cardiac drugs :the latest and greatest - wallace state
TRANSCRIPT
Cardiac Drugs :The Latest and Greatest
Mir Varquez MD, FACC

Topics
u Corlanor (Ivabradine)
u Entresto (Sacubitril/Valsartan)
u Brilinta (Tigagrelor)
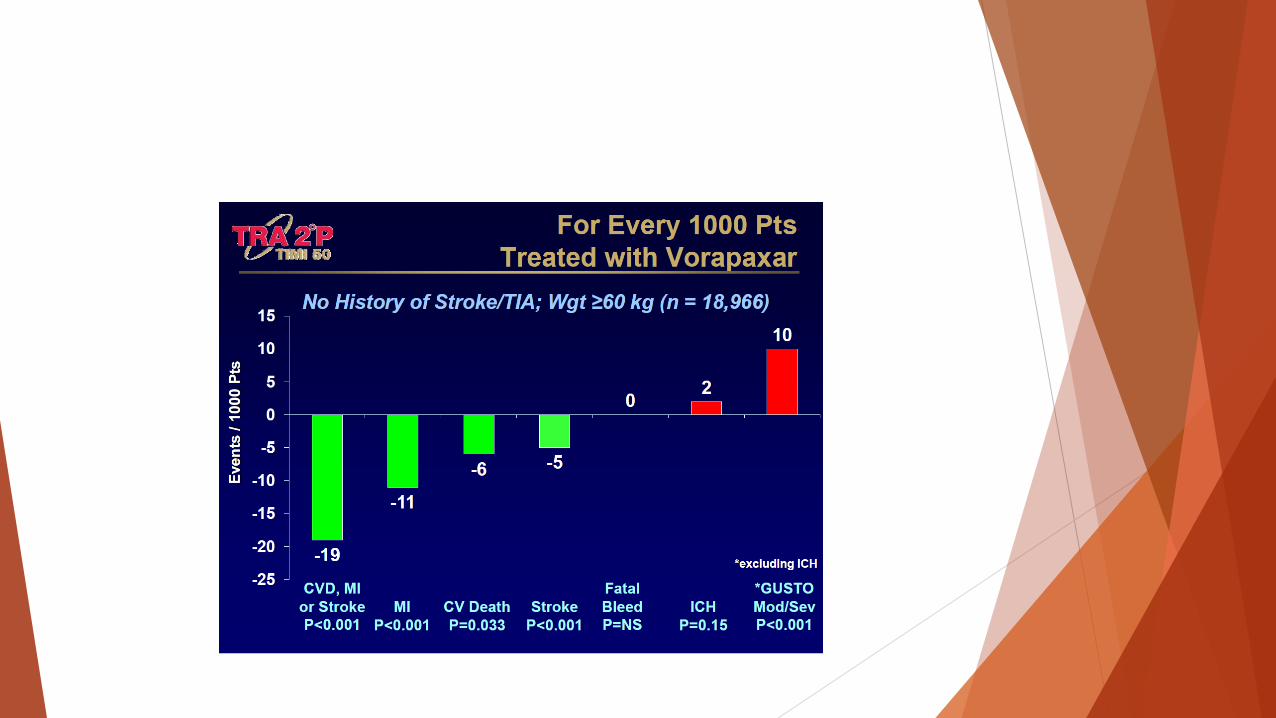
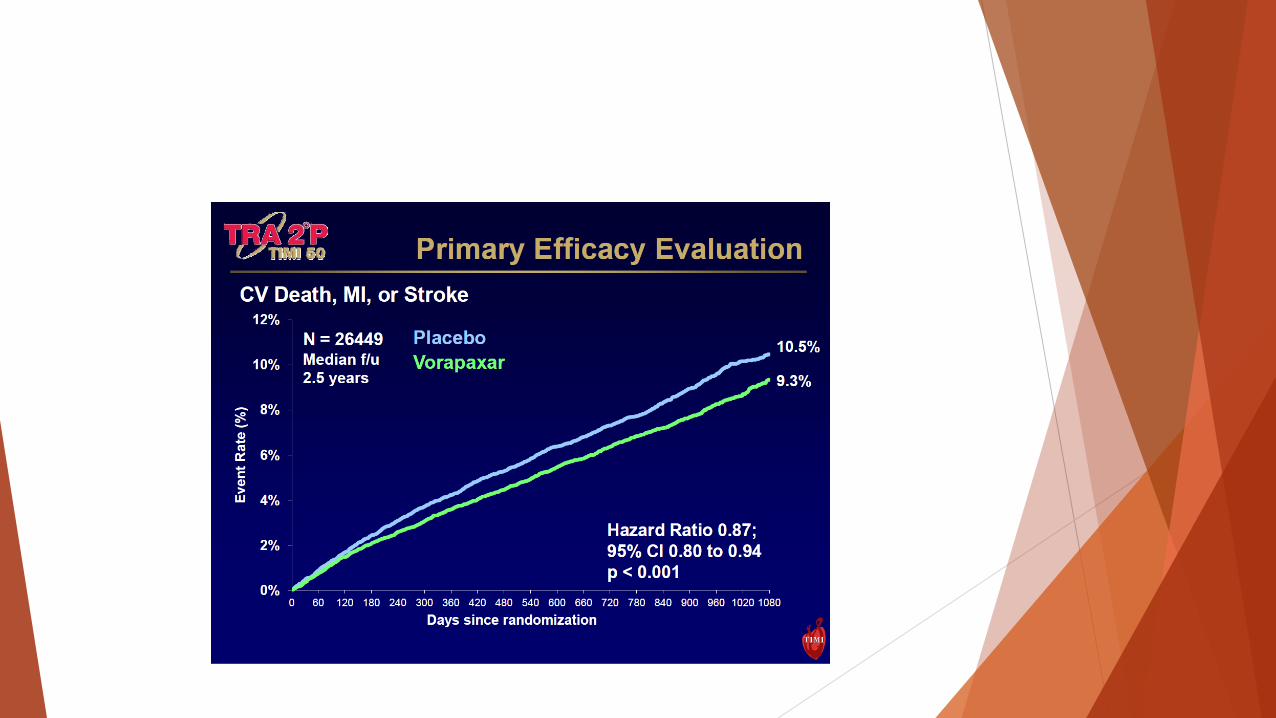
u Zontivity (Vorapaxar)
u PCS K9 Inhibitors:
§ Praluent (Alirocumab)
§ Repatha (Evolocumab)
u NOAC’S:
§ Xarelto, Eliquis, Pradaxa, Salaysa
Carlanor (Ivabradine)
Medication to reduce the risk of hospitalization for worsening HF in patients with stable, symptomatic chronic HF with LVEF less than or equal to 35%, who are in sinus rhythm with resting HR greater than 70 BPM and either are on maximally tolerated doses of a BB or have a contraindication to BB use.

