bundle primary & community care committee 10 october 2018cwmtafmorgannwg.wales/docs/primary care...
TRANSCRIPT
Bundle Primary & Community Care Committee 10 October 2018
0 AGENDA1 Agenda Primary and Community Care Committee 10 October 2018.docx
1 PART 1 - PRELIMINARY MATTERS1.1 Welcome & Introductions1.2 Apologies for absence1.3 Declarations of Interest1.4 Unconfirmed Minutes of the meeting held on 27 June 2018
1.4 Unconfirmed minutes Primary and Community Care Committee 27 June 2018 PCCC 10 Oct 2018GR.doc
1.5 Matters Arising1.6 Action Log
1.6 Action Log PCCC 10 October 2018.docx
1.7 Chairs Report2 PART 2 - ITEMS FOR APPROVAL/ENDORSEMENT2.1 Baby Teeth Do Matter - 12 Month Evaluation Report
2.1 Baby Teeth DO Matter PCCC 10 Oct 2018 GR.docx
2.2 Organisational Risk Register2.2 Org Risk Register PCCC 10 Oct 2018 GRa.doc
3 PART 3 - GOVERNANCE, PERFORMANCE & ASSURANCE3.1 Report of the Director of Primary, Community & Mental Health
3.1 DPMH report PCCC 10 October 2018.doc
3.2 Primary & Community Care Internal Audit Report3.2 IA Report Governance Arrangements - Primary and Community Care Committee PCCC 10 Oct
2018.pdf
3.3 Inverse Care Law/Population Health Management Pilot Update3.3 Inverse Care Law and Population health management pilot report PCCC 10 October 2018.docx
3.4 Cluster Update3.4 Cluster update PCCC 10 October 2018.docx
3.5 Delivery Agreements3.5 Delivery Agreement Progress Updates Q 1 and 2 PCCC 10 October 2018.docx
3.5.1 Appendix 1 Composite Delivery Agreement Progress Update report PCCC 10 October 20183.5.1 Appendix 1 Composite Delivery Agreement Progress Update report PCCC 10 October 2018.pdf
4 PART 4 - FOR INFORMATION4.1 Primary Care Newsletter
4.1 Primary Care Newsletter (Welsh Government) Summer 2018 PCCC 10 October 2018.pdf
4.2 IMTP Monitoring Report4.2 IMTP Monitoring Report paper PCCC 10 October 2018.docx
4.2.1 Appendix 1 IMTP tracker quarterly report PCCC 10 October 20184.2.1 Appendix 1 IMTP tracker quarterly report PCCC 10 October 2018.docx
5 PART 5 - OTHER MATTERS5.1 To Review the Forward Look for 2018/19
5.1 Forward Look PCCC 10 October 2018.doc
5.2 Any other urgent business5.3 Date of Next Meeting

0 AGENDA
1 1 Agenda Primary and Community Care Committee 10 October 2018.docx
PRIMARY AND COMMUNITY CARE COMMITTEE
Wednesday 10 October 2018 Ynysmeurig House, Navigation Park, Abercynon
09.00 - 12.00
AGENDA
Lead / Attachment
PART 1 - PRELIMINARY MATTERS
1.1 Welcome and Introductions Chair / Oral
1.2 Apologies for Absence Chair / Oral
1.3 Declaration of Interests Chair / Oral
1.4 Unconfirmed Minutes of the meeting of the Primary
Care Committee held on 27 June 2018.
