butterworth-heinemann linacre house, jordan hill, oxford ... · linacre house, jordan hill, oxford...
TRANSCRIPT

Butterworth-HeinemannAn imprint of Elsevier ScienceLinacre House, Jordan Hill, Oxford OX2 8DP225 Wildwood Avenue, Woburn, MA 01801-2041
First published 2002
© 2002, Elsevier Science Ltd. All rights reserved
No part of this publication may be reproduced in any material form (includingphotocopying or storing in any medium by electronic means and whether ornot transiently or incidentally to some other use of this publication) withoutthe written permission of the copyright holder except in accordance with theprovisions of the Copyright, Designs and Patents Act 1988 or under the termsof a licence issued by the Copyright Licensing Agency Ltd, 90 TottenhamCourt Road, London, England W1T 4LP. Applications for the copyrightholder’s written permission to reproduce any part of this publication shouldbe addressed to the publishers
British Library Cataloguing in Publication DataWilliams, David L.
Veterinary ocular emergencies1. Veterinary ophthalmology 2. Veterinary emergenciesI Title II. Barrie, Kathy III. Evans, Thomas Ffrangcon636'.08977'026
Library of Congress Cataloging in Publication DataA catalog record of this book is available from the Library of Congress
ISBN 0 7506 3560 6
Medical knowledge is constantly changing. As new information becomesavailable, changes in treatment, procedures, equipment and the use of drugsbecome necessary. The authors and the publishers have taken care to ensurethat the information given in this text is accurate and up to date. However,readers are strongly advised to confirm that the information, especially withregard to drug usage, complies with the latest legislation and standards ofpractice.
Composition by Scribe Design, Gillingham, Kent, UKPrinted and bound in Great Britain by MPG Books Ltd, Bodmin, Cornwall

All too many veterinarians leave veterinarycollege with little exposure to ophthalmiccases and certainly next to no experience ofeven the most common ocular emergencies.Veterinary colleges generally admit referralcases, and so even when ophthalmology iswell taught as a major core curriculum subjectthere is little opportunity to see ocularemergencies which are dealt with in first-opinion settings. This book is designed as ahelping hand to all practitioners who arepresented with an ocular emergency havinghad little introduction, either theoretical orpractical, to veterinary ophthalmology orespecially to ocular emergencies.
The book is not designed, however, to doaway with the need for referral consultationin a specialist centre. If it is considered thatthe ocular disorder for which the animal ispresented may be serious, with ocular pain orpotential blindness, a referral or secondopinion should always be offered to the
client. Many pets are insured and it is to thebenefit of the animal, the owner and yourselfto have a second opinion on the case.
The eye is without doubt a special structureand vision is, some would say, a veritablemiracle and a delicate one at that. Surgery ofthe eye, in particular, should always involvesensitive tissue handling with plenty of irrigat-ing fluid. Cadaver practice prior to one’s firstsurgical enterprise is essential. But the eye isnot holy, not an organ which can only be dealtwith by specialists. The aim of this volume isto allow veterinarians in general practice todeal better with emergencies which wouldotherwise result in pain and/or blindness.Thus our ultimate hope is that the book willimprove the treatment of animals presented, aswell as helping the vets who treat theseanimals to feel better-equipped to diagnoseand treat these often difficult cases.
Thomas Evans 2002
Preface

1. Intense conjunctival redness associatedwith corneal ulceration in a cross-bred dogafter a road traffic accident
It is vital to assess the entire eye given that blunttrauma may cause severe intraocular injury. The ulcershould heal within seven to ten days but antibiosisand anti-inflammatory medication (using a topicalnon-steroidal such as ketorolac rather than topicalsteroid) should be used during this time. One concernshould be that the conjunctival swelling or chemosismay preclude full eyelid closure. This wouldcompromise rapid ulcer healing and thus use of asurface protective agent such as viscotears carbomergel or hylashield a hyaluronic acid preparation wouldbe advisable. Should complete healing not occurrapidly debridement of devitalized epithelium may benecessary to promote ulcer healing.
2. Chlamydial conjunctivitis in a domesticshorthaired cat
Conjunctivitis in the cat is often caused by Chlamydia(now renamed Chlamydophila felis by someauthorities) or feline herpesvirus. Given the difficulty ofdiagnosing these by isolation and culture of the agent,polymerase chain reaction (PCR) tests may be valuable.A cheaper alternative is to treat the cat with topicalchlortetracycline (Aureomycin). A positive response totherapy strongly suggests Chlamydia to be the agentresponsible while a negative response indicates that atopical antiviral such as trifluorothymidine or acycloviris a worthwhile agent to use.
3. Uveitis with hypopyon in a Jack Russellterrier
An eye with a profound hypopyon such as thisneeds aggressive topical steroid medication withprednisolone acetate (Pred Forte) used four timesdaily. Before that, however, a full systemicexamination should be undertaken and ahaematological profile: all too often theseintraocular inflammatory conditions can be apresenting sign of lymphosarcoma or leukaemia.
4. Acute glaucoma with pain, blindness,episcleral congestion and corneal oedema in aWelsh springer spaniel
Here measurement of intraocular pressure isimportant but even without the facility to performthis it should be assumed that the intraocularpressure is high. Use of mannitol in the acutephase can be valuable as topical anti-glaucomaagents such as dorzolamide (Trusopt). the betaantagonist timoptol or pilocarpine are unlikely toreduce the intraocular pressure sufficiently orrapidly enough to prevent irreversible blindness.

5. Scleritis with intense ocular redness andscleral nodules in a Rotweiler
This intense scleral inflammation requires bothtopical steroid medication and systemic prenisoloneat up to 1 mg/kg. Other agents such as azathioprinecan be valuable in particularly severe cases.
6. Globe prolapse in a Pekingese dog(courtesy of Dr S.M. Crispin)
A pulse dose of steroid should be given first toreduce periocular swelling and ocular surfacelubrication should be maintained with a damp swabor with copious surface protectant such as acarbomer gel such as viscotears. Early surgery toperform a lateral canthotomy should be performedto allow easy replacement of the globe, followed bya tarsorraphy, held in place for 2 weeks minimum.
7. Globe penetration with corneal, iris andalso possible lenticular damage
Here the concern lies in multiple directions. Theloss of aqueous when the foreign body is removedwill result in a plasmoid secondary aqueous andsevere inflammation. Intraocular infection is to beexpected. Worse still is possible damage to thelens; lens capsule rupture with loss of corticalmaterial into the anterior chamber will result in asevere uveitis with supervening glaucoma in themajority of cases. Removal of the lens is the onlyviable treatment option to prevent this occurring.
8. Acute keratoconjunctivitis sicca aftersystemic sulphasalazine administration
The key step here is realizing that the intense redeye is a result of acute total ocular surface drying.Use of a Schirmer tear test will demonstrate this ina minute but there has to be the index of suspicionto move one to perform this test in such asituation. Treatment with tear replacement isrequired and topical cyclosporine can be evaluatedalthough in many such drug-induced cases of dryeye there is little response to this usually excellentdrug.

9. Chronic keratoconjunctivitis sicca withpigmentary keratitis
In a more chronic case of keratoconjunctvitis siccasuch as this there can still be situations that presentas emergencies. Pigmentary keratitis can give adisturbance of vision which resembles a suddenblindness which corneal ulceration may supervenewhere there is no ocular surface lubrication.
10. Deep corneal ulceration showing lack ofstromal oedema in centre of deep ulcer bed
This presentation of a corneal ulcer is an acuteemergency. Note the stromal oedema giving awhite appearance to the corneal, except in thecentre of the ulcer. Here the excavation of corneahas been so extensive that there is little stroma leftto be oedematous and waterlogged. The ulcer isclose to rupturing with catastrophic consequences.A conjunctival pedicle flap is required rapidly.
11. Descetocoele in a West Highland whiteterrier
Again the finding of a bulging clear dome in thecentre of the ulcer shows that the ulcer hasprogressed to the very farthermost depth of thecornea. Here a pedicle flap may not be sufficientand a corneoscleral transposition may be requiredto preserve structural integrity of the cornea.
12. Stromolytic (melting) Pseudomonascorneal ulcer in a Shetland pony
This acute emergency results frommetalloproteinase (collagenase and gelatinaselactivity originating both from the Pseudomonasorganisms infecting the corneal surface and theneutrophils recruited to destroy them. Thus theanimal needs frequent administration of anappropriate antibiotic (topical polymycin/bacitracinor a topical fluoroquinolone) and anti-collengasessuch as EDTA, acetyl cystein and the alpha-2macroglobulin anti-proteases in serum.

13. Keratic precipitates in feline uveitisdemonstrated in the fine beam of a slit lamp
The finding of anterior uveitis. in one eye should befollowed up with evaluation of the anterior andposterior segments of the other eye for similarpathology. Serology for organisms such as FIP, FIV,FeLV and Toxoplasma can be worthwhile but thetreatment is topical steroid apart from the latterorganism where clindamycin is curative.
14. Anterior lens luxation with the edge ofthe lens clearly demonstrated by the circularlight reflection
Surgery to remove the lens is the only option herealthough topical anti-glaucoma medications may begiven to relieve high intraocular pressure shouldsurgery be delayed. Another important feature tonote before surgery is the state of the second eye;a subluxated lens in this eye may beprophylactically removed under the sameanaesthetic.
15. Feline hypertensive retinopathy withserous retinal detachment
The signs of hypertensive retinopathy, such asserous detachment, intraretinal or choroidalhaemorrhage and abnormalities of the retinalvessels, call for measurement of the animal's bloodpressure. Even without this facility the above signsmay be considered sufficiently indicative to warrantinstigation of treatment with amlodipine at 0.625 mgdaily.
16. Haemorrhagic optic neuritis and retinalvasculitis in a Dachshund
Blinding optic neuritis requires emergencytreatment with parenteral steroid at 1 mg/kgalthough prognosis for recovery of vision is poor.Infections such as distemper and mycoses orrickettsiae should be considered and a detailedhistory including foreign travel should be taken aswell as a full haematological and biochemicalprofile.

Some may consider that there are quiteenough veterinary ophthalmic texts on themarket at present – why do we need another?We suggest that there are two specificproblems with the current texts, excellent andcomprehensive as they are. The first is that tofind diagnostic and therapeutic strategies inan emergency is almost impossible. Mosttexts require at least an evening’s read todistil out the necessary diagnostic featuresand treatment requirements for a specificemergency condition be it a surgical condi-tion at the ocular surface, such as a staphy-loma (see Appendix B for the Oculardictionary), or a predominantly medicalcondition in the posterior segment such as asudden total retinal detachment.
Secondly, most texts are presented with ananatomical breakdown of ocular conditions.The animal does not, however, present as ifsaying ‘I have a problem with my irido-corneal angle,’ but rather ‘I have a red eye’ or‘I am suddenly blind’. Thus to be useful anemergency text needs to be thoroughlyproblem-oriented, not an easy task given astructure such as the eye which is so neatlypackaged anatomically.
This text aims to fill that gap in the marketin four ways. A problem-based first part willgive the basics on diagnostic signs such as thered eye, the painful eye or the blind eye. Thatis where to start in assessing an ocularemergency. Secondly, each ocular emergencyis discussed with regard to diagnostic testsapplicable and therapeutic regimes advised.
Thirdly, both of these first two areas areheavily illustrated not by pictures: these canbe found in the growing number of excellentatlases being produced by Barnett (1990),Barnett et al. (1995), Crispin and Barnett(1997) and Walde (1990); but by diagramsdemonstrating the plan of attack in both thediagnostic work up of a case and the treat-ment regimen to be used. Fourthly, theauthors feel that veterinarians are muchbetter placed to deal with an emergencywhen knowing a reasonable amount of thebasic science background behind the patho-genesis of ocular damage and the mech-anisms underlying successful treatment.Therefore, while the text gives diagnostic andtherapeutic suggestions including step-by-step flow diagrams, it also discusses thebackground to the disease processes and theameliorating effects of treatment.
Reading through the whole text sequen-tially, one may be struck by a number ofrepetitions: these are unavoidable to ensurethat each section has the opportunity to standon its own when read in an emergency situa-tion. It is hoped, however, that having thesame information presented in differentcontexts throughout the text will be helpful inaiding understanding and remembering factsrather than be annoying and repetitious. Theaim of this book is to provide a useful start-ing point in an emergency situation where thestep-by-step diagram and table format allowrapid appreciation of important information.Also, once the emergency is over, it will be
Introduction

possible to read the discussion sections atleisure to elucidate some of the basic sciencebackground. In this way, should the sametype of emergency arise again, it will bepossible to approach it with a greater degreeof understanding both regarding pathogenicmechanisms and therapeutic rationale.
We have attempted to write the portionsfor background reading in a style which iseasy and enjoyable to read. Some may findthis annoying and prefer a more scientific andless familiar manner. Given the number oftexts in densely written scientific prose wehave sought not to use that approach, andhope that readers will find this text easy touse both in the emergency situation and alsofor reading once the emergency has beenresolved.
Chapter 1 touches on the diagnostic princi-ples and techniques in dealing with anemergency; Chapter 2 looks as the variouscommonly presented conditions associatedwith problems with the eye; while Chapters 3to 10 cover the initial diagnosis and treat-ment. Three appendices are also provided.Appendix A deals with the common applieddiagnostic methods. This section is notincluded in the main text as some veterinarysurgeons may find it common knowledgewhile others will find a thorough descriptionof instruments such as a Schiotz tonometeruseful. Appendix B is a veterinary ophthalmicdictionary. As ophthalmic nomenclature isvery specialized all specific words mentionedin the text are explained in this section of thehandbook. Appendix C is a drug index,where we have tried to include most of thedrugs (human as well as veterinary) that areused for treatment of eye diseases in animals.
One final criticism is likely, perhaps notfrom general veterinary surgeons but fromour colleagues in specialist practice. They willsay, with perhaps some justification, that ingeneral practice one does not need to knowthe ins and outs of treatment of uveitis or
glaucoma cases. Such animals, they will say,need referring to a specialist trained indealing with the sort of ophthalmic night-mares considered in this book. This may wellbe the case, and some specialists may evenfeel done out of a job if the diagnostic proto-cols and therapeutic regimens used are setout in detail. We feel, however, that such anapproach would be short sighted and in thebest interests of nobody, let alone the animalitself. Even when the specialist practice isonly a car ride away, and the owners arehappy to pay, the referring veterinarian mustbe able to define that referral is needed andgive immediate treatment in every situation.In many cases distance, financial considera-tions or the time delay between presentationand an emergency referral means that it is upto the veterinarian to give care for theemergency case through the short term andoften for longer. And who knows – perhapsdealing in this way with a few such cases,with the help of this book, will attract youfurther into the fascinating world of veteri-nary ophthalmology, leading you to train tobe one of those specialists. Nevertheless theauthors understand that many of these casesare, in the normal run of events, betterreferred immediately to a specialist. Situa-tions where this is the case are marked thus® in the text: referral is recommended inthese cases.
It may be argued that most of theparagraphs here are preceded by an ®.Obviously, as veterinarians earning our livingfrom ophthalmic referrals we are hardlygoing to dissuade you from asking for asecond opinion, are we! Most cases willbenefit from a referral, yet the whole point ofthis book is to equip veterinary surgeons withthe knowledge to give immediate treatmentthat is appropriate, to recognize cases requir-ing referral and, in cases where referral is notappropriate, to make the best diagnostic andtherapeutic interventions possible.
x Introduction

1.1 Performing an ocularexamination in an emergencysituation
The temptation, in an emergency, is toabandon the standard ophthalmic examina-tion which would be undertaken undernormal circumstances and merely concentrateon the immediately obvious ocular signs.Thus, in a dog with an eyelid laceration theglobe is only cursorily examined. Given a catwith a corneal ulcer, the lids and intra-ocularstructures are ignored. This failure to performa standard examination will, in many if notthe majority of cases, result in failure eitherfully to reach the correct diagnosis or toidentify important, but less obvious, concur-rent ocular disease or damage. In the dogmentioned above there may be a globerupture as well as the eyelid laceration. In thecat the corneal pathology may be related to apost-traumatic eyelid defect with trichiasiswhile the corneal lesion may cause reflexmiosis or more pronounced uveitis. In thefirst case failure to appreciate concurrentdisease could result in loss of the eye, whilein the second the rushed examination missesboth the cause of the presenting sign and thepotentially important intra-ocular sequelae.
Thus, a systematic approach is vital toevery emergency ocular examination, asshown in Box 1.1. The evaluation shouldbegin with an assessment of vision using themenace and startle responses, and then deter-mination of pupil size and pupillary light
response, including the swinging light test todetect functional optic nerve defects. Theexamination of the eye itself starts withdistant direct ophthalmoscopy. This calms theanimal rather than beginning the examinationwith one’s head close to the animal’s muzzle.It allows evaluation of pupil size and anyopacity of the ocular media. Next the eyelidsand adnexa, including the conjunctiva, areexamined with the direct ophthalmoscope ata setting of +20 D. Remember that theconjunctiva is found covering the globe(bulbar conjunctiva) and the inner aspect ofthe eyelid (palpebral conjunctiva). Thus whileuveitis or glaucoma affect the vasculature ofthe globe alone, conjunctivitis involves thevessels of the bulbar and palpebral conjunc-tiva. In assessing the conjunctiva bothsurfaces of the nictitating membrane shouldbe examined as should the conjunctiva rightto the depths of the fornices. This may bedone later, after topical anaesthesia and fixingthe margin of the third eyelid with a pair ofhaemostats or Babcock forceps, everting andlooking behind the third eyelid. Next, inorder, the cornea, anterior chamber, iris, lens,vitreous, retina and optic nerve head areexamined with the dioptre settings of thedirect ophthalmoscope at from +20 D (corneaand sclera) and +10 D (iris and lens) to 0 D(retina).
After full examination, ancillary aidsshould be brought into play. We considerthat, given the simplicity of the test, everyanimal presenting as an ocular emergency
Chapter 1
Diagnostic principles and techniques

should have a Schirmer I tear test performed(Appendix A). Measurement of intra-ocularpressure by applanation tonometry is moredifficult given the expense of tonometers suchas the Tonopen, but on the other hand thepurchase of a Schiotz tonometer is wellwithin the budget of a practice keen toprovide an adequate ophthalmic work up.The importance of early diagnosis of raisedintra-ocular pressure, and of following treat-ment response in animals with glaucoma,renders it almost essential that every practicehas access to at least a Schiotz tonometer(details of using the Schiotz to optimal effectare given in Appendix A).
1.2 Recording observations madein an ocular emergency
The ophthalmic emergency might seem theleast appropriate time to make detailed notesand drawings of the ocular signs presented.However, if one is already in the habit ofcarefully recording what one sees at anophthalmic examination, this is tremendouslyuseful for two reasons. First, it is important tohave written and diagrammatic records ofwhat was seen at presentation, in order betterto be able to monitor the progress andhopefully the recovery of ocular health.Secondly, recording observations and
2 Veterinary Ocular Emergencies
1 Assessment of vision:Menace responseDazzle responsePupillary light reflexSwinging light test
2 Distant direct ophthalmoscopy:Assess pupil size and symmetryAssess clarity of ocular media
3 Adnexa:LidsConjunctivaNictitating membraneNasolacrimal system
4 Cornea:Transparency +20 DStructural integrity
5 Uvea:Colour +10 DContour
6 Lens:Transparency +10 D ± 5 DPositionStability
7 Vitreous and retina:PositionTapetal reflectivity 0 ± 3 DVascular system
Box 1.1 Routine ophthalmological examination

particularly drawing annotated diagramstend to improve one’s assessment of lesionsin the eye and ensure that small lesions havenot been missed. In the ophthalmicemergency it is, however, important to beable to record ocular signs quickly and tohave a ready method of diagrammaticallynoting signs in such a way as to differentiate,
for instance, between corneal oedema, infil-tration and scarring or a retinal haemorrhage,cellular infiltrate or a small area of retinaldetachment. Two useful papers have beenproduced in the human ophthalmic literaturesuggesting methods of recording ocular signs.A diagnosis sheet for any ophthalmic exami-nation is given in Figure 1.1 and may be
Diagnostic principles and techniques 3
adnexa
cornea
retina
Name
i.d.
species
age/sex
history
lens/anterior chamber
Figure 1.1 An example of a diagnostic sheet for ophthalmic examination. Note that a full-page version ofthis figure (available for photocopying and use by readers) is provided on page 95

copied to give an acceptable method ofrecording ophthalmic lesions in anemergency (see page 95). Alternatively,readers can devise their own scheme torecord ophthalmic signs in an emergencysituation and in everyday practice.
1.3 Equipment and aids requiredto deal with the ocular emergency
It has already been indicated that a simpletonometer is required as a basic tool in everypractice. What other items should be close tohand to deal with the ocular emergency?Clearly a good ophthalmoscope is essential.Although many veterinary ophthalmologistsarm themselves with an indirect ophthalmo-scope and slit lamp as basic tools for anophthalmic examination, in reality a gooddirect ophthalmoscope will suffice in a
general practice setting. As well as enablingexamination of the retina at the 0 D settingand the iris and lens at a setting of +10 D, thedirect ophthalmoscope is a very usefulmagnifying lens for the cornea and adnexawhen used at +20 D. With a powerful halogenlight source such an instrument, although notlooking as impressive as a slit lamp, is muchless expensive and yet invaluable if used tomaximum effect.
A cheap solution for indirect ophthal-moscopy is a plastic 20 D lens held close tothe cornea of the animal and a simple pentorch held to the ear of the examiner (Figure1.2a). This will enable the examiner to viewmost of the fundus at one time. For examina-tion of the iridocorneal angle a goniolensmight be considered worth obtaining, theKoeppe or Franklin lenses being particularlyeasy to use (Figure 1.2b). Their application isconsidered further in Appendix A.
4 Veterinary Ocular Emergencies
Figure 1.2 Indirect ophthalmoscopyusing a plastic 20 D lens held closeto the cornea of the animal and asimple pen torch held to the ear ofthe examiner. (a) Uni-ocular indirectophthalmoscopy; (b) binocularindirect ophthalmoscopy
(a)
(b)

Schirmer tear test strips are valuable andshould be used to determine tear productionor lack of it before any manipulation of theeye is attempted. The dyes fluorescein androse bengal should be a key part of thediagnostic armamentarium: their use isdescribed further in the corneal section.Bacteriology swabs should be at hand asshould a Kimura spatula for the collection ofcytology samples. Kimura spatulas are expen-sive and the blunt end of a Bard-Parkerscalpel handle may be used in its place. Amore recent innovation is that of cytologybrushes (Figure 1.3) which increase cellrecovery and reduce sampling-induceddamage to recovered cells (Wills et al. 1997).
Local anaesthetic is necessary in manyinstances. Profound anaesthesia can beobtained by soaking a cotton-tipped applicatorand pressing it firmly onto an area of conjunc-tiva before, for instance, the collection of aconjunctival biopsy in the conscious patient.
Figures 1.4 to 1.7 show both the basic, aswell as the more specialized, sets ofophthalmic equipment.
Diagnostic principles and techniques 5
Figure 1.3 Use of a cytology brush will increasecell recovery and lessen sampling-induced damageto recovered cells
Figure 1.4 Direct ophthalmoscope Figure 1.5 Slit biomicroscope
Figure 1.7 Schiotz tonometerFigure 1.6 Gonio lens

1.4 Some preliminary notes ontreatment of ocular infections
Ocular infections are generally considered asadnexal diseases resulting in conjunctivitis,be it purulent, chemotic or hyperaemic. Butinfection of the eye may involve the orbit,giving a purulent cellulitis; or the cornealstroma, giving either a well-defined stromalabscess or a more diffuse stromal infiltration;or may be intra-ocular, with a purulentanterior uveitis or a more generalizedpanophthalmitis. There are several differ-ences between the bacteriological investiga-tion of an ocular infection and an infectioninvolving skin or soft tissue. The most im-portant difference is the frequent paucity oforganisms isolated from the eye. This meansthat when a swab from the conjunctiva istaken into transport medium and later platedonto agar, there is often only a scanty growthof organisms. Plating directly from the swabis much to be preferred. The prevalence offungal disease of the ocular surface, especiallyin warm climates, means that a Saboraud’sagar plate should be used as well as a bloodagar plate. This, in practice, mostly applies toequine ocular infection and to cases in otherspecies where the trauma has been caused byvegetable matter such as a thorn or a branch.
Antibiotic sensitivities for cultured organ-isms should be viewed with caution: sensi-tivities are based on likely blood levels oforally or parenterally delivered antibiotics,and the much higher concentrations are givenlocally by topically applied antibiotics.Whenever possible MIC-determinations willbe of greater value than sensitivity testingbased on disc diffusion.
There are many instances of drug resistancein bacteria affecting the ocular surface,especially with regard to gentamicin in thetreatment of Pseudomonas. The use of fortifiedpreparations, as detailed in Appendix C, hasbeen widespread to overcome this problem ofresistance but itself is likely to induce resist-ance at higher levels. The more appropriatealternative would be any of the lesscommonly used aminoglycosides, such astobramycin, to which resistance has been lessfrequently noted. More potent antibioticsinclude the quinolones: ofloxacin,ciprofloxacin or norfloxacin. Their mode ofaction, inhibiting DNA gyrase, is novel and
thus resistance to other drugs would notaffect these drugs. As with every antibiotic,however, the important factors in discourag-ing resistance are regular dosing and persist-ence with treatment until well after the signshave gone. Inadequate dose frequency andcessation of treatment while there are stillsome organisms present are likely to lead toresistance development.
Apart from such considerations, we recom-mend two drugs for general topical use inexternal eye disease in dogs and cats respec-tively before bacteriology results are avail-able. These are fusidic acid for dogs andchlortetracycline for cats. These choices aremade given the common organisms seen inthese species. Normal bacterial conjunctivalflora in dogs include Staphylococci and Strep-tococci (Gerding and Kakoma 1990). Normalflora in cats include these Gram-positivespecies; common agents causing disease aremore likely to be Gram-negative organisms,Chlamydia and Mycoplasma (Gerding andKakoma 1990), more sensitive to the tetracy-clines. Better than either of these for trans-corneal penetration, and thus indicated inintra-ocular infections, is chloramphenicol.This has a wide range of activity, importantwhen the full identity of the organisminvolved is not known.
The use of general broad-spectrum antibi-otics is based on the assumption that theresult of bacteriological culture and sensitiv-ity will not be available for at least two orthree days from the time of sampling, evengiven a courier dispatch service and the mostrapid laboratory turn-around. Clearly a morerapid system is needed to give an indicationof which class of infectious agent is presentand whether corneal integrity is threatened.In an emergency situation it is important tobe proficient in preparing bacteriologicalstains of smeared swab samples or scrapesfrom cornea or conjunctiva. Three suchsmears, stained with Gram’s stain, Diff Quik(Giemsa) and lactophenol cotton blue willallow a very rapid assessment of whether aGram-positive organism is present, probablysensitive to fusidic acid, a Gram-negativeorganism requiring chloramphenicol or tetra-cycline, or a fungal agent best treated withketaconazole. It may be argued that in notevery case is the offending organism seen ona scrape or smear – exfoliative cytology in
6 Veterinary Ocular Emergencies

such cases will render a neutrophilic infil-trate, which even if no organisms are seenshould be taken as evidence of bacterial infec-tion (Lavach et al. 1977, Severin and Thrall1981, Ugomori et al. 1991).
1.5 Analgesia in ocularemergencies
All too often in veterinary medicine, theseauthors feel, we pay too little attention to painrelief either post-operatively or after atraumatic incident. The fact that many animalsappear to cope stoically with what we wouldconsider an acutely painful injury or conditionshould not let us negate our duty to provideadequate, or perhaps it should be said betterthan adequate, pain relief. The eye is anexquisitely delicate organ with an amplenociceptive nervous supply. This is especiallyso on the ocular surface, with a nerve networkat a very superficial level in the cornea. Theophthalmic division of the trigeminal nerveinnervates the cornea through the long ciliarynerves, radiating into the stroma from thelimbus, there losing their myelin sheaths andforming a subepithelial plexus (Prince et al.1960). From there fine axons, devoid even ofSchwann cells, pierce the epithelium forming
an intra-epithelial plexus highly sensitive topain and to changes in temperature. Thesebare nerve endings are therefore less than50 µm from the ocular surface. This detail ofanatomy is highlighted to impress upon thereader the importance of analgesia in ocularsurface disease (see Figure 1.8, Spreull 1966).
Diagnostic principles and techniques 7
Ocular pain: origins and analgesicsBox 1.2 Ocularpain
Figure 1.8 Diagrammatic representation of thesensory nerve pattern of the cornea (after Princeet al. 1960)
ch01 8/3/02 11:58 Page 7

