cáncer colorrectal: nueva clasificación molecular. ¿qué ... · cáncer colorrectal: nueva...
TRANSCRIPT

Cáncer colorrectal: Nueva clasificación molecular.
¿Qué hacemos ahora? Implicaciones en la práctica asistencial
Dr. Ramon Salazar
Institut Català d’Oncologia
L’Hospitalet de Llobregat, Barcelona

2
– CIN, MSI (dMMR) – Individual mutations/amplifications/fusions….
• (RAS/BRAF…)
– Supervised signatures • (Oncotype/Coloprint…)
– CRCSC Consensus Classification • (Intrinsec subtypes)
PROGNOSIS & PREDICTION
Clinical setting
Molecular criteria (tumor)

MSI (stage II/III) – ACCENT DBase
MMR data available in 7803 patients (IHC and/or MSI testing)
Sargent et al., ASCO Annual Meeting 2014
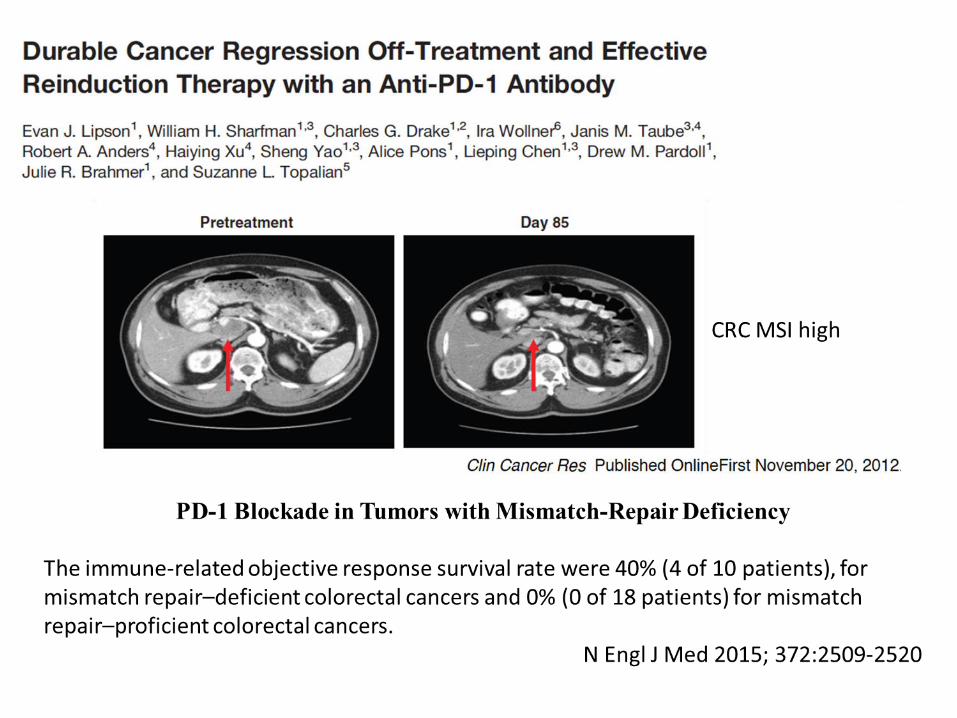
Stage II: MSI Good Prognosis 5FU no benefit in MSI & marginal benefit in MSS
Stage III: MSI Good Prognosis 5FU benefits both MSI and MSS

• MSI & BRAF: poor prognostic after relapse • Oxaliplatin: benefits stage III both MSS & MSI,
no benefit in stage II
C07 (FULV+/-Ox) and C08 (Ffox+/-Bev):
Stage II and III Colon Cancer
Gavin P G et al. Clin Cancer Res 2012;18:6531-6541 *Pogue-Geile K et al, JNCI 2013: 105 , 989-992
5

