business case for the reconfigured cleft lip and palate ... · business case for the reconfigured...
TRANSCRIPT

Business case for the reconfigured
Cleft Lip and Palate Surgical Service
Release: v1.0 Date: August 2013
Meeting: NoSPG
Date: 4th December 2013
Item: 60/13 (a)

2
Author Marjorie Johns, Planning Manager, NHS Greater Glasgow and Clyde Lyn Hutchison, Project Manager, National Services Division
Date June 2013 Version Draft v0.3
Document control Key personnel
Title: Cleft Lip and Palate Surgical Service – business case
Author: Lyn Hutchison, Project Manager Approver: Jonathan Best, Project Executive Owner: Project Board
Version history
Version Date of revision Summary of changes Changes marked
0.1 June 2013 First draft MJ/LH/DS 0.2 12 June 13 Second draft MJ/JB 0.3 July 2013 Third draft Stakeholders 1.0 Aug 2013 Final JB/DE/GC/MJ/LH
Distribution
Name Organisation
Mr Jonathan Best NHS Greater Glasgow and Clyde Ms Fiona Mitchell NHS Lothian Deirdre Evans NHS National Services Division Dr Mike Winter NHS National Services Division Cleft Lip and Palate surgical service – Service Redesign Project Board. Final document will be distributed to the Surgical service and the managed clinical network, the Tayside network office, and all other primary stakeholders
====

3
Table of Contents Executive Summary .........................................................................................4
Background and introduction........................................................................4
Project Board................................................................................................5
Clinical service models and specification .....................................................5
Management arrangements .........................................................................6
Workforce.....................................................................................................6
Additional activity projections and costings ..................................................7
1. Aims and Objectives of the Cleft lip and/or palate surgical service...........8
2. Service description ...................................................................................8
2.1 Service model .....................................................................................9
2.2 Care Pathway - Paediatrics ..............................................................10
2.3 Adult Services...................................................................................13
2.4 Principles of care ..............................................................................13
2.5 Clinical responsibility ........................................................................14
2.6 Service configuration ........................................................................14
2.7 Workforce requirements....................................................................15
2.8 Other services to be provided ...........................................................16
2.9 Radiology systems............................................................................16
2.10 Facilities and equipment................................................................16 3. Clinical Governance………………………………………………………….17 4. Audit .......................................................................................................18
5. Finance...................................................................................................19
Appendix 1.....................................................................................................22
Appendix 2.....................................................................................................26
4
Executive Summary
Background and introduction
• Following the review of Cleft Lip & Palate Services, it was recommended that there should be a single service for both adults and children, with one management structure and one clinical lead.
• Board Chief Executives asked that the existing providers, NHS Greater Glasgow & Clyde and NHS Lothian, work together to provide a single service across two sites.
• A Project Board, chaired by Jonathan Best, NHS GG&C, comprising
representatives of both provider boards and NSD, has been meeting to agree a business proposal for the Board Chief Executives’ Group.
• The Project Board have, from the outset, agreed the following assumptions:
• The range of multidisciplinary cleft lip and palate services provided locally across NHS Scotland which meet the healthcare needs of patients, with the exception of specialist surgery, are out of scope and should be unaffected by the proposed change to the specialist surgical service.
• NHS Greater Glasgow & Clyde will be the lead Board for the single specialist surgical service, although day-to-day operational management and clinical governance will remain with each of the surgical provider units.
• There will be a single SLA between NSD and the lead Board, NHS Greater Glasgow & Clyde, with two separate financial profiles detailing the expected funding for each site.
• The SLA will be signed by the Chief Executives of both Boards.
• The overall management of the service and the monitoring of the SLA will be overseen by a Service Board comprising representatives of management and clinical teams on both sites.
• There will be a single Mid-Year Report and Annual Report from the Service Board to NSD.
• Primary and secondary paediatric surgery will only take place in Edinburgh and Glasgow.
• There will be a single Clinical Lead for the service, and this should be advertised openly among both the Cleft community and senior clinical staff with appropriate skills.
• Clinicians will work together as a single surgical team.
• The Project Board remit is to cover nationally-designated surgical services, although will liaise closely with CLEFTSiS on other non-designated areas to ensure a seamless approach to care.
• There will be a single nationally agreed clinical pathway for surgical services, based on the existing standards set by CLEFTSiS and other national guidelines (HIS, SIGN, NICE, Craniofacial Society for Great Britain & Ireland etc).
• It is envisioned that patients and/or surgical and other specialist staff may move between sites, as appropriate and based on clinical need, to ensure the highest levels of clinical care are provided.

5
• Telecare will be promoted where clinically appropriate to reduce the need to travel.
• The adult service will be specified and costed.
Project Board
• The Project Board has met monthly since January 2013, with additional checkpoint meetings and offline work in between. Its remit has been to consider:
• Proposed service models for both children and adults
• Service configuration
• Care pathways
• Clinical responsibility and governance
• Workforce issues
• Management arrangements
• A half-day workshop session was also arranged at the CLEFTSiS Annual Meeting on 1 May 2013 to share progress to date and to seek the widest possible clinical input into the process (see appendix 1). This session covered the following topics:
• Patient pathway for paediatrics
• Patient pathway for adults
• Clinical standards and audit, particularly for transition and adult services
• A further clinical meeting of the surgeons who provide the existing designated paediatric service was held in June 2013.
• The business case has been widely distributed for stakeholder input
Clinical service models and specification
• Based on the work of the Project Board and the feedback from the clinical community, two main patient pathways have been identified:
• New patients identified at, or before, birth
• New patients presenting as adults
• The patient pathway for new cases identified at birth is clear and agreed by all clinicians in Scotland. To ensure maximal care through to adulthood, there is only a need to extend the current surgical provision through to final definitive surgery. For most patients, this is already before their sixteenth birthday; for others, it will be in their late teens or early twenties.
• The second group covers patients who have previously been treated outwith Scotland; patients treated in Scotland prior to CLEFTSiS being established who may come forward seeking revisional surgery; and adults who have received no treatment prior to presenting.
• Clinical opinion is that this group do not need to have a specific pathway, but that there should be agreed standards and outcomes for their individual episodes of care and that these should be monitored and audited through CLEFTSiS as with existing paediatric surgery.