Contraindications
§ Acute decompensated heart failure
§ Blood pressure <90/50
§ Severe hepatic failure
§ Use of strong P450 3A4 inhibitors (CYP3A4)
§ Increased risk of atrial fibrillation
§ Renal toxicity

Mechanism of Action
§ Within SAN-blocks the HCN channel, inhibits If current, lowers HR hyperpolarization- activated cyclic nucleotide gated.
§ Has no effect on myocardial contractility (no negative inotropic effect)
§ No effect on ventricular repolarization
§ Reduction in HR with Corlanor is dose dependent and baseline heart rate dependent.

Adverse Drug Effects
u Bradycardia
u Hypertension
u Atrial Fibrillation
u Phosphenes- Translucently enhanced brightness in a limited area of visual field, usually triggered by variations in light intensity.Onset is generally within two months of treatment( usually mild to moderate) and led to discontinuation in less than 1% of patients. Most resolved during or after treatment.

SHIFT
u Systolic Heart Failure Treatment with the If inhibitors Ivabradine Trial
u Admission criteria:
§ Optimized and stable treatment ≥ 4 weeks.
§ Sinus rhythm with resting heart rate ≥70.
§ NHHA class II-IV
§ Reduced LVEF (≤35%)
§ Hospitalization for worsening HF within 12 months.
§ 2.5-7.5 mg BID
§ Recommended starting dose 5mg BID, after 2 weeks increase by 2.5 mg 2x/day.

Goal
u 50-60 BMP
u No dose adjustment is required for patients with moderate to severe renal impairment CRCL 15-60 ml/min.
u Does not require routine lab monitoring.

Entresto (Sacubitril/Valsartan)
u Sacubitril, a neprilysin inhibitor, and Valsartan (Angiotensin II receptor blocker) are indicated to reduce the risk of CV death and hospitalization for heart failure in patients with chronic HF (NYHA class II-IV) and reduced EF.
Dosage
u Starting dose 49/51mg BID, increase after 2-4 weeks to target 97/103 mg.
u Reduce starting dose 24/26 mg in severe renal impairment or moderate hepatic impairment.
Contraindications
u Hypersensitivity
u Angioedema to ACEI/ARB
u Concurrent use of ACEI
u Concurrent use of Aliskiren in patients with DM.

