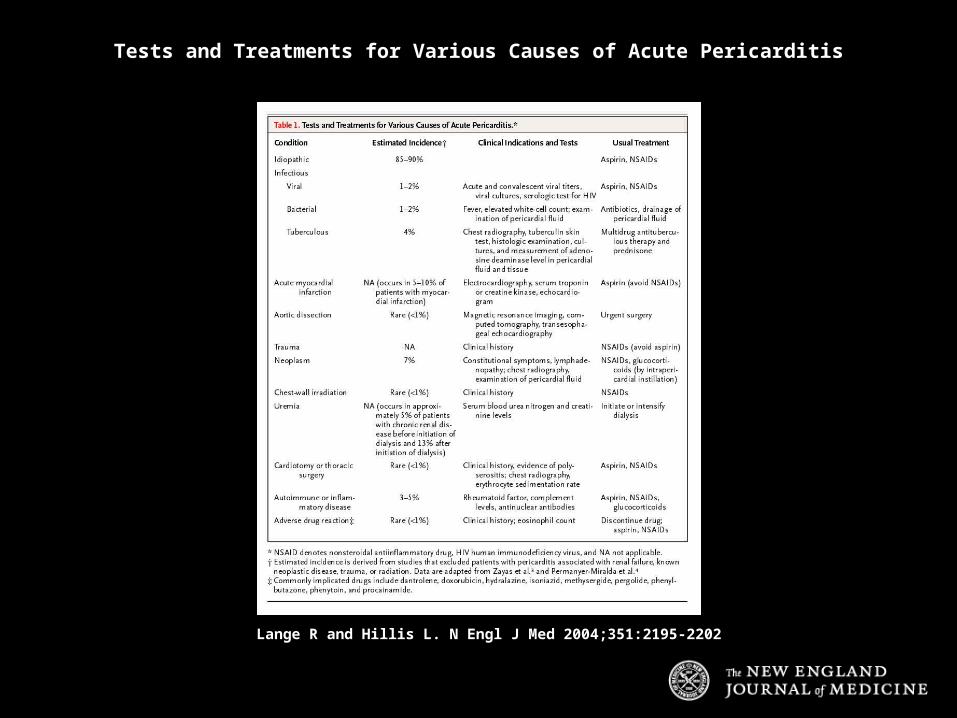
Tests and Treatments for Various Causes of Acute Pericarditis


Lange R and Hillis L. N Engl J Med 2004;351:2195-2202
Large Pericardial Effusion
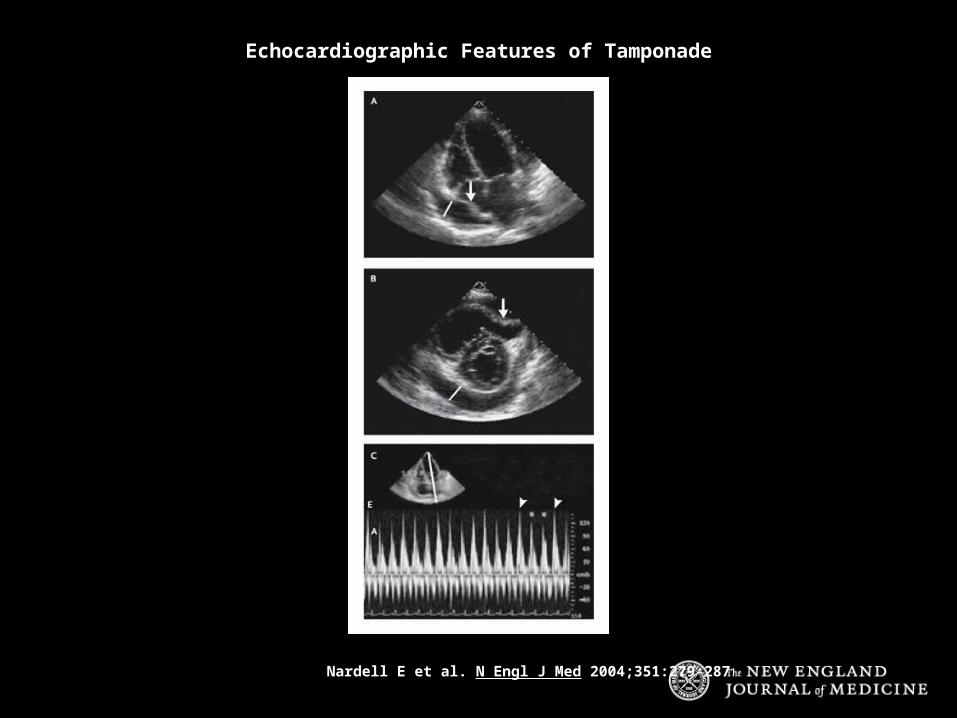
Nardell E et al. N Engl J Med 2004;351:279-287
Echocardiographic Features of Tamponade

Yurchak P and Deshpande V. N Engl J Med 2003;348:243-249
