cardiac anatomy, function and metabolism in elite cyclists assessed
TRANSCRIPT

European Heart Journal (1996) 17, 1271-1278
Cardiac anatomy, function and metabolism in elitecyclists assessed by magnetic resonance imaging
and spectroscopy
B. M. Pluim*. J. C. Chin*+, A. De Roost, J- Doornbost, H.-M. J. Siebelink*,A. Van der Laarse*, H. W. Vliegen*, R. M. J. N. Lamerichs§, A. V. G. Bruschke*
and E. E. Van der Wall*
*Department of Cardiology, University Hospital, Leiden, The Netherlands; ^Department of Radiology UniversityHospital, Leiden, The Netherlands; %Centre for Heart and Lung Rehabilitation, Rijnlands Zeehospitium, Katwijk,
The Netherlands; ^Philips Medical Systems, Best, The Netherlands
We investigated whether left ventricular hypertrophy inelite cyclists is associated with functional changes orabnormal energy metabolism.
Left ventricular hypertrophy is a powerful risk factor forsudden cardiac death with different prognostic signifi-cance among the various geometric forms. Cyclists mayhave a combination of mixed eccentric and concentrichypertrophy.
Magnetic resonance imaging was used to define left ven-tricular mass, geometry and function. Thirteen highlytrained male cyclists and 12 healthy controls were investi-gated. Proton-decoupled phosphorus-31 cardiac spectro-scopy was performed to assess parameters of myocardialhigh-energy phosphate metabolism. Left ventricular massand end-diastolic volumes normalized for body surface areawere significantly higher in cyclists (124-1 ±9-4 g . m ~ 2 and106-2 ± 11-4 ml . m~ 2 , respectively) than in controls(85-9 db 9-3 g . m ~ 2 and 79-1 ± 11 -6 ml . m ~ 2, respectively),
(both /><00001). The left ventricular mass to end-diastolicvolume ratio, as a parameter of left ventricular geometry,was not significantly increased in cyclists compared tocontrols. Resting left ventricular ejection fraction, cardiacindex, and systolic wall stress in cyclists did not differsignificantly from those of controls. The phosphocreatine toadenosine triphosphate ratio was not significantly differentbetween cyclists and controls (2-2 ±0-34 vs 2-2 ±0-17, ns).
Cyclists show prominent left ventricular hypertrophy withnormal geometry. The finding that the hypertrophic heartsof the cyclists had normal left ventricular function and anormal phosphocreatine to adenosine triphosphate ratiosuggests that sport-induced left ventricular hypertrophy is aphysiological adaptation rather than a pathophysiologicalresponse.(Eur Heart J 1996; 17: 1271-1278)
Key Words: Left ventricular hypertrophy, magneticresonance imaging, spectroscopy.
Introduction
Previous studies have shown that elite athletes havesigns characteristic of left ventricular hypertrophy,generally called 'athlete's heart'11"41. Dependent on thetype of exercise performed, two morphological forms ofathlete's heart can be distinguished: hearts with eccentric
Revision submitted 1 August 1995, and accepted 20 September1995.
This work was supported by a grant from the Ministry of Welfare,Health and Cultural Affairs, The Hague, The Netherlands.
Correspondence: Ernst E. Van der Wall, MD, Departmentof Cardiology, Building 1, C5-P25, University Hospital,Rijnsburgerweg 10, 2333 AA Leiden, The Netherlands.
hypertrophy or concentric hypertrophy13"71. Eccentrichypertrophy, found in athletes who participate in sportwith a high dynamic component (e.g. running), ischaracterized by a large absolute left ventricular massand chamber size. Concentric hypertrophy, found inathletes who participate in sport with a high staticcomponent (e.g. weight-lifting), is characterized by alarge left ventricular mass without an increase in cham-ber size. A combination of eccentric and concentrichypertrophy is found in athletes who participate in sportwith both high dynamic and static demands (e.g. rowingand cycling)'6'.
Left ventricular hypertrophy is a powerfulindependent risk factor for the development of cardio-vascular morbidity and mortality18". In the athletic
0I95-668X/96/08127I+08 $18.00/0 1996 The European Society of Cardiology
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021
1272 B. M. Pluim et al.
population left ventricular hypertrophy is generally notconsidered to be an independent risk factor for cardio-vascular disease or sudden cardiac death'101. However,the unexpected death of a number of elite, seeminglyhealthy cyclists has raised questions about the long-term health aspects of extreme physical training1"1.Two echocardiographic studies have demonstrated de-pressed left ventricular function in several older profes-sional cyclists, which may indicate that extremephysical training of long duration has indeed a negativeeffect on the heart of athletes, manifested by partlyirreversible left ventricular hypertrophy and impairedleft ventricular filling"2131.
Using magnetic resonance imaging and magneticresonance spectroscopy, the purpose of the present studywas to investigate whether elite cyclists have depressedleft ventricular function and abnormal myocardialhigh-energy phosphate metabolism. We chose to studycyclists, not only because impaired left ventricular func-tion has already been demonstrated in this group, butalso because of the current public discussion regardingthe health aspects of intensive professional cycling1141.
Magnetic resonance imaging has good repro-ducibility and accuracy in the quantification of leftventricular mass and left ventricular end-systolic andend-diastolic volumes'15"191, and phosphorus-31 spectro-scopy has recently been used to characterize themetabolic state of the myocardium'20"231.
