cardiac anesthesia basics for the “non- anesthesiologist” kimberly d. milhoan, md assistant...
TRANSCRIPT
Cardiac Anesthesia Cardiac Anesthesia Basics for the “Non-Basics for the “Non-Anesthesiologist”Anesthesiologist”
Kimberly D. Milhoan, MDKimberly D. Milhoan, MDAssistant Clinical Professor, University of Texas Health Assistant Clinical Professor, University of Texas Health Science Center, San Antonio, TXScience Center, San Antonio, TX
2011 Cardiac Critical Care Course2011 Cardiac Critical Care CourseKathmandu, NepalKathmandu, NepalOctober 16, 2011October 16, 2011

Anesthetic Order of Anesthetic Order of Events: Cardiac Events: Cardiac BypassBypass
Pre-operative evaluationPre-operative evaluation Sedation outside ORSedation outside OR Induction in ORInduction in OR Pre-bypassPre-bypass Initiation of bypassInitiation of bypass Maintenance of bypassMaintenance of bypass Re-warmingRe-warming Separation from bypassSeparation from bypass Post-bypassPost-bypass (Extubation)(Extubation) Transport to ICUTransport to ICU
Pre-operative Pre-operative Evaluation:Evaluation:NPO GuidelinesNPO Guidelines 8 hours: solid foods8 hours: solid foods 6 hours: formula6 hours: formula 4 hours: breast milk, formula for 4 hours: breast milk, formula for
infants <6 monthsinfants <6 months 2 hours: clear liquids2 hours: clear liquids

Pre-operative Pre-operative Evaluation:Evaluation:URIURI 5x risk of laryngospasm5x risk of laryngospasm 10x risk of bronchospasm10x risk of bronchospasm 11x risk of adverse perioperative respiratory 11x risk of adverse perioperative respiratory
eventevent RSV + CPB => post-op ARDs with high mortalityRSV + CPB => post-op ARDs with high mortality Risks increased in patients with baseline Risks increased in patients with baseline
pulmonary condition, e.g. asthmapulmonary condition, e.g. asthma History of allergic rhinitis or “usual runny nose” History of allergic rhinitis or “usual runny nose”
reassuringreassuring Consider postponing case until 2 weeks Consider postponing case until 2 weeks
symptom-freesymptom-free
Pre-operative Pre-operative Evaluation:Evaluation:URIURI Definite postponement of surgery Definite postponement of surgery
(until 2 weeks symptom free):(until 2 weeks symptom free):– Acute onsetAcute onset– FeverFever– Mucopurulent nasal dischargeMucopurulent nasal discharge– ““Wet” coughWet” cough

Pre-Operative Pre-Operative EvaluationEvaluation Greatest source of Greatest source of
information: information: pediatric pediatric cardiologist! Find cardiologist! Find their last note!their last note!
Evaluate their Evaluate their history, physical, history, physical, EKG, echo, cath, EKG, echo, cath, and radiographic and radiographic findingsfindings
Pre-Operative Pre-Operative Evaluation:Evaluation:Required DataRequired Data Height and weight (calculate body mass Height and weight (calculate body mass
index)index) Vital signsVital signs
– Temperature, heart rate, blood pressure, Temperature, heart rate, blood pressure, respiratory rate, BASELINE OXYGEN SATURATIONrespiratory rate, BASELINE OXYGEN SATURATION
LaboratoryLaboratory– Complete blood count, coagulation profile, Complete blood count, coagulation profile,
electrolytes, complete blood chemistry, type & electrolytes, complete blood chemistry, type & screenscreen
Chest x-rayChest x-ray EKGEKG EchoEcho +/- Cath findings+/- Cath findings

Emergency MedsEmergency Meds
Atropine: 20 mcg/kg or 100 mcg minimum Atropine: 20 mcg/kg or 100 mcg minimum Neosynephrine: 1 mcg/kgNeosynephrine: 1 mcg/kg
– Dilute syringe to 1 mcg/cc if <5 kg, 10 mcg/cc if 5-Dilute syringe to 1 mcg/cc if <5 kg, 10 mcg/cc if 5-10 kg, and 100 mcg/cc if over 40 kg10 kg, and 100 mcg/cc if over 40 kg
Epinephrine: 1-10 mcg/kgEpinephrine: 1-10 mcg/kg– Same serial dilutions as neosynephrineSame serial dilutions as neosynephrine
Adenosine: 150 mcg/kgAdenosine: 150 mcg/kg Amiodarone: 5 mg/kgAmiodarone: 5 mg/kg