In the emergency setting such analgesiamay involve topical local anaesthetic such asamethocaine or proxymethocaine, but this canonly be used in the short term because of toxiceffects on corneal epithelium (Grant andAcosta 1994). Such local analgesia may berequired fully to examine the eye. The use ofprofound sedatives such as the alpha 2agonists alone perhaps should be questioned,since while they render the animal more easilyhandled, the degree of analgesia may be insuf-ficient. Parenterally administered analgesicssuch as a non-steroidal anti-inflammatoryagent (e.g. carprofen or flunixine meglumine)or in more severe circumstances an opiatesuch as methadone or butorphenol should beconsidered in such cases and for moremedium-term pain relief. In the cat ketopro-fen should be used in the place of carprofen.
In the case of pain associated withprofound miosis, as seen in uveitis, the maincause of pain is spasm of the cilary body. Forthis reason a mydriastic cycloplegic (ciliary-body paralysing agent) such as atropine maybe a better analgesic than a standard non-steroidal or even opiate analgesic. Whiletropicamide is more rapidly acting it has lesscycloplegic action than atropine, so it is thelatter drug which should be used as a ciliary-body spasmolytic agent in uveitis.
1.6 Dealing with ocular emergenciesin horses and ruminants
Ophthalmology is a wonderfully trans-speciesdiscipline. While at first it was intended thatthis book would aim solely at small animalveterinarians, the authors then decided thatincluding horses and food animals would beappropriate. We still focus on the smallanimal but include large animals, and partic-ularly companion equine ophthalmicemergencies throughout the text. There aresome significant differences in these species,particularly considering the approaches bothto clinical examination and to medication, andit is these which are covered by this section.
1.6.1 Techniques facilitating large animalocular examination
Examination in a light environment rendersophthalmoscopy difficult and thus a darkened
box should be sought or, if this is not possi-ble, a large sheet of fabric (preferably darkblue or black) can be put over the head of theexaminer as well as of the horse, as a tent tosimulate a darkened room.
The examination of a painful eye is alwayssomewhat tricky, but this is accentuated withhorses and food animals where the tempera-ment of the animal and the muscular powerof the blepharospastic eyelids combine to
8 Veterinary Ocular Emergencies
Figure 1.9 Use of an auriculo palpebral nerveblock in the horse
Figure 1.10 Needle placement for a Petersen blockin cattle (after Lavach, 1990)

render safe visualization of the ocular surfacedifficult. Mild sedation remedies the firstproblem, but may not ameliorate the coveringof the globe by lids in muscular spasm. Theuse of an auriculopalpebral nerve block in thehorse (Figure 1.9) and the Petersen block,commonly used in cattle (Figure 1.10), allowfull examination without the interference ofeyelid spasm (Lavach 1990). Retrobulbarmuscle spasm may give considerable enoph-thalmos in cattle which, again, complicatesexamination. Here the Petersen block amelio-rates the problem (Lavach 1990).
1.6.2 Techniques facilitating large animalocular therapeutics
Here we consider three techniques – first thesimple method of subconjunctival drug deliv-ery. This is particularly useful in ruminantdiseases such as New Forest Eye – infectiousbovine keratoconjunctivitis (IBK) associatedwith Moraxella bovis and Mycoplasma bovicula.In the treatment of IBK, systemic tetracyclinetherapy may be necessary (Lavach 1990); butoften a subconjunctival depot injection of anappropriate antibiotic such as cloxacillin isefficacious for around three days beforerequiring a second application.
There are some theoretical considerationsto take note of before accepting that this is theoptimum route for all large animal ocularmedication. Drugs injected subconjunctivallymight be supposed to enter the eye by trans-scleral penetration. A significant volume ofinjected solutions, however, has been shownin other species to exit from the injection siteand be absorbed by topical transcornealpenetration. Entry by the trans-scleral routecan be optimized by a deeper injection at asub-Tenon’s level. This can be importantwhen the aim is to give high intra-ocularlevels of antibiotic rather than corneal orocular surface medication. Such injectionsmay require considerable sedation: in anycase subconjunctival injections should beattempted only after topical ocular surfaceanaesthesia.
The main indication for subconjunctivaldelivery in the horse or small animal is theinjection of antibiotics for the emergencymanagement of anterior segment infection.Corticosteroid depot injections can also begiven in this manner for treatment of corneal
inflammation. In either case, subconjunctivalmedication supplements topical therapyrather than replacing it. Similarly the appli-cation of mydriatics in emergency situationsby the subconjunctival route might be consid-ered in equine or in small animal anterioruveitis. There are, however, potentialproblems of systemic absorption of potentautonomic agents with the injection of drugssuch as atropine and adrenaline.
The need to provide frequent topical ocularmedication to painful eyes is especiallyimportant in equine uveitis and ulcerativekeratitis. In these conditions horses will oftenvigorously resent regular instillation ofmedication and thus placement of a drugdelivery system allowing interference withthe eye to be minimized is advantageous.Two systems have been reported. Thenasolacrimal lavage system involves a lengthof tubing placed from the nasal nasolacrimalpunctum to reach the upper end of the duct(Figure 1.11). Drug solutions can then beinstilled topically up the nasolacrimal duct.While having the considerable advantage of
Diagnostic principles and techniques 9
Figure 1.11 Length of tubing is placed from thenasal nasolacrimal punctum to reach the upper endof the duct

ease of placement this system has the disad-vantage that drug delivery may also flushpotentially infectious material from thenasolacrimal duct back to the ocular surface.
In many cases the preferable technique isone of transpalpebral drug delivery, as illus-trated diagrammatically (Figure 1.12A–F).The optimal technique is a through-and-through placement with the tube anchored bya knot on the dermal (external) surface of thelid. This is preferable to the technique usinga single lid passage flare-ended tube: theflared end causes at best ocular irritation andat worst corneal damage. Securing the tubingafter a second passage through the lid may bemore time consuming to perform but avoidsany possibility of corneal damage. Polyethyl-ene tubing (PE 190) or a premature infantnasogastric feeding tube is used, with holescut at the appropriate site to allow the drugsolution to bathe the ocular surface. Horses,and especially those in considerable oculardiscomfort, need profound sedation before
the placement is attempted. Local anaesthesiawith intradermal lignocaine and topicaladministration of proparacaine or proxymeta-caine should also be given.
Two key features of tube placement shouldbe noted. First, the guide used to penetratethe lid, either a 14 gauge needle or preferablya 10 gauge flexible angiocatheter, alwayspasses from the conjunctival (internal) to thedermal (external) side of the lid. In this waythe cornea is always protected from abrasionor penetration. This does necessitate removalof the hub of the needle or catheter for thesecond pass through the lid, ensuring that theguide can be passed through the lid over thetubing after placement through the lid.
The second feature to note is that thetubing should be placed as deep in theconjunctival fornix as possible, to ensure thatcorneal abrasion does not occur while thedelivery system is in place. Then a smallquantity of drug is injected into the tubing,followed by a considerable bolus of air to
10 Veterinary Ocular Emergencies
Figure 1.12 Transpalpebral drug delivery via insertion of a cannula. (A) The cannula is placed through thelid from the conjunctival to the dermal surface; (B) the tubing is drawn through the cannula from the dermalto the conjunctival surface and the cannula withdrawn; (C) the cannula is placed through the lid from theconjunctival to the dermal surface, ensuring that the tubing has been removed; (D) the tubing is drawnthrough the cannula and then the cannula is withdrawn over the tubing; (E) the tubing is placed well abovethe globe surface; (F) the tubing is secured by knotting

force the solution through the deliverysystem to the ocular surface. The alternativeis to use a constant infusion device to delivera constant small flow to the ocular surface:such equipment can readily be fastened to thehead-collar, as can injection ports if frequentbolus deliveries are given.
A spray medication can be a valuable meansof delivering drugs to the anterior surface ofthe equine eye. The usual eye medication istransferred to a spray unit and the drizzle onthe cornea is likely to cause less reflex tearing;also the horse is less affected by the spray thanby topical delivery from traditional drop-bottles and eye-medication applied at thelateral canthus with a 1 ml syringe.
When using topical antibiotics in the horse,one must always consider the possibility offungal overgrowth. Thus if the infection is notresponding to topical medication, perform a
corneal scraping and investigate for fungusby microscopy as well as culture. For anexample of broad-spectrum antibioticsolutions for equine keratitis see Appendix C.
1.7 Ocular emergencies in exoticspecies
The majority of ocular emergencies in smallmammals, birds, reptiles and amphibia can bedealt with by simple extrapolation from whatis known from dealing with the dog and cat: acorneal ulcer in a parrot can be treated in muchthe same way as in a dog. On the other handthere are some significant differences whichshould be taken into consideration whendealing with an emergency in these species.These are discussed throughout the text but aregathered in Table 1.1 for ease of reference.
Diagnostic principles and techniques 11
Table 1.1 Where ocular emergencies in exotic animals differ from the dog and cat
Adnexal masses inlower vertebrates
Uveitis in lowervertebrates
Uveitis in lowervertebrates and birds
Traumatic keratitis inparrots
Pox virus in parrots
Dacryocystitis in rabbits
Myxomatosis in rabbits
Uveitis in rabbits
Often not neoplastic but inflammatory
Often associated with Gram-negative septicaemia
Miosis requires non-depolarizing muscle relaxant, not atropine
Reported particularly in Amazons and mynnah birds and requiringsupportive therapy predominantly with artificial tears
Early serious discharge becomes mucopurulent but the main lesions are lidscabs from self-trauma – prevent this with supportive tear replacement orbathing with mild baby shampoo
Causing significant white purulent ocular discharge – requires nasolacrimalcannulation and systemic antibiosis with enrofloxacin often the besttherapeutic agent
Swollen lids and white mucopurulent discharge or, in vaccinated animals,adnexal masses and lid distortion
May be associated with Pasteurella infection or encephalitozoan cuniculi-related phacoclastic uveitis

2.1 The red eye
This ophthalmic term refers to an eye inwhich the white of the eye is abnormallyreddened. There are other conditions result-ing in redness of the eye, such as hyphaemain which the blood in the anterior chamberimparts a red coloration to the eye. Inaddition trauma may lead to subconjunctivalhaemorrhage giving a red eye. Here,however, we will confine discussion to eyesreddened in a more diffuse manner. The fourclassic differential diagnoses of the red eyethus defined are
• Conjunctivitis• Uveitis• Glaucoma• Scleritis/episcleritis complex (less common).
One key point to note when considering thedifferential diagnosis of this clinical sign isthat the ‘white of the eye’ is made up anatom-ically of three structures: the conjunctiva, theepisclera and the sclera, each with its ownperilimbal vascular plexus. Inflammation ofeach layer of the covering of the eye resultsin vascular engorgement in the correspond-ing plexus. These can be differentiated to adegree by careful examination but alsopharmacologically. On examination, theconjunctival vascular plexus moves as theconjunctiva is gently moved while the deeperplexuses cannot be moved to this degree.Differentiating between episcleral and scleral
plexus involvement, however, calls for theapplication of the topical vasoconstrictorphenylephrine (see Appendix C). This willconstrict and thus visually obliterate anepiscleral plexus engorged through inflam-matory involvement but does not have thesame effect on the deeper scleral plexus.
A second key point in the differentiationof the red eye is that redness can include anumber of different clinical presentations.The redness may be a diffuse feature or oneassociated either with numerous smallblood vessels or a few engorged vessels.Each of these different rednesses can beassociated with a different diagnosis. A mildoverall redness normally indicates conjunc-tivitis, while a deeper more ‘angry’ red closeto the limbus is typical of ciliary flush, oftenassociated with uveitis. Deeply engorgedepiscleral vessels against a generally whitescleral background more often indicatesglaucoma.
The most important feature to note incoming to a diagnosis does not, however,concern the redness itself but rather other signsin the eye. The eye with conjunctivitis is oftenin other respects unremarkable. A causativefeature may be an eyelid abnormality such asentropion, ectopic cilium or distichiasis. Anassociated ocular sign in lymphocytic/plasma-cytic conjunctivitis may be corneal involvementwith chronic superficial keratitis (pannus).Similarly, the bulbar surface of the nictitatingmembrane may be involved in follicularconjunctivitis (plasmoma) and indeed the
Chapter 2
Commonly presented conditions – aproblem-oriented approach

Commonly presented conditions – a problem-oriented approach 13
Table 2.1 Differential diagnosis of the red eye
Feature Acute conjunctivitis Acute uveitis Acute glaucoma
Pain
Vision
Discharge
Blood vessels
Cornea
Aqueous
Iris
Pupil
Intraocularpressure
Lens
Posteriorsegment
Painfree to mild irritation
Unaffected except insystemic disease such asdistemper where theblindness is central ratherthan ocular
Moderate to copious andmay be serous, mucoid orpurulent
Conjunctival hyperaemiawith mobile vessels oftenassociated withoedematous inflamedconjunctiva. Note that lidand globe conjunctivae areboth affected
Clear unless keratitis isalso occurring
Clear
Unaffected
Unaffected
Unaffected
Unaffected
Unaffected except insystemic diseases such asdistemper
Can be extremely severe
Often severe impairment toprofound blindness
Generally confined tolacrimation because of painand increased blinking
Episcleral vesselengorgement and congestionwith stasis hyperaemia
A classically steamy orground-glass diffuse cornealoedema
Clear
Usually of normalappearance but possibly ashallow anterior chamber
Dilated and fixed
Increased
May be in situ, subluxatedor luxated secondary toglobe enlargement inbuphthalmos
Often not visible but retinalvascular attenuation or opticnerve cupping may occur
Mild to severe pain
Slight impairment withmiosis through to blindnesscaused by retinaldetachment
Generally confined tolacrimation because ofpainful and increasedblinking
Limbal flush and diffuseredness in episcleral vesselsdeeper than those of theconjunctiva. Note that thebulbar vessels are involvedwhile those of the lid arenormal
Varying from clear throughbeing affected with keraticprecipitates to being franklyoedematous
Affected with cells and fibringiving flare, hypopyon orhyphaema
Muddy, thickened or darkwith indistinct surfacefeatures and ofteniridolenticular adhesions(synechiae)
Small (miotic) irregular orfixed with a sluggishresponse to light
Decreased because of ciliarybody involvement
May be involved withpigment deposition orsynechiae
Hyalitis, pars planitis,chorioretinitis or opticneuritis may occur inpanuveitis
Differential diagnosis of the red eye
• Conjunctivitis Note involvement of palpebral and bulbar conjunctiva• Uveitis Note generalized globe redness often increasing at limbus (ciliary flush); note
other ocular signs – keratic precipitates, hypopyon, miosis, posterior synechiae,also pain and photophobia in acute cases
• Glaucoma Congestion/injection of episcleral vessels; other ocular signs – blindness, pain• Episcleritis Deeper vascular involvement with swelling at appropriate level
or scleritis
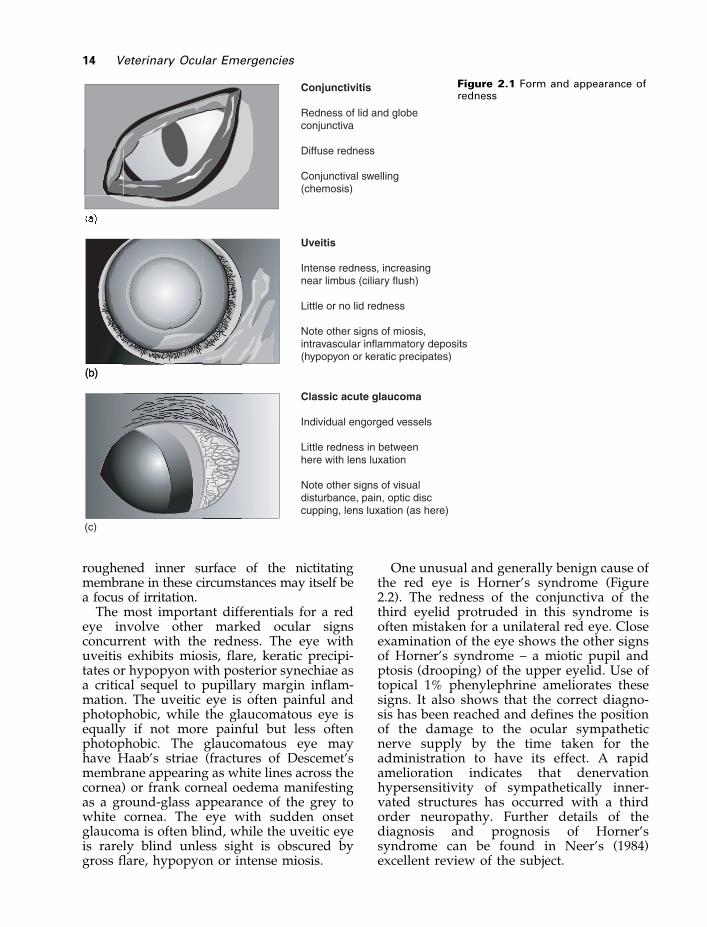
roughened inner surface of the nictitatingmembrane in these circumstances may itself bea focus of irritation.
The most important differentials for a redeye involve other marked ocular signsconcurrent with the redness. The eye withuveitis exhibits miosis, flare, keratic precipi-tates or hypopyon with posterior synechiae asa critical sequel to pupillary margin inflam-mation. The uveitic eye is often painful andphotophobic, while the glaucomatous eye isequally if not more painful but less oftenphotophobic. The glaucomatous eye mayhave Haab’s striae (fractures of Descemet’smembrane appearing as white lines across thecornea) or frank corneal oedema manifestingas a ground-glass appearance of the grey towhite cornea. The eye with sudden onsetglaucoma is often blind, while the uveitic eyeis rarely blind unless sight is obscured bygross flare, hypopyon or intense miosis.
One unusual and generally benign cause ofthe red eye is Horner’s syndrome (Figure2.2). The redness of the conjunctiva of thethird eyelid protruded in this syndrome isoften mistaken for a unilateral red eye. Closeexamination of the eye shows the other signsof Horner’s syndrome – a miotic pupil andptosis (drooping) of the upper eyelid. Use oftopical 1% phenylephrine ameliorates thesesigns. It also shows that the correct diagno-sis has been reached and defines the positionof the damage to the ocular sympatheticnerve supply by the time taken for theadministration to have its effect. A rapidamelioration indicates that denervationhypersensitivity of sympathetically inner-vated structures has occurred with a thirdorder neuropathy. Further details of thediagnosis and prognosis of Horner’ssyndrome can be found in Neer’s (1984)excellent review of the subject.
14 Veterinary Ocular Emergencies
Figure 2.1 Form and appearance ofredness

2.2 The painful eye
The spectrum of what we might call ocularirritation ranges from the mild but chronicdiscomfort caused by an ectopic cilium to therapid onset severe pain of acute glaucoma.Here we will consider first the acutely painfuleye, since these are the emergency situations,before discussing briefly conditions withchronic ocular discomfort. To some extentthere is an overlap in presentation in themiddle of the nociceptive spectrum.
The acutely painful eye may be the resultof a traumatic episode with tissue disruptionby external injury, or of two conditions inwhich ocular damage is the result of internalinjurious mechanisms: uveitis and glaucoma.Diagnosis of these latter two conditions
relies on evaluation of ocular signs onophthalmoscopy. Their differential diagnosispresented above.
Commonly presented conditions – a problem-oriented approach 15
Figure 2.2 Other causes of ocularredness
Mild irritation Severe pain
Some blepharospasm Lid closureIncreased lacrimation Substantial lacrimation
Distichia Retained foreign bodyEctopic cilia Orbital cellititis
Trichiasis Glaucoma
Box 2.1 Ocular pain

Understanding the origin of the pain isimportant for its relief. If it stems from ciliarymuscle spasm, as in uveitis, then paralysis ofthis muscle will reduce pain. If it stems froma defective tear film exposing corneal nerveendings to drying effects then tear replace-ment is required. However, the origin of painin ocular disease is not in all cases completelyunderstood. Where does the photophobia inuveitis originate, especially as it can beameliorated by the use of topical non-steroidal anti-inflammatories in many cases?And where does the acute pain in glaucomaoriginate and why do rabbits not seem to beat all concerned by it? There are as manyquestions left to answer in ophthalmology asthere are satisfactorily solved!
Ocular trauma can result in external and/orinternal tissue disruption and widely differingdegrees of pain. The pain accompanyingcorneal injury can too easily be underestimated(although anyone wearing contact lensesknows the quite severe pain of an apparentlyminor ocular surface abrasion). There seems tobe quite a range of response to corneal ulcera-tion between individual animals: some with adeep ulcer will appear to feel little discomfortwhile others with only a mild surface abrasionwill exhibit marked blepharospasm andlacrimation suggesting a considerable nocicep-tive response. The anatomy and physiology ofcorneal nociception is discussed below Thereason for this difference in response maypossibly be individual variation in degree ofcorneal innervation between animals; or morelikely differences in individual tolerance ofpainful stimuli; or conceivably because super-ficial ocular surface damage massively stimu-lates trigeminal pain receptors while deeperstromal injury actually exposes fewer pain-fibre endings.
The same variation can be seen in glaucoma.Some animals with early rises in ocularpressure have exceptionally painful eyes whileothers with catastrophic rises in pressureaccompanied by buphthalmos seem not to
suffer pain although they are irreversiblyblind. This may relate to differences in intra-ocular innervation or in central perception ofpain but is also likely to be linked with degen-eration of pain fibres once intra-ocularpressure has been high for some time.
The differential diagnosis of less severeocular discomfort centres mostly aroundcauses of physical irritation (see Box 2.1).Ocular foreign bodies are an obvious potentialcause of irritation which may be mild orsevere. These may be readily visible but oftenare hidden from immediate view in theconjunctival fornix or behind the nictitatingmembrane. Local anaesthesia with topicalamethocaine drops (or other local anaesthetics:see Appendix C) is necessary for adequateinvestigation while in some cases generalanaesthesia may be essential. Irritative focimay be integral to ocular structures ratherthan from an external agency such as a foreignbody. Ectopic cilia, distichial lashes or hairfrom surrounding skin (trichiasis) may beresponsible for considerable ocular irritation.Investigation of these lashes again oftenrequires local anaesthesia. Magnification isoften necessary to diagnose distichiasis andalmost always required to localize ectopic cilia.
Distichial lashes arise from the meibomiangland orifices. Ectopic cilia often arise frommeibomian glands but through the conjunc-tiva, or have distinct hair follicles which mayoccur at any point in the palpebral tissue. Thisdifference is reflected in the treatmenttechniques for these cilia. Distichia may simplybe plucked with forceps. In some cases ownersare happy to perform this from time to time.While this may seem optimal to some clients,distichia plucked may recur rapidly. Becausenew distichia can be shorter and more irritantsometimes such plucking can increase, ratherthan eliminate, irritation. Distichia can beremoved by electrolysis, by cryosurgicalablation or by sharp knife surgery (Lawson1973, Chambers and Slatter 1984, Wolfley1987). Electrolysis aims to deal lash by lashwith the distichia while cryosurgery on thelids seeks to destroy the meibomian glandsfrom which the lashes originate. Both of thesetechniques can cause considerable palpebralinflammation and presurgical medication withnon-steroidal anti-inflammatory agents isadvised. Some veterinary ophthalmologistsapply a cold/ice pack to the eyelids after
16 Veterinary Ocular Emergencies
Differential diagnosis of the painful eye
• The difference between ocular irritation(distichia, ectopic cilia, trichiasis) anddeeper pain (uveitis, glaucoma, globepenetration, foreign body)

cryosurgery has been performed and leave thepack until the animal wakes up. Sharp-knifesurgery aims to remove the meibomian glandseats of the lashes and thus avoids incisions inthe lid. In the past lid margin resection wasadvocated to remove distichia, but the risk oflid scarring is too great to warrant use of thattechnique today.
Treatment of ectopic cilia requires sharp-knife resection of the area from which thecilia arise. Ectopic cilia often originatetogether and during surgery a number ofhairs may be found together in the thickeningon the palpebral conjunctiva.
2.3 The white eye
Normally the term white eye is used todifferentiate a quiet or disease-free eye froma red eye, as discussed above, but here we
use the term to denote a pathological whiteappearance. The key here is determination ofwhere the white opacity is within the eye. Awhite cornea or an opaque aqueous humourprevent visualization of intra-ocular struc-tures beneath it, while iris detail can still beseen around a white lens opacity. The differ-entiation of an opaque cornea or aqueous ismore difficult. A slit beam allows theanterior and posterior faces of the cornea tobe identified in the latter case while showingthe opacity to be intracorneal in the former.In any case corneal opacification is far morecommon than is a white aqueous.
A white opacity in front of the lens can onlybe one of four things
• Cellular invasion• Oedema• Scar tissue• Lipid
Commonly presented conditions – a problem-oriented approach 17
Figure 2.3 The white eye

All four can occur in the cornea while in theaqueous humour only cellular infiltration andlipid involvement are seen (Figure 2.3).Corneal oedema is a sign of what one mightconsider a true emergency situation,glaucoma. Other white corneal changes occurmostly in chronic lesions which cannot beconsidered to be emergencies. Cellular infil-tration of the cornea is normally accompaniedby vascular invasion, giving a pink hue asseen in chronic superficial keratitis. Cornealoedema, however, gives a classical groundglass appearance through which, when mild,some intra-ocular detail can be seen using abright light source such as a Finhoff transillu-minator. The differential diagnosis of condi-tions associated with corneal oedema includes
• Glaucoma• Endothelial dystrophy• Endothelitis associated with uveitis often
after canine adenovirus infection• Endothelial trauma
The appearance of corneal lipid depositiondepends on the type of lipid or lipoproteininvolved. Cholesterol, for instance, formscharacteristic crystals while low densitylipoprotein gives a finer lipid infiltrate. Scartissue is readily recognizable as such, havinga heterogeneous white-grey appearance.Blood vessels are often seen in associationwith corneal scar tissue.
Cellular infiltration of the aqueousproduces a flare which can properly beappreciated only by making use of theTyndall effect, and thus is not a truly whiteeye (Figure 2.4). Oedema and scar tissue donot occur in the aqueous, leaving lipid andfibrin deposition as the only reasons for adense white aqueous humour. Lipid-ladenaqueous does indeed give a completely white
eye as a very startling diagnostic feature. Thiscould be considered an emergency, given thatit disturbs vision and because it can followuveitis where an abnormally high circulatinglipid also occurs. Fibrin in the anteriorchamber gives a grey or yellow colour to theaqueous rather than white but signals anemergency in some cases, as it is associatedwith uveitis. In the vitreous a total retinaldetachment could be confused with a whiteeye, and a posterior chamber tumour mayproduce a white pupil or leucocoria.
With regard to the lens, cataract is clearly asignificant cause of white opacity, but the onlycataractous change which could be classed asan emergency is the diabetic cataract. This isan emergency both because it can occurrapidly and be a cause for sudden change inthe appearance of the ocular media and visualdeterioration, and also because it is a manifes-tation of a serious systemic endocrine disease.
2.4 The suddenly blind eye
The suddenly blind eye is clearly an emergencyfirst because visual compromise is a cause forconcern even if only temporary. Secondly,sudden blindness is often the prelude topermanent blindness.
Sudden blindness is caused through one offour mechanisms.
1. The first mechanism is opacification of theocular media. The only two conditions inwhich media opacification occurs withrapid onset are lipid-laden aqueous anddiabetic cataract (as covered above underthe white eye) or vitreal or retinal haemor-rhage.
2. The second mechanism is disruption ofretinal function. Rapid deterioration in
18 Veterinary Ocular Emergencies
Differential diagnosis of the blue/white eye
• Where is the opacity? – cornea, aqueous, lens?• What is the appearance of the opacity? – dense crystalline, ground glass, etc.?• How widespread is the opacity? – across whole cornea, focal, only in pupil?
• Cornea Corneal lipidosis (dense white, diffuse or micro crystalline)Corneal scar (diffuse, often off-white striate appearance)
• Aqueous Lipid-laden aqueous (diffuse throughout aqueous)Hypopyon (ventrally often with a horizontal margin dorsally)
• Lens Cataract (only seen within pupil, behind lens)

retinal activity occurs either as a conse-quence of complete retinal detachment orfailure of retinal electrical function insudden acquired retinal degeneration.Retinal detachment may occur as theresult of posterior uveitis, hypertension ortrauma. It may be related to inheriteddisease such as retinal dysplasia or Collieeye anomaly. The syndrome of suddenacquired retinal degeneration (SARD)gives no observable retinal changes at thetime of first visual loss, but electroretino-graphy shows no measurable retinalelectrical activity. Later indicators ofretinal degeneration such as increasedtapetal reflectivity occur, but as these arenot present early in the disease they arenot helpful diagnostic signs in theemergency situation.
3. The third mechanism for sudden loss ofvision is optic nerve dysfunction.Glaucoma and optic neuritis are the twoconditions most commonly giving rise todysfunction although tumours of the opticnerve or surrounding structures can onoccasion cause loss of function.
Although we associate glaucoma withocular disease at the iridocorneal anglethe mechanism of visual loss relates todamage at the optic nerve head. Cuppingof the optic nerve head is a visiblechange, but before this happens pressurenecrosis of the nerve fibres coursing overthe edge of the cribriform plate to enter
the optic nerve itself accounts for visualloss.
Optic neuritis may be visible at thepapilla by fundoscopy, with a swollenoptic nerve head with or without peripap-illary haemorrhages. On rare occasions theinflammatory process occurs not at theoptic nerve head but in the nerve at theretrobulbar level. Diagnosis of retrobulbaroptic neuritis is generally by exclusion butultrasonographic or magnetic resonanceimaging (MRI) or computerized tomogra-phy (CT) can show a swollen retrobulbaroptic nerve, and electroretinographyreveals normal retinal activity.
Tumours of the optic nerve itself, suchas optic nerve meningiomas, can causevisual disturbance as can adjacent massespressing on the optic nerve. Of thesepituitary tumours are classical causes ofbilateral visual disturbance throughpressure on the optic chiasm. Such caseshighlight the necessity for a full clinicalwork up. They manifest also in endocrineabnormalities such as diabetes insipidus,and diagnosis can be aided by tests suchas the ACTH stimulation test.
4. The fourth mechanism causing suddenvisual loss is central blindness. Here allparameters of ocular function are normaland the diagnosis rests on electrodiagnosiswith abnormalities shown in visuallyevoked potentials by electroencephalogra-phy. Magnetic resonance or CT imaging
Commonly presented conditions – a problem-oriented approach 19
Figure 2.4 As happens (or rather,used to happen) in a smoke-filledcinema, the light lens highlights theparticles in the gas phase, or in theaqueous the liquid phase. This is thekey diagnostic test to evaluate flarein anterior uveitis

may reveal an intracranial mass or adiagnosis of generalized disease such asgranulomatous meningio-encephalitis maybe made. Such a condition may alsoaccount for some cases of optic neuritis.
2.5 Ocular lesions in systemicdisease
Several of the diseases mentioned above,from diabetic cataract to granulomatous
meningo-encephalitis (GME), are ocularmanifestations of a systemic condition (Table2.2). The prevalence of ocular abnormality asa sign of systemic disease shows the impor-tance of a thorough general work up for allanimals presenting with ocular disease. Thefact that the ocular signs are the reason foremergency presentation should not detractfrom a thorough clinical examination of thewhole animal as soon as possible. Thesystemic diseases producing ocular signs areshown in Table 2.3.
20 Veterinary Ocular Emergencies
Box 2.2 The suddenly blind eye
Ophthalmicexam
Normal eyeElectroretinogram
Abnormal eye
Opaque media
Glaucoma
Retinal detachment
Optic nerve pathology
SARD
Retrobulbar optic neuritis(confirm by ultrasound)
Central blindness(perform full neurological work-up)
+ tive result
– tive result
Papilloedema
Optic neuritis
Differential diagnosis of the suddenly blind eye
• Opacification of media Lipid laden aqueousDiabetic cataractIntraocular haemorrhage (aqueous or vitreous)
• Disruption of retinal function Retinal detachmentSudden Acquired Retinal Degeneration (SARD)
• Optic nerve dysfunction Optic neuritisGlaucomatous optic neuropathyOptic nerve compression
MeningiomaPituitary tumour at the optic chiasm
• Central blindness Other intracranial space occupying lesion? raising intracranial pressure? causing compression of optic radiation

Commonly presented conditions – a problem-oriented approach 21
Table 2.2 Ocular lesions in systemic disease (provided by T.F. Evans)
Disease Species Ocular change Aetiology
Vitamin A deficiency
Hyperadrenocorticism
Infectious bovinerhinotracheitis (IBR)
Diabetes mellitus
Hyperthyroidism
Chr/acute renal failure
Toxoplasmosis
Canine distemper
Feline herpes virus
Chlamydiosis
Equine viral arteritis
Equine herpes virus
Feline infectiousperitonitis
Leptospirosis
Thiamine deficiency
Listeriosis
Bovine virus diarrhoea(BVD)
Liver disease
Lymphosarcoma
GME
Erlichiosis
Taurine deficiency
Eq, bo, ov
Ca
Bo
Ca, fe
Fe
Ca, fe
Fe, ca
Ca, ferret
Fe
Fe, avian
Eq
Eq
Fe
Eq
Fe, eq, bo, ov
Bo, ov, su
Bo
Ca, fe, eq
Ca, fe
Ca
Ca
Fe
Night blindness, poor PLRs
Corneal ulcers, KCS, hypertensiveretinopathy, SARD
Conjunctivitis, blepharaospasm,cornea generally clear
Cataract
Retinal detachment, perivascularcuffing, tortuous retinal vessels
Retinal detachment, perivascularcuffing, tortuous retinal vessels
Anterior uveitis, chorioretinitis
Conjunctivitis, KCS, chorioretinitis,brown retinal scars
Conjunctivitis, chemosis, dentritickeratitis
Conjunctivitis, chemosis
Corneal opacity, uveitis,conjunctivitis
Conjunctivitis, dendritic keratitis
Uveitis
Anterior uveitis, equine recurrentuveitis, secondary cataracts
Blindness, ataxia
Chorioretinitis, blindness (unilateralor bilateral), KCS
Cataract, vitreal opacities, opticnerve atrophy, retinal dysplasia
Scleral icterus
Uveitis, retinal haemorrhages,secondary glaucoma
Uveitis, retinal haemorrhages, opticneuritis
Central retinal atrophy(hyperreflectivity in area centralis)
Less production ofrhodopsin
Hypercortisolaemia
Osmotic (sorbitol,glucose and aldosereductase)
Hypertension
Hypertension
Toxoplasma gonditachyzoites
Canine distemper virus
Feline herpes virus 1
Chlamydia psittaci
EVA-virus
EHV-1
Feline coronavirus
Leptospira interrogans
Listeria monocytogenesbacteraemia
Hyperbilirubinaemia
Neoplasia, metastasis,phagocytosis
Ehrlichia canis
References are available in Gelatt (1999) and Lavach (1990).