Chair
Attachment
1.5 Matters Arising Chair / Oral
1.6 Action Log Chair
Attachment
1.7 Chair’s Report Chair / oral
PART 2 - ITEMS FOR APPROVAL / ENDORSEMENT
2.1 Baby Teeth DO Matter – 12 month evaluation report
Director of Public Health
Attachment
2.2 Organisational Risk Register Director of Corporate Services
and Governance / Board
Secretary
Attachment
PART 3 - GOVERNANCE, PERFORMANCE AND ASSURANCE
3.1 Report of the Director of Primary, Community and Mental Health
Director of Primary,
Community & Mental Health
Presentation
3.2 Primary and Community Care Internal Audit Report (Substantial Assurance)
Director of Corporate Services
and Governance / Board
Secretary
Attachment
3.3 Inverse Care Law / Population Health Management Pilot update
Director of Public Health
Attachment
3.4 Cluster Update Locality Clinical Director
Attachment
3.5 Delivery Agreements Director of Primary,
Community & Mental Health
Attachment
PART 4 - FOR INFORMATION (These items will only be discussed if related issues are raised with the Chair in
advance of the meeting)
4.1 Primary Care Newsletter
Director of Primary,
Community & Mental Health
Attachment
4.2 IMTP Monitoring Report Director of Primary,
Community & Mental Health
Attachment
PART 5– OTHER MATTERS
5.1 To review the Forward Look for 2018/19 Chair
Attachment
5.2 Any other urgent business Chair / Oral
5.3 Date of Next Meeting
Wednesday 9 January 2019 at 9.00am
Rhondda and Cynon Rooms, Ynysmeurig House, Abercynon CF45 4SN
1.4 Unconfirmed Minutes of the meeting held on 27 June 2018
1 1.4 Unconfirmed minutes Primary and Community Care Committee 27 June 2018 PCCC 10 Oct 2018 GR.doc
Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 1 of 8
Primary and Community
Care Committee Meeting
10 October 2018
CWM TAF UNIVERSITY HEALTH BOARD
MINUTES OF THE MEETING OF THE PRIMARY AND COMMUNITY
CARE COMMITTEE HELD ON 27 JUNE 2018 AT YNYSMEURIG HOUSE, ABERCYNON
PRESENT:
Mrs M K Thomas − Vice Chair of the Health Board (Chair) Cllr R Smith − Independent Member
Mr K Montague − Independent Member
IN ATTENDANCE: Mr A Lawrie − Interim Director Primary, Community &
Mental Health Prof K Nnoaham − Director of Public Health
Dr S Hackwell − Assistant Medical Director for Primary Care
Mrs A Riley − Head of Finance for Primary Care Mrs S Scott-Thomas − Head of Medicines Management
Mrs A Davies − Assistant Director for Therapies and Health Sciences
Mr C Wilson − Assistant Director for Primary Care, Children and CAMHS
Mrs J Howard − Community Pharmacy Wales Mr I Jones − Optometry Wales
Mrs S Bradley − Head of Primary Care & Localities Manager Merthyr/Cynon, Merthyr and Cynon Locality
Mrs A Lagier − Locality Manager, Rhondda and Taff Ely Locality
Dr K Burkhardt − Clinical Director (Taff Ely Locality) Dr K Thomas − Local medical Committee Representative
Mrs K Clarke − Primary Care Dental Representative
Ms G Roberts − Head of Corporate Services Mrs J Gibbs − Secretariat
Ms K Rowe − Internal Audit - Observer
PCCC/18/038 WELCOME & INTRODUCTIONS
Mrs M Thomas (Chair) welcomed everyone to the meeting and members were invited to introduce themselves. The Chair also
apologised for the change of date at short notice.
PCCC/18/039 APOLOGIES FOR ABSENCE
Apologies for absence were received from Dr D Miller, Dr N Lewis, Mrs L Williams, Dr G Jordan, Ms S Thomas, Mr K Asaad, Mr R Williams, Ms
R Treharne and Mrs J Davies. Mrs M Thomas thanked Mrs L Williams
and Mrs K Clarke on behalf of the Committee for all their hard work and contribution to Primary Care on their respective retirements.

Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 2 of 8
Primary and Community
Care Committee Meeting
10 October 2018
PCCC/18/040 DECLARATIONS OF INTERESTS
Mr K Montague reminded the Committee that was a board member of
Merthyr & Valleys MIND organisation and Dr S Hackwell also reminded the Committee that he was a partner at the Morlais Medical Practice in
Merthyr Tydfil.
PCCC/18/041 MINUTES OF THE PREVIOUS MEETING
The minutes of the meeting held on 4 April 2018 were RECEIVED and APPROVED.
