canadian journal - csmls · csmls receives feedback through written correspondence, email and...
TRANSCRIPT

English Edition2011 vol 73 no 3
JOURNALof medical laboratory science
canadian
Official publication of:
PM #
4078
7580
Direct-To-ConsumerGenetic Testing
PEI Gets Government Attention
ValidationOf ProthrombinTime Reagent:Where Are We?

REGISTER before December 31 to take advantage of 2011 early bird rates AND become eligible to win a FREE LABCON registration.
CSMLS’s National Conference of Medical Laboratory ScienceCongrès national de science de laboratoire médical de la SCSLM
June 2 - 4, 2012 · Gatineau, QC
Let LABCON2012 be the vital piece of your professional development plan.VISIT csmls.org/labcon2012
REGISTERNOW!
REGISTER before December 31 to take advantage of 2011 early bird rates AND become eligible to win a FREE LABCON registration.
CSMLS’s National Conference of Medical Laboratory ScienceCongrès national de science de laboratoire médical de la SCSLM
June 2 - 4, 2012 · Gatineau, QC
Let LABCON2012 be the vital piece of your professional development plan.VISIT csmls.org/labcon2012
REGISTERNOW!

CJMLS Fall 2011 | 1
Editorial tEamMichael Grant, Christine Nielsen
Michelle Squarciotta
ContributorsCathy Bouwers, William Brien,
Allison Caisey, Vanessa ChanMarion Fraser, Michael Grant,
Stephanie Harper, Marilyn Johnston,Roberta Martindale,
Chinedu Ogbonna, Gene Shematek,Arlene L. Thiessen,Christopher Ward
Editorial and businEss offiCEPO Box 2830 LCD 1
Hamilton, ON L8N 3N8 Phone: (905) 528-8642 FAX: (905) 528-4968
e-mail [email protected]
CouriEr addrEss33 Wellington Street North Hamilton, ON L8R 1M7
PublisHEd bY:
www.mediaedgepublishing.com
Toll Free: (866) 216-0860 5255 Yonge Street, Suite 1000
Toronto, ON M2N 6P4
PublisHErMichael Bell
PublisHEr’s statEmEnt and PoliCYThe Canadian Journal of Medical Laboratory Science (the Journal) is owned and published by the Canadian Society for Medical Laboratory Science (CSMLS). Canada Post Publications Mail Agreement #40063021.
Papers are accepted by the Canadian Journal of Medical Laboratory Science on the understanding that they have not been published elsewhere. The publishers accept no responsibility for opinions expressed by contributors. Contents may be reproduced only with permission.
The Journal is a quarterly publication. Subscriptions are complimentary for CSMLS members. Subscription is $24 per year in Canada, $35 in the USA and $45 for all other countries. Current issues are available at $6.00 each.
Advertising inquiries, orders and production material can be sent via e-mail to [email protected]. Advertising rates are available online at www.csmsl.org/cjmls.
Return Postage Guaranteed
issn 1207-5833 PrintEd in Canada
in focus
Executive Director’s Message
2-3
The Inbox 4-5
Promoting Awareness With The Next Generationby Cathy Bouwers 6
PEI Gets Government Attentionby Cathy Bouwers 6
Direct-To-Consumer GeneticTesting (DCGT): Dangerous OrEmpowering The Publicby Chinedu Ogbonna 9-11
Maintaining the Schedule of Unit Values for the Clinical Laboratory Workload Measurement Systemby Arlene L. Thiessen 12-14
PERsPEcTiVEs
A Safety Perspective Measuring Safety Performance in the Laboratoryby Gene Shematek 16-17
An Educator’s Perspective How Effective Are Your Questions When Training Students On The Bench?by Roberta Martindale, Christopher Ward and Marion Fraser 18
A Student’s Perspective 10 Things Lab Students Value Most During Their Clinical Rotationby Stephanie Harper 19
A Perspective from “the Bench” Hard Decisions: Returning from Maternity Leaveby Allison Caisey 20-21
sciEnTific sEcTion
Validation of Prothrombin Time (INR) Reagent: Where are we?by Vanessa Chan, Marilyn Johnston, William Brien
24-28
sociETy nEws
Looking back at LABCON2011by Michael Grant
32-34
LABCON Hotline
35
Website Renovation
35
What does 75 years of CSMLS mean to you?
36
CSMLS – The National Voice of Canada’s Medical Laboratory Profession
36
JOURNALof medical laboratory science
canadian
REGISTER before December 31 to take advantage of 2011 early bird rates AND become eligible to win a FREE LABCON registration.
CSMLS’s National Conference of Medical Laboratory ScienceCongrès national de science de laboratoire médical de la SCSLM
June 2 - 4, 2012 · Gatineau, QC
Let LABCON2012 be the vital piece of your professional development plan.VISIT csmls.org/labcon2012
REGISTERNOW!

2 | CJMLS Fall 2011
Message from the Executive Director
Christine Nielsen, Executive Director
The Power of community
community. We at CSMLS often refer to the medical laboratory community when
we speak about all of the dedicated people working in Canadian laboratories, whether they are members of CSMLS or not. We do this because we believe that there is
the laboratory community. I respectfully disagree. Signs of this community are all around us. We simply need to look for them.
This is our first issue since LABCON2011 and I would be remiss if I did not point to this event as a sterling example of the
a common connection between all of us; a shared set of goals, values and aspirations that unify us as a collective — a community.
Recently a member challenged us on the use of this term, stating that there is no such thing as
lab community at work. In early June, I was fortunate to witness hundreds of lab professionals come together in Halifax to learn, laugh and grow.
If you ask the organizers what draws members to LABCON,
they would likely answer that it is dynamic and relevant educational content that attracts people. Often, when we poll attendees, we hear that it is the social events that are key. Our marketing folks might tell you that it is the advertising that gets people into the seats. Who can resist a giant recurring lobster after all?
While all these perspectives are valid, I would argue that there is something more to LABCON than educational sessions and social events. It is the act of coming together itself that engages people. It is the chance to see former colleagues and forge new relationships with people you’ve just only met. This is possible because we share the same reasons for entering, and staying in, this profession. We have a connecting passion about our work. We
“ Our marketing folks might tell you that
it is the advertising that gets people
into the seats.”

take comfort in sharing success, challenges and the occasional war story with each other. We are a community.
This community can do great things when we work together. Back in March we proved this with the success of the Knowing Matters campaign (visit www.knowingmatters.ca to see the campaign), which generated over a million media impressions.
And yet, many of our members have expressed a feeling that we are a small and relatively powerless group when it comes to raising awareness or advocating with government and hospital administrators. Regardless of our size, we will only see success on a national level if we band together and create a united front.
We have certainly seen success
at a provincial level. The Prince Edward Island Society for Medical Technologists (PEISMT) has recently seen their advocacy efforts
result in umbrella legislation that will see MLTs become a regulated health profession in that province. See page 7 for more information on how this came about.
Author Vista Kelly wrote, “Snowflakes are one of nature’s most fragile things, but just look at what they can do when they stick together.” It is an appropriate metaphor for our community.
country, with the power to raise awareness, pressure government and affect meaningful change.
It is time to stop feeling like we are all alone. Let’s start talking about the issues that are facing the entire profession and how we can address them together. Change is possible, and it all starts with our community.
Individually you may only be one person in a lab. Together we are a community of over 30,000 laboratory professionals across the
CJMLS Fall 2011 | 3
Message from the Executive Director
“ Regardless of our size, we will only see
success on a national level if we band
together and create a united front.”

4 | CJMLS Fall 2011
The inboxIn Focus
The Inbox is a new addition to the Canadian Journal of Medical Laboratory Science and is meant to provide a public forum for us to address questions, concerns or issues that are raised by members. CSMLS receives feedback through written correspondence, email and through our various social media portals. If you have a question or comment you would like to have addressed in an upcoming issue, talk to us on Facebook, Twitter or through email at [email protected].
Q. I saw the new CSMLS logo in the last journal. This is the third logo that CSMLS has had over the course of my career. Why keep changing?
A. Almost all of your favourite brands have seen logo changes throughout their history. Did you know that Apple’s first logo depicted Isaac Newton underneath an apple tree? As industries and organizations change over time, those changes are often reflected in an organization’s logo. These changes can be subtle evolutions or complete revisualizations. Pepsi, for example, has had eleven distinct logos over the organization’s history.
Similarly, as CSMLS has evolved over the years, our logo has changed to reflect that evolution. The recent logo change would fit into the evolution category rather than a revisualization. The new logo was designed to encapsulate the essence, credibility and
familiarity that some members felt about the previous logo, while modernizing the logo to appeal to the next generation of members.
We understand that members are often fond of the logo that was in use when they joined the society. Over time it becomes a meaningful symbol and letting go of it can be difficult. With the new logo we are not letting go
of the past, but rather bringing our visual identity up to date to better reflect the profession and the society.
A member put it very well in a response to a 2011 survey: “The lab world is changing; CSMLS should be changing and adapting.” It is with that spirit that we move forward with this new brand and new logo.
1937-1960s 1960s-1980s
1980s-2000s Today

CJMLS Fall 2011 | 5
In Focus
hospital and was promoted though the local schools. This was such a great idea and one that could be done anywhere in the country, at any time of year. Grassroots initiatives like this are great at building awareness at the local level and when replicated across the country can make a significant contribution to national awareness.
We may not have the financial resources to run multiple national television campaigns, but that shouldn’t limit our creativity when it comes to building awareness.
Q. The television commercial was great but we need more public awareness. Why not air commercials all year long rather than just during National Medical Laboratory Week (NMLW)?
A. The simple answer is cost. National television air time is very expensive and we simply do not have the resources to run commercials during the entire year. It would cost hundreds of thousands of dollars to saturate the air waves.
Your question does raise an important point. There is no reason why awareness activities have to be constrained to National Medical Laboratory Week. There is a marketing rationale for trying to coordinate awareness-building efforts to all happen during the same week. By doing so, we increase the likelihood of garnering media attention.
That being said, members should never feel like they have to wait until NMLW if they have an idea to raise public awareness. CSMLS would be thrilled to work with you or support your initiatives year round. In this issue (see Page 5) there is an article about a Lab Professional for a Day contest that was hosted by lab staff at a British Columbia
Q. CSMLS sends out a lot of paper to its members. The Journal is a prime example. I would like to see the society be more environmentally friendly and deliver its publications electronically instead of in paper form.
A. We believe in being environmentally responsible and have taken measures to reduce the amount of paper being used at the society. This year, we produced our Annual Report as an online publication with limited paper versions available by request. We are looking to do this with other publications in the future.
However, we do believe that some materials should exist in physical form and currently the Journal fits in this category. The Journal is often seen as the outward face of the society. It is important that it projects the quality and professionalism associated with the medical laboratory community. Online publications are not viewed as having the same impact as printed publications and we feel that it is prudent to continue to create a printed journal.