Simultaneous Left (Yellow) and Right (Green) Ventricular Pressure TracingsShowing the Square-Root Sign
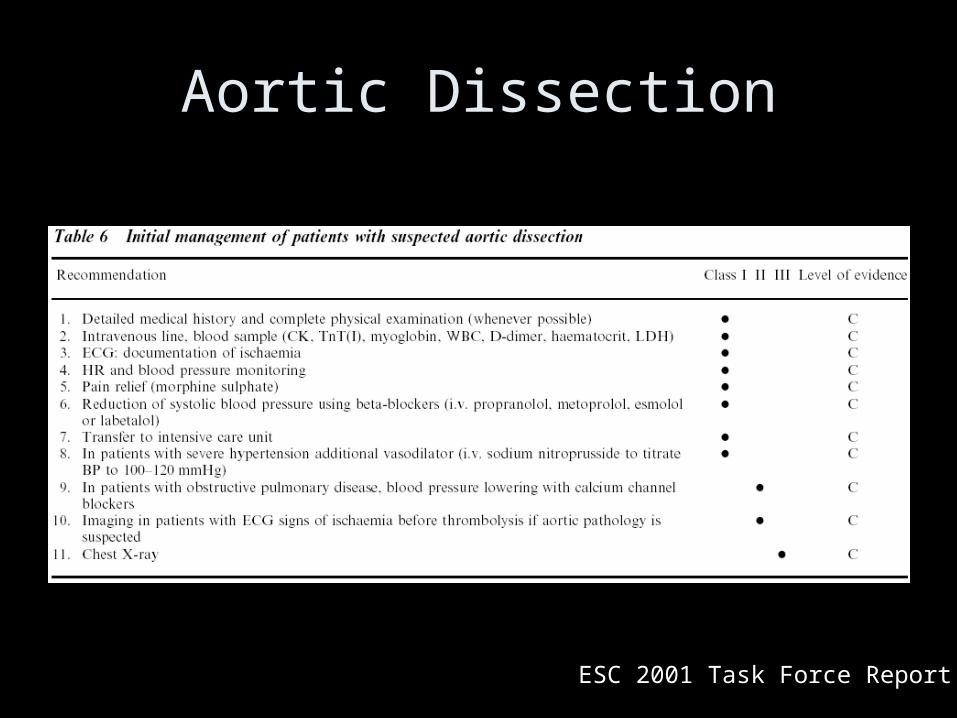
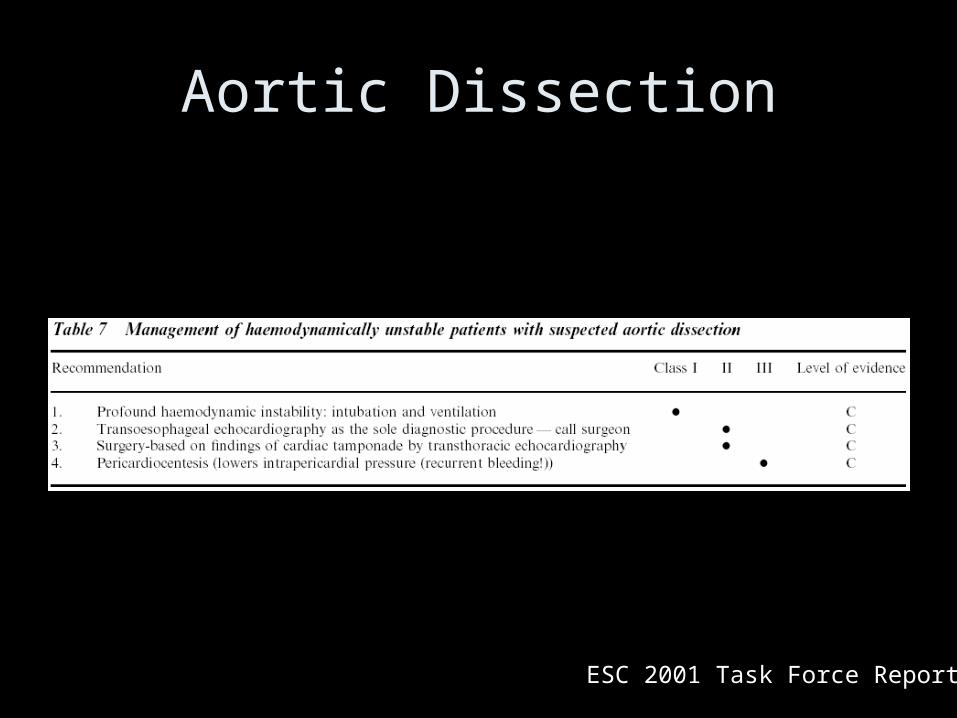
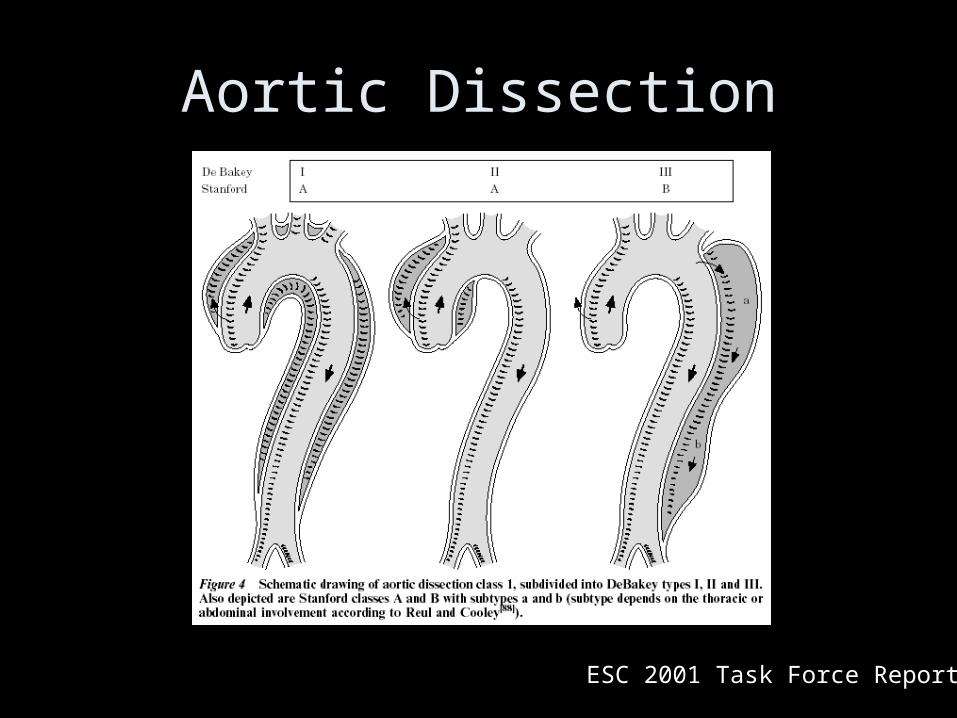
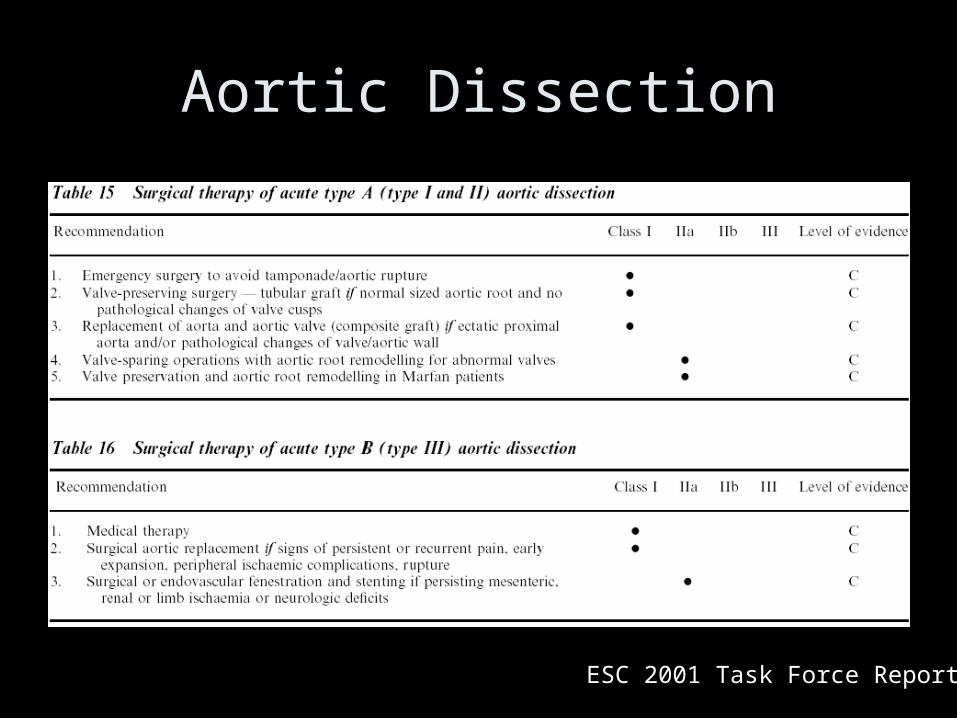
Aortic Disease
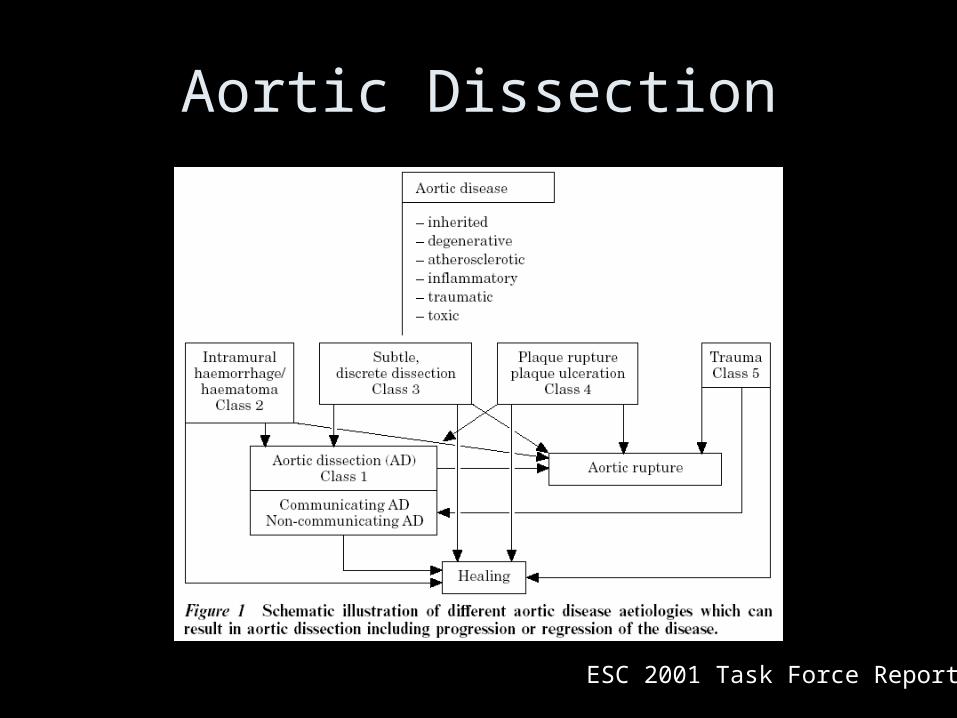
Aortic Dissection
