california department of aging (cda) presentation on disaster preparedness and avian/pandemic...
TRANSCRIPT

California Department of Aging (CDA) Presentation on Disaster Preparedness and
Avian/Pandemic Awareness March 23, 2006
By: Robert Ramsey-Lewis, Policy Manager
Prepared For: California Association of Area Agencies on Aging (C4A)
Materials From: California Department of Health Services, World Health Organization, US Health and Human Services, and Canadian Network for Emergency Preparedness and Response

Introduction
“Any community that fails to prepare with the expectation that the federal government will, at the last moment, be able to come to the rescue will be tragically wrong.
--Mike Leavitt, US Health and Human Services Secretary
• When is an Emergency a Disaster?– A disaster occurs when the impact on the community
exceeds its normal coping resources– A community’s coping resources are its people,
materials, equipment, and services used to meet demand created by an incident
• Preparedness moves the disaster threshold.– Preparedness measures, e.g., evacuating vulnerable
populations, increases the disaster threshold, permitting the community to cope better.
Source: Canadian Network for Emergency Preparedness and Response, 2004

Area Plan Guidance
• Appendix XI, Disaster Preparation Planning, is optional for the 2006-2007 planning period.
• Appendix XI will be required for the 2007-2008 planning period, in addition to an area plan objective concerning preparedness.
• Opportunity for input on the 2007-2008 Area Plan Guidance in the Fall, 2006.

Avian and Pandemic Influenza
Howard Backer, MD, MPHCalifornia Department of Health Services
Sandra Shewry, Director
Mark Horton, State Public Health Officer


WHO Lab Confirmed Human Cases
CasesCases DeathsDeaths
IndonesiaIndonesia 16 16 (29)(29) 11 11 (22)(22)
VietnamVietnam 9393 4242
ThailandThailand 2222 1414
CambodiaCambodia 44 44
ChinaChina 7 7 (15)(15) 3 3 (10)(10)
TurkeyTurkey
AzerbaijanAzerbaijan
IraqIraq
4 4 (12)(12)
77
22
2 2 (4)(4)
55
22
TotalTotal 146 146 (184)(184) 76 76 (103)(103)
As of Mar. 21 2006 Mortality 52%
Requirements for a Pandemic
• Unusual type of influenza virus found in humans
• Little or no immunity in the population
• Virus can multiply and cause disease in humans
• Easily spreads from person to person

WHO Pandemic PhasesPhase 1 Interpandemic No new subtype
Phase 2 Interpandemic Risk from novel type
Phase 3 Alert phase Human infection-rare spread to contact
Phase 4 Alert phase Limited human to human transmission
Phase 5 Alert phase Small clusters; poorly adapted
Phase 6 Pandemic period
sustained transmission
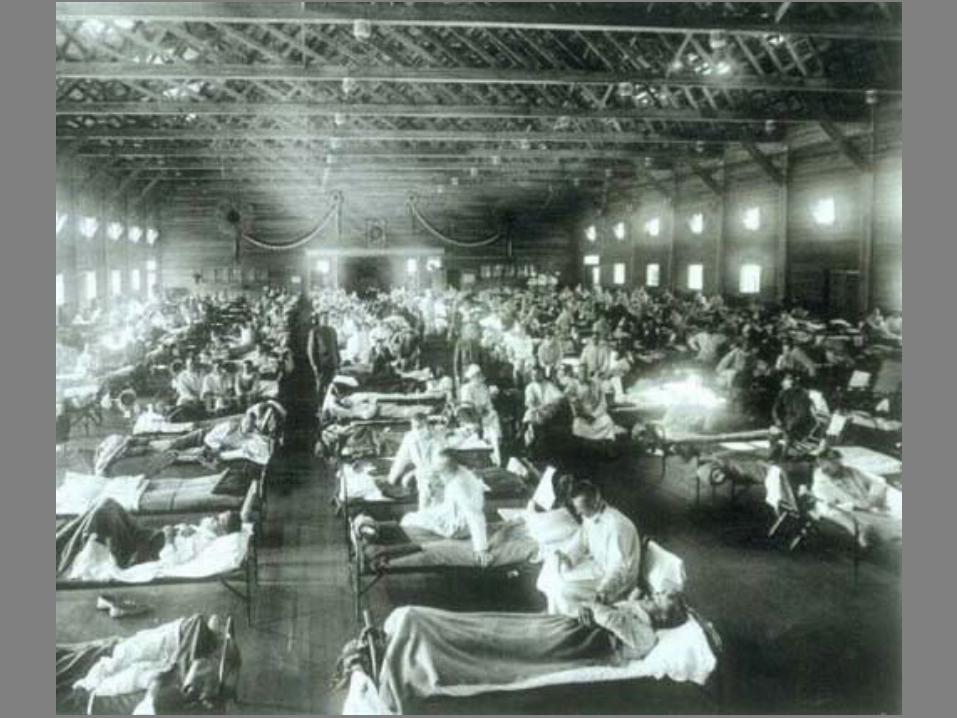
Human influenza transmission