In Focus
6 | CJMLS Fall 2011
Promoting Awareness Withthe Next Generation
Cathy Bouwers
Communications Associate
When asking children about their future careers, you are sure to get the usual answers: police officer, teacher, medical laboratory technologist…okay, maybe being an MLT is not the most common dream of children, but it doesn’t mean that it can’t be! Laboratory staff at Northern Health in British Columbia recently discovered 12 such kids that were very interested in the medical laboratory field.
This past April, as part of National Medical Laboratory Week, laboratory staff at Fort St. John Hospital welcomed three contest winners into the lab to be a ‘‘Laboratory Professional for a Day’’ after winning the laboratory-hosted contest.
“We got the idea to hold the contest from the local fire department, they hold a ‘Fire Chief for the Day’ contest and we played on that concept.” says Lisette Vienneau, Regional Laboratory Technologist and CSMLS board member. The idea proved to be an innovative way to promote the profession and to expose the younger generation to the inner workings of the lab, a place they don’t normally get to see.
The contest was announced in a media release sent out through the Northern Health communications department and through presentations made at local schools. Students between grades three and 12 were invited to write an essay explaining why they would want to be a “Laboratory Professional for a Day”. The essay could
include personal experiences with lab results that made a difference to their life or that of a loved one. The winners, one from each of three age categories, were able to spend a few hours in the Fort St. John Hospital laboratory where they learned about laboratory sample collection and testing procedures. The essays were reviewed by a judging panel that included an MLA and MLT, which based their decision on the author’s motivation and future goals of becoming a lab professional.
“All the winners loved their experience,” says Vienneau. “I think we discovered some future lab professionals here.” Based on the essays, it’s easy to see how the experiences you have as a young person can influence your career decisions as an adult.
The “Laboratory Professional for a Day” contest was a success on many levels, and CSMLS congratulates not only the three winners, but also the laboratory staff at Northern Health. They used a creative grassroots approach to building awareness within their community, something that was done with very little time and expense. The three students that won have walked away with a unique experience and the lab community now has three new future professionals.
COnGRATulATIOns TO ThE WInnERs!
MaKayla Todd, Grade 4
“…I have always been curious about the lab when I have come with my mom. She has to go there every three
months to get her blood tested because she had thyroid cancer. This is important to help save my mom’s life. I like to watch the lab staff and ask questions. I have noticed that there are different vials with different colours. I have learned about the butterfly needle. I would like to learn more...”
Meghan Pimm, Grade 3
“...Another time the lab helped me because I had the mumps and they wanted to make sure that I had the
mumps. The lady was very nice to me she gave me a teddy bear and a sticker. I want to go to the lab because I want to see how they test the blood...”
Taryn Johnston, Grade 11
“…In grade four I got really sick, my mom took me to the hospital and they admitted me into the emergency
room. The doctor told us that I had mononucleosis. He said we had to get my blood tested to make sure that I did have mononucleosis. A lab professional then came to take a sample of my blood, she was very gentle which was nice because I was nervous and scared...Then they tested my blood and I did have mononucleosis, ever since then learning science in school has fascinated me…I am thinking about going into a career that involves science...”

CJMLS Fall 2011 | 7
In Focus
Cathy Bouwers
Communications Associate
PEI Gets Government Attention
They may be small, but they sure are mighty. The Prince Edward Island Society for Medical Technologists (PEISMT) has recently been rewarded for their determination and persistence in the fight for professional regulation.
In April, the Health and Wellness Minister Carolyn Bertram made an announcement that will change the face of the medical laboratory profession in Prince Edward Island. During the statement readings at Province House, Minister Bertram announced the PEI government will be moving forward in developing legislation for health professionals seeking regulation. This umbrella legislation will cover seven health professions including medical laboratory technologists. To make the announcement even more significant, it came during National Medical Laboratory Week and MLTs that attended the assembly were introduced by name and honoured for their work.
Consultations with each of the seven interested health professions will occur throughout the summer and fall. These consultations will help the government to develop criteria that will be used for assessing regulation requests. The umbrella approach to health professional
legislation is common across Canada, as many jurisdictions have learned that stand-alone legislation and regulation for every health profession can be inefficient and costly. The umbrella approach
with mobilizing the profession in the past, mostly due to the relatively small population of working lab professionals. Although the overall population hasn’t increased substantially in 20 years, the
creates one encompassing statute that applies standards and practices to all the professions governed under the legislation. This doesn’t mean that it is a “cookie-cutter” approach to regulation by any means. Each profession under the legislation has provisions that address their own profession-specific issues.
Members of the PEISMT are thrilled with the progress of their advocacy efforts, which began over 20 years ago. No one said government change would be quick or easy, but with persistence, change can happen. The PEISMT had struggled
tight-knit group of MLTs on the island did feel strongly enough about the future of the profession in order to do something to get the government’s attention.
In September 2010, CSMLS hosted the Collaboration Roadshow in Summerside, PEI. Here, members of the PEISMT had the opportunity to meet with Executive Director, Christine Nielsen and Director of Marketing, Communications and Membership, Michelle Squarciotta. Society members used this opportunity to interact with the staff and “pick their brains” on the best way to approach
“ Members of the PEISMT are
thrilled with the progress of their
advocacy efforts, which began over
20 years ago.”

8 | CJMLS Fall 2011
government officials. Christine and Michelle urged the society to attend and present at an upcoming town hall meeting of government candidates where the topic of discussion was health care, a perfect venue for MLTs to voice their concerns.
“Without Christine and Michelle’s encouragement, I don’t think we would have gone to that meeting at all,” says former PEISMT President Michele
McCarville that not only would Health Minister Bertram be reading a statement regarding National Medical Laboratory Week, that she would also be making an announcement regarding the start of a consultation process for umbrella regulation. This exciting news quickly motivated PEISMT members to step out of the lab and represent the profession at the Province House that day.
Perry. “They had experience advocating government officials, so we trusted their advice and leaned on them for support.” CSMLS staff helped PEISMT members prepare questions and general statistics that could be presented at the town hall meeting to help capture the audience’s and the politician’s attention.
A team of seven MLTs arrived at the meeting in their white lab coats, garnering attention from not only the public, but also from the Honourable Olive Crane, Leader of the Progressive Conservative provincial party. The event was an eye-opener for the audience and especially Crane. Not to lose a golden opportunity, Crane was quickly invited on a lab tour soon after the meeting, which opened the doors of communication between PEISMT and the government officials.
This ongoing communication paid off this past spring when Carolyn McCarville, VP for PEISMT was contacted by the communications officer for the legislature. The phone conversation informed
“The house was packed when she read the statement, and there was a hearty round of applause after (the announcement),” said McCarville. “Afterwards we met with Minister Bertram where she told us that medical laboratory technologists would be top priority for consultations.”
With the consultation process underway, PEISMT is keeping pressure on the government to ensure that the umbrella legislation remains at the top of their agenda. “We know that regulation takes time,” says McCarville, “but we have to make sure that is isn’t pushed aside for other issues.”
Crane continues to be a supportive force for the issues in the medical laboratory profession in PEI, as she recently made contact with PEISMT to arrange another lab tour. With the upcoming fall election, the leader of the official opposition is a very good friend to have.
“We have a good relationship with both the Liberal party (currently elected) and the opposition party heading into the upcoming provincial election,” says McCarville. With CSMLS’s help, the PEISMT will make sure that their voices continue to be heard and ensure that the legislative process keeps moving at an efficient pace.
The CSMLS is proud of the PEISMT, continuing year-after-year to reach its goals. They took advantage of opportunities that are quite common in all provinces to get the attention of key members of the government. With the help of CSMLS they were able to formulate a concise plan of action for every step of the way.
“CSMLS has been absolutely fantastic to us in the past year,” says McCarville. “They were always available to help with anything from advice on a presentation to wording of a letter to a politician. PEISMT would not be where we are right now without the CSMLS.”
Since the best advocacy campaigns begin at the grassroots level, CSMLS encourages members to take advantage of opportunities that might be in their own back yard. “We’re here to support our members and their advocacy efforts,” says Squarciotta. “We have a communications and advocacy team that can help you polish the delivery of your message and make sure your voice is being heard by the right people.”
So although the journey is far from over, the PEISMT can give themselves a pat on the back for reaching a major milestone for the profession in PEI. Hopefully this success will motivate and inspire others to keep pressing forward for positive change in the interest of all Canadians.
In Focus
“ They were always available to help with
anything from advice on a presentation
to wording of a letter to a politician.
PEISMT would not be where we are
right now without the CSMLS.”

CJMLS Fall 2011 | 9
In Focus
Direct-To-ConsumerGenetic Testing (DCGT):
Dangerous OrEmpowering The Public
Genomics research has evolved rapidly in the past decade. The consequence of this growth is that the translational techniques have outpaced the corresponding regulations. The burgeoning field of direct-to-consumer genetic testing (DCGT) has been triggered by this swift advance in genomic technology. Individuals are now craving for a shift of power to control their medical information, rather than relying on their healthcare providers. The major questions being asked by concerned healthcare professionals are:
• Doesthegeneticanalysisdonebythesestart-up firms have enough predictive value for its subjects to take action?
• Aretheresultsofthesetestsbeingcommunicated by a person authorized by the Health Profession Act?
• Arethereregulatoryframeworksandpolicies that that will ensure compliance of the testing facilities or the applicable techniques to best practices for testing and interpretation?
sInGlE-nuClEOTIDE POlymORPhIsms (snPs) As RIsk FACTORs In DIsEAsE DEVElOPmEnT
The general approach adopted by DCGT firms is to analyze parts of a chromosome known as single-nucleotide polymorphisms (SNPs), which are evolutionarily stable and useful for population studies, rather than the entire genome. This approach is based on the assumption that variation of the SNPs is associated with certain diseases and supported by results of peer-reviewed scientific studies. An example of how SNPs influences a disease condition is the apolipoprotein E (ApoE) gene that is associated with Alzheimer’s disease.1 Two variations of the SNPs of ApoE results in three possible alleles for this gene: E2, E3 and E4. Each allele results in an amino acid product that is different by one amino acid. The consequences of this alteration are proteins that differ in structure and function, which could lead to different conditions. Each individual inherits one maternal copy of ApoE and one paternal copy of ApoE, and an individual
that inherits a copy of an E4 allele is predisposed to developing Alzheimer’s disease, while someone inheriting the E2 allele is less likely to develop Alzheimer’s. However, this scenario is not as simple as this example implies as well as for other diverse chronic disease conditions like diabetes, heart disease and cancer.
Undoubtedly, SNPs are associated with certain diseases, but there is a strong likelihood that there could be other genes that are putative and might lower the risk of predisposition to these diseases. Most disease conditions are predicted by a complex combination of various genes, including life-style patterns and environmental factors, making genetic testing very complex. The main problem associated with the approach applied by direct-to-consumer genetic testing firms is the limitation posed by published association studies that these predictions are reliant on. The sample sizes are often insufficient for statistical support of a hypothesis and positive associations observed in one report are often not reproduced in subsequent studies.2
Chinedu Ogbonna M.Sc., Cert.Reg Affairs, MLT
Prairie North Health Region