6
• It was, however, identified that there should be a national MDT to discuss adult patients.
• A full service specification, based on both CLEFTSiS standards and clinical models used elsewhere in the UK, has been drafted and shared with CLEFTSiS for comment. The service specification explains both of the clinical pathways and the services which should be expected at each stage of the patient journey.
• A full review of all outreach work has been started by identifying patient cohorts by NHS Board. This is a longer piece of work which will be progressed by the Service Board.
Management arrangements
• The Project Board has agreed the future management arrangements for the service from 1 April 2014 as:
� There will be a single SLA between NSD and the lead Board, NHS Greater
Glasgow & Clyde, with two separate financial profiles detailing the expected funding for each site.
� The SLA will be signed by the Chief Executives of both Boards. � The overall management of the service and the monitoring of the SLA will be
overseen by a Service Board comprising representatives of management and clinical teams on both sites.
� There will be a single Mid-Year Report and Annual Report from the Service Board to NSD.
� As individual legal organisations, there are already robust clinical governance structures in place on both sites. These should continue as normal for managing local issues.
� In addition, the Service Board will expect regular clinical governance reports for issues which require escalation to the single clinical lead or have implications beyond the local clinical service(s).
Workforce
• With the planned retirement of one of the existing three consultants in 12-18 months, a proleptic appointment was made following agreement with NSD and NHS GG&C and the project board.
• Whilst the postholder is employed by GGC, the appointment is to the national cleft surgery service and the postholder will support and/or deliver services across Scotland as required.
• Interviews were held in July 2013. Both NHS GGC and NHS Lothian were represented on the panel.
• Previously, the service had a disparity in funding for consultant time, with only one consultant of the three being funded for all elements of cleft care covered by the national service.
• Benchmark reviews with English services have indicated that a cleft surgeon should ideally have 7 DCC PAs + 1 SPA built into their job plan to cover assessment, operating, outpatients and all other follow-up, including outreach

7
clinics, MDTs, etc. (The balance of 2+ DCC PAs in the contract should be in the host specialty, including on-call, in order to maintain wider skills).
• To cover the full cleft service, the Project Board therefore recommends that there should be an increase from the existing 13 DCC PAs funded across both sites to 24 PAs - 21 DCC / 3 SPA, distributed among three surgeons.
Additional activity projections and costings
• Extending the existing paediatric pathway into adulthood is relatively straightforward, as this work is predominantly carried out by the teams responsible for paediatric care. Approximately 40 adult cases per annum are anticipated based on the best evidence available.
• Activity within the second population, new presentations as adults, is more difficult to forecast. As with all services which have not previously been available, it is expected that there may be an initial surge of patients who have not previously presented for treatment.
• The Project Board is therefore proposing that all adult workload should be funded on a cost-per-case basis to reflect the variable nature of the service.

8
1. Aims and Objectives of the Cleft lip and/or palate surgical service
Cleft Lip and/or Palate (CLP) is a congenital anomaly resulting from failure of fusion of embryological parts forming the lip, nose and palate, with about 100 new cases occurring each year in Scotland (SNAP 19981). Its management requires the multidisciplinary involvement of many specialties through growth and development to the age of at least 20 years, as well as treatment of adults of any age. Techniques in cleft surgical care have advanced over recent years and adult patients who have received surgery in the past sometimes require further specific intervention from the CLP teams to optimise previous procedures. From birth to maturity, children with orofacial clefts undergo many surgical and non-surgical procedures that can cause disruption to their life and the lives of their family members. There are often psychological consequences of both this treatment and the deformity itself. Care covers pre-natal and post-natal diagnosis and advice including feeding advice, corrective surgery including specialist and outreach nursing, lip and palate repair, speech assessment, investigation and treatment/surgery, children’s dentistry, bone grafting, orthodontics, dento-alveolar surgery, restorative dentistry including implant treatment, rhinoplasty, orthognathic surgery, audiology/ENT (hearing and ENT problems), clinical psychology, genetics, and revision treatment. The aim of the clinical management of cleft lip and palate patients at the completion of treatment is to ensure that patients achieve an aesthetic and functional facial appearance, and to maximise oral feeding, hearing, speech and psycho-social well being.
2. Service description
The surgical service will be provided (where clinically appropriate) at times and ages as required by agreed clinical protocols and within national waiting times on the basis of equity of access based on clinical need for the population served. Providers will contribute to and participate in local and national audits and contribute data as required to the clinical audit system (CAS), and to the Quad centre audit group via the CLEFTSiS NMCN. The surgical service will strive to contribute to clinical research and when possible basic research into aetiology of cleft lip and / or palate and the best means of treating the conditions. The paediatric surgical element of the cleft lip and palate service has been commissioned nationally for residents within Scotland (up to 16 years of age). This includes the surgical input to all stages of assessment, all aspects of the inpatient hospital stay, and to surgical follow-up. Following the recommendation of the review of the cleft lip and palate surgical service the nationally commissioned service will now also include adult surgery. All other aspects of assessment and follow-up care are funded by the local NHS Boards and are co-ordinated via the CLEFTSiS managed clinical network.
A comprehensive cleft lip and palate service comprises of the following elements: - ▪ Prenatal and postnatal diagnosis ▪ Hospital and community paediatric care ▪ Pre- and post natal specialist cleft nursing including support of newborn
feeding and on-going assessment and management
1 Scottish Needs Assessment Programme. Cleft Lip and Palate Scottish Forum for Public Health Medicine, 69
Oakfield Avenue, Glasgow, November 1998