Year Flu Virus Mortality
1918-1919 “Spanish” H1N1 20 million
550,000 US
1957-1958 “Asian” H2N2 70,000 US
1968-1969 “Hong Kong” H3N2 34,000 US
Glezen WP. Epidemiol Rev. 1996;18:65.CDC. Influenza Prevention and Control.
20th Century Influenza Pandemics Which will the next pandemic resemble?
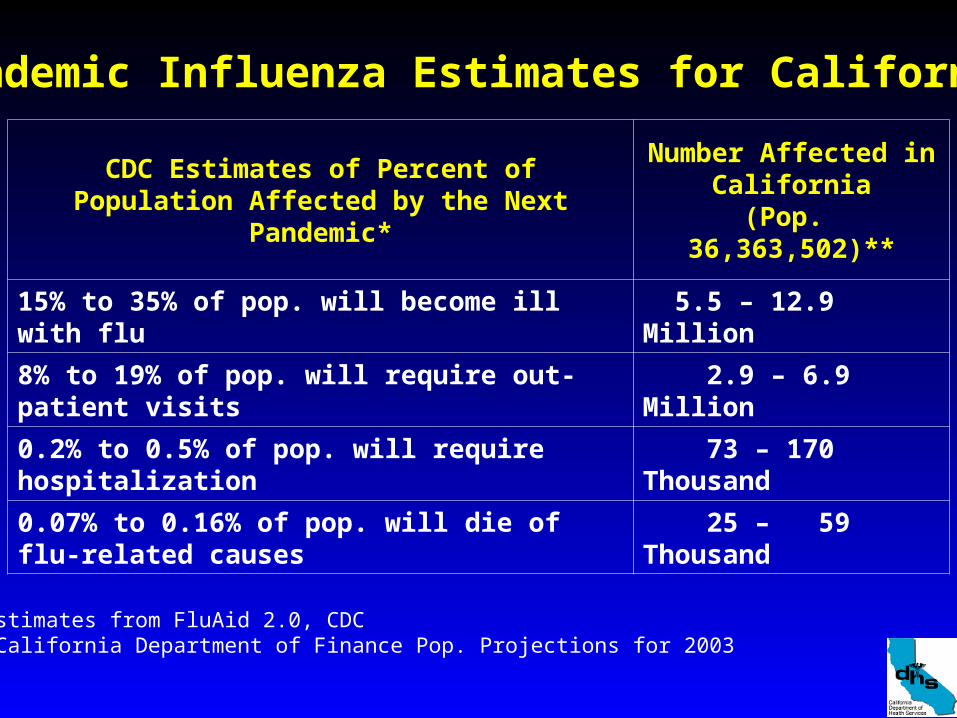
CDC Estimates of Percent of Population Affected by the Next Pandemic*
Number Affected inCalifornia
(Pop. 36,363,502)**
15% to 35% of pop. will become ill with flu 5.5 – 12.9 Million
8% to 19% of pop. will require out-patient visits 2.9 – 6.9 Million
0.2% to 0.5% of pop. will require hospitalization 73 – 170 Thousand
0.07% to 0.16% of pop. will die of flu-related causes
25 – 59 Thousand
Pandemic Influenza Estimates for California
*Estimates from FluAid 2.0, CDC**California Department of Finance Pop. Projections for 2003
Components of CDHS Pandemic Planning
• Organization of response and authorities• Surveillance• Lab Capacity• Infection control• Case Management• Vaccine and antiviral• Community Outbreak Control--nonmedical• Health care planning--surge capacity • Communications
Planning Assumptions
• It will not be business as usual
• All sectors of society and government will be involved
• Widespread impact limits mutual aid
• Sustained response required
• Workforce will be impacted, adding to disruption

Major response challenges
• Health care capacity – Estimates of hospitalizations and deaths vary by
factor of 10, based on prior pandemics
• Pharmaceutical solution overly optimistic• Need to maintain critical infrastructure• Coordination of volunteers• May introduce extreme and unusual measures • Public will adopt their own measures• Communication
Avian H5N1 VaccineCurrent influenza vaccine is not protective
Federal government – Support R&D, production capacity, and stockpile
Federal HHS plans to buy vaccine for 20 million
– Distribute vaccine to states
Estimate 6 month to produce enough vaccine
CDHS – Distributes to local health departments– Technical assistance for mass vaccination– Sets prioritization policy

