by elliot feinberg, d.d.s.* edward m. feinberg, …€¦ · · 2015-07-30prefabricated...
TRANSCRIPT

by ELLIOT FEINBERG, D.D.S.*EDWARD M. FEINBERG, D.M.D.*
Stud attachments: This attachment is composedof a projection soldered to a post-type crown and acorresponding female receptacle that is embedded inan overlay type of denture prosthesis.
Bar attachments: This type of attachment consistsof a bar spanning an endentulous area that splints theexisting teeth together. The bar is then used to supporta denture prosthesis that houses matching, prefabri-cated sleeves.
The intracoronal type of attachment is probablythe most widely used attachment. For more than 30years, we have used intracoronal attachments, in par-ticular the APM Sterngold #7 precision attachment.They have functioned with great success. In our ex-perience, the average case has lasted from 15 to 20years, with many cases still functioning after 30 years..(Figures la, lb and lc). To obtain such results, how-ever, it is essential that exacting and precise techniquesas well as strict adherence to basic engineering andmechanical principles are followed at all times. Thefollowing fundamentals which are based on experiencefrom 1,500 clinical cases are required for maintainableperiodontal health and abutment longevity.
Removable partial dentures fabricated with precisionattachments for retention and support are the bestprosthesis available to dentistry where fixed restora-tions are contraindicated. Precision attachments areprefabricated attachments consisting of two matchedmetal components, male and female. They are usuallymade of precious metal and are machined to a closetolerance. They are used in le movable partial denturesto join the removable prosthesis to a fixed restoration.
The proper application of internal attachments hasthe following advantages over clasp-type removablepartial dentures:I. Cosmetics: Unlike the clasp~type partial denture,
there is no visible evidence of labial or buccal metalretainers.
2. Periodontal health: The precision attachment is lessstressful to the abutment teeth than clasp-typeattachments. There are decreased lateral vectors offorce since most of the forces are directed along thelong axis of the tooth and can be more easily resistedby the fibers of the periodontal ligament. This typeof directed stress places less leverage on the abut-ment teeth and thus provides abetter environmentfor maintainable periodontal health.
Prefabricated AttachmentsThere are many different types of prefabricated
attachments available. They are usually classified onthe basis of shape and form.
lntracoronal attachments: These attachmentsconsist of two parts a slot (female) and a flange (male).The flange is connected to the removable prosthesisand fits into the slot which is embedded in a fixedrestoration. This attachment was designed by HermanChilyes in 1906 and with only slight modifications, isstill in use.
Extracoronal attachments: These attachmentshave most of their mechanism outside of the diameterof the abutment restoration. In most types, a projectingreceptacle is soldered to the crown, and a correspond-ing fitting or housing is incorporated in the removableprosthesis. With this type of attachment, there is usu-ally a certain amount of movement between the twosections of the prosthesis .
Fundamental Criteria for AttachmentsI. Preparation of abutment teeth: The prepara-
tion of choice is a fuII~shouldered preparation with aneven, circumferential width of shoulder on the corres-ponding casting. Since most of the stress from thefunctioning attachment case is transmitted in a verticaldirection, the even shoulder helps to equally distributethe load to the supporting structures with little lateralstress inflicted on the abutment. The shoulder shouldalso be related as close to the bone as possible toprevent undue torquing of the abutment teeth. Thisapproach to the preparation of abutment teeth con-forms to accepted engineering principles of design andconstruction.
2. Splinting of abutments: In every case, at leasttwo attachments should be placed in crowfiS that aresplinted to other teeth in order to aid in distributing theforces. Auxiliary attachments may then be used onavailable single teeth to provide additional support andretention. The only exception is the placement of at-tachments in long canines that have good bone sup-port. For patients who have lost most of their posteriorteeth, cross arch splinting of the remaining anteriorteeth, that includes the two strategic attachments, isthe method of choice .
Dr. Elliot Feinberg is clinician associate professor at TempleUniversity School of Dentistry.' Dr. Edward M. Feinberg is inprivate practice is Scarsdale.