22 Veterinary Ocular Emergencies
Table 2.3 Systemic diseases with ocular associations having emergency implications
Canine distemper ConjunctivitisKeratoconjunctivitis siccaChorioretinitis
Canine adenoviral hepatitis Corneal oedema – ‘blue eye’Anterior uveitis – endothelitis
Feline dysautonomia Dilated unresponsive pupilsFeline herpes virus Conjunctivitis, keratoconjunctivitis
Corneal ulcerationFeline chlamydial infection Conjunctivitis, chemosisFeline FIV infection UveitisFeline FIP infection Anterior uveitisFeline Felv infection Anterior uveitis, uveal lymphosarcomaFeline chlamydial infection Conjunctivitis, chemosisRickettsial infections Anterior uveitisBacterial toxaemia Anterior uveitis
ChorioretinitisRickettsial and fungal disease Anterior uveitis
Retinal haemorrhagesToxoplasmosis Uveitis, scleritisLeishmaniasis Anterior uveitis, keratitis, scleritisDirofilariasis Anterior chamber worms, corneal oedemaToxocariasis ChorioretinitisDiabetes mellitus Rapidly developing cataract
Diabetic retinopathy – retinal haemorrhagesHypocalcaemia Punctate and linear cataractsHyperadrenocorticism Corneal ulceration, corneal lipidosisHypothyroidism Corneal lipidosis, keratoconjunctivitis siccaLysozomal storage diseases Faint corneal lipidosis
Retinal depositsHypertension Retinal haemorrhages
Retinal detachmentHyperlipidaemia Corneal lipidosis, lipid keratopathy
Lipaemia retinalisAnaemia Retinal haemorrhagesThrombocytopaenia Retinal haemorrhagesHyperviscocity syndrome Dilated tortous vessels
Retinal haemorrhagesPapilloedema
Vogt-koyanagi-harada syndrome Anterior uveitisRPE and choroidal depigmentation
Lymphosarcoma Anterior or posterior uveitisRetinal haemorrhages
Intracranial neoplasia PapilloedemaBlindness

3.1 Lid laceration
Four key points should be taken into consid-eration when approaching the emergencycase of a lid laceration.
1. Are there other ocular injuries? In many,if not the majority, of cases penetrating
globe injury also occurs and, given thehaemorrhage and swelling accompanyinglid trauma, such lacerations may be diffi-cult to evaluate. However critical weconsider lid injuries, a concurrent globepenetration is considerably more import-ant from the viewpoint of potential long-term visual handicap. Missing such aninjury is to be avoided at all costs.
2. When should surgery be undertaken? Aswe have said, there is often considerable lidswelling and haemorrhage associated withlid injury. As veterinarians we are often
Chapter 3
Adnexa and orbit
Prognostic indicators in lid lacerations
1. The profuse vascularization of the lidensures that even substantial lacerationsheal well
2. The key factor in ensuring adequatehealing is adequate apposition of the lidmargin to avoid long-term ocular surfaceirritation
3. Extensive damage and loss of tissuerequiring reconstructive surgery
Emergency management of lid lacerations
1. Perform full ophthalmic examinationunder sedation so as not to miss moresevere globe trauma
2. If a very recent injury (less than 6 hours)repair immediately ensuring good lidmargin apposition
3. If longer than 6 hours since injurybandage and give systemic NSAID,delaying repair until lid swelling hassubsided
4. Always ensure that further self-traumacannot occur by using Elizabethan collar,together with adequate analgesia
Eyelid injury in blunt trauma
1. Haemorrhage2. Oedema3. Important factor to look beyond the
eyelid lesions to assess globe integrity,intra-ocular normality
4. The importance of shock-wave damageto tissue boundaries in the eye
Eyelid injury in sharp trauma
1. Laceration2. Haemorrhage3. Oedema4. Critical: how much the tissue swelling
compromises accurate re-apposition oflid edges?
5. If lids are well vascularized, tissues canbe left protected, lubricated and clean forseveral days until swelling has reduced

tempted in such a situation to rush in withan immediate repair. This may oftencompromise our ability to perform anoptimal repair. Assessing whether tissue isviable can be difficult in such circum-stances, and ensuring that the lid margin isperfectly aligned may be impossible, giventhe degree of tissue swelling encountered.It may, in many cases, be preferable toprotect the ocular surface with ointment, toprovide a compress with a moistenedbandage over the peri-orbital area and totreat with systemic non-steroidal anti-inflammatory agents for several daysbefore attempting primary repair. Thisshould be done only after thorough cleans-ing of the area. Systemic and local antibi-otic therapy should be ensured. If thenasolacrimal system is damaged immedi-ate primary repair may be deemed prefer-able or a nasolacrimal cannula can besutured in place until repair is attempted.Once swelling has subsided and tissueviability can better be assessed a primaryrepair can be undertaken.
3. What tissue should be retained after asubstantial injury and what removed? A
strong temptation in lid repair is topreserve as much tissue as possible evenwhere considerable damage has occurred.This may be counterproductive, as non-viable lid tissue will have to be removedin a secondary repair and subsequentproblems of trichiasis or corneal exposuremay occur. A preferable option is toremove substantially damaged tissue atprimary repair and provide replacementtissue through skin rotation or bucket-handle flaps.
4. Finally, and perhaps most importantly,the repair of the lid margin in as nearperfect apposition as possible is vital. Anarea of defective lid edge with associatedtrichiasis or the formation of a ‘step’ in themargin can give continual cornealproblems and ocular surface irritation.
The correct placement of the first suture atthe eyelid margin in a lid repair is thus criticalin ensuring a successful result. A simple inter-rupted suture at the lid margin might beconsidered sufficient but in fact causes anunstable tissue union without adequatesupport. What is required is a cruciate (or
24 Veterinary Ocular Emergencies
Remove non-viable tissue
Perform reconstruction
Remove vascularity of lids – facilitates reconstruction
Are there more serious globe injuries? Full examination required
Is immediate repair possible?
Yes
No
Proceed
Give immediate treatment – suture nasolacrimal cannula in placeHow much lid can be preserved?
Box 3.1 Lid trauma

figure of 8) suture as shown in Figure 3.1.Starting at the external surface of the lid about3 mm from the margin the suture is passedthrough the lid tissue and exits the lid at themargin. Re-entering the lid on the other sideof the incision the suture again passes throughthe lid tissue to exit opposite the first sutureentry-point. The suture thus firmly opposesthe two parts of the lid both at the margin andat a point away from the lid edge. Single inter-rupted sutures of the lid skin oppose the edgesof the lid incision, but beforehand sutures inthe conjunctiva should be placed with theirknots buried in the tissue of the conjunctiva.
A number of surgical options are availablefor long-term repair of substantial lid injurywhere tissue defects remain. These techniquesare not really the subject for an emergencytextbook but line diagrams illustrating thepossible methods to remedy lid injuries withdefects of upper and lower lids are given here(Figures 3.2–3.5).
3.2 Conjunctivitis
It might be objected that conjunctivitis cannotbe considered an emergency: it is normally achronic disease with an insidious onset, notcausing overt pain or visual loss. Yet as adifferential diagnosis for the red eye, and as acondition occasionally resulting in alarmingchemosis and ocular discharge, it is right to
include it here. Conjunctivitis can be caused byphysical factors such as distichia or ectopiccilia (Helper and Magrane 1970); or entropionand trichiasis (Miller and Albert 1988); through
Adnexa and orbit 25
Figure 3.1 Suturing the lid margin
Figure 3.2 Reconstruction of lower lid from upper-lid with a skin flap
Figure 3.3 Pavletic lip-to-lid technique toreconstruct lower lid

immunological pathways that occur in follicu-lar conjunctivitis in dogs; or from infectiousagents such as herpes virus, Chlamydia orMycoplasma in cats (Nasisse et al. 1993). Assuch, conjunctivitis warrants a close ocularexamination. In particular the bulbar aspect ofthe third eyelid should be examined. Oftenconjunctivitis persists even when the incitingcause of ocular irritation has been removed,because the lymphoid follicles which haveformed on the bulbar surface of the nictitating
membrane in response to chronic irritation arethemselves a focus for ocular irritation. Theyshould be removed by physical abrasion with
26 Veterinary Ocular Emergencies
Figure 3.4 Reconstruction of upperlid defect from lower lid (Mustardétechnique)
Figure 3.5 Bucket-handletechniques for lid defect
Differential diagnosis in conjunctivalhaemorrhage
• Ocular trauma• Coagulopathy• Systemic infections such as Rickettsia
rickettsiae

a cotton-tipped swab after topical anaesthesia,or in severe or refractory cases by the applica-tion of phenol, again with a cotton-tippedapplicator (Dolowy 1987).
Conjunctivitis should never be treatedinitially with topical antibiotic with steroidmedications. For one thing such polyphar-macy reveals nothing about the possiblecausative agent even if the treatment has thedesired effect. More importantly, in the cat, ifthe conjunctivitis is caused by ocular felineherpes virus infection, the steroid often hasthe effect of converting a mild harmlessepithelial viral infection into a chronic sight-threatening corneal stromal infection withinflammation, neovascularization and refrac-tory corneal oedema.
Feline keratoconjunctivitis may be causedby chlamydial or mycoplasmal as well asherpetic infection. Thus the use of topicaltetracycline medication will have the effect ofcontrolling the former two agents or, in theevent of treatment failure, strongly suggest-ing viral infection to be the cause. In that caseantiviral treatment may be considered to bethe preferable course of action with diagnosisbeing achieved if such treatment is effective.A conjunctival scraping may be submitted forviral culture: for an immunofluorescentantibody (IFA) test to investigate the presence
of Chlamydia and/or herpes virus, or forpolymerase chain reaction (PCR) testing. Inpast years diagnosis of herpes viral infectionwas difficult and amelioration of signs ontreatment was presumed to confirm diagno-sis. Today with the availability of polymerasechain reaction-based diagnostic tests we canbe more sure of a diagnosis of herpetic aetiol-ogy in feline keratoconjunctivitis. In the UKviral culture is most often used for diagnosis,but while the specificity here is high the sensi-tivity is poor with many false negativeresults. PCR testing is only available in theUSA, while immunofluorescence is under-taken in Europe and is used by the twoauthors of this text residing on the easternside of the Atlantic.
Treatment of FHV-1-related corneal diseasecan involve topical antiviral drops: idoxyri-dine (Herplex or Stroxil in USA) or trifluo-rothymidine (Viropticin USA or MoorfieldsEye Hospital formulation in UK) drops fourtimes daily. Topical interferon alpha(3000 IU/ml) has been used as has oral inter-feron (again 3000 IU/ml), 1 ml daily for sevendays then alternating weeks. Other support-ive but not curative treatment protocolsinclude sytemic L-lysine (200–250 mg dailyfor the cat), and tear substitutes if tearproduction is reduced (Quinn 2000).
Adnexa and orbit 27
IFA(immunofluorescenceantibody technique)
PCR(polymerase chain reaction)
Culture andidentification ofcytopathic effects
Conjunctivitis
What is the cause?
Treat with aureomycin/tetracycline Identify possible virus
Success Failure
Chlamydia/Mycoplasma was the cause
Look for another cause
Local irritation
Expensive
method
Cheap
method
Box 3.2 Conjunctivitis
As the above-mentioned antiviral drugs arenot widely available outside the USA, one ofthe authors (DLW) has successfully used apreparation of acyclovir (Zoviraxophthalmic), which is a licensed humanophthalmic ointment, for treatment of felineherpes virus keratitis even though the onlypaper on this subject showed poor antiviraleffects in vitro (Nasisse et al. 1989). The resultshave so far been promising, but it is advisableto notify the owner that the drug is notlicensed for veterinary use.
3.3 Dacryocystitis
An eye with severe frank purulent dischargemay have a conjunctivitis but often the infec-tion is related to a persistent infectious focus,either in the form of a foreign body or asdacryocystitis, where the infection centres inthe nasolacrimal duct. In either of these casesexamination under anaesthesia is often neces-sary: a full investigation of the depths of theconjunctival fornices should be undertaken tolocate a foreign body such as a grass seed andthe nasolacrimal duct should be flushed toassess the presence of dacryocystitis. In eithercase topical antibiosis should be provided butwith dacryocystitis systemic medication isoften needed and bacteriological culture andsensitivity are worthwhile to ensure that thecorrect drug is being used.
3.4 Conjunctival foreign body
The presentation of a non-penetratingconjunctival foreign body can be highlyvaried. Since foreign material can range froma grass awn to a piece of grit, signs occupythe whole spectrum from mild discomfortand purulent ocular discharge with theformer to acute pain and chemosis with thelatter. The key problem is finding such aforeign body in an eye where chemosis andadnexal swelling may easily hide the object.This is compounded by the tendency of manysuch foreign bodies to work their way intothe fornix or to the very base of the thirdeyelid. This is especially true of grass awns.
In many cases the only way to investigatean eye where the possibility of a conjunctivalforeign body is high is to examine the entirety
of the conjunctival sac under general anaes-thesia. Particular attention should be paid tothe space behind the third eyelid and the fullextent of the fornix around 360° of the globe.Copious irrigation will both clear any muco-purulent discharge which would otherwiseobscure the view and also flush out smallforeign bodies which might otherwise bemissed.
3.5 Acute keratoconjunctivitissicca
While keratoconjunctivitis sicca (KCS) mightwell be thought of as a chronic conditionwhich would never be presented as anemergency, a small number of dogs withsudden-onset total failure of lacrimationpresent as acutely painful eyes with orwithout corneal ulceration. A considerablenumber of these cases, in the authors’ experi-ence, are the result of drug-induced KCS,mostly with salazopyrin use. Here theSchirmer tear test is zero and the wholeocular surface has a gritty appearance. Itwould appear, in our opinion, that thesehyperacute failures of tear production are sosevere because the conjunctiva has not hadthe opportunity to adjust its goblet-cellnumbers and production of mucus. Theclassic mucopurulent ocular discharge sofamiliar in more chronic KCS is not seen inthese cases, at least not in the first two tothree weeks after emergency presentation.They do not seem responsive to managementwith topical cyclosporine although one mightthink that they should as lacrimal glandtissue has not been destroyed through a long-standing immune-mediated destruction (asoccurs in the more chronic cases seen in theWest Highland White terrier and Cockerspaniel).
Other cases of acute KCS include traumaticdamage to the facial nerve or trigeminaldamage resulting in reduced/absent cornealsensation and therefore reduced tear-produc-tion. In the former case there is often a drynose, suggestive of denervation damageaffecting the nasal glands which producemoisture at the external nares. In such neuro-logical cases topical cyclosporine is less useful.
Even in cases of chronic dry eye the animalmay be brought in as an emergency if a
28 Veterinary Ocular Emergencies

corneal ulcer supervenes. As will bediscussed below one key feature in the inves-tigation of a corneal ulcer is the determinationof its cause: here a Schirmer tear test is justabout obligatory to exclude KCS as a cause ofthe ulcer.
3.6 Exophthalmos
3.6.1 Globe protrusion or exophthalmos
This may be a gradually worsening disease ormay be a sudden-onset emergency. It maysignal a retrobulbar infection which can berelatively easily diagnosed and cured, or aretrobulbar neoplasm difficult to diagnosewithout recourse to expensive imagingtechniques and often impossible to cure.Because of this dichotomy; the long-termdamage to the eye from prolonged exposure;and, for the owner, the unpleasant appear-ance of the protruding globe it is important tomanage these cases correctly from the start.
3.6.2 Orbital cellulitis and retrobulbarinfection
The former may present as an acutely painfuleye with a profuse mucopurulent oculardischarge or, if the infection has organized intoan abscess, there may be the exophthalmosthat occurs with a retrobulbar space-occupying
mass, as discussed in section 3.6.3 below.Conjunctival hyperaemia is seen concurrentwith the exophthalmos as may a serous or amucopurulent discharge.
Retrobulbar infection often presents asexophthalmos associated with peri-apicaldental disease – a tooth-root abscess mayerupt as a open lesion on the skin or as aclosed infected mass in the orbit producingglobe protrusion.
The key feature in the diagnosis of suchinfective orbital disease is acute severe pain.Retropulsion of the globe is painful as isopening the mouth. This is important inassessment of the case as a fluctuant swellingmay be detected behind the last molar tooth.Animals may be febrile and show signs ofsystemic malaise but this is not invariable. Ahaemogram is likely to reveal a neutrophilia.
Investigation of the area behind the lastmolar tooth should include an incision in theoral mucosa and gentle introduction of aclosed haemostat into the orbit through thepterygoid muscle, followed by opening andwithdrawal of the haemaostat, thisobviously performed under general anaes-thesia (Figure 3.6). While the literaturewould have one believe that ‘purulentmaterial usually drains from the affectedarea’ (Speiss and Wallin-Håkanson 1999), in
Adnexa and orbit 29
Differential diagnosis in exophthalmos
Investigation should include• Full ocular examination (including
examination from above)• Investigation of ocular movements
(including forced retropulsion)• Full cranial examination including
opening mouth• Ocular and orbital ultrasound• Skull radiography and other imaging
techniques (CT/MRI)
Causes1. Retrobulbar mass
• Abscess (painful on opening mouth)• Tumour (not generally painful on
opening mouth)2. Retrobulbar fluid
• Oedema• Haemorrhage
Figure 3.6 Incision of the oral mucosa, gentleintroduction of a closed haemostat into the orbitthrough the pterygoid muscle followed by openingthe haemaostat and withdrawal while animal isanaesthetized. Note that here the endotracheal tubeand throat pack have been removed for sake ofclarity, but should normally be used in such cases

our experience this is often not the case. Wepropose that the anatomy of the retrobulbararea often traps purulent material in lacunaebut that drainage supported by aggressivesystemic antibiotic treatment is almostalways successful. Advancement of a bac-teriological swab into the retrobulbar spacecan give useful culture data and the preva-lence of anaerobes in a small series (DLW)supports the use of metronidazole togetherwith a prolonged course of cephalosporin inthese cases.
In rabbits and larger rodents such as thechinchilla the close apposition of the globe tothe posterior dental molar roots leads to arange of problems, from the persistentepiphora often seen in chinchillas with dentaldisease to the frank severe exophthalmosseen in rabbits infected with Pasteurella orStaphylococcus. Dealing with this can beproblematic since the extraction of infectedteeth is difficult and yet without eliminationof the focus of infection the condition cannotbe remedied.
3.6.3 Other orbital space occupyinglesions®
The gradually increasing exophthalmosoccurring with a retrobulbar space-occupyinglesion does not render it likely to bepresented as an emergency, but three featureshere are important.
1. It will not be painful, as would theinfected orbital cellulitis or retrobulbarabscess detailed above.
2. The exophthalmic globe should be differ-entiated from a hydrophthalmic, enlargedglobe. The position of the nictitatingmembrane is important here: an exoph-thalmic globe will be characterized by araised protuberant third eyelid while anenlarged globe, after severe glaucoma forinstance, will not (Figure 3.7a–d).
3. The position of the retrobulbar space-occupying lesion, whether within theextra-ocular muscle cone (intraconal) oroutside it (extraconal) substantially alters
30 Veterinary Ocular Emergencies
Figure 3.7 Differentiating exophthalmos. (a) Exophthalmos; (b) enlarged globe; (c) Intraconial disease; (d)extraconial disease

the appearance of the eye. Intraconaldisease leads to a staring appearance withsclera visible around the circumference ofthe cornea and, perhaps surprisingly, alack of nictitating membrane protrusion(Figure 3.7). Intraconal disease may occurwith an optic nerve tumour such as anintra-orbital menigioma but is more likelyto occur acutely as an extra-ocular myosi-tis (Ramsey et al. 1995, Ramsey and Fox1997). In cases of eosinophilic extra-ocularmyositis, leukocytosis and eosinophilia ina peripheral blood sample are seen andserum creatinine kinase levels are elevated.
Immunosuppressive doses of oral corticos-teroids are usually ameliorative althoughazothioprine may also be valuable for twoto three weeks at 1–2 mg/kg.
Other non-infectious space-occupyinglesions do not of course have to be neoplas-tic. Masticatory myositis causes severe exoph-thalmos but also obvious signs of limited jawmovement, pyrexia, malaise and anorexia.Salivary retention cysts and mucocoeles cancause of slowly progressing extraconal exoph-thalmos which on draining yields a tenaciousyellow fluid.
Adnexa and orbit 31

4.1 Blunt trauma to the globe
Emergencies involving the entire globe arealmost without exception traumatic. Penetrat-ing injuries may involve the cornea or thesclera and are dealt with below. Blunt trauma
to the globe might be considered less sight-threatening than penetrating injury but theshock waves that issue from severe blunttrauma can actually have more devastatingeffects than the localized injury resultingfrom penetrating trauma. A fracture of thebone surrounding the eye may similarlyinjure the globe and/or extra-ocular tissues.
In the same manner as an earthquakecauses widespread disruption, the shockwaves following blunt trauma have particu-larly catastrophic effects at boundariesbetween tissues with different physicalcharacteristics (Figure 4.1). This is particularlyseen at the iridocorneal angle where theconnective tissues of the cornea and sclerameet the delicate soft tissue and vascularstructures of the iris and ciliary body. Theshearing forces following the shock wavesresulting from a blunt traumatic episodecause irreversible tissue damage, separatingthe uveal structures from the connectivetissue of the globe. Similarly the reboundforces occurring at the posterior face of theglobe tear retina from choroid (or morecorrectly neurosensory retina from retinalpigment epithelium, given the potential spacewhich exists between the two layers of theembryological optic cup). Such shearingforces may also tear vascular structuresgiving retinal or choroidal haemorrhages orvitreal haemorrhage arising from damage tothe richly vascular ciliary body. Thus it canbe seen that while penetrating trauma mayitself cause significant local damage, blunt
Chapter 4
Globe
Emergency management of ocularcontusion
1. Perform full ophthalmic examination,noting that damage may be as severe aswith a penetratng injury
2. Perform fluorescein test to evaluate forsurface ulceration
3. Measure intra-ocular pressure and treataccordingly
4. Give systemic corticosteroids andantibiotics
5. Give topical steroid if no cornealulceration is present, otherwise givetopical NSAID ketorolac (Acular,Allergan) or flurbiprofen (Ocufen,Allergan)
6. Give topical atropine twice daily7. Hospitalize patient and evaluate eye
every 3–4 hours
Prognostic indicators in ocular contusion
1. Intra-ocular haemorrhage is a poorprognostic sign
2. Intra-ocular inflammation is to beexpected and can be ameliorated iftreated aggressively
3. Glaucoma similarly may occur and ismuch less easily controllable than uveitis

trauma often gives rise to irreversible damagethroughout the globe, even quite distant fromthe sight of blunt impact.
4.2. Globe prolapse
Perhaps the most acute ocular emergency,one for which treatment given within the first
few minutes after injury may be sight-preserving, is globe prolapse. This occurspredominantly in brachycephalic dogs inwhich globe exposure and a considerabledegree of lagophthalmos is a naturalphenomenon. The eyes are congenitally veryexophthalmic and a frightening action such asa over-exuberant restraint of the neck regionmay cause prolapse of the globe.
Lateral trauma to the globe (the sort result-ing from the animal’s head being trapped ina closing door for instance) can result in globeprolapse in any breed. The entire globe isprolapsed beyond the lid margins. Hereseveral pathological events occur (Figure 4.2).The optic nerve is obviously stretched, thispotentially causing permanent visual loss.Vascular supply to the globe is compromised,with massive peribulbar tissue swelling andpotentially disastrous effects on ocular health.Extra-ocular muscles may be damaged andavulsed from their globe origins, resulting inlong-term strabismus.
In the time that it takes for an animal to betransported to the surgery the immediatetrauma resulting from the prolapse will becompounded massively by the swellingoccurring in the next few minutes. It is vitaltherefore to urge the owner to attempt toreplace the globe behind the lids using adamp towel or piece of cotton wool placed onthe globe surface, with a quite considerabledegree of force exerted to replace the globe.As the inflammation is extensive, applicationof cold towels to the eye will reduce theswelling and act to prevent globe prolapse. In
Globe 33
Figure 4.1 Shock waves followingblunt trauma have particularlycatastrophic effects at boundariesbetween tissues with differentphysical characteristics
Emergency management of the prolapsedeye
1. Advise owner to attempt globereplacement in first minutes after injurywith damp cotton wool pad
2. Advise owner to cover ocular surfacewith damp cotton wool pad whilebringing to surgery
3. Administer shock dose of steroid i.v.(2 mg/kg)
4. Perform lateral canthotomy5. Replace globe using only limited force –
if more required enlarge canthotomy6. Apply topical atropine and appropriate
antibiotic (i.e. fusidic acid) ointment7. Suture lids closed and leave for 10 days
on systemic antibiotic and NSAID
Prognostic indicators in the prolapsed eye
1. Extra-ocular muscle avulsion andstrabismus gives a poor prognosis
2. Hyphaema with haemorrhage in theglobe gives a poor prognosis as itsuggests severe intra-ocular damage
3. The presence of a consensual light reflexis a good prognostic sign

34 Veterinary Ocular Emergencies
Figure 4.2 Pathological events in globe prolapse
Effects of prolapse
Stretching of Entrapment of veins Peri-ocular oedema andretrobulbar tissue draining globe swelling
Optic nerve damage Damage to extra-ocular muscles, Further prolapseespecially short medial rectus
Ocular surface dryness Blindness Strabismus (globe deviation) and subsequent damage
(exposure keratopathy)
Dealing with a globe prolapse (see Figure 4.2(d))
Immediate action Retropulse globe into orbit if possible (before transport to hospital)Cover with wet swab or cotton wool (to prevent corneal dessication)
Definitive action Give i.v. shock dose of dexamethasonePerform lateral canthotomyReplace globePerform tarsorrhaphy and leave for 2–3 weeks
Long-term action Give tear replacement if KCS occursResuture medial rectus muscle if lateral strabismus occurs

the first few minutes globe replacement ispossible without surgery, but after this anextensive lateral canthotomy will be requiredto reposition the globe in the orbit because ofthe peribulbar conjunctival swelling occur-ring during this time. If the owner is not ableto reposition the globe the animal should betransported to a veterinary centre withutmost urgency. The ocular surface must beprotected and moistened to prevent surfacedrying and long-term damage before theglobe can be surgically replaced in the orbit.A shock dose (2 mg/kg) of intravenousdexamethasone together with mannitol(1.0–1.5 g/kg) should be given slowly (aninfusion pump delivering the total volumeover 15–20 minutes is ideal) and will ameli-orate the immediate after-effects of such atrauma.
After repositioning the globe a tarsorrha-phy should be performed. The eyelids shouldbe re-opened only after several days. Only atthat point can the eye be assessed to give anadequate prognosis regarding both return ofvision and long-term cosmetic appearance;even if the eye will be non-visual a goodemergency treatment will leave a cosmeticallyacceptable eye, and most owners will be satis-fied and happy not to go through an enucle-ation. The prognosis will not in any case beparticularly good unless the eye has beenmanaged optimally in the critical periodimmediately after the prolapse.
4.3 Penetrating globe injury®
Suture patterns in the repair of globe lacera-tions are discussed in more detail undercorneal lacerations: it is in the cornea thatrepairs require careful attention to ensure thattransparency is maintained as much as possi-ble. While iris prolapse occurs with discon-certing regularity through a corneallaceration, penetrating injury of the scleraclearly results more often in uveal trauma,given the anatomical proximity of the choroidto the sclera. Often in cats, having earlier hada laceration to the eye, the prolapse of asection of the iris would result in healing ofthe cornea, which may be observed at theannual booster. The eye is still visual butpupillary miosis and mydriasis are slightlyimpaired. The main problem with iridalprolapse through a corneal laceration – that isto say what tissue to resect as necrosed andnon-viable – does not generally occur with achoroidal prolapse through a scleral wound.This is because the choroid usually bulgesonly to a limited extent through a sclerallaceration. On the other hand the free pupil-lary edge of the iris can extend through acorneal laceration with vascular compromise,resulting in ischaemic necrosis of the iris onthe external surface of the staphyloma. Thuswhile the difficult decision regarding theresection of such compromised and necrotictissue has to be made for iris passing througha corneal laceration, the choroid exposedthrough a scleral laceration is generallyhealthier and easier to manage.
The problem posed by scleral laceration isone of infectious panophthalmitis. While onemight be tempted, considering vascularcompromise, to replace all exposed choroidaltissue back though a scleral laceration, thethreat of intra-ocular infection and subse-quent panophthalmitis is ever present. Thedanger is heightened by the fact thatwhatever caused the laceration must havepassed into the eye, however briefly. As willbe discussed below, lacerations at the limbusmay be the result of blunt trauma, but sclerallacerations are normally direct injuries. Thismeans that the lacerating agent may wellhave deposited some bacterial contaminationin the posterior cavity. Unchecked, multipli-cation of such organisms can give rise to afulminant panophthalmitis.
Globe 35
Differential diagnosis in strabismus
• Full ophthalmic examination• Investigation of passive ocular
movement (including forced ductiontests)
• Investigation of active ocular movement• Full neurological examination
Strabismus may be caused by
• Retrobulbar mass• Cranial nerve palsy (i.e. abducens or
ocular motor involvement)• Extra-ocular muscle trauma/fibrosis (post
proptosis medial rectus damage)