Phase 1B study of vemurafenib in combination with irinotecan and cetuximab in
patients with BRAFV600E-mutated advanced cancers and metastatic colorectal cancer
David S. Hong1, Van Morris2, Badi El-Osta1, Siqing Fu1, Michael Overman2, Sarina Piha-Paul1, Vivek Subbiah1, Bryan Kee2, Apostolia Tsimberidou1, Ralph Zinner1, David Fogelman2, Jorge Bellido1, Imad Shureiqi2, Funda
Meric-Bernstam1, Scott Kopetz2
ASCO 2015

Responses by HER2 IHC Score
Presented By Salvatore Siena at 2015 ASCO Annual Meeting
35% RR 78% Dis. control
HERACLES TRIAL A: Lapatinib + Herceptin in HER ++/+++ Fish >50%

8
– CIN, MSI (MMR)/CIMP/hypermutated – Individual mutations
• (RAS/BRAF…)
– Prognostic Signatures (stage II) • (Supervised trainning e.g. Oncotype/Coloprint…)
– CRCSC Consensus Classification • (Intrinsec subtypes)
PROGNOSIS & PREDICTION
Molecular criteria (tumor)

Multivariable Analysis: Relationship of RS, T Stage, and MMR with Risk of Recurrence
Venook et al., J Clin Oncol 2013
ONCOTYPE DX® IN CALGB 9581
The 12-gene RS was calculated by using the prespecified genes and algorithm previously validated in QUASAR
Recurrence risk groups
% patients 5-year RR
Low RS 44% 13% (10% - 16%)
Int RS 34% 16% (13% - 19%)
High RS 22% 21% (16% - 26%)
Subgroup analysis in T3-MSS patients
Recurrence risk groups
% patients 5-year RR
Low RS NR 12% (10% - 15%)
Int RS NR 15% (12% - 17%)
High RS NR 18% (14% - 22%)
Recurrence risk in the overall population. NR = not reported
CALGB 9581 trial: edrecolomab vs observation – stage II colon cancer
ONCOTYPE DX® IN NSABP C07 (FULV+/-Ox) st II & III

Multivariable Analysis: Relationship of RS, T Stage, and MMR with Risk of Recurrence
Venook et al., J Clin Oncol 2013
ONCOTYPE DX® IN CALGB 9581
The 12-gene RS was calculated by using the prespecified genes and algorithm previously validated in QUASAR
Recurrence risk groups
% patients 5-year RR
Low RS 44% 13% (10% - 16%)
Int RS 34% 16% (13% - 19%)
High RS 22% 21% (16% - 26%)
Subgroup analysis in T3-MSS patients
Recurrence risk groups
% patients 5-year RR
Low RS NR 12% (10% - 15%)
Int RS NR 15% (12% - 17%)
High RS NR 18% (14% - 22%)
Recurrence risk in the overall population. NR = not reported
CALGB 9581 trial: edrecolomab vs observation – stage II colon cancer
ONCOTYPE DX® IN NSABP C07 (FULV+/-Ox) st II & III

Algorithm for chemotherapy decision
Stage III Stage II
FOLFOX
NO MSI Determination
needed
Colon Cancer
MSS
CT may be discussed Other Markers: T3/T4, Other Factors: age, patient wish...
Prognostic signatures?*
MSI
NO CT Good prognosis, resistance to FU

