c ase s tudy 1 micr 410 - h ematology s pring, 2011 hiba allo christina castro claire endo adrian...
TRANSCRIPT

CASE STUDY 1MICR 410 - HEMATOLOGYSPRING, 2011
HIBA ALLO
CHRISTINA CASTRO
CLAIRE ENDO
ADRIAN VALONES
CASE SUMMARY
John, a 4 year old boy, complains of weakness, fatigue, and dyspnea (labored breathing).
Parents encounter bouts of fatigue, but have never consulted a physician.
Parents are from Greece. Significance: Greeks have a genetic
predilection for certain diseaseshttp://www.inmagine.com/unx202/u14837207-photo

KEY INFORMATION POINTING TO DIAGNOSIS Patient presents with anemia. Weakness, fatigue, and dyspnea are symptoms
of anemia.
CBC Low RBC, Hemoglobin, and HCT Anemia Hypochromic, Microcytic
Peripheral Blood Smear Poikilocytosis, Polychromasia and Target Cells (dominant)
NOTE: Target Cells are also found in Hemoglobinopathies, Iron Deficiency Anemia, & Thalassemia
http://www.med.cmu.ac.th/dept/pediatrics/06-interest-cases/ic-52/case52-page-1.HTM

KEY INFORMATION POINTING TO DIAGNOSIS
Additional lab test confirming the diagnosis:Hemoglobin Electrophoresis & Iron Panel
Hemoglobin Electrophoresis Results Abnormal HbA levels are low 8% Hb Bart’s and 24% Hb H are abnormally present
Iron Studies are normal α-Thalassemia is commonly found in
Mediterranian people (Greeks and Sardinians)
THE DIAGNOSIS FOR CASE 1 R/O Iron Deficiency Anemia
Iron panel normal R/O Hemoglobinopathies & β-Thalassemia
Alpha chains decreased: low Hgb A 66% (95-98%)
β and ϒ chains in excess: Hgb H 24%, Hgb Bart’s 8%
Hgb S, SC, C: No sickle cells or crystals present
Diagnosis: Hemoglobin H Disease (Alpha Thalassemia)
PATHOPHYSIOLOGY OF HB H DISEASE
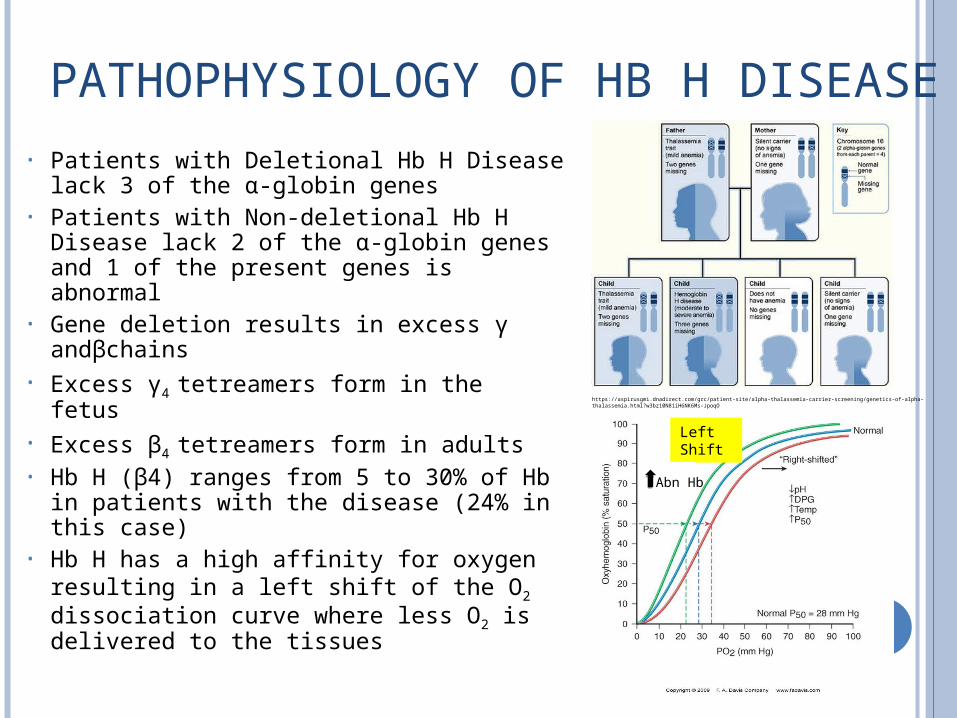
• Patients with Deletional Hb H Disease lack 3 of the α-globin genes
• Patients with Non-deletional Hb H Disease lack 2 of the α-globin genes and 1 of the present genes is abnormal
• Gene deletion results in excess γ andβchains
• Excess γ4 tetreamers form in the fetus• Excess β4 tetreamers form in adults• Hb H (β4) ranges from 5 to 30% of Hb
in patients with the disease (24% in this case)
• Hb H has a high affinity for oxygen resulting in a left shift of the O2 dissociation curve where less O2 is delivered to the tissues
https://aspirusgmi.dnadirect.com/grc/patient-site/alpha-thalassemia-carrier-screening/genetics-of-alpha-thalassemia.html?w3bz10N81iH6NK6Ms-JpoqO
Left Shift
Abn Hb