The question is then how to deal with sucha laceration. Unless obviously necrotic it isadvised that the choroid bulging through thelaceration be replaced but only after a bac-teriology swab of the exposed tissue has beentaken and broad spectrum intravitreal andsystemic antibiosis has been started. This isfollowed by medication specific to the organ-isms cultured from the bacteriological inves-tigation. Swabbing for bacteriology may seemacademically correct, but in the clinicalsetting intra-ocular deposition of antibiotics
will be effective. Intra-ocular antibiotics maybe used as detailed in Appendix C.
If compromised or necrotic choroid is to beremoved, topical 1:1000 adrenaline should beapplied to produce vasoconstriction andminimize bleeding from resected tissue. It isalways better, as will be repeated with regardto iris presenting through a corneal lacera-tion, to be more radical in removing healthytissue at the edge of diseased uvea, than to becautious and risk replacing tissue which willonly act as a focus for necrosis and infection.
36 Veterinary Ocular Emergencies

5.1 Corneal ulceration
Disruption of the integrity of the cornea maybe divided into the following three categories(Schmidt 1977):
• Corneal erosion: disruption to the epithe-lial surface of the cornea without stromaldamage
• Corneal ulceration: disruption of epithe-lium and a variable depth of cornealstroma
• Descemetocoele: disruption of cornealstroma to the level of Descemet’smembrane with subsequent protrusion ofelastic Descemet’s membrane throughstromal ulcer
Not all corneal ulcers present as emergen-cies. A logical approach to their diagnosisand treatment will aid in determining whichare emergency cases. In any case the logicaldiagnostic protocol described below willallow evaluation of which therapeuticregimen is required for which particularulcer type. Any reader who has had acorneal ulcer will be able to testify to theacute pain that may accompany such ocularsurface erosion. For this reason, as well asthe potential threat to globe integrity posedby a deep ulcer, corneal ulceration shouldalways be viewed as a possible emergencysituation.
5.1.1 Is an ulcer present? – the use ofophthalmic stains
Corneal ulcers frequently present as a painfuleye and as such the ocular surface of anypainful eye should be closely examined toassess whether the epithelial surface is contin-uous or whether a discontinuity in the epithe-lial covering is present (Figure 5.1). In severe
Chapter 5
Cornea
Emergency management of deep cornealulceration
1. Perform full ophthalmic examination2. Define cause and depth of ulcer3. If ulcer is small and mid depth consider
performing radial keratotomy to promotestromal regeneration
4. If ulcer is small and deep performconjunctival pedicle flap
5. If ulcer is larger and deep performcorneoscleral transposition
6. Provide protection through contact lens,nictitans flap or use porcine intenstinalsubmucosal graft
Prognostic indicators in corneal ulceration
1. Size and depth are critical factors indefining treatment success
2. Any evidence of stromal melting a poorprognostic sign
3. Any evidence of intra-ocularinflammation a poor prognostic sign

38 Veterinary Ocular Emergencies
Disrupted withabnormality ofcorneal epitheliumand/or tearfilm
Clear Purkinjeimage in normalocular surface
Broken up
Clear
Purkinje imageat border of ulcer
Clear centre ofulcer in deep lesion
Fluorescein showingnon-adherent edge inrecurrent erosion
The ocularsurface
(a)
(b)
Well defined ulcer bedin a simple ulcer
Figure 5.1 Assessing for corneal ulceration. (a) Careful ophthalmic examination; (b) the fluorescein test
Questions to ask
1. What has caused the ulcer?• Exogenous trauma:
physical injurychemical injury:
acidalkalidetergent
• Internal factorsbasement membrane dystrophyKCSprofound corneal oedema
2. How deep is the ulcer?• Superficial – involving epithelium only• Mid stromal• Deep stromal• Descemetocoele
3. Is the ulcer healing?• How long has it been present?
(i.e. over seven days)• Is there a devitalized epithelial lip at
the edge of a superficial ulcer?• Is there stromal vascularization?
Approach to the corneal ulcer
Initial full ophthalmic examination
Perform Schirmer tear test
Take bacteriology or virology swab ifnecessary
(i.e. if associated with purulentdischargeor history of infected traumaor apparent FHV-1 infection)
Use fluorescein fully to delineate extent ofulcer

ulceration even a cursory examination willshow a defect in the ocular surface but insuperficial epithelial defects the lesion mayeasily be missed. Fluorescein is an invaluablediagnostic aid in such circumstances. Fluores-cein for ocular diagnostic use may be appliedusing a fluorescein impregnated strip orfluorescein drops (see Appendix C). Whenusing the strip some merely place the stripunder the upper eyelid and use the tear filmto dissolve and distribute the dye (Figure 5.2).A better method is to apply a drop or so oftear substitute or local anaesthetic to the stripbefore placing it gently on the ocular surface.This not only optimizes dye distribution butalso will not cause any further ocular surfacedamage in an already compromised eye.
Whether this technique or a drop offluorescein liquid is used, the diagnostic testshould be attempted only after a Schirmertear test has been performed. Tear evaluationshould be the first diagnostic test in any
assessment of the ocular surface: other testsmay well disturb the tear film and giveerroneous Schirmer readings. Similarlycorneal sampling for bacteriology, viral isola-tion or cytology should be carried out beforethe application of fluorescein. Topical anaes-thetics should only be applied after bacteriol-ogy as some anaesthetics have been shown tobe bacteriotoxic (Kleinfeld and Ellis 1966).
A key step in the fluorescein dye test is toflush away excess dye before examining theocular surface. The irrigation of the eye withsterile water or saline using a syringe is ideal,although in an emergency a cotton wool padsoaked with water may be used to flushexcess dye away. A minor but importantprecaution is a paper towel under the eye tokeep dye away from clothing. For the samereason the animal’s head should be wellcontrolled.
Examination of the eye after staining is bestperformed with a blue light or by illumination
Cornea 39
Figure 5.2 Fluorescein for ocular diagnostic use

with ultraviolet light from a Wood’s fluores-cent lamp. This may reveal subtle epithelialerosions which are much more difficult toexamine with white light. A second advantageis that ulceration is so obvious with blue lightthat the owner can readily be shown theextent of the lesion, often not so easily appre-ciated with white light.
Fluorescein is an exceptionally polarmolecule, and as such is excluded from thecornea by a healthy continuous epitheliumwith intact tight junctions between cells. Thecornea is composed of hydrophobic epithe-lium and stroma Fluorescein, beinghydrophilic, does not penetrate the epithe-lium but will penetrate the stroma when asuperficial ulcer is present. The extent of thecoloration must be assessed shortly afterapplication, as the dye can diffuse bothvertically and horizontally, giving a falseimpression of the area involved (Gelatt1978). In the Boxer indolent ulcers dyediffuses quickly under the epithelial flap,but this is normally obvious given the clearedge of the ulcer. Any defect in the epithe-lium, allowing water to pass from the tearfilm to the stroma, will be revealed byfluorescein which moves with the water intothe stroma, instead of being flushed awayby ocular surface irrigation. This is whygood flushing of the eye is important: aslight surface irregularity in which epithe-lium is still intact and not ulcerated mayotherwise appear to pick up stain justbecause the dye is pooling in these surfaceepithelial irregularities. Such an irregularityis called a pit or a facet, where an ulcer haspreviously caused a defect in the stromalthickness, later being covered by intactepithelium.
Rose bengal was previously thought tostain devitalized corneal tissue. It is now usedfor staining the ocular surface when themucin layer of the precorneal tear film isdeficient (Feenstra and Tseng 1992): thisoccurs in situations where the epithelialsurface is compromised, but not perhapscompletely obliterated. If the epithelial barrieris not destroyed fluorescein will not stain.Thus rose bengal is useful to stain partialthickness epithelial defects. Such ulcers occurin ulcerative feline herpes keratitis beforecomplete thickness epithelial ulcers are seenstained with fluorescein. The theoretical
disadvantage of using rose bengal is that it isreported as being painful when used inpeople. In our experience, cats in which thestain has been used do not generally showany signs of discomfort such asblepharospasm. Other drugs such as tropi-camide can be a quite severe irritant for a fewseconds in humans but do not seem to illicitsimilar signs in companion animals. It is nottherefore considered inappropriate to usesuch a drug routinely in dogs and cats.
5.1.2 Three key questions regarding anycorneal ulcer (see Figure 5.3)
• How deep is the ulcer?• Is the ulcer healing adequately?• Why is there are ulcer there is the first
place?
The first two questions are in many wayslinked as will be seen below, but here eachwill be taken separately.
5.1.2.1 Ulcer depth Regarding the depth ofthe lesion, ulcers can be classified as beingsuperficial, partial thickness or descemeto-coeles. In this classification superficial ulcersreally involve only epithelial erosion withoutstromal destruction. Partial thickness ulcershave stromal extension of epithelial defectsand this can run from margin stromalinvolvement to deep ulceration. Descemeto-coeles form when all stromal tissue has been destroyed, leaving only Descemet’smembrane. This, being elastic in naturebecause of its collagen type IV content, bulgesthrough the stromal defect under intra-ocularpressure.
How are these different depths of ulcer tobe differentiated? Close examination, ideallywith a slit lamp but more usually in anemergency situation with a magnifying loupeor direct ophthalmoscope at +20 D asdescribed above, shows the depth of ulcerclearly merely by the appearance of the ulceredge; but some further clues aid evaluation.The first is the degree of stromal oedemaassociated with the ulcer. A superficialepithelial erosion will have little or nostromal oedema, simply because the stromahas had little opportunity to imbibe waterand has not undergone tissue damage. Apartial thickness ulcer will have a varying
40 Veterinary Ocular Emergencies

Cornea 41
Figure 5.3 Key questions to ask of an ulcer

degree of stromal oedema around it depend-ing on how much excess water has been takenup by stromal tissue. This involves the centreof the ulcer and also a halo of cornea aroundthe lesion. Most important is the deep ulcer,which may have considerable peri-ulcerativeoedema but in which the centre of the ulceris clear of oedema, often manifesting quite abright appearance because of tapetal reflec-tivity through the remaining corneal tissue. Infact the clarity of tapetal reflection, in contrastto the surrounding stromal oedema, showsthat the ulcer has all but completely perfo-rated the corneal stroma. These ulcers are realemergencies, as a little more stromal destruc-tion will lead to a descemetocoele. Thedescemetocoele is generally easy to recognizesince the clear Descemet’s membraneprotrudes through the surrounding stroma tosome extent, producing a dome-like structurein the midst of considerable oedematousstromal opacity.
5.1.2.2 Ulcer healing The degree of healingresponse of the cornea around the ulcershould be determined to give a full evalua-tion of the corneal ulcer. Each of the aboveclasses of ulcer depth can be assessed forsigns of healing.
The superficial corneal ulcer or erosionwhich is going to heal will have done so, orat the very least shown a significant reductionin ulcer size, within three to five days, givenadequate corneal protection. The superficialulcer which is not going to heal this rapidlywill be characterized by a lip of non-healingdevitalized non-adherent epithelial tissue.The deeper stromal ulcer which is in theprocess of healing will show a gradual epithe-lialization of the ulcer crater within the firstfew days, eventually leaving a fully epithe-lialized corneal facet. Such a healing ulcerwill also be characterized by vascular in-growth from the limbus. The problem is not,perhaps, so much one of not healing, but ofhealing that is not progressing rapidlyenough or filling in the stromal deficitcompletely enough. Given the propensity ofsuch ulcers to deepen further it is importantto treat them as if they were liable to perfo-rate at any moment. It is with these ulcersthat the third question must be answeredquickly: what is the reason for the ulcer? Theanswer is likely to show also what is causing
progression in ulcer depth and what can bechanged to remedy the situation.
5.1.2.3 The aetiology of the ulcer Theprimary reason for ulcer formation may arisefrom within the cornea itself or from withinthe rest of the ocular apparatus, or there maybe an external infectious or external physicalcause. The prime case of a corneal defect itselfbeing responsible for ulcer formation is theepithelial basement membrane dystrophydiscussed below. Here in fact the dystrophymay not be responsible for the initial ulcerformation but is the underlying defect whichprevents rapid healing of a minor erosionwhich might, in a normal cornea, not evencause enough of a problem to necessitate theanimal being presented to a veterinarian.
Abnormalities in the rest of the eye fall intoseveral groups. Lid defects may give rise tocorneal abrasions in several conditions. Entro-pion and post-traumatic lid defects in anybreed, or congenital abnormalities such as thelid colobomas in cats, can all lead to trichia-sis where normal hair abrades the cornealsurface. The same can be seen when a skinfold in a brachycephalic breed causes normalhair to contact the cornea. Medial canthallashes can cause a similar problem and, beingshort and stubby, these can result in consid-erable corneal pathological changes, either asaberrant pigmentation and keratitis, or acorneal ulcer. Similarly distichiasis, withaberrant cilia from the meibomian glandopenings, or an ectopic cilium from aconjunctival hair follicle, can cause cornealabrasion resulting in a corneal ulcer. A neuro-logical deficit such as a facial paralysis cancause an exposure keratopathy which maywell include corneal ulceration.
Other intrinsic defects that can lead tocorneal ulceration include conditions causingcorneal oedema. These range from endothe-lial dystrophies to glaucoma. Corneal oedemaleads to ulceration through bullous keratopa-thy. When oedema is severe water from thestroma can extrude in blebs under the cornealepithelium, with formation of epithelialbullae. These are prone to burst, eitherspontaneously or with the slightest of exter-nal forces, giving rise to a corneal ulcer. Thedifficulty is that the underlying cornealoedema renders healing problematic: sponta-neous healing is unlikely to occur and
42 Veterinary Ocular Emergencies

techniques used to promote epithelial healingwith a normal stroma often fail to work in theface of stromal oedema. More promisingmethods are discussed in section 5.2.2.
An important intrinsic cause of ulcerationis keratoconjunctivitis sicca (KCS). Adeficiency in the all-important lubricatingtear covering of the ocular surface is acommon factor in the genesis of corneal ulcer-ation. KCS may be the root of chronic ulcera-tive problems but can also result in acute andvery painful surface ulceration. KCS as anunderlying problem shows the importance offully investigating the eye before attemptingto treat the ulceration. Any therapeuticregimen attempted in the presence of a dryeye will fail. Amelioration of tear deficiency,either with tear replacement or better withtopical cyclosporine, may allow ulcer healingwith little in the way of intensive ocularsurface management.
It might seem surprising that discussion ofinfection as a predisposing cause of cornealulceration has not been considered earlier inthis list of causes of corneal ulceration.
Corneal Gram-negative or fungal infectionmay be an important complicating factor incorneal ulceration but bacterial or fungalagents are not particularly common as predis-posing factors in corneal ulceration. Viraldisease is a prime cause but such virallymediated ulcerations are recognized withcertainty only in the cat. Here feline herpesvirus is the primary cause of dendritic, andpossibly also geographic, ulceration. Equineherpes virus is thought to have a similar rolein the horse but definitive evidence for this islacking. A number of cases of punctate ulcer-ation occur in the dog, and given the preva-lence of similar ulceration in man with anadenoviral aetiology, a viral cause may occurhere although none has been determined todate.
Finally, trauma is at the root of manycorneal ulcers, with or without other compli-cating factors as discussed above. Traumaticincidents, from superficial abrasions to deepwounds, would be relatively easy to treatbut for the addition of complicating factorsfrom inherited corneal defects to external
Cornea 43
Treating the corneal ulcer
The assumption is made that any predisposing cause has been addressed
• The healing superficial ulcer: antibiotic cover using chloramphenicol drops or other antibiotics
• The non-healing superficial ulcer:protection:
therapeutic contact lensthird eyelid flaptarsorraphy
debridement:removal of devitalized epithelium with dry swab or scalpel bladealteration of ulcer bed: punctate or grid keratomyor by partial thickness keratectomy
analgesia:use of systemic NSAID such as oral carprofen
• The stromal ulcer less than 1/2 corneal depthprotection:
therapeutic contact lensthird eyelid flap not recommended as deepening of ulcertarsorraphy � will be more difficult to recognize
• The deeper stromal ulcer or descemetocoeleconjunctival pedicle flapcorneoscleral transposition

infections. In section 5.2 we consider themanagement of the different forms of ulcerdescribed above. Only when the ulcer hasbeen fully assessed for depth, healing andaetiology can one be happy to proceed withthe correct course of ulcer management.
5.2 Dealing with different ulcers
5.2.1 The simple healing superficial ulcer
A superficial erosion with solely epithelial orepithelial and only superficial stromalinvolvement can be effectively managed withtopical antibiosis and re-examined in fivedays, as long as no intrinsic or infectiouscause is determined. In such a case topicalantibiosis with fucidic acid in the dog or
topical chlortetracycline in the cat would beappropriate. Within this time a non-compli-cated ulcer will have healed. Any persistenceof ulceration would call for re-appraisal of theulcer and possible recategorization of thelesion as a persistent ulcer, as discussedabove.
5.2.2 The recurrent or persistent non-healing superficial ulcer
Healing response is particularly important ingauging the superficial ulcer. While some ofthese ulcers will occur as a result of traumato a healthy cornea many of them will berefractory, recurrent ulcers in which healingis not occurring as it should. This generallyoccurs for one of three reasons. The first andbest recognized is true epithelial basement
44 Veterinary Ocular Emergencies
Box 5.1 Treating the non-healing ulcer

membrane dystrophy. The second is severecorneal oedema where cystic blebs arise fromstromal excretion of water giving a bullouskeratopathy. The third is less than optimalhealing in an older animal. These three condi-tions will be discussed further below.
The most common condition resulting in anon-healing ulcer is that occurring in dogswith epithelial basement membrane dys-trophic change: here there is a diminution inthe number of hemidesmosomes, the anchor-ing points by which the basal epithelial cellcomplex attaches to the underlying stroma.These ulcers are seen in Boxer dogs andPembroke corgis particularly althoughrecently a number of West Highland Whiteterriers have been seen by one of us withsimilar disease.
The classic recurrent ulcer has a lip ofdevitalized epithelium around the edge of theulcer. This prevents the healthy cornealepithelium migrating to the ulcer edge andcommencing the healing response. Thus thefirst step in any therapeutic protocol for suchulcers must be to remove this dying non-adherent epithelium, as described furtherbelow.
Disturbance of the ocular surface with adry swab or with a piece of cotton woolwrapped around a fine haemostat will peeloff this poorly adherent epithelium, confirm-ing the diagnosis of epithelial basement
membrane dystrophy. The technique ofepithelial debridement is for that reasonimportant diagnostically as well as therapeu-tically.
Determining healing is equally, if not more,important for deeper ulcers involving thestroma. Here a key feature indicating a vigor-ous healing response is the invasion of bloodvessels from the limbus to the ulcer edge. Afirm grasp of the pathophysiology of cornealulcer healing requires considerable under-standing of the mechanisms at work in bothepithelial and stromal healing, as presentedbelow.
Removal of all devitalized, poorly adherentepithelium is vital to allow full healing of
Cornea 45
Figure 5.4 Third eyelid flap anchoring to (a) upper eyelid; (b) episclera
Box 5.2 Devitalized epithelium becomes white afterphenol cautery

dystrophic epithelial erosions. Often quiteextensive amounts can readily be strippedfrom a dystrophic cornea. One should not beconcerned that normal epithelium will beremoved by such a technique. Even quite avigorous rubbing will not disturb a healthyepithelium while it takes little effort todislodge devitalized tissue.
Today this dry debridement is generally allthat is documented in the standard texts. Intimes past, however, agents such as phenol ona cotton tipped applicator were used to goodeffect and might be considered appropriate, ifnot actually preferable, to dry debridement.As with the latter technique phenol does notdamage healthy epithelium and so is usefullyselective of dystrophic epithelial tissue.
In some cases debridement and cornealbandaging are all that is necessary to promotefull healing. In cases where this fails anumber of treatment regimens have beenreported on. It is generally the case thatwhere several treatment options exist one canassume that none is universally successful.This is the case with persistent recurrenterosions: the best treatment for these ulcers isdifficult to determine. The very terms recur-rent, persistent and recidivistic stronglysuggest that achieving full permanent healingis not easy. Given the failure of any onetechnique to give acceptable results in everycase it will be worthwhile to consider thedifferent options for treatment.
The basic science behind the different treat-ment regimens should be understood to facil-itate treatment planning. We have alreadydiscussed measures to remove devitalizedepithelial tissue from the path of new epithe-lial cell migration. The second importantfeature in a therapeutic plan should be tominimize trauma to the epithelial surfaceduring healing. In her comparative survey oftreatment methods, Susan McLaughlin deter-mined that of all the options the most success-ful, either alone or in combination with othermethods, was the third eyelid flap. Today wemight prefer to provide a corneal bandageusing a therapeutic contact lens. This has theadvantage that the eye can both see and beseen but the disadvantage that, while thenictitating membrane flap will be secure untilreleased, a contact lens may not stay in placefor ten or so days until full corneal healinghas taken place.
If a third eyelid flap is to be placed one oftwo techniques can be used, each favouredby different groups of ophthalmologists(Figure 5.4). Some say that the third eyelidshould be secured not to the lid but to thebulbar conjunctiva. This ensures that whenthe eye moves so does the flap. Whensecured to the lid there is always the possi-bility of some friction between the flap andthe cornea as the globe moves. This is proba-bly very slight but in destabilized ocularsurface problems it is wise to take every steppossible to minimize even mild surfacetrauma. Nevertheless other ophthalmologistsprefer anchoring the third eyelid to the uppereyelid, since if long ends are left to thesutures the flap can be released and thenrepositioned without the need to anaes-thetize the animal again.
Removing diseased tissue and protectingthe corneal surface are the bare essentials oftreatment for such persistent erosions. As hasbeen suggested a considerable proportion ofthese ulcers will heal with this treatmentalone. The rationale for subsequent treat-ments is either to disrupt the epitheliostromalboundary with its basement membrane or toprovoke a considerable superficial stromalscarring effect. The first retains good vision atthe end of the treatment period while thelatter tends to give scar formation reducingvisual acuity considerably. Such treatmentsshould be used either when the eye is alreadyblind or when nothing else will work. Theformer rationale is the basis for thetechniques of grid or punctate keratotomy.The latter is the reason behind the thermalkeratoplasty described below.
Grid keratotomy uses a 21–23 gauge needleto produce, as its name suggests, a grid oflines over the ulcerated area while punctatekeratotomy merely produces pinpointpunctures in the most superficial stroma(Figure 5.5). The aim of both these techniquesis that the epithelium which grows down intothe gridline or puncture points should serveto anchor the whole epithelial sheet in place.For this reason the gridlines or punctures donot need to be as close together as when theaim is to disturb the whole basementmembrane surface. The technique can beundertaken in the conscious dog with topicalanaesthesia and perhaps mild sedation in anervous or boisterous individual. In a matter
46 Veterinary Ocular Emergencies

of a few days epithelial healing occurs aftersuch a keratotomy, although in many casesaccompanied by considerable vascularization.This can be removed once full ulcer healinghas occurred by the use of topical steroids.Many ophthalmologists rightly feel that usingsteroids in an eye predisposed to ulceration isunwise. Steroids markedly impair epithelialhealing and, were a subsequent ulcer tooccur, the use of these agents would be mostdefinitely contra-indicated. The advent ofreadily available topical non-steroidal anti-inflammatory drugs such as flurbiprofen ordiclofenac has on the whole rendered unnec-essary the use of steroids to reduce post-healing vascularization of the ulcer bed.
5.2.3 Ulceration secondary to bullouskeratopathy®
In recurrent ulceration secondary to bullouskeratopathy in corneal oedema, techniquessuch as the keratotomies often fail to work.Here a technique to produce epitheliostromalscarring can be used, where the eye has littlevision in any case. In thermal keratoplasty athermocautery tip produces spot-welds in thecornea with about the same distribution asthe stromal punctures in punctate kerato-tomy, that is leaving a distance of about 1 mmbetween applications (Wilkie and Whittaker1997) (Figure 5.5). Some ophthalmologistsperform this without stripping the overlying
epithelium while others thoroughly debridethe ocular surface first.
5.2.4 Partial thickness stromal ulceration
Ulcers with stromal involvement may bemanaged conservatively if they are less thanone third of the corneal thickness in depth.The decision whether to leave the ulcer toheal or to perform a grid keratotomy or asuperficial lamellar keratectomy is oftendifficult. If the ulcer is extensive and re-epithelialization of the cornea has notoccurred, a debridement including gridkeratotomy or lamellar keratectomy can beused. Grid keratotomy can be performedunder local anaesthesia. It is important torest the hand with the needle on the faceinferior to the eye, so if the animal suddenlymoves (which is most often drawing thehead back) a penetration of the globe willnot happen. The use of bandage contactlenses may be preferred over performing athird eyelid flap, for it is in these partialthickness ulcers that regular monitoring isessential to ensure that the ulcer is healingrather than becoming deeper. If epithelial-ization of a partial thickness ulcer isprogressing, this shows that healing is occur-ring and in most cases, where there is stillsome considerable thickness of cornealstroma intact, careful observation can beappropriate.
Cornea 47
Figure 5.5 Debridement and gridkeratomy for an indolent ulcer

A progressing ulcer one over a third of thecorneal thickness in depth or a descemeto-coele where the ulcer has breached the entirethickness of the stroma should all be consid-ered as urgent emergencies and treated withconjunctival pedicle flaps or possibly withGaiddon’s technique of radial keratotomy(Gaiddon 1996), as discussed further in thissection.
In the case of a partial thickness ulcerwhich is not showing any signs of healing,there are perhaps three therapeutic optionsavailable. The first is to perform a conjuncti-val pedicle flap as described in section 5.2.5.This has the great advantage that it ensures aresult which is watertight and also allowsserum from the cut surface of the pedicle flapto seep continually into the underlying ulcer-ated stroma providing both growth factorsand collagenase inhibitory alpha 2macroglobulins. It does, however, give asignificant obstruction to vision, often in theprimary line of sight. The conjunctival flapmay not always be the perfect choice of treat-ment for a midstromal ulcer but it is a safemethod, where the veterinary clinician is atlittle risk of perforating the globe. Thus theauthors recommend the conjunctival flap as asafe surgical treatment which may causesome scarring of the cornea postoperatively.
A second option, regularly used in humanophthalmology but employed less frequentlyin the veterinary field, is the use of cyano-acrylate glue in the stromal wound (Figure5.6).
Use of butyl cyanoacrylate glue requires
• an anaesthetized patient with an immobi-lized eye
• a completely dry corneal surface. The bestway of ensuring this is to use a photogra-pher’s drying gas aerosol over the surfaceof the cornea
• a well controlled application of a smallamount of glue painted onto the ulcer bedwith a fine (25 G) needle (Figure 5.7).
5.2.5 Near-penetrating ulcers,descemetocoeles and penetrating ulcers®
As noted above an ulcer which is at the pointof penetrating or has developed a descemeto-coele should be taken to surgery urgently.Even if perforation does occur duringsurgery, it is clearly much to be preferred thatsuch an entry into the anterior chambershould occur in the controlled sterile environ-ment of the operating theatre rather than in ahome or field setting.
48 Veterinary Ocular Emergencies
Box 5.3 Treating the perforated cornea
• Is the cornea perforated?The Seidel test showing a perforation:
dry the corneaapply drop of fluorescein (uniformyellow colour)watch for ‘snaking’ stream of aqueousfrom the laceration
• Is there prolapse of iridal tissue?Evaluate the health of protruding iris
for 24 hours the surface covering ofexuded serum protects iris, thus asubstantial number of staphylomas canbe replaced. ‘If it bleeds it is not toocompromised’ is a useful maxim
• Aim to replace as much non-infected recentlytraumatized tissue as possible
• Use visco-elastic gel to break downiridocorneal adhesions

The optimal technique for performing aconjunctival pedicle flap is shown in Figure5.8. A pinch of conjunctiva is taken around5 mm from the limbus and a pair oftenotomy scissors used to incise the conjunc-
tiva and then bluntly dissect under theconjunctival epithelium. It is easy to achievea single plane of dissection if the whole flapis prepared by blunt dissection through onesmall keyhole incision. Making a larger
Cornea 49
Figure 5.6 Bullous keratopathy – pathogenesis and treatment
Figure 5.7 Painting glue onto the ulcer bed

incision early in the procedure results in anumber of planes of dissection and generallygives a thicker and less ideal flap. The flapshould be thin enough to be moved easilyaround and stretched over the ulcer bed.Always make the flap square and larger thanthe ulcer so it can be trimmed to fit thedefect. It should be sutured in place with a
fine absorbable suture such as 6/0 or betterstill 8/0 vicryl. The neck of the pedicleshould be left unsutured so that when theulcer has healed the pedicle can be divided,leaving a small island of conjunctiva which,deprived of blood supply, will eventually beincorporated into a small corneal scar, allow-ing vision even when in the visual axis.
50 Veterinary Ocular Emergencies
Figure 5.8 Techniques for performing the conjunctival pedicle flap. (a) Undermine conjunctiva from oneentry point; (b) cut flap with base opposite ulcer; (c) position flap; (d) suture flap and close
Performing the conjunctival pedicle flap
Reasons: Deep corneal ulcer Melting ulcer Descemetocoele
Mechanism: Immediate physical repair of defectSource of serum with immunoglobulins and macroglobulins
For the technique, see Figure 5.8.