PCCC/18/042 ACTION LOG
Members RECEIVED and discussed the action log and the following
items were discussed:
• PCC/17/16 Baby Teeth Do Matter – end of year reports had not
yet been received, the final report would be received at the October meeting.
• PCC/17/57 Sexual Assault Referral Centre (SARC) – There was no update as Mrs L Williams had attended the set up meeting
27 June for SARC and an update would be received at the next meeting.
• PCC/17/61 – Inverse Care Law – Data would be available in
September 2018 and it is anticipated that feedback would be
received at October meeting
PCCC/18/043 MATTERS ARISING
There were none.
PCCC/18/044 COMMITTEE CHAIR’S REPORT
The Chair provided an oral update and the following areas were highlighted:
Vice Chairs meeting – Mrs M Thomas advised Members that the Vice
Chairs had met with the Cabinet Secretary in March and that Dr Andrew Goodall was also in attendance. The agenda had been primarily focused
on transformation work, the long term plan (which had now been published), current cluster funding as well as several discussions around
Out of Hours/General Practitioners contract negotiations and GP services/working together. Members NOTED that the Wales Audit
Office would be conducting an All Wales Review of Primary Care Services and that Mrs Sarah Bradley & Mrs Alison Lagier would feed
back to the Committee.
Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 3 of 8
Primary and Community
Care Committee Meeting
10 October 2018
Mrs Suzanne Scott-Thomas explained that the issue surrounding cluster
funding affected recruitment as posts could not be offered on a permanent basis which was NOTED.
Members RESOLVED to:
• NOTE the Chair’s update.
PCCC/18/044 PRIMARY AND COMMUNITY CARE COMMITTEE ANNUAL REPORT
Ms G Roberts presented the Primary and Community Care Committee (PCCC) Annual Report. The aim of the report was to present the PCC
Committee’s draft Annual Report from 2017-2018, which provided an overview of the work undertaken during the year and set out how the
Committee it met its Terms of Reference. Members NOTED that the Terms of Reference had been slightly amended and that there was an
Independent Member vacancy (3rd sector) but the change had been
made to reflect that the committee would be quorate with 2 Independent Members in attendance.
Members RESOLVED to:
• ENDORSE the annual report for submission to the Health Board for approval including the Terms of Reference.
PCCC/18/045 ORGANISATIONAL RISK REGISTER
Members RECEIVED and DISCUSSED a copy of the Organisational
Risk Register. The purpose of the report was to provide the Committee with the organisational risk register and to consider whether the
recorded risks were appropriately assigned.
Ms G Roberts presented the report and provided an update on the risk
register categories and the summary of the assessed risks. The Committee had 4 assigned risks and Members were asked to consider
the risk rating and any mitigating actions.
Members were asked to NOTE that since the last review the report had been presented to the Executive Board in March and the Quality
and Safety Committee in May where 4 risks associated to this Committee had been identified.
Risk 033 – The Chair felt that this did not sit with the Committee and
should be allocated to the Quality, Safety & Risk Committee (QSR). It was NOTED that this would be allocated to the QSR Committee for
scrutiny (Added to Action Log).
Risk 029 – it was agreed that the risk would be reviewed by Mr Alan
Lawrie & Mr Robert Williams in terms of wording (Added to Action Log).
Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 4 of 8
Primary and Community
Care Committee Meeting
10 October 2018
Members RESOLVED to: • NOTE the report
• ENDORSE the allocated risks to the Committee subject to the amendments being done.
GOVERNANCE PERFORMANCE AND ASSURANCE
PCCC/18/046 PRESENTATION OF THE EARLY WORK IN RELATION TO THE
PRIMARY AND COMMUNITY TRANSFORMATION PLAN
Mr A Lawrie gave a short presentation on Transforming the Future Shape of Primary and Community Health Services – Influencing Whole
System Change.
Mr Lawrie gave an overview of the progress to date on several key
areas and highlighted: • The Transformational Plan
• Outputs from the Primary Care Workshops • The Long Term NHS Plan
• The Parliamentary Review • The new model
• Potential examples • The extended Community Resource Team
• Outcomes • The Next Steps………
Members RESOLVED, following discussion members NOTED the work
to date and agreed to RECEIVE an update at the next meeting (Added to Action Log)..