Methods
Study population
Initially, the study group consisted of 30 subjects i.e. 15highly trained male cyclists and 15 male control subjects.In five subjects (two cyclists, three control subjects) themagnetic resonance images were of insufficient qualityand these subjects were excluded from participation inthe study. Therefore, the evaluable study populationcomprised 13 cyclists (mean age 22-3 ± 2-1 years) and 12healthy volunteers who served as controls (mean age26-8 ± 3-8 years). The cyclists were participants in thenational championships in 1992 and 1993 and cycled atleast 20 000 km (12 500 miles) per year; all had cycledcompetitively for more than 5 years (mean 10-5 years).The 12 control subjects were healthy, non-sedentaryindividuals, not engaged in any routine physical train-ing. All subjects were free of known cardiovasculardisease, were normal by physical examination, and hadnormal cardiac anatomy by two-dimensional echo-cardiography. The resting electrocardiograms werecompletely normal in nine cyclists; three cyclists demon-strated incomplete right bundle branch block and onecyclist non-specific T-wave abnormalities. The study wasapproved by the Human Research Committee at ourinstitution, and all individuals gave informed consent.Table 1 shows the baseline characteristics of the 25subjects included in the study.
Table 1 Baseline characteristics in 25 subjects (meanvalues ± 1 SD)
Variable
Age (years)Height (cm)Body weight (kg)Body surface area (m2)Body fat (%)Lean body mass (kg)Systolic blood pressure (mmHg)Diastolic blood pressure (mmHg)Mean blood pressure (mmHg)Resting heart rate (min " ')VO2 max (1 . min" ' )VO2 max (ml. kg ~ ' . min ~ ')
Controls(n=12)
26-8 (3-8)181-8 (6-9)75-6 (9-3)2-0(0-1)
16-7 (6-2)62-6 (60)
116-5 (8-2)661 (5-9)82-9 (6-0)600 (6-7)
3-7 (0-6)491 (7-3)
Cyclists(n=13)
22 3 t (2-1)182-9 (5-7)74-8 (5-6)2-0(0-1)
11-5J(3-1)66-2 (4-8)
122-7 (8-4)63-7 (6-2)83-4 (5 9)55-9 (111)4-9* (0-4)
66-2* (4 4)
•/><0-0001 vs controls; f/ J<0005 vs controls; J/><0-05 vs controls.V02max = maximal oxygen consumption
Anthropometry and exercise test
Height, body weight, body surface area, lean body massand percent body fat were determined for each subject.Body surface area was calculated from height andweight. Lean body mass and percent body fat wereobtained by measuring four different skinfold sites'24'. Astandard 12-lead electrocardiogram was recorded at restand during exercise. Exercise testing was performedusing a bicycle ergometer (Siemens, Enhorna, Sweden).The initial exercise intensity was 100 W during the first3 min of the test, increasing to 150 W during the 4 min,which was further increased by 25 W every min untilexhaustion. The highest oxygen uptake obtained duringthe test by an oxygen analyser (Jager, Breda, TheNetherlands) was taken as the maximal oxygen uptake.
Magnetic resonance imaging protocol
Magnetic resonance imaging was performed with aGyroscan system (Philips Medical Systems, Best, TheNetherlands) at a field strength of l-5Tesla, usingelectrocardiographic gating. Images were acquired in theshort-axis plane of the heart, derived from coronal andsagittal scout views, using double oblique angulation.Cine magnetic resonance imaging was performed using agradient echo sequence (flip angle 40°). Echo-time was13-7 ms; repetition time was equal to the average R-Rinterval. Twelve slices were obtained (thickness 10 mm,interslice gap I mm), encompassing the entire left ven-tricle from apex to base. The shortest possible triggerdelay was 8 ms after the R wave of the electrocardio-gram. The acquisition matrix was 102 x 128 and wasinterpolated to 256 x 256 for display purposes. The fieldof view was 300 mm2 and two acquisitions were aver-aged to improve the signal-to-noise ratio. Two sliceswere acquired interleaved in time, which reduced thetemporal resolution by a factor of 2 and resulted in an
Eur Heart J, Vol. 17, August 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021

Cardiac MR techniques in athletes 1273
average final time resolution of 60 ms. During themagnetic resonance imaging examination (average20 min), heart rate and blood pressure were recordedevery 3 min with a Dynamap sphygmomanometer(Critikon, Tampa, FL, U.S.A.) and average heart rateand blood pressure were determined from thesereadings.
Magnetic resonance image analysis
The images were displayed on a computer monitor in amovie loop mode to visualize the contraction patternthroughout the cardiac cycle with an average of 14frames per cycle. The window setting was standardizedby adjusting the high level just below the signal intensityindicating pericardial fat, and by adjusting the low levelsignal intensity slightly above the intraventricular signalintensity. High intensity epicardial fat was carefullyexcluded from analysis, but the papillary muscles wereincluded in the area traced. The subendocardial andsubepicardial boundaries were manually traced used atrackball cursor. The enclosed surface areas were meas-ured by a computer. The criteria for a high qualitymagnetic resonance image were the recognition of anexcellent border definition (maximal contrast difference)both for the transition of the left ventricular cavity to thesubepicardium, and for the transition of the sub-epicardium to the right ventricle or to extracardiacstructures. If these criteria were not met the subject wasexcluded from the study (two cyclists, three controlsubjects). We also excluded those imaging planes fromanalysis that showed discontinuity in the subendocardialand subepicardial borders, mostly caused by interferenceof aortic or mitral valve structures within the imagingplane. In our study, five of 30 subjects (16%) had to beexcluded because excessive respiratory motion disruptedthe magnetic resonance image artifacts.