MARCH 1984 161

3. Attachments: The manufacturer fabricates themale 7mm in length. This is the ideal length, but it is notalways possible to create this much space without in-terfering with the occlusion. The average crown canusually accept between five and seven millimeters ofrn:aleattachment if the teeth and the periodontium havebeen prepared properly. Any attachment under 4mm inlength will function more as a rest than as an attach-ment and should not be used as one of the two essentialstrategic functioning attachments.
A full,.shoulder preparatiQn is the recommendedmethod of tooth preparation. Due to the flat undersur-face of the housing, a shoulder allows the female to beplaced in a more gingival direction. Thjs relationship ofthe female to the abutment will result in the placementof the maximum length of usable male, which in mostcases is a clitical factor. The abutment teeth should beprepared normally, with no additional emphasis ondeepening the axial wall for the acceptance of thefemale. The female housing will not be completelywithin the confines of most normally contoured abut-ments (unless endodontic therapy was instituted) butwill force the restoration to have a slightly largerdiameter. Since most components of force are appliedvertically by the functioning attachment, this slightoverextension appears to have no clinical significance,
in the health of the supporting structures. If this over-extension is a critical factor in the esthetics of the case,the fIrst pontic tooth on the prosthesis may be extendedlabially to overlap the excess metal and hide the truediameter of the abutment tooth. For this reason, pro-cessed acrylic teeth adjacent.to the abutments are usedto relate the shape and form of the pontics estheticallywith the fixed restorations.
4. Retention mechanism: Every type of remova-ble partial denture has to handle the problem of pre-venting gravitational and muscular forces from dislodg-ing the partial denture during function. This is espe-cially true for the average distal extension partial den-ture. To resist these forces, many different mechanicalaids have' been developed, including all varieties ofclasps, rests, springs, flanges, snaps, latches, plungersand retentive arms. Despite the differences in designand application, almost all of these retentionmechanisms are used to grip the abutment teeth withenough rigidity to prevent a force from dislodging theprothesis.
Unfortunately, while being retentive, thesemechanisms inflict lateral stresses on the abutmentteeth through their torquing action. These additionallateral stresses may eventually harm the periodontalsupport of the abutment teeth and limit the longevity oftheresotration. An ideal retainer should be passive andplace minimal stress on the abutment teeth. The use ofa double-tilt for the path of insertion of the parallelprecision attachment is an alternative method ofmechanical retention that eliminates the torquingstresses that most abutments are forced to absorb fromconventional mechanical retention mechanisms.
Traditiorially, intracoronal attachments have beensurveyed so that they are approximately perpendicularto the occlusal plane. This method requires a strongadditional retention mechanism to resist dislodgingforces. Double-ti1t retention, however, uses an uncon-ventional path of insertion to retain the prosthesis. Ananterior-posterior tilt as well as a mesio-distal tilt isused in the surveying procedure to place the attach-ments.'The resulting path of removal does not coincidewith the path that any oral movement or gravitationalforce will produce to dislodge the partial. It is, there-fore, unlikely that any normal function of the muscula-ture and tongue will have any affect.Figure la~Patient displaying lower precision attachment partial with
remaining teeth splinted after 21 years..
figure lc-1983 radiographs after 21 years oftunction. Note bonelevel, especially on left lateral.
162 NYS DENTAL JOURNAL
Establishing the Doub.le- Tilt Path of InsertionAfter waxing the abutments, the dentist or techni-
cian simply mounts the model on the parallelometerwith the occlusal table approximately parallel to thefloor and the anterior teeth facing forward. The heel ofthe model is raised approximately 10 degress to pro-vide an anterior-posterior tilt. The left-or right-handside of the model is then raised approximately 10 de-grees to provide a mesio-distal tilt. This double-tilting of.the model results in the correct line of insertion for theprosthesis, whether it be an upper or lower prosthesis.The parallelometer is now locked, and the attachments
are placed into the restorations (Figure 2).The double-tilt technique for retention was refined
by I. Franklin Miller and has been used for more than50 years. Traditionally, males have been fabricatedwith a slit so that retentive adjustment can be ac-complished by spreading the wings of the male. Whenoveradjusted these wings can weaken and presentbreakage problems. The double-tilt technique, how-ever, eliminates the need for adjustment because only aprecision fit of the attachment as well as a close fit ofthe partial base to the tissue are required for proper fit.Since no adjustments are necessary, a solid male is farsuperior toa male with a slit.** It can be machined to acloser fit and has far less tendency to wear and requirereplacement {Figure 3}.