9
▪ Genetic assessment and chromosomal studies ▪ Multi-disciplinary pre-surgery assessment � Respiratory Paediatrician assessment and Sleep Diagnostics ▪ Initial lip and/or palate surgery and post-operative assessment ▪ Paediatric dentistry including dental health education and oral promotion ▪ Alveolar cleft bone grafting and associated orthodontics ▪ Cleft-related dento-alveolar surgery ▪ Velopharyngeal dysfunction (VPD) investigations, therapy, surgery and/or
prosthetics with follow-up ▪ Speech and language assessment and therapy ▪ Audiology and otology assessment and treatment for hearing problems ▪ Orthodontics ▪ Restorative dentistry including implants and prosthetics ▪ Orthagnathic surgery/distraction osteogenesis techniques to correct cleft
related jaw deformities, and associated orthodontics ▪ Rhinoplasty ▪ Cleft lip and palate revisions and fistula repair ▪ Psychological care for children, adults and their families ▪ Revision treatment, which may include surgery, orthodontics and restorative dentistry, in adulthood ▪ Locally-provided services (e.g. health visitors, children’s community services, education, speech and language therapy, primary dental care) supported by the specialist cleft centre team
2.1 Service model
The cleft lip and palate service will work as a ‘Hub and Spoke’ model with all cleft surgery taking place in a twin centred hub in Glasgow or Edinburgh, with all core disciplines being centred at and directed from the hub in multidisciplinary combined clinics in Ayr, Aberdeen, Dundee, Edinburgh, Glasgow, Kirkcaldy, Inverness, Larbert and Perth (see appendix 2). Services may be delivered by hub clinicians in the centre, by outreach, or by local specialist clinicians for example in SLT, dentistry, orthodontics, ENT/Audiology as appropriate to local circumstances. Treatment will be co-ordinated through a dedicated multidisciplinary team of clinicians to achieve optimum outcomes. The team will work with locally identified specialist clinicians (for example SLT, orthodontics, ENT and Audiology) when possible or by the centre clinicians working by outreach to ensure the care pathway is in place. CLEFTSiS will have shared responsibility with the surgical service to monitor outcomes and ensure the pathway continues to be based on national policy, guidelines and best practice. Timely referral and treatment to achieve optimal outcomes across the patient pathway will be required as will close liaison with the patient’s General Practitioner and General Dental Practitioner, and non-healthcare professionals, e.g. school authorities.
Commissioning arrangements Nationally Commissioned NHS Board Commissioned Prenatal and Postnatal diagnosis Hospital & Community Paediatric
Care Pre and post-natal specialist cleft nursing support
Speech and Language Therapy & Assessment
Pre-surgery assessment Paediatric dentistry including dental health education and oral promotion
Initial lip and/or palate surgery and post-operative assessment
Audiology and otology assessment and treatment
Alveolar Cleft Bone Grafting Orthodontics

10
Cleft related dentoalveolar surgery Orthognathic associated orthodontics Velopharyngeal Dysfunction (VPD) investigations and surgery
Orthodontics and restorative dentistry in adulthood
Cleft Surgical element of orthagnathic surgery/distraction osteogenesis techniques to correct cleft related jaw deformity
Restorative Dentistry
Rhinoplasty CLP revisions and fistula repairs Clinical Genetic Assessment Cleft revision treatment in adulthood Locally provided services e.g. HVs,
S<, Primary Dental care Genetics Tests (under Genetics Laboratory consortium)
Respiratory Paediatric assessment and Sleep Diagnostics
Psychological Care
2.2 Care Pathway - Paediatrics

Ante-natal Birth to 8 wks 9 wks - 2 yrs 3 - 7 years 8 years – 14 years 15 – 21+ years > 21 yrs returning Local Obstetric Units
Ultrasound scan diagnosis, confirmed if necessary by fetal medicine specialist Local obstetric unit to contact Cleft Team within 24 hours of diagnosis
Local maternity unit to contact Cleft Team within 24 hours of birth
Main ‘Hub’ Cleft surgical twin centres (including MDT clinics)
Contact by Cleft Clinical Nurse Specialist (CNS) within 24 hours of referral. Provide printed information Negotiate face to face meeting Offer contact with CLAPA
CNS visit within 24 hrs of referral Specialist feeding assessment and management, printed information, offer CLAPA referral Meet Cleft team and/or MDT Baby clinic before any cleft surgery Ensure appropriate Paediatric surveillance for co-morbidity & syndromes Clinical Psychology support offered at all team clinics and available throughout all the time points in the care pathway. Genetics referral if indicated
Lip repair at 3-6 months Palate Repair at 6-12 months Refer for local ENT assessment and management if cleft palate Speech and language assessment, at 12 months, with 6 monthly reviews and management Paediatric dentist for dental health education/ advice by 6 months of age and direction / liaison with appropriate general dental care Later investigation (e.g. nasendoscopy and videofluoroscopy) for speech problems if necessary and this may
Psychological support prior to school entry Surgery to revise lip and speech (velopharyngeal) surgery if necessary, these to be available if needed throughout the care pathway Full MDT and records at 5 years as per the CLEFTSiS dataset document Paediatric Dentistry advice and/or intervention if necessary
Assessment between 7 years of age and before 9 years by Cleft team Orthodontist, Paed Dentist and Surgeon responsible for ABG, if an alveolar defect is present Paediatric dentistry and Orthodontic treatment If required, pre-ABG orthodontic care followed by Alveolar bone grafting completed before 12 years – follow-up at 6 months post-op Full MDT and records at 10 years as per the CLEFTSiS dataset document Speech and hearing checked and managed if palatal involvement Definitive orthodontic care
Definitive orthodontic care Full MDT and records at 15 and 20 years as per the CLEFTSiS Dataset document . Offer genetic referral. Team assessment for orthagnathic surgery if indicated Planning and pre-treatment for skeletal surgery Orthognathic Surgery and associated Orthodontics if indicated Revisional Surgery if indicated (nose, lip) Paed to Restorative Dentistry as indicated Completion of post-
Continuation of or return to care from previous period Adult patients returning for care may require:- Speech and language assessment and therapy Lip and / or Nose revisional surgery Speech revision surgery, Palatal fistula repair Orthodontics ABG if not done previously Orthognathic surgery Clinical Psychology Hearing assessment and treatment Restorative Dentistry

12
be required at any stage in the care pathway
Paediatric Dentistry if necessary
orthagnathic surgery records and speech assessment. ?speech revision surgery
Local Care
Paediatric surveillance for co-morbidity & syndromes Neo-Natal Hearing Test within first few days after birth for ALL babies Genetic counselling to parents if indicated
10 months hearing test if cleft palate and treatment as necessary Annual hearing assessments up to 3 years of age if cleft palate Speech and language therapy assessment
Speech and language therapy ENT and audiology assessment if cleft palate at 3 years of age, pre-school entry and 5 years of age (5 years of age assessment may be local or at Cleft Team 5 year MDT)
Speech and hearing problems managed Local Orthodontics
Continuing orthodontic treatment-paediatric and restorative dental care in close liaison with ‘centre’
Primary Care
Dental health education in liaison with main centre
Dental health education in liaison with main centre Routine child health surveillance
Routine preventative dental advice and treatment
Routine preventative dental advice and treatment
Regular dental care
Regular dental care
“Full MDT” is Cleft surgeons, Lead Orthodontist. Lead Paediatric Dentist, Clinical Psychologist, Specialised Speech and Language Therapist/s, Lead for ENT/Audiology and may also include Consultant in Restorative Dentistry, local Orthodontists, local Speech and Language Therapists, Paediatrician and Paediatric Anaesthetist, Nurses and Coordinator Patients attend a clinic as locally as possible. Photographic facilities, radiography/radiology and dental laboratory support are required at all clinics and for pre- and post-op photographs. Children and/or parents can be referred to Genetics at any time during their care. Specialist nurses will carry out regular home visits as necessary until after all primary surgery has been completed.