The following measurements were obtained: (1)Left ventricular mass. To calculate left ventricular mass,measurements of left ventricular wall volume wereperformed using up to 12 slices. The endocardial andepicardial borders in end-diastolic frames were outlined(Fig. 1). By subtracting the endocardial cross-sectionalarea from the epicardial cross-sectional area, the end-diastolic left ventricular wall area was obtained. Thepapillary muscles were outlined and considered to bepart of the left ventricular wall. The values of leftventricular wall area in each section were multiplied bythe sum of slice thickness and interslice gap, and com-bined to obtain left ventricular wall volumes'251. Totalleft ventricular wall volume was multiplied by thespecific gravity of cardiac muscle (105g .ml~ ' ) toobtain left ventricular wall mass (g) at end-diastole. (2)Indexed left ventricular mass was defined as left ven-tricular mass divided by body surface area, expressed ing. m~2. (3) Left ventricular end-diastolic volume andleft ventricular end-systolic volume were determined bysummation of the end-diastolic and end-systolic cross-sectional endocardial areas, respectively. The end-
Figure 1 Short-axis cardiac cine magnetic resonanceimages at mid-papillary level of a control subject (left),and cyclist (right). The end-diastolic magnetic resonanceimages without (upper panel) and with (lower panel)epicardial and endocardial contours are shown. Note theincreased left ventricular dimensions of the cyclist.
systolic image was determined by the moment the leftventricular cavity showed its minimal surface area in theselected imaging plane, whereas the end-diastolic imagewas determined by the moment the left ventricularcavity showed its maximal surface area. The values ofarea in each section were multiplied by the sum of theslice thickness and the interslice gap and combined toobtain left ventricular end-diastolic and end-systolicvolumes (in ml) according to the volumetric method'251.(4) Indexed left ventricular end-diastolic and end-systolic volumes equalled left ventricular end-diastolicand end-systolic volume divided by body surface area(ml. m ~2). (5) Left ventricular mass to left ventricularvolume ratio equalled the ratio of left ventricular massover left ventricular end-diastolic volume'261 (g . ml ~ ').(6) Left ventricular stroke volume was calculated as thedifference between left ventricular end-diastolic and end-systolic volume (ml). (7) Left ventricular stroke indexequalled left ventricular stroke volume divided by bodysurface area (ml. min ~ ' ) . (8) Left ventricular ejectionfraction was calculated as the ratio of the left ventricularstroke volume over left ventricular end-diastolic volumemultiplied by 100 (%). (9) Cardiac output was calculatedas left ventricular stroke volume multiplied by averageheart rate (ml. min" ') . (10) Cardiac index was calcu-lated as cardiac output divided by body surface area(ml. min" ' . m~2). (11) Left ventricular systolic wallstress (LVSWS) was calculated using the followingformula:'271
LVSWS=0133xPx[(3 x LVESV/LVWV)+1] (kN . m " 2 ) ,
in which 0133=conversion factor; P=systolic bloodpressure; LVESV = left ventricular end-systolic volume;LVWV = left ventricular wall volume.
Eur Heart J, Vol. 17, August 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021

1274 B. M. Pluim et al.
Proton-decoupled phosphorus-31 magneticresonance spectroscopy
Within 6 months of the magnetic resonance imagingstudies, 13 cyclists and four control subjects underwentproton-decoupled phosphorus-31 spectroscopy on a15 Tesla magnetic resonance system (Gyroscan; PhilipsMedical Systems, Best, The Netherlands)'281. Theexercise level of the athletes remained the same through-out both studies. A transmit/receive single-tunedphosphorus-31 surface coil with a diameter of 10 cm waspositioned on the chest wall anterior to the cardiac apexwith the subject in the supine position. Electrocardio-graphically triggered multisection axial spin-echo scoutimages were obtained. The position of the surface coilwas verified on thee images. Shimming of the magneticfield over the volume of interest was performed with anautomatic procedure, yielding a water resonance of0-2-0-3 parts per million full width at half maximum.The acquisition of the spectra was gated to the R waveof the electrocardiogram, with a trigger delay time of200 ms and a repetition time between 3 and 4 s, result-ing in a total acquisition time of 25-30 min. Protondecoupling was applied during acquisition of thephosphorus-31 signal. The localization scheme to obtainthe phosphorus-31 cardiac spectra comprised one-dimensional phase encoding along the axis perpendicu-lar to the left ventricular wall combined with two-dimensional image-selected in vivo spectroscopy (ISIS),resulting in spectra from a series of 1 cm thick sections inthe oblique coronal plane1281. Selection of the appropri-ate sections was done after inspection of both theanatomical position of the 1 cm thick slices on themagnetic resonance images and the decay of the phos-phocreatine signal when going from skeletal muscle intothe myocardium.