The double-tilt prosthesis is designed to fit lightlyand is not rigidly held in place. During functionalmovements, if one side of the prosthesis is overloaded,the males may rise a fraction of a millimeter. Theprosthesis cannot be dislodged because the direction ofthe forces applied do not coincide with the path ofinsertion. It will then gently slide back into place. Thisbarely visible movement breaks the stress applied tothe abutment teeth and gently massages the soft tissueat the same time. Clinical experience suggests that thishighly restricted movement in a vertical directionphysiologically preserves the alveolar crests, produc-ing firm and healthy soft tissue as well as maintainingthe stability of the abutment teeth.
M aintenance : The continued periodontal accep-tance for case longevity requires an exacting mainte-nance program. All of the patients are recalled everyfour months for complete prophylaxis therapy and clin-ical evaluation. Physiological changes in oral anatomyare normal and occur at different rates for each indi-vidual. Periodically, therefore, the prosthesis will re-quire alteration in occlusion as well as rebasing fortissue readaptation. A close fit of the partial to the softtissue is essential for proper functioning of the double-tilt prosthesis. A slight rock of the appliance uponpressure or a feeling of looseness of the case con-sequently indicates that a relining procedure is neces-sary. (Figure 4). There is minimal wear in a properly
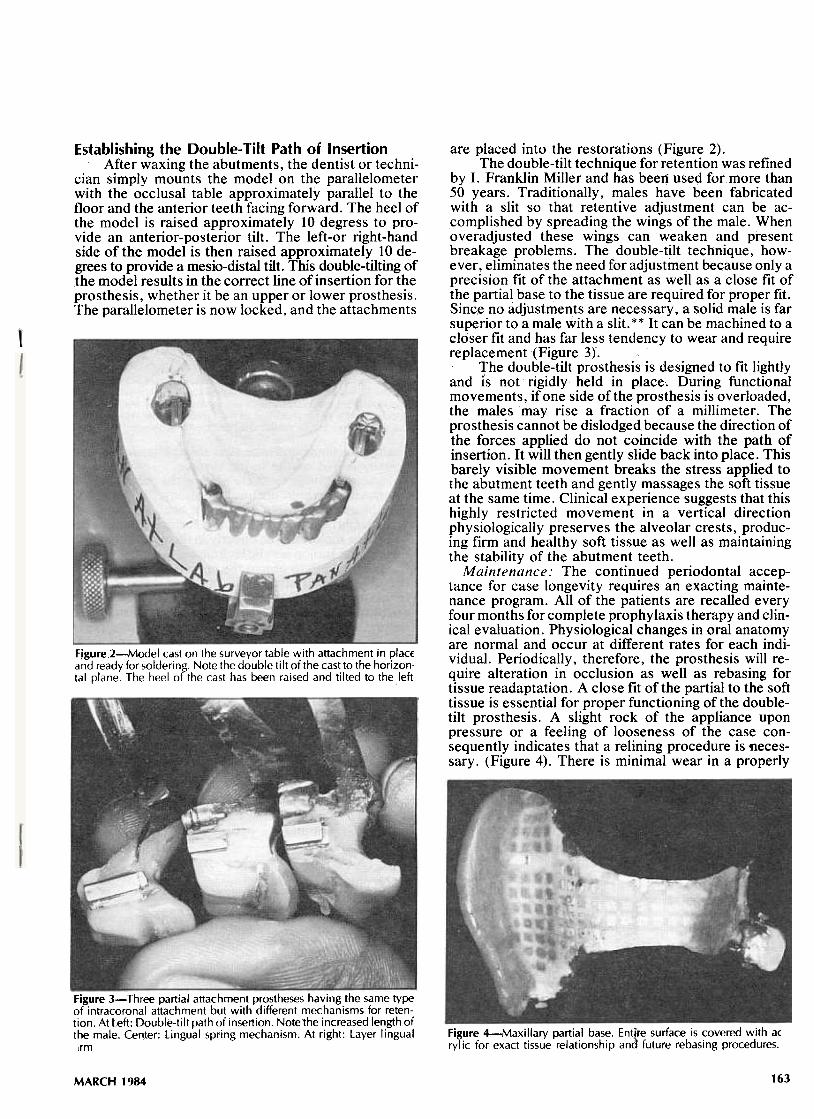
F,gure2-Model cast on the surveyor table with attachment in plac;:Eand ready for solderi ng. Note the double ti It of the cast to the horizon.tal plane. The heel of the cast has been raised and tilted to the left
Figure 3- Three partial attachment prostheses having the same typeof intracoronal attachment but with different mechanisms for reten-tion. At Left: Double-tilt path of insertion. Note1he increased length ofthe male. Cen,ter: Lingual spring mechanism. At right: Layer lingual Figure 4-Maxillary partial base. EntIre surface is covered with a(
rylic for exact tissue relationship and future rebasing procedures.lrm
163MARCH 1984

Figure Sa-Housing for female attachment is not covered with porce-lain so that canine does not appear large mesiodistally.