2.3 Adult Services
Extending the existing paediatric pathway into adulthood is relatively straightforward, as this work is predominantly carried out by the teams responsible for paediatric care. Around 40 cases per annum have been identified from figures available. Transition of children/young people to adult services will need to be planned and managed well in advance of the actual transfer to ensure that the service remains responsive to the specific needs of this patient group and that they continue to have access to cleft surgical services. In addition there will be a secondary group of activity, new presentations as adults. This level of activity is more difficult to forecast. As with all services which have not previously been available, it is expected that there may be an initial surge of patients who have not previously presented for treatment, but this will plateaux. Any adult who has missed out on the care pathway should be assessed and treated in so far as that is clinically possible and appropriate regardless of age, according to clinical need and in an appropriate environment as in some cases there will be benefit to the patient of having these procedures performed on a specialised site. Many of those presenting will not pursue a surgical intervention following consultation and others will only need interventions from the non commissioned elements of the service. All adult workload should be funded on a cost-per-case basis to reflect the variable nature of the service.
2.4 Principles of care
To provide a safe, cost effective, high quality specialised service for people with Cleft Lip and/or Palate to improve their quality of life by -
• Offering informed choice to people with Cleft Lip and/or Palate and providing a personal service, sensitive to the physical, psychological, intellectual and developmental needs of the patients and their family/carers
• Ensuring equity of access to services for those with Cleft Lip and/or Palate taking into account a patient’s location and the distance they travel
• Ensuring an appropriate transition to adult care
• Ensuring effective communication and support between patients, their family/carers and the service providers
• Ensuring the Service has a formal appointment policy and follow-up process in case of non-attendance. The Service should have a clear written policy for children who do not attend 2 successive appointments in order to ensure that no child is disadvantaged. This should be based on a team discussion, agreement on action which may include a letter or direct approach to parents/carers and if this does not resolve the situation may require referral to social agencies. In all such cases the paramount interests of the child must be placed first. In principle, no child will be discharged from the service for non-attendance or non-compliance with treatment in order to ensure that children are not disadvantaged.
• Since service delivery in some disciplines (e.g. speech and language therapy) is delivered locally, the NMCN will monitor provision to ensure that the NHS Board provider has the means to ensure such delivery to the agreed service standards, and clear processes in place in order that any shortcomings/service gaps can be escalated for action as appropriate.

14
2.5 Clinical responsibility
NHS Greater Glasgow and Clyde and NHS Lothian will be responsible for all risks arising in connection with the provision of the surgical service in their own NHS Board area (whether arising directly or indirectly) under the terms of this specification including the scheduling of clinics/theatre sessions. All patients who are treated in local or community facilities shall remain under the overall clinical CLP care of the hub. Clinical management of eligible patients will be in line with the agreed care pathway and any relevant regulations governing delivery of services. The precise pathway will vary with the cleft diagnosis, dependent to some extent on co-morbidity, geography and the way in which local and centre services are delivered. NHS Greater Glasgow and Clyde will be responsible for the coordination of any associated in-patient, day care and out-patient services to ensure continuity of care in collaboration with the NMCN. Specialist Cleft Lip and Palate staff, equipment and care will be available irrespective of the care setting, for patients with Cleft Lip and/or Palate admitted to hospital. A proportion of patients with Cleft Lip and/or Palate conditions may have single or multiple medical/congenital conditions and treatment may need to be developed in conjunction with other clinical priorities.
2.6 Service configuration
The service will work as a ‘Hub and Spoke’ model with all cleft surgery taking place at the specialist twin centres (Hub) in Glasgow and Edinburgh with all core disciplines being centred at and directed from the main Hub. NHS Greater Glasgow and Clyde will provide overall management and clinical governance responsibility for the surgical service but will subcontract some aspects of care with NHS Lothian providing a surgical service in the twin centre. NHS Greater Glasgow and Clyde will appoint an overall clinical lead with clinical responsibility for the whole service. The lead clinician should be able to demonstrate a commitment to continuing professional education and training for all staff involved in the network of provision of cleft care. NHS Greater Glasgow and Clyde will agree ‘hub’, ‘outreach’ and ‘spoke’ arrangements with local providers including the frequency of outreach provision. Care in the hub centres will be provided by the main team and by other practitioners linked to the extended team. The main team may provide 'outreach' services on other sites. The main team will also specify the range of services to be provided by other practitioners on distant sites (the spoke teams). Services that need to be provided on the same site as CLP surgery are:
• Paediatric ENT airway support or appropriate protocols for paediatric airway support
• Paediatric Critical Care, generally high dependency but in some cases access to Paediatric intensive care (PICU) will be required.
• Specialised Paediatric Anaesthesia
The main team is responsible for ensuring close liaison with the extended team and
monitoring the quality of care undertaken by the extended team including the
appropriate training and accreditation of staff. Members of the main team will provide
support to local providers in their spoke network, which may include outreach visits.
There should be effective communications between the cleft team and other
professionals. There should be up to date information readily available on the CLEFTSiS website and in appropriate formats for patients, parents, all staff within the hospital and other