Spectroscopic analysis
Fourier transformation was applied in the k domain.The resulting time domain signals were quantified bymodel function analysis, using a priori knowledge toimprove the accuracy of the spectral parameters. Theprior knowledge consisted of assuming fixed values forthe J-coupling pattern of the adenosine triphosphateresonances, a fixed position for the phosphatidylcholineand for the serum phospholipid signal, fixed amplituderatios and decay (line-width) ratios for the three adeno-sine triphosphate signals and fixed line-widths for thediester, inorganic phosphate and 2,3-diphosphoglyceratesignals. The average of all adenosine triphosphateresonances was used for quantification purposes. Therelationship of adenosine triphosphate resonancesremained constant, which was verified by close inspec-tion of the 'difference spectra' (observed spectrum minusmodel fit). None of the difference spectra showed signalsexceeding the spectral noise in the adenosine tri-phosphate region. The adenosine triphosphate level inmyocardial spectra was corrected to take account of the
adenosine triphosphate contribution from intraventricu-lar blood'281. There were no constraints in any relevantparameter as regards the determination of phospho-creatine to adenosine triphosphate ratios and pH values.In case the inorganic phosphate peak could be resolvedin the spectrum, pH values were quantified from thechemical shift between the inorganic phosphate andphosphocreatine resonance peaks'281. Metabolite ratioswere corrected for partial saturation, using previouslypublished values for myocardial tissue1291.
Inter-observer and intra-observer variability
Magnetic resonance imaging inter-observer variabilitywas determined by comparing left ventricular mass andvolumes measured by two observers, who used the samewindow width and window level settings. Intra-observervariability was determined by comparison of leftventricular mass and volumes as determined by oneobserver on two separate occasions at least 6 weeksapart.
Statistical analysis
Statistical analysis of the magnetic resonance imagingand spectroscopy data was performed using the Studentt-test to compare average values from cyclists andnormal subjects. All values are reported as mean ±standard deviation, except where stated otherwise. Thenull hypothesis was rejected if its statistical probabilitywas less than 5%. The results of the inter-observerand intra-observer variabilities are presented as thedifference expressed as a percentage of the mean value.
Results
Subject characteristics
The anthropometric characteristics of the 13 cyclists andthe 12 control subjects are presented in Table 1. Athletesand sedentary subjects were of similar height (183 ± 6 vs182 ± 7 cm, ns) and weight (75 ± 6 vs 76 db 9 kg, ns). Theathletes were younger than the sedentary subjects(22 ± 2 vs 27 ± 4 years, /><0005). Resting heart rate wasslightly, but not significantly, lower in cyclists than incontrols (56±11 vs 60± 1 min" ' , ns). Systolic bloodpressure was slightly, but not significantly, higher inathletes at supine rest (123 ± 8 vs 117±8mmHg, ns).Resting electrocardiograms were completely normal in21 of 25 subjects (nine cyclists, all control subjects).Three cyclists showed incomplete right bundlebranch block and one cyclist showed aspecific T-waveabnormalities.
Exercise test
In cyclists, maximal oxygen uptake was higher than incontrols, irrespective of notation in 1. min ~ ' (4-9 vs
Eur Heart J, Vol. 17, August 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021

Cardiac MR techniques in athletes 1275
Table 2 Left ventricular mass, geometry, and functiondetermined by magnetic resonance imaging in 25 subjects(mean values ± 1 SD)
Variable
LV mass (g)LVmass/BSA ( g . m " 2 )LVEDV (ml)LVESV (ml)LVEDV/BSAOnl.m-2)LVESV/BSAOnl.m"2)LV mass/LVEDV (g . m l " ' )LVSV (ml)LVSI ( m l . m - 2 )LVEF (%)Cardiac output (1 . min~ ')Cardiac index (1. min ~ ')Systolic wall stress (kN . m"" *)
Controls(n=12)
168-7 (18-2)86-3 (8-5)
154-3 (220)55-6(13-6)791 (11-6)28-5 (6-9)
11 (01)98-7 (15-9)50 6 (8-4)641 (6-7)5-9(1-1)3-0 (0-6)
31-4(3-0)
Cyclists(n=13)
243-2* (19-2)124-3* (9-3)207-9* (22-4)
74-4t (12-5)106-2* (11-4)38-O| (6-1)
1-2(0-1)133-4* (21-3)681* (111)640 (5-8)
7-5 (2-3)3-8(1-2)
32-0 (2-8)
*/><0-0001 vs controls; t^<0-005 vs controls.LV=left ventricular; BSA = body surface area; EF = ejection frac-tion; EDV = end-diastolic volume; ESV = end-systolic volume;SV=stroke volume; SI = stroke index.
3-7 1. min~ ', /)<00001) or in ml. kg ' . min" ' (66-2vs 491 ml. kg" ' . min" ', /)<0-0001, Table 1). Duringexercise no serious rhythm disturbances were observed,and in none of the 25 subjects did the exercise electro-cardiograms show any significant changes compared tothe resting electrocardiograms.
Imaging quality
Magnetic resonance imaging showed high qualityimages in 25 out of 30 subjects (13 cyclists, 12 controls).
