c7 – squire foundations shoulder exam
TRANSCRIPT
Dr Pam Squire 2016
Speakers Bureau/Honoraria: Eli Lilly, Purdue,CanniMed Consulting Fees: Purdue, Eli Lilly Other:none
Potential sources of bias identified in the preceding slide have been mitigated as follows: ¡ Information in this talk is restricted to examination
techniques of the shoulder. No specific treatment recommendations will be made.
At the end of this presentation attendees will be able to: ¡ Discuss the concept of different “pain layers” and pain mechanisms that can contribute to an individuals chronic shoulder pain experience
¡ Demonstrate a brief shoulder exam designed to help evaluate 3 common presentations of chronic shoulder pain – the painful arc/subacromial impingement, adhesive capsulitis and shoulder pain due to myofascial pain syndrome.
A patient presents with a painful arc, shoulder weakness and anterior crepitus. Positive Hawkins and Neer tests would confirm which diagnosis?
1.Subacromial impingement 2.Myofascial pain 3. Rotator cuff tear 4. Labral tear 5. None of the above
A patient presents with a painful arc, shoulder weakness and anterior crepitus. Positive Hawkins and Neer tests would confirm which diagnosis?
1.Subacromial impingement 2.Myofascial pain 3. Rotator cuff tear 4. Labral tear 5. None of the above Hegedus E Br J Sports Med 2012;46:964–978
¡ There is no special tests that can distinguish between those conditions
¡ Current tests (Hawkins/Neer) have low sensitivities (best 74%/81%) and specificities (range 40-‐60%/10-‐55%)
¡ The tests used “structural failure” as the gold standard
¡ This is based on the premise that the structural failure is causing the pain
¡ But-‐ there are many studies demonstrating a very poor relationship between structural failure and pain
In one study of 59 people that used ultrasound to evaluate rotator cuff tears, what percentage of individuals with full thickness rotator cuff tears did not report pain? 1.40% 2.27% 3.12% 4. 80%
In one study of 59 people that used ultrasound to evaluate acromial shape, age and rotator cuff tears, what percentage of individuals with full thickness rotator cuff tears did not report pain? 1.40% correct answer 2.27% 3.12% 4. 80% Worland RL J South Orthop Assoc 2003
¡ Given that there is a poor relationship between pain and structural abnormality, how do we determine when there might be a causal relationship?
¡ There are over 108 special tests for the shoulder, which ones are most helpful clinically?
¡ 31-‐48% of general practice patients in the UK
¡ Other surveys 7-‐46%
¡ Only 50% seek medical care
¡ 95% managed by primary care
¡ Of all new cases-‐ 50% resolve within 6 months, 40% persist for up to one year
Meislin RJ, A Supplement to American Journal of Orthopedics Dec 2005, Wofford JL BMC Musculoskeletal Disord 2005
13
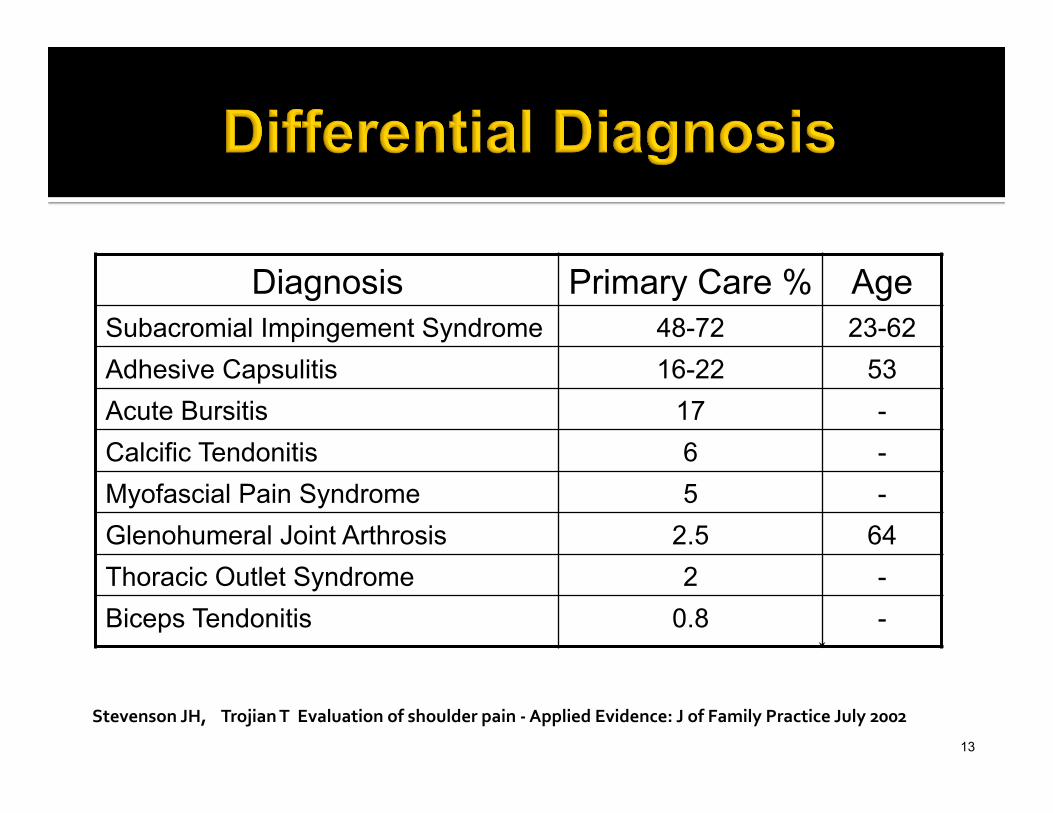
Diagnosis Primary Care % Age Subacromial Impingement Syndrome 48-72 23-62 Adhesive Capsulitis 16-22 53 Acute Bursitis 17 - Calcific Tendonitis 6 - Myofascial Pain Syndrome 5 - Glenohumeral Joint Arthrosis 2.5 64 Thoracic Outlet Syndrome 2 - Biceps Tendonitis 0.8 -
Stevenson JH, Trojian T Evaluation of shoulder pain -‐ Applied Evidence: J of Family Practice July 2002

¡ After 3 years, 90% report significant disability ¡ Sleep impairment ¡ Cognitive impairment (if moderate to severe) ¡ Functional difficulties with ADL’s
Macfarlane GJ, J Rheumatology 1998

15
Components of the assessment include 1. Focused history of pain and pain modifiers 2. Attentive physical examination 3. Thoughtfully ordered tests/studies ▪ for future discussion
Mary is a 58 yr old bank manager who is referred with the following diagnoses: ¡ supraspinatus tendinopathy ¡ myofascial pain ¡ deconditioning My exam: ¡ excessive sensitivity to gentle palpation and light touch consistent with abnormal pain processing/central sensitization.
¡ Her average pain score : 8/10
0
1
2
3
4
5
6
7
8
9
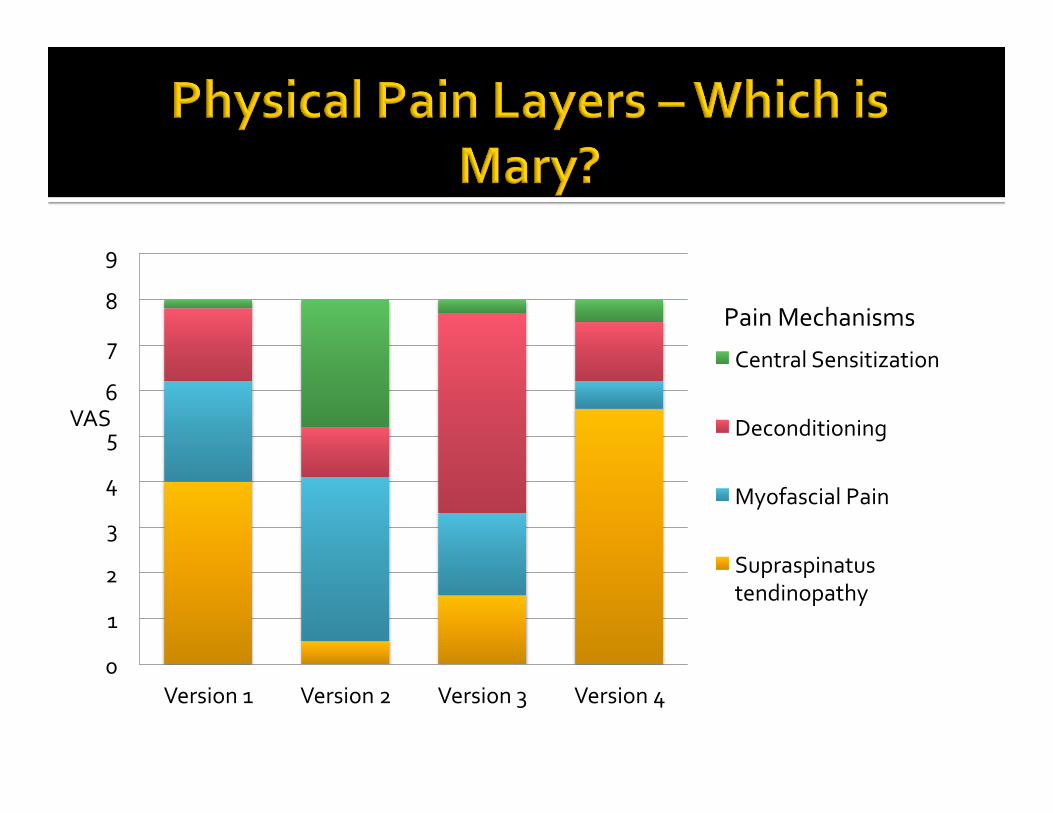
Version 1 Version 2 Version 3 Version 4
Central Sensitization
Deconditioning
Myofascial Pain
Supraspinatus tendinopathy
Pain Mechanisms
VAS
¡ In addition to physical mechanisms of pain there are other factors that can affect a pain experience.
¡ Thinking of your experience with individuals with chronic pain, please list other possible “layers” that could be contributing to Mary’s pain experience.
Pain Layers The physical pain layers
The emotional pain layers-How much the pain bothers you
The cognitive pain layers-What the pain means to you
¡ Try to develop a standard routine ¡ Reassure patient ¡ Compare shoulders ¡ Observation
§ Undress waist → up, women tank top or sports bra ¡ Palpation ¡ ROM ¡ Strength testing ¡ Special tests ¡ Assess -‐ “Inject”-‐ Reassess
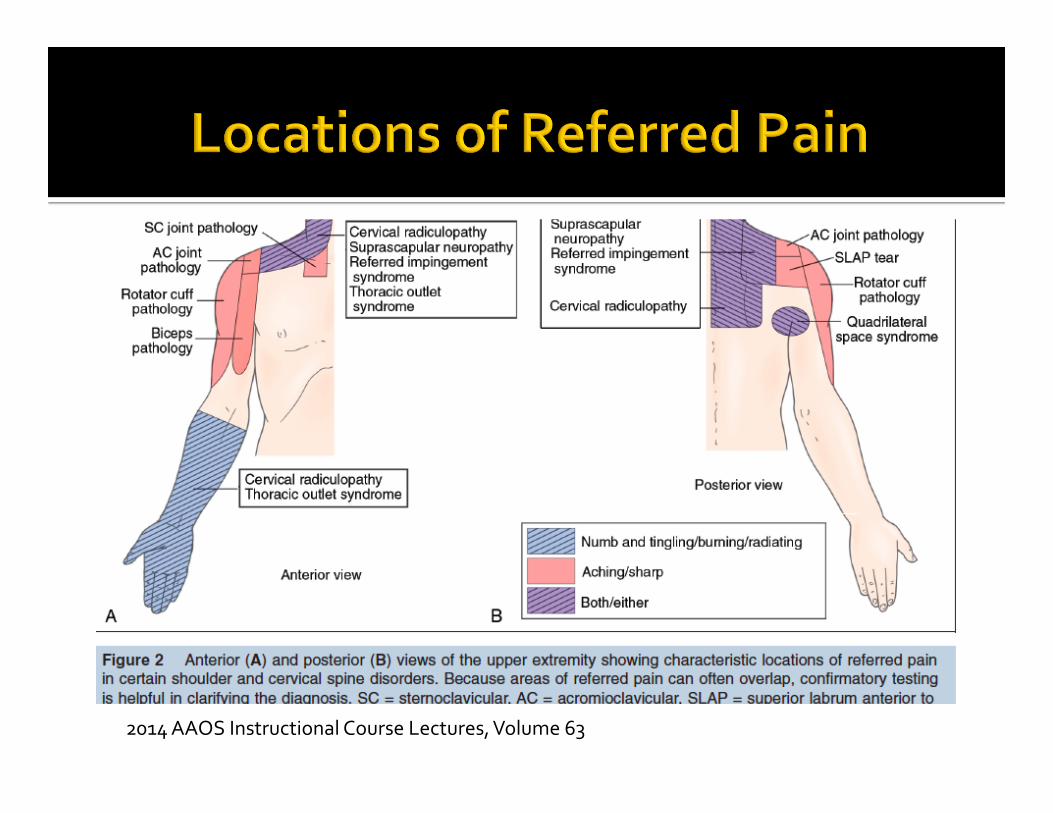
2014 AAOS Instructional Course Lectures, Volume 63
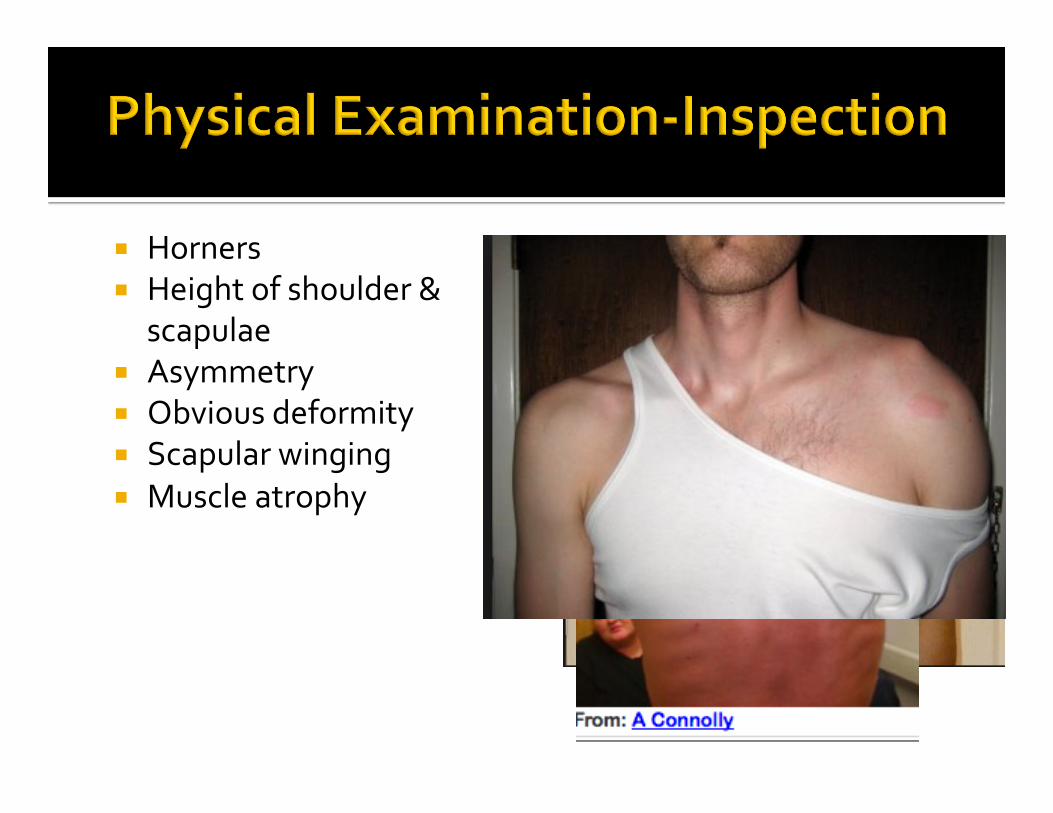
¡ Horners ¡ Height of shoulder &
scapulae ¡ Asymmetry ¡ Obvious deformity ¡ Scapular winging ¡ Muscle atrophy
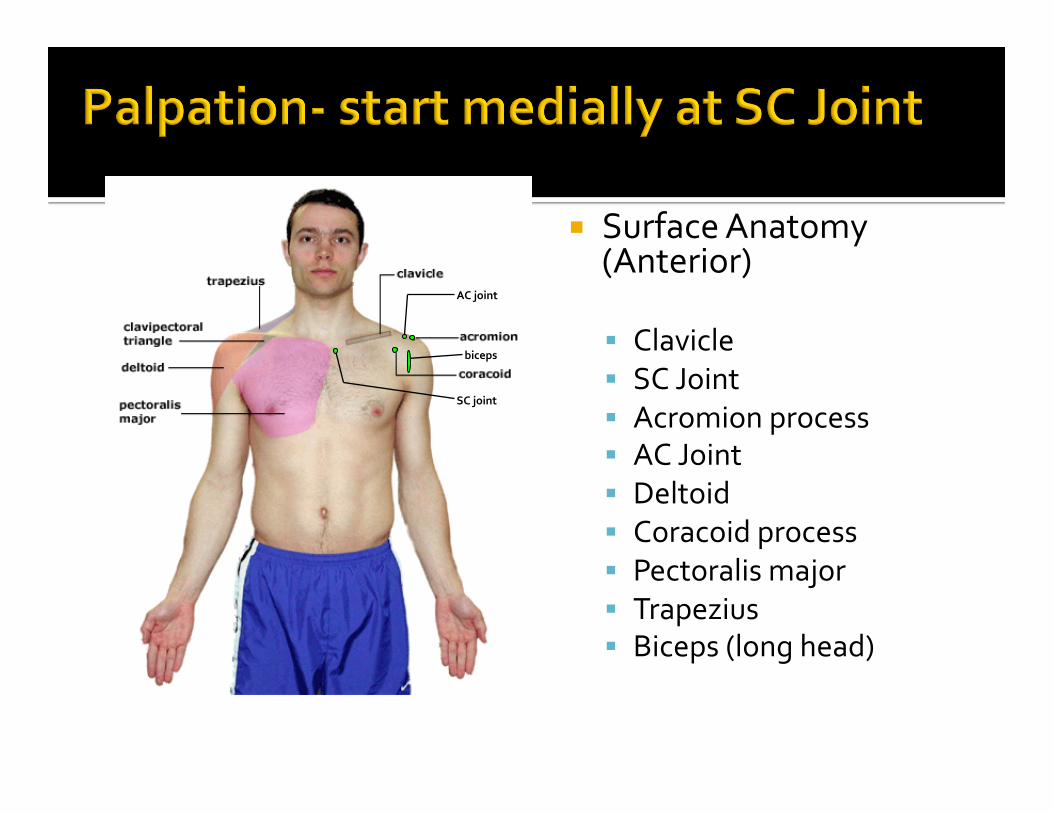
¡ Surface Anatomy (Anterior)
§ Clavicle § SC Joint § Acromion process § AC Joint § Deltoid § Coracoid process § Pectoralis major § Trapezius § Biceps (long head)
AC joint
SC joint
biceps
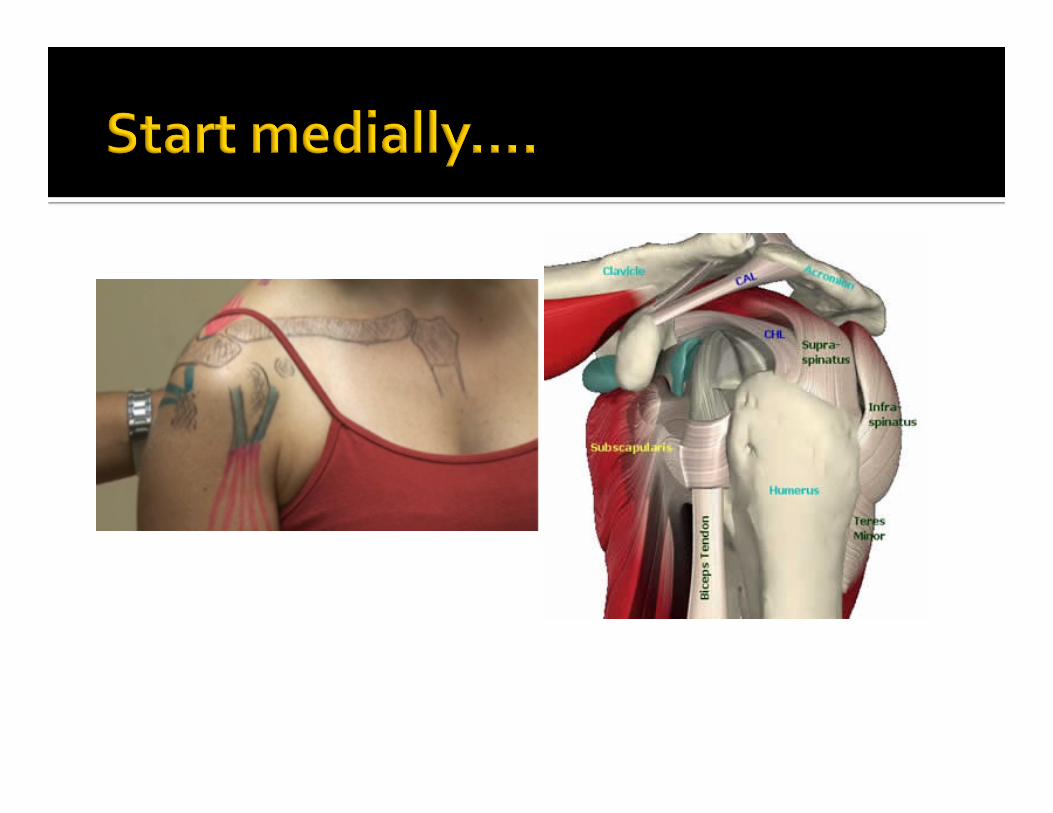

¡ Surface Anatomy (Posterior)
§ Scapular spine § Acromion process § Supraspinatus § Infraspinatus § Deltoid § Trapezius § Latissumus dorsi § Scapula ▪ Inferior angle ▪ Medial border
Supraspinatus
Infraspinatus
Inferior angle of scapula
¡ Coordinated shoulder motion
§ Glenohumeral motion
§ Scapulothoracic motion § Acromioclavicular motion
§ Sternoclavicular motion Scapulohumeral rhythm
¡ Always start with active ROM-‐ if its normal you’re done
¡ If movement limited evaluate glenohumeral movement-‐ stabilize acromium and clavicle
¡ How far can you abduct and forward flex without activating the scapula?
¡ What movements do not require any scapular movement?

¡ glenohumeral movement-‐ stabilize acromium and clavicle
¡ abduction to 110 ¡ forward flex to 120 ¡ and full ER or IR these movements do not require scapular movement
¡ Then assist passively

¡ Scapular dyskinesis
§ Compare scapular motion through ROM on both sides
§ Wall push-‐ups
§ Symmetrical § Smooth § No or minimal winging
Kibler WB. Clinical implications of scapular dyskinesis in shoulder injury: the 2013 consensus statement from the ‘scapular summit’. Br J Sports Med 2013;47:877–885.

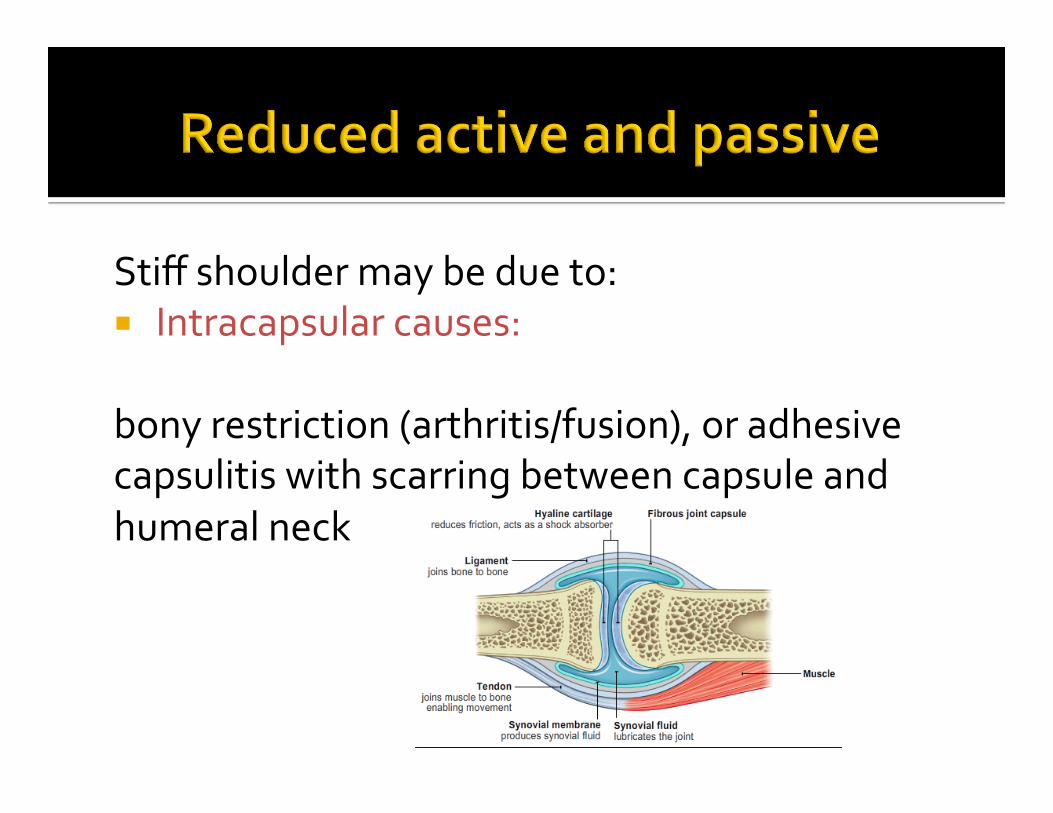
Stiff shoulder may be due to: ¡ Intracapsular causes: bony restriction (arthritis/fusion), or adhesive capsulitis with scarring between capsule and humeral neck
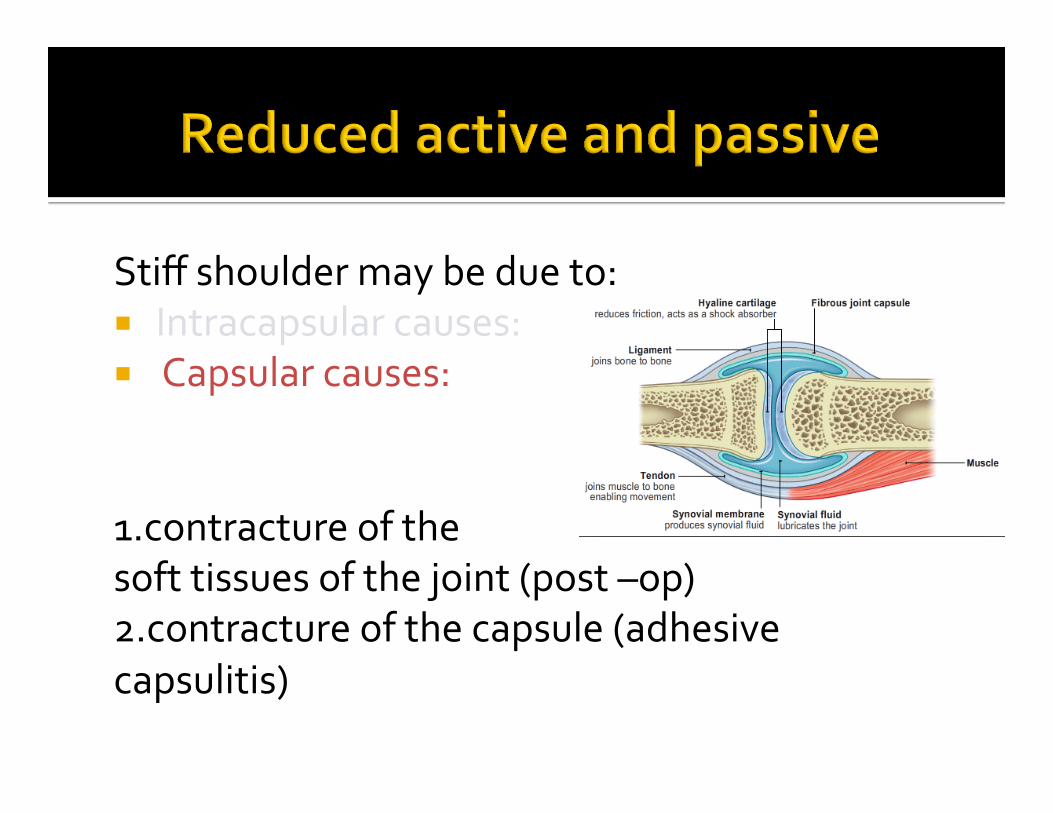
Stiff shoulder may be due to: ¡ Intracapsular causes: ¡ Capsular causes: 1.contracture of the soft tissues of the joint (post –op) 2.contracture of the capsule (adhesive capsulitis)
Stiff shoulder may be due to: ¡ Intracapsular causes: ¡ Capsular causes: ¡ Extracapsular causes: muscle tightness (myofascial pain) …..or interaction of all of these
What would differentiate an adhesive capsulitis
from myofascial pain?
¡ True muscle weakness ¡ Look for trick movements that hide weakness
Name three causes of weakness of shoulder abduction. ¡ C5 radiculopathy ¡ Rotator cuff tear ¡ C5/6 brachial plexus injury (telephone pole drill)
¡ Axillary nerve injury
Pain inhibition ¡ From an impinged structure ( painful arc)
¡ Muscle tightness due to trigger points and myofascial related pain.
Forward Flexion 150-‐ 180° Extension 40° Abduction 150-‐ 180° palm up Adduction 45° (J Shoulder Elbow Surg 2006;15:306-‐310.)
¡ The normal range of motion of external rotation is different if you test it with the elbow at the side or at 90° of abduction. Which position has the greater range of motion.
¡ Why?
External rotation arm by side 30-‐60° External rotation arm at 90° abd 70-‐90° Internal rotation arm at 90° abd 70-‐90° (J Shoulder Elbow Surg 2006;15:306-‐310.)
When evaluating internal ROM “reach your hand up your back” movement above what spinal level is not associated with shoulder joint movement? What is the commonest cause of failure to reach above T 12?
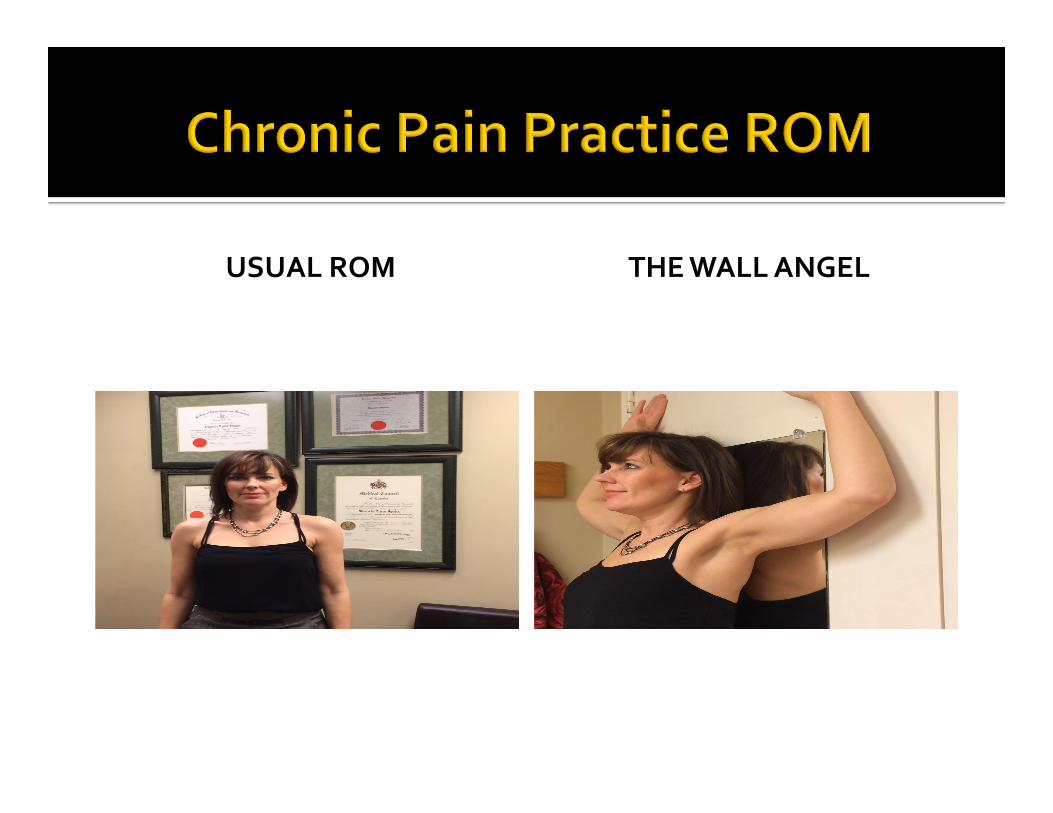
USUAL ROM THE WALL ANGEL
¡ Test & compare both sides
¡ Be specific to muscle or muscle group if possible
¡ DO NOT Grade strength 0-‐5 unless ROM is normal

Posterior Deltoid…. Extend your arm behind you Thumb down Examiner pushes arm down while patient resists
48
Flexion Ant deltoid Pec major Coracobrachialis (deltoid trigger points,C5 or axillary n compression)
Extension Post deltoid Teres major Lat dorsi (deltoid trigger points,C5 or
axillary n compression)
Gopura RARC et. al A Study on Human Upper-‐Limb Muscles Activities during Daily Upper-‐Limb Motions . I nternational Journal of Bioelectromagnetism www.ijbem.org Vol. 12, No. 2, pp. 54 -‐ 61, 2010
49
External rotation Infraspinatus Posterior deltoid Teres minor (infraspinatus trigger point or
tear, rotator cuff tear, common finding in “impingement” & suprascapular neuropathy)
Internal rotation Subscapularis Lat dorsi Teres major Ant deltoid (subscapularis trigger point or
tear) Gopura RARC et. al A Study on Human Upper-‐Limb Muscles Activities during Daily Upper-‐Limb Motions . International Journal of Bioelectromagnetism www.ijbem.org Vol. 12, No. 2, pp. 54 -‐ 61, 2010
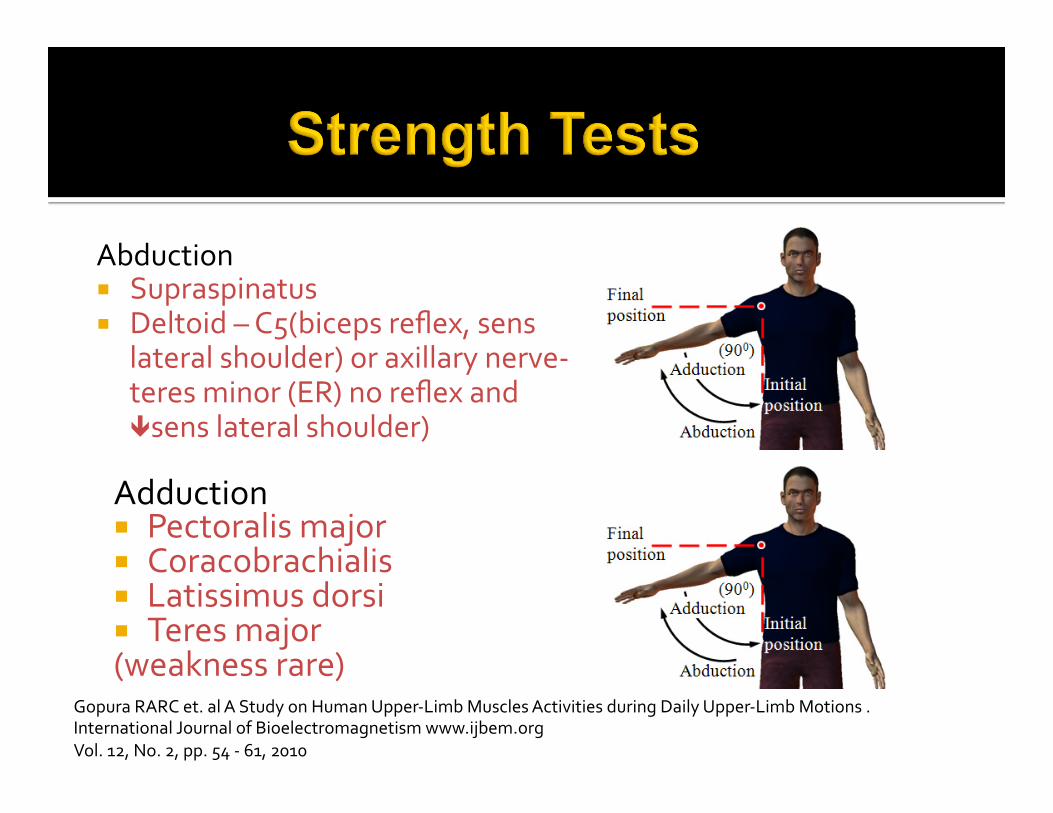
Abduction ¡ Supraspinatus ¡ Deltoid – C5(biceps reflex, sens
lateral shoulder) or axillary nerve-‐ teres minor (ER) no reflex and êsens lateral shoulder)
Adduction ¡ Pectoralis major ¡ Coracobrachialis ¡ Latissimus dorsi ¡ Teres major (weakness rare)
Gopura RARC et. al A Study on Human Upper-‐Limb Muscles Activities during Daily Upper-‐Limb Motions . International Journal of Bioelectromagnetism www.ijbem.org Vol. 12, No. 2, pp. 54 -‐ 61, 2010
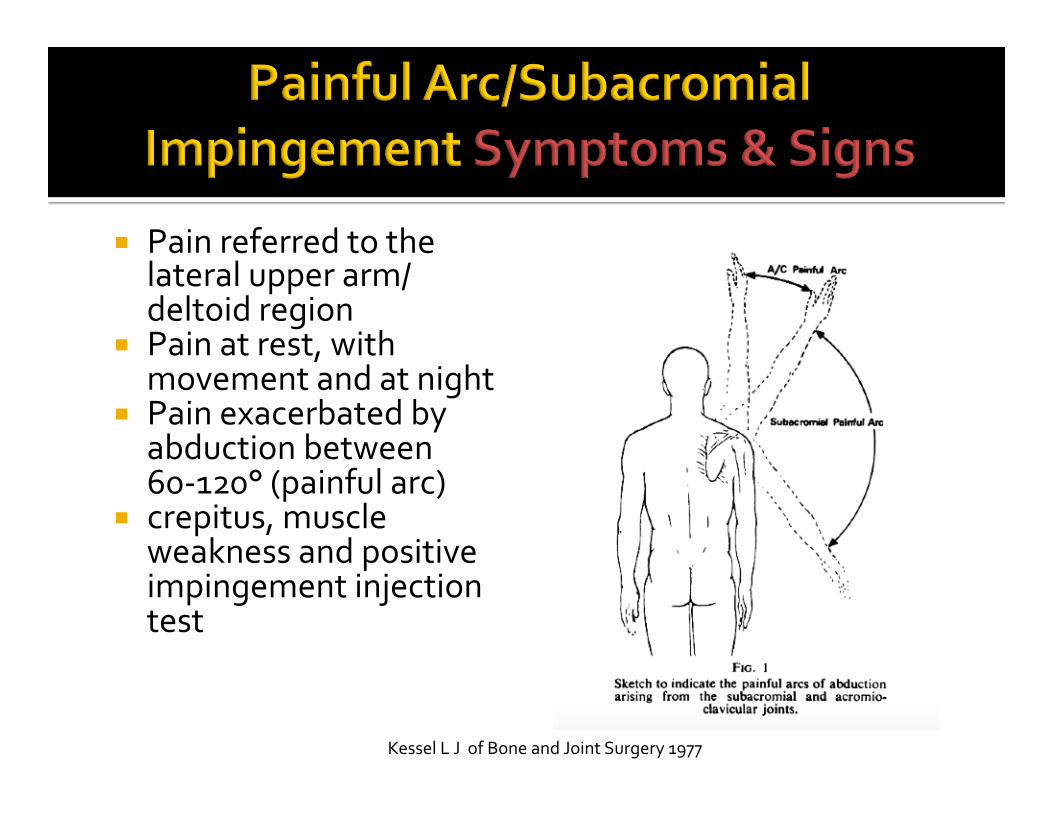
¡ Pain referred to the lateral upper arm/deltoid region
¡ Pain at rest, with movement and at night
¡ Pain exacerbated by abduction between 60-‐120° (painful arc)
¡ crepitus, muscle weakness and positive impingement injection test
Kessel L J of Bone and Joint Surgery 1977
Kessel L J of Bone and Joint Surgery 1977
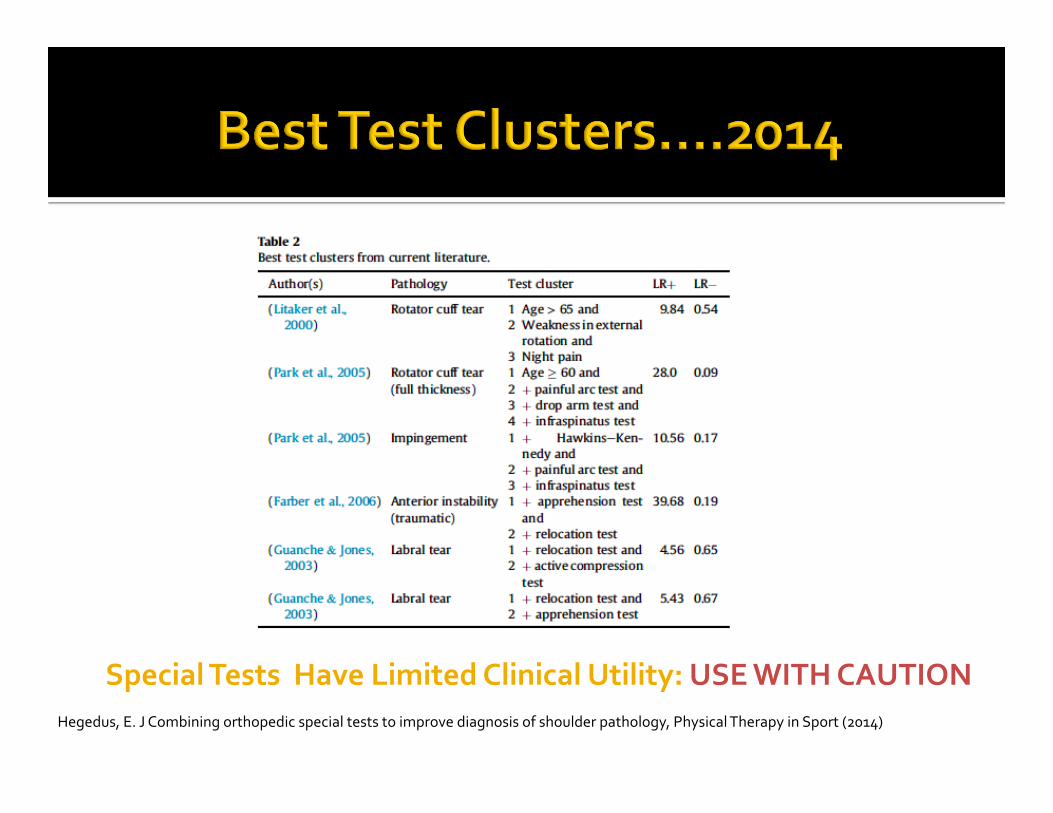
Hegedus, E. J Combining orthopedic special tests to improve diagnosis of shoulder pathology, Physical Therapy in Sport (2014)
Special Tests Have Limited Clinical Utility: USE WITH CAUTION
If all 3 of these test clusters § Painful Arc (60-120°) § Positive Hawkins-Kennedy test § Positive Infraspinatus test
¡ Sensitivity 75% -‐ for every 4 positive results, 3 are associated with
structural change and one will not have structural change if structural change is the gold standard
¡ Specificity 74% – for every 4 negative results, 3 will have no structural change but one will have structural change
¡ Overall accuracy 75% Hegedus Physical Therapy in Sport 2014

57
¡ Patient standing ¡ Examiner forward flexes
shoulder to 90° ¡ Elbow at 90° flexion ¡ Then forcibly internally
rotates the arm ¡ Positive test = pain in
area of superior GH joint or AC joint
Patient asked to : Hold arm at side Bend elbow to 90° Externally rotate to 45° Externally rotate against resistance Positive test is pain or weakness
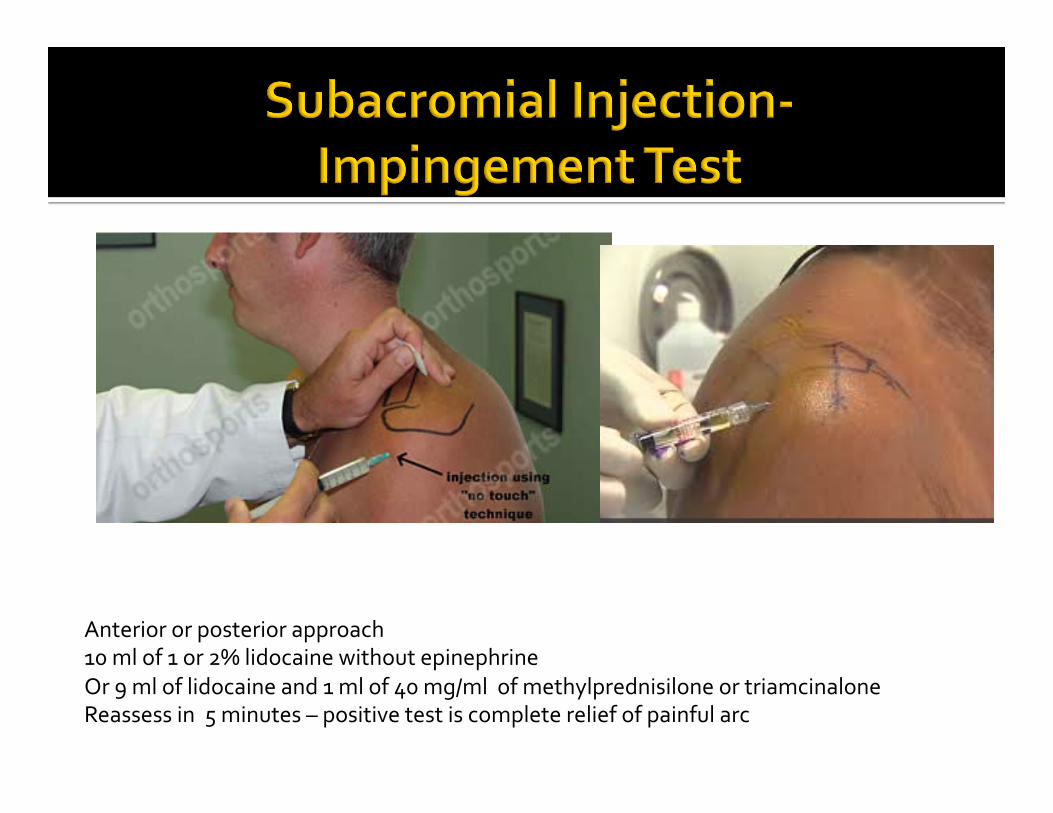
Anterior or posterior approach 10 ml of 1 or 2% lidocaine without epinephrine Or 9 ml of lidocaine and 1 ml of 40 mg/ml of methylprednisilone or triamcinalone Reassess in 5 minutes – positive test is complete relief of painful arc
“From the meta-‐analysis portion of this review, the Hawkins-‐Kennedy initially appears to be of value in ruling out subacromial impingement when negative. However, the LR− is poor and further, a strong argument can be made that subacromial impingement is not a valuable diagnosis but rather a cluster of diagnoses.”1
“It is not clear what the source of the pain is during positive clinical impingement testing. It is increasingly advocated that this diagnosis is no more specific than a diagnosis of anterior or posterior shoulder pain, and no more effective in directing treatment.”2
1.Hegedus E Br J Sports Med 2012;46:964–978. 2.Kibler WB Br J Sports Med 2013;47:877–885.

List as many of the 6 diagnostic criteria as you can 1.Slow onset of pain over the insertion of the deltoid 2.Inability to sleep on the affected side 3. Atrophy of the scapular muscles 4. Local tenderness 5. Loss of both passive and active ROM 6. MRArthrogram -‐ Thickening of the coracohumeral ligament (CHL) and joint capsule in the rotator cuff interval (RCI), as well as the subcoracoid triangle sign
¡ Usually loss of both active and passive ¡ Look for loss of glenohumeral movements “ Capsular Pattern” (irritated joint or capsule due to trauma, disease, inflammation, degeneration) ER>ABD > IR
Two New Tests 1. The Shrug Sign 2.The Coracoid Test
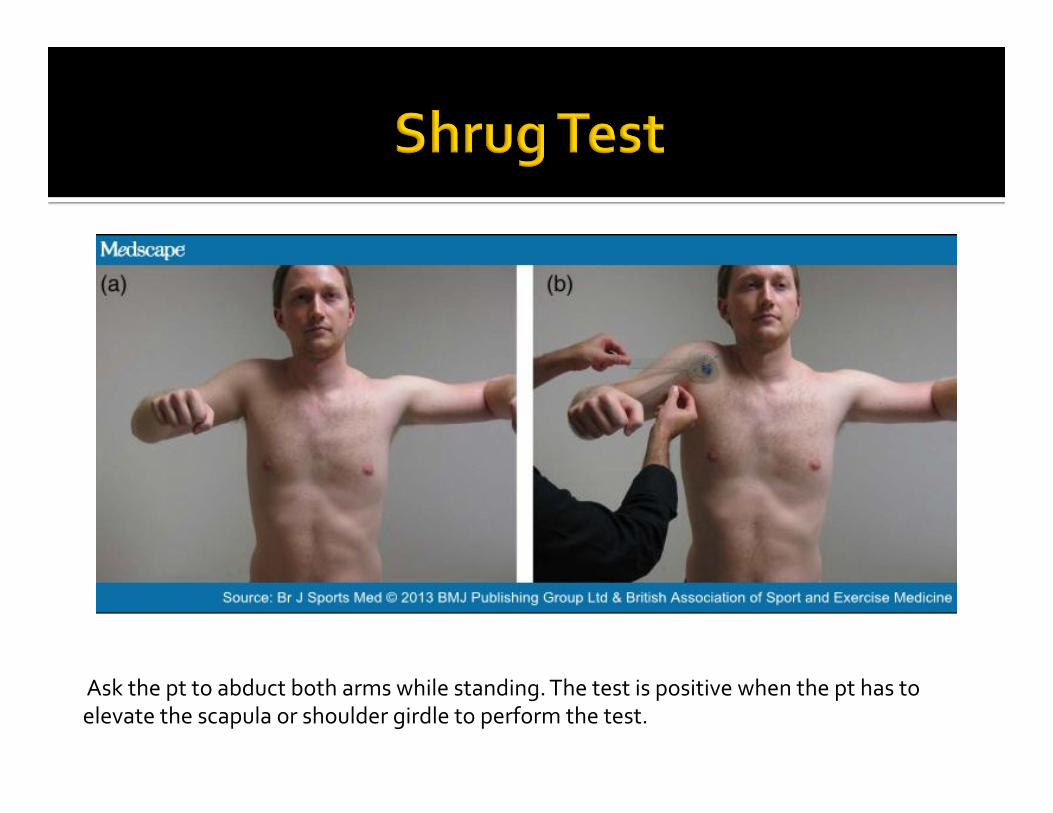
Ask the pt to abduct both arms while standing. The test is positive when the pt has to elevate the scapula or shoulder girdle to perform the test.
¡ “The shrug sign appears to be a sensitive test for stiffness-‐related disorders (osteoarthritis and adhesive capsulitis) as well as rotator cuff tendinopathy.” Hegedus 2012
¡ 830 patients enrolled ¡ The diagnosis of… ¡ Adhesive capsulitis was based on Codman’s criteria,shoulder stiffness and MRI findings
¡ Rotator cuff tears diagnosed based on clinical and MRI evaluation
¡ Calcifying tendonitis,glenohumeral arthritis and AC arthropathy were based on clinical and radiographic findings
Carbone S. International Orthopaedics (SICOT) (2010) 34:385–388
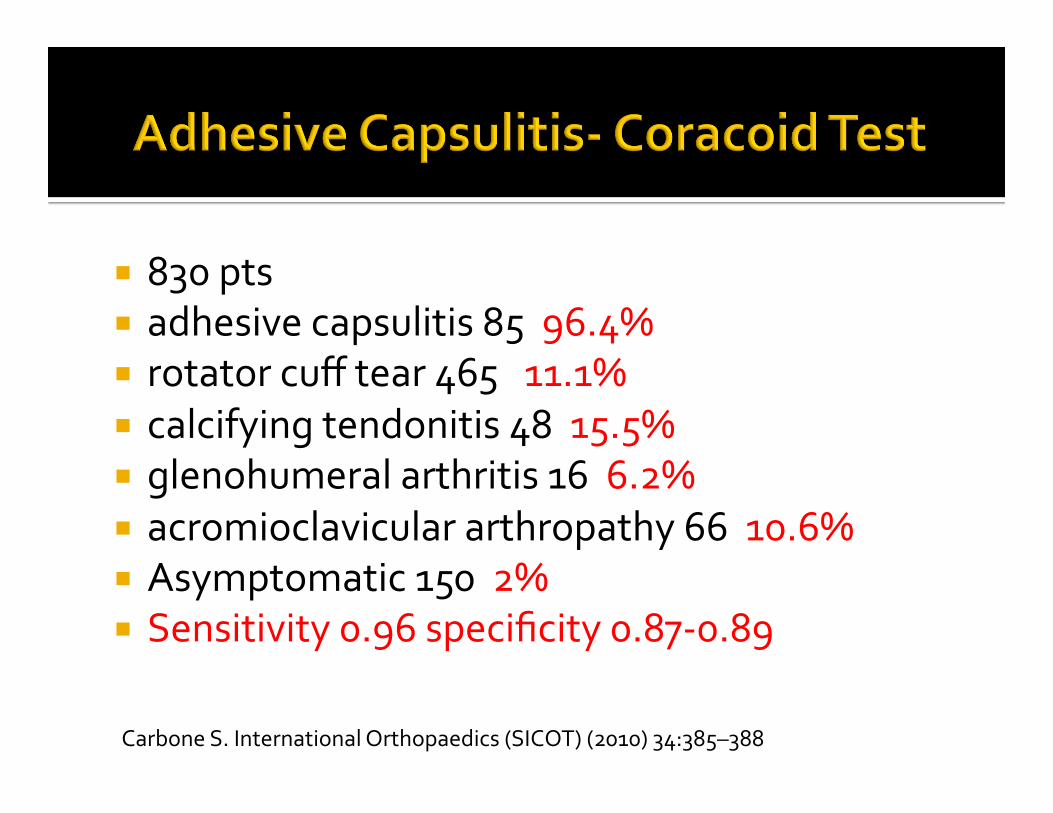
¡ 830 pts ¡ adhesive capsulitis 85 96.4% ¡ rotator cuff tear 465 11.1% ¡ calcifying tendonitis 48 15.5% ¡ glenohumeral arthritis 16 6.2% ¡ acromioclavicular arthropathy 66 10.6% ¡ Asymptomatic 150 2% ¡ Sensitivity 0.96 specificity 0.87-‐0.89 Carbone S. International Orthopaedics (SICOT) (2010) 34:385–388
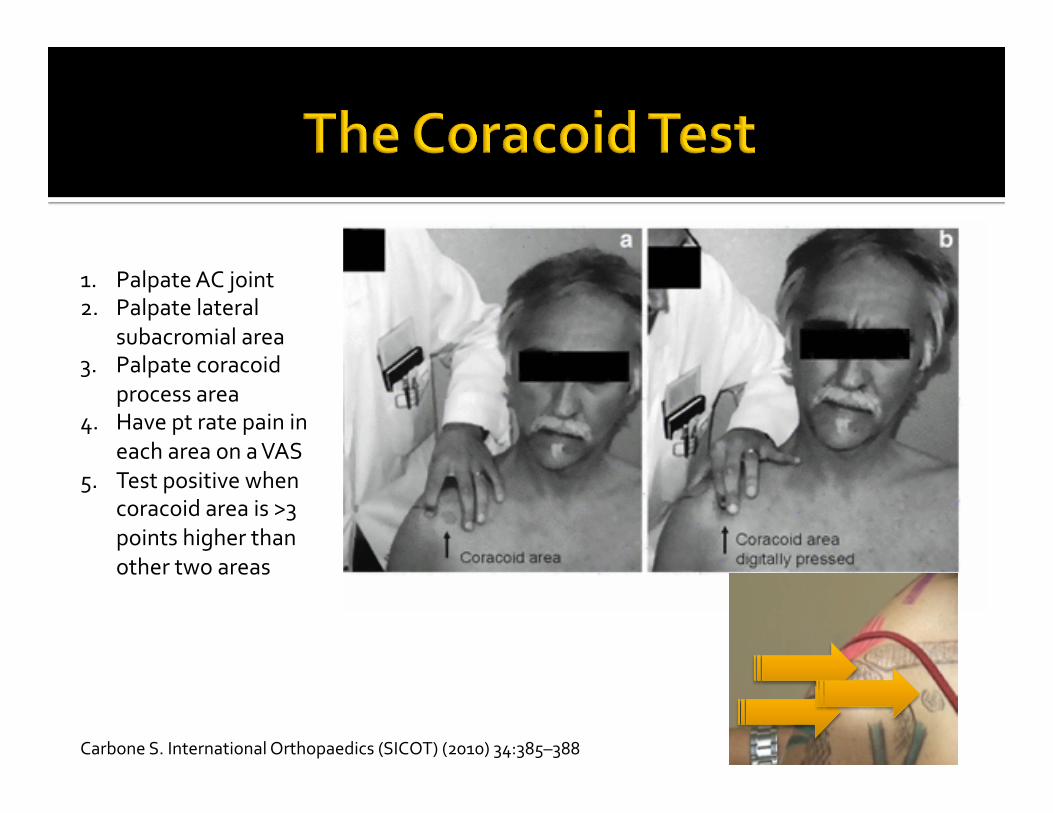
1. Palpate AC joint 2. Palpate lateral
subacromial area 3. Palpate coracoid
process area 4. Have pt rate pain in
each area on a VAS 5. Test positive when
coracoid area is >3 points higher than other two areas
Carbone S. International Orthopaedics (SICOT) (2010) 34:385–388
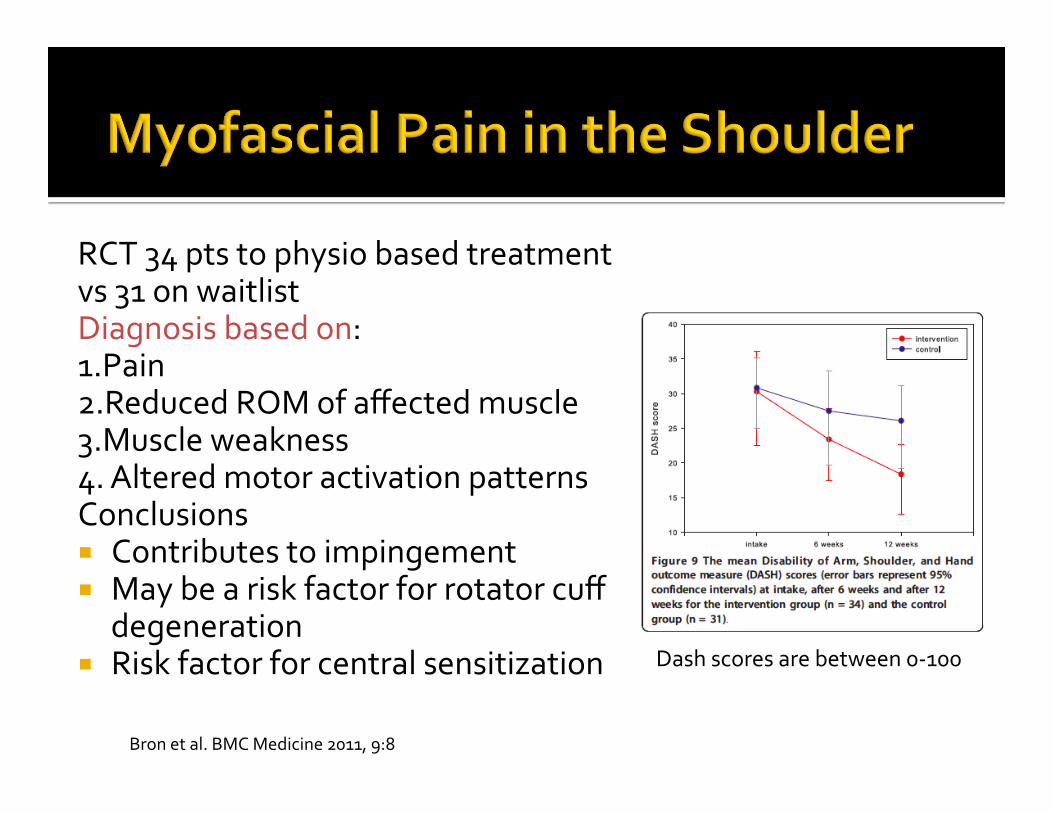
RCT 34 pts to physio based treatment vs 31 on waitlist Diagnosis based on: 1.Pain 2.Reduced ROM of affected muscle 3.Muscle weakness 4. Altered motor activation patterns Conclusions ¡ Contributes to impingement ¡ May be a risk factor for rotator cuff
degeneration ¡ Risk factor for central sensitization
Bron et al. BMC Medicine 2011, 9:8
Dash scores are between 0-‐100

ABD
FLEXION

INTERNAL ROTATION

• Unable to reach behind their back to fasten a bra or get their wallet out of a back pocket.
• Unable to raise their arm up to wash their hair, brush their teeth, or even to bring food to their mouth while eating (co-‐involvement of supraspinatus and posterior deltoid)
• Shoulder pain and weakness when using their arms to push up out of a chair or when pushing up out of bed in the morning
• Night pain
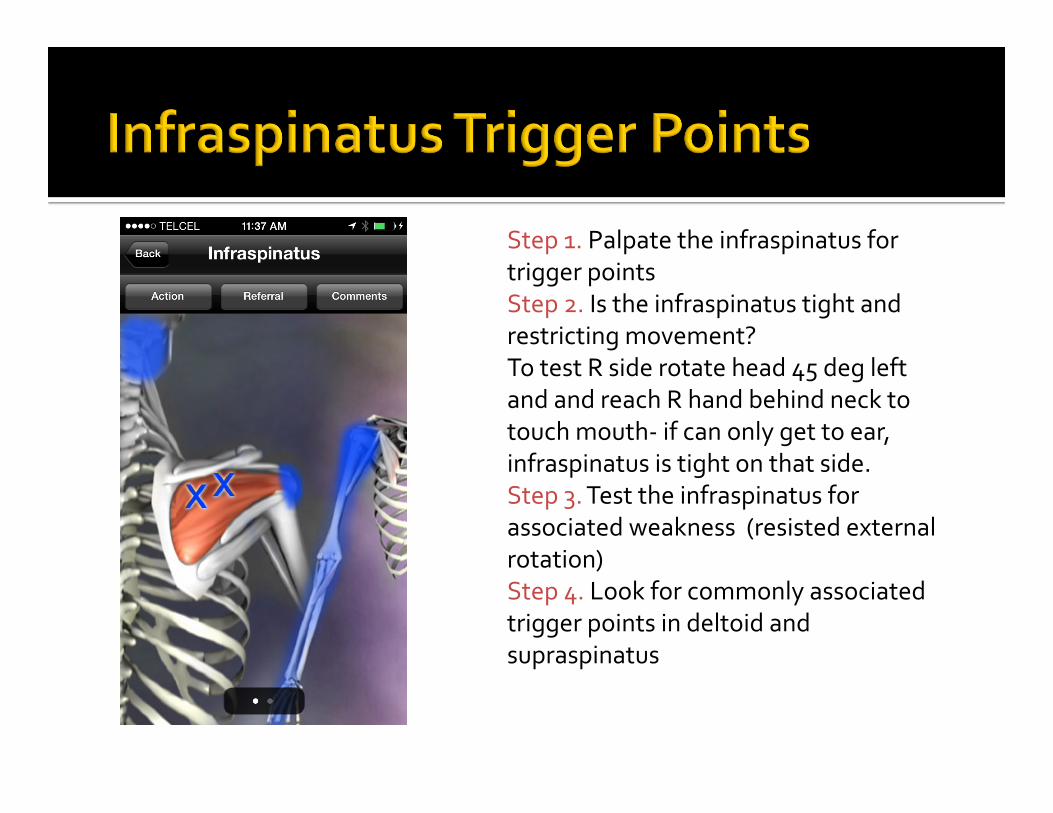
Step 1. Palpate the infraspinatus for trigger points Step 2. Is the infraspinatus tight and restricting movement? To test R side rotate head 45 deg left and and reach R hand behind neck to touch mouth-‐ if can only get to ear, infraspinatus is tight on that side. Step 3. Test the infraspinatus for associated weakness (resisted external rotation) Step 4. Look for commonly associated trigger points in deltoid and supraspinatus
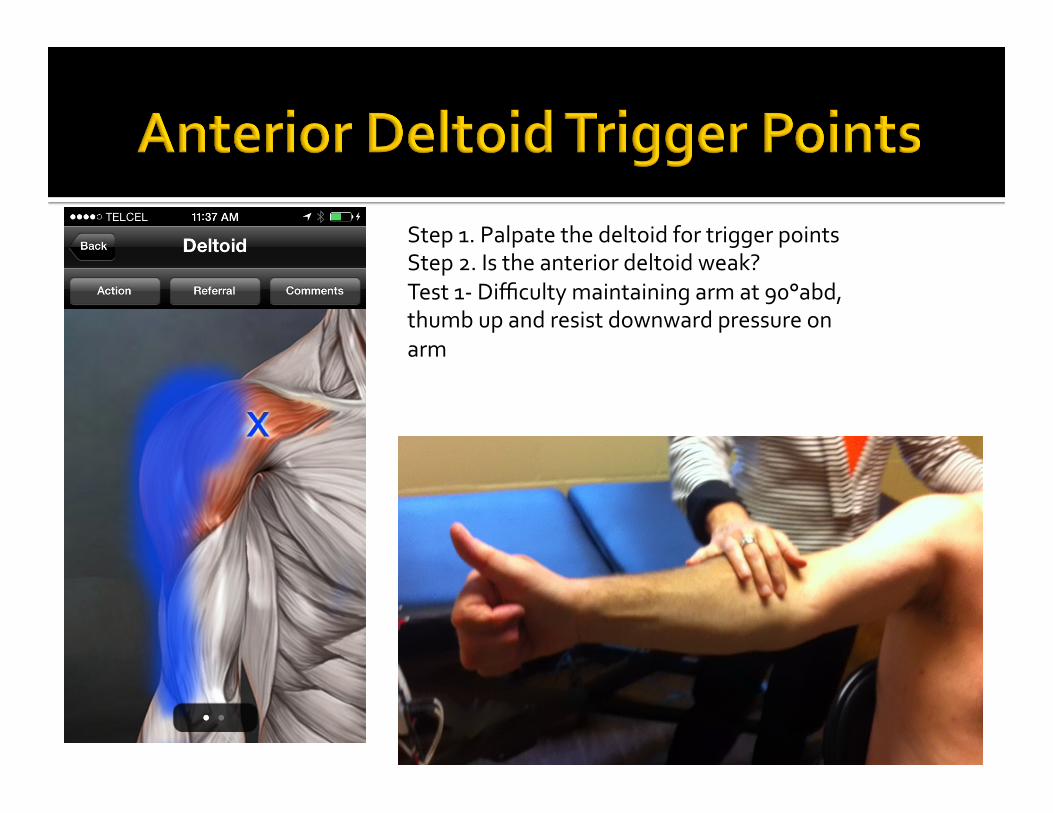
Step 1. Palpate the deltoid for trigger points Step 2. Is the anterior deltoid weak? Test 1-‐ Difficulty maintaining arm at 90°abd, thumb up and resist downward pressure on arm
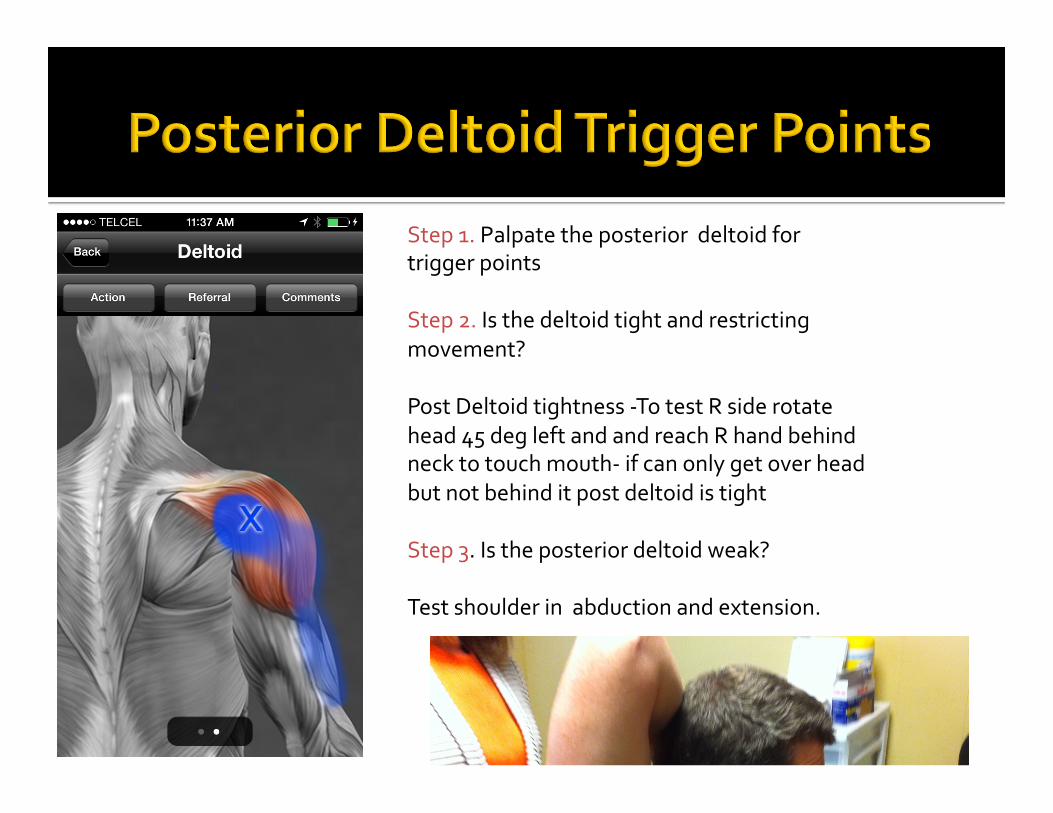
Step 1. Palpate the posterior deltoid for trigger points Step 2. Is the deltoid tight and restricting movement? Post Deltoid tightness -‐To test R side rotate head 45 deg left and and reach R hand behind neck to touch mouth-‐ if can only get over head but not behind it post deltoid is tight Step 3. Is the posterior deltoid weak? Test shoulder in abduction and extension.
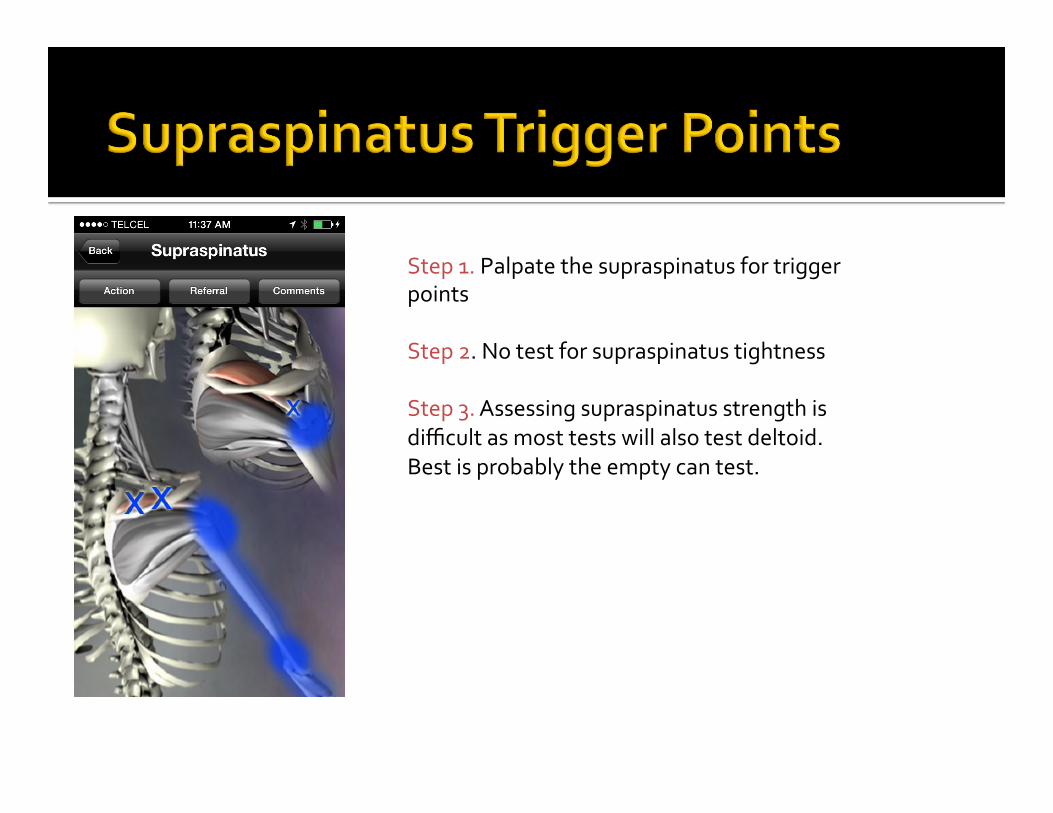
Step 1. Palpate the supraspinatus for trigger points Step 2. No test for supraspinatus tightness Step 3. Assessing supraspinatus strength is difficult as most tests will also test deltoid. Best is probably the empty can test.


PRE-‐TREATMENT STRENGTH POST-‐ TREATMENT STRENGTH
¡ Determining the cause of shoulder pain is complex
¡ Often, there are multiple contributing causes ¡ Use test combinations to increase diagnostic sensitivity and specificity of your exam findings
¡ Myofascial pain is more common than we were taught