Algorithm for chemotherapy decision
Stage III Stage II
FOLFOX
NO MSI Determination
needed
Colon Cancer
MSS
CT may be discussed Other Markers: T3/T4, Other Factors: age, patient wish...
Prognostic signatures?*
MSI
NO CT Good prognosis, resistance to FU
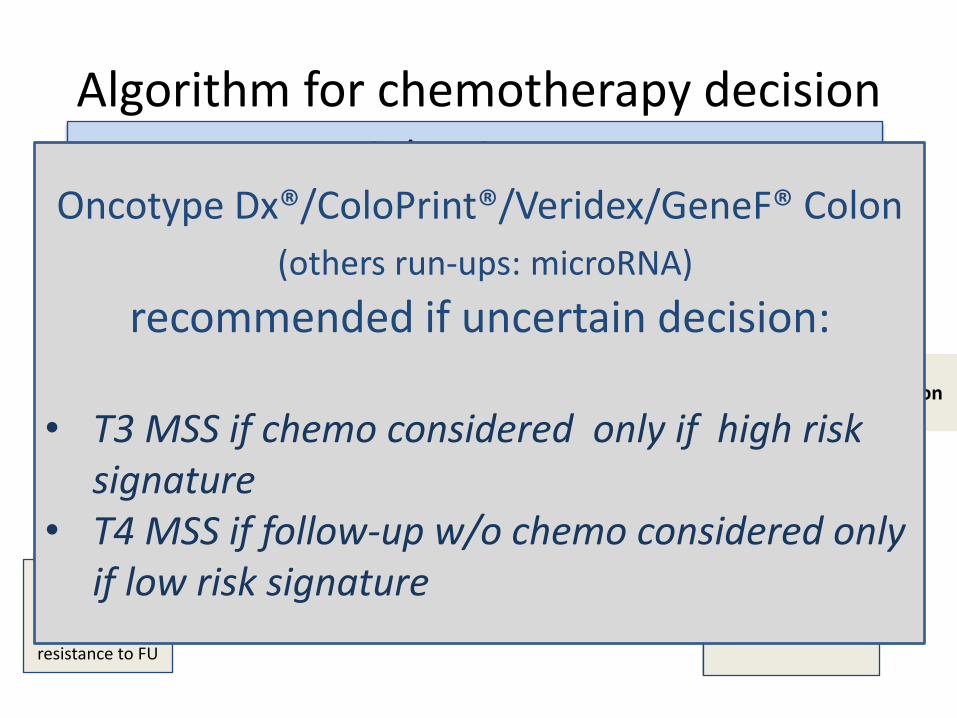
Oncotype Dx®/ColoPrint®/Veridex/GeneF® Colon
(others run-ups: ColoStage, microRNA, CDX2)
recommended if uncertain decision:
• T3 MSS if chemo considered only if high risk signature
• T4 MSS if follow-up w/o chemo considered only if low risk signature

CRCSC – Original Individual Group Classifiers

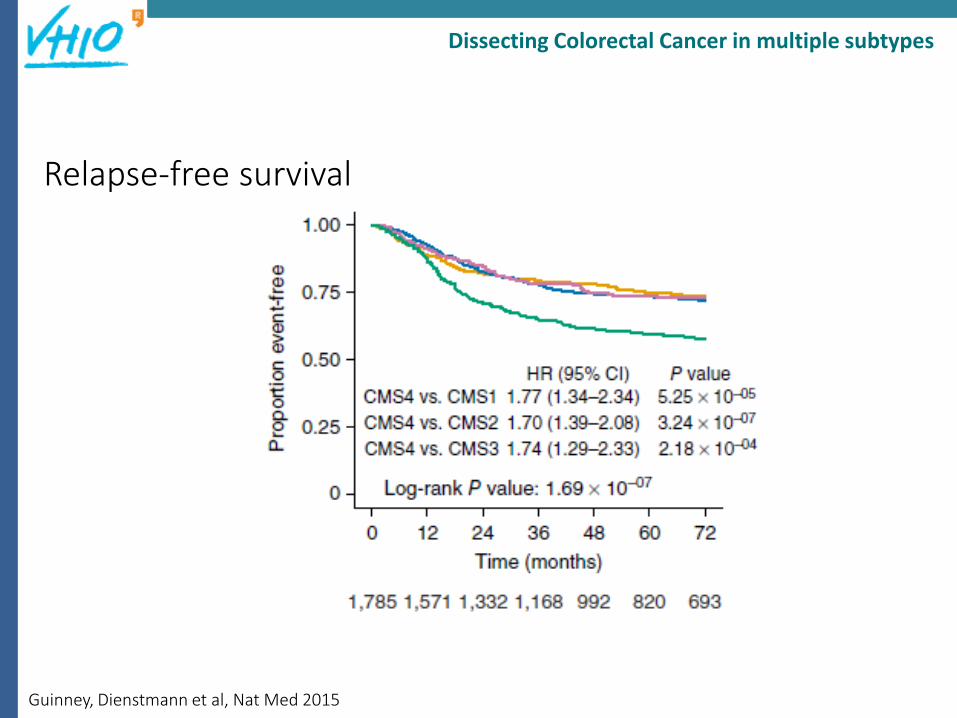
Guinney, Dienstmann et al, Nat Med 2015
Dissecting Colorectal Cancer in multiple subtypes