ESC 2001 Task Force Report
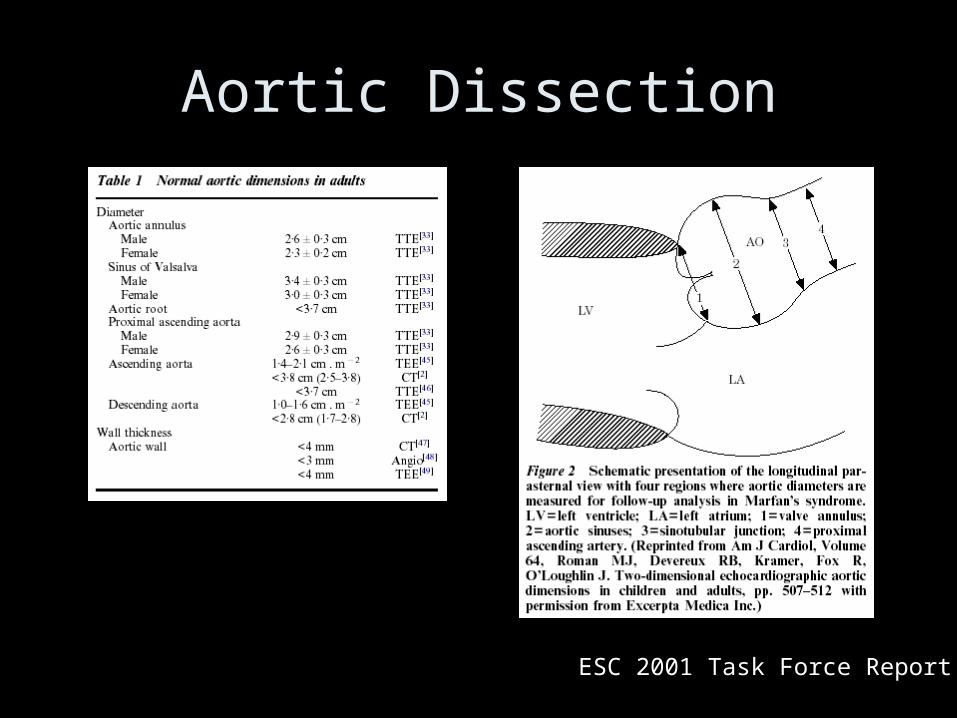
Aortic Dissection
ESC 2001 Task Force Report
ESC 2001 Task Force Report
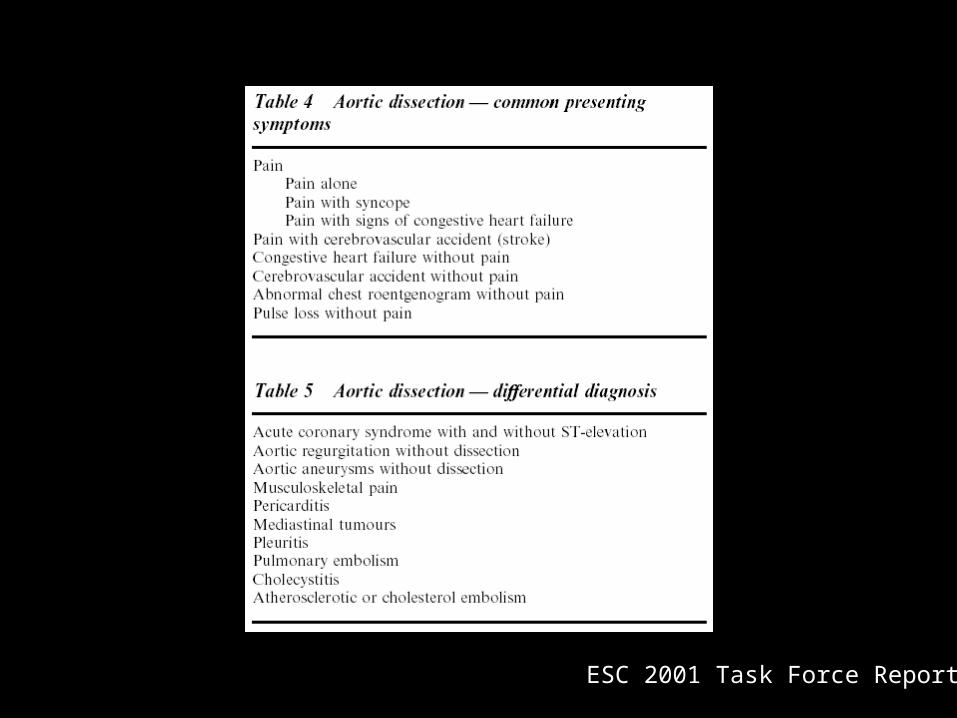
Aortic Dissection
ESC 2001 Task Force Report
Aortic Dissection
ESC 2001 Task Force Report
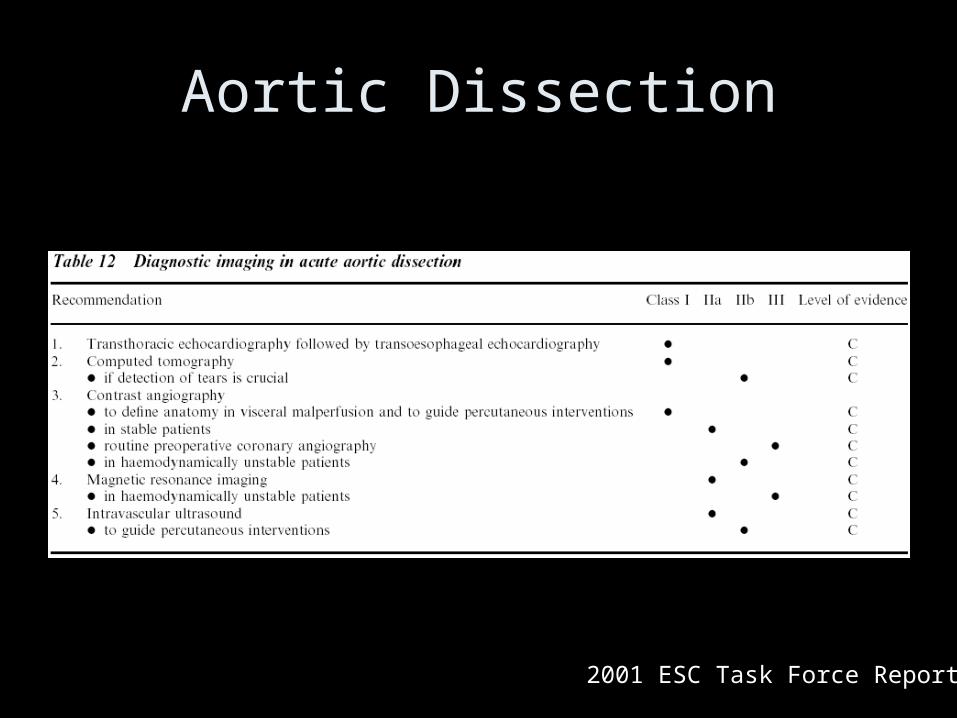
Aortic Dissection
2001 ESC Task Force Report
Aortic Dissection