Magnetic resonance imaging of leftventricular morphology
In cyclists, the absolute mean left ventricular mass was44-2% higher than in controls (/><0-0001, Table 2). Also,after correction for differences in body surface area, theleft ventricular mass in cyclists remained higher (440%,P<00O0\).
Both absolute and indexed values of leftventricular end-diastolic and end-systolic volumes weresignificantly larger in cyclists than in controls (Z'<0005).The cyclists had a slightly, but not significantly, higherleft ventricular mass to left ventricular end-diastolicvolume ratio, when compared to controls (Table 2).
Magnetic resonance imaging of leftventricular function
Left ventricular ejection fraction, cardiac output andcardiac index were not significantly different between
cyclists and controls (Table 2). Although left ventricularstroke volume and stroke index were significantly higherin cyclists, this was compensated for by a lower restingheart rate in cyclists, resulting in a cardiac output andcardiac index not significantly different from the controlgroup (Table 2). Left ventricular systolic wall stressdid not differ significantly between cyclists and controlsubjects (Table 2).
Proton-decoupled phosphorus-31 magneticresonance spectroscopy
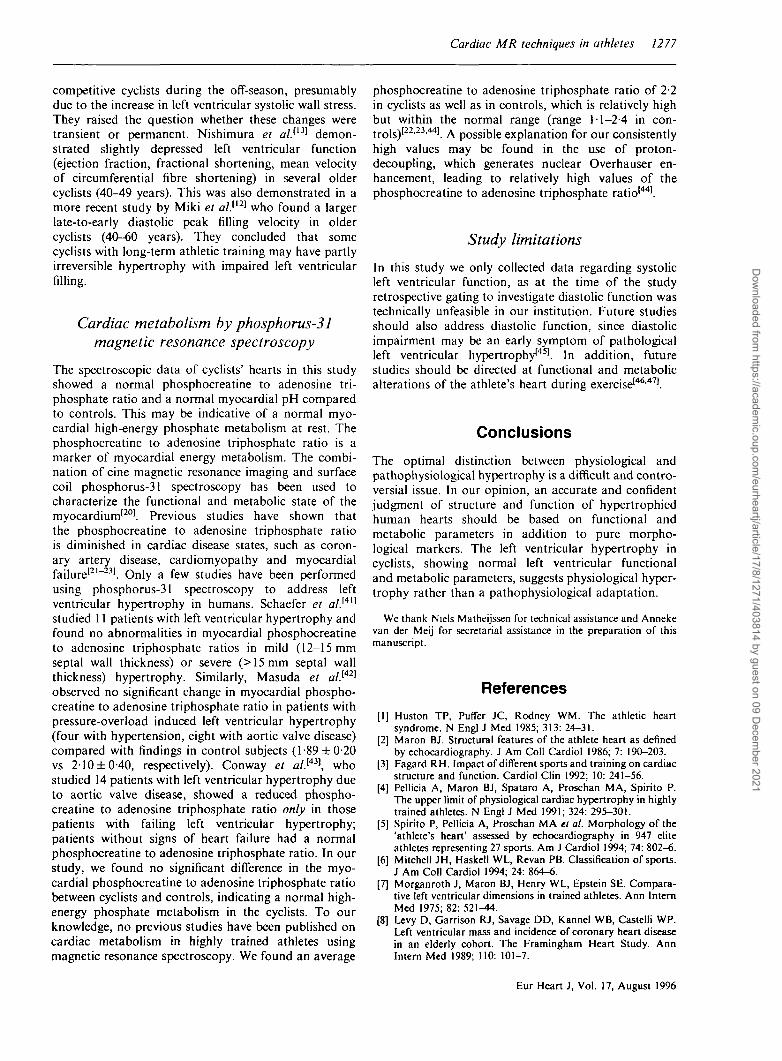
The myocardial phosphocreatine to adenosine tri-phosphate ratio after correction for blood and partialsaturation was not significant different between 13cyclists and four controls (2-2 ± 0-34 vs 2-2 ±017, ns)(Fig. 2). The displayed spectra were processed with a5 Hz line-broadening function and have a signal to noiseratio of approximately 14. The inorganic phosphatepeak was resolved in five cyclists with high spectralquality, allowing calculation of pH. Myocardial pH incyclists was normal (7-16 ±0-04, n = 5; reference value7-14±0-l)[3O-31].
Inter-observer and intra-observer variability
Measurement of left ventricular mass with magneticresonance imaging had an intra-observer variability of3-7% and an inter-observer variability of 4-4%.
Discussion
Our study is the first to use magnetic resonancetechniques to determine left ventricular mass, geometry,function, and metabolism of athletes' hearts in onecomprehensive study. We demonstrated that cyclistsshowed increased left ventricular mass, but withnormal geometry, normal left ventricular function, andnormal metabolic parameters. This suggests thepresence of physiological hypertrophy rather than apathophysiological adaptation in high trained cyclists.
Left ventricular morphology by magneticresonance imaging
Our results can be explained by the specific demands ofcycling, i.e. an increased cardiac output (volume-overload) and a raised blood pressure (pressure-overload) lasting up to 6 h a day*5"32"351. Fagard et al.[3S1
demonstrated an average systolic blood pressure incyclists of at least 200 mmHg at 70% of peak oxygenconsumption.