Proposed taxonomy of colorectal cancer
Prognosis
Liver Surgery
outcome? ?
Guinney, Dienstmann et al, Nat Med 2015
Relapse-free survival
Dissecting Colorectal Cancer in multiple subtypes

A BC
Salazar et al, J Clin Oncol 2011: 29:17-24

Guinney, Dienstmann et al, Nat Med 2015
Survival after relapse
Dissecting Colorectal Cancer in multiple subtypes

Guinney, Dienstmann et al, Nat Med 2015
Dissecting Colorectal Cancer in multiple subtypes
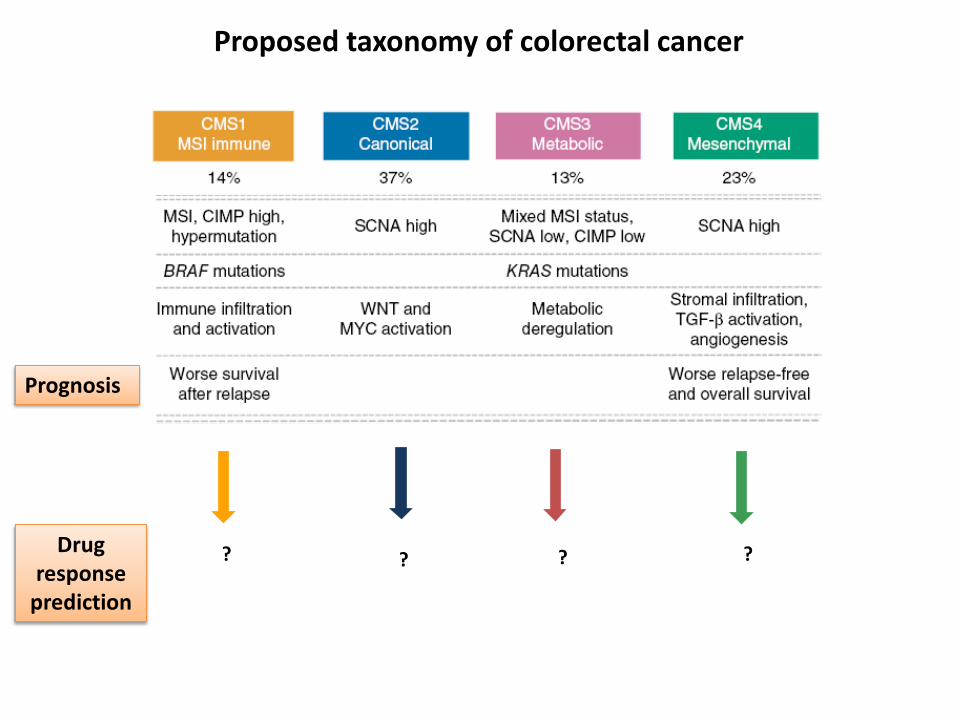
Proposed taxonomy of colorectal cancer
?
Prognosis
Drug response
prediction
? ? ?