10 | CJMLS Fall 2011
In Focus
Population stratification has also often been identified as a cause for false-positive results of genetic association studies. Other issues posed for the majority of these studies are: the control population does not properly represent samples for comparison with the disease groups, the controls are not usually family-based to reduce population stratification, and the studies are conducted on diverse ethnic groups — SNP allele frequencies can differ widely in different populations.2
There have been more than 1,000 published associations using SNPs in one or two candidate genes to assess an association between a genetic variant
population and they only had a 1.67-fold increased chance of obesity.
ADVERTIsInG AnD COmmunICATInG DIRECT-TO-COnsumER GEnETIC TEsTInG REsulTs
Traditionally, diagnostic or genetic tests are ordered by healthcare providers who determine the clinical validity and utility of such tests and interpret the test results for consumers. However, DCGT can be advertised and sold directly to consumers and the results of these tests released directly to consumers.5 This approach of releasing test results and advertisement has become subject of intense controversy.
and a cardiovascular end point like hypertension, lipid levels, ventricular hypertrophy, or coronary heart disease. A majority of these studies had design flaws, lacked adequate statistical support and were not reproducible in subsequent studies, which failed to confirm the putative genetic association.3 The identification of a gene variant associated with obesity was promoted as the discovery of the “fat gene” and with the insinuation that it was the most important determinant for obesity.4 However, the study only showed that patients carrying two copies of the gene variant weighed about 3 kilos more than the average
If the adverts for these tests are not regulated, there is a strong possibility the claims could be embellished and exaggerated to cause panic and anxiety and consequently increasing the ordering of these tests. Providers of DCGT have argued that their procedure does not equate with practicing diagnostic medicine and that an individual should have the freedom to access their own DNA data without restriction. They also argue that DNA-analysis is not medical testing but personal genetic “informational services” and should be regulated like over-the-counter tests, just like pregnancy testing. If the providers are telling people that
they are likely to develop a severe disease condition, then it should be assumed to be a medical advice and diagnosis. In most jurisdictions in Canada, communicating a diagnosis is a controlled act which may only be performed by a person authorized by a health profession Act. An example is the Ontario Regulated Health Professions Act.6
A majority of doctors still rely on people with adequate knowledge and training to provide quality genetic counseling to their patients who have undergone genetic tests. If doctors who have been highly trained require assistance in genetic counseling, then the level of ambiguity and complexity of information that consumers of DCGT are dealing with can only be imagined. There is also a strong chance of misusing genetic information by third parties, especially employers and insurance companies who may discriminate against individuals on the basis of these genetic testing results without understanding the full picture.
WhAT REGulATIOns ARE In PlACE FOR DIRECT-TO-COnsumER GEnETIC TEsTInG kITs AnD FACIlITIEs?
Most regulations and guidelines on genetic testing were set up in the 1990s and there was no indication that genetic testing would be offered directly to consumers. In the US, the federal government has oversight of In-Vitro Medical Devices (IVMD) and laboratories that perform these diagnostic tests under the Clinical Laboratory Improvement Amendments of 1988 (CLIA) and the Federal Trade Commission Act (FTCA). The Food and Drug Agency (FDA) categorizes commercially marketed IVMDs in terms of their complexity and assesses the safety, effectiveness, quality and design of these devices. CLIA regulations focus on the quality of the clinical testing process, this includes laboratory quality control. None of the genetic tests offered directly to consumers
“ Direct-to-Consumer Genetic testing
appears to be an excellent business
model and would provide new business
opportunities in pharmacogenomics
and nutrigenomics if properly
regulated.”

CJMLS Fall 2011 | 11
In Focus
has undergone premarket review by FDA to ensure that the test results being provided to consumers are accurate, safe and clinically useful.7
Similarly, there have been no reports of inspections of any of the sites where these genetic samples are processed to ensure compliance of their procedures to good laboratory practice. This includes home-use saliva collection kits that were being sold in approximately 6,000 Walgreen stores with the claim of offering “Genetic Health Report”.7 The test was intended to report the presence or risk of more than 70 health conditions, prescription medication response, and other information that will guide the consumers to modify their lifestyles, perhaps to live a healthier and longer life. Recently, the FDA has become very proactive by sending letters to a substantial number of these firms warning them that their products meet the statutory definition of medical device. There are also ongoing discussions between the FDA and some of the manufacturers as well as providers of DCGT to develop a risk-based and fair regulatory framework for these kits.7 Currently, 25 states and the District of Columbia permit direct-to-consumer genetic testing without restriction, 13 other sates completely prohibit it.
In Canada, in-vitro diagnostic devices are regulated under the Food and Drugs Act and as high-risk Class III medical devices if intended for genetic testing. Like the US, medical devices cannot be sold or imported without a license and manufacturers need to provide evidence of safety and effectiveness of the device before approval. Licensing and quality of testing process by medical laboratories is regulated by provincial health authorities. However, Heath Canada has classified DCGT kits as personal kits which are neither prohibited by any statute, nor subject to federal regulation. In European Union member states, except Germany, France and Switzerland, In-Vitro-Diagnostics Devices Directive stipulates
that the marketing of in-vitro diagnostic does not cover genetic testing and treats gene tests as “low-risk” devices for which no pre-marketing approval is provided.8 Whether these relaxed approaches are acceptable is subject of debate, and would require a vigorous evaluation of the validity of the tests. Most importantly, there should at least be minimum codes of practice to ensure quality of standards.
COnClusIOnThere is no doubt that genetic testing
is a huge breakthrough in science and has a remarkable potential for preventive medicine. Direct-to-Consumer Genetic testing appears to be an excellent business model and would provide new business opportunities in pharmacogenomics and nutrigenomics if properly regulated. However, by considering the potential indirect harm that the consumers of DCGT might be exposed to there is a strong requirement for a regulatory framework to protect consumers. At least the following minimum codes of practice should be defined: laboratory accreditation and proficiency testing requirements; qualification of staffs to interpret the results and offer counseling services; legislation to ensure enforcement of the appropriate claims; acceptable evidence of gene-disease association.
REFEREnCEs1. Ganguli M, Chandra V, Kamboh IM,
Johnston JM, Hiroko H, Thelma B.K et.al Apolipoprotein E Polymorphism and Alzheimer Disease: The Indo-US Cross-National Dementia Study Arch Neurology. 2000; 57:824-830.
2. Bell J. Single Nucleotide Polymorphisms and Disease Gene Mapping Arthritis Research and Therapy 2002; 4 (Suppl 3):S273-S278
3. Tabor HK, Risch NJ, Myers RM. Candidate-Gene Approaches for Studying Complex Genetic Traits:
Practical Considerations. Nature Reviews Genetics 2002; 3: 391–397
4. Frayling TM, Timpson NJ, Weedom MN, Zeggini E, Freathy RM, Lindgren CM. et.al A Common Variant in the FTO Gene Is Associated with Body Mass Index and Predisposes to Childhood and Adult Obesity Science 2007;316:889-894
5. Hogarth S, Javittand G,D Melzer The Current Landscape for Direct-to-Consumer Genetic Testing: Legal, Ethical and Policy Issues Annual Review of Genomics and Human Genetics 2008;9:161-182
6. Regulated Health Professions Act Chapter 18, Section 27.(2)
7. Congressional Testimony Direct-to-Consumer Genetic Testing and the Consequences to the Public: Statement of Director, Center for Devices and Radiological Health Food and Drug Administration [Online] 2010 [cited 5 June 2011] Available from: http://www.fda.gov/NewsEvents/Testimony/ucm219925.htm
8. European Parliament Science and Technology Options Assessment, Direct to Consumer Genetic Testing, Study P/A/STOA/FWC/2005-28/SC32 & 39 [Online] 2008 [cited 4 June 2011] Available from: http://www.europarl.europa.eu/stoa/publications/studies/stoa32and39_en.pdf

12 | CJMLS Fall 2011
Maintaining the Schedule of Unit Values for the Clinical Laboratory Workload Measurement System
mAkE yOuR RECOmmEnDATIOn COunT — AnD ObTAIn sOlID DATA TO AssIsT yOuR hEAlTh sERVICE ORGAnIzATIOn In sTAFFInG, PlAnnInG, buDGETInG AnD PERFORmAnCE mOnITORInG
This article will introduce the clinical laboratory workload measurement system (WMS) continuous quality improvement maintenance cycle for the Standards for Management Information Systems in Canadian Health Service Organizations (MIS Standards). The following questions will be answered:
• WhoisCIHI?
• WhataretheMISStandards,WMS,and schedule of unit values?
• Whatspecificchangesweremadein2009 and 2011, and why?
• Howwillfuturemaintenancecyclesbeconducted?
• Howcanpractitionersofferrecommendations for the revision of the schedule of unit values for the 2013 MIS Standards?
In Focus
FIGuRE 1: Graphic representation of the data generated by the MIS Standards. Its components include: accounting principles and applications (white boxes), WMS — Workload Measurement System (light blue box), and the Schedule of Unit Values (dark blue box).
Arlene L. Thiessen R.N.
Senior Analyst, MIS Team Canadian Institute for Health Information