Paradigm HF
u Multinational randomized double-blinded study comparing Entresto and Enalapril in 8442 with NHHA II-IV and systolic dysfunction ( EF≤ 40%).
u Superior to Enalapril in reducing the risk of combined endpoint of CV mortality HF hospitalizations.
u Improve overall survival.


Brilinta (Tigagrelor) P2Y12 Platelet inhibitor u Indications: Reduce rate of CV death, MI and stroke in ACS
or Hx of MI, for at least 12 months following ACS.
u Superior to Clopidogrel.
u Reduces stent thrombosis in patients stented for ACS.

Dosing
u Titrate with 180 mg load, 90 mg BID for 1 year, then 60 mg PO BID.
u Maintenance doses of ASA above 100 mg reduces the effectiveness of Brilinta.
u Do not start in patients undergoing urgent CABG.
u In clinical trail 14% of pts. developed dyspnea. No adverse effects in pulmonary function, no specific treatment is required.

Contraindications
u Avoid use in severe hepatic impairment, no dosage adjustment in renal impairment.
u Drug interactions with CYP3A inducers and inhibitors.
u No known treatment to reverse Brilinta ,and not dialyzable.

Zontivity




PCSK9
u PCSK9 (Proprotein Convertase Subtilisin/Kexin type 9) is a critical regulator of cholesterol mechanism though its interactions with the hepatic LDL receptor (LDLR) PCSK9 is a kexin (endopeptidase) found in the kidneys, liver, and intestines.
u Circulating PCSK9 binds to the extracellular EGFR-like domain of LDLR, followed by endocytosis and lysosomal degradation of the complex.
u LDL-R upregulation by SREBP ( sterol regulatory element-binding protein).
u Given SQ prefilled pen, or syringe (Alirocumab) or prefilled auto injector (Evolocumab) every 2 weeks or once a month.

Indications
u Used with statins in CV disease and high risk of stroke or heart attack who do not reach goals with statins alone.
u With side effects to statins
u Familial hypercholesterolemia

Dosing
Repatha (Evolocumab)
u 140 mg every 2-4 weeks
Praluent (Alirocumab)
u 75-150 mg every 2 weeks

NOAC’s
Novel (or newer) oral anticoagulant
u Minimal reaction with medications and foods, with no need for blood monitoring.
u NOT approved for valvular heart disease.
u All NOAC’s are associated with reduced rate of IC bleeding compared with Warfarin in treatment of AF.



Pradaxa (Dabigatran)
u Pradaxa (Dabigatran) at 150 mg BID is superior to Warfarin for the reduction of ischemic strokes in nonvalvular AF (RE-LY).
u Dabigatran 110 mg BID and Rivaroxaban 20 mg daily non-inferior to Warfarin in stroke reduction.
u Eliquis (Apixaban) 5 mg associated with similar ischemic stroke risk, but superior to overall stroke.
u Apixaban associated with overall reduction in mortality compared with Warfarin (ARISTOTLE)

Dosing
Eliquis (Apixaban)
u DVT 10 mg BID X 7 days then 5 mg BID x 3 months.
u Prevention of recurrent disease 2.5 mg BID following 6 months of 5 mg BID.
Pradaxa (Dabigatran)
u 150 mg BID preceded by 5 days with parenteral anticoagulant.
u Consider 110 mg BID if > 80 years old, taking Verapamil, or renal impairment.

Dosing
Salaysa (Edoxaban)
u 60 mg daily with prior 5 day parenteral anticoagulant.
u Lower dose to 30 mg daily in low body weight, or those taking P-gp inhibitors: Cyclosporin, Multaq, Ketoconazole, Erythromycin.
Xarelto (Rivaroxaban)
u 15 mg BID for 3 weeks then 20 mg daily.


References
u Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2013 Dec 3. [Epub ahead of print]
u Connolly SJ, Ezekowitz MD, Yusuf S, et al; RE-LY Steering Committee and Investigators. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139-1151.
u Patel MR, Mahaffey KW, Garg J, et al; ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883-891.
u Granger CB, Alexander JH, McMurray JJ, et al; ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981-992.
u Giugliano RP, Ruff CT, Braunwald E, et al; ENGAGE AF-TIMI 48 Investigators. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093-2104.
u Staritz P et al. (2008) Platelet reactivity and clopidogel resistance are associated with the H2 haplotype of the P2Y12-ADP receptor gene. Int J Cardiol [doi:10.1016/ j.ijcard.2007.12.118]