cancers of the head and neck - uclahealth.org
TRANSCRIPT

5/11/2016
1
Cancers of the Head and Neck
Raquel Branom, DNP, RN, ACNS-BC
ObjectivesAt the end of this course, the participant will be able to:
Describe the normal anatomy and physiology of the head and neckDefine the most common cancers in head and neck patientsFormulate evidence based care plan for the post-operative head and neck patient
OverviewHead and neck cancers include cancers of the larynx (voice box), throat, lips, mouth, nose, and salivary glands.Most types of head and neck cancer begin in squamous cells that line the moist surfaces inside the head and neck (for example, the mouth, nose, and throat).Tobacco use, heavy alcohol use, and infection with the human papillomavirus (HPV) increase the risk of many types of head and neck cancer.
5/11/2016
2
OverviewMore than 90% of head and neck malignancies are squamous cell carcinomasTends to spread within the mucosaInvolve the lymph nodesDisfigurementPatients leave the hospital with radical changes in body functions, lifestyle, body imagePermanent or temporary alternation in communication, sound reception, taste, smell
Incidence and MortalityCancers of the head and neck account for 3% of all malignant cancersIncidence decreasing over last 30 yearsCancer of larynx decreasing each year since 1988Mortality rate still higher in African Americans
EtiologyAlcohol and tobacco
15X greater than non-smokers
InfectionsHuman papillomavirus-16 (HPV)Isolated in 36% of oral cavity cancers
Inflammatory cause
Genetic factors
• Mixing cured tobacco with betel nuts
– 2.8 times higher – 10 times if combined with
smoking• Dental factors• Endocrine disturbances• Radiation• Occupational exposures
5/11/2016
3
Cancers of the Head and Neck
TNM Classification for Glottic Cancer
T1: Tumor limited to vocal cords
T2: Tumor extends to supraglottis with impaired vocal cord mobility
T3: Tumor limited to the larynx, minor thyroid cartilage erosion
T4: Tumor invades thyroid cartilage and tissues beyond Larynx
Staging for Regional MetastasisNX: Regional lymph nodes cannot be assessedN0: No regional lymph node metastasis
N1: Metastasis in single ipsilateral lymph nodeN2: Metastasis to single lymph node 3-6 cm
N3: Metastasis in lymph node larger than 6 cmM1: Distant metastasis

5/11/2016
4
Test Your KnowledgeWhich of the following are risk factors for head and neck cancer?
Helicobacter pylori infection and history of herpes zosterHuman papillomavirus (HPV) infection, alcohol use, and all forms of tobacco usePetroleum cleaning solvents, asphalt paving, and painting suppliesGluten allergies and dairy allergies
Clinical FeaturesUnfortunately patients are most often identified only after development of symptoms at advanced stages of diseaseDiscomfort is the most common symptomExamination includes high risk sites
Lower lipAnterior floor of mouthLateral border of the tongueCervical and submandibular lymph nodes
Symptoms and Warning Signs
Any sore in the mouth or throat that does not healNeck or jaw pain that radiates to the earAbnormal growth in the mouthChange in mole or new skin lesion
• A lump in the neck that doesn’t go away
• Chronic cough or hoarseness
• Sore throat that does not improve
• Coughing up blood• Unilateral nasal
obstruction or bleeding