15
professionals (e.g. GPs, Paediatricians, Community Midwives, and Health Visitors etc.) which identifies members of the cleft team including the extended team. The information should cover both the services available at the twin surgical centres and across the extended network.
2.7 Workforce requirements
For extending the existing paediatric surgical pathway to cover treatment through to adulthood, the number of consultant surgeon PAs should be increased from the existing 13 DCC PAs to 21 DDC PAs, plus 1 supporting PA per consultant (a total of 24 PAs) distributed equitably between 3 surgeons. Due to ongoing difficulties experienced by all of the NHS Boards in providing clinical psychology input to this service and given that clinical psychology care is seen as essential for a functional cleft service it is recommended that 1.6 wte clinical psychology input is included within the workforce of this service going forward. It is recognised that patients with Cleft Lip and/or Palate have complex medical, emotional and social needs. Access to a broad range of professionals (either nationally or locally commissioned) is essential for delivering optimum and timely therapy.
The Multi-disciplinary Team Lead Clinician, responsible for the oversight of all aspects of clinical care and to ensure that each discipline has sufficient staff to provide the service and to maintain high standards and skills Service Manager responsible for job planning and the overall configuration of the hub services Care Co-ordinator organising service provision over 2 surgical sites and multiple outreach centres Cleft Surgeons, who will devote a majority of their clinical time to cleft care and will work within the multi-disciplinary team, bearing in mind the team’s need to manage succession planning. Surgeons undertaking primary lip and palate repair should be treating not less than 30 new babies per year. New surgeons shall have met the requirements of a TIG approved cleft surgery fellowship training or equivalent. Paediatric Anaesthetist, with a special interest in cleft care Specialists in Dentistry (adult and paediatric), with a special interest in cleft care Consultant Orthodontist, with major commitment to cleft care Specialist Speech and Language Therapist, with major commitment to cleft care Consultant Paediatrician/s, ensuring good paediatric surveillance and on-going paediatric care Consultant ENT surgeons, including those with paediatric otology experience and Audiological Physicians, including those with an interest in children’s hearing. Clinical Nurse Specialist (CNS) Clinical Psychologist Consultant Restorative Dentist Consultant Clinical Geneticist Respiratory Paediatric and Sleep team
The cleft team will facilitate/encourage user involvement by including (a minimum of 2) patient representative(s) in their service development and review processes and meetings. The MDT team will require the support of clinical photography, dedicated IT support especially for archiving of records and to support general team activity, radiologists and radiographers, maxillofacial and orthodontic technicians, secretarial and clerical

16
staff, and audit support staff. The extended team will include local speech and language therapists, audiologists, orthodontists, local and community paediatricians, geneticists and ENT surgeons. There will also be close liaison with ultrasound diagnosticians, foetal medicine experts and Respiratory Paediatric and Sleep teams. The provision of orthodontic treatment for patients with clefts which will involve orthognathic surgery should be planned in conjunction with the orthognathic surgeon who will carry out the orthognathic surgery, with speech and language and clinical psychology input.
2.8 Other services to be provided
Patient education The service will offer all patients, together with their family and carers, appropriate opportunities to learn more about their diagnosis and prognosis and the treatment options available to them. In some cases, more formal education may be offered which might include members from the multi-professional team who can provide a wider range of information according to the individual patient’s needs, e.g. dental care, speech development, eating and drinking skills. The provider will offer appropriate printed information covering advice, treatment and care to patients, general practitioners and patient groups that is non-discriminatory and culturally appropriate. The information should also be accessible to patients with additional needs such as physical, sensory or learning disabilities. Providers should also make patients aware of other sources of information, including appropriate websites and local/national support groups. The CNS in the Cleft team will offer printed information and training to maternity services in their area to promote early identification and referral.
Patient support groups The service should ensure that patients and carers are provided with information about local and national support groups and how to access them, as it is recognised that these are a vital source of peer support, advice and information for patients. Signposting information will be displayed within the provider’s facilities.
2.9 Radiology systems
The main host NHS Board will ensure full access to the radiology PACS of the hospital where most radiology investigations of the patient are undertaken.
2.10 Facilities and equipment Facilities
• access to HDU/PICU
• access to paediatric surgical area including recovery area
• dental clinics for orthodontics and paediatric dental services with appropriate support services including diagnostic imaging and laboratory services.
• computer support which facilitates web based data entry for submission to the CLEFTSiS Clinical Audit System (CAS) database
• appropriate facilities for multidisciplinary clinics (number and kind of rooms, play areas, waiting areas)

17
Equipment
• appropriate imaging equipment for the management and assessment and management of orthodontic care (including orthognathic care)
• appropriate dental radiology facilities meeting radiological standards
• access to videofluoroscopy
• equipment for nasendoscopy
• operating microscope
3. Clinical Governance As individual legal organisations, there are already robust clinical governance structures in place on both sites. These should continue as normal for managing local issues. In addition, the Service Board will expect regular clinical governance reports for issues which require escalation to the single clinical lead or have implications beyond the local clinical service(s). NHS Greater Glasgow and Clyde and NHS Lothian will provide and ensure that all staff adheres to its policies, procedures, and clinical guidelines as agreed with the National commissioner. The Service Board will meet with the National commissioner on an annual basis at a minimum to review the service utilisation and improve on any aspects of the service as required. A representative of service users will be invited to this meeting. Every patient must have a named consultant responsible for their care. The provider will ensure that all services are delivered in a timely manner and in accordance with national standards. Treatment will be prioritised according to clinical need and where clinical need is the same, through chronological waiting list management provided this does not contravene agreed treatment protocols. The service will accept inward referrals from primary, secondary, tertiary and community care clinicians. The service will accept referrals for patients who meet one of the following criteria:
• Patients with Cleft Lip and/or Palate
• Patients with non-cleft Velopharyngeal dysfunction (VPD)
• Expectant mothers with a prenatal diagnosis of a baby with CLP. Referrals will be handled by the receiving service according to the decisions made by the clinical director in conjunction with the multidisciplinary team. The point at which a patient with Cleft Lip and/or Palate requires treatment is a shared decision between the patient and their family/carer and their clinician. There are no specific exclusion criteria that apply to this service. The surgical team will work directly with, but not limited to, the following professionals to ensure a seamless service:
• Local Paediatric Services e.g. Health visitors, School nurses, SLT, Dentists, Audiology/Hearing services
• General Practitioners, General Dental Practitioners and community services
• Secondary and Tertiary provider clinicians and specialist nurses
• Patient Transport Services

18
4. Audit
In order to demonstrate health outcomes it is essential that the national clinical audit database is utilised and the service actively engage with CLEFTSiS. All patients' records must be maintained including study models, relevant radiographs, clinical photographs, speech recordings and videotaped investigations of velopharyngeal function etc. Records should be maintained in a form that supports both national and international audit.