CJMLS Fall 2011 | 13
WhO Is CIhI? The Canadian Institute for Health
Information (CIHI) is an independent, not-for-profit corporation that provides essential information on Canada’s health system and the health of Canadians by being a leading source of unbiased, credible and comparable data and information that will enable health leaders to make better-informed decisions.
WhAT ARE ThE mIs sTAnDARDs? The MIS Standards are a set of national
accounting standards used across the health care system by health service organizations to collect and report financial and statistical data from their daily operations. The MIS Standards were developed to generate better information and measures of health service organizations’ functional centre activity. However, they do not attempt to quantify or assess the quality of service recipient care, treatment or clinical status. Clinical laboratory services that are funded by provincial and territorial ministries of health (except Quebec and Nunavut), rely upon the MIS Standards to report financial and statistical data.
hOW DO hEAlTh sERVICE ORGAnIzATIOns usE mIs DATA?
MIS data provides information on the inputs and outputs of clinical laboratory services for comparison and trending among facilities, for planning, informed decision-making, and for management of laboratory operations. It is used by decision-makers at many levels, from ministries of health to individual functional centres, for collaborative information-sharing, budgeting, planning, policy-setting and comparison.
WhAT Is A WORklOAD mEAsuREmEnT sysTEm (Wms)?
A WMS is an integral part of the MIS Standards. It is a tool that measures the
volume of activity provided by a specific functional centre, such as a clinical laboratory, using standardized units of time. The clinical laboratory WMS enables health service organizations to record the hands on time spent on service recipient and non-service recipient activities. It serves two main purposes. First, it systematically quantifies workload in specific health care disciplines to assist managers in staffing, planning, budgeting, and performance monitoring. Second, it yields uniform data for external reporting, which permits national and peer group comparisons.
WhAT Is A sChEDulE OF unIT VAluEs?
A schedule of unit values is a list of activities commonly performed in a clinical laboratory, as well as the unit values associated with each activity. Its purpose is to track the hands-on time, in minutes, required to perform laboratory activities. The published unit value is based on the average time it takes the average unit producing personnel to perform the activity under average circumstances for the average service recipient. The values are derived from time studies or time estimates and reviewed by subject matter experts.
Any activity in the schedule of unit values can be utilized by any clinical laboratory functional centre if the unit value is accurate and reflective of the realistic average time required to perform a specified activity. If the published unit values are not realistic in a particular circumstance, the laboratory is encouraged to use standard times (site specific average times) or actual times (the actual time required for each activity).
Maintenance of the clinical laboratory schedule of unit values within the MIS Standards workload measurement system enhances good data quality through more representative unit values, deletion of obsolete activities, creation of new
activities to match advances in science, and increased clarity of definitions.
WhAT sPECIFIC ChAnGEs WERE mADE TO ThE 2009 mIs sTAnDARDs, AnD Why?
In response to stakeholder concerns that the existing WMS for clinical laboratory no longer represented the current environment CIHI extensively redeveloped the 2009 MIS Standards, and particularly the clinical laboratory WMS. This was a two-year project that involved more than: 60 volunteer laboratory experts serving on 12 committees, 12 face-to-face meetings, 195 teleconferences.
Key changes to the 2009 clinical laboratory WMS included revisions to functional centres to better reflect current service delivery. Terminology was updated. The new service activity statistic was defined as the “laboratory intervention”. Also, categories of service recipients were adjusted to align with all other workload measurement systems within the MIS Standards.
Additionally, the 2009 clinical laboratory schedule of unit values was redeveloped to better reflect the hands-on time required to perform the service recipient activities and to exclude daily or routine preparation, maintenance and repair, solution preparation, glassware wash up, and technical supervision. The activities were described in a more granular level of detail, which allows each laboratory to customize the workload for a particular test based on the specific activities performed (for example, level of automation). A number of activities were classified as non-service recipient activities (such as quality control and calibration) to align with all other workload measurement systems. Importantly, CIHI committed to a scheduled maintenance process to ensure the clinical laboratory WMS remains current.
In Focus

In Focus
14 | CJMLS Fall 2011
WhAT ChAnGEs WERE mADE TO ThE 2011 ClInICAl lAbORATORy sChEDulE OF unIT VAluEs?
CIHI’s inaugural maintenance project for the 2011 MIS Standards clinical laboratory schedule of unit values resulted in an updated schedule that was published for implementation April 1, 2011. This project spanned nine months, involved more than 45 volunteer laboratory experts serving on 13 committees. More than 116 teleconferences were held.
and device/instrument procurement, evaluation, selection and validation, decommissioning equipment and more.
hOW WIll FuTuRE mAInTEnAnCE CyClEs bE COnDuCTED?
CIHI will conduct a biennial maintenance project for the schedule of unit values beginning this fall. The 2013 MIS Standards will include the results of this project which will focus solely on
Key changes to the 2011 clinical laboratory schedule of unit values included deletion of obsolete activities, creation of new activities to match advances in science, including an expanded microarray section, and significantly fewer unit values that are listed as “to be determined” (TBD). The service activity for the anatomical pathology functional centre was clarified as the autopsy or specimen. Unit values were reviewed to ensure accuracy. They were adjusted for being too high or too low and more consistently align with similar activities in other laboratory disciplines. Where required, the activity was defined with more granularity. For example an item for count may have been clarified as batch or single slide/tube/plate. The non-service recipient activity list was expanded with the addition of several activities including; preparation of gels and Formvar grids, sterile chamber environments, batch autoclaving;
improving the schedule of unit values. Following this maintenance cycle, CIHI will evaluate the efficacy of the 2013 clinical laboratory maintenance project so the MIS Standards remain as relevant and current as possible. CIHI anticipates a six-month project involving more than100 volunteer laboratory professionals, approximately 10 expert reviewers, and three teleconferences.
After completing the 2011 maintenance of the schedule of unit values, CIHI recognized that the project was resource-intensive for subject matter experts in terms of person hours, time away from laboratory duties, etc. Therefore, in the future, CIHI will leverage electronic survey techniques to elicit feedback from a wider base of laboratory volunteers. For 2013, and every two years thereafter, CIHI plans to adjust the schedule of unit values to keep pace with advances in science, instrumentation and
computerization, as well as ever-changing processes in the laboratory.
hOW CAn PRACTITIOnERs OFFER RECOmmEnDATIOns FOR ThE REVIsIOn OF ThE sChEDulE OF unIT VAluEs FOR ThE 2013 mIs sTAnDARDs?
In the fall of 2011, CIHI will survey clinical laboratory professionals in the field to obtain suggested improvements (clarifications, deletions, changes etc.) to be made to the schedule of unit values. The following professionals will be invited to participate in the survey: medical laboratory managers/directors, medical laboratory technologists, clinical laboratory information systems (HIS/LIS) professionals and members from the 13 Clinical Laboratory Working Group committees from the 2011 project. “ The MIS Standards were developed
to generate better information
and measures of health service
organizations’ functional centre
activity.”
To receive the MIS Standards for Clinical Laboratory survey (for yourself or for a colleague), for more information, or for specific laboratory WMS questions please contact CIHI by email at [email protected]. You can also visit www.cihi.ca > Standards and Data Submission > Standards > MIS Standards.

CJMLS Fall 2011 | 15
Perspectives is a new addition to the Canadian Journal of Medical Laboratory Science (CjMLS). This section seeks
to provide thoughts, insights, and opinions from individuals with different points of views. We hope that as this
section evolves, it allows us to present a broader array of topics that reflect the varied careers and experiences of
our members. If you are interested in contributing to the Perspectives section, email us at [email protected].
PERsPECTIVEs

16 | CJMLS Fall 2011
Perspectives
Most laboratories expect that work will be performed safely and that all proper precautions are taken to ensure all aspects of the work — accuracy, efficiency, safety — are considered and all standards are met. While many laboratories monitor and measure accuracy (errors) and efficiency (tests conducted over time), not many laboratories monitor or measure safety. The old adage, “what gets measured gets done” is often borne in laboratories, where worker safety may take a backseat to productivity. How is safety measured in a laboratory?
There are two major categories of health and safety performance metrics. The most commonly used measures are “lagging indicators”. This means they are “after-the-fact” and represent data related to adverse effects that have already occurred. Examples of lagging indicators are:
• Numberoftimelossaccidents
• Typesofinjuriesthatoccur
• Costoftimelossaccidents
• Numberofdaysabsentduetoinjury/illness
• Numberofincidentsthatrequiredmedical aid, but did not include time loss
• Numberoffires,spillsorothersafetyemergencies
• Numberofexposurestochemicalsorbiological hazards
While we can learn something about the types and frequency of injuries from this data, we do not often identify what needs to be done to prevent the incidents.
“Leading indicators” are measures of activities done to prevent incidents from occurring. Leading indicators are often considered “proactive” measures of safety performance. Examples of leading indicators are:
• percentageoflaboratoryinspectionsconducted as per schedule
• percentageofhazardsidentifiedininspections that have been corrected
• percentageoftasksonwhichaformalrisk assessment has been conducted
• percentageofscheduledhealthandsafety committee meetings that occurred
• percentageofincidentsthatwereproperly investigated to find and correct root causes
• percentageofrequiredemergencyresponse drills conducted
• percentageofworkersusingproperpersonal protective equipment
• percentageofnewlyhiredworkerswhoreceived orientation within the first week of work
• percentageofworkerswhoattendedrefresher training
Laboratories often develop a false sense of security because they do not have many time loss incidents. Workers compensation costs are often low, and property damage from worker incidents is captured as “equipment breakdown” and not associated with the incident. Does this mean laboratories are safe places to work? Not necessarily. Many laboratory workers have had “close calls” or “near misses” or have witnessed them. Under slightly different circumstances, these close calls may result in serious injuries. Chemical or biological exposures may go unnoticed if
A safety Perspective
Measuring Safety Performance in the Laboratory