An alternative technique is that of JacquesGaiddon using the radial keratotomytechnique perfected for the treatment ofhuman myopia (Gaiddon 1996). Gaiddonreasoned that since the basis of radial kerato-tomy for myopia was the induction of stromalremodelling, and this was just what wasneeded in deep stromal ulceration, deepradial keratotomy would be appropriate indeep ulceration in the dog. This certainlyworks, with substantial reduction in depth ofthe ulcer and eventual complete healing, buthas yet to be taken up by veterinary ophthal-mologists in any great number.
5.2.6 The melting ulcer®
5.2.6.1 The melting ulcer: diagnosis Thesigns of a melting, or collagenolytic, cornealulcer are obvious at clinical presentation.Where a normal stromal ulcer may haveconsiderable corneal oedema or vascular andcellular infiltrate, its edge is relatively welldefined and the surrounding stroma appearspredominantly healthy. The melting ulcerhas, as its name suggests, an appearance ofprogressing from the tectonically structuredsolid stroma to an almost fluid consistency.While oedema gives a ground-glass appear-ance to the cornea such stromal lysis oftenproduces a much more dense white opacifi-cation of the stroma. The collagen fibrilswhich are the support structures in thestroma are broken down by a variety ofenzymes resulting in degraded stroma whichin many cases is so fluid as gradually to runfrom the ocular surface down the eyelid.These collagenolytic enzymes may be derivedfrom bacteria such as Pseudomonas or frompolymorphonucleocytes infiltrating infectedcornea. It is the presence of bacteria produc-ing the enzymes and the action of theenzymes which must be considered in formu-lating the diagnostic and therapeutic plan.
In the horse a recent report (Brooks et al.2000) described melting ulcers being causedby Streptococci, demonstrating that it isimportant not to assume that a melting ulceris caused by Pseudomonas and thus onlyapplying aminoglycosides. These antibioticsmay have little if any action on staphylococciand streptococci, thus aggravating theproblem.
A bacteriology swab should be taken asdiscussed above and cultured with urgency.A smear of such a swab on a couple of micro-scope slides allows one to be stained withGram’s method and the other with lactophe-nol cotton blue and immediate evaluation ofwhether a Gram-positive or, more likely, aGram-negative or fungal agent is responsible.A corneal scraping under local anaestheticand/or sedation should also be undertakenand the scraping applied directly to a bloodagar plate for immediate inoculation. Evenbefore the full result of these bacteriologicalinvestigations is known treatment must beinstituted with haste as discussed in section5.2.6.2.
The anamnesis of the case as well as thecharacteristics of previous disease in thegeographical area are important in a fullevaluation of the disease. In some areasparticular organisms are more common thatothers and this, together with informationregarding the involvement of, say, an injurywith possibility of a plant material cornealforeign body, is important in the full investi-gation of such an ulcer.
5.2.6.2 The melting ulcer: treatmentFrequent – initially hourly – application of abroad spectrum antibiotic with actionagainst the bacteria most likely to becausing this collagenolysis – predominantlyPseudomonas and Proteus – is very important.Previously, as discussed above, this meantthe use of topical gentamicin but drug resis-tance in many cases has led to changes.Fortified preparations, with powder forintravenous gentamicin use, dissolved inartificial tears or in a topical base have beenrecommended. Recently in the UK a formu-lation of gentamicin with EDTA andtrometamol has been licensed. The EDTA isnot likely to be at a sufficient dose forefficacy in collagenase inhibition (see belowin this section) but it does increase theefficacy of the gentamicin by facilitatingdrug uptake by bacteria. Trometamol alsoincreases drug absorption by bacteria andthus similarly raises drug efficacy. Morerecently available drugs include thequinolones, but although these are effectiveagainst Gram-negative organisms their usein veterinary ophthalmology has yet to beassessed fully (Figure 5.9).
Cornea 51

52 Veterinary Ocular Emergencies
A diagnostic and therapeutic approach
History – often history of trauma– possible involvement of plant or other organic material– rapid deterioration in corneal condition
Appearance – white/cream ill-defined corneal opacity– irregular corneal surface– frank corneal liquefaction– ocular pain
Treatment
(i) Sedation (and/or peri-ocular nerve blocks in the horse)(ii) Take swabs and scrapings from affected cornea, including lesion edge cytology – Gram and Diff
Quick stains for immediate presumptive identification of infectious organisms’ culture and sensitivity– both bacterial and fungal
(iii) Insert subpalpebral or nasolacrimal medication device(iv) Apply antibiotic and anticollagenolytic medication hourly to start
Antibiotics fluoroquinolones (Exocin (Allergan))fortified preservative-free antibiotic solution
Drug Commercially Suggested Shelf-lifeavailable strength fortified strength
Amikacin 10 mg/ml 30 daysCarbenicillin 4–8 mg/ml 3 daysGentamicin 3 mg/ml 30 daysTobramycin 3 mg/ml 14 mg/ml 30 daysVancomycin 50 mg/ml 4 days
Anticollagenolytics – serum (�2-macroglobulin antiprotease)– EDTA (chelates Ca2+ as enzyme cofactor)– acetyl cysteine (binds Zn2+ cofactor)
(Most easily produced by taking autologous blood into EDTA, spinning down and transferring resultingplasma through several EDTA blood tubes) (Figure 5.9)
Box 5.4 Diagnosis and treatment of collagenolytic ‘melting’ ulcers
Mechanisms in collagenolytic ulceration
Enzyme origin: Bacterial Fungi Neutrophils
Gelatinase Collagenase Protease
Mechanism: Collagenolysisand stromal
Inhibited by: 10% acetyl cysteine EDTA Autologous serum
Through action of: Zn chelation Ca chelation Alpha 2 macroglobulins

Controlling the infective agent is importantwill do little in the short term to preventstromal degradation by collagenolyticenzymes. We need to inhibit action of theseenzymes: difficult, because more than oneenzyme is active in most of these ulcers. Infact there is a large family of matrix metallo-proteinases (MMP1–9 at the time of writing)which, together with collagenases and gelati-nases, produce the stromolysis. Some of theseMMPs are agents of normal corneal remodel-ling in the healthy eye, while others arederived from infiltrating leucocytes. Stillothers come from infecting micro-organisms.Each enzyme has a slightly different substrateand a different milieu is required for theinhibition of each one. EDTA binds divalentcations such as Ca2+ and since many of theseenzymes need calcium as a cofactor, EDTAhas an important role in inhibition across theboard. Serum alpha 2 macroglobulinssimilarly are natural inhibitors of a number ofthese enzymes. Acetylcysteine has an import-ant inhibitory action by chelating zinc.
Thus, the best therapeutic regimen in theface of a melting ulcer is an aggressive onecombining, for the first few hours at least,hourly application of appropriate antibiotic –fortified gentamicin, tobramycin withpolymyxin B, or a quinolone such asciprofloxacin or ofloxacin – with serumcontaining 0.2M EDTA and an acetylcysteineformulation.
The surgical option of a reasonably deepkeratectomy and the placement of a conjunc-tival pedicle flap should not be overlooked.This will have the advantage of removing asubstantial microbial and stromolytic enzymeburden on the one hand, and allowing contin-ual natural application of serum to the ulcer-ated area through the pedicle flap ofconjunctiva.
5.2.7 Chemical injury
Severe corneal ulceration and long-lastingdamage to the ocular surface may be causedby chemical injury to the eye. With differentchemicals the pathogenesis of damage is verydifferent as is the remedy, although in allcases generous ocular lavage is called forimmediately. The centrality of knowing theexact nature of the agent involved shows theimportance of taking as thorough a history aspossible.
The most serious chemical causing ocularsurface damage is alkali – lye or ammonium-based fertilizers are the most commonlyencountered alkaline chemicals but burnsfrom such agents are fortunately rare inveterinary ophthalmology. The severity of analkaline burn stems from the fact that a highpH destroys both epithelium and stromawithout causing a coagulative change. In thecase of an acid burn, this coagulationprevents further penetration of the chemicaland thus limits the depth of the burn.Alkaline burns can be deep and, in addition,they very rapidly destroy all cells in theirpath, including the stem cells of the cornealepithelium, leading to chronic non-healingulceration.
Because an alkaline burn acts in many wayslike the collagenolysis of a melting ulcer, thesame inhibitors of metalloproteinase enzymesare used in addition to copious irrigation ofthe ocular surface.
Cornea 53
Figure 5.9 Close examination of a wound

5.3 Corneoscleral laceration®
5.3.1 Defining the extent of a corneallaceration
Proper management of a corneoscleral lacer-ation depends on full pre-operative assess-ment of the degree of injury. It has beenfound useful in both human and veterinaryophthalmic trauma management to considerthis assessment as a hierarchy of injuries andrepair techniques. Such a hierarchy beginswith the non-perforating corneal laceration.This may be gaping or a self-sealing stromalwound. Next comes the bevelled lacerationwhich, although perforating, has self-closedwithout involvement of other ocular struc-tures. The more complicated lacerations arethose with significant damage to and oedemaof surrounding stroma and those in whichinvolvement of iris plugging the leakingwound has created a staphyloma.
Close examination of the wound, ideallywith a slit-beam, is essential to evaluateseveral features (see Figure 5.9). First, howdeep is the wound? In some injuries it is clearthat the cornea is fully perforated. Othersmay only involve the epithelium and anteriorstroma. The intermediate lacerations are themost difficult to evaluate. There may, forinstance, be considerable stromal damagewith oedema which may seal a fully perfo-rating wound. The management of a perfo-rating wound is quite different from that ofa non-perforating wound, and it is importantto define into which category the traumafalls.
The key test here is the Seidel manoeuvre(Figure 5.10). Fluorescein solution 2% isapplied to the ocular surface. Even a smallamount of aqueous leaving the anteriorchamber through a corneal puncture woundwill be observed as a clear wandering streakthrough the fluorescein lake on the ocularsurface, leaving no doubt that the cornea isfully perforated. It may be necessary, in thecase of a self-closing wound, to perform aforced Seidel test where slight digitalpressure is applied to the globe through theupper lid. This presents certain risks andshould be done with caution, especially if thecorneal stroma appears compromised.
Another important feature is whether thewound gapes at all (Figure 5.11). Some lacer-ations ‘yawn’, as it were, at the ocular surfaceand need a different suturing pattern toensure correct apposition at the end ofsurgery. Gaping wounds may be associatedwith significant anterior and epithelialstromal damage, again requiring differentsurgical management. Another importantfeature to note is the amount of corneal
54 Veterinary Ocular Emergencies
Evaluating the lacerated cornea
• How deep is the laceration?• Is the laceration perforated? – the Seidel
test (see below)• Are the edges clean or is there foreign
material involved?• Is there other ocular damage?• Is there one laceration, or several, or a
starburst appearance?• Is the laceration perpendicular to the
corneal surface, or with a flap of tissue?
Emergency management of a corneallaceration
1. After careful examination, stain eye withfluorescein
2. If non-perforating cover with third eyelidflap or contact lens and treat withatropine and topical antibiotic
3. Definitive repair may involvecyanoacrylate tissue glue or merelycontact lens bandaging if superficial andnon-perforating
4. If perforating cover with contact lensbefore definitive repair once oedema hassubsided (on atropine and antibiotictreatment topically, with NSAID topicallyand systemically)
5. Definitive repair in such a case willinvolve microsurgical repair of corneallaceration
Prognostic indicators in the corneallaceration
1. Substantial corneal oedema andvascularization can resolve after treatment
2. Prolapse of intra-ocular contents (suchas iris in a staphyloma) is a poorprognostic sign
3. Length of time between laceration andspecialist attention is critical forsuccessful management.

Cornea 55
Figure 5.10 Evaluating a potentially penetrating globe injury
Figure 5.11 Treating the non-perforating corneal injury

damage surrounding the laceration. This willdefine where suture entry points can bemade, and whether excision of non-viablecornea is needed before the wound edges canbe apposed.
5.3.2 Defining involvement of otherocular structures
The most obvious ocular structure whichmay be affected in a corneal laceration is theiris. The eye is designed, it might be said, tominimize the after-effects of trauma. One ofthe features of that design is the manner inwhich the outrush of aqueous after a corneal laceration carries with it the iris,plugging the laceration and forming astaphyloma. The highly vascular iris itselfproduces a coat of fibrin protecting it fromthe desiccating effects of its externalposition. All this renders repair moresuccessful than often appears on first exami-nation of a staphyloma.
Other ocular structures may be involved ina corneal laceration, with or without staphy-loma formation. The penetrating agent mayhave reached the lens surface, where a capsu-lar perforation may result in cataract in thelong term or even a so-called phacoanaphy-lactic reaction upon sudden leakage of lensmaterial.
5.3.3 Repairing a simple non-penetratingcorneal laceration
A non-perforating clean laceration, as deter-mined by the Seidel test and in which theedges lie either flat together or gaping open,may be managed appropriately with antibi-otic cover and a mild pressure bandage suchas that provided by a bandage contact lens.This has the dual effect of supporting thewound by a splinting action and shielding thecornea from the mild abrasion which mayoccur by natural lid movement. Antibioticdrops such as chloramphenicol or aquinolone should be given two to four timesdaily. A cycloplegic such as atropine can beuseful in preventing ocular pain. After thefirst day or so it will probably be needed onlyonce daily because of its long duration ofaction in the otherwise uncompromised eye.If a flap of tissue has been created but notdetached from the underlying cornea a thin
layer of tissue glue can be painted onto theulcer bed and the flap replaced (Figure 5.7).
5.3.4 Repairing a simple perforatingcorneal laceration
Most if not all deep corneal lacerations, andcertainly all in which there is still aqueousleakage at the time of examination, requiresecure wound closure with suture placement.It is important to avoid pressure on the eyeduring anaesthetic induction or placement ofthe eyelid speculum. If the globe is alreadyreformed there is no necessity to enter theanterior chamber, but if the chamber needs tobe reformed with either balanced salt solutionor a visco-elastic this is better irrigated intothe anterior chamber through a limbal needle-stab incision rather than through the wounditself, which may be infected or alreadycompromised. When inserting a needle at thelimbus it is important to have the needleparallel to the iris, thus not lacerating the irisand causing a haemorrhage from this richlyvascularized tissue.
Simple interrupted sutures should be used.The important point is that the sutures shouldbe deep – at least three quarters of the depth ofthe stroma to ensure that the wound is stablepost-surgically (see Figure 5.12). For cornealsuturing vicryl or nylon is best; both types ofsuture are removed when healing is complete.For corneal surgery 6/0 to 10/0 sutures may beused, the thickness being related to availabilityof microsurgical instruments, means of magni-fication and surgeon’s preference. The suturesshould not penetrate the full thickness of thecornea since this gives an excellent wick forentry of infectious organisms from the ocularsurface, but a suture that is too shallow resultsin a gaping wound (see Figure 5.11). Thenumber of sutures should be the minimumrequired to achieve a watertight closure. Toomany sutures result in further stromal compro-mise. The distance of suture entry from thewound edge is difficult to decide. On the onehand the ideal suture placement is symmetri-cal, the distance from the wound edge beingequal to the depth of the suture. On the otherhand the wound edge is often so compromisedand oedematous as to render impossible sutureentry at the optimal position. In such caseslonger sutures can be used but still the inten-tion should be to produce a deep symmetrical
56 Veterinary Ocular Emergencies

suture. For best suture placement consider thevector forces (Figure 5.11) which render anoptimal distance between two interruptedsutures equal to half the distance of the suture-length across the wound (Eisner 1990).
5.3.5 Repairing a corneal lacerationcomplicated by iris inclusion
In a major laceration, or one in which‘shallowing’ of the anterior chamber hasoccurred, iris may be incarcerated in thewound or prolapsed through it (Figure 5.13).In either case iris tissue should be inspected
carefully in deciding whether it should beremoved or retained. Incarcerated iris shouldbe freed from the edges of the corneal wound.If the wound is less than 24 hours old it canbe replaced in the anterior chamber unlessobviously macerated or otherwise damaged.Even after this period healthy-looking tissuecan, with care, be replaced. The tissue shouldalso be examined for signs of epithelializa-tion: a grey covering of cells may occur aftera day or so. If tissue covered by these cells isreplaced, further epithelial cell proliferationmay occur giving aberrant epithelialization ofanterior segment structures. This can cause
Cornea 57
Figure 5.12 Deep ulcer suturing. (a) Frontal/cross-section diagrams; (b) horizontal mattress sutures (smallulcers can be closed with just one horizontal suture; (c) horizontal sutures are slowly drawn tight; (d) initiallythe cornea is flattened but will return to normal within days

glaucoma if the sheet of growing cells coversthe pectinate ligament in the iridocornealangle.
In the case of prolapsed iridal tissue 24hours is again an important cut-off point.Before that time dehydration of prolapsedtissue is reduced by the fibrin overlying theprolapsed iris, as discussed above (Figure5.14). After this time both dehydration fromoutside, and vascular compromise caused bythe iris being entrapped in the cornealwound, tend to cause tissue death in theprolapsed iris.
There are two aims always to be kept inmind: that is, correct reposition of viable iristissue, as well as adequate closure of thecorneal wound. A shallow anterior chambershould first be deepened by the injection ofbalanced salt solution, or better still visco-elastic, through a paralimbal needle place-ment. Injection through the traumatic woundis more likely to compromise the structures tobe manipulated during repositioning andclosure. In some cases where the traumatic
wound is presented early, the iridal damageis minimal and iris adhesions to the exposedstroma have yet to occur, repositioning can beby pharmacological means. The pupillaryconstriction caused by intra-ocular depositionof carbachol or the dilation following intra-cameral 1:10 000 adrenaline may be sufficientto resolve the mild incarceration. More oftenthan not such a regimen is not effective andmechanical repositioning must be attempted.Visco-elastic irrigated into the wound orthrough a paralimbal paracentesis site may besufficient to break down early iridostromaladhesions but a more aggressive approach isoften needed (see Figure 5.12). The maintechnique used in such circumstances is oneof sweeping the iris off the corneal woundthrough a paralimbal incision with a cyclo-dialysis spatula or an irrigating cannula.Finally visco-elastic can be deposited toensure that the iris remains in a posteriorposition apposed to the lens and not thecornea, or an air bubble can be placed in theanterior chamber as shown opposite.
58 Veterinary Ocular Emergencies
Figure 5.13 Treatment of staphyloma or anterior synechiae

Cornea 59
Figure 5.14 Prolapsed iris. (a) Perforating corneal laceration – frontal and cross-section; (b) amputatedprolapsed iris, corneal iris adhesions reduced with an iris spatula and suturing of the wound; (c) suturing eyeswhich present with severe corneal oedema with horizontal sutures should seal the endothelial surface; (d)interrupted sutures placed between the horizontal mattress sutures ensure easy closure of the epithelial edge

The difficult question in these instances ishow much iris to excise and how much toreposition. Any iris which has been outsidethe eye for over 24 hours should be excisedand any iridal tissue which does not bleed onhandling and starting an excision should beremoved. During many such proceduresiridal bleeding is encountered. The use ofvisco-elastic tends to restrict the hyphaemaand keep blood localized so as to minimizeinterference with the surgeon’s operatingfield of view. Again 1:10 000 adrenalineirrigated into the anterior chamber willreduce haemorrhage substantially.
Where lenticular damage has also occurreda decision must be made regarding the advis-ability of performing lentectomy at the timeof primary anterior segment repair. The manyproblems associated with lentectomy in theface of other post-traumatic ocular complica-tions, such as corneal oedema or iritis, makeit unlikely that removal of lens materialwould be advisable at the time of primaryrepair. The one situation in which removal oflens material is required early in such oculartrauma management is when capsularrupture leads to the release of lens materialinto the anterior chamber, when a phacoana-phylactic reaction may occur.
5.4 Corneal foreign body®
5.4.1 Recognizing a corneal foreign body
It might seem easy to identify a cornealforeign body: a piece of plant material, athorn or a shaft of cat claw should readily bevisible in the transparent background of thecornea. Sometimes this is the case. But oftensignificant ocular pathology accompaniesthe foreign body. Considerable chemosismay obscure the ocular surface or cornealchange, such as oedema, infiltration orvascularization, and haemorrhage maycomplicate the view of a possible foreignbody. Often the pain which is associatedwith a corneal foreign body precludesdetailed observation. For all these reasonstopical anaesthesia is almost always essentialand sedation or brief general anaesthesiamay also be necessary.
Several features suggest that a cornealforeign body may be present. Pain is often,but not invariably, a feature. A discharge may
be present with corneal pathology such asoedema, infiltration and vascularization.After a traumatic incident giving rise to acorneal foreign body many animals are liableto hide away and not present to the owner fora period, giving time for these sequelae toarise. The problem is that, as well as compli-cating diagnosis, such signs make it signifi-cantly more difficult to remove the foreignbody.
If the foreign body is perforating the corneaone may see a uveitis or even a shallowanterior chamber with anterior synechiae or afibrin clot where there has been leakage. Insuch cases it is important to refrain fromattempting to remove the foreign body untilin an aseptic theatre situation with the animalunder anaesthetic, so that aqueous leakagethrough the resulting wound can be dealtwith.
In assessing a corneal foreign body it isimportant to note several features.
1. What is the foreign body? Plant materialcan be difficult to remove in one piece andmay carry potentially dangerous bacteria.It is preferable in such a case not only toculture a bacteriological swab from thetrauma site but also to place the materialitself on an agar plate and grow organismsdirectly from it.
2. How deeply is the foreign body penetrat-ing the cornea? A foreign body penetrat-ing the cornea completely but by only asmall amount may show few signs of thisuntil it is removed, when aqueous leakageoccurs. This is where careful observationfrom the side as well as in front will allowa better evaluation of depth. Other ocularsigns such as mild uveitis, with a slightanisocoria caused by miosis on theaffected side, will show that a penetrationis likely to have occurred. This is notalways the case, since a corneal irritativefocus can give rise to a reflex miosis,through a retrograde neural pathwayfrom the trigeminal nerve.
5.4.2 Dealing with a non-perforatingcorneal foreign body (Figure 5.15)
Removing a foreign body which does notperforate the cornea is clearly a much lesshazardous task than dealing with one which
60 Veterinary Ocular Emergencies

does penetrate the full thickness of thecornea. Yet the same care should be taken toensure complete immobility of the patientand good illumination and visibility: withoutthese it is all too easy to worsen the situationor even cause perforation.
The matter is urgent as a foreign body inthe cornea for over 24 hours will provoke aninflammatory corneal infiltrate and gradualdegradation of surrounding stroma, makingremoval more difficult. The presence ofaqueous flare is common, but more severeanterior segment inflammation and especially
a hypopyon should alert one to the possibil-ity of perforation.
First it may be that a very superficialforeign body can be removed simply byirrigation. In any case the ocular surfaceshould be well irrigated and sterilized beforean attempt to remove a more deeply lodgedforeign body is made. If an initial flushing ofthe cornea is unsuccessful, as will often be thecase, a more interventionist approach shouldbe taken.
The key instrument to be used in removingthe majority of foreign bodies is nothing more
Cornea 61
Figure 5.15 Treating a corneal foreign body

complicated than a 25 G needle. The mostimportant detail in using the needle is toemploy it at 90° to the entry track of theforeign body, as shown in Figure 5.12. In thisway one can be sure not to push the itemfurther into the corneal stroma. A movingglobe complicates matters considerably, sobefore removing the foreign body ocularstability must be ensured with haemostats orstay sutures anchoring the conjunctiva atthree points. Haemostats can be particularlyuseful because the one in line with the direc-tion of the entry track can be the fixationagainst which the foreign body can bewithdrawn, as shown in Figure 5.15.
There are times when the foreign body istoo deeply embedded to allow a simpleremoval: where no part of it protrudesbeyond the ocular surface. In such cases theeasiest method of removal is, using the fineneedle and always in the direction by whichthe foreign body will eventually be removed,to chisel away at the stroma immediatelysurrounding the surface end of the foreignbody, as shown in Figure 5.15. While this willcreate a small crater leaving a superficialulcer, it will allow a standard removal of theforeign body by the technique suggestedabove.
5.4.3 Dealing with a fully penetratingcorneal foreign body®
Ensuring globe stasis is even more importantwhere a full perforation of the cornea hasoccurred. Here we will consider managementwhere the foreign body is still within thebody of the stroma and thus is plugging thegap. Larger corneal injuries with involvementof a foreign body are considered under thesection on corneal laceration. How is it possi-ble to know, other than by careful clinicalexamination, that corneal perforation hasoccurred? If aqueous is leaking from the siteof foreign body entry the answer is clear butoften the small degree of swelling whichaccompanies corneal oedema tightly seals thewound, locking the foreign body in place.Then the Seidel test is useful.
With a corneal foreign body that haspenetrated the cornea, with some transientloss of aqueous there are four aims to beachieved in dealing with the problem (Figure5.15). Note that the following list ranks
neither these aims in order of importance norin the order in which they should beremedied.
• First, the foreign body should be removed,maintaining or regaining corneal clarity
• Second, the globe integrity should bemaintained, this being particularly impor-tant to remember if the corneal deficitafter foreign body removal is substantial
• Third, the inflammatory sequelae of lossof aqueous must be remedied or hopefullyprevented
• Fourth, intra-ocular or corneal stromalinfection should similarly be remedied orprevented.
The last two of these should be consideredfirst when dealing with a lacerated cornea.Antibiotic and anti-inflammatory treatmentshould be in place before attempting surgi-cally to correct the damage present as aconsequence of a penetrating foreign body.Intensive topical and systemic antibiosis iscritical given the likelihood that microbialcontamination will occur either in the cornealstroma or the anterior segment. Choosing theantibiotic to use has been covered above butit is important to repeat that the involvementof plant material as the foreign body mustalways alert one to the possibility of fungalinfection.
With any corneal perforation inflammatorysequelae can cause significant morbidity in theeye. In the case of a penetrating foreign bodythere may be considerable loss of aqueous asthe foreign body is removed. In this situationboth the loss and its prostaglandin-mediatedinflammatory consequences can be controlled.Where relatively little loss has occurred witha penetrating foreign body, there is ampleopportunity to give a topical non-steroidalanti-inflammatory agent such as flurbiprofen(Ocufen), diclofenac (Voltarol) or ketorolac(Acular) before attempting surgical removal.Where aqueous loss has already happened, asin a corneal laceration, any ameliorative anti-inflammatory action is rather late. However,surgical intervention will cause further fluidloss and inhibiting the prostaglandin-mediated inflammatory response as above isstill important.
After these partially reparative andpartially prophylactic steps have been taken,
62 Veterinary Ocular Emergencies

the foreign body can be removed. The impor-tant feature of such a removal, as with that ofa non-penetrating foreign body, is not tomake matters worse. It is so tempting to usea small pair of forceps and try to pluck theforeign body from the corneal surface. Toooften, however, this merely results in embed-ding the item further in the stroma or, worsestill, pushing it through into the anteriorchamber. Here it floats and is significantlymore difficult to apprehend and remove fromthe eye.
A foreign body embedded in and perfo-rating the depth of the stroma can becarefully removed with a needle as for thenon-perforating foreign body. It may benecessary to enlarge the entry wound witha needle or blade, having already stabilizedthe foreign body to ensure it is not lost intothe anterior chamber. The most difficultcases are those in which the majority of theforeign body has passed into the anteriorchamber leaving a small stub in the poste-rior stroma. In such a case removal shouldnot be retrograde, reversing the entry pathof the foreign body through the cornea, butfurther through the anterior chamber using
microforceps through a limbal incision(Figure 5.15).
5.5 Antibiosis and mydriaticcycloplegia in corneal emergencies
The reader is referred to the opening chapterof this volume for a fuller discussion of thediagnosis and treatment of infectious oculardisease. Again we emphasize the benefits oftaking samples and using in the first place abroad-spectrum antibiotic. The samples canbe examined directly after appropriate stain-ing with Gram’s method, Giemsa or Diff Quiktechniques and with lactophenol cotton bluefor fungal hyphal elements as well as forbacteriological and fungal culture.
With regard to analgesia, paralysis of theciliary body is a useful analgesic adjunct iniritis, as above. This also applies in cornealdisease where miosis is noted, the iridalspasm being caused by retrograde trigeminalnerve conduction. In every corneal conditionpresenting with apparent pain or a degree ofanisocoria, a mydriatic cycloplegic agentshould be used.
Cornea 63

6.1 Iritis®
Iritis is one of the key conditions causing thered eye. It can be painful and sight-threaten-ing and thus is an important condition calling
for immediate and sustained action. Inflam-mation of the iris is a relatively common condi-tion in small animal ophthalmology. It formsthe most obvious part of uveitis, inflammationof the uveal tract which also comprises theciliary body and the choroid. While interme-diate and posterior uveitis causing inflamma-tion of the ciliary body or choroid are notnoticed by the owner they can provide usefulsigns to the veterinary surgeon investigating auveitic eye.
6.1.1 Diagnosis: clinical signs
The classic signs of an anterior uveitis arerelated to anterior uveal inflammation, iridalmuscle spasm and, in many cases, ciliarybody dysfunction (Figure 6.1). The keyfeatures of inflammation have always beendefined as rubor, calor, tumor et dolor togetherwith reduction of function.
Rubor, redness, is seen in iritis in the increasedvasculature of rubeosis iridis. Iridal vasculatureis in some places dilated and in otherconstricted. Where vascular dilation occurs theiris appears criss-crossed with engorged vesselsgiving a rubeotic appearance, hence the termrubeosis iridis. In areas of vascular constrictionischaemia occurs. Ischaemic tissue releasesangiogenic factors which promote new bloodvessel formation seen as small vascular sproutsin rubeosis iridis. Redness is also manifest in theepisclera as the red eye and is due to vasculardilation secondary to inflammatory cytokineproduction.
Chapter 6
Iris
Emergency management of anterior uveitis
1. Perform full ophthalmic examination2. Measure intra-ocular pressure3. Evaluate possibility of systemic infection
(Gram-negative bacteria, Toxoplasma,viral disease)
4. Treat with mydriatic until mydriasis isachieved
5. Treat with topical steroid if no cornealulceration present, otherwise use topicalnon-steroidal agent
6. Treat with systemic steroid if severe ornon-responsive to topical steroid alone
7. Refer for treatment with tissueplasminogen activating factor ifsubstantial fibrin deposition occurs
Prognostic indicators in anterior uveitis
1. Substantial intra-ocular haemorrhage apoor prognostic sign
2. Substantial posterior synechiae non-responsive to mydriasis a poorprognostic sign
3. Concurrent posterior segment signs suchas retinal detachment a poor prognosticsign
4. Viral systemic cause a poor prognosticsign for the uveitis and the systemichealth of the animal