Few studies on magnetic resonance imaging ofcyclists' hearts have been reported. Milliken et al.l36]
Eur Heart J, Vol. 17, August 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021

7276 B. M. Pluim et al.
-10 -20
Ippm]
(b)Cyclist
2,3-DPG
dI V PDE
JUIA
PCr
1
XyATP
i
Kv v ^
rxATPiL
PCr/ATP = 2.00
(3ATP
A
10 -10 -20
[ppm]
Figure 2 Representative cardiac phosphoms-31 magnetic reso-nance spectroscopy spectrum of a normal subject (A) and of acyclist (B) with left ventricular hypertrophy. Comparison of thespectra shows no significant differences in PCr/ATP ratio. Theartifact between the PCr and the yATP resonances did not posea problem since spectral fitting in the time domain was used.ATP=adenosine triphosphate; PCr = phosphocreatine; 2,3-DPG = 2,3-diphosphoglycerate; PDE = phosphod icsters.
studied the hearts of endurance-trained athletes andincluded cyclists along with cross-country skiers andlong-distance runners, using magnetic resonanceimaging. Their data concerning left ventricular mass arein agreement with our results, showing a left ventricularmass of 258 g in cyclists, and 189 g in controls. Theauthors studied neither left ventricular geometry norleft ventricular function. Riley-Hagan et a/.1371, usingmagnetic resonance imaging, found a left ventricularmass of 160g in female cyclists compared to 115 g infemale control subjects. The authors'371 studied leftventricular geometry and found that female cyclists hada left ventricular mass to left ventricular end-diastolicvolume ratio within normal limits (1 -3 g . ml ~ '). In theirstudy, left ventricular function was not evaluated.
Left ventricular function by magneticresonance imaging
Our study shows that left ventricular systolic functionparameters, such as left ventricular ejection fraction,cardiac index, and systolic wall stress did not differsignificantly between cyclists and controls. To ourknowledge, the present study is the first magneticresonance imaging study on left ventricular function incyclists.
Normal systolic and diastolic function and wallstress in cyclists have been shown before132'33'38^401.However, few studies have demonstrated depressed leftventricular function in cyclists1'213-351. Fagard et al.[3S]
observed a decrease in left ventricular function in
Eur Heart J, Vol. 17, August 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021
Cardiac MR techniques in athletes 1277
competitive cyclists during the off-season, presumablydue to the increase in left ventricular systolic wall stress.They raised the question whether these changes weretransient or permanent. Nishimura et alP3] demon-strated slightly depressed left ventricular function(ejection fraction, fractional shortening, mean velocityof circumferential fibre shortening) in several oldercyclists (40-49 years). This was also demonstrated in amore recent study by Miki et al.ll2] who found a largerlate-to-early diastolic peak filling velocity in oldercyclists (40-60 years). They concluded that somecyclists with long-term athletic training may have partlyirreversible hypertrophy with impaired left ventricularfilling.
Cardiac metabolism by phosphorus-31magnetic resonance spectroscopy
The spectroscopic data of cyclists' hearts in this studyshowed a normal phosphocreatine to adenosine tri-phosphate ratio and a normal myocardial pH comparedto controls. This may be indicative of a normal myo-cardial high-energy phosphate metabolism at rest. Thephosphocreatine to adenosine triphosphate ratio is amarker of myocardial energy metabolism. The combi-nation of cine magnetic resonance imaging and surfacecoil phosphorus-31 spectroscopy has been used tocharacterize the functional and metabolic state of themyocardium'201. Previous studies have shown thatthe phosphocreatine to adenosine triphosphate ratiois diminished in cardiac disease states, such as coron-ary artery disease, cardiomyopathy and myocardialfailure121"231. Only a few studies have been performedusing phosphorus-31 spectroscopy to address leftventricular hypertrophy in humans. Schaefer et a/.14'1
studied 11 patients with left ventricular hypertrophy andfound no abnormalities in myocardial phosphocreatineto adenosine triphosphate ratios in mild (12-15 mmseptal wall thickness) or severe (>15mm septal wallthickness) hypertrophy. Similarly, Masuda et al.[42]
observed no significant change in myocardial phospho-creatine to adenosine triphosphate ratio in patients withpressure-overload induced left ventricular hypertrophy(four with hypertension, eight with aortic valve disease)compared with findings in control subjects (1-89 ±0-20vs 210 ±0-40, respectively). Conway et a/.1431, whostudied 14 patients with left ventricular hypertrophy dueto aortic valve disease, showed a reduced phospho-creatine to adenosine triphosphate ratio only in thosepatients with failing left ventricular hypertrophy;patients without signs of heart failure had a normalphosphocreatine to adenosine triphosphate ratio. In ourstudy, we found no significant difference in the myo-cardial phosphocreatine to adenosine triphosphate ratiobetween cyclists and controls, indicating a normal high-energy phosphate metabolism in the cyclists. To ourknowledge, no previous studies have been published oncardiac metabolism in highly trained athletes usingmagnetic resonance spectroscopy. We found an average
phosphocreatine to adenosine triphosphate ratio of 2-2in cyclists as well as in controls, which is relatively highbut within the normal range (range 11-2-4 in con-trols)[22-23>44!. A possible explanation for our consistentlyhigh values may be found in the use of proton-decoupling, which generates nuclear Overhauser en-hancement, leading to relatively high values of thephosphocreatine to adenosine triphosphate ratio'441.
