by rebecca banzhof 1,, carrie burns 2, zuolu liu 3, sarah ratcliffe, 4 teresa scattergood 2, nalaka...
TRANSCRIPT

by Rebecca Banzhof1,, Carrie Burns2, Zuolu
Liu3, Sarah Ratcliffe,4 Teresa Scattergood2, Nalaka S. Gooneratne1,3 Anne Cappolla2

IntroductionFrailty refers to a clinical syndrome
characterized by decreased physiologic reserves across multiple systems resulting in an increased risk of mortality.(1-7)
The importance of early diagnosis, assessment and intervention to differentiate between disability and frailty is critical in determining appropriate treatment.(1)

Introduction Our specific study aim was to assess the
potential role of wrist activity monitors in identifying the presence of frailty syndrome.
We hypothesized that frail participants would have reduced activity counts relative to non-frail study participants.
Our study examined a group of ten older women whose frailty status had been carefully defined using the Cardiovascular Health Study Frailty criteria.(1)

Study Methods Participants in this trial were assessed for
the presence or absence of frailty syndrome . Participants were randomly assigned to
receive ghrelin or placebo as the first infusion. They were given the wrist-activity monitor after their first infusion and returned the device before their second infusion.
They were treated with intravenous ghrelin in a cross-over design to determine if ghrelin would increase oral intake.

Study Methods
Subjects were community-dwelling, ambulatory females recruited from geriatric and internal medicine clinics at the University of Pennsylvania Health System. Research study participants were given wrist activity monitors which they wore starting at 12:00 noon on day 1.

Study MethodsThey wore these units for a seven day period
until 10:00 AM on the non-dominant wrist. Concurrently, they completed a sleep diary on which they recorded their time in bed, time they fell asleep, time they woke up and got out of bed.

Actiwatch

Results The Average Activity Count method and the
Fixed Daytime Average Activity Count showed significant differences between frail and non-frail study participants (p=0.008).
All five frail subjects had Average Activity Counts less than or equal to 97, while all five non-frail study participants had Average Activity Counts greater than 97.

ResultsWhen examining night-only data, either
derived using a fixed day-night criteria or a variable criteria based on the sleep diary, there was no statistically significant difference between frail and non-frail groups.
The prevalence of rest and active epochs differed between frail and non-frail study participants, with frail participants having a higher percentage of rest periods.
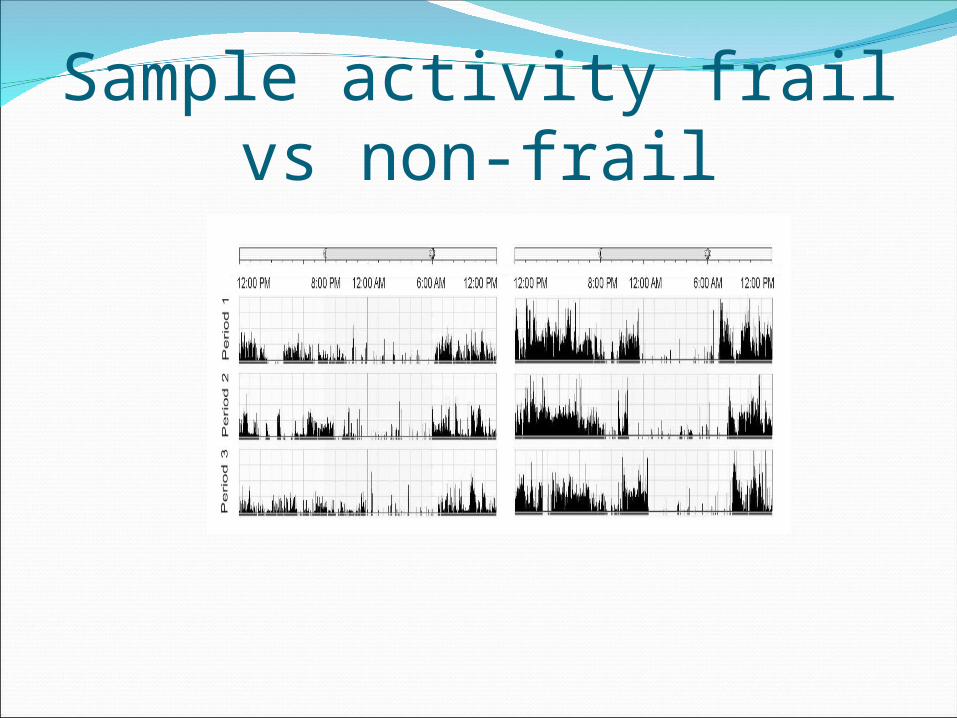
Sample activity frail vs non-frail

Discussion We observed a relationship between wrist
activity and frailty status, with frail patients having average activity counts less than 97.
This may occur because the pathophysiologic process underlying frailty is often linked to reductions in muscle mass (1).
This may translate into reduced overall activity levels from weakness and deconditioning.(1)

DiscussionAnother factor that could contribute to the
reduced activity level in frail adults is that they may have higher amounts of sleep or rest periods due to drowsiness.
There are several potential benefits of using wrist-activity monitors as a tool to identify the frailty syndrome.

DiscussionFirst, it does not depend on self-report and
does not require completion of questionnaires that may be difficult in patients with limited literacy skills.
Second, the wrist-activity monitor is simple for subjects to wear and involves a lower subject assessment burden relative to other measures.

Discussion In conclusion, the results of this study
suggests that wrist-activity monitors may be a useful tool for the identification of the frailty syndrome. Their ease of use and minimal patient burden may be of use in both clinical and research settings.
Thank You

References [1] Fried LP, Ferrucci L, Darer J, Williamson JD,
Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59: 255-263.
[2] Pel-Littel RE, Schuurmans MJ, Emmelot-Vonk MH, Verhaar HJ. Frailty: defining and measuring of a concept. J Nutr Health Aging. 2009;13: 390-394.
[3] Ferrucci L, Guralnik JM, Studenski S, Fried LP, Cutler GB, Jr., Walston JD. Designing randomized, controlled trials aimed at preventing or delaying functional decline and disability in frail, older persons: a consensus report. J Am Geriatr Soc. 2004;52: 625-634.
[4] Kanapuru B, Ershler WB. Inflammation, coagulation, and the pathway to frailty. Am J Med. 2009;122: 605-613.

References [5] Sarkisian CA, Gruenewald TL, John Boscardin W, Seeman TE.
Preliminary evidence for subdimensions of geriatric frailty: the MacArthur study of successful aging. J Am Geriatr Soc. 2008;56: 2292-2297.
[6] Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. Cmaj. 2005;173: 489-495.
[7] Graham JE, Snih SA, Berges IM, Ray LA, Markides KS, Ottenbacher KJ. Frailty and 10-year mortality in community-living Mexican American older adults. Gerontology. 2009;55: 644-651.
[8] Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56: M146-156.
[9] Hubbard RE, O'Mahony MS, Woodhouse KW. Characterising frailty in the clinical setting--a comparison of different approaches. Age Ageing. 2009;38: 115-119.
[10] Jones D, Song X, Mitnitski A, Rockwood K. Evaluation of a frailty index based on a comprehensive geriatric assessment in a population based study of elderly Canadians. Aging Clin Exp Res. 2005;17: 465-471.