ESC 2001 Task Force Report
Aortic Dissection
ESC 2001 Task Force Report
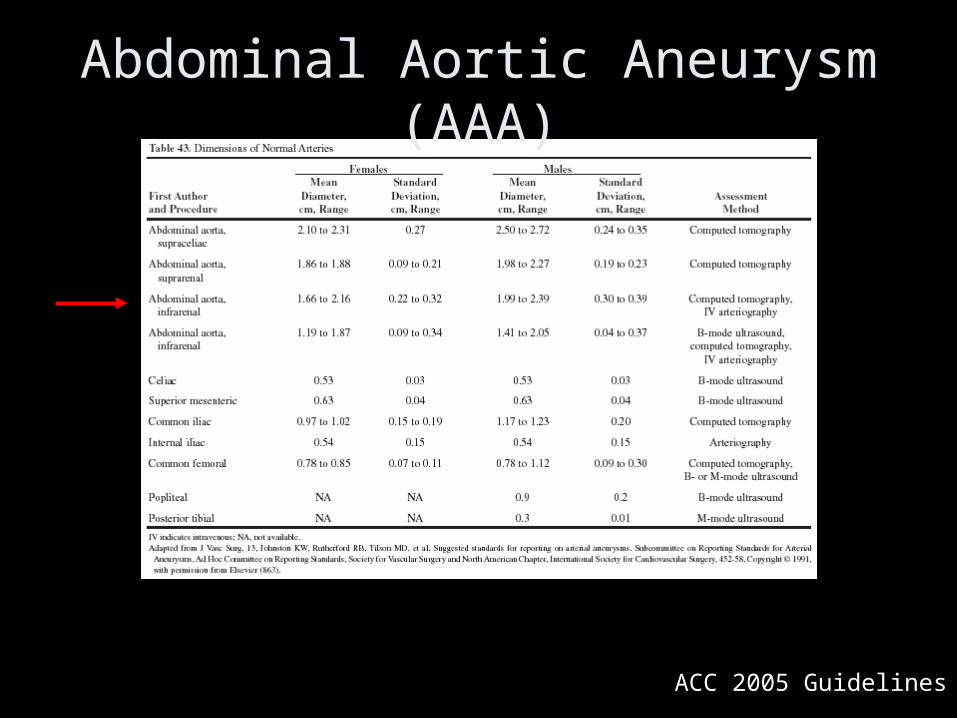
ACC 2005 Guidelines
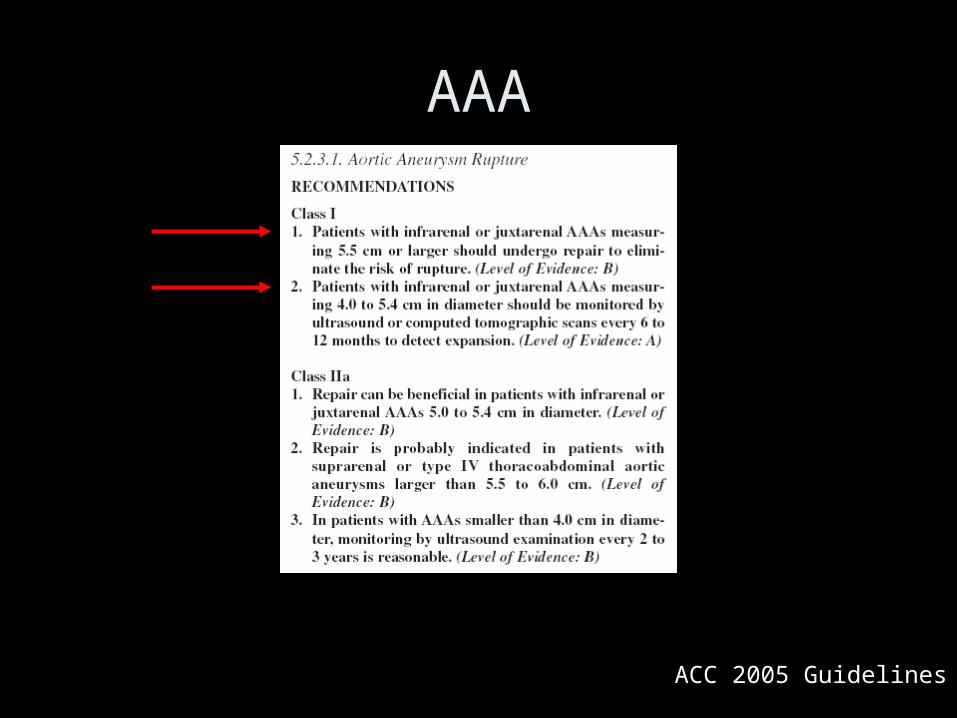
Abdominal Aortic Aneurysm (AAA)
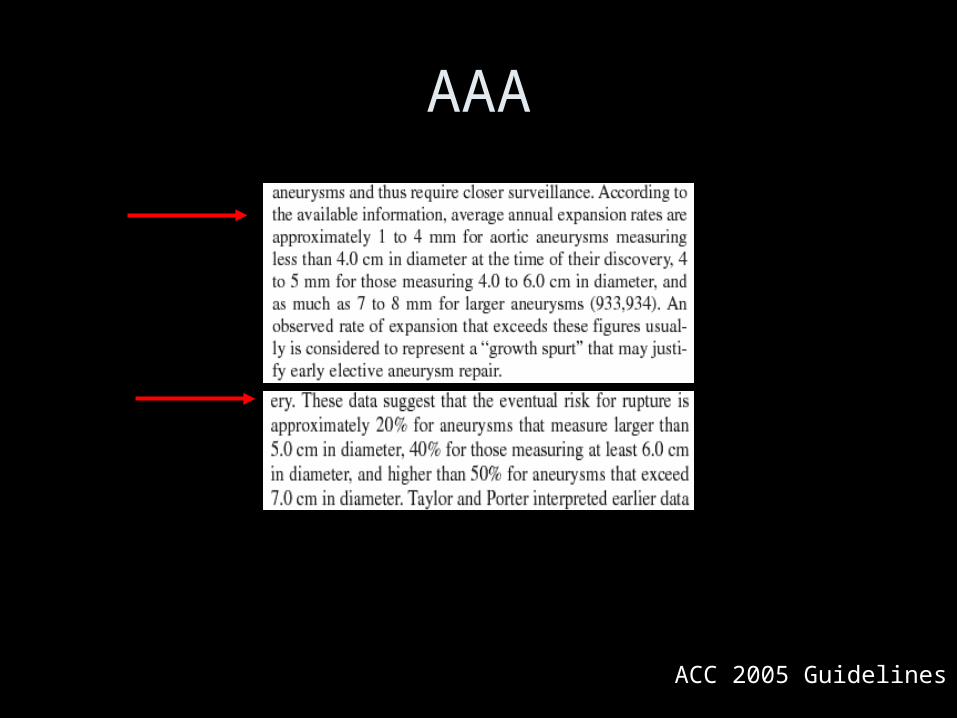
AAA
ACC 2005 Guidelines
ACC 2005 Guidelines
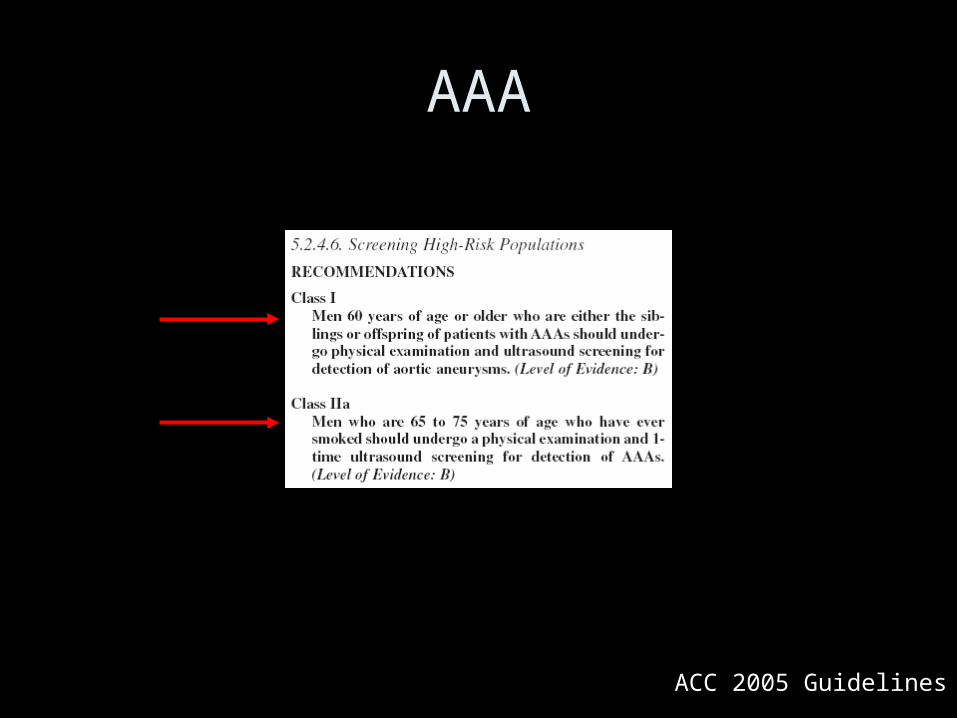
AAA
ACC 2005 Guidelines