19
5. Finance
The cost of the nationally-designated paediatric surgical service in 2012/13 was £1.268 million as follows: NHS GG&C £676,901 NHS Lothian £591,055
5.1 Proposed additions to existing costs
Two elements of service are proposed to the existing cost base for the paediatric service:
5.1.1 Consultant sessions
Because of historical funding patterns, only surgical operating time is funded at RHSC Glasgow, while all elements of cleft care are funded at RHSC Edinburgh. As highlighted under workforce, the input of the surgical team to all levels of care – MDTs, case reviews, outpatients and liaison with local services, including the delivery of outreach clinics – is key to the quality of the service. The agreed English job plan for cleft surgeons is 7 DCCs in cleft + 1 SPA, based on a 9+1 job plan, with the remaining two clinical sessions within the host specialty of either Plastic Surgery or Oral and Maxillofacial Surgery. The Project Board therefore proposes to use this model for all consultant job plans going forward to ensure equity across Scotland and between team members. The extension of consultant input will underpin the redesign of services to cover a single pathway from first patient contact through to final surgery and discharge to local services. At present, 13 PAs are funded nationally, leaving a gap of 11 PAs. This will require an increase in funding of £123,600
5.1.2 Clinical psychology
The clinical meetings held in May and June 2013 highlighted dedicated clinical psychology input as the most important development requirement after surgical time. Services in the rest of the UK have dedicated clinical psychologists as part of the core team. In Scotland, this has been considered part of the role of local child and family psychology services. To provide support to MDTs, clinics and to meet the needs of the existing cohort, it is estimated that there is a need for 1.6WTE Clinical Psychologists (Band 8a, midpoint). This will require an increase of funding of £84,140.

20
5.2 Adult services
Adult services are difficult to predict. As noted above, the levels of previously untapped need which may present to a new service is unknown. Not all cases require the surgical input of a full cleft team. Many are minor and could – and should – remain within local orthodontic or dental surgery services in each NHS Board, suitably supported by national advice. The proposal is therefore that there should be two levels of nationally-funded adult cleft provision:
• Alveolar bone graft
• Other complex cleft procedure requiring inpatient admission Rather than designate one (or two) surgical sites, the Project Board proposal is that there should be a cost-per-case rate adopted for these two procedures. The admission point to the national service should be through the national MDT. To minimise patient travel, the MDT will nominate a site for surgery, as these procedures can be carried out by a number of suitably trained Oral and Maxillofacial Surgeons and Plastic Surgeons across Scotland.
5.2.1 Proposed cost The proposed cost-per-case rates (at 2013/14 prices) for these two caseloads is: Alveolar bone graft £2,250 Other cleft £2,500
Comparative costs English tariffs for these specific procedures are not available as cleft surgery is excluded from payment by results. The following tariffs may, however, be used as a proxy:
Major oral and maxillofacial procedures without CC* £4,115 Complex oral and maxillofacial procedures without CC* £4,954 Complex oral and maxillofacial procedures with reconstruction £10,520
Notes * co-morbidities or complications 2013/14 PbR Handbook prices Costs are before market forces factor is applied
Procedures in under 19s attract a 44% top-up 5.2.2 Activity
The existing numbers of patients being seen over age 16 are approx 40-45 per annum. To maintain existing caseload, the Project Board is therefore suggesting a planning assumption of fifty cases per annum. This would require an increase in funding of £125,000.
21
(In previous years, the majority of surgery has been carried out by NHS Greater Glasgow & Clyde and cases are already charged at these prices to all NHS Boards.) It must be noted that Year 1 and 2 may require additional non-recurring funding over and above this to cope with a potential spike in referrals.
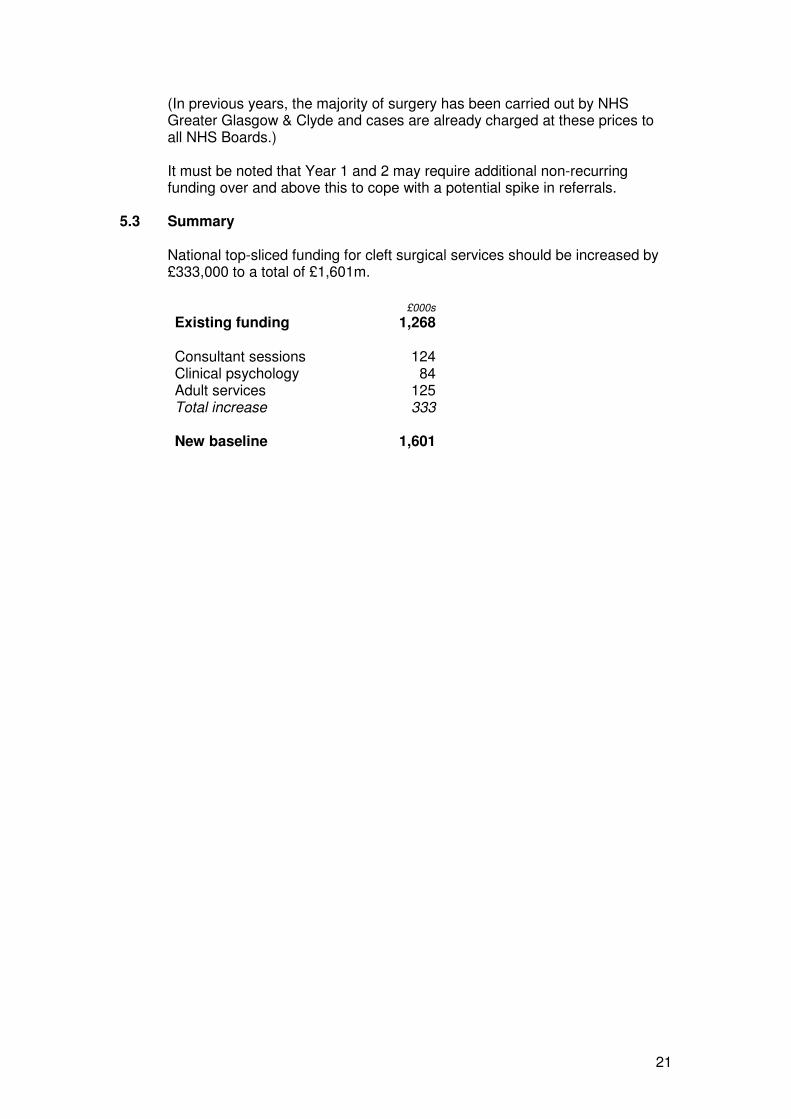
5.3 Summary
National top-sliced funding for cleft surgical services should be increased by £333,000 to a total of £1,601m.
£000s
Existing funding 1,268 Consultant sessions 124 Clinical psychology 84 Adult services 125 Total increase 333 New baseline 1,601
====
====