CJMLS Fall 2011 | 17
Perspectives
there are no acute effects. Musculoskeletal injuries are often attributed to factors outside the work environment.
To ensure that the laboratory is on a continual improvement path, performance measures should focus on leading indicators (in addition to proving data related to lagging indicators). This helps promote the important safety activities that should be carried out in the laboratory and allows the lab to track trends and identify weak areas. When we identify leading indicators as a percentage of activities that should occur (such as the percentage of required laboratory inspections conducted), we are comparing the actual occurrences with a desired or established standard. For example, if a laboratory requires monthly lab inspections, and they are conducted nine times in one year, that means that they
have a 75 percent compliance rate with the standard. If this improves each year, the trend can be tracked. On the other hand, if one of these activities starts to be neglected, that is picked up as a negative trend.
One of the most effective ways to measure health and safety is to involve all lab workers in the process. While labs commonly post information related to quality control issues, lab errors, and workload statistics, most laboratories do not have posted laboratory safety metrics. Make laboratory workers more aware of safety standards and enlist their help in tracking performance. Consider placing progress charts of health and safety activity measures on the bulletin boards and having employees fill them in. Set and publicize goals related to health and safety performance.
The key to continual improvement in health and safety lies in awareness of prevention activities and documentation of their performance. Keep in mind that old adage: “What gets measured gets done”.
Gene Shematek
Occupational Health and Safety Consultant to CSMLS
Projet : Annonce MMI 2011
Client : Meloche Monnex
No de dossier : II-MM8437-10 MMI.EN•csmls (7x4.875)
Province : Ontario
Publication : CDN Journal of Med Lab Sci
Format : 7x4.875
Couleur : Quad
Épreuve # : 1
Date de tombée : 15/01/2011
Graphiste : Yannick Decosse
Hamelin Martineau • 505, boul. de Maisonneuve O. Bureau 300 • Montréal (Québec) H3A 3C2 • T : 514 842 4416 F : 514 844 9343ATTENTION : Merci de vérifier attentivement cette épreuve afin d’éviter toute erreur.
At TD Insurance Meloche Monnex, we know how important it is to save wherever you can. As a member of the Canadian Society for Medical Laboratory Science, you can enjoy preferred group rates on your home and auto insurance and other exclusive privileges, thanks to our partnership with your association. You’ll also benefit from great coverage and outstanding service. At TD Insurance, we believe in making insurance easy to understand so you can choose your coverage with confidence.
The TD Insurance Meloche Monnex home and auto insurance program is underwritten by SECURITY NATIONAL INSURANCE COMPANY. The program is distributed by Meloche Monnex Insurance and Financial Services Inc. in Quebec and by Meloche Monnex Financial Services Inc. in the rest of Canada.
1Certain conditions and restrictions may apply. Due to provincial legislation, our auto insurance program is not offered in British Columbia, Manitoba or Saskatchewan.*No purchase required. Contest ends on January 13, 2012. Each winner may choose the prize, a 2011 MINI Cooper Classic (including applicable taxes, preparation and transportation fees) for a total value of $28,500, or a cash
amount of $30,000 Canadian. Odds of winning depend on the number of eligible entries received. Skill-testing question required. Contest organized jointly with Primmum Insurance Company and open to members, employees and other eligible persons belonging to all employer groups, professional groups and alumni groups which have an agreement with and are entitled to group rates from the organizers. Complete contest rules and eligibility criteria available at www.melochemonnex.com. Actual prize may differ from picture shown. MINI Cooper is a trade-mark, used under license, of BMW AG, which is not a participant in or a sponsor of this promotion.
®/The TD logo and other trade-marks are the property of The Toronto-Dominion Bank or a wholly-owned subsidiary, in Canada and/or other countries.
“ I saved just for being a member of my professional association.”
– Bob Raposo, satisfied client since 2002
Insurance program endorsed by
Get an online quote at www.melochemonnex.com/csmlsor call 1-866-269-1371Monday to Friday, 8 a.m. to 8 p.m. Saturday, 9 a.m. to 4 p.m.
YOU COULD
1 OF 2 MINI COOPER CARSOR $30,000 IN CASH!*
WIN
II-MM8437-10 MMI.EN•csmls (7x4.875).indd 1 11-08-02 2:19 PM

18 | CJMLS Fall 2011
Perspectives
Research shows that most preceptors ask only basic knowledge questions when training new staff or students and fail to ask higher level questions to stimulate critical thinking.1 Bloom’s taxonomy describes the levels of understanding from basic to more complex.2 The most basic type of question is at the knowledge level, which is the easiest type to formulate. These questions do have their purpose (to confirm grasp of basic facts and to correct misinformation), however, to facilitate and evaluate deeper-level learning, higher-order questions are needed.1,3
Knowledge-based questions can be used to assess the ability of the trainee to recall facts. Examples of recall questions are: “What is the correct anticoagulant to blood ratio for collecting coagulation specimens?”; “How are samples for pre-transfusion testing labeled at this hospital?”; “What special precaution should be taken with samples for bilirubin testing?”
Once knowledge of basic facts are assessed, the trainer can then ask questions to gauge comprehension. These types of questions might ask the student to explain concepts, give examples, or summarize information. An example would be, “Explain why proper cleansing of the arm is important when collecting a blood culture specimen.” Asking, “Why is a 9:1 ratio of blood to anticoagulant used for coagulation testing?” determines if the trainee understands the reason why the ratio is important.
Application questions require the learner to perform calculations, organize information or solve basic problems. Questions in this category might include, “Given the appropriate parameters,
calculate the osmolal gap.” Or “Blood is spilled in a water bath. How would you appropriately deal with this situation?” Integrating several areas of knowledge is necessary for the learner to answer these questions correctly, whether it is recalling a formula and using it to perform calculations, or correctly applying knowledge of disinfectants to different situations.
Higher-order questions include analysis, synthesis, and evaluation of information.1-3 To answer these questions, the student would have to move beyond the understanding of basic facts and comprehension of theory, to questioning of viewpoints, creating new ideas, or predicting outcomes based on evaluating information. For example: “How would you design a training manual for the collection of coagulation samples that would be appropriate for non-laboratory personnel?” Or “Given stained tissue slides that failed QC, how would you trouble-shoot the problems that could have occurred from fixation to staining?” Case studies are one way that trainers can stimulate and challenge learners to think at a higher level. Basic knowledge questions can be asked about a situation, and then the trainer can proceed to more in-depth questioning that includes multiple aspects of the case beyond the main principles.
Questioning is a skill that can be developed to enhance both teaching and learning on the bench. Knowledge-based questions have their place, but should not be the only questions asked. To promote critical thinking the use of probing, open-ended, higher level questions will challenge students’ perceptions, link
existing knowledge to new situations, and explore different frames of reference.
References1. Profetto-McGrath J, Bulmer Smith K,
Day RA, Yong O. The questioning skills of tutors and students in a context based baccalaureate nursing program. Nurs Educ Today 2004;24:363-72.
2. Bloom BS. Taxonomy of educational objectives: the classification of educational goals. New York: D. McKay Co.;1956.
3. Lord T, Baviskar S. Moving students from information recitation to information understanding: exploiting Bloom’s taxonomy in creating science questions. J College Sci Teaching 2007;36(5):40-4.
Roberta Martindale, MEd, BSc (MLS), MLT, MT (ASCP), Assistant Professor
Christopher Ward, MEd, BSc (MLS), MLT, Associate Professor
Marion Fraser MBA, BSc (MLS), MLT, Assistant Professor
Division of Medical Laboratory Science Department of Laboratory Medicine & Pathology University of Alberta Edmonton, Alberta
An Educator’s Perspective
How Effective Are Your Questions When Training Students On The Bench?

CJMLS Fall 2011 | 19
Perspectives
During clinical rotation there are certain experiences that can shape a student’s path towards becoming a competent medical laboratory technologist. The experiences or moments that stand out most to me are the little things that MLTs in the lab did to help guide my learning. This list highlights what I believe to be some of the most valuable aspects of clinical rotation, demonstrating how MLTs can create a positive and valuable learning experience for students.
1. Being included in professional activities: Taking part in staff meetings, lunch and learns, seminars, and symposiums helps us learn the way hospitals work and to feel part of the hospital culture.
2. Being trusted: When you treat us like co-workers, it generates the confidence we need to take chances with our learning. When we’re allowed and encouraged to work on samples on our own, it gives us a significant feeling of accomplishment.
3. Being told that the mistakes we make are OK: If you have the opportunity to let us know that we’re not the only ones to make a certain mistake, please do. It makes us feel much less disheartened and much more encouraged than if we’re made
to feel stupid. Acceptance in spite of our errors goes a long way in building confidence.
4. A nurturing environment: Your kindness, encouragement and patience means more to us than you know. When we start our placement, and each time we start a new rotation, we step into unfamiliar territory. It can be intimidating and we don’t want you to think we’re incompetent. Knowing that we’re in an environment that is nurturing and safe makes it infinitely easier to learn.
5. Your geekiness: We love that you’re as much of a science geek as we are! We get excited about interesting samples and test results and love to see your enthusiasm.
6. Feeling welcome: We’re doing our placement as the final step in our education. We take this very seriously and have worked hard to get to this point. Going into a new environment is never easy, so being made to feel welcome in your lab can get us off to a great start and will provide an emotionally safe environment for learning. No one wants to feel like a burden or an annoyance.
7. Hands on work: We just spent a great deal of time in lectures learning
theory. We are very ready to get our gloves dirty!
8. Contributing to the team: Being part of your team and contributing to the care of real patients is very rewarding for us. As you know, going home feeling like you’ve made a difference is exhilarating.
9. Troubleshooting with you: We know that one of the main skills we need to develop as a technologist is the ability to troubleshoot. Going through a problem alongside you, even seeing you make mistakes, can be an invaluable learning experience for us.
10. Applying all that book knowledge to real lab work: During the in-class portion of our education, it’s very difficult to comprehend how things all fit together in a real lab. Being in your lab every day, being part of the work and seeing the big picture really ties together all of our learning and reinforces our studies. We really appreciate the opportunity.
Stephanie Harper B.Sc. MLT
Medical Laboratory Science Student
St. Lawrence College
A student’s Perspective
10 Things Lab Students Value Most During Their
Clinical Rotation
20 | CJMLS Fall 2011
Perspectives
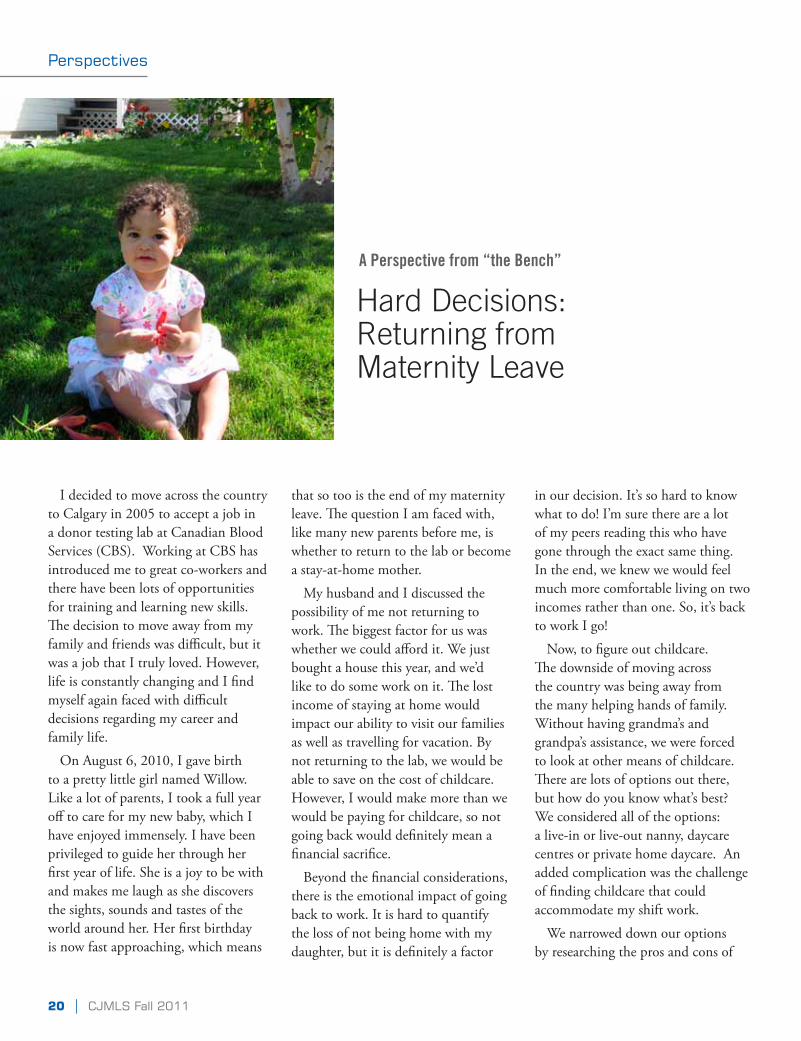
A Perspective from “the bench”
Hard Decisions: Returning from Maternity Leave
I decided to move across the country to Calgary in 2005 to accept a job in a donor testing lab at Canadian Blood Services (CBS). Working at CBS has introduced me to great co-workers and there have been lots of opportunities for training and learning new skills. The decision to move away from my family and friends was difficult, but it was a job that I truly loved. However, life is constantly changing and I find myself again faced with difficult decisions regarding my career and family life.
On August 6, 2010, I gave birth to a pretty little girl named Willow. Like a lot of parents, I took a full year off to care for my new baby, which I have enjoyed immensely. I have been privileged to guide her through her first year of life. She is a joy to be with and makes me laugh as she discovers the sights, sounds and tastes of the world around her. Her first birthday is now fast approaching, which means
that so too is the end of my maternity leave. The question I am faced with, like many new parents before me, is whether to return to the lab or become a stay-at-home mother.
My husband and I discussed the possibility of me not returning to work. The biggest factor for us was whether we could afford it. We just bought a house this year, and we’d like to do some work on it. The lost income of staying at home would impact our ability to visit our families as well as travelling for vacation. By not returning to the lab, we would be able to save on the cost of childcare. However, I would make more than we would be paying for childcare, so not going back would definitely mean a financial sacrifice.
Beyond the financial considerations, there is the emotional impact of going back to work. It is hard to quantify the loss of not being home with my daughter, but it is definitely a factor
in our decision. It’s so hard to know what to do! I’m sure there are a lot of my peers reading this who have gone through the exact same thing. In the end, we knew we would feel much more comfortable living on two incomes rather than one. So, it’s back to work I go!
Now, to figure out childcare. The downside of moving across the country was being away from the many helping hands of family. Without having grandma’s and grandpa’s assistance, we were forced to look at other means of childcare. There are lots of options out there, but how do you know what’s best? We considered all of the options: a live-in or live-out nanny, daycare centres or private home daycare. An added complication was the challenge of finding childcare that could accommodate my shift work.
We narrowed down our options by researching the pros and cons of