Supervised immune and stromal infiltration analysis
Becht et al, Clin Car Res 2016
CMS1 CMS2 CMS3 CMS4
Dissecting Colorectal Cancer in multiple subtypes

Supervised immune infiltration analysis
Becht et al, Clin Car Res 2016
CMS1 CMS2 CMS3 CMS4
Dissecting Colorectal Cancer in multiple subtypes

6 cells
Unpublished
Broad Institute Pharmacogenomic collection
Dissecting Colorectal Cancer in multiple subtypes

Proposed taxonomy of colorectal cancer
Inmune checkpoints
blockade
TGF-
inhibition + Inmune
checkpoint blockade
Prognosis
Drug response
prediction
Metabolism &
DNA damage
Oncogene drivers
Amplifications

Summary
• Prognostic Clinically Relevant Molecular Variables – MSI in Stage II – BRAF and MSI in stage IV – Supervised & Intrinsec Signatures?
• Predictive Clinically Relevant Molecular Variables – MSI in stage II (5FU) and IV (PD1) – RAS and BRAF in stage IV – CMS 1-4 (Clinical Trials) – Still unknown what combination of genomic features
(mutation + MSI + gene expression + immune + stromal) will provide will provide the best prediction of drug response.

CRSC:

Acknowledgements & Collaborations Agendia
Iris Simon
Paul Roepman
Annuska Glas
Sun Tian
Laura V´Veer
IDIBELL CRC Group, HUB & ICO CRTeam
Víctor Moreno
Adriana López-Doriga
Rebeca Sanz-Pamplona
Susanna Aussó,
UMC Leiden
Rob Tollenaar
Wilma Mesker
H. Del Mar BCN
Clara Montagut
NKI R. Bernards Lab
Anirudh Prahallad
Begoña Diosdado
Magali Michaut Slotervaart Hospital
Johan Westerga
Sjoerd Bruin
Rechts der Isar Munich Robert Rosenberg Ulricht Nitsche
Hospital Gasthuisberg Leuven Sabine Tejpar
Swiss Inst Bioinformat
Vlad Popovici Mauro Delorenzi
VHIO BCN
Josep Tabernero
Rodrigo Dienstmann
E.Élez, Fiorella Ruiz, Ariadna Garcia, Marta Vilaro,
Gabriel Capellà
Alberto Villanueva
Dani Azuara
M. Nadal, M. Martínez
E. Kreisler, S.Biondo
Xavier Sanjuan
Antonio Soriano
Cristina Santos
Gemma Soler
Merche Martínez V.
Alex Teulé
Julieta Grasselli
Xavi Pérez
JL Manzano
UBB
LRT UGR
HUB UFCCR
ICO CRT
SOM UIC
IRB
E Batlle E.Sancho
Idibell M Esteller G.Thomas
MDACC S. Kopetz

BACK up slides….

Other RAS mutations: CRYSTAL & OPUS
Ciardiello F et al. Ann Oncol 2014; Tejpar S et al. Ann Oncol 2014
Study N Method Sensitivity Other RAS
mt, %
CRYSTAL 430 BEAMing† 0.01% 14.7
OPUS 118 BEAMing† 0.01% 26.3
FIRE-3 407 Pyrosequencing 1-5% 16.0
PRIME 620 Dideoxy sequencing/WAVE 5% 17.4
PEAK 221 Dideoxy sequencing/WAVE 5% 23.1

RAS mutations: Which is the right
sensitivity cut-off?
Ciardiello F et al. Ann Oncol 2014
?
?