AAA
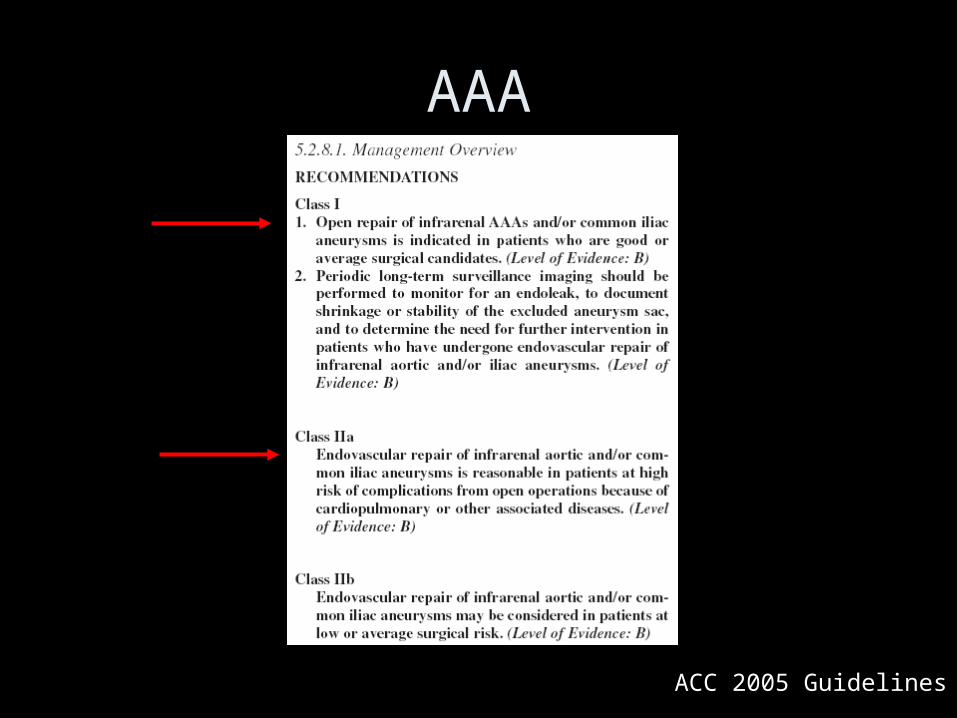
ACC 2005 Guidelines
AAA

Cardiomyopathies
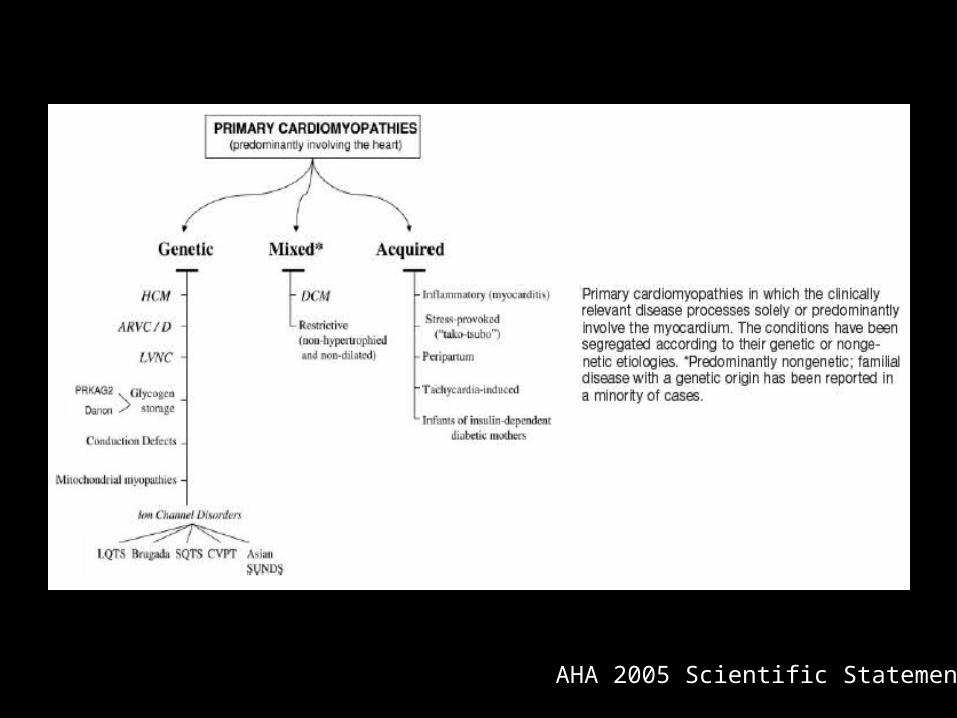
AHA 2005 Scientific Statement
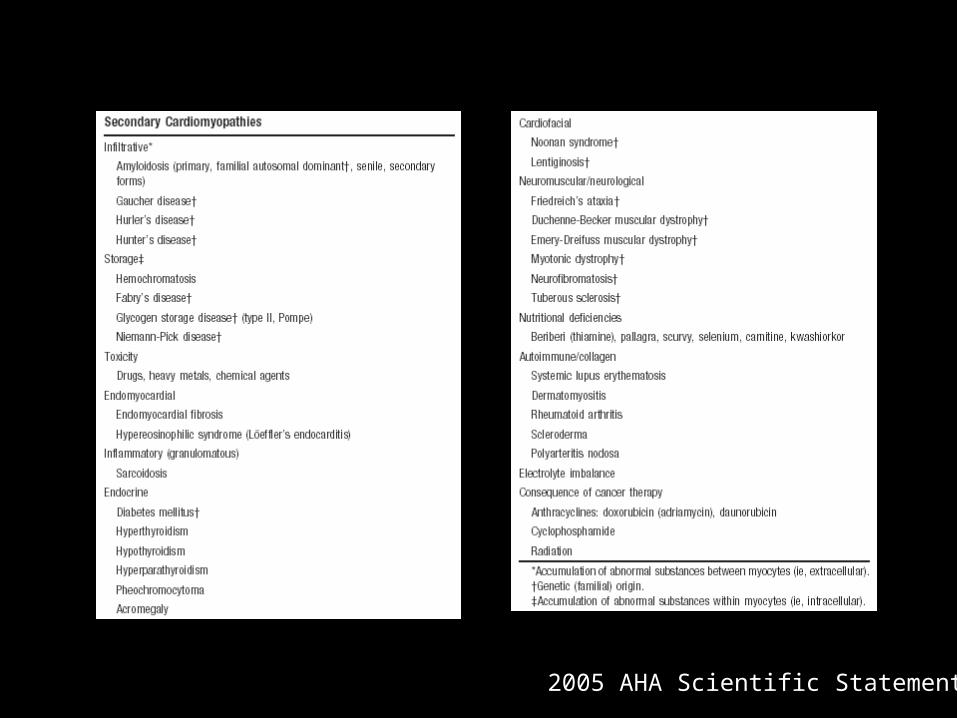
2005 AHA Scientific Statement
Hypertrophic Cardiomyopathy (HCM)
• Typically diagnosed by 2-D echo– LV wall thickness ≥ 15 mm– Asymmetric septal hypertrophy (ASH)– Anterior septal motion of mitral valve (SAM)