CJMLS Fall 2011 | 21
Perspectives
“ In our largely female profession,
this is a balancing act that many of
you probably struggle with on an
ongoing basis. ”
each and then went from there. A live-in nanny was the first we crossed off the list. Although our basement is finished, it doesn’t have a separate bedroom or bathroom. If we were going to have a live-in nanny we felt those are two things we would want for her, so that our living space is ours, and hers is hers alone. The next option off the list was a live-out nanny; they are usually a lot more expensive than their live-in counterparts, so this was never really an option we considered for very long. So we were left with a daycare centre or a private home daycare.
It’s unfortunate that from nearly the moment Willow was born, I was concerned about how to balance my career with providing care for my child. In our largely female profession, this is a balancing act that many of you probably struggle with on an ongoing basis. Although I did decide to return to the lab, the balancing act has lead me to make a change in my career.
A couple of weeks ago I was offered a position in a lab where there is no shift work. It’s a day job, from Monday to Friday with no weekend, evening or night shifts. This is a rarity in the Medical Technology field, and
of parenthood. I found that by being realistic about our options, doing research and taking advantage of work opportunities all made for a smooth transition. I recommend starting early by making a list of your own options with the pros and cons of each. Every situation is different and you have to figure out what is best for your unique family and work situation.
Allison Caisey
Medical Laboratory Technologist Rocky Mountain Analytical
just too good to pass up. Although I love my job at CBS, this new position will allow more time for me to focus on my daughter. So, sadly, I resigned from CBS, but I am eagerly looking forward to this new opportunity.
At the same time we found a wonderful home daycare for Willow. She’ll be one of five kids in the home of a loving and caring woman in our area. We think it will be great for Willow as she’ll make some new friends and practice sharing toys, something she hasn’t had to do much at home.
As many new parents, I experienced the anxiety and stress of going back to work after staying home with my baby. Now that I’ve been through this process I can offer some advice to anyone just beginning this stage

Join us for the 30th anniversary
www.ifbls-dvta2012.comFor more information contact the Congress Secretartiat at: [email protected]
Topics will include:• Multiresistant Infectious Agents (MRE):
Methodical Challenges for the Laboratory• Renaissance of “Declared Dead” Diseases?• Haematological Neoplasia: Between Morphology
and Next-Generation Sequencing• Molecular Medicine: State of the Art - Between
Individualized Diagnostics and TransparencyFor the full list of topics please visit the congress website
Call for AbstractsDeadline for submission:
15th February, 2012

sCIEnTIFIC sECTIOn
CJMLS Fall 2011 | 23

Vanessa Chan, MLT, BScMarilyn Johnston, MLT, ARTWilliam Brien, MD, FRCPC
Scientific Section
24 | CJMLS Fall 2011
Since the introduction of the International Normalized Ratio (INR) in 1983, the INR has served as an international tool for standardizing and monitoring oral anticoagulant therapy. The INR has made a significant improvement in standardizing patient results from one medical center or country to the next, but recent studies and surveys have shown that INR results are
not as comparable across different institutions as it may appear.1,2 To further improve standardization of INR results, the Clinical Laboratory Standards Institute (CLSI), the International Society on Thrombosis and Haemostasis (ISTH) and other organizations have included sections on local ISI calibrations and validations in their guidelines.3,4,5
Validation of Prothrombin Time (INR) Reagent: Where are we?
DEFInITIOns Calibrant plasmas – certified plasmas used for calibrating a local ISI or a direct PT-INR calibration curve. Calibration – set of operations that establishes, under specific conditions, the relationship between values of quantities indicated by a measuring instrument or measuring system, or values represented by a material measure or a reference material, and the corresponding values realized by standards (CLSI).3 Certified plasmas – normal or abnormal plasma samples assigned a PT/INR value by a manufacturer, using a manual method based on a WHO accepted protocol determined against an appropriate thromboplastin IRP that has been calibrated against the appropriate WHO standard in a multicenter study (CLSI).3 Both CLSI and ISTH recommends a minimum of 3 certified plasmas spanning the therapeutic INR range of 1.5-4.5 and an additional normal plasma be used for both ISI calibration and validation.3,4 Direct INR determination – INR determined from a PT/INR calibration line determined using certified plasmas without employing an ISI and MNPT (CLSI).3
Generic ISI – an ISI determined for a thromboplastin that is not instrument-specific (ie., determined for a group of instruments that uses the same general method for endpoint detection, such as manual, photo-optical, or mechanical methods) (CLSI).3 International Normalized Ratio (INR) – patient’s prothrombin time test result expressed as a ratio to a normal population which has been standardized (or normalized) for the potency of the thromboplastin used in the assay (CLSI).3
•INR=patientPT/MNPT International Sensitivity Index (ISI) – a quantitative measure, in terms of the first International Reference Preparation of thromboplastin, human, combined, coded 67/40, of the responsiveness of a prothrombin-time system to the defect induced by oral anticoagulants (CLSI).3 The responsiveness of PT system to the defect induced by oral anticoagulants (ISTH).4 Overall sensitivity to the depression of factors II, VII and X during oral anticoagulant treatment (WHO).6 Mean normal prothrombin time (MNPT) – the geometric mean of the prothrombin times of the healthy adult population. A minimum of 20 samples from both sexes is a reliable approximation of the MNPT (CLSI).3

Scientific Section
CJMLS Fall 2011 | 25
Prothrombin time (PT) – time in seconds required for a fibrin clot to form in a plasma sample after tissue thromboplastin and an optimal amount of calcium chloride have been added to the sample (CLSI).3 The clotting time of a plasma (or whole blood) sample in the presence of a preparation of thromboplastin and the appropriate amount of calcium ions (WHO).6
Specific ISI – a thromboplastin ISI that is generated by the reagent manufacturer specific for the particular thromboplastin/instrument combination. Validation – the action (or process) of proving that a procedure, process, system, equipment, or method used works as expected and achieves the intended result (WHO).6
ImPROVInG InR VARIAbIlITy
Many factors can contribute to a compounding effect of an inaccurate INR. Factors including but not limited to increasing inter-laboratory precision are:
• incorrectISIassignmentbythemanufacturer,
• usingtheincorrectmanufacturerassignedISI,
• usingagenericISInotvalidatedlocally,and
• failuretoestablishorcalculateageometricmeanfortheMNPT.
Throughout the 1990s, improving inter-laboratory variability of the INR using either a direct PT-INR calibration curve or a locally calibrated ISI was recognized. Although both methods can improve the precision of INRs reported, the direct PT-INR calibration curve has the potential to provide greater accuracy.7 However, this has not been implemented for two reasons: first, instrumentation software is not available to most instruments and second, there is a lack of validator/calibrator plasmas.
The focus of this article is to review the present state of the validation and calibration of the ISI and to offer suggestions when validating lots of PT reagent.
VAlIDATIOn AnD CAlIbRATIOn OF ThE IsI The ISI is used in the INR calculation as a measure of the
responsiveness of the thromboplastin reagent to levels of vitamin K-dependent coagulation factors. The process of deriving a reagent and instrument specific ISI is long and labour-intensive, thus manufacturers provide ISIs specific to their reagent/instrument combination and/or a generic ISI. If the laboratory’s reagent/instrument combination is not listed, laboratories tend to use the generic ISI if available; however, this may not be the true ISI as even instruments using the same principle of analysis may be different due to mechanisms of analysis and the laboratory’s conditions. CLSI guidelines state that the thromboplastins with a generic ISI should never be used clinically unless validated locally.3
Whether a specific or generic ISI is used, the most suitable ISI for each instrument within a laboratory is a successfully validated ISI or a locally derived ISI. To ensure the application of the most suitable ISI, the laboratory must first validate the manufacturer’s
ISI. It is only when validation fails that a calibration is necessary to obtain a local ISI.
To validate or verify the manufacturer’s ISI, obtain a set of certified validator plasmas from the thromboplastins manufacturer and assay according to the laboratory’s standard procedure. If none of the INRs deviate more than 15% from the validator plasmas assigned INR, the manufacturer’s ISI is validated and is therefore, the most suitable ISI for use. If any one of the recovered INRs deviate more than 15% from the validator plasmas assigned INR, a local ISI calibration should be performed.
To calibrate, obtain a set of certified calibration plasmas different than those used for validation and assay according to the laboratory’s standard procedure. Plot the recovered calibrant values in seconds against the assigned PT value of certified plasmas. The local ISI is determined from the slope of the orthogonal regression.3 Manufacturers may also provide this service for the laboratory. Finally, using the new ISI, re-validation must be performed and the resulting INRs should now all be within 15% of the assigned values. If the re-validation INRs still differ more than 15% from the assigned values, the reagent manufacturer should be consulted in an attempt to determine the root cause of the discrepancy.3
Manufacturers may also provide a local MNPT from the calibration data. If the manufacturer’s MNPT differs from the locally calculated MNPT, it is important to perform a correlation comparison between the old lot’s ISI and MNPT to both the new lot’s ISI and locally calculated MNPT and to the new lot’s ISI and manufacturer calculated MNPT to determine the most suitable MNPT for the laboratory.
The validation and calibration combination for ISI verification is strongly recommended for all laboratories and especially for laboratories using different reagent/instrument combinations. Laboratories strive to be accurate and precise in the results they provide and the local ISI validation and calibration is one of many tools we can use to achieve that goal. However, although much has been published about the local validation and calibration of the ISI, there are few products available in the market for laboratories.