National Vaccination Priority Recommendations*Tier Element
1A • Health care involved in direct patient contact and essential support• Vaccine and antivirals manufacturing personnel
1B • Highest risk group (6 mos to 64 yrs with 2 or more risk conditions)
1C • Household contacts of children <6 months and severely immune compromised, and pregnant women
1D • Key government leaders and critical public health responders
2 • Remainder of high risk group (1 risk condition, healthy 6-23 mo)• Other public health responders and infrastructure personnel
3 • Other key government health decision makers and mortuary services
4 • Healthy 2-64 years not in other groups
*Approved by NVAC/ACIP committee on July 19, 2005
# indv
9 m
40 K
26 m
11 m
151 K
60 m
8.5 m
500 K
180 m

• Single manufacturer• Worldwide shortage• Use for treatment or
prevention• Prioritization
challenges• Virus may develop
resistance• Federal and state
stockpiles
Anti-viral Medication

Outbreak Containment Measures vary as pandemic develops
• Steps to reduce individual exposure to virus—(respiratory hygiene, masks)
• Isolation (confinement) of ill persons
• Quarantine of exposed persons
• Pharmaceuticals
• Community-based containment– Cancellation of events, schools, public
meetings, malls, businesses, transportation– Snow days: nearly everyone stays home


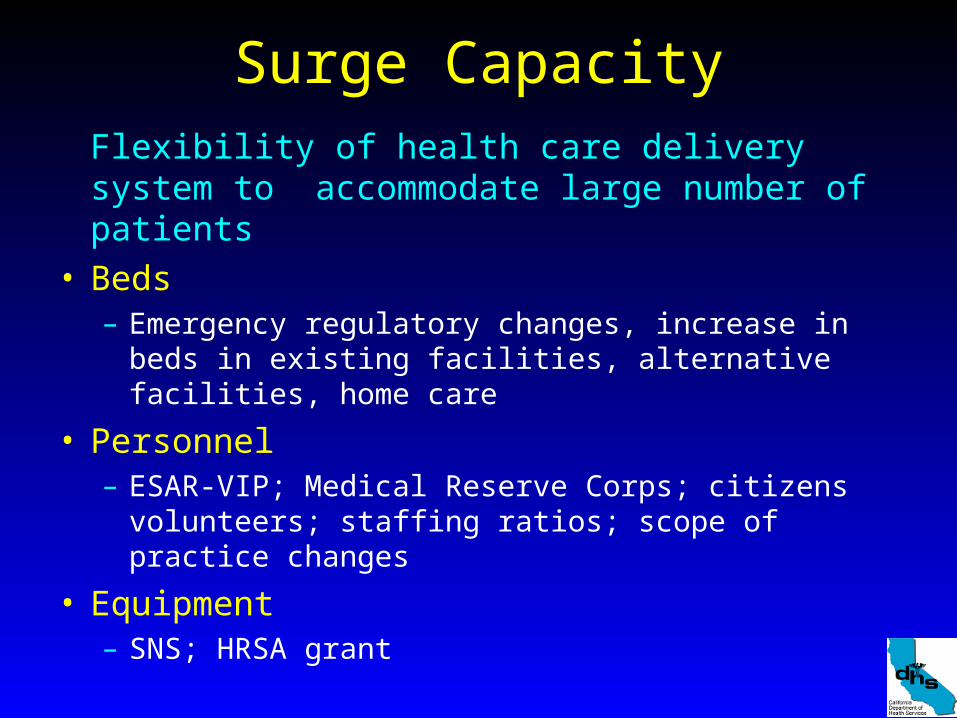
Surge CapacityFlexibility of health care delivery system to accommodate large number of patients
• Beds– Emergency regulatory changes, increase in beds in
existing facilities, alternative facilities, home care
• Personnel– ESAR-VIP; Medical Reserve Corps; citizens
volunteers; staffing ratios; scope of practice changes
• Equipment– SNS; HRSA grant
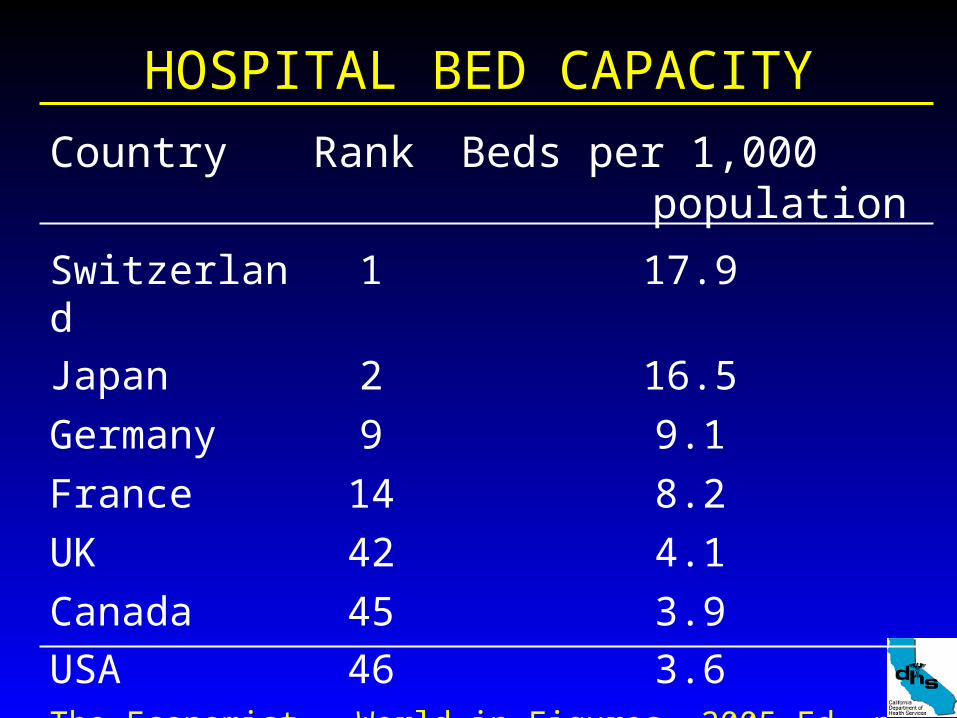
HOSPITAL BED CAPACITY
Country Rank Beds per 1,000 population
Switzerland 1 17.9
Japan 2 16.5
Germany 9 9.1
France 14 8.2
UK 42 4.1
Canada 45 3.9
USA 46 3.6The Economist. World in Figures, 2005 Ed, p 85