HCM
• LV outflow tract (LVOT) obstruction diagnosed using Doppler echo– LVOT pressure gradient (PG) 30 mmHg at
rest = “obstructive”– LVOT PG < 30 mmHg at rest but 30 mmHg
with provocation (Valsalva) = “latent”– LVOT PG < 30 mmHg at rest and with
provocation = “nonobstructive”
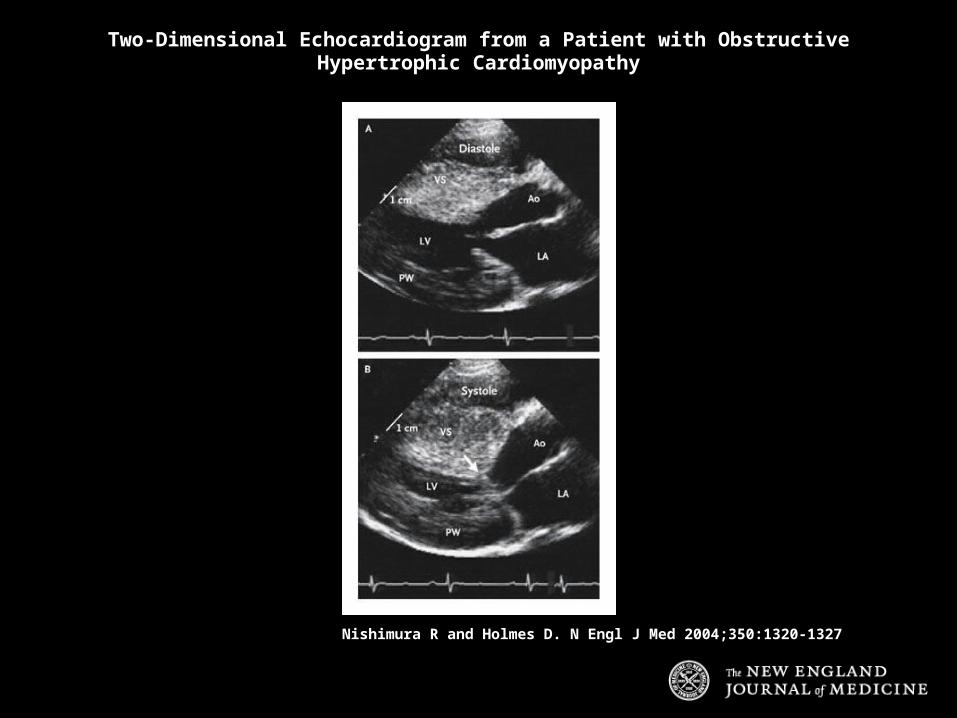