PCCC/18/047 REPORT OF THE DIRECTOR OF PRIMARY, COMMUNITY AND MENTAL HEALTH
Mr A Lawrie presented the report and the aim was to provide
information for the Committee to assure that progress against key areas was taking place and to provide high level information on a
range of services.
• Advanced Training Practice/Pacesetter initiative – Members NOTED that this was progressing well, although were
made aware that the activity of primary care nurses and in the locality team had not been captured within the report.
• Managed Practices – Mrs S Bradley advised the committee that there were currently 4 managed practices but from the 1
October 2018 the number would reduce to 2. The Members
NOTED that a report would be presented to Executive Board in relation to the proposed change and the consultation process
would begin with the other two practices.

Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 5 of 8
Primary and Community
Care Committee Meeting
10 October 2018
• Welsh Government Delivery Agreement – Members NOTED
the project underspend at month 2 which would be closely monitored and refined over the next quarter. Any underspend
position would be reported to the Chair of the Committee prior to the next meeting.
• Welsh Community Care Information System – Mr A Lawrie advised that at present the system was not ready for live use
and further work was continuing with the national team.
Members RESOLVED to: • NOTE the report.
PCCC/18/048 POST PAYMENT VERIFICATION PROGRESS REPORT (FROM
AUDIT COMMITTEE)
Mr C Wilson presented the report which requested that the Committee
receive and NOTE the contents of the Post Payment Verification Year End Report for the period 1 April 2017 to 31 March 2018. Members
NOTED that where issues had been raised they should be aware of the mitigation in place to provide assurance. Members were aware that the
Audit Committee had referred the report to the Committee for ongoing monitoring.
Members NOTED that the report was prepared by staff from the NHS
Wales Shared Services partnership (NHSWSSP) with the aim to provide Cwm Taf with assurance that contractors had made
appropriate financial claims. Members noted that monies recovered was still relatively small in terms of the over-claim rate. In General
Medical Services (GMS) this was 4.70% and in General Ophthalmic Services (GOS) was 7.43%. The errors in GMS were in relation to
minor surgery; where inappropriate claims were made due to a lack of
clinical knowledge. Members NOTED that near patient testing, which was a relatively new service had proved to be a steep learning curve
for the GP Practices and ongoing work was in place to adapt the approach in the future.
Following discussion Members RESOLVED to:
• NOTE the report.
PCCC/18/049 CYNON VALLEY CLUSTER OVERVIEW
Mrs S Bradley presented the report. The purpose of the report was to
present Members with an update on work being undertaken by the Cynon Primary Care Cluster. The report highlighted areas of work
currently being delivered for patients using the Primary Care Cluster
funding. An update was provided on the key ongoing schemes.
Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 6 of 8
Primary and Community
Care Committee Meeting
10 October 2018
The Committee was advised that the main change was a cluster re-
organisation whereby Cynon Valley Cluster had now split into 2 clusters but will continue to work as one. The GP practices had agreed
the re-grouping and there were no concerns identified in relation to the change. Members NOTED that the Cynon cluster meetings were very
well attended. The next step would be to inform Welsh Government and the Observatory of the change, it was also added that other health
boards in Wales also worked in smaller population based clusters.
Members RESOLVED to: • NOTE the report and the progress being made by the Cynon
Valley Primary Care Cluster and the reorganisation into two smaller clusters.
PCCC/18/050 PRIMARY CARE MEASURES
Mrs S Bradley presented the report which aimed to provide the
Committee with an update summary on the progress of Cwm Taf University Health Board against the current Primary Care Measures. In
presenting the report Mrs Bradley thanked Victoria Jeynes for her work on the report.
Mrs Bradley informed the Committee that there were issues within the
report and also limitations to the dashboard meaning that not all information was up to date and that further information would be
provided at the next meeting.
Following discussion Members RESOLVED to:
• NOTE the Primary Care Measures for Cwm Taf University Health
Board. • NOTE that the Directors of Primary Community and Mental Health
were working on 5/6 key measures for General Medical Services (GMS) which may give more valuable information.