Calor, heat, is difficult to determine in theeye. Tumor, swelling, is seen in the swollendull-coloured iris. In some cases, especiallywith a lightly pigmented iris, the formation ofraised lymphoid follicles within the iris tissuecan be visualized, especially with a slit lampor slit setting in a direct ophthalmoscopewhich readily demonstrates a raised profile.
Dolor, pain, is a frequently presenting signin uveitis. It is predominantly related toiridal and ciliary body muscular spasm.Photophobia is also a classical sign, althoughexactly where the mechanism of photopho-bia lies is still unclear: it may be related tomuscular spasm as the pupillary light reflexoccurs. Knowing the mechanism of paingeneration is at the heart of ocular analgesia,
is very important and is discussed in section6.1.3.
The glory of the eye and of ophthalmologyis that tissue changes can be directly assessedby ophthalmoscopy. This is particularly truein uveitis. Early influx of leucocytes into theiris and the formation of lymphoid folliclesare often visible even at the very earlieststages. Thickening of the iris and loss of irissurface detail are other results of cellular infil-tration into the body of the iris. Leucocytediapedesis from the iris surface, and fibrinformation and release from iridal and ciliarybody vasculature result in flare. In flare, parti-cles such as cells and fibrin form a haze in theanterior chamber through the Tyndall effectwhen a beam of light is shone through theanterior chamber. With experience flare canbe graded, allowing a semi-quantitativeestimate of the degree of inflammation. Whilethis is not particularly useful in comparingdisease in different animals, it plays animportant part in determining whetheruveitis is improving under treatment.
A higher number of cells in the aqueousresults in deposit of cells on the posterior faceof the cornea as keratic precipitates. Thesemay have different appearances dependingon the type of cells and the inflammatoryprocesses involved. Non-granulomatousinflammation may show small keratic precip-itates with a wide distribution across thecornea. Granulomatous inflammation pro-duces larger keratic precipitates, often knownas mutton fat KPs. These may form a crescentin the inferior cornea Cells fall in thedownward current, as cooler aqueous falls inthe centre of the anterior chamber and thenrises at the limbus. The bicircular aqueouscurrents thus formed are slowest at the lowestpoint where they change direction (Figure6.1) and the cells are thus deposited in thisposition. If a larger number of cells enter theaqueous they fall under gravity to give ahypopyon in the ventral anterior chamber.Thus, the degree of anterior segment inflam-matory change can readily be assessed byvisualizing cell infiltration directly.
Posterior segment inflammation is impor-tant in investigations also. The uvea, asdetailed above, comprises the iris, the ciliarybody and the choroid. Fundoscopy of theuveitic eye may show anterior vitreal cell-related flare in pars planitis (intermediate
Iris 65
Figure 6.1 The classic signs of an anterior uveitisare related to anterior uveal inflammation, iridalmuscle spasm and, in many cases, ciliary bodydysfunction giving reduced intraocular pressure

uveitis), or chorioretinal inflammatory exu-date or retinal detachment in posterioruveitis. Where there is an anterior uveitis inone eye but on casual examination an appar-ently normal fellow eye, it is always worthperforming fundoscopy on both eyes even ifthis means waiting some time for mydriasisto take effect. Finding signs of a posterioruveitis in the other eye will make the differ-ence between topical therapy in the unilateralanterior inflammation and systemic anti-inflammatory medication in the bilateralpanuveitis.
Iridal muscle spasm manifests as pupilconstriction, miosis. This, combined with thereadiness of the pupil to adhere to the under-lying lens, produces posterior synechiaewhich can, in an untreated eye, result in apermanently miotic pupil or iris bombé. Inthe latter case iridal adhesion to the lensprevents movement of aqueous forwardthrough the pupil and hence gives a precipi-tous increase in intra-ocular pressure. Allthese possibilities render amelioration ofmiosis an exceptionally important factor intreatment of the uveitic eye, as discussed insection 6.1.5.
It may seem that the ciliary body, beinginvisible by routine fundoscopy, has fewsecrets to give away in the investigation ofthe uveitic eye. Yet when we consider reduc-tion in function as a key feature of inflamma-tion, the ciliary body gives the onlyquantifiable feature in uveitis: the level ofintra-ocular pressure. While it may bethought that the diagnosis of glaucoma is theonly reason for the measurement of intra-ocular pressure, determination of pressure inthe uveitic eye should perhaps be consideredequally important. A uveitic eye with a lowintra-ocular pressure has an active uvealinflammation, while a treated eye with ahigher (but still abnormally low) pressurethan at the previous examination, is an eyewith a resolving uveitis. Tonometry is thus akey diagnostic step in uveitis.
6.1.2 Diagnosis: diagnostic tests
It might be thought that the clinical appear-ance of a uveitic eye is sufficient foundationon which to base a diagnosis of uveitis. Clini-cal signs together with a measurement of alow intra-ocular pressure are indeed sufficient
66 Veterinary Ocular Emergencies
Emergency management of hyphaema
1. Perform full ophthalmic examination,noting concurrent signs of uveitis orglaucoma
2. Measure intra-ocular pressure and treataccordingly if raised
3. Perform ocular ultrasonography ifavailable, looking for tissue trauma orintra-ocular tumour
4. If recurring hyphaema without signs ofocular trauma, evaluate dog forhaemorrhage elsewhere and performcoagulation profile
5. Give topical steroids if ulceration is notpresent and signs of uveitis are present
6. Give topical NSAIDs if ulceration ispresent
7. Give topical atropine if uveitis ispresent but not if glaucoma supervenes
8. Tissue plasminogen activating factormay be useful in resolving a clot, butcare is needed as this can causefurther haemorrhage
Prognostic indicators in hyphaema
1. Signs of intra-ocular neoplasia areclearly a poor prognostic sign
2. Supervening glaucoma and thedarkening of the blood as it clots arepoor prognostic signs
3. Recurring hyphaema may signal asystemic coagulopathy or intra-ocularstructural defect involving vasculature,both of which are poor prognosticsigns
Differential diagnosis in hyphaema
• Ocular trauma• Uveitis• Intra-ocular tumour• Coagulopathy• Retinal detachment (in more chronic
detachments)• Retinal vascular haemorrhage (such as
occurs in Collie Eye Anomaly)
Thus work up for hyphaema shouldinclude:Further ocular examination (signs ofuveitis, lesions in fellow eye)Ocular ultrasound (retinal detachment,intra-ocular tumour)Coagulopathy work up (platelet count,clotting time, PPT, APT)

as a basis but confirmation can be gained byperforming a paracentesis. A cytocentrifuga-tion of 0.2 ml of aqueous will show the celltypes and indicate whether any infection ispresent by documenting local antibodyproduction. This might be seen as somewhatacademic, but the important diagnostic tests,especially in cats, are those which determinewhether a viral aetiology underlies the uveitis.Serology for FIP, FeLV, FIP and Toxoplasma isconsidered the standard systemic work uproutine in Britain. Note that with travel ofanimals abroad increasing recently Leishma-nia and Ehrlichia should be included asdifferentials for uveitis. In the USA serologyshould be carried out for fungal agents suchas Blastomyces and Coccidioides, which causesystemic fungal disease not infrequentlymanifesting as ocular disease. Bartonellahenslae is another organism recently foundassociated with feline uveitis. In all these casesdetermining the ratio of aqueous to serumantibody titre is vastly superior to serologyalone (Chauvkin et al. 1994).
A different set of pathogens may be impor-tant in equine recurrent uveitis: Leptospiraspecies and particularly L. interrogans havebeen found in a significant proportion ofcases while Brucella, Toxoplasma and possiblyequine herpes virus 1 may be involved.Documenting which organism is involved isprobably not particularly important, althoughtreatment of toxoplasmosis with a drug suchas clindamycin may be valuable in additionto the classical topical anti-inflammatories.
6.1.3 Treatment: pain relief
As has been noted above, pain relief in uveitisshould be an admixture of spasmolytic anale-gesia through cycloplegia, analgesia throughthe anti-inflammatory action of the non-steroidal agents and in addition classicalanalgesia with opiates if necessary. Earlyreduction of ciliary body spasm and earlyanti-inflammatory medication reduce painquite substantially without resort to the morepowerful systemic analgesics.
6.1.4 Treatment: anti-inflammatorymedication
Since inflammatory disease is at the heart ofuveitis, anti-inflammatory medication must
be at the centre of anti-uveitic therapy. Suchtreatment needs to be titrated relative to theseverity of the uveitis and its position. A mildanterior uveitis will require topical 1%prednisolone acetate. A severe uveitis withposterior segment involvement will requiresystemic (per os) predisolone at the anti-inflammatory dose of 1.5 mg/kg or evenazathioprine.
Subconjunctival injection in an alreadypainful eye can be eased dramatically by theapplication of topical anaesthetic. Merelyplacing a drop of proxymetacaine or ametho-caine in the eye will, however, have a limitedeffect. A much more effective protocol is tosoak a cotton-tipped swab in the anaestheticand press it onto the globe in the positionwhere the injection will be given. Thisproduces profound local anaesthesia in afocused area not just superficially on theconjunctiva but deep in the episclera andsclera.
6.1.5 Treatment: reducing miosis andpreventing synechia formation
One of the key concepts to bear in mind whenfaced with an emergency is that the first timethe patient is seen is the best (and sometimesthe only) opportunity to reduce disease activ-ity and signs. This is certainly the case withthe profound miosis seen in acute uveitis andthe formation of synechiae so common inintra-ocular inflammation.
A uveitic eye with a miotic pupil needsattention until the pupil is dilated, not a quickapplication of atropine and re-examination ina few days time. Often atropine is sufficientto produce mydriasis in a mild uveitis, buteven in such a case the response to a long-acting mydriatic such as atropine is difficultto gauge at the first consultation. A firstapplication of mydriatic should include tropi-camide as well as atropine to ensure rapidmydriasis. Should both of these fail, phenyle-phrine can be added and the three drugs usedtogether every 15 minutes until mydriasis isachieved. Should all topical mydriatics fail toact adequately, a subconjunctival injection of0.05 ml 1% atropine, 0.05 ml 1% tropicamideand 0.05 ml 10% phenylephrine should begiven. There is some risk of a systemicreaction and cardiovascular parametersshould be monitored immediately before and
Iris 67

after such a subconjunctival injection. There isevidence that reduction of inflammation willpromote the action of topical mydriatics.Thus, should mydriasis not occur it is worthhospitalizing the animal and trying againafter a few hours of intensive anti-inflamma-tory medication.
At this point it is important to note that useof powerful agents such as atropine in horsesmust be approached with caution. The possi-bility of development of ileus even withtopical use of atropine must always beremembered and use of an atropine ointment,with concomitant reduction of systemicabsorption, is to be recommended.
Another peculiarity of the equine eye is therecent use of vitrectomy to treat recurrentcases of uveitis (Frühauf et al. 1998). Theremoval of pathogens such as Leptospira maybe important, or it may be the removal of the‘soup’ of inflammatory mediators whichremain in the vitreous which is important.Nevertheless vitrectomy can certainly beuseful in reducing the frequency and severityof attacks in horses. It may be that in thefuture this approach will show benefit in thedog and cat also, where recurrent or persis-tent intra-ocular inflammation is a significantproblem.
6.2 Change in iris appearance
Clearly a case of iritis, as discussed above,will cause changes in iris appearance: newvascularization, iris swelling, miosis andiridal darkening all cause such changes.There are other lesions which alter irisappearance: neoplasia is one. Iris masses maybe primary tumours, part of a more general-ized disease such as feline lymphosarcomacomplex or a sign of metastolic disease froma tumour elsewhere.
The development of benign iris pigmenta-tion is another which may be rapidly devel-oping and therefore a potential neoplasmrequiring immediate intervention. The differ-ential diagnosis of a benign iris pigmentarynaevus and a diffuse iris melanoma can bedifficult, particularly in the cat (Williams1994). In some cases the raised profile of aniris melanoma above the iris is pathogno-monic but in other animals diffuse irismelanoma and iris naevi can appear identical.One might think that the naevi would becongenital and not change in appearancefrom birth. Yet in the authors’ experiencefeline iris pigmentation can develop rapidlyand in a multifocal manner which is indistin-guishable from melanoma. Given the poor
68 Veterinary Ocular Emergencies
Pathogenic mechanisms in uveitis
• Inflammatory cell infiltration lymphoid nodules in iris stroma inflammatory cells in keratic precipitates larger number of cells form hypopyon
• Iris ischaemia from vessel constriction giving rise to new vessel sprouts(rubeosis iridis)
• Pupillary constriction through muscular spasm producng miosis
• Iridal adhesion posterior synechiae (iris-lens adhesion) and also peripheralanterior synechiae which can lead to glaucoma
• Pain particularly through ciliary body spasm also because ofphotophobia (mechanism unclear)
Thus treatment must reduce inflammation (steroid and NSAIDs)
reduce pain (analgesics but also cycloplegics to reduceciliary spasm)
dilate pupil (mydriatic high dose frequency)

prognosis of feline iris melanoma once itreaches the iridal periphery and associatedlimbal and ciliary body vasculature, enucle-ation is the preferred option.
The key factor here, as in any veterinarymedicine, is without a doubt client commu-nication. In such a case the outcome canalways seem negative. If the lesion is neoplas-tic the cat has a chance of systemic metasta-sis. If the lesion is benign the eye will havebeen removed to no purpose. If the client isinformed that the condition may be benign,but that the eye should be removed in case aneoplasm is present, then the outcome canalways be presented as positive: either thelesion was neoplastic but we have removed it
early and therefore the prognosis is good; orthe lesion was benign so no neoplasm waspresent, the cat will live a normal, if unocu-lar, life and the client can be reassured thattumour was not present.
It may seem strange to include this sectionin a book on emergency ophthalmology. Yetin the emergency consultation optimal clientcommunication is supremely important. Thevery fact that the animal has been presentedas an emergency shows that owner is worriedby an acute problem. It is at this very pointthat the veterinarian’s calm well-informedmanner reassures the owner and ensures thatthe animal benefits through the strengtheningof the client–veterinarian relationship.
Iris 69

7.1 Introductory remarks
Glaucoma is a condition of increased intra-ocular pressure that may be seen in patientssecondary to intra-ocular inflammation,intra-ocular neoplasia or more often in thedog as a progressive disease resulting frominherited abnormality of the irido-cornealangle (Figure 7.1).
A large number of dog breeds have beenshown to have an inherited dysplasia ofstructures in the iridocorneal angle (ACVO1996, Whitley et al. 1995) shown in Table 7.1.Several features of glaucoma are particularlyimportant in an emergency situation but themain problem with glaucoma is the long-termcontrol of intra-ocular pressure either byocular medication or by surgery.
Glaucoma is a blinding, painful conditionand in many cases the changes which causepain and result in blindness occur in the firstfew hours of an acute episode of glaucoma
and need rapid treatment to reduce the intra-ocular pressure.
The key diagnostic aid in glaucoma ismeasurement of intra-ocular pressure. As wehave noted earlier, having a tonometer to
Chapter 7
Glaucoma
Table 7.1 Dog breeds predisposed to glaucoma
Akita Chihuahua Lakeland terrier Sealyham terrierAlaskan malaute Dalmatian Maltese Shih tzuAmerican cocker spaniel Dandie dinmont terrier Miniature pinscher Siberian huskyBasset hound Daschund Miniature schnauzer Skye terrierBeagle English cocker spaniel Norfolk terrier Smooth fox terrierBorder collie German shepherd Norwegian elkhound Tibetan terrierBoston terrier Giant schnauzer Norwich terrier Welsh springer spanielBouvier de Flandres Greyhound Poodle Welsh terrierBrittany spaniel Irish setter Samoyed West Highland White terrierCairn terrier Italian greyhound Scottish terrier Wire fox terrierCardigan Welsh corgi
Figure 7.1 Is this uveitis in the right eye orglaucoma in the left?

hand is important and acquiring and regularlyusing a Schiotz tonometer, as described inAppendix A, is highly recommended.
The long-term control of intra-ocularpressure should be undertaken by referral toa veterinary ophthalmologist.
An important aspect of glaucoma presentingunilaterally is the possible future involvementof the remaining visual eye. Several studieshave shown that topical anti-glaucoma treat-ment of the non-glaucomatous eye can preventor at least postpone the disease in this eye.
7.2. Diagnosis
7.2.1 Clinical signs
The eye with acute glaucoma is, together withglobe prolapse, one of the few extreme ocularemergencies. In the vast majority of cases theeye is red and painful and immediate reduc-tion in ocular pressure is required to amelio-rate these signs. More important in the longterm is the effect of high intra-ocular pressureon vision. The acutely glaucomatous eye isblind and, without a rapid reduction in intra-ocular pressure, this loss of vision will bepermanent.
7.2.2 Diagnostic tests
The key diagnostic test in glaucoma as werecognize it in veterinary ophthalmology ismeasurement of intra-ocular pressure (IOP).In human ophthalmology, while glaucoma
used to be defined as ocular disease associ-ated with increased IOP, the tendencyrecently has been to move away from IOP asthe defining criterion of glaucoma. Some eyeswith a raised IOP have no signs of oculardisease nor visual defect (Figure 7.2). In thesecases people are said to have ocular hyper-tension but not glaucoma. Conversely thereare a growing number of people with loss ofvisual fields as determined by perimetry anda cupped optic disc, the classic signs ofglaucoma, but with a normal or even lowintra-ocular pressure (Figure 7.3). These casesare termed ‘low tension glaucoma’, a descrip-tion which used to be considered an
Glaucoma 71
Figure 7.2 Normal (a) and abnormal (b) iridocorneal angle
(a) (b)
Figure 7.3 Closed iridocorneal angle

oxymoron. It may be wondered whatrelevance this has to the veterinary field. Theimportance is that glaucoma is now recog-nized as a disease with its origin not primar-ily in the iridocorneal angle, where all theattention used to be focused, but in the opticdisc. The optic neuropathy in classicalglaucoma is related to and indeed directlycaused by increased IOP. But optic nervechanges may be caused by degenerative orvascular changes in the nerve head as well asby the physical damage associated withincreased IOP. It is not being suggested thatwe should forget high IOP as the predomi-nant cause of glaucoma in animals, but ratherthat we should broaden our view regardingthe mechanisms underlying sight loss in thedisease. Currently this may have little impacton how we treat glaucoma in our patients,which are generally so much more advancedin ocular deterioration than are humanpatients who present with early glaucoma.But in the future new agents may be intro-duced adding to the small armamentarium ofanti-glaucoma drugs we possess at present.
7.3 Treatment
7.3.1 Immediate systemic hypotensivetherapy®
Treatment in the emergency situation wherea dog presents with a high IOP in primaryglaucoma is, and has been for many years, theuse of systemic hyperosmotic agents. Intra-venous mannitol at up to 2 g/kg or oralglycerol at 2 ml/kg acts to draw fluid fromboth the anterior segment of the eye and thevitreous humour. They act rapidly and forseveral hours reduce intra-ocular pressure by10+ mmHg, reducing a pathologically highpressure to normality. In an emergency situa-tion where no such agents are available orwhere a systemic condition such as renaldisease precludes use of a hyperosmoticagent, a 25 G needle can gently be driven atan angle through the sclera at the limbus,allowing aqueous just to fill the needle hubbefore the needle is withdrawn. Such a pro-cedure is not without complications: the rapidreduction of pressure by such a physicalmethod may result in intra-ocular bleedingand is probably only to be recommended
when performed by an ophthalmologist withexpertise in emergency management ofglaucoma. Systemic osmotic agents also havetheir disadvantages, particularly contra-indication in cases of renal failure. Since theyare to be used in the emergency situation,little time is available for a full renal work up.Nevertheless a careful history will ascertainwhether the animal is polydipsic and there-fore likely to have renal compromise. A rapidevaluation of blood urea can be performed inorder more fully to ensure that one is notgoing to save the eye while ignoring the moregeneral problems of the animal.
7.3.2 Long-term reduction of IOP®
The problem with a stabilized acute glaucomais what to do to maintain low pressure in aglaucomatous eye in the face of abnormallylow aqueous drainage. This question presentsitself soon after stabilization with oral orintravenous osmotic ocular hypotensivedrugs as discussed above, as it is not advis-able to give more than two administrations ofmannitol or glycerol to any one animal.
72 Veterinary Ocular Emergencies
Emergency management of glaucoma
1. Perform full ophthalmic examination2. Determine cause of glaucoma (inherited
with gonioscopic changes, post-uveitis,lens luxation etc.)
3. Measure intra-ocular pressure4. If IOP over 30 mmHg give 20% mannitol
solution intravenously at 1–2 g/kg over30 minutes
5. Start topical carbonic anhydrase inhibitortreatment at least q.i.d.
6. Monitor intra-ocular pressure hourly inacute phase
Prognostic indicators in glaucoma
1. Degree and duration of intra-ocularpressure increase are critical inprognosis
2. Degree of visual loss in eye important3. Presence of optic disc cupping a poor
prognostic sign4. History of previous ocular signs or
disease in other eye generally a poorprognostic sign

Detailed discussion of methods of long-term management of glaucoma might seeminappropriate here, as they are not aimed atthe emergency situation. Briefly, the optimallong-term management is surgical. Whilelong-term medical inhibition of aqueousproduction is possible, since the withdrawalof dichlorphenamide from the market no onedrug is particularly efficacious. NeverthelessTrusopt, a topical CAI, can be useful forcontrol of mild glaucoma.
More invasive methods to reduce aqueousproduction involve ciliary body ablation,either by trans-scleral photo-ablation using alaser or by trans-scleral cryosurgery. Whilethese carry a risk of severe damage to otherocular structures and associated intra-ocularinflammatory sequelae, they have been usedwith success in sighted eyes. Intravitrealgenticin has been used successfully pharma-cologically to ablate the ciliary body butshould be reserved for blind painful eyes (butprobably not in cats, for fear of causing po-sterior segment post-traumatic sarcoma). Thistreatment is not advised in the emergencysituation and the reader is referred topublished reports for further information.
Pharmacological reduction of aqueousformation by carbonic anhydrase inhibition
has been achieved with dichlorphenamide(Daranide) for many years, but now that thisdrug has been withdrawn in favour of thetopical dorzolamide (Trusopt) other agentswill have to be employed by those not favour-ing a surgical treatment. Acetazolamide(Diamox) is another carbonic anhydraseinhibitor but works less well than dichlor-phenamide and tends to have worse emeticand nauseous side effects. Methazolamide(Naptazane) has not, to our knowledge, beenassessed in dogs.
Other drugs regularly used in humanglaucoma relax the musculature of the ciliarybody. In the primate eye at least these have amajor effect on the outflow capacity of thedrainage pathways. Whether this is the casein the dog is rather unclear because dogs donot accommodate to a great extent. Theirciliary musculature is therefore not particu-larly well-developed and relaxing ciliarymuscle in non-primate mammals has lesseffect on the drainage pathways. This meansthat many of the drugs used in people havequestionable efficacy in dogs.
Nevertheless cholinergic miotics are usefulin the dog. They probably act in a morecomplex way in the dog than in man, widen-ing the sclerociliary cleft by a compoundaction involving the iris sphincter muscle aswell as the ciliary body musculature.Certainly demecarium bromide (Humorsol), along-acting anticholinesterase, worksextremely well but is only available in theUnited States. Pilocarpine, a direct-actingparasympathomimetic, is perhaps the mostcommonly used miotic. A single dose reducesintra-ocular pressure for six to eight hours;4% drops produce no greater pressure reduc-tion than do 2% drops, but a gel formulationgives longer-lasting pressure reduction, atleast in people.
Other ocular hypotensive preparationswhich could potentially be used in the doginclude adrenergic agonists acting on bothalpha and beta receptors. Topical alphaagonists, such as apraclonidine, causevasoconstriction of vessels in the ciliaryprocesses thus decreasing aqueous humourproduction. But they also dilate the pupil, withpressure-increasing effects in man but less soin the dog. Beta receptor effects of adrenergicagonists increase aqueous production but alsoact directly on the trabecular meshwork to
Glaucoma 73
Emergency therapy in glaucoma
Osmotic agentsMannitol 1–2 g/kg by intravenous infusionGlycerin 1–2 g/kg per os
ParacentesisLimbal placement of 25 G needleRemoval of needle when hub is filledwith aqueousPre-treatment with calcium channelblockers (e.g. verapamil) advised
Mechanisms of drug action in glaucoma
Reduction of aqueous productionCarbonic anhydrase inhibitorsBeta blockersAdrenergic agonists
Outflow facility modulationDirect and indirect cholinergic agonists

increase outflow. Thus an agent such asepinephrine, or the less irritant pro-drugdipivalyl epinephrine, variously increases anddecreases pressure through actions on alphaand beta receptors. In man, and in the dog, theoverall effect is to lower pressure. The compli-cating factor is that beta antagonists as well asagonists have pressure-lowering effects. Betablocking agents bind to receptors in the ciliaryepithelium and reduce aqueous secretion. Inhuman ophthalmology, timolol maleate has amajor role as a topical antiglaucoma drug.Timolol has no effects on the pupil, accommo-dation or outflow facility but can reduceaqueous production in man by nearly 50% atconcentrations as low as 0.25%. In the dog,concentrations up to 20 times that amount arerequired to give significant reductions in intra-ocular pressure (Gelatt 4% paper).
To return to the question regardingwhether glaucoma pathology is at the irido-corneal angle, where so many of these drugsact, or at the optic nerve head, it is now beingsuggested that perhaps the beta blockers havemore effect on the vasculature around theoptic nerve head than they do on the irido-corneal angle or the ciliary body. Indeed thereare other workers who claim that by reduc-ing aqueous production with medicationthese drugs are starving the iridocornealangle cells of the nutritious aqueous theyneed to survive – possibly iridocorneal anglepathology is being made worse!
7.3.3 Neuroprotection
As noted above a recent change of emphasishas occurred in glaucoma pathophysiology.The focus on ocular damage from merelyhigh intra-ocular pressure caused byimpaired iridocorneal angle drainage hasmoved to effects of pressure and other factorson the optic nerve head and its vasculature.
We have known for many years that disccupping leads to visual impairment. Anextension of that concept leads to thehypothesis that blindness in glaucoma ispredominantly related to optic nerve pathol-ogy. Does this change of emphasis changeour treatment regimens for glaucomapatients? In one sense it changes nothing.For the vast majority of canine and felineglaucoma patients the problem is high intra-ocular pressure and the necessary treatmentlowers that pressure. But in another sense itchanges a lot. If optic nerve damage is thefocus of glaucoma pathology then at leastpart of our glaucoma therapy should beaimed at neuroprotection.
The sort of tissue changes and mechanismsat the heart of optic nerve damage relate toevents such as calcium influx to nerve cellsafter damage. Any neural damage, be itrelated to a head injury, a cerebrovascularaccident or pressure-induced damage ofganglion cell axons in the optic nerve head,produces a chain reaction of neurotransmit-ter-related events resulting in the opening ofneural ion channels which allow the lethalinflux of calcium ions into neurons. If this canbe prevented, perhaps by the use of calciumchannel blockers such as verapamil, some ofthe long-term damage associated with thesudden rise in IOP in acute glaucoma (seenso often in dogs with compromised irido-corneal angle aqueous drainage) may also beprevented.
This, however, is all in the future – the keyfactors in diagnosing and treating glaucomain the emergency situation are being able torecognize the signs, confirm the diagnosis bytonometry and then lower the pressure withsystemic osmotic ocular hypotensive agentsbefore deciding what to do for the long-termimprovement of aqueous drainage in suchcases.
74 Veterinary Ocular Emergencies

Conditions of the lens presenting asemergencies are luxation and damage. Muchregarding this latter situation is coveredabove as a complication of globe perforationbut here the consequences of lens rupturewill be noted. The only other acute conditionof the lens which could present as anemergency is a rapidly progressing cataract,such as is seen in diabetes. This also isdiscussed here, although the diagnosis isnormally easy and management is cataractextraction. Sudden onset cataract might notbe covered as an emergency in some texts. Itis sufficiently concerning for owners to bepresented as an emergency and therefore iscovered here.
8.1 Lens luxation®
The clearest emergency presenting as adisease of the lens is lens luxation. Once seennever forgotten: lens luxation is obvious in itspresentation once one knows what to lookfor. The characteristics of the animal involvedcan be very instructive This condition oftenoccurs in middle-aged terrier breeds andsudden ocular pain or discomfort in such adog should focus one’s attention on lensluxation as a likely diagnosis. The ocularsigns can be immediately diagnostic. There isa red eye with raised pressure and an aphakiccrescent where the lens is obviously displacedfrom its normal central position, leaving anarea where an uninterrupted tapetal reflex
can be seen between lens and pupillarymargin (Figure 8.1). If there are also lenschanges such as cataract the edge of the lenscan be seen even more clearly and thediagnosis be made.
In other cases the lens luxates completelyinto the anterior chamber. Here it may bepossible to see reflected light beautifullyoutlining the lens (Figure 8.2). In such a casean area of corneal oedema often occurswhere the lens presses on the cornealendothelium.
Unfortunately, diagnosis is not so easy inmany cases. Lens luxation may occur anteri-orly followed by a falling back of the lensbehind the iris and diagnosis can be difficultif an aphakic crescent is not obvious. Sincethe iris is not supported by the lens posteri-orly in such cases it wobbles on slight manip-ulation of the head. As ‘iris wobble’ soundsless than 100% scientific, the term iridodone-sis is used.
Signs of lens luxation are
• Lens clearly present in anterior chamber• Lens clearly eccentric in position with an
aphakic crescent visible• Lens less obviously displaced but
iridodonesis occurring
Another complication in the presentation of adog with lens luxation is that the conditiondoes appear in breeds other that the terriersin which it is a clearly inherited trait. Andeven more confusingly, while glaucoma can,
Chapter 8
Lens

and often does, occur secondary to lensluxation, lens luxation itself can occursecondary to glaucoma. Thus the manage-ment of a luxated lens is not always lentect-omy. When the luxation occurs as a result ofglobe enlargement removal of the lens will donothing to ameliorate ocular signs. Theglaucoma which has caused buphthalmosmust originate elsewhere. This may be at theiridocorneal angle, a primary goniodysgene-sis glaucoma or perhaps through peripheralanterior synechiae following uveitis. Thedifferentiation of whether glaucoma followslens luxation, or lens luxation followsglaucoma, relies on two questions.
• Is there a reason for glaucoma other thanthe lens luxation?
• What is the primary ocular defect –zonular breakdown or globe enlargementfollowing glaucoma?
This calls, as do all ophthalmologicalquestions, for a close examination of theglobe. Look in particular for
• the position of the lens – use a slit beam ifpossible
• a possible area of corneal oedema in thecentral cornea suggestive of current orprevious anterior lens luxation
• vitreal strands protruding into the aqueous• any signs of subluxation in the other eye• the size of the globe – visual inspection
and the presence of Haab’s striae orDescemet’s fractures. These are caused by
76 Veterinary Ocular Emergencies
Note: reflected light often outlines thelens in the anterior chamber
Figure 8.1 Subluxation of lens

the posterior influx of aqueous humourinto the stroma at the sites of rupture inDescemet’s membrane. An enlarged globewith an acute lens luxation suggests thatthe lens luxation is secondary
• any other signs of disease producingglaucoma – inflammation or neoplasia.
In the cat, lens luxation is almost alwaysseen following glaucoma, uveitis or rarelytrauma (Olivero et al 1991). The mechanismof zonule breakdown subsequent to uveitis isunclear but this link with other ocular abnor-malities shows, yet again, the importance ofassessing the whole eye and not just focusingon the obvious abnormality. The link withuveitis is noteworthy, both because it showsthe importance of assessing the underlyingcause of intra-ocular inflammation in suchcases (see Chapter 6) and also because theanterior segment in such cases is already in astate of inflammatory activity. Entry into theglobe in such circumstances should not beattempted without considerable local (topical)and systemic anti-inflammatory medicationbefore surgery.
8.2 Diabetic cataract®
As noted above, it might seem surprising toclass any cataract as an emergency, but fromtime to time owners fail to recognise earlysigns of lenticular opacification in theiranimal and see a complete cataract as asudden change. The animal’s visual distur-bance is the first sign they notice and thewhite cataract the second. With suchunobservant owners the cataract may be thefirst sign they notice of their animal’sdiabetes, polyuria and polydipsia havingbeen missed or ignored. Cataract can occurvery rapidly in an uncontrolled diabeticanimal. The markedly increased glucoselevels in the lens swamp the classic EbdenMyerhoff metabolic pathway. This allowsexcess glucose to be metabolized by theenzyme aldose reductase which is normallynot able to act on the sugar at low concen-trations, given its lower affinity for thesubstrate. Aldose reductase converts glucoseinto sorbitol and this insoluble sugar createsan osmotic gradient across the cell membraneand leads to lens fibre swelling, and then
irreversible opacification. Management ofthis situation is lentectomy by extracapsularextraction, or more frequently today phaco-emulsification. The important factor here isrecognition that the cataract is secondary todiabetes: every cataract case should undergoa full haematological and serum biochem-istry profile as a key part of the work upbefore surgical treatment.
8.3 Lens capsule rupture andphacoanaphylactic uveitis®
In circumstances where lenticular traumaliberates lens proteins, severe, almost anaphy-lactic changes in the eye are seen, termedphacoanaphylactic or phacoclastic uveitis. Inthe majority of these instances rupture of thelens capsule by a penetrating foreign body isresponsible for release of lens material. Atypical setting is a thorn or cat-claw injury tothe globe, typically through the cornea. Thusin any case of corneal damage it is importantto assess the anterior surface of the lenscapsule. If a means of magnification is not tohand, fluorescence such as a Wood’s lamp ina dark room will help detect any damage: thelens will autofluoresce to some degree, aidingobservation of capsular rupture or perfora-tion.
In one interesting situation trauma fromwithin the lens itself causes capsularrupture. This is the case of lens-induceduveitis in the rabbit where the protozoanparasite Encephalitozoon cuniculi, transmittedvertically from mother to offspring in utero,is found in the lens of the young adultrabbit. In some circumstances these proto-zoan larvae rupture the capsule and a lens-induced uveitis follows. This does notappear to be a phacoanaphylactic uveitis assuch, rather a phacoclastic inflammationwith a white inflammatory focus occurringin the anterior chamber. This must be differ-entiated from a Pasteurella multocida uveitiswhich could give a similar white purulentinflammatory deposit. Discussion of suchcases is beyond the remit of this volume,since these animals are not generallypresented as emergencies but rather aschronic problems.
In cases of lens rupture aggressive anti-inflammatory treatment is advised, such as
Lens 77

topical dexamethasone or prednisoloneacetate 3–4 times daily. Removal of the lensat this stage by phaco-emulsification is proba-bly the best treatment option while medicaltreatment with anti-inflammatories may be
sufficient in mild cases. In many cases asevere uveitis with secondary glaucomasupervenes and the removal of the lens byphaco-emulsification is probably the thera-peutic route to be recommended.
78 Veterinary Ocular Emergencies