Study limitations
In this study we only collected data regarding systolicleft ventricular function, as at the time of the studyretrospective gating to investigate diastolic function wastechnically unfeasible in our institution. Future studiesshould also address diastolic function, since diastolicimpairment may be an early symptom of pathologicalleft ventricular hypertrophy1451. In addition, futurestudies should be directed at functional and metabolicalterations of the athlete's heart during exercise146'471.
Conclusions
The optimal distinction between physiological andpathophysiological hypertrophy is a difficult and contro-versial issue. In our opinion, an accurate and confidentjudgment of structure and function of hypertrophiedhuman hearts should be based on functional andmetabolic parameters in addition to pure morpho-logical markers. The left ventricular hypertrophy incyclists, showing normal left ventricular functionaland metabolic parameters, suggests physiological hyper-trophy rather than a pathophysiological adaptation.
We thank Niels Matheijssen for technical assistance and Annekevan der Meij for secretarial assistance in the preparation of thismanuscript.
References
[1] Huston TP, Puffer JC, Rodney WM. The athletic heartsyndrome. N Engl J Med 1985; 313: 24-31.
[2] Maron BJ. Structural features of the athlete heart as definedby echocardiography. J Am Coll Cardiol 1986; 7: 190-203.
[3] Fagard RH. Impact of different sports and training on cardiacstructure and function. Cardiol Clin 1992; 10: 241-56.
[4] Pellicia A, Maron BJ, Spataro A, Proschan MA, Spirito P.The upper limit of physiological cardiac hypertrophy in highlytrained athletes. N Engl J Med 1991; 324: 295-301.
[5] Spirito P, Pellicia A, Proschan MA et a!. Morphology of the'athlete's heart' assessed by echocardiography in 947 eliteathletes representing 27 sports. Am J Cardiol 1994; 74: 802-6.
[6] Mitchell JH, Haskell WL, Revan PB. Classification of sports.J Am Coll Cardiol 1994; 24: 864-6.
[7] Morganroth J, Maron BJ, Henry WL, Epstein SE. Compara-tive left ventricular dimensions in trained athletes. Ann InternMed 1975; 82: 521-44.
[8] Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP.Left ventricular mass and incidence of coronary heart diseasein an elderly cohort. The Framingham Heart Study. AnnIntern Med 1989; 110. 101-7.
Eur Heart J, Vol. 17, August 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021

1278 B. M. Pluim et al.
[9] Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WPPrognostic implications of echocardiographically determinedleft ventricular mass in the Framingham Heart Study. N EnglJ Med 1990; 322: 1561-6.
[10] Rost R. The athlete's heart: historical perspectives. CardiolClin 1992; 10: 197-207.
[11] Linse J. Death travels along Sport International 1990; 4:4-12.
[12] Miki T, Yokota Y, Seo T, Yokoyama M. Echocardiographicfindings in 104 professional cyclists with follow-up study. AmHeart J 1994; 127: 898-905
[13] Nishimura T, Yamada Y, Kawai C. Echocardiographicevaluation of long-term effects of exercise on left ventricularhypertrophy and function in professional bicyclists.Circulation 1980; 61: 832-40.
[14] Carriere EGJ. Sudden death in elite sports. Netherlands HeartAssociation, The Hague, 1992
[15] Longmore DB, Underwood SR, Hounsfield GN et al.Dimensional accuracy of magnetic resonance in studies of theheart. Lancet 1985; 1: 1360-2
[16] Shapiro EP, Rogers WJ, Beyar R el al. Determination of leftventricular mass by magnetic resonance imaging in heartsdeformed by acute infarction. Circulation 1989; 79: 707-11
[17] Pattyname PMT, Lamb HJ, Van der Velde EA, Van der WallEE, De Roos A. Left ventricular measurements with cine andspine-echo MR imaging: a study of reproducibility withvariance component analysis. Radiology 1993; 187. 261-8.
[18] Markiewicz W, Sechtem U, Kirby R, Derugin N, Caputo GC,Higgins CB. Measurement of ventricular volumes in the dogby nuclear magnetic resonance imaging. J Am Coll Cardiol1987; 10: 170-7.
[19] Helak JW, Reichek N. Quantification of human left ventricu-lar mass and volume by two-dimensional echocardiography:in vitro anatomic validation. Circulation 1981; 63: 1398-407.
[20] Higgins CB, Saeed M, Wendland M, Chew WM. Magneticresonance spectroscopy of the heart-overview of studies inanimal and man. Invest Radiol 1989; 24' 962-8
[21] Weiss RG, Bottomley PA, Hardy CJ, Gerstenblith G.Regional myocardial metabolism of high-energy phosphatesduring isometric exercise in patients with coronary arterydisease. N Engl J Med 1990; 323: 1593-600
[22] Hardy CJ, Weiss RG, Bottomley PA, Gerstenblith G. Alteredmyocardial high-energy metabolities in patients with dilatedcardiomyopathy. Am Heart J 1991; 122: 795-801.
[23] Yabe T, Mitsunami K, Okada M, Morikawa S, Inubishi T,Kinoshita M. Detection of myocardial ischaemia by 3 IPmagnetic resonance spectroscopy during handgrip exercise.Circulation 1994; 89: 1709-16.