Cobas 4800 (ROCHE) – Cobas Kits Sensitivity 1-5%
PyroMark (QIAGEN) – TherascreenPyro Kits Sensitivity 1%
BioMark Digital PCR Arrays (Fluidigm) Sensitivity 0.1%
LightCycler 480 Sensitivity 1-5 %
Sensitivity 5-10%
The puzzle of RAS testing
Slide provided by R. Salazar
BEAMing Sysmex Inostics Sensitivity 0.01%

Response to anti-EGFR according to fraction of mutant
alleles by quantitative digital PCR
CR n=1
PR n=29
SD n=26
PD n=37
% o
f m
uta
ted
alle
les
p<0.005
D.Azuara, C. Santos, et al. Nanofluidic digital PCR and extended genotyping of RAS and BRAF for improved selection of metastatic colorectal cancer patients to anti-EGFR therapies
MOLECULAR CANCER THERAPEUTICS. In Press

D.Azuara, C. Santos, et al. Nanofluidic digital PCR and extended genotyping of RAS and BRAF for improved selection of metastatic colorectal cancer patients to anti-EGFR therapies
MOLECULAR CANCER THERAPEUTICS. In Press
Improvement in response prediction by assessing mutation status of each gene

Vilar E & Tabernero J, Nature 2012
“Under pressure” clonal selection vs evolution

35
Treatment of Resistance (primary or secondary)
in present or future clinical trials
RAS mutants:
Cetuximab + Irinotecan in KRAS G13D mutant CRC….
MEK inhibitors + pan HER inhibitors
BRAF mutants:
BRAF + EGFR + PIK3Ca or WNT inhibitors
S492R mutants:
Panitumumab
C-MET amplifications
C-MET inhibitors ?
Tumor debulking in unresectable metastasic disease
proof of principle cfDNA load as surrogate endpoint of
effective debulking of clones with resistance potential

QUASAR col. group, Lancet 2007
Adjuvant chemotherapy - benefit
QUASAR

Risk stratification in stage II colon cancer
• Clinicopathological features
• Microsatellite instability, KRAS and BRAF
• Supervised Prognostic signatures – Do gene signatures currently add information to the decision making
progress?
• Intrinsic molecular subtypes

ACCENT – MSI (stage II)
MMR data available in 7803 patients (IHC and/or MSI testing)
Sargent et al., ASCO Annual Meeting 2014
dMMR patients had better outcome without adjuvant treatment 5FU resistance should not be considered for chemo

ACCENT – MSI (stage III)
Treated dMMR stage III retained favourable prognosisMMR should not guide decission in stage III
MOSAIC and NSABP-C07
Sargent et al., ASCO Annual Meeting 2014 *Gavin PG et al., Clin Cancer Res 2012; Fléjou JF et al., ASCO Annual Meeting 2013
Oxaliplatin seem to benefit equally both MSS and MSI patients*
both MSI and MSS should be considered for chemo (OXL based)

• MSI: prognostic factor with HR 0.48 for RFS (and OS) • MSI: oxaliplatin similar benefit in pMMR and dMMR • BRAF (& MSI): poor prognostic after relapse • MSI: predictive of BEV benefit OS HR 0.52 p:0.02 favours BEV *
C07 (FULV+/-Ox) and C08 (Ffox+/-Bev):
Stage II and III Colon Cancer
Gavin P G et al. Clin Cancer Res 2012;18:6531-6541 *Pogue-Geile K et al, JNCI 2013: 105 , 989-992

Stage II and III dMMR MOSAIC study
Fléjou JF, ASCO 2013
100
80
20
40
60
0
RFSprobability(%)
109876543210Time(years)
LV5FU2FOLFOX4
LV5FU2FOLFOX4
5144
4440
4039
4038
3738
3737
3636
3235
2934
2732
2026
Nbatrisk
100
80
20
40
60
0
DFSprobability(%)
109876543210Time(years)
LV5FU2FOLFOX4
5144
4440
4039
4038
3738
3737
3636
3235
2934
2732
2026
109876543210Time(years)
LV5FU2FOLFOX4
5144
4741
4540
4339
4239
4139
3938
3437
3136
2924
2228
100
80
20
40
60
0
0Sprobability(%)
109876543210Time(years)
LV5FU2FOLFOX4
2918
2315
2015
2014
1814
1814
1813
1612
1511
1411
119
100
80
20
40
60
0DFSprobability(%)
109876543210Time(years)
LV5FU2FOLFOX4
2226
2125
2024
2024
1924
1923
1823
1623
1423
1321
917
100
80
20
40
60
0
DFSprobability(%)
STADESII&III
DFSRFS OS
STADEIIISTADEIIDFS DFS
LV5FU2FOLFOX4
Nbatrisk
LV5FU2FOLFOX4
Nbatrisk