functioning attachment. This procedure is the onlymethod ever used to retighten the removable partialdenture. The acrylic saddles are rebased indirectly bylaboratory processing or directly by the use of Biolonacrylic impressions from the mouth. Biolon impres-sions have a great advantage since they can be proces-sed, without making models, in 30 to 40 minutes whilethe patient waits. A pressure pot with pressure andtemperature controls is used to cure the acrylic.
Every case is routinely rebased, 30 to 60 days afterinsertion, as the tissue will normally exhibit slight
Figure Sb-Upper and lower attachment cases, seven years later. Thebicuspid pontic overlaps the canine housing for esthetics. Note thegroove on the gingival portion of the lower bicuspid makes it easierfor patient to remove partial with doubie-tilt pathway.
changes in shape and tone after the appliance has func-tionally rested on the tissue surface.
Acrylic pontic teeth are used on the partial dentureto provide greater occlusal harmony. Within threemonths after insertion, the acrylic occlusals are shor-tened slightly and a new occlusal surface is establishedbyadding Biolon acrylic directly in the patient's mouth.Prior to the Biolon acrylic technique, wax was added tothe pontic teeth to obtain the correct occlusion. Thenthe case was routinely flasked and packed in thelaboratory. This direct method provides a much betterocclusal harmony with either dental restorations ornatural teeth than the traditional grinding in of porce-lain denture teeth. Every five to seven years, anewocclusion may be added to compensate for the wearand physiologic changes that occur. (Figures Sa andSb).
SummaryClinical evaluation of approximately 1,500 cases
over a 30-year period indicates that intracoronalattachments using a double-tilt retention mechanismoffer one of the most successful approaches for remov-able partial denture therapy. Adherence to precisiontechniques, proper diagnosis and periodic recall pre-ventative therapy will result in successful treatmen_tand preservation of the patient's existing dentition formany years. O
ReferencesI. Feinberg, E.; 1970, Full Mouth Restorations in Daily Practice,
J.B. Lippincott, Phila., Pa.2. Preiskel, H.W.; 1979, Precision Attachments in Dentistry, 3rd
Edition, C. V. Mosby, St. Louis, Mo.3. Miller, E.L.; 1972, Removable Partial Prosthodontics, Williams
and Wilkens, Baltimore, Md.4. Singer, F.; Schon F.; 1973, Partial Dentures Die, Quintessence,
Chicago, Ill.5. Feinberg, E.; Diagnosing and Prescribing Partial Dentures,
New York State Dental ,Journal: Vol. 48 No.1, Jan. 1982.
'*Feinberg Modified Stem #7 Attachment-APM-Stemgold,Stamford, Conn.
NYS DENTAL JOURNAL164