PCCC/18/051 LOCAL ORAL HEALTH DELIVERY PLAN UPDATE
Mr C Wilson presented the report. The purpose of the report was to provide Members with an update on the progress of the National Oral
Health Plan and Oral Health Priorities. The national plan was completed in January 2018 and Cwm Taf received a positive response
from the Chief Dental Officer in February 2018 outlining several areas of progress this year including:
• Continued dental representation within cluster networks • Design to Smile/Baby Teeth do Matter highlighting the
engagement between the University Health Board and Rhondda
Cynon Taf County Borough Council and Welsh Water • Appointment of Restorative Consultant and Dental Nurse

Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 7 of 8
Primary and Community
Care Committee Meeting
10 October 2018
• Continued engagement with the Post Graduate Medical and
Dental Education • The alternative pathway developed for oral surgery within a
primary care setting.
However, the response highlighted areas for action and these would be incorporated in the local oral health plan:
• Poor oral health in young children • General anaesthetic treatment for special care patients
• High incidences of late presenting cancer cases • Community Dental Service/Domiciliary Service.
Members RESOLVED to:
• NOTE the report, action plan and progress to date. • Baby teeth DO matter would be presented at the October meeting.
PCCC/18/052 DIRECTOR OF PUBLIC HEALTH REPORT
Professor K Nnoaham presented the report which aimed to update the Committee of key areas within the portfolio of the Director of Public
Health. This report focussed on the Community Joint Care Programme. Due to key data not being available until September, a further report
focussing on the Inverse Care Law / Health Check programme would be presented to the next meeting.
Members NOTED that more recently access has been widened to
include referrals from health checks and sleep apnoea although we are still reflecting on the degree of uptake and whether the current
pathway is correct for those sources referrals.
Members NOTED the committee that the validated outcomes are
measured against other key benchmarks are very good and those who engage and complete the programme, however only 50% of those who
are referred actually complete the programme. Professor Nnoaham asked the committee to NOTE the uptake from the Merthyr Tydfil
locality was considerately lower than uptake in Rhondda Cynon Taf.
Mr C Wilson responded that feedback received suggested that referral into this scheme was quite complex and not straightforward. The
Primary Care team are looking into facilitating a better referral process and added that they are currently reviewing the whole Clinical
Musculoskeletal Assessment and Treatment Service (CMATS) process and have invited Public Health to be part of that process.
Members RESOLVED to:
• NOTE the report.
Agenda Item 1.4
Unconfirmed minutes of the Primary and
Community Care Committee
27 June 2018
Page 8 of 8
Primary and Community
Care Committee Meeting
10 October 2018
FOR INFORMATION
PCCC/18/053 WALES AUDIT OFFICE DISCHARGE PLANNING REPORT
Members NOTED that the Audit Committee had referred the report to
the Committee for ongoing monitoring. The Report was RECEIVED and it was agreed to have a full response at a future meeting (Added
to the Action Log).
Members RESOLVED to: • RECEIVE the report.
PCCC/18/054 NATIONAL PRIMARY CARE BOARD
The minutes of the meeting of the National Primary Care Board which
was held on 16 March were received by the Committee.
PCCC/18/055 INTEGRATED MEDIUM TERM PLAN (IMTP) MONITORING
REPORT
Members RECEIVED the usual overview of the IMTP for information which linked closely with the ongoing transformation work.
Mr A Lawrie added that GP Out of Hours had not been discussed in
detail but a paper would presented at the Executive Board looking at a significant re-design.
PCCC/18/056 TO REVIEW THE FORWARD LOOK
The forward look was received and would be amended in line with the
agreed actions
PCCC/18/056 ANY OTHER URGENT BUSINESS
There was none.
PCCC/18/037 DATE OF NEXT MEETING
The next Primary and Community Care Committee meeting was
planned to take place 3rd October 2018, 9am to 12pm, Ynysmeurig House, Abercynon.
SIGNED …………………………………………………….