9.1 Retinal detachment
Retinal detachment presents as an emergencywhen it occurs bilaterally with sudden visualimpairment and often complete blindness.Several systemic or ocular conditions may bethe cause of a retinal detachment. A key aim
of full diagnostic work up in retinal detach-ment is thus the investigation of whether andwhich of these diseases is the cause of thedetachment. On the other hand, there areretinal detachments which are the result ofintra-ocular abnormalities such as anomaliesof the vitreous, retina, optic disc or choroid.For this reason a full ocular examination ismandatory, this including scleral indentation,in order to visualize the peripheral retinawhere many tears leading to detachmentoccur. Sometimes it may be difficult to seewhat is actually happening in the eye, asextensive haemorrhages after the detachmentmay impair visual diagnosis. Ocular ultra-sound equipment provides very valuableinformation in such circumstances. Thetypical features of a retinal detachment areshown in Figure 9.1 and Table 9.1.
One systemic disease which may be anunderlying cause is hypertension, eitheralone or associated with chronic renal failureor hyperthyroidism, more so in the cat thanthe dog. An ocular condition leading todetachment which may be part of a systemicdisease is posterior uveitis. While this canoccur on its own, it can be part of a systemicauto-immune condition such as uveoderma-tological syndrome (VKH or Vogt-Koyanagi-Harada-like disease) in which peri-ocularloss of pigmentation (poliosis and vitiligo) isseen. Retinal detachment can occur as part ofa recognized ocular syndrome in a specificbreed such as retinal dysplasia in theBedlington or Sealyham terrier, or Collie eye
Chapter 9
Retina and vitreous
Emergency management of retinaldetachment
1. Perform full ophthalmic examination2. Define whether detachment is
rhegmatogenous (with retinal tear) ornon-rhegmatogenous
3. Determine whether systemic disease(hypertension, inflammatory focus etc.)is present
4. Manage hypertension with amlodipineper os
5. Manage posterior uveitis withprednisolone per os
Prognostic indicators in retinal detachment
1. Prolonged detachment before diagnosisa poor prognostic sign, as retinalatrophy often occurs with time
2. Rhegmatogenous detachment moredifficult to treat than non-rhegmatogenous
3. Association with hypertension a goodprognostic sign, as medical treatmentoften resolves detachment in such cases
4. Association with posterior uveitis apoorer sign, as complete resolution isless common

80 Veterinary Ocular Emergencies
Table 9.1 Differential diagnosis of retinal detachment
Pathogenesis of detachment
Exudative detachment – inflammatory or exudative fluid between neuroretina and RPE
Rhegmatogenous detachment – retinal tear causes detachment
Traction detachment – vitreal bands pull neuroretina away
Differential diagnosis
Exudative detachment: – UveitisHypertension
Rhegmatogenous detachment – TraumaDetachment associated with hypermature cataract
Traction detachment – TraumaPost-inflammatory
Figure 9.1 (a) Total funnel detachment visible through pupil; (b) detachment with disinsertion; (c) partialdetachment with retinal dysplasia; (d) partial detachment with optic nerve coloboma

anomaly in the Collie breeds. It can occurfollowing a space-occupying lesion such as atumour in the retrobulbar space or can followtrauma. With regard to the globe itselfdetachments can occur at the rim of acoloboma of the optic disc, these beingrelated to anatomical abnormalities of retinaladhesion at the edge of the optic disc.
The relationship between the vitreous andthe retina are important in maintaining theretina correctly positioned. Vitreal degenera-tion, which occurs in many older animals, canlead to vitreal cavitation with liquefaction(synchysis scintillans). This condition shouldbe differentiated from asteroid hyalosis andposterior vitreal detachment. Here the attach-ment of the vitreous to the inner retina fails.In the majority of animals this goes unnoticedand causes no visual disturbance. It may,however, cause peripheral retinal tears,which can extend centrally to give significantvisual disturbance. Rhegmatogenous retinaldetachments, i.e. those associated with retinaltears, most often occur between theneuroretina and the retinal pigment epithe-lium as the connection between these twostructures is tenuous. Non-rhegmatogenousdetachments occurring after serous exudationinto this intraretinal space (commonly butrather confusingly termed the subretinalspace) also manifest at this weak point of theretina. Cataracts and lens luxations may causeretinal tears; retinal detachment may be acomplication of cataract surgery in animals.
Some detachments associated with asystemic problem such as hypertension occuralmost simultaneously in both eyes. Alterna-tively it may be that one detachment haspreceded the other by some considerableperiod, and that the visual deficit is notnoticed until the second eye is affected andthe animal becomes completely blind. By thatstage treatment is difficult and often notparticularly effective for the eye with thelong-standing detachment, but certainly stillworth attempting for that eye and also for theeye with the recent detachment.
Ideally, blood pressure measurementshould be undertaken using either an oscillo-metric sphygomomanometer or a dopplerunit which, being relatively cheap, should beavailable in every larger practice for monitor-ing blood pressure during anaesthesia as wellas the less for diagnosis of hypertensive
retinopathy. Hypertensive cats are often inearly to moderate or severe renal failure ormay be typical of feline hyperthyroidism,with signs such as weight loss and tachycar-dia. Amlodipine in the cat (0.625 mg daily)often results in retinal re-attachment andrestored vision, but management of theunderlying cause is vital.
Other causes of retinal detachmentspresenting as emergencies can be rapid fluidoverload in renally compromised animals inwhich case bullous retinal detachments canbe seen (Martin 1999).
9.1.1 Examination of the animal with aretinal detachment
The fundus is readily examined by ophthal-moscopy using either direct or indirectmethods. With direct fundoscopy the retinacan be seen in focus only with the directophthalmoscope on a setting of over 0 D,indicating that the retina is placed anterior toits normal position at the most posterioraspect of the globe. With binocular indirectophthalmoscopy a three-dimensional view ofthe retina is obtained showing clearly that itis detached. When the retina balloons to thefront of the vitreous is readily visible evenwithout an ophthamoscope, through thewidely dilated pupils resulting from lack ofvisual stimulus. It usually looks like a veryfine silk veil floating behind the lens. Asnoted above scleral indentation allows acomplete view of the peripheral retina. Localanaesthetic should be applied to the eye anda scleral indentor used gently to push theglobe inwards behind the limbus. Using thehead-mounted binocular indirect ophthalmo-scope and full mydriasis, the portion of theperipheral retina indented can be visualizedand checked for retinal degeneration orretinal tears.
The eye with a retinal detachment devel-oping as a consequence of hypertension mayoften have several tell-tale signs beforecomplete detachment occurs. Retinal vesselsmay be tortuous and appear like a chain ofsausages with lengths of vessel constrictionand dilation. Retinal haemorrhages and/orvascular exudates may be seen with smallareas of flat detachment occurring beforebullous exudative detachments lead on tocomplete detachment.
Retina and vitreous 81
When unilateral detachment is seen, usefuldiagnostic information can be gained fromexamination of the fellow eye. Often this hasdisease at an earlier stage, in a progressivedisease such as hypertension. Alternatively itmay be that the other eye shows signs of acondition with multiple ocular features one ofwhich can lead to retinal detachment, such asoccurs in retinal dysplasia or Collie eyeanomaly. In the former the apparentlyunaffected eye may have retinal folds ormultifocal areas of dysplasia; in the latterthere may be a coloboma or chorioretinaldysplasia.
In animals, particularly cats, in which ahypertensive aetiology is likely, indirectblood pressure measurement is essential for afull diagnostic work up. Doppler sphygmo-manometry has been reported in dogs andcats as being successful, although the morereliable (and more costly) method of oscillo-metric measurement reported recently givesmore reproducible results (Bodey and Michell1996). Certainly direct measurement requir-ing an arterial line is not necessary tomeasure blood pressure in cats and dogsnow, and measurement of mean bloodpressure should be within the grasp of anyinterested veterinarian. Time is required toensure that several reproducible results froma calm animal are obtained. The normalmeasurements reported in the literature canbe found in Bodey et al. 1994, Bodey andMichell 1996. The differences in normalvalues between different breeds of dogshould be noted. A consistently high readingin a dog or cat should alert one to the likeli-hood of a hypertensive detachment, althoughsuch a finding in an animal with a detach-ment does not necessarily prove a causativerelationship. Essential hypertension, althoughcommon in people, is not seen frequently indogs and cats. Animals with a finding ofhypertension should be investigated for renaldisease and, in the case of cats, also for hyper-thyroidism.
9.1.2 Treatment of retinal detachmentsecondary to hypertension
In the absence of renal disease or hyperthy-roidism, hypertension may be treated with acalcium channel blocker such as amlodipine(Istin). For cats 0.625 mg s.i.d. (1⁄8 of a 5 mg
tablet of amlodipine) in the evening is suffi-cient to give a significant reduction in bloodpressure (Henik et al. 1997). It is sometimesimpractical to prescribe 1⁄8 of a tablet and1.25 mg (1⁄4 tablet) has yielded no side effectsin our experience. The frequency of sponta-neous retinal re-attachment after normaliza-tion of blood pressure is difficult to assess,but is high enough to convince that the treat-ment is worth pursuing. In many cases whileone retina is chronically detached, thesecond eye has a recent detachment givingrise to the total blindness which alerts theowner and leads to presentation of theanimal.
The authors have seen amlopidine therapyused to good effect in cats with hypertensiveretinopathy and renal disease. Lowering theblood pressure will have beneficial effects onthe chronic renal failure as well. The chroni-cally detached retina may not be functionaleven if re-attachment occurs, but the acutelydetached retina often regains useful functionafter antihypertensive treatment has beensuccessfully implemented.
9.1.3 Treatment of retinal detachment inposterior uveitis
Retinal detachment in a case such as a Vogt-Koyanagi-Harada-like syndrome in the dog isrelated to inflammatory changes causingeffusion into the subretinal space. The breedsfound to be affected with VKH-syndromeinclude Akika, Siberian husky, Chow chow,Golden retriever, Samoyed, Irish setter,Shetland sheepdog, Saint Bernard, OldEnglish sheepdog and Australian shepherd(Martin 1999). The main presenting signsinclude sudden blindness, bullous retinaldetachments and secondary glaucoma. Insuch cases aggressive anti-inflammatorytreatment with systemic prednisolone at1.5 mg/kg or with azathioprine at 2 mg/kgs.i.d. reducing to 0.5 mg/kg. Forty-eighthours is required for steroid effects althoughazathioprine requires a longer period to gainefficacy.
Fungal disease can be a cause of retinaldetachment following granulomatous retini-tis or choroiditis associated with systemicinfection with organisms such as Crypotococ-cus neoformans or Neosporum canis. Diagnosiscan be by visualization of organisms on a
82 Veterinary Ocular Emergencies

vitreous tap or by serum antigen detection.Treatment is with agents such as itraconazole(Carlton et al. 1976, Jacobs et al. 1997).
9.1.4 Treatment of idiopathic retinaldetachment
Retinal detachment which has occurredwithout an obvious predisposing cause maybe rhegmatogenous or non-rhegmatogenous,see section 1.9.1. The treatment of these twoforms differs in some important respects.
Rhegmatogenous detachments are besttreated surgically with one of three techniques.Scleral contour can be altered to bring thesclera in apposition to the detached retina byscleral buckling. Alternatively re-attachmentcan be achieved by production of a chorioreti-nal scar though cryosurgery, diathermy ortranspupillary photocoagulation. Thirdlysubretinal fluid can be drained trans-sclerally.Recently complex vitreoretinal surgericaltechniques used in human ophthalmologyhave been performed in the dog. All of thesetechniques clearly should be attempted only ata specialist referral clinic. The reader is thusdirected to more comprehensive texts andpapers in the specialist literature for informa-tion regarding specialist vitreoretinal surgery(Smith 1999, Vainisi and Packo 1995).
9.2 Sudden acquired retinaldegeneration
The diagnosis of sudden acquired retinaldegeneration (SARD) is based on a historyof sudden unexplained visual deteriorationand a complete absence of retinal responseon electroretinography. Performing an
electroretinogram (ERG) in such cases mightseem academic as there is no treatment forSARD. The test is, however, essential todifferentiate from problems where the ERGdoes show retinal activity and a centralcause for the blindness must be sought.
While the history of sudden visual lossmight seem a clear one, investigation of anumber of cases in our clinics and thefindings of several others show that what istermed sudden visual loss can cover quite arange of circumstances. Some animals arevisual one minute and then blind a momentor two afterwards, this state remainingpermanently. This severe manifestationremains however quite rare. The majority ofdogs finally diagnosed as having SARD havesuffered a rapidly progressing but not ultra-rapid deterioration in sight, perhaps over amatter of a few days. It is the ERG whichdetermines the diagnosis in these cases.
No mechanism is understood for thissudden visual deprivation and no identicalcondition is seen in man, or apparently inanimals, other than the dog. A similar condi-tion in man known as cancer-associatedretinopathy occurs, particularly with smallcell carcinoma of the lung. These patients cansuffer with sudden loss of vision and there isan associated finding of circulating antibodiesto recoverin, a molecule in the visual pathwaywhich has antigenic similarities to a moleculefound in small cell carcinoma cells. No associ-ation with a neoplastic process has beenreported in dogs with SARD, but many havehypothalamopituitary axis defects such asCushing’s syndrome or at least abnormalACTH stimulation tests (Van der Woerdt etal. 1991, Mattson et al. 1992). Dogs presentingwith SARD should thus be evaluated for suchendocrine abnormalities.
Retina and vitreous 83

10.1 Optic neuritis®
Optic neuritis generally presents as suddenblindness and as such the differentialdiagnosis includes sudden acquired retinaldegeneration and central blindness. Here theclinical feature allowing a diagnosis to bemade is optic nerve swelling. The problem isthat the appearance of optic nerve headswelling is very difficult, if not impossible,to differentiate from the papilloedema whichcan be seen with a space-occupying lesionthat could present as central blindness.
Generally, however, the difference is thatoptic neuritis produces visual dysfunction,whereas papilloedema does not unlessresulting from an intracranial lesion whichconcurrently causes blindness. Optic nervehead swelling is characterized by a domedenlargement of the optic papilla with a fuzzyindistinct border to the disc and surfacehaemorrhages. It is the authors’ experiencethat optic neuritis is more likely to presentwith haemorrhage at the optic disc than ispapilloedema, although vessels of the opticdisc are engorged in both. To date, however,we have no definitive evidence that this isthe case.
The big question centres around whatother neurological inflammatory foci may bepresent. A full neurological examination ismandatory and the use of computerizedtomography (CT) or magnetic resonanceimaging (MRI) is invaluable to show if otherinflammatory lesions are occurring intra-cranially. Optic neuritis occurs in humans aspart of multiple sclerosis and in dogs as amanifestation of granulomatous meningo-encephalitis (GME). It is thus essential thatother manifestations of GME be investigated.Whether other neurological lesions arefound or not, the treatment is systemicsteroid at an anti-inflammatory dose andthis may need to continue for a significanttime if recurrence of blindness on cessationof treatment is to be avoided. If the patientcannot be seen by a veterinary ophthalmol-ogist for electroretinography, or referral for
Chapter 10
Optic nerve
Emergency management of optic neuritis
1. Perform full ophthalmic examination2. Specifically evaluate pupillary light
reflexes and swinging light test3. Evaluate other neurological parameters
with suspicion of diseases such as GME4. Give systemic steroid at 1–2 mg/kg
Prognostic indicators in optic neuritis
1. Duration of blindness an importantprognostic sign, more than five dayspoor
2. Degree of optic nerve swelling andhaemorrhage potentially a poor signalthough can resolve on aggressivetreatment
3. Degree of optic disc pallor an importantsign as this suggests the onset of opticatrophy

CT/MRI, the veterinary surgeon has thevision of the animal to gain and nothing tolose by using anti inflammatory agents.
Retrobulbar optic neuritis has the sameeffects on vision without the fundus changesseen where the optic nerve head is involved;high resolution retrobulbar ultrasound can beuseful in defining it. The incidence of thiscondition is not clear, but apparently low.
10.2 Central blindness®
Blindness not associated with disease of theglobe or the extracranial optic nerve can be
associated with intracranial mass lesions.These may have effects on vision predomin-antly through two mechanisms. One is a risein intracranial pressure while the other isdirect effect on the visual pathways. The mostcommon lesion producing an acute decreasein vision is a tumour at the level of the opticchiasm causing chiasmal compression. Mostoften these are pituitary macro-adenomaswhich may, or may not be associated withhormonal imbalances and such obviouschanges as polydipsia and polyuria. All theseintracranial lesions require a neurological aswell as an ophthalmological, and quite possi-bly also an oncological referral.
Optic nerve 85

1. Performing the Schirmer teartest
The pack is opened and the little snip is bentinside the plastic pack. With one hand thelower eyelid is everted and the snip is placedlike a hook over the eyelid margin. The eyelidis returned to rest on the eye. Care must betaken to avoid the test strip falling out onceplaced, and if the animal is agitated theeyelids may be held slightly closed to preventloss of the strip.
After one minute the STT-strip is removedand the reading noted. The STT-strip mayhave a colour indicator (Schering-Plough/Eagle Vision). If no markings are onthe STT-strip the length of wetted paper mustbe measured against the STT-strip pack or aruler.
With a little practice the clinician will beable to place two strips in each eye at thesame time and thus perform the Schirmer teartest in both eyes simultaneously.
While a number of reports havedocumented different ranges of normalvalues in various species, it can be said that aSchirmer tear test over 15 mm/min demon-strates a normal tear production in the cat ordog In the dog a value under 5 mm/min isindicative of keratoconjunctivitis sicca and avalue between 5 and 10 mm/min suggestsearly or mild changes in the aqueouscomponent of tears. In the cat some animalswith a healthy ocular surface have very lowreadings but in general the same figures can
be applied. Small mammals have, under-standably, lower tear production and in somespecies such as the rabbit the little researchcarried out demonstrates substantial differ-ence in STT values between different breeds.
2. Measurement of the intra-ocularpressure (IOP) with Schiotztonometer
While the optimal tonometer for small animaluse is considered to be the Tonopen applana-tion tonometer, the much cheaper Schiotzindentation tonometer can, with practice, beused accurately to assess intra-ocularpressure.
An anaesthetic is instilled topically onto thecornea. The nose of the animal is held in anupright position so the cornea is horizontal.Then the Schiotz tonometer is applied to thecornea and the reading is noted. It is import-ant that the foot of the tonometer is on thecentral cornea as the identation of the sclerawill cause a faulty reading of the intra-ocularpressure.
The Schiotz tonometer is an indentationtonometer, where hardness of the eye isinversely proportional to the indentation (i.e.a higher reading indicates a lower intra-ocular pressure and a low reading indicateshigh intra-ocular pressure). The reading onthe scale is correlated to the intra-ocularpressure by using a table. Friedenwald’sresearch in the 1950s resulted in a table for
Appendix A (compiled by T. Evans)
Diagnostic methods used in veterinaryophthalmology

human values. (Friedenwald 1957). Since thenpapers have been published proposing theuse of different tables for Schiotz tonometryon the canine eye (Peiffer et al. 1977a, Peifferet al. 1977b), but the latest conclusions arethat the original Friedenwald table revised in1955 (Friedenwald 1957) is the most accurateand applicable to the dog (Miller and Pickett1992a). The Friedenwald Table from 1955 isshown below for weights 5.5 g, 7.5 g and10.0 g, and may also be used in the cat (Millerand Pickett 1992b), although Schiotz tonome-try is more easily performed in the dog.
The optimal method of using the Schiotztonometer takes several measurements withdifferent weights which make possible a moreaccurate estimation of the intra-ocularpressure. Separate readings with the 5.5 g,7.5 g and 10 g weights can be used with thegraph depicted below using data from theoriginal Friedenwald table. The best estimateof intra ocular pressure is the y axis intercept.
88 Veterinary Ocular Emergencies
Friedenwald's Normogram 1955
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
0 5 1 0 1 5 2 0
Schiotz Tonometer Scale reading
IOP
mm
Hg
5.5g
7.5g
10.0g

Acuity: the ability to see the details of an objectseparately and unblurredAphakic: without lens – as in aphakic crescent inlens luxationAsteroid hyalosis: deposition ofchlolesterol/calcium deposits in vitreous humour.See Synchysis scillitansBlepharospasm: excessive blinking, tonic orclonic spasm of the m. orbicularis oculi. Associ-ated with irritation or pain of the eye, most oftencorneal painBuphthalmos: enlargement of the globe due tochronic glaucomaCAI (carbonic anhydrase inhibitor): drug thatreduces aqueous humour formation in the treat-ment of glaucomaCataract: an opacity within the lens. Must bedifferentiated from nuclear sclerosis (q.v.)Chalazion: chronic inflammatory granulomaresulting from retention of secretion from a meibo-mian glandChemosis: oedema of the conjunctivaChronic superficial keratitis (pannus): super-ficial predominantly lymphocytic inflammation ofthe cornea seen as a distinct entity in dog breedssuch as the German Shepherd and CollieCiliary flush: a diffuse, rose-red colorationsurrounding the cornea as a result of congestionof the branches of the anterior ciliary arteries, incyclitis, iridocyclitis or deep keratitisCornea: the transparent front part of the eyejoining the sclera at the limbusDescemetocoele: a forward building of Descemet’smembrane through a weakened or absent cornealstroma as a result of trauma or a deep corneal ulcer
Distichiasis: hairs growing from the meibomianglandsEctopic cilia: hairs growing from areas thatshould be devoid of hair. Usually on the palpebralconjunctiva, and with origins in the meibomianglands as these evolutionarily were hair folliclesEctropion: eversion of the eyelid margin. Mostoften seen in giantdog breeds such as SaintBernard, Chow Chow etc. Often the patients havea chronic exposure conjunctivitisEnophthalmos: recession of the eyeball into theorbitEntropion: turning inward (inversion) of theeyelid. Most commonly the lower eyelid, and oftenassociated with trichiasisEnucleation: surgical removal of the globeERG (electroretinography): an electrophysio-logical method of measuring the retinal responseto lightEvisceration: surgical removal of the contents ofthe globe followed in most cases by implantationof a silicone sphere as a prosthesisExenteration: surgical removal of the globe andextra-ocular structures. Indication for extentera-tion is infection of the eye and orbital tissuesand/or metastatic neoplasiaExophthalmos: an abnormal protrusion of theeyeball from the orbit. Physiological in brachy-cephalic breedsFacet: depression in the cornea covered by cornealepithelium and seen after corneal ulceration withloss of corneal stromal tissueFlare (aqueous flare, Tyndall’s effect): thescattering of a thin beam of light as it transversesthe anterior chamber, caused by an increase in the
Appendix B (compiled by T. Evans)
Ocular dictionary

protein content of the aqueous humour. A sign ofuveitis. May be graded 1 to 4Follicular conjunctivitis (plasmoma):conjunctivitis often seen in conjunction withpannus, in which lymphoid follicles give a nodularappearanceFornix (of the conjunctiva): the part of theconjunctiva that joins the palpebral and the bulbarconjunctiva, and which is unattached to the eyelidor the eyeball. Much deeper in the dog than in thehuman, it may be difficult to obtain cells from thefornix for exfoliative cytologyGlaucoma: increased intra-ocular pressure.Often manifests with dilated pupil, negative PLR,corneal oedema and potentially breaks indescemets membranes (Haab’s striae)Gonioscopy: optical examination of the irido-corneal angle using a goniolens and a means ofmagnificationHaab’s striae: Breaks in descemets membranecausing aqueous humour to impede into thecorneal stroma.The breaks are caused by globestretching. See GlaucomaHordeolum: external hordeolum is a purulentinfection of a sebaceous gland along the eyelidmargin. Internal is an acute purulent infection ofa meibomian glandHorner’s syndrome: sympathetic denervation tothe eye resulting in miosis, ptosis and enophthal-mosHyphaema: accumulation of red blood cells/bloodin the anterior chamber. Usually associated withcoagulopathy, uveitis, feline hypertension orocular traumaHypopyon: accumulation of pus in the anteriorchamber. The pus usually sinks to the bottomfilling the lower angle of the anterior chamberIridodonesis: trembling of the iris when the eyeis moved (by examiner). Associated with lensluxationKeratic precipitates (KPs): cellular deposits onthe posterior surface of the cornea, usually inassociation with iritis or iridocyclitisKeratoconjunctivitis sicca (KCS): decreasedquantitative tear production resulting in patho-logical changes of the cornea and conjunctivaLagophthalmos: the eyelids do not meet whensupposed to be closed. Test by applying touch tolateral canthus. If lagophthalmos is present thecentral cornea may be exposed during sleep, thusdehydrating. Often a central corneal ulcer isconcurrent with lagophthalmosLens-induced uveitis (LIU): uveitis induced byleakage of lens protein
Limbus: the junction of the cornea and scleraLymphocytic/plasmacytic conjunctivitis: con-junctivitis often seen with pannus in whichlymphoid follicles give a nodular appearance or, inless severe cases, a generalized red conjunctivaMeibomianitis: inflammation of the meibomianglands resulting in qualitative tear film diseaseand increased evaporation of tearsMiosis: decrease in pupil size. Seen in uveitis andin Horner’s syndrome (q.v.)Mydriasis: increase in pupil size. Often seen inglaucoma or in nervous animals, particularly catsNuclear sclerosis: the natural ageing of the lenscauses impaction/hardening of the nucleus of thelens, as the growth of lens fibres continuesthroughout lifePannus: see Chronic superficial keratitisParacentesis: sampling aqueous humour fromthe anterior chamber by means of a hypodermicneedle inserted at the limbusPhotophobic: an abnormal intolerance or fear oflight. Often associated with uveitisPlasmoma: see Follicular conjunctivitisPRA (progressive retinal atrophy): a congeni-tal progressive blindness found in a number ofcanine breeds and the Abyssinian cat. Diagnosisis by ERG (q.v.). Ophthalmoscopically retinalvessels are attenuated and the retina is hyper-reflectiveProptosis: protrusion of the globe beyond theeyelids (see Exophthalmos)Ptosis: drooping of the eyelid. Usually a sign ofneurological deficit as seen in Horner’s syndromeor facial nerve paralysis. May also be seen inenophthalmosSARD (sudden acquired retinal degenera-tion): blindness characterized by rapid onset andflat electroretinogram – of unknown causeStaphyloma: a bulging or protrusion of thecornea or the sclera usually containing adherentuveal tissueSynchysis scillitans: liquefaction of the vitreous,to be differentiated from asteroid hyalosis. If thehead of the animal is shaken synchysis scillitanswill show an appearance of bright dots fallingfrom the sky. In asteroid hyalosis the white opaci-ties are fixed within the corpus vitreous and onlyvibrate after a shakingSynnechae: anterior, posterior. Adhesion of theiris to the cornea or to the capsule of thecrystalline lensTarsorraphy: tying the eyelid margins togetherwith sutures, mostly applying horizontal mattresssutures or a horizontal Lembert suture pattern
90 Veterinary Ocular Emergencies

Trichiasis: inversion of eyelashes thus touchingthe eyeball and causing irritaion, most oftenassociated with normal hair in an abnormalposition, such as in entropionUvea: iris, ciliary body and choroid. Anterioruvea: iris and ciliary body. Posterior uvea: choroid
VKH (Vogt-Koyonagi-Harada syndrome): aninherited auto-immune disease, where melanin isthought to be the antigen. It is phagocytosed,resulting in posterior uveitis, poliuosis andvitiligo with depigmentation of peri-ocular andother structures
Appendix B 91

Appendix C (compiled by T. Evans)
International ocular drug formulary
Trade Generic Formulation Company Action
Acular Ketorolac 0.5% drops Allergan NSAIDAK-CON™ Naphazoline HCI 0.1% drops Akorn Anti-HAK-NaCI® Sodium Chloride 5% ointment Akorn OsmoticAK-TAINE® Proparacaine HCI 0.5% Akorn AnaestheticAK-TROL Dexamethasone 0.1%, Akorn Steroid A-pos/neg
Neomycin sulphate, Polymixin B
Albalon 0.1% Naphazoline HCI 0.1% drops Allergan Anti-HAlcaine Proparacaine HCI 0.5% drops Alcon AnaestheticAlomide Lodoxamide 0.1% drops Alcon Anti-HAmethocaine Amethocaine 0.5% drops generic AnaestheticAtropine Atropine 0.5–1% drops generic AntimuscarinicAureomycin Chlortetracycline 1% ointment Lederle A-pos/neg ChlaAzopt Brinzolamide 1% drops Alcon CAIBacitracin Bacitracin 500–1000 units/ml Upjohn A-pos (Staph)Betnesol Betamethasone 0.1% drops Medeva SteroidBetnesol-N Betamethasone and Medeva Steroid + A
neomycinCepravin Cephalonium 8% ointment Schering-Plough A-pos/neg
Animal HealthChloromycetin Chloramphenicol 1% ointment Goldshield A-pos/negCiloxan Ciprofloxacin 0.3% drops Alcon A-pos/negCiproxin Ciprofloxacin 2 mg/ml 50 ml bottle Bayfarm A-pos/negDaranide Dichlorphenamide 50 mg tabs Merck & Co CAIDiamox Acetazolamide 125/250/500 mg tabs Wyeth Lederle CAIExocin Ofloxacin 0.3% drops Allergan A-pos/negFinadyne Flunixine meglumine Inject/granules Schering-Plough NSAID
Animal HealthFluorescein Fluorescein 1 or 2% minim drops Chauvin DyeFML Fluorometholone 0.1% drops Allergan SteroidFucithalmic Vet Fusidic acid 1% ointment LEO A-pos (Staph)Garamycin Gentamicin 3% Schering A-negGenticin Gentamicin 0.3% Roche A-negGlauctabs Methazolamide tabs Akorn CAIGlaupax Acetazolamide 125/250 mg tabs Orion Pharma CAIHerplex Idoxuridine 0.1% drops Allergan V-HHumorsol Demecarium bromide 0.25% drops Merck & Co Parasympatho-
mimeticsIntron-A Interferon alpha-2b 5x10E6 IU/ml Schering-Plough V-H