22
Appendix 1
CLEFTSiS workshop feedback
Table 1 Person Centred Topic Patient Engagement –Paediatric services
Aim o Determine how to use patient experience to drive improvement in
delivery of paediatric services
Feedback
How does the current configuration of paediatric patient services fit with the patient pathway � Cross cover work voluntary/goodwill outwith the centrally designated
service – needs to be more formalised arrangements or levers in place to ensure the right people are always released and available for outreach clinics/locally provided services. This should be coordinated and supported by CLEFTSiS and the designated service.
� In regard to the administration of the patient records there needs to be more IT alignment between local care settings and the centre to cut down on duplication of tests and data entry. This would also facilitate continuity from paediatric to adult care
� Patient information needs to be reviewed and developed to reflect the patient pathway (what to expect and where provided)
What should the future designated two centre service look like going forward � Ensure support of their local services from the network and surgical
service. Surgeons need to be available to participate in outreach clinics � Need to consider availability of transport/accessibility of MDT clinic for
remote/deprived areas � Ensure the infrastructure in the peripheral clinics to ensure well run
effective clinics – right people/right time. More availability of paediatric dentistry and clinical psychology support. Consider having some nurse led clinics.
� Ensure appropriate facilities for the local services e.g. SLT Where should the outreach clinics be located to best meet patient needs and what should be the frequency be � Base location on cohort numbers available from the last 20 years � In regard to the NHS Grampian clinic the frequency of this needs to be
increased perhaps from one to two per month and the VP function clinic needs to be retained.
Table 2 Person Centred Topic Patient Engagement – Transitional care and adult services
Aim o Determine how to use patient experience to drive improvement in
delivery of transition and adult services
Feedback
What needs to be in place for the smooth Transition from paediatric to adult services?
• Recognition that many of the Team members in the paediatric service, particularly the medical staff, already provide services to adult Cleft patients.
• When moving into adulthood, the young people need to be provided with the necessary information such as a checklist of potential conditions that will enable them to make informed choices as they grow older as to whether they need subsequent