MARIA THOMAS, CHAIR
DATE ……………………………………………………
1.6 Action Log
1 1.6 Action Log PCCC 10 October 2018.docx
AGENDA ITEM 1.6
Action Log Page 1 of 1
Primary and Community Care Committee Meeting 10 October 2018
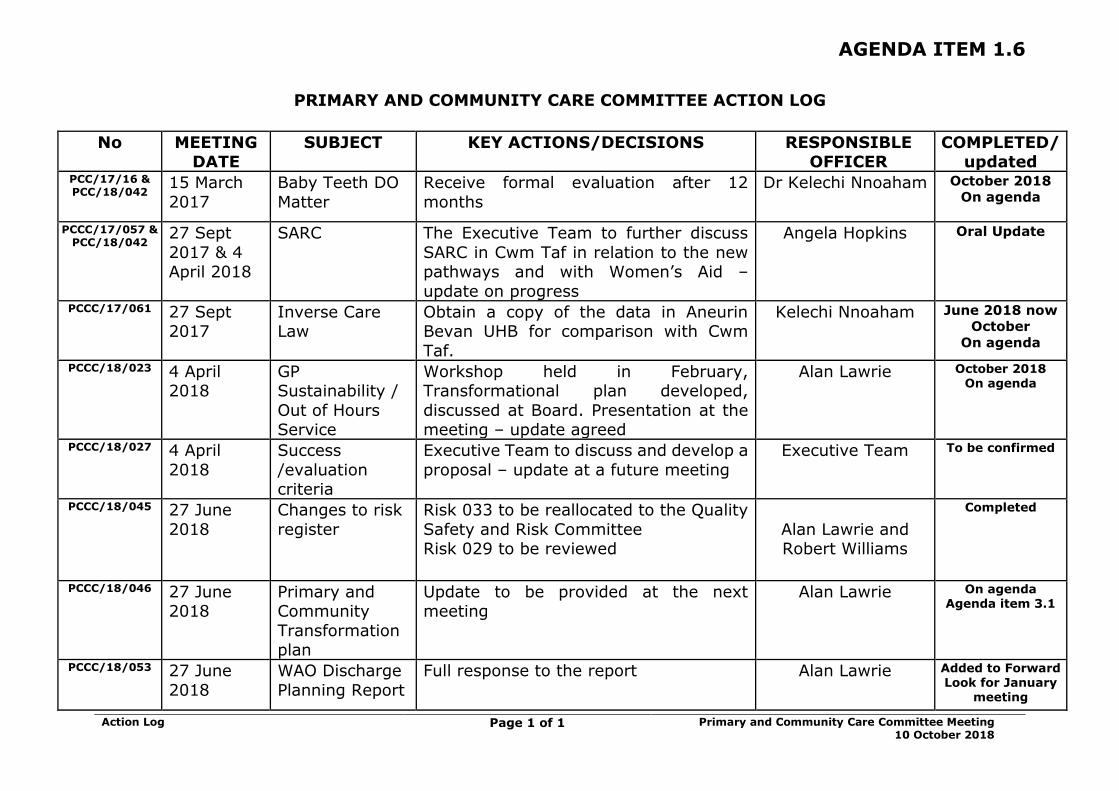
PRIMARY AND COMMUNITY CARE COMMITTEE ACTION LOG
No MEETING
DATE SUBJECT KEY ACTIONS/DECISIONS RESPONSIBLE
OFFICER COMPLETED/
updated PCC/17/16 & PCC/18/042
15 March
2017
Baby Teeth DO
Matter
Receive formal evaluation after 12
months
Dr Kelechi Nnoaham October 2018
On agenda
PCCC/17/057 & PCC/18/042
27 Sept
2017 & 4 April 2018
SARC The Executive Team to further discuss
SARC in Cwm Taf in relation to the new pathways and with Women’s Aid –
update on progress
Angela Hopkins Oral Update
PCCC/17/061 27 Sept 2017
Inverse Care Law
Obtain a copy of the data in Aneurin Bevan UHB for comparison with Cwm
Taf.