Sedation outside OR:Sedation outside OR:PhilosophyPhilosophyA bad medical A bad medical
experience for an experience for an adult is a “story” adult is a “story” while a bad while a bad medical medical experience for a experience for a child can be a life- child can be a life- or personality-or personality-changing eventchanging event
Considerations: e.g., Tetrology of Considerations: e.g., Tetrology of Fallot patientsFallot patients
Induction in ORInduction in OR
Baseline SpO2, EKG, blood pressureBaseline SpO2, EKG, blood pressure IV or Inhalation inductionIV or Inhalation induction
– If no IV, inhalation induction with If no IV, inhalation induction with sevoflurane or halothane sevoflurane or halothane followed by IV placementfollowed by IV placement
Left-to-right shunt physiology:Left-to-right shunt physiology:– more sensitive to inhalation more sensitive to inhalation
agents and less sensitive to IV agents and less sensitive to IV agentsagents
– decreased pulmonary vascular decreased pulmonary vascular resistance results in pulmonary resistance results in pulmonary overcirculation overcirculation low inspired low inspired oxygen concentration, oxygen concentration, normocarbianormocarbia
Cyanotic physiology: Cyanotic physiology: – less sensitive to inhalation less sensitive to inhalation
agents and more sensitive to IV agents and more sensitive to IV agentsagents
NO BUBBLES!!NO BUBBLES!!
Induction in ORInduction in OR
Intubation--ETT:Intubation--ETT:– <1 kg: 2.5 uncuffed<1 kg: 2.5 uncuffed– <3 kg or <1 mth: 3.0 uncuffed<3 kg or <1 mth: 3.0 uncuffed– >3 kg or 1-6 mths: 3.5 uncuffed or 3.0 cuffed>3 kg or 1-6 mths: 3.5 uncuffed or 3.0 cuffed– 6 mths – 2 yrs: 3.5 – 4.0 cuffed6 mths – 2 yrs: 3.5 – 4.0 cuffed– Age/4 + 4: round down to lower size and use Age/4 + 4: round down to lower size and use
cuffed tubecuffed tube Baseline SpO2, EKG, blood pressure Baseline SpO2, EKG, blood pressure– Place just enough air in cuff to occlude leak at 20 cm Place just enough air in cuff to occlude leak at 20 cm
H2O pressureH2O pressure Second IVSecond IV Placement of invasive monitoring linesPlacement of invasive monitoring lines Placement of foley catheterPlacement of foley catheter
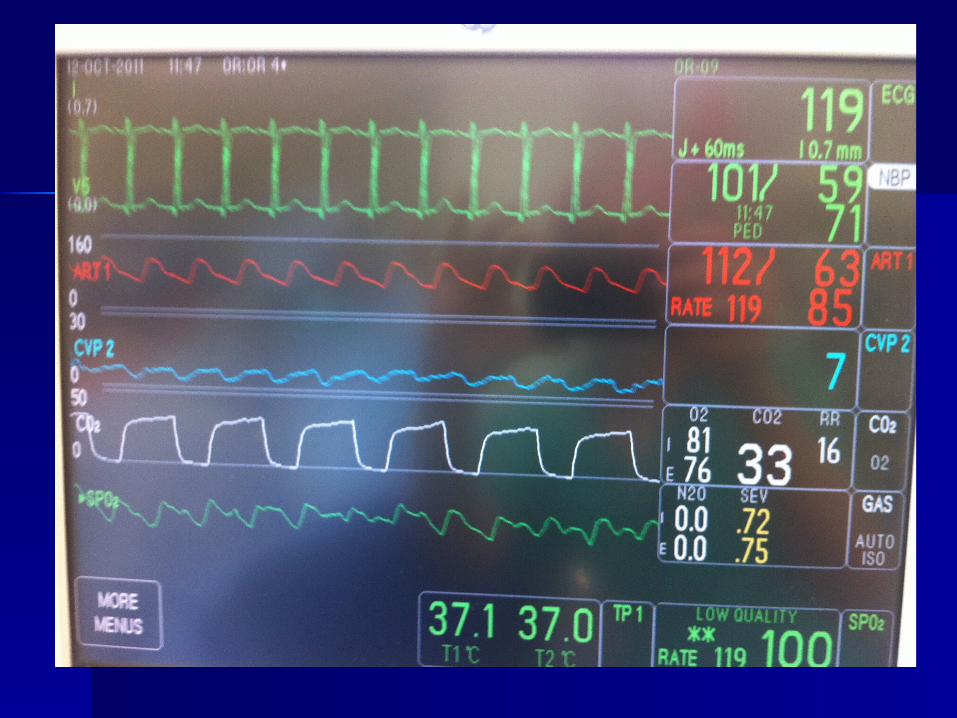
Intraoperative Intraoperative MonitoringMonitoring Pulse oximetryPulse oximetry EKGEKG Blood pressureBlood pressure
– Non-invasive prior to inductionNon-invasive prior to induction– Invasive post-induction (usually 24G in neonates, 22G in infants Invasive post-induction (usually 24G in neonates, 22G in infants
and children, and 20G in adults)and children, and 20G in adults) TemperatureTemperature
– NasopharyngealNasopharyngeal– RectalRectal
End tidal CO2End tidal CO2 Inspired/expired oxygen and inhalational agent concentrationInspired/expired oxygen and inhalational agent concentration Central venous pressureCentral venous pressure
– Up to 3 kg: 3 Fr single lumenUp to 3 kg: 3 Fr single lumen– 4–10 kg: 4 Fr double lumen4–10 kg: 4 Fr double lumen– 11-40 kg: 5 Fr double lumen11-40 kg: 5 Fr double lumen
Urine outputUrine output