Scientific Section
26 | CJMLS Fall 2011
At this time, only one company, Instrumentation Laboratory, has just recently introduced a Food and Drug Administration (FDA) and Health Canada (HC) approved ISI validator/calibrator
set for use on their own reagent/instrument combination. Table 1 is a summary of the products currently available on the market:
Manufacturer Product Validator Calibrator FDA andHC approved
Comments
Instrumentation Laboratory (IL)
HemosIL® INRValidate / ISICalibrate and ISIweb
specific to IL reagents andinstruments
Stago Etaloquick® HC approved doesn’t meet minimum numberof calibrant plasmas
Siemens PT-Multi Calibrator HC approved specific to Siemens reagents andinstruments, has been used with Stago instruments
Technoclone AK-Calibrant can be used on different reagents, instrument combinations (not instrument specific, thus only a validator)
TCoag (formerly Trinity Biotech)
Accuclot INRCalibrator Set
not currently in production, onlyCE approved (European marking)
Table 1. Current Validator and Calibrator Kits.
We are seeking interested CSMLS members to serve on the CSMLS Nominating Committee. This commitee plays an essential role in recruiting members to stand for election to the CSMLS Board of Directors. The term of appointment is up to three years.
Representatives are needed for each of the following positions:
Position TermQuebec 2012 - 2014
Alberta & NWT 2012 - 2014
Eligibility:Must be a member in good standing and be willing to serve for the time allocated.
How to Apply:
Submit a letter of application to:Carol Green, Chair 2011 Nominating Committeec/o CSMLS PO Box 2830 LCD 1Hamilton ON L8N 3N8oremail your letter to:Christine Nielsen, Secretary of the Nominating [email protected]
Help shape the future of your national society!
Call for Nominating Committee Volunteers
Application Deadline: October 20, 2011

Scientific Section
CJMLS Fall 2011 | 27
The lack of commercially available certified validator and calibrator plasmas make it difficult for the laboratory to comply with the guidelines. So what should we do when changing reagent lot numbers, instruments or evaluating new reagents?
VAlIDATIOn OF nEW lOTs OF PT REAGEnT
Past and Current Practices
For many laboratories large and small, the current practice when changing PT reagent lots is simply to run a set of normal donor plasmas to check the MNPT and to run normal and abnormal patient plasma samples in parallel with the old lot of reagent. The INRs using the new reagent are calculated using the new MNPT and the stated manufacturer’s ISI. The MNPT should not deviate significantly from lot to lot if the same reagent is used. If the new and old reagent lots correlate within the criteria set by the laboratory, the new lot may be accepted.
Currently, no published guideline is available on new and old lot correlation acceptability criteria. However, as per the CLSI guidelines, validation INRs may deviate 15% from the assigned “true” value of the certified plasma.3 A paper published by Cary et al. on the implementation of instruments in a multi-site network set their acceptable ProTime deviation criteria to 5% and the Diagnostica Stago Protocol states an INR deviation of 10% for new and old lot correlation.8,9 Laboratories should also account for any obvious bias. If the new and old lot’s INRs do not correlate despite troubleshooting, the new lot should be returned to the manufacturer in exchange for another. This is a situation in which the availability of a local ISI validator and calibrator would be helpful.
Guideline of Recommended Practices and the Laboratory
Recent guidelines recommending the use of a local ISI validation and calibration along with other testing before introducing a new lot of PT reagent has even larger laboratories offering an extensive Coagulation testing panel searching for answers.3,5 Since few manufacturers offer an ISI validation and calibration kit, the best we can do for now is:
1. Use a reagent instrument combination which the manufacturer has an assigned specific ISI. Validate the ISI using validation plasmas if available.
2. If a reagent with a generic ISI must be used, ask the reagent manufacturer for a recommendation on validating the ISI.
3. Laboratories may try using other manufacturer’s calibrator kits as a validator (see Table 1) but not all of these kits are approved by Health Canada and the derived insert INR values used to validate or calculate a local ISI may not be applicable to all instruments. Consultation with the reagent manufacturer should be considered.
If the above solutions are not available, validate the new PT reagent using the following method. Note that these crossover studies should still be performed even if local validation/calibration is available.
1. Validate the MNPT by running 20 normal plasmas with each reagent set. Plasma may be obtained locally from normal volunteers or normal donor sets may be purchased from Precision Biologicals, Dartmouth, NS or Affinity Biological, Ancaster, ON. Both these manufacturers collect the plasmas into 3.2% sodium citrate. If using other sources for normal plasma, assure the citrate concentration is 3.2%.
2. Run a minimum of 20 abnormal plasmas. Ideally, half of these should be from patients on oral anticoagulants. If your laboratory does not test many patients on oral anticoagulants, it is a good policy to store these plasma at -35°C or colder throughout the year in anticipation of the next lot, reagent or instrument change. However, if not available, a normal plasma diluted in buffer may be used.
3. Calculate the INRs for the normal and abnormal plasmas using the established MNPT and ISIs for each reagent (old and new) and determine the differences between the pairs. If within the accepted percent difference and the bias is acceptable, the new lot of reagent may be used.
4. Factor and heparin sensitivities may be performed although neither are indicated by the CLSI guidelines for PT reagents.
When switching to a different manufacturer’s reagent or instrument, more normal and abnormal plasma should be correlated and factor sensitivities may be measured. The factor sensitivity of the reagent can be a useful reference for the laboratory and the clinician since it provides an overall sensitivity of the reagent to certain factors. However, determining the factor sensitivity for each change in lot of reagent may not be necessary. Each lot of reagent from the same manufacturer should be comparable to previous lots and local lot to lot correlations should either confirm or reject this assumption. Secondly, factor sensitivity determinations can be costly, especially to smaller laboratories who do not use and stock deficient plasmas. Furthermore, it is important to note that factor sensitivities are only an estimate and will vary with different deficient plasma and normal plasma preparations.
While it is important for laboratories to strive for the most accurate patient results, we are limited to the tools available on the market and secondly to the limited resources all laboratories are faced with. A remarkable effort is being made by manufacturers to produce reagents that compliment the laboratory’s need and the local ISI validator/calibrator set is likely the next new addition to each manufacturer’s product line-up.

REFEREnCEs
1. Horsti J, Uppa H, Vilpo JA. Poor agreement among prothrombin time international normalized ratio methods: comparison of seven commercial reagents. Clin Chem. 2005;51:553-560.
2. Shahangian S, Labeau KM, Howerton DA. Prothrombin time testing practices: adherence to guidelines and standards. Clin Chem. 2006;52:793-794.
3. CLSI, Procedures for Validation of INR and Local Calibration of PT/INR Systems; Approved Guideline. CLSI document H54-A. Wayne, PA: Clinical Laboratory Standards Institute; 2005.
4. van den Besselaar AMHP, Barrowcliffe TW, Houbouyan-Réveillard LL, Jespersen J, Johnston M, Poller L, Tripodi A on behalf of the Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the ISTH. Guidelines on preparation, certification, and use of certified plasmas for the ISI calibration and INR determination. J Thromb Haemost 2004;2:1946-53.
5. Quality Management Program – Laboratory Services. Broadsheet – Evaluation of a New Lot Number of Prothrombin Time and Activated Partical Thromboplastin Time Reagent. [Database on the Internet]. Toronto (ON). QMP-LS QView™. c 2009. [updated 2009-12-09; cited 2009 Jun15] Available in: https://home.qmpls.org/qview/FileView.aspx?resourceid=296900
6. WHO/LAB/98.3. The Prothrombin Time. c 1998.
7. Adcock DM, Johnston M. Evaluation of frozen plasma calibrants for enhanced standardization of the International Normalised Ratio (INR): a multi-center study. J Thromb Haemost 2002;87: 74-79.
8. Diagnostica Stago, Protocol Quick User Guide, v4-07, [email protected]
9. Cary ER, Fink, LM, Stokes SL, Simmons VL, Kaczor DA, Harmon S, Quarles L, Escobar C, Joiner Maier D. Selection and implementation for coagulation instruments/reagents in a multiple hospital/clinic network. Blood Coagulation and Fibrinolysis 2000;11:599-608.
Scientific Section
28 | CJMLS Fall 2011
Happy HalloweenFrom Learning Services
Laboratory Diagnosis of Malaria (#4049)
Microanatomy 1 (#4988)
Microanatomy 2 (#4989)
Lymphocytes in Disease (#3050)
Kidney: Physiology, Disease and Measurement of Function (#4120)
Liver: Physiology, Disease and Measurement of Function (#2934)
Transfusion Medicine Refresher Course (#4336)
Systèmes de Contrôle de la Qualité pour le Laboratoire Clinique: Partie I (Introduction) (#4812)
Systèmes de Contrôle de la Qualité pour le Laboratoire Clinique : Partie II (Planification/Conception) (#4923)
Medical Mycology (#4344)
Register for one of these courses starting in October and scare 10%
off the total price!
For more information visit www.csmls.org/ce
*In order to take advantage of the 10% member discount please register via fax 905-528-4968. Online registration is unavailable.
Happy HalloweenFrom Learning Services
Laboratory Diagnosis of Malaria (#4049)
Microanatomy 1 (#4988)
Microanatomy 2 (#4989)
Lymphocytes in Disease (#3050)
Kidney: Physiology, Disease and Measurement of Function (#4120)
Liver: Physiology, Disease and Measurement of Function (#2934)
Transfusion Medicine Refresher Course (#4336)
Systèmes de Contrôle de la Qualité pour le Laboratoire Clinique: Partie I (Introduction) (#4812)
Systèmes de Contrôle de la Qualité pour le Laboratoire Clinique : Partie II (Planification/Conception) (#4923)
Medical Mycology (#4344)
Register for one of these courses starting in October and scare 10%
off the total price!
For more information visit www.csmls.org/ce
*In order to take advantage of the 10% member discount please register via fax 905-528-4968. Online registration is unavailable.