Kelechi Nnoaham June 2018 now
October
On agenda
PCCC/18/023 4 April 2018
GP Sustainability /
Out of Hours Service
Workshop held in February, Transformational plan developed,
discussed at Board. Presentation at the meeting – update agreed
Alan Lawrie October 2018 On agenda
PCCC/18/027 4 April
2018
Success
/evaluation criteria
Executive Team to discuss and develop a
proposal – update at a future meeting
Executive Team To be confirmed
PCCC/18/045 27 June
2018
Changes to risk
register
Risk 033 to be reallocated to the Quality
Safety and Risk Committee Risk 029 to be reviewed
Alan Lawrie and Robert Williams
Completed
PCCC/18/046 27 June 2018
Primary and Community
Transformation plan
Update to be provided at the next meeting
Alan Lawrie On agenda Agenda item 3.1
PCCC/18/053 27 June
2018
WAO Discharge
Planning Report
Full response to the report Alan Lawrie Added to Forward Look for January
meeting

2.1 Baby Teeth Do Matter - 12 Month Evaluation Report
1 2.1 Baby Teeth DO Matter PCCC 10 Oct 2018 GR.docx
Baby Teeth DO Matter Page 1 of 7 Primary and Community Care
Committee Meeting
10 October 2018
AGENDA ITEM 2.1
10 October 2018
Primary and Community Care Committee Report
BABY TEETH DO MATTER
Executive Lead: Director of Primary Care, Community & Mental Health
Author: Allison Green, Primary Care Development Manager
Contact Details for further information: 01685 351310 or email
Purpose of the Primary and Community Care Committee Report
The purpose of this report is to provide the Committee with an evaluation
of the first year of the ‘Baby Teeth DO Matter’ initiative. One of the actions being undertaken as part of the action plan to improve children’s oral health
across Cwm Taf.
Governance
Link to Health Board Strategic
Objective(s)
The Board’s overarching role is to ensure its Strategy outlined within ‘Cwm Taf Cares’ 3 Year Integrated
Medium Term Plan 2015-2018 and the related organisational objectives aligned with the Institute of
Healthcare Improvement's (IHI) ‘Triple Aim’ are being progressed, these in summary are:
• To improve quality, safety and patient experience. • To protect and improve population health.
• To ensure that the services provided are accessible and sustainable into the future.
• To provide strong governance and assurance.
• To ensure good value based care and treatment for our patients in line with the resources made available
to the Health Board. This report supports all of the Strategic Objectives.
Supporting evidence
N/A
Engagement – Who has been involved in this work?
Primary Care, General Dental Practices & GP practices
Baby Teeth DO Matter Page 2 of 7 Primary and Community Care
Committee Meeting
10 October 2018
Primary and Community Care Committee Resolution to:
APPROVE ENDORSE DISCUSS NOTE
Recommendation The Primary and Community Care Committee is
asked to • NOTE the ENDORSE the report.
Summarise the Impact of the Primary and Community Care Committee Report
Equality and diversity
To ensure that high quality oral health care is available to all children served by Cwm Taf
University Health Board.
Legal implications n/a
Population Health The initiative aims to promote the importance of oral health care in children.
Quality, Safety &
Patient Experience
The initiative aims to improve the quality, safety
and patient experience in oral health care.
Resources No additional resources required as managed from
within the existing GDS Contracts
Risks and Assurance Failure to increase the number of children
attending a general dental practice resulting in no
improvement to children’s oral health.
Health & Care
Standards
The 22 Health & Care Standards for NHS Wales
are mapped into the 7 Quality Themes: Staying Healthy Safe Care
Effective Care Dignified Care Timely Care Individual Care
Staff & Resources http://www.wales.nhs.uk/sitesplus/documents/1
064/24729_Health%20Standards%20Framework_2015_E1.pdf
Workforce No additional UHB staff are required. Initiative is
delivered by general dental practices.
Freedom of
information status
Open
Baby Teeth DO Matter Page 3 of 7 Primary and Community Care
Committee Meeting
10 October 2018
BABY TEETH DO MATTER
1. SITUATION / PURPOSE OF REPORT
The purpose of this report is to provide the Committee with an evaluation of the first year of the ‘Baby Teeth DO Matter’