5/11/2016
5
Treatment• Whether to treat or not depends on
• Age
• Health status
• Advanced stage
• Local disease
• Chemotherapy
• Radiation therapy
• Surgery
• Combined therapies
• Full assessment will lead to one of the following
• Patient is potentially curable• Primary tumor is curable but
patient develops another illness• Patient is incurable but should
be treated• Patient is incurable and should
not be treated
Patient ProfileGenerally over 45 yearsYears of tobacco useYears of alcohol usePoor prognosis related to patients poor overall healthTumors developing in immunocompromised patients do not respond to any treatment modality
Test your KnowledgeThose diagnosed with head and neck cancer are at an increased risk for developing other primary tumors because of
The immunosuppressive side effects of treatment for head and neck cancerThe prolonged exposure of the mucosal surface to carcinogensHPV 16Repeated exposure to petrolatum products
5/11/2016
6
Cancer of the Mouth
Examination of the Mouth
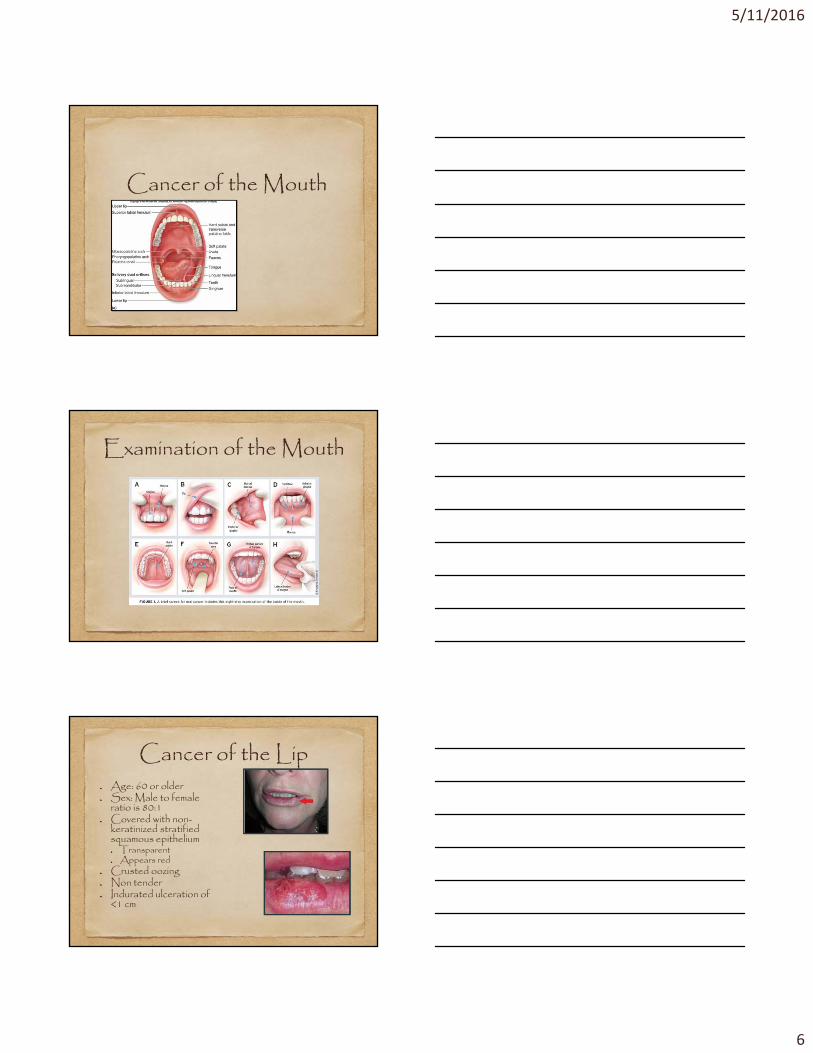
Cancer of the LipAge: 60 or olderSex: Male to female ratio is 80:1Covered with non-keratinized stratified squamous epithelium
TransparentAppears red
Crusted oozingNon tenderIndurated ulceration of <1 cm

5/11/2016
7
Cancer of the Buccal Mucosa Lump or non-healing ulcerWhite or red patches
LeukoplakiaBleedingPain or numbnessMetastasis by the submandibular lymph nodes on the lower deep cervical chain
Cancer of the Floor of the Mouth
Signs and SymptomsPainful or painless lesionRestricted tongue movementSlurred speechExcessive salivationLoosening or exfoliation of teeth
The floor is close to the skin and appears as a palpable lump in the submandibular areaLymphatic drainage through submandibular lymph nodes to upper deep cervical chains
Cancer of the TongueMiddle aged to elderly85% occurs on lateral borderPainless indurated mass or ulcerLesion may be infiltrated –small on the outside, but palpation shows deep invasionRisk factors
SmokingAlcoholSpicy foodSharp teethGlossitis