Appendix C 93
Istin Amlodipine 5 mg, 10 mg tab Pfizer Ca-channelblocker
Ketofen Ketoprofen 5 mg tabs, inj Fort Dodge NSAIDAnimal Health
Lacri-lube White petrolatum, Allergan Artificial mineral oil, lanolin tears/ocular derivatives lubricant
Lissamine green Lissamine green Dry powder Sigma-Aldrich DyeLivosten Levocabastine 0.05% drops Ciba-vision AntihistamineLysine L-lysine 250 mg tabs generic V-HMannitol Mannitol Fluid for i.v. generic OsmoticMaxidex Dexamethasone Drops Alcon SteroidMaxitrol Dexamethasone 0.1%, Drops Alcon Steroid A-pos/neg
Neomycin Sulphate, Polymixin B Sulphate
Methazol-amide USP Methazolamide 25 mg and 50 mg Lederle CAIMuro-128 Sodium chloride 5% ointment Bauch & Lomb OsmoticMydriacyl Tropicamide 0.5% Alcon AntimuscarinicNebcin (a) Tobramycin 40 mg/ml inj Lilly A-negNeptazane Methazolamide Tabs Stortz Ophthalmics CAINorvasc Amlodipine 2.5 mg, 5 mg, Pfizer Ca-channel
10 mg tabs blockerOcufen Flubiprofen 0.03% drops Allergan NSAIDOphthaine Proparacaine HCI 0.5% drops Bristol-Myers AnaestheticOptimmune Cyclosporine 0.2% ointment Schering-Plough T-cell inhibOralcon Dichlorphenamide 50 mg tab Alcon CAIPhenylephrine Phenylephrine 10% drops generic Sympathomi-
meticPilocarpine Pilocarpine 0.5-3% drops generic MioticPred forte Prednisolone acetate 1% drops Allergan SteroidRimadyl Carprofen Tab/inj Pfizer NSAIDRose Bengal Rose Bengal 1% minim vials Chauvin DyeSandimune Cyclosporine 50 mg/ml Novartis T-cell inhibitor
1 ml/5 ml ampsStroxil Idoxuridine 0.1% drops Smith Kline & V-H
FrenchTobrex Tobramycin 0.3% drops Alcon A-negTrusopt Dorzolamide 2% drops MSD CAIVira A Vidarabine 3% ointment Parke Davis V-HViroptic Trifluridine 1% drops Borroughs V-H
WellcomeVistamethasone Betamethasone 0.1% drops Martindale SteroidVoltarol/Voltaren Diclofenac 0.1% drops Ciba-Vision NSAIDXalatan Latanoprost 50 μg/ml Pharmacia & Prostaglandin
Upjohn analogueZinacef Cefuroxime 250/750 mg amp Glaxo Wellcome A-posZovirax Acyclovir 3% eye ointment Glaxo-Wellcome V-H
200 mg, 400 mg and 800 mg tabs
Varieties of the same drug sold under different names are included inthe above table. Most of these (generic) drugs are from Akorn, asthis is the largest generic eye drug company in the US. In other partsof the world most of the products may be made up in localpharmacies or hospital pharmacies if the original product is not used.
AbbreviationsNSAID: Non steroid anti-inflammatory drugAmp: ampoulesA: antibioticA-neg: antibiotic for Gram-negative infectionA-pos: antibiotic for Gram-positive infectionA-pos/neg: antibiotic for Gram-negative and Gram-positive infectionCAI: carbonic anhydrase inhibitorChla: ChlamydiaDye: ocular diagnostic dyeStaph: staphylococcusV-H: antiviremica against herpes-virus (including stimulation of
immune response)
Trade Generic Formulation Company Action

General instructions for eye medicationOnly apply one drop to each eye. Alwayswait a minimum of five minutes betweentopical applications in the same eye, or reflextearing may wash out the first application. Ifpossible hold the head of the animal flexedback for up to one minute after application sothat more drug is absorbed by ocular tissuesbefore draining through the nasolacrimalduct (to be absorbed systemically).
Dosages for intra-vitral injection of antibi-otics in treatment of enophthalmitis. Ifperforming intra-vitral injections it is ofutmost importance not to damage the lens asthis will lead to lens-induced inflammation
Drugs that are difficult to obtain in yourcountry may be supplied by IDIS(www.idis.co.uk)
94 Veterinary Ocular Emergencies
A good fortified topical antibiotic solution foruse in the horse may be made as follows:
Nebcina (tobramycin) 4 vials of 40 mg in 1 ml:160 mg/4 ml
Zinacef (cefuroxime) 250 mg disolved in 3 mlsterile water: 250 mg/3 ml
Serum (from centrifuge-spun blood taken fromthe horse) 5 ml
This will constitute a solution of1.3% tobramycin + 2.1% cefuroxime +collagenase-inhibitors from the serum.If the serum is spun in an EDTA-tube, EDTA’santi-collagenase action will be included in thesolution.This solution should be refrigerated and bediscarded after 48 hrs and a new batchmade up.
Drug Dosage (up to) Species
Ciprofloxacin 100–250 μgram RabbitGentamicin 100 μgramCefazolin 2.25 mgCeftriaxone 5 mg RabbitVancomycin 1 mg

95
adnexa
cornea
retina
Name
i.d.
species
age/sex
history
lens/anterior chamber

ACVO (1996). Ocular disorders presumed to beinherited in purebred dogs, Genetics Commit-tee of the American College of VeterinaryOphthalmologists.
Barnett, A. (1990). Color atlas of veterinaryophthalmology. Wolfe.
Barnett, K.C., Crispin, S.M., Matthews, A. andLavach, D. (1995). Color atlas and text ofequine ophthalmology. Mosby-Wolfe.
Bodey, A.R. and Michell, A.R. (1996).Epidemiological study of blood pressure indomestic dogs. J Small Anim Pract, 37,116–125.
Bodey, A.R., Young, L.E., Barthram, D.H. etal. (1994). A comparison of direct andindirect (oscillometric) measurements ofarterial blood pressure in anaesthetiseddogs, using tail and limb cuffs. Res Vet Sci,57, 265–269.
Brooks, D.E., Andrew, S.E., Biros, D.J. et al.(2000). Ulcerative Keratitis caused by beta-hemolytic Streptococcus equi in 11 horses.Veterinary Ophthalmology 3, 121–126.
Chambers, E.D. and Slatter, D.H. (1984).Cryotherapy (N2O) of canine distichiasisand trichiasis: an experimental and clinical report. J Small Anim Pract, 25,647–659.
Chauvkin, M.J., Lappin, M.R., Powell, C.C. etal. (1994) Toxoplasma gondii specificantibodies in serum and aqueous humourof cats with experimental toxoplasmosis.Am J Vet Res 55, 1244–1249.
Crispin, S.M. and Barnett, K.C. (1997). Felineophthalmology. Saunders.
Dolowy, W.C. (1987). A safe, simple treat-ment for follicular conjunctivitis. Vet Med,790–792.
Eisner, G. (1990). Eye Surgery. Springer-Verlag, New York.
Feenstra, R.P.G. and Tseng, S.C.G. (1992).What is actually stained by Rose Bengal?Arch Ophthalmol, 110, 984–993.
Fischer, C.A. (1995). Ocular FelineHerpesvirus. A ten step approach to clientcommunications. Veterinary Forum, 48–50.
Friedenwald, J.S. (1957). Tonometer calibra-tion. Trans Am Acad Ophthal Otol, 61,108–123.
Frühauf, B., Ohnesorge, B., Deegen E. andBoevé, M. (1998). Surgical management ofequine recurrent uveitis with single portpars plana vitrectomy, Vet Ophthalmol, 2,137–152.
Gaiddon, K., Kaswan, R.L., Hirsh, S.G. (1996)Radial keratotomy and third eyelid flap:Results of a novel approach to treatment ofnonprogressive stromal ulcers and defectsamong dogs and cats. Veterinary andComparative Ophthalmology 6, 218–219.
Gelatt, K.N. (1978). Veterinary ophthalmicpharmacology and therapeutics. VM Publish-ing Inc, Bonner Springs, Kansas.
Gelatt, K.N. (1979). A modified subpalpebralsystem for the horse. J Eq Med Surg, 3,141–143.
Gelatt, K.N. (1999). Veterinary ophthalmology.3rd edn. Lippincott, Williams and Wilkins.
Gerding, P.A. and Kakoma, I. (1990). Micro-biology of the canine and feline eye.
Bibliography (compiled by T. Evans)

Veterinary Clinics of North America. J Small Anim Pract, 20, no. 3, May. Saunders.
Grant, R.L. and Acosta, D. (1994). Compara-tive toxicity of tetracaine, proparacaine andcocaine evaluated with primary cultures ofrabbit corneal epithelial cells. Exp Eye Res,58(4), 469–478.
Helper, L.C. and Magrane, W.G. (1970).Ectopic cilia of the canine eyelid. J SmallAnim Pract, 11, 185–189.
Henik, R.A., Snyder, P.S. and Volk, L.M.(1997). Treatment of systemic hypertensionin cats with amlodipine besylate. J AmAnim Hosp Assoc 33(3), 226–234.
Kleinfeld, J. and Ellis, P.P. (1966). Effects oftopical anesthetics on growth of microor-ganisms. Arch Ophthalmol, 76, 712–715.
Lavach, J.D. (1990). Large animal ophthalmol-ogy. Mosby.
Lavach, J.D., Thrall, M.A., Benjamin, M.M.and Severin, G.A. (1977). Cytology of thenormal and inflamed conjunctiva in dogsand cats. J Am Vet Med Assoc, 170(7),722–727.
Lawson, D.D. (1973). Canine distichiasis. JSmall Anim Pract, 14, 469–478.
Martin, C.L. (1999). Ocular manifestations ofsystemic disease. The dog. In: Gelatt, K.N.(ed.). Veterinary ophthalmology, 1401–1448.Lippincott, Williams and Wilkins.
Mattson, A., Roberts, S.M. and Isherwood,J.M.E. (1992). Clinical features suggestinghyperadrenocorticism associated withsudden acquired retinal degenerationsyndrome in a dog. J Am Anim Hosp Assoc,28, 199–202.
Miller, P.E. and Pickett, J.P. (1992a). Compar-ison of the human and canine Schiotztonometry conversion tables in clinicallynormal dogs. J Am Vet Med Assoc, 201(7),1021–1025.
Miller, P.E. and Pickett, J.P. (1992b). Compar-ison of the human and canine Schiotztonometry conversion tables in clinicallynormal cats. J Am Vet Med Assoc, 201(1),1017–1020.
Miller, W.W. and Albert, R.A. (1988). Canineentropion. Compendium of Continuing Educa-tion. 10(4), 431–438.
Nasisse, M.P., Guy, J.S. and Davidson, M.G.(1989). In vitro susceptibility of felineherpesvirus-1 to vidarabine, idoxyuridine,trifluridine, acyclovir or bromovinyl-deoxyuridine. Am J Vet Res, 50, 158–160.
Nasisse, M.P., Guy, J.S., Stevens, J.B. et al.(1993). Clinical and laboratory findings inchronic conjunctivitis in cats: 91 cases(1983–1991). J Am Vet Med Assoc, 203(6),834–837.
Neer, T.M. (1984). Horner’s syndrome:anatomy, diagnosis and causes.Compendium of Continuing Education, 6 (6),740–746.
Olivero, D.K., Riis, R.C., Dutton, R.G. et al.(1991). Feline lens displacement. A retro-spective analysis of 345 cases. Prog VetComp Ophthal, 1, 239–244.
Peiffer, R.L., Gelatt, K.N. and Gwin, R.M.(1977a). Schiotz calibration table for thecanine eye. Canine Practice, 49–51.
Peiffer, R.L., Gelatt, K.N., Jessen, C.R. et al.(1977b). Calibration of the Schiotz tonome-ter for the normal canine eye. J Am Vet MedAssoc, 38(110), 1881–1889.
Prince, J.H., Diesem, C.D., Eglitis, I andRuskell, G.L. (1960). Anatomy and histologyof the eye and orbit in domestic animals.Charles C Thomas.
Quinn, A. (2000). Corneal diseases in felines:treatments and comments. Proc ASVO, April2000, p. 17. Toronto.
Ramsey, D.T. and Fox, D.B. (1997). Surgery ofthe orbit. In: Nasisse, M.P. (ed.). Surgicalmanagement of ocular disease. VeterinaryClinics of North America. 27(5), 1215–1264.
Ramsey, D.T., Hamor, R.E. and Gerding, P.A.(1995). Clinical and histological manifesta-tions of extraocular polymyositis of dogs.Trans Am Coll Vet Ophthalmol, 26, 37.
Schmidt, G.M. (1977). Problem orientedophthalmology part 4: Corneal ulceration.Mod Vet Pract, 25–28.
Severin, G.A. and Thrall, M.A. (1981). Ocularexfoliative cytology. Proc 5th Kan Kal,11–15.
Smith, P.J. (1999). Surgery of the canine poste-rior segment. In Veterinary Ophthalmology,ed by Gelatt, K.N., Lippencott, Williamsand Wilkins, London 935–980.
Speiss, B.M., Wallin-Haakanson, N. (1999).Diseases of the Canine Orbit. In VeterinaryOphthalmology, ed by Gelatt, K.N., Lippen-cott, Williams and Wilkins, London,511–534.
Spreull, J.S.A. (1966). Symposium: TheCorneal Ulcer I. Anatomy and physiologyof the cornea of the dog. J Small Anim Pract,7, 253–255.
98 Veterinary Ocular Emergencies

Ugomori, S., Hayasaka, S. and Setogawa, T.(1991). Polymorphonuclear leukocytes andbacterial growth of the normal and mildlyinflamed conjunctiva. Ophthalmic Res, 23,40–44.
Vainisi, S.J., Packo, K.H. (1995). Managementof giant retinal tears in dogs. Journal of theAmerican Veterinary Medical Association 15,491–495.
Van der Woerdt, A., Nasisse, M.P. andDavidson, M.G. (1991). Sudden acquiredretinal degeneration in the dog: Clinicaland laboratory findings in 36 cases. ProgVet Comp Ophthal, 1(1), 1–18.
Walde, I. (1990). Atlas of opthlmology in dogsand cats. B.C Decker Inc.
Whitley, R.D., McLaughlin, S.A. and Gilger,B.C. (1995). Update on eye disorders
among purebred dogs. Vet Med, 90,574–592.
Wilkie, D.A and Whittaker, C. (1997). Surgeryof the cornea. Vet Clin North Am: SmallAnim Pract, 27(5), 1067–1107.
Williams, D.L. (1994). Feline iridal disease –local and systemic implications. FelinePractice, 22, 22–30.
Wills, M., Bounous, D.I. and Hirsch, S. (1997).Conjunctival brush cytology: evaluation ofa new cytological collection technique indogs and cats with a comparison toconjunctival scraping. Vet Comp Ophthalmol,7: 74–81.
Wolfley, D. (1987). Excision of individualfollicles for the management of congenitaldistichiasis and localized trichiasis. J PediatrOphthalmol Strabismus, 24(1), 22–26.
Bibliography 99

Abscess:retrobulbar, 29stromal, 6
Acetazolamide, 73, 95Acetylcysteine, 53Acid burns, 53Acuity, 92Acyclovir, 28, 96Adrenaline, 36, 58, 60Alkaline burns, 53Alpha agonists, 73Amethocaine, 8, 67, 95Amlodipine, 82, 96Anaemia, 22Analgesia, 7–8
corneal emergencies, 63iritis, 68
Antibiotic treatment, 6, 97cellulitis, 30conjunctivitis, 26–7corneal emergencies, 64corneoscleral laceration, 54foreign body, 60ulceration, 43, 51–3dacryocystitis, 28drug delivery, 9lid laceration, 24penetrating globe injury, 36resistance, 6, 53
Antiviral treatment, conjunctivitis, 27, 28Apraclonidine, 73Aqueous humour:
Flare, 18lipid laden, 18, 20
Asteroid hyalosis, 81, 92
Atropine, 8, 56, 67, 68, 95Azathioprine, 31, 68, 82
Bacitracin, 95Beta agonists, 74Betamethasone, 95, 96Blepharospasm, 92Blindness:
central, 20, 85glaucoma and, 71optic neuritis, 84retinal detachment and, 79sudden acquired retinal degeneration
(SARD), 83sudden blindness, 19–20
Bovine virus diarrhoea (BVD), 21Brinzolamide, 95Bullous keratopathy, 47Buphthalmos, 92Butorphenol, 8
Calor, 65Canine adenoviral hepatitis, 22Canine distemper, 21, 22Carbachol, 58Carbonic anhydrase inhibitors (CAI), 73,
92Carprofen, 8, 96Cataract, 18, 56, 81, 92
diabetic, 18, 20, 75, 77Cats:
antibiotic treatment, 6conjunctivitis, 27feline dysautonomia, 22feline herpes virus infection, 21, 22, 27–8, 40
Index

Cats: (Contd)corneal ulceration and, 43feline infectious peritonitis, 21iris melanoma, 68lens luxation, 77retinal detachment, 81, 82See also Specific conditions
Cefuroxime, 96Cellular infiltration:
aqueous humour, 18cornea, 17
Cellulitis, 6orbital, 29–30
Central blindness, 20, 85Cephalonium, 95Cephalosporin, 30Chalazion, 92Chemical injury, 53Chemosis, 92Chlamydiosis, 21, 22Chloramphenicol, 6, 56, 95Chlortetracycline, 6, 44, 95Ciliary flush, 92Ciprofloxacin, 53, 95Clindamycin, 67Collie eye anomaly, 19, 79–81, 82Conjunctiva:
assessment, 1foreign body, 28fornix, 93
Conjunctivitis, 6, 25–8follicular, 93keratoconjunctivitis sicca, 28–9lymphocytic/plasmacytic, 93redness and, 12–14
Cornea, 37–63, 92cellular infiltration, 18erosion, 37, 40, 42foreign body, 60–6management of non-perforating foreign
body, 60management of penetrating foreign body,
62–3recognition of, 60laceration, See Corneoscleral lacerationlipid deposition, 17oedema, 17–18, 42, 60, 62scar tissue, 17, 18
Corneal glue, 48Corneal ulceration, 29, 37–53
causes of, 42–3management, 44–53chemical injury ulcers, 53melting ulcers, 51–3
near-penetrating/penetrating ulcers anddescemetocoeles, 48–51
partial thickness stromal ulceration, 47–8recurrent or persistent non-healing
superficial ulcer, 44–7simple healing superficial ulcer, 44ulceration secondary to bullous
keratopathy, 47melting ulcer, 51–3ophthalmic stains, 37–40pain and, 16, 37prognostic indicators, 37ulcer depth, 40ulcer healing, 42
Corneoscleral laceration, 35, 54–60involvement of other ocular structures, 56penetrating corneal foreign body, 62–3prognostic indicators, 54repair, 56–60corneal laceration complicated by iris
inclusion, 57–60simple non-penetrating corneal laceration,
56simple penetrating corneal laceration, 56–7
Cyclosporine, 43, 96Cytology brushes, 5
Dacryocystitis, 28Demecarium bromide, 73, 95Descemetocoele, 37, 40, 42, 92
management, 48–51Descemet’s fractures, 76, 77Dexamethasone, 35, 95, 96Diabetes mellitus, 21, 22Diabetic cataract, 18, 20, 75, 77Dichlorphenamide, 73, 95, 96Diclofenac, 47, 62, 96Diff Quik (Giesma) stain, 6, 63Dipivalyl epinephrine, 74Dirofilariasis, 22Distichiasis, 12, 16, 25, 92
corneal ulceration and, 42treatment, 16
Dogs:antibiotic treatment, 6canine adenoviral hepatitis, 22canine distemper, 21, 22corneal ulceration, 44–5glaucoma, 70–3globe prolapse, 33keratoconjunctivitis sicca, 28lens luxation, 75–8retinal detachment, 79–81, 82See also Specific conditions
102 Index

Dorzolamide, 73, 96Drug delivery systems, 9–11
nasolacrimal lavage, 9–10spray medication, 11subconjunctival delivery, 9transpalpebral delivery, 10–11
Dry eye, 28–9corneal ulceration and, 43
Ectopic cilia, 12, 17, 25, 92corneal ulceration and, 42treatment, 17
Ectropion, 92EDTA, 51–53Electroretinography (ERG), 83, 92Enophthalmos, 92Entropion, 12, 25, 92
corneal ulceration and, 42Enucleation, 92Epinephrine, 74Episcleritis, 15Equine herpes virus, 21, 43Equine viral arteritis, 21Equipment, 4–5Erlichiosis, 21Evisceration, 92Examination, See Ocular examinationExenteration, 92Exophthalmos, 29–31, 92
orbital cellulitis, 29–30orbital space occupying lesions, 30–1retrobulbar infections, 29–30
Exotic species, 11exophthalmos, 30lens-induced uveitis, 78
Eyelid laceration, 23–5, 56
Facet, 92Feline dysautonomia, 22Feline herpes virus infection, 21, 22, 27–8, 40
corneal ulceration and, 43Feline infectious peritonitis, 21Fibrin, 18, 56, 65Flare, 65, 92–3Flubiprofen, 96Flunixine meglumine, 8, 95Fluorescein dye, 5, 54, 95
corneal ulceration and, 37–40Fluorometholone, 95Flurbiprofen, 47, 62Follicular conjunctivitis, 93Foreign bodies, 28
conjunctival, 28corneal, 60–3
management of non-perforating foreignbody, 60
management of penetrating foreign body,62–3
recognition of, 60pain and, 16
Fundoscopy, 66, 81Fusidic acid, 6, 44, 95
Gaiddon radial keratotomy, 48, 51Gentamicin, 52, 53, 95
resistance, 6, 53Glaucoma, 2, 16, 66, 70–4, 77, 93
clinical signs, 71diagnostic tests, 71pain and, 15–16prognostic indicators, 72redness and, 13, 14sudden blindness and, 20treatment, 72long-term reduction of intra-ocular
pressure, 72–4neuroprotection, 74systemic hypotensive treatment, 72
Globe, 32–6blunt trauma, 32–3penetrating injury, 35–6prolapse, 33–5
Glue, 49Glycerol, 72Goniolens, 4Gonioscopy, 93Gram’s stain, 6, 63Granulomatous meningio-encephalitis
(GME), 20, 21, 84Grid keratotomy, 46, 47
Haab’s striae, 14, 77, 93Harada’s syndrome, 79Herpes virus:
equine, 21, 43feline, 21, 22, 27–8, 43corneal ulceration and, 43
Hordeolum, 93Horner’s syndrome, 14, 93Horses, 8–11
drug delivery systems, 9–11nasolacrimal lavage, 9–10spray medication, 11subconjunctival delivery, 9transpalpebral delivery, 10–11equine herpes virus, 21, 43equine viral arteritis, 21melting ulcer, 51–3
Index 103

Horses, (Contd)ocular examination, 8–9ulcerative keratitis, 9uveitis, 9, 66–7See also Specific conditions
Hyperadrenocorticism, 21, 22Hyperlipidaemia, 22Hypertension, 22
retinal detachment and, 20, 79, 81, 82treatment, 82
Hyperthyroidism, 21, 79, 81Hyperviscosity syndrome, 22Hyphaema, 12, 93
emergency management, 57, 66prognostic indicators, 66
Hypocalcaemia, 22Hypopyon, 93Hypothyroidism, 22
Idoxuridine, 27, 95, 96Infections, 18, 22, 27, 62, 67
corneal ulceration and, 43retrobulbar, 29–30See also Specific infections
Infectious bovine keratoconjunctivitis (IBK), 9
Infectious bovine rhinotracheitis (IBR), 21Inflammation, iritis, 64–6
treatment, 67Interferon treatment, 95
conjunctivitis, 27Intra-ocular pressure (IOP), 70–1
long-term reduction, 72–3measurement, 71, 90–1uveitis, 66See also Glaucoma; Tonometer
Iridodonesis, 75, 93Iris, 64–9
benign pigmentary naevus, 69changes in appearance, 68corneoscleral laceration and, 56–60melanoma, 68prolapse, 35
Iritis, 64–8clinical signs, 64–6diagnostic tests, 66–7treatment, 67
Itraconazole, 82
Keratectomy, 47, 53Keratic precipitates (KCs), 93Keratitis, 12
chronic superficial, 92ulcerative, 9
Keratoconjunctivitis (KCS), 93corneal ulceration and, 43feline, 27infectious bovine (IBK), 9
Keratoconjunctivitis sicca, 28–9, 43Keratotomy, 46, 47, 51Ketoprofen, 8, 96Ketorolac, 62, 95Kimura spatula, 5
L-lysine treatment, 27, 96Laceration, See Corneoscleral laceration;
Eyelid lacerationLactophenol cotton blue stain, 6, 63Lagophthalmos, 93Large animals, ocular examination, 8–9
See also Horses; RuminantsLatanoprost, 96Leishmaniasis, 22Lens, 75–8
capsule rupture and phakoanaphylacticuveitis, 77–8
damage by corneoscleral laceration, 56,60
lens-induced uveitis (LIU), 93luxation, 75–7, 81See also Cataract
Lentectomy, 60Leptospirosis, 21Levocabastine, 96Lid laceration, 23–5, 54Lipid deposition:
aqueous humour, 18, 20cornea, 17
Lissamine green, 96Listeriosis, 21Liver disease, 21Local anaesthetic, 5Lodoxamide, 95Luxation, lens, 75–7, 81Lymphocytic conjunctivitis, 93Lymphosarcoma, 21, 22Lysozomal storage diseases, 22
Mannitol, 35, 72, 73, 96Matrix metalloproteinases (MMPs), 53Meibomian glands, 16Meibomianitis, 93Melanoma, iris, 68Melting ulcer, 51–3
diagnosis, 51treatment, 51
Methadone, 8Methazolamide, 72–3, 95, 96
104 Index

Miosis, 60, 63, 66, 93reduction, 67
Mucocoeles, 31Mydriasis, 93Myositis, extra-ocular, 31
Naphazoline HCl, 95Nasolacrimal lavage, 9–10Neomycin sulphate, 95, 96New Forest Eye, 9Nuclear sclerosis, 93
Ocular examination, 1–2large animals, 8–9recording observations, 2–4
Ocular infections, 6–7Oedema:
corneal, 17–18, 42, 60, 62stromal, 40–2, 53, 54
Ofloxacin, 53, 95Optic nerve tumours, 19, 31Optic neuritis, 19, 84–5
sudden blindness and, 20Orbital cellulitis, 29–30Orbital space occupying lesions, 30–1
Painful eye, 15–17Pannus, 12, 93Panophthalmitis, 35Papilloedema, 84Paracentesis, 93Phacoanaphylactic reaction, 56, 60, 77–8Phenylephrine, 67, 96Photophobia, 93Pilocarpine, 73, 96Pituitary tumours, 19, 85Plasmacytic conjunctivitis, 93Plasmoma, 12, 93Polymixin B, 95Prednisolone, 67, 82, 96Progressive retinal atrophy (PRA), 93Prolapse:
globe, 33–5iris, 35, 59
Proparacaine, 10, 95, 96Proptosis, 93Proxymetacaine, 8, 10, 67Ptosis, 93
Quinolones, 51, 53, 54
Recording observations at examination, 2–4Red eye, 12–14Renal failure, 21, 79
Retina:dysplasia, 19, 79, 82haemorrhage, 19, 81progressive atrophy (PRA), 93sudden acquired retinal degeneration
(SARD), 19, 20, 83, 93Retinal detachment, 19, 20, 66, 79–83
examination, 81–2prognostic indicators, 79treatment, 82–3idiopathic retinal detachment, 83in posterior uveitis, 82secondary to hypertension, 82
Retrobulbar infections, 29–30Rose bengal dye, 5, 96
corneal ulceration and, 40Ruminants, 8
ocular examination, 8–9subconjunctival drug delivery, 9
Salivary retention cysts, 31Scar tissue, 18Schiotz tonometer, 2, 71, 90–1
See also Intra-ocular pressureSchirmer tear test, 2, 5, 28, 29, 39, 90Scleral laceration, See Corneoscleral
lacerationScleritis, 15Seidel manoeuvre, 54, 62Sodium chloride, 95, 96Spray medication, 11Staphyloma, 54, 56, 93Steroid treatment:
conjunctivitis, 26–7corneal ulceration, 46drug delivery, 9extra-ocular myositis, 31
Strabismus, 35Stromal abscess, 6Stromal oedema, 40–2, 54Subconjunctival drug delivery, 9Subconjunctival haemorrhage, 12Sudden acquired retinal degeneration
(SARD), 19, 20, 83, 93Sudden blindness, 18–20Synchysis scintillans, 81, 93–4Synechiae, 67, 77, 94
prevention, 67Systemic diseases, 20–2
Tarsorraphy, 94Taurine deficiency, 21Tear deficiency, 28–9
corneal ulceration and, 43
Index 105

Tear test, 2, 5, 28, 29, 39, 90Tetracyclines, 6, 27Thermal keratoplasty, 47Thiamine deficiency, 21Thrombocytopaenia, 22Timolol, 74Tobramycin, 6, 53, 96Tonometer, 2, 4, 70–1, 90–1
See also Intra-ocular pressureToxocariasis, 22Toxoplasmosis, 21, 22Transpalpebral drug delivery, 10–11Trauma:
corneal ulceration and, 43corneoscleral laceration, 35, 54–60globe, 32–6blunt trauma, 32–3penetrating injury, 35–6prolapse, 33–5lid laceration, 23–5pain and, 16retinal detachment and, 20subconjunctival haemorrhage, 12
Trichiasis, 16, 24, 25, 94corneal ulceration and, 42
Trifluorothymidine, 27Trifluridine, 96Trometamol, 51Tropicamide, 67, 96Tumor, 65
Tumours:iris melanoma, 68lymphosarcoma, 21, 22optic nerve, 19, 31pituitary, 19, 85
Ulceration, corneal, See Corneal ulcerationUlcerative keratitis, equine, 9Uveitis, 65, 66, 67, 69
corneal foreign body and, 60, 61equine, 9, 67lens-induced (LIU), 93pain and, 15–16phacoanaphylactic, 77–8prognostic indicators, 66redness and, 13, 14retinal detachment and, 20, 79, 82See also Iritis
Verapamil, 73, 74Vidarabine, 96Vitamin A deficiency, 21Vitreal cavitation with liquefaction, 81Vitreal detachment, 81Vitreal haemorrhage, 20Vogt–Koyanani–Harada syndrome, 22, 79,
82, 94
White eye, 17–18
106 Index