Intraoperative Intraoperative Laboratory MonitoringLaboratory Monitoring
Arterial blood gas (ABG)Arterial blood gas (ABG) I-StatI-Stat
– HematocritHematocrit– SodiumSodium– PotassiumPotassium– Ionized CalciumIonized Calcium– GlucoseGlucose
Activated clotting time Activated clotting time (ACT)(ACT)– Baseline 90-120 Baseline 90-120
secondsseconds

Base-line, post-inductionBase-line, post-induction After heparinizationAfter heparinization Every 20 to 30 minutes during cardiac Every 20 to 30 minutes during cardiac
bypassbypass Immediately prior to separation from bypassImmediately prior to separation from bypass After protamine given after bypassAfter protamine given after bypass As often as deemed necessary during post-As often as deemed necessary during post-
bypass phasebypass phase Immediately prior to transfer to ICUImmediately prior to transfer to ICU On arrival to ICUOn arrival to ICU
Intraoperative Intraoperative Laboratory Monitoring: Laboratory Monitoring: Schedule Schedule
Pre-bypassPre-bypass
HeparinizationHeparinization– While placing aortic cannulaWhile placing aortic cannula– Infants: 400-500 units/kgInfants: 400-500 units/kg– Children and adults: 300-400 Children and adults: 300-400
units/kgunits/kg– Goal Activated Clotting Time (ACT) > Goal Activated Clotting Time (ACT) >
400 seconds (checked 3 minutes 400 seconds (checked 3 minutes after heparin given)after heparin given)

Initiation of BypassInitiation of Bypass
Discontinue Discontinue ventilation when ventilation when heart no longer heart no longer ejectingejecting
3-5 mm Hg positive 3-5 mm Hg positive end expiratory end expiratory pressure (PEEP) with pressure (PEEP) with airair
Re-dose sedation, Re-dose sedation, muscle relaxant, muscle relaxant, narcoticnarcotic

ResourcesResources
Andropoulos DB, Stayer SA, and Russell IA. Andropoulos DB, Stayer SA, and Russell IA. Anesthesia for Anesthesia for Congenital Heart DiseaseCongenital Heart Disease. Malden: Futura, 2005.. Malden: Futura, 2005.
Cohen MM, Cameron CB. Should you cancel the operation Cohen MM, Cameron CB. Should you cancel the operation when a child has an upper respiratory tract infection? when a child has an upper respiratory tract infection? Anesth Analg 1991;72:282-8.Anesth Analg 1991;72:282-8.
Cote, Charles J. et al. Cote, Charles J. et al. A Practice of Anesthesia for Infants A Practice of Anesthesia for Infants and Childrenand Children, 3, 3rdrd ed. Philadelphia: Saunders, 2001. ed. Philadelphia: Saunders, 2001.
Lake CL and Booker PD. Lake CL and Booker PD. Pediatric Cardiac AnesthesiaPediatric Cardiac Anesthesia, 4, 4thth ed. Philadelphia: Lippincott, Williams, & Wilkins, 2005.ed. Philadelphia: Lippincott, Williams, & Wilkins, 2005.
Morgan, G. Edward et al. Morgan, G. Edward et al. Clinical AnesthesiologyClinical Anesthesiology, 3, 3rdrd ed. New ed. New York: Appleton & Lange, 2002.York: Appleton & Lange, 2002.