5/11/2016
8
Treatment for Lip and Oral Cancer
Early stage cancers (stage I and stage II)
Highly curableSurgery or radiationTreatment determined by functional and cosmetic results
Advanced stage cancer (stage III and stage IV)
Surgery and radiationConsider for clinical trials
• Survival– Advanced cancers have
increased chance of developing a second primary tumor of the aero digestive tract
Cancer of the Neck and Throat
Neck structuresHyoid bone
Cricoid cartilage
Tracheal rings
Thyroid isthmus
Lateral lobes of thyroid curves posteriorly around sides of trachea and esophagus

5/11/2016
9
Regions of the Pharynx
Cancer of the Nasopharynx• Often subtle initial
symptomsSlowly enlarging neck massOtalgia – ear acheHearing lossNasal obstruction
• Predisposing factors– Chinese ancestry
– Epstein-Barr virus exposure
– Heavy alcohol intake• Not linked to tobacco or
alcohol Older age and male
Cancer of the OropharynxUncommonAge 50-70Males more than femalesSoft palate and oropharyngeal mucosaRisk factors
SmokingHPV infection
Symptoms: DysphagiaPain and radiating to ear

5/11/2016
10
Cancer of the HypopharynxUncommonAge 50-60Tends to be aggressive
High rate of distant spread>50% of patients have positive cervical nodes
SymptomsSore throatEar pain“lump in throat”Marked weight loss
Generally poor prognosis
Prognosis and Treatment OptionsChronic pulmonary and hepatic diseases related to excessive tobacco and alcohol usePoor prognosis related to
Presentation at late stageMultisite involvementExcessive regional lymphatic networkRestricted surgical options for complete resection
Surgery followed by radiotherapyTreatment failures occur within first 2 years after definitive surgery
Cancer of the Larynx (Voice Box)MalesAge 60 and aboveSmoking and alcohol25% of patients diagnosed with laryngeal cancers have another cancer
Mouth, esophagus, lung15% will later develop cancer in one of these areasHighest risk for recurrence in first 2-3 years

5/11/2016
11
Cancer of the LarynxSymptoms
Hoarseness of voiceLump in the neckSore throat or ear acheDifficulty breathingPain and difficulty in swellingPain is a late sign
Prognosis and Treatment OptionsSmall cancers without spread to lymph nodes have very good cure rates 75%-95%Treatment goal is to preserve the larynxRadiotherapySurgery
Complete or total laryngectomyRadical neck dissection
Total LaryngectomyInvolves removal of epiglottis, thyroid cartilage, vocal cords, hyoid bone, cricoid cartilage and 2-3 tracheal rings
Indicated in bilateral and extensive lesions of the vocal cords
Patient will have a permanent laryngeostome or “neck stoma or hole”
Voice is not preserved

5/11/2016
12
Total Laryngectomy Trach Care
AssessmentAirwayStoma
Trach assessmentCuffed vs uncuffedSutures vs trach tiesInner cannula: disposable vs reusableAir humidity
Test Your KnowledgeMr. R. is a 73 year old chicken farmer. He is in for pre-op work up for scheduled radical neck dissection. Mrs. R reports they do not understand why Mr. R. needs to have his neck operated on when he only had the lump under his tongue. He has had many tests, which have “only found a few spots on his bones”. You know that:
Test Your KnowledgeHis disease has likely spread to the lymphatics and the bone
The surgery on his neck will allow placement for a tracheostomy tube
The neck surgery is needed for placement of a PEG feeding tube
The disease has spread to the lymph nodes; the surgery will stop this spread

5/11/2016
13
General Nursing ConceptsAirway assessmentFlap and graft assessments
Neck dressingIncisionDoppler checks for circulationGraft donor dressing
Neuro status Changes from baselineTics, tremors
Radical Neck Dissection
General Nursing ConceptsTrach Management
Suction Stoma careOxygenHumidification

5/11/2016
14
General Nursing ConceptsManaging complications
Airway obstructionmucous plug
Suctioning
Maintaining humidityInfection
Incisional careFlap and skin graft donor sites
Circulation
Flap viabilityDoppler checks