23
Cleft / complex dental surgery or the input from other services in the MDT.
• This information also required to be available to their GP, in order to enable them to make referrals when required –with them taking on an Active Awareness role in the continuum of their care.
What should the adult patient pathway look like?
• The pathway will be one that is clear and provides the opportunity for the patient to re-engage with the service when they feel they have an unmet need or their GP/other care provider considers there to be a need to make an appropriate referral on their behalf.
• There should be the same MDT approach for adults as exists for paediatrics.
• A key role for the MDT being part of the decision making process on what treatment is required and by whom and where this will be best be provided.
• The pathway requires being one that will allow for patients who have existing historical unmet needs to be referred in. (This level of historical unmet need will require to be modelled into the Business Case).
• To be effective this pathway will require that there is sufficient MDT staff capacity to provide the required level of input.
• In addition there needs to be recognition that MDT discussions can still take place out with the Team meetings.
• Where appropriate and relevant, telehealth approaches will be required to support the delivery of the pathway – with technology such as Patient Information Websites (CLAPA), Social Networking and Clinical Video Telehealth.
What factors should be considered when deciding where adult surgery should take place? As part of this, what will require the full MDT input and what should be delivered by local teams?
• The default position should be that Adult Cleft services need to be as local as possible.
• The starting point for this will be the local availability of treatment that does not require the particular skills of a specialised Cleft Surgeon.
• Where specialist Cleft Surgery is to be performed – pre and post operative care requires to be provided as local as possible by the local teams. This model works best at supporting patients.
• In line with the two points above –there needs to be agreement on those procedures that should only be provided by a specialist Cleft Surgeon.
• It needs to be acknowledged that for the majority of adult Cleft patients, the procedures to be provided will predominantly be secondary ones; correcting problems that result from ageing etc. (i.e. the Adult service will not be as specialised as that for paediatrics).
What should be the Locations and the frequency of clinics for adults and transition care?
24
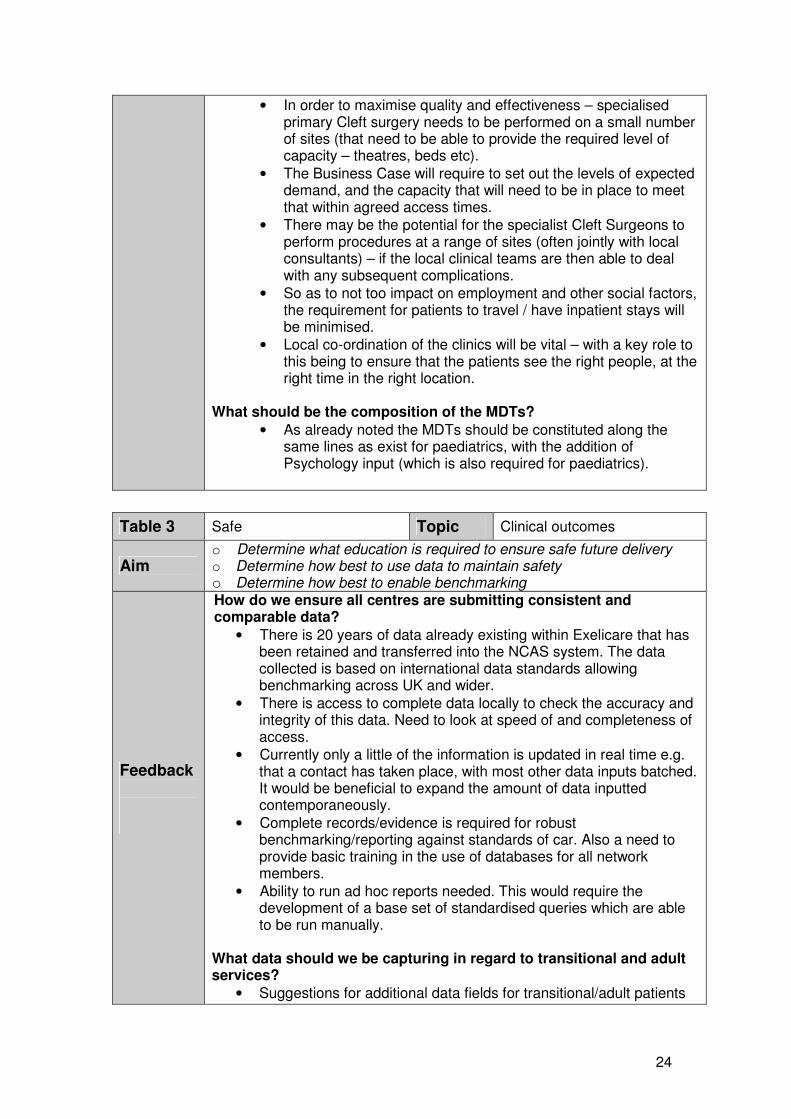
• In order to maximise quality and effectiveness – specialised primary Cleft surgery needs to be performed on a small number of sites (that need to be able to provide the required level of capacity – theatres, beds etc).
• The Business Case will require to set out the levels of expected demand, and the capacity that will need to be in place to meet that within agreed access times.
• There may be the potential for the specialist Cleft Surgeons to perform procedures at a range of sites (often jointly with local consultants) – if the local clinical teams are then able to deal with any subsequent complications.
• So as to not too impact on employment and other social factors, the requirement for patients to travel / have inpatient stays will be minimised.
• Local co-ordination of the clinics will be vital – with a key role to this being to ensure that the patients see the right people, at the right time in the right location.
What should be the composition of the MDTs?
• As already noted the MDTs should be constituted along the same lines as exist for paediatrics, with the addition of Psychology input (which is also required for paediatrics).
Table 3 Safe Topic Clinical outcomes
Aim o Determine what education is required to ensure safe future delivery o Determine how best to use data to maintain safety o Determine how best to enable benchmarking
Feedback
How do we ensure all centres are submitting consistent and comparable data?
• There is 20 years of data already existing within Exelicare that has been retained and transferred into the NCAS system. The data collected is based on international data standards allowing benchmarking across UK and wider.
• There is access to complete data locally to check the accuracy and integrity of this data. Need to look at speed of and completeness of access.
• Currently only a little of the information is updated in real time e.g. that a contact has taken place, with most other data inputs batched. It would be beneficial to expand the amount of data inputted contemporaneously.
• Complete records/evidence is required for robust benchmarking/reporting against standards of car. Also a need to provide basic training in the use of databases for all network members.
• Ability to run ad hoc reports needed. This would require the development of a base set of standardised queries which are able to be run manually.
What data should we be capturing in regard to transitional and adult services?
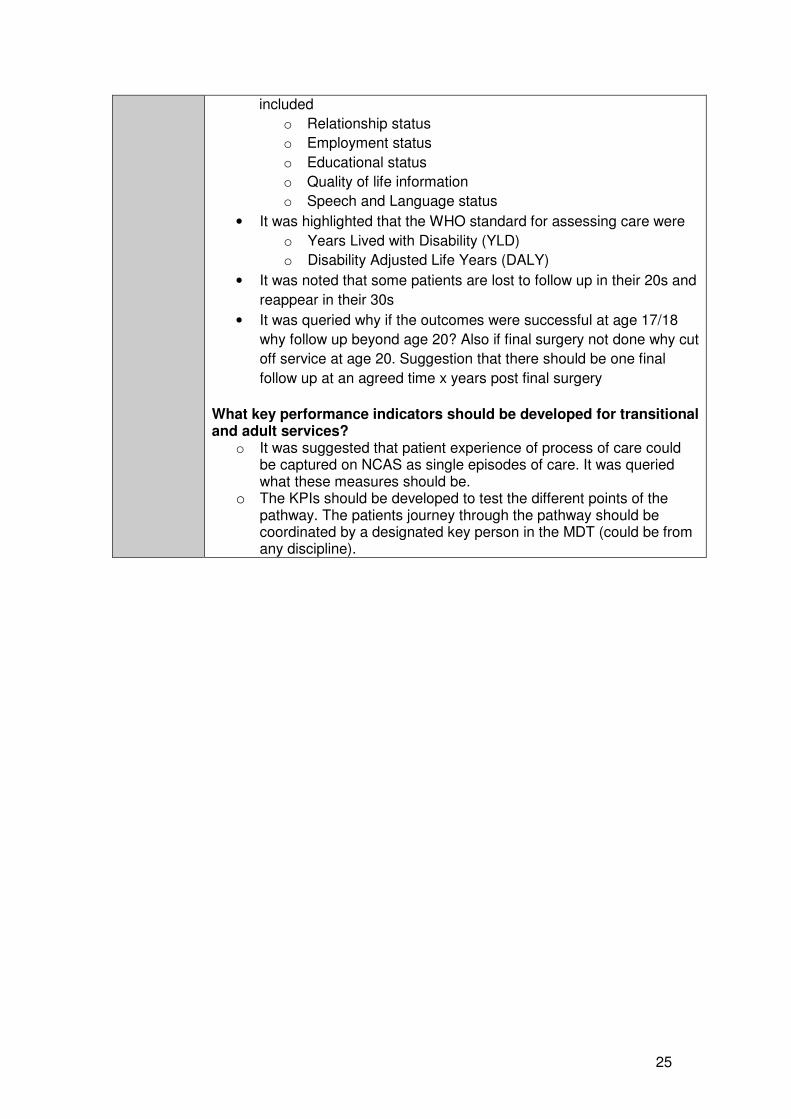
• Suggestions for additional data fields for transitional/adult patients
25
included
o Relationship status
o Employment status
o Educational status
o Quality of life information
o Speech and Language status
• It was highlighted that the WHO standard for assessing care were
o Years Lived with Disability (YLD)
o Disability Adjusted Life Years (DALY)
• It was noted that some patients are lost to follow up in their 20s and
reappear in their 30s
• It was queried why if the outcomes were successful at age 17/18
why follow up beyond age 20? Also if final surgery not done why cut
off service at age 20. Suggestion that there should be one final
follow up at an agreed time x years post final surgery
What key performance indicators should be developed for transitional and adult services?
o It was suggested that patient experience of process of care could be captured on NCAS as single episodes of care. It was queried what these measures should be.
o The KPIs should be developed to test the different points of the pathway. The patients journey through the pathway should be coordinated by a designated key person in the MDT (could be from any discipline).

26
Appendix 2