Located minutes from Parliament Hill, the luxurious five-star Hilton Lac-Leamy offers a variety of restaurants and bars, a fitness centre, a spa, indoor and outdoor pools, tennis courts, not to mention the Theatre and Casino!
RESERVE YOUR ACCOMMODATIONS NOWfor LABCON2012 June 2nd - 4th as CSMLS/SCSLM celebrates its 75th anniversary.
HILTON LAC-LEAMY PROUD HOST OF
1, Boulevard du Casino, Gatineau (Québec)[email protected] | casinolacleamy.ca 1 866 488.7888
CSMLS’s National Conference of Medical Laboratory Science
Rates starting at $189mention room block: CMUor reserve online at www.csmls.org/labcon2012
Located minutes from Parliament Hill, the luxurious five-star Hilton Lac-Leamy offers a variety of restaurants and bars, a fitness centre, a spa, indoor and outdoor pools, tennis courts, not to mention the Theatre and Casino!
RESERVE YOUR ACCOMMODATIONS NOWfor LABCON2012 June 2nd - 4th as CSMLS/SCSLM celebrates its 75th anniversary.
HILTON LAC-LEAMY PROUD HOST OF
1, Boulevard du Casino, Gatineau (Québec)[email protected] | casinolacleamy.ca 1 866 488.7888
CSMLS’s National Conference of Medical Laboratory Science
Rates starting at $189mention room block: CMUor reserve online at www.csmls.org/labcon2012

Too often customer service and support means listening
to recorded messages or waiting for answers that never
come. Maine Standards Company has experts ready to
help: people who know our products in detail and can
help you with any question or concern. Working with us
is always a guarantee of responsive service.
To learn more, call us at 1-800-377-9684 or visit
mainestandards.com.
Expert service and support that won’t keep you waiting.

sOCIETy nEWs
CJMLS Fall 2011 | 31

Society News
32 | CJMLS Fall 2011
More than 465 lab professionals descended on Halifax, Nova Scotia on Friday, June 10 to take part in LABCON2011, Canada’s premier medical laboratory conference. LABCON is CSMLS’s hallmark event of the year and the 2011 edition was no exception.
The opening ceremonies kicked-off the event with an interactive drum session. This high-energy performance by Drum!Power set the tone for LABCON2011 and the event just got better from there.
Over 50 speakers were on-hand to deliver first-rate scientific sessions on a wide variety of laboratory topics. The LABCON agenda included sessions with broad appeal, such as the challenges of Millenials, Gen X and Boomers working together, and those geared towards specific specialties, such as current trends in genetics and molecular biology. No matter your specialty or area of interest, there was something for everyone. With participants receiving four Professional Enhancement Program (PEP) hours per day of attendance, LABCON was an efficient way to meet your professional development goals.
LABCON was also a great way to see the latest and greatest in technology. The trade show exhibits allowed LABCON attendees an opportunity to browse the latest equipment, reagents and supplies from some of the industry’s largest
vendors, including Siemens, who were our LABCON2011 Elite Sponsor. Over 45 vendors took part as exhibitors, making this one of the largest tradeshows in LABCON history.
As anyone who has attended LABCON in the past can attest to, the LABCON experience is more that just a formal learning opportunity. An important part of the experience is networking and building relationships with lab professionals from across the country. To facilitate this — and have a little fun too — LABCON organizers planned a series of social events.
The President’s Reception was held at the historic Pier 21. For over 50 years Pier 21 welcomed over a million immigrants, refugees, war brides and their children to Canada. Now a museum, this venue served as a fascinating and poignant backdrop for the formal reception.
As Sunday’s sessions came to a close, LABCON attendees took to the seas for what was touted as the “Ultimate Halifax Experience”. The name was not misleading. The evening included a harbour tour aboard the Haligonian II and Harbour Queen, a traditional lobster dinner, and ended with local music and dancing. This fun evening was a great way to let go of some stress and recharge for the return home.
LABCON2011 closed with a retrospective look back on the glory days in lab
sciences, humorously delivered by former CSMLS President Barbara Hall. It was a fitting topic as we look forward to CSMLS’s 75th anniversary in 2012. A new bar of excellence was set in Halifax, but plans are already underway to make LABCON2012 even better. We hope you will be able to join us in Gatineau, Quebec and help us celebrate 75 years of CSMLS.
Looking back at LABCON2011Michael Grant
Team Leader, Communications
CSMLS’s National Conference of Medical Laboratory ScienceCongrès national de science de laboratoire médical de la SCSLM
For more information about LABCON2012
visit www.csmls.org/labcon2012 or email [email protected].

Society News
CJMLS Fall 2011 | 33

Society News
34 | CJMLS Fall 2011

Society News
LABCON2012 HotlineNeed help getting to LABCON2012? This year, CSMLS wants to give you a helping hand when planning your trip to LABCON2012. We will be setting up the LABCON2012 Hotline, where CSMLS staff will be ready to take your calls during regular office hours. We can help simplify your travel arrangements and offer you great cost-saving tips and ideas.
• Willtravellingbytrainhelpsavememoney?
• Howmuchwillacabridecostfromtheairport?
• Whatarethe‘must-see’attractionsofOttawaandGatineau?
We will be happy to answer all of your questions and help you make the most of your LABCON2012 experience.
Our phone lines are open. Call us today at 1-800-263-8277 (Monday-Friday 9 a.m.-5 p.m. EST) to reach our LABCON2012 Travel Hotline.
CJMLS Fall 2011 | 35
Website RenovationIn the next few months CSMLS will be launching a newly redesigned website. We are very excited about this transition. Not only will the website incorporate the new CSMLS branding, but it will also introduce some exciting new features.
One major change will be the addition of a Members Only section on the website. Here, CSMLS members will have full access to discount programs, job postings, publications and other exclusive content. We are also planning some fun and interactive components too, just for members.
The website will be integrated with the new member database system, which will allow members to access and maintain their own information. With a click of the mouse each member will be able to change their address, sign-up for courses or register for LABCON. Easy-to-use tools will make your online experience simple and efficient.
Having trouble finding things on our website? The new site will have a simplified menu and an easy search feature to help you find what you are looking for. Whether it’s news on the profession, resource information, or job postings, you will be able to find it quickly and easily. We want the new CSMLS website to be the only website members need for professional news, education and information.
At the same time the website will also be a hub of information for the general public looking to learn more about the medical laboratory profession, education and the society’s role. As a vital link between CSMLS, our members and the general public, the new website will project an image of professionalism and quality. Keep an eye out for this exciting new development in the late fall.

July:Collaboration Roadshow: Ontario (Toronto)
International Qualifications Network (IQN)
Meeting with Diane Finley, Minister of Human Resources and Skills Development – HRSDC
AuGusT:Collaboration Roadshow: Ontario (Toronto, Kingston and Peterborough)
sEPTEmbER:Michener English Language Assessment (MELA) Working Group
Ontario Society of Medical Technologists (OSMT) Conference
International Federation of Biomedical Laboratory Science General Assembly of Delegates
British Columbia Society of Laboratory Science (BSCLS) Conference
Canadian Network of National Association of Regulators (CNNAR) Meeting
Health Canada Meeting
Health Action Lobby
CSMLS – The National Voice of Canada’s Medical Laboratory Profession
As the national voice of Canada’s medical laboratory profession, CSMLS is represented on several laboratory and health care-related organizations. Members of the CSMLS Board of Directors and staff attended meetings of these organizations, and represent the Society at provincial congresses and special events across the country. Here’s where your voice was heard recently:
Society News
36 | CJMLS Fall 2011
Share your memories, stories and old photos to celebrate our 75th anniversary!In 2012, Canadian Society of Medical Laboratory Science (CSMLS) will mark its 75th anniversary. We want you, our valued members, to share your memories of belonging to the organization that has been representing the medical laboratory profession in Canada since 1937.
What does 75 years of CSMLS mean to you? What has made you feel proud of being a CSMLS member? What event(s) stand out to you? Send us your stories and fond memories and we will share them on our micro-website devoted to commemorating our 75th anniversary. E-mail your stories and old photos along with your full name and address to [email protected].
Celebrating 75 years / Célébrons nos 75 ans
What does 75 years of CSMLS mean to you?

A91
DX-
9158
-A1-
4A00
. Not
ava
ilabl
e fo
r sal
e in
the
U.S
. ©20
11 S
iem
ens
Hea
lthca
re D
iagn
ostic
s In
c. A
DV
IA C
enta
ur a
nd a
ll as
soci
ated
mar
ks a
re tr
adem
arks
of S
iem
ens
Hea
lthca
re D
iagn
ostic
s In
c.
Testing for vitamin D has always been a complicated process. Now labs can test for total 25(OH) vitamin D (D2 and D3) in 18 minutes or less on the ADVIA Centaur® family of instruments — quickly, accurately, and with full automation. This new assay arrives just in time. Demand for vitamin D testing continues to grow, prompted by emerging research on the importance of vitamin D to wellness. With the new Siemens equimolar Vitamin D Total assay, testing is within the reach of labs of all sizes. That means physicians
and patients can benefit from getting their vitamin D testing results faster. And it means labs will be better prepared to meet today’s demands — and tomorrow’s. Learn more about how the new ADVIA Centaur Vitamin D Total assay is a viable solution for your lab by downloading educational white papers at www.siemens.com/vitamindtotal
Answers for life.

Enhance your skills and build your resume! csMLs is proud to offer new certificates available through our Learning services team. Discipline-specific and interdisciplinary certificates are available with more certificates in development.
certificates available in three levels: Refresher, Basic and Advanced
• Refresher or Basic certificate you must complete at least 60 hours
• Advanced certificate you must complete at least 90 hours
for more information, visit www.csmls.org
Refresher
certificate in Hematology Refresher
certificate in Transfusion Medicine Refresher
certificate in Microbiology Refresher
basic
certificate in Leukocytes
certificate in Basic Microbiology
certificate in Pre-Analytical Procedures; Great for mlAs!
certificate in Laboratory safety; Great for mlAs!
Advanced
certificate in Transfusion Medicine challenges
certificate in fungi
certificate in Quality systems
learning services Certificates
CSMLS PO Box 2830, LCD 1 Hamilton, ON L8N 3N8 www.csmls.org