Nishimura R and Holmes D. N Engl J Med 2004;350:1320-1327
Two-Dimensional Echocardiogram from a Patient with ObstructiveHypertrophic Cardiomyopathy
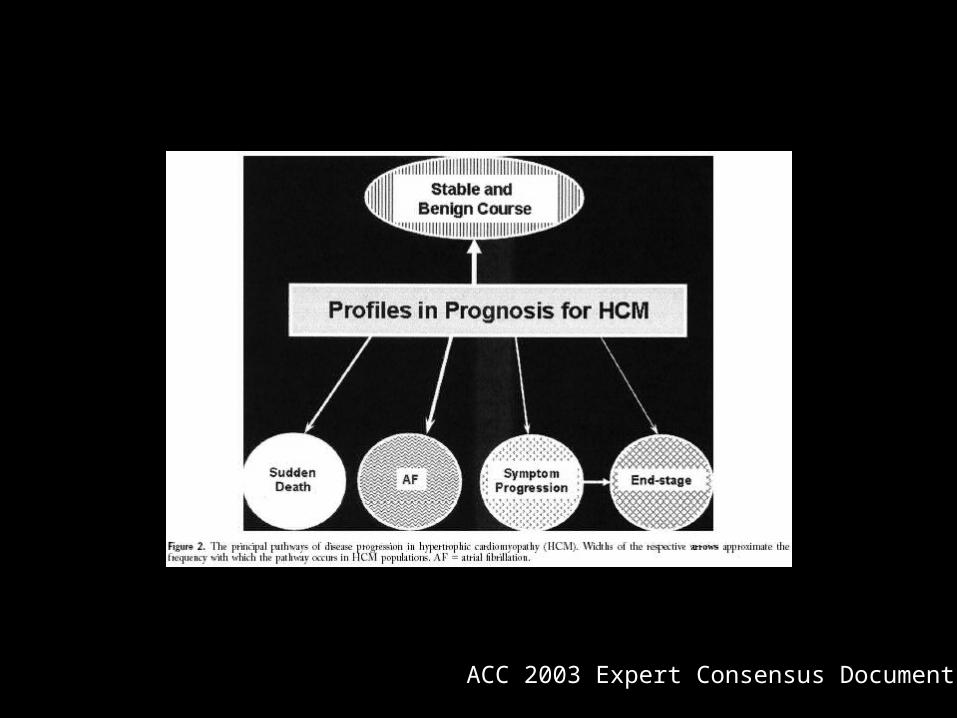
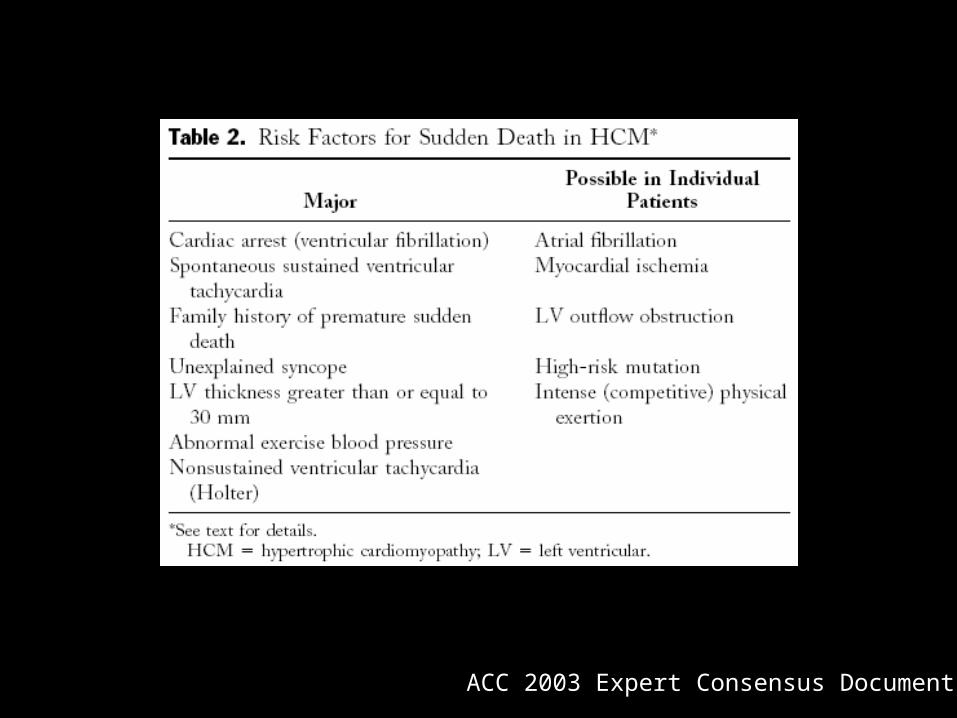
ACC 2003 Expert Consensus Document

ACC 2003 Expert Consensus Document
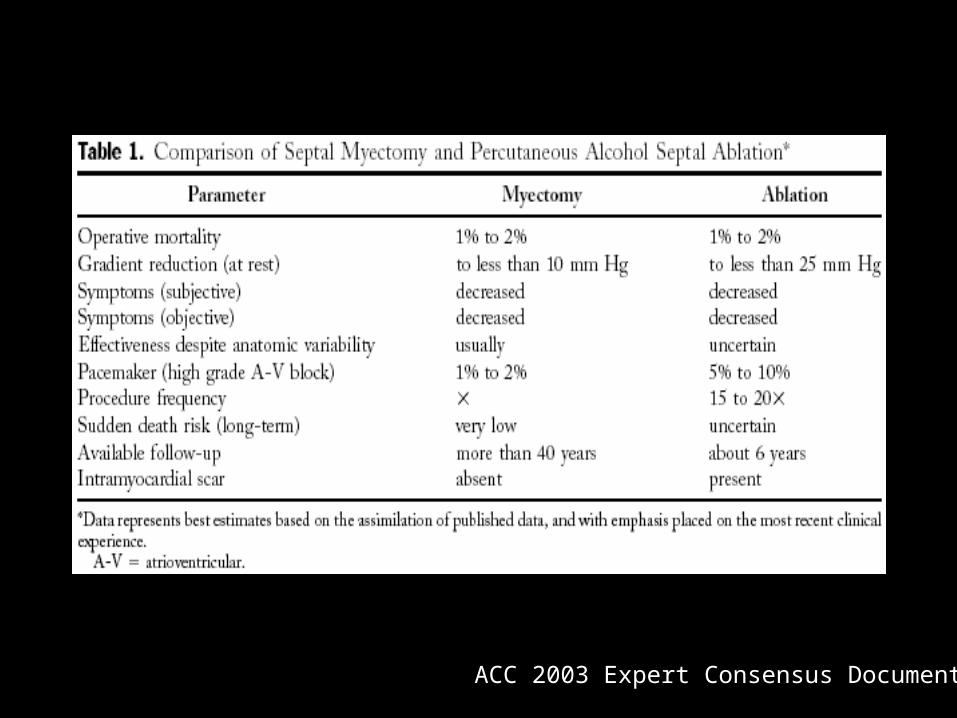
ACC 2003 Expert Consensus Document