Algorithm for chemotherapy decision
Stage III Stage II
FOLFOX
NO MSI Determination
needed
Colon Cancer
MSS
CT may be discussed Other Markers: T3/T4, BRAF, KRAS?
Other Factors: age, patient wish... Prognostic signatures?*
MSI
NO CT Good prognosis, resistance to FU

Algorithm for chemotherapy decision
Stage III Stage II
FOLFOX
NO MSI Determination
needed
Colon Cancer
MSS
CT may be discussed Other Markers: T3/T4, BRAF, KRAS?
Other Factors: age, patient wish... Prognostic signatures?*
MSI
NO CT Good prognosis, resistance to FU
*Are gene signatures ready for use in the selection of patients
for adjuvant treatment?

Kerr et al., ASCO Annual Meeting 2009 Gray et al., J Clin Oncol 2011
ONCOTYPE DX® IN QUASAR
Recurrence risk groups
% patients 3-year RR
Low RS 43.7% 12% (0% - 16%)
Int RS 30.7% 18% (13% - 24%)
High RS 25.6% 22% (16% - 29%)

Multivariable Analysis: Relationship of RS, T Stage, and MMR with Risk of Recurrence
Venook et al., J Clin Oncol 2013
ONCOTYPE DX® IN CALGB 9581
The 12-gene RS was calculated by using the prespecified genes and algorithm previously validated in QUASAR
Recurrence risk groups
% patients 5-year RR
Low RS 44% 13% (10% - 16%)
Int RS 34% 16% (13% - 19%)
High RS 22% 21% (16% - 26%)
Subgroup analysis in T3-MSS patients
Recurrence risk groups
% patients 5-year RR
Low RS NR 12% (10% - 15%)
Int RS NR 15% (12% - 17%)
High RS NR 18% (14% - 22%)
Recurrence risk in the overall population. NR = not reported
CALGB 9581 trial: edrecolomab vs observation – stage II colon cancer
ONCOTYPE DX® IN NSABP C07 (FULV+/-Ox) st II & III

ColoPrint®
HR = 3.41 (P> 0.0001) 5-year DMFS 82%(95CI, 76-89%) low-risk 50%(95CI, 38-66%) high-risk
30%
DM
FS
Whole Genome analysis on 44K Agilent microarrays
70% N = 188 (SI:24; SII:100; SIII:56; SIV:8) RC: 92; LC:74; Rectum: 17)
No Chemo: 145; Chemo: 31
18 gene signature
18 genes identified that correlate Distant Metastasis-free Survival, 18 most stable genes selected
Salazar et al., J Clin Oncol 2011

Algorithm for chemotherapy decision
Stage III Stage II
FOLFOX
NO MSI Determination
needed
Colon Cancer
MSS
CT may be discussed Other Markers: T3/T4, BRAF, KRAS?
Other Factors: age, patient wish... Prognostic signatures?*
MSI
NO CT Good prognosis, resistance to FU
Algorithm for chemotherapy decision
Stage III Stage II
FOLFOX
NO MSI Determination
needed
Colon Cancer
MSS
CT may be discussed Other Markers: T3/T4, BRAF, KRAS?
Other Factors: age, patient wish... Prognostic signatures?*
MSI
NO CT Good prognosis, resistance to FU
Oncotype Dx®/ColoPrint®/Veridex/GeneF® Colon
(others run-ups: microRNA)
recommended if uncertain decision:
• T3 MSS if chemo considered only if high risk signature
• T4 MSS if follow-up w/o chemo considered only if low risk signature