[24] Durnin JVGA, Rahaman MM. The assessment of the amountof fat in the human body from the measurements of skinfoldthickness. Br J Nutr 1967; 21: 681-9.
[25] Dulce MC, Mostbeck GH, Friese KK, Caputo GR, HigginsCB. Quantification of the left ventricular volumes andfunction with cine MR imaging: Comparison of geometricmodels with three-dimensional data. Radiology 1993; 188:371-6.
[26] Gaasch WH. Left ventricular radius to wall thickness ratio.Am J Cardiol 1979; 43: 1189-94.
[27] Arts T, Veenstra PC, Reneman RS. Epicardial deformationand left ventricular wall mechanics during ejection in the dog.Am J Physiol 1982; 243: H379-90.
[28] De Roos A, Doornbos J, Luyten PR, Oosterwaal LJMP,Van der Wall EE, Den Hollander JA. Cardiac metabolismin patients with dilated and hypertrophic cardiomyopathy:assessment with proton-decoupled P-31 MR spectroscopy.JMRI 1992; 2: 711-9.
[29] Den Hollander JA, Evanochko WT, Dell'Italia L, PohostGM. 31P NMR T, Inversion recovery measurements of thehuman heart. Proc Soc Magn Reson Med 1993; 3: 1098
[30] Bottomley PA, Herfkens RJ, Smith LS, Bashore TM. Alteredphosphate metabolism in myocardial infarction: P-31 MRspectroscopy. Radiology 1987; 165. 703-7.
[31] Wilson JR, Fink L, Maris J etnal. Evaluation of energymetabolism in skeletal muscle of patients with heart failurewith gated phosphorus-31 nuclear magnetic resonance.Circulation 1985; 71: 57-62.
[32] Douglas PS, OToole ML, Hiller WDB, Reichek N. Leftventricular structure and function by echocardiography inultraendurance athletes. Am J Cardiol 1986; 58: 805-9.
[33] Sepulveda F, De Oliveira E, De Oliveira PG et al. M-modeechocardiography study of twenty-two top class racingcyclists J Sports Med Phys Fitness 1989; 29: 136-40.
[34] Snoeckx LHEH, Abeling HFM, Lambregts JAC, SchmitzJJF, Verstappen FTJ, Reneman RS. Cardiac dimensions inathletes in relation to variations in their training program. EurJ Appl Physiol 1983; 52: 20-8.
[35] Fagard R, Aubert A, Lysens R, Staessen J, Vanhees L, AmeryA Noninvasive assessment of seasonal variations in cardiacstructure and function in cyclists. Circulation 1983; 67:896-901
[36] Milliken MC, Stray-Gundersen JS, Peshock RM, Katz J,Mitchell JH. Left ventricular mass as determined by magneticresonance imaging in male endurance athletes. Am J Cardiol1988; 62: 301-5.
[37] Riley-Hagan M, Peshock RM, Stray-Gundersen J, Katz J,Ryschon TW, Mitchell JH. Left ventricular dimensions andmass using magnetic resonance imaging in female enduranceathletes. Am J Cardiol 1992; 69: 1067-74.
[38] Bekaert I, Pannier JL, Van de Weghe C, Van Durme JP,Clement DL, Pannier R. Non-invasive evaluation of cardiacfunction in professional cyclists. Br Heart J 1981; 45: 213-8.
[39] Fagard R, Aubert A, Staessen J, Vanden Eynde E, Vanhees L,Amery A. Cardiac structure and function in cyclists andrunners. Br Heart J 1984; 52: 124-9.
[40] Schairer JR, Keteyian S, Henry JW, Stein PD. Left ventricularwall tension and stress during exercise in athletes andsedentary men. Am J Cardiol 1993; 71: 1095-8.
[41] Schaefer S, Gober JR, Schwartz GG, Twieg DB, Weiner MW,Massie B. In vivo phosphorus-31 spectroscopic imaging inpatients with global myocardial disease. Am J Cardiol 1990;65: 1154-61.
[42] Masuda Y, Tateno Y, Ikehira H et al. High-energy phosphatemetabolism of the myocardium in normal subjects andpatients with various cardiomyopathies. Jpn Circ J 1992; 56:620-6
[43] Conway MA, Alhs J, Ouwerkerk R, Niioka T, RajagopalanB, Radda GK. Detection of low phosphocreatine to ATP ratioin failing hypertrophied human myocardium by 31P magneticresonance spectroscopy. Lancet 1991; 338: 973-6.
[44] Bottomley PA. MR Spectroscopy of the human heart: thestatus and the challenges. Radiology 1994; 191: 593-612.
[45] Cuocolo A, Sax FL, Brush JE, Maron J, Bacharach SL,Bonow RO. Left ventricular hypertrophy and impaireddiastolic filling in essential hypertension. Circulation 1990; 81:978-86.
[46] Hittinger L, Patrick T, Ihara T et al. Exercise induces cardiacdysfunction in both moderate, compensated, and severehypertrophy. Circulation 1994; 89: 2219-31.
[47] Vatner SF, Shannon R, Hittinger L. Reduced subendocardialcoronary reserve. Circulation 1990; 81: HIS—III 14.
Eur Heart J, Vol. 17, August 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/8/1271/403814 by guest on 09 D
ecember 2021