January 4, 2006Flu outbreak in Phoenix metro area
• Flood of visits to the emergency department and from illnesses on their own staff.
• Medical Center temporarily closed ED.• Half-day waits in overcrowded EDs. • Ambulance rides to other hospitals miles away. • Postponements of routine elective surgeries
and other medical procedures.• Ambulance patients diverted to other hospitals.• Staff sick calls are up 25 percent from last year.
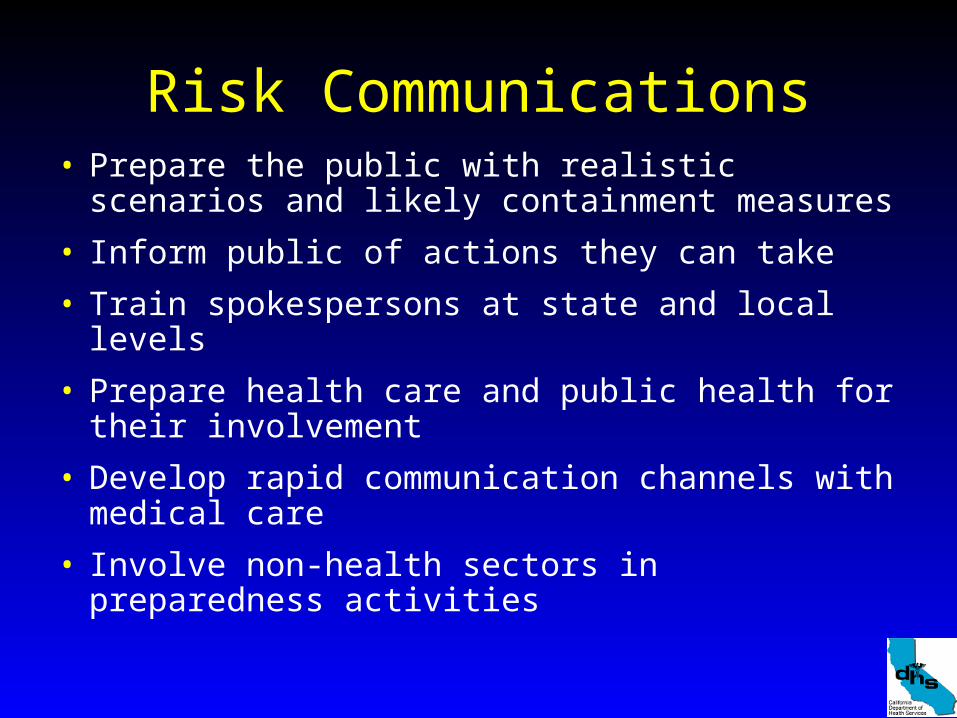
Risk Communications• Prepare the public with realistic scenarios and
likely containment measures
• Inform public of actions they can take
• Train spokespersons at state and local levels
• Prepare health care and public health for their involvement
• Develop rapid communication channels with medical care
• Involve non-health sectors in preparedness activities

HHS Department Collaboration
• Identify roles and responsibilities• Coordinate response in CA• Partners for social distancing decisions and
implementation• Continuity of government and operations• Communication channels• Educating workforce• Essential personnel for pharmaceuticals• Plans for institutional populations