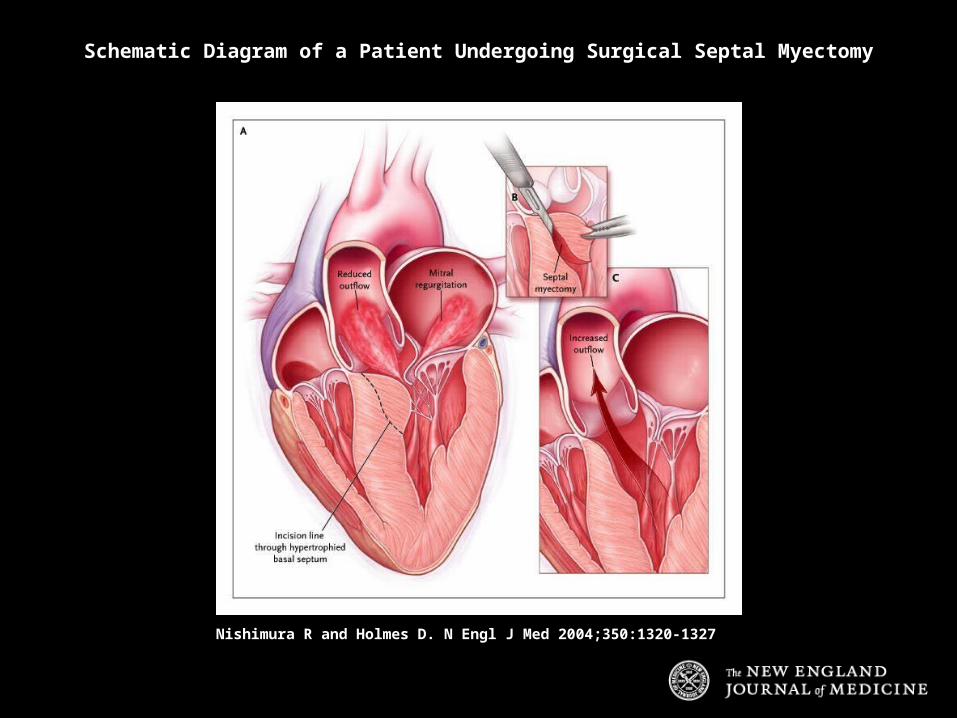
Nishimura R and Holmes D. N Engl J Med 2004;350:1320-1327
Schematic Diagram of a Patient Undergoing Surgical Septal Myectomy
ACC 2003 Expert Consensus Document
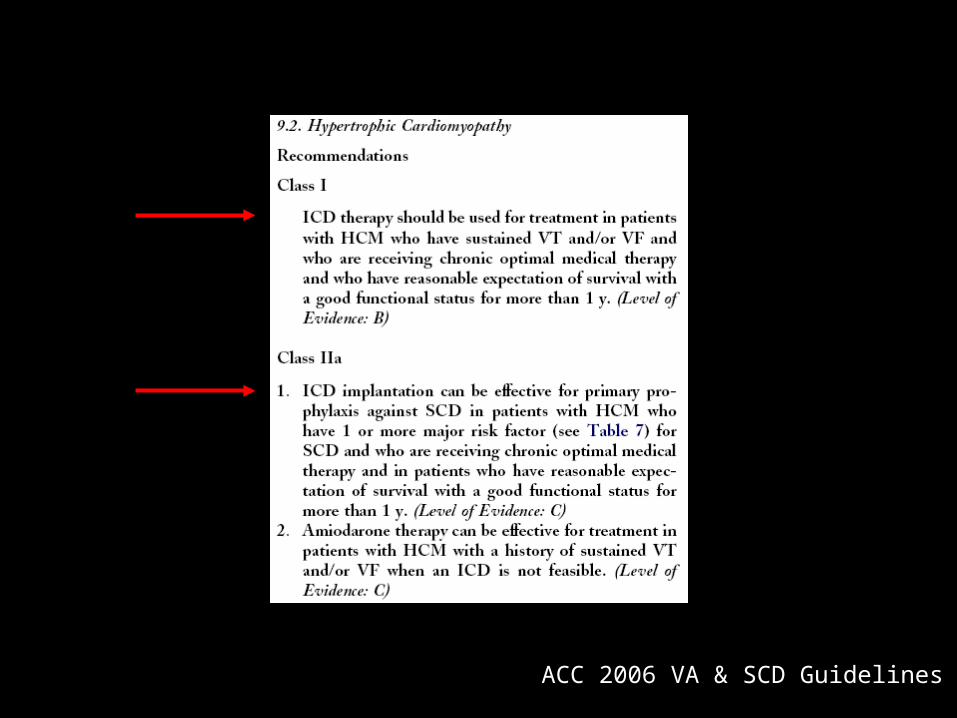
ACC 2006 VA & SCD Guidelines
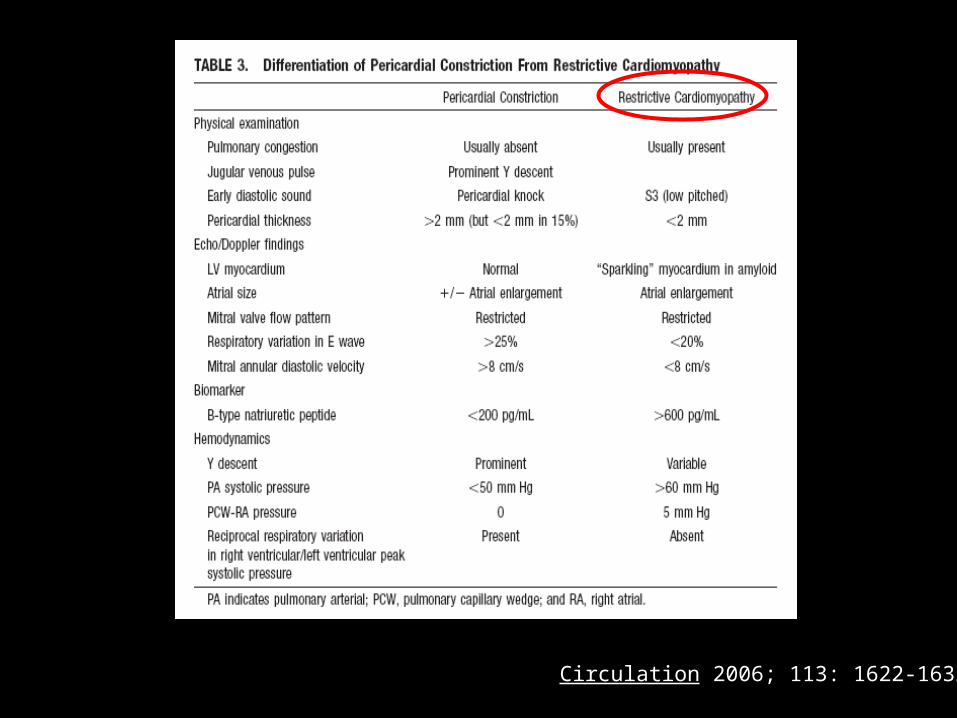
Circulation 2006; 113: 1622-1632