PATHOPHYSIOLOGY OF HB H DISEASE
• Hb H forms an intracellular precipitate
• As RBCs age they contain more precipitated Hb H due to attachment to the cell membrane
• Precipitates make Hb H RBCs more rigid leading to culling in the spleen – Hb H Disease is mainly a
hemolytic disorder• Precipitates may also cause
ineffective erythropoiesis
http://emedicine.medscape.com/article/958850-overview
http://bloodjournal.hematologylibrary.org/content/105/2.cover-expansion
DIAGNOSTIC TESTS FOR HB H DISEASE
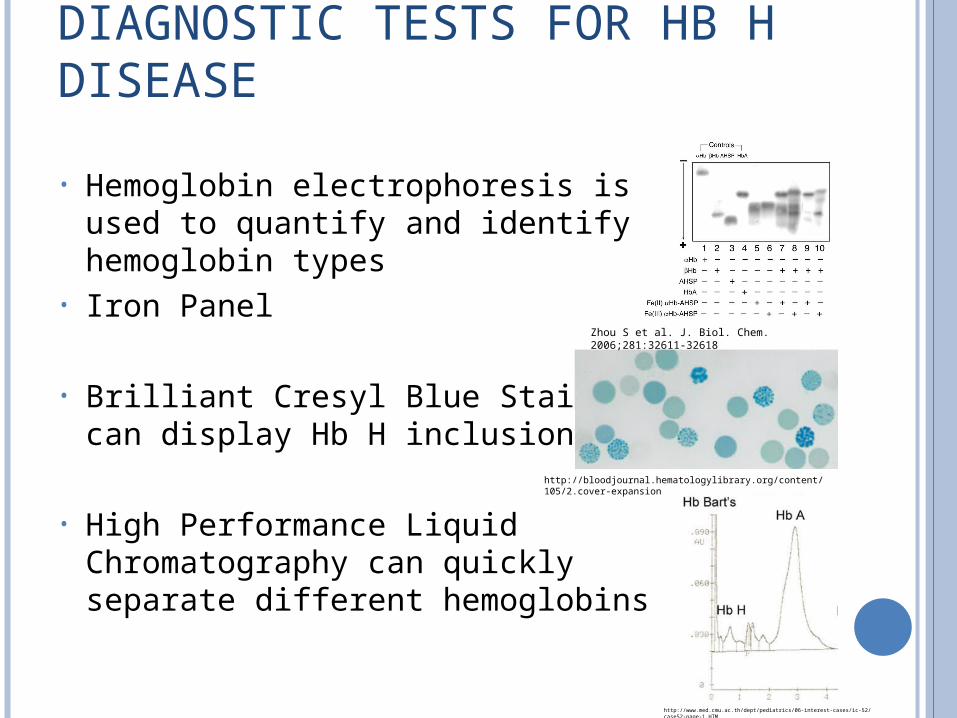
• Hemoglobin electrophoresis is used to quantify and identify hemoglobin types
• Iron Panel
• Brilliant Cresyl Blue Stain can display Hb H inclusions
• High Performance Liquid Chromatography can quickly separate different hemoglobins
http://bloodjournal.hematologylibrary.org/content/105/2.cover-expansion
Zhou S et al. J. Biol. Chem. 2006;281:32611-32618
http://www.med.cmu.ac.th/dept/pediatrics/06-interest-cases/ic-52/case52-page-1.HTM
THERAPY AND PROGNOSIS FOR HB H DISEASE
Therapy For severe anemia: blood transfusions
Monitor for Hemochromatosis Splenectomy Hematopoietic Stem Cell Transplantation
Requires bone marrow transplant Only used in severe cases
Avoid certain medications sulfa drugs, analgesics Avoid mothballs and fava beans: causes severe
anemia Prognosis
Proper care reduces medical complications Good prognosis with treatment Nondeletional Hb H Disease has more severe
complications than Deletional Hb H Disease
PREVENTION OF HB H DISEASE
Family history – genetic counseling Likelihood of Hgb Bart’s (Hydrops Fetalis)
Prenatal Testing Amniocentesis & Chorionic Villus Sampling Ultrasound Monitoring of Hydrophobic Changes
Preimplantation Genetic Diagnosis (PGD) Embryos grown in vitro Increase chance of a healthy child
TAKE HOME MESSAGE The diagnosis is Hemoglobin H (alpha thalassemia) Typical symptoms
Fatigue, weakness & dyspnea The cause of the disease
3 Alpha chain gene deletions Diagnostic tests
CBC, Iron Panel & Hemoglobin electrophoresis Treatment
Intermittent blood transfusions for severe anemia Splenectomy then bone marrow transplant in severe cases Dietary restriction & avoiding certain medications
Prognosis Prognosis is good with proper medical care
Prevention is genetic counseling with family history, prenatal testing & PGD
REFERENCES Cheerva, A.C. and Coppes, M.J. (2011). Hemoglobin H Disease
(Alpha Thalassemia). Retrieved from http://emedicine.medscape.com/article/955496-overview
Chui, D. H. K. et al. (2003). Hemoglobin H Disease: not necessarily a benign disorder. Blood, 101(3), 791-800.
Harmening, D. (2008). Clinical Hematology and Fundamentals of Hemostasis. (5th ed.). Baltimore, MD: F.A. Davis
Company. Knapp, A. et al. (2010). Evidence Review: Hemoglobin H
Disease.Retrieved from http://www.hrsa.gov/heritabledisorderscommittee/
reports/hemogolbinh.pdf London Fertility Centre. Information Sheet for Thalassemias and
Preimplantation Genetic Diagnosis. Retrieved from http://www.fertilityplus.org.uk/data/documents/PGD-THALINFOSHEET74%20V4%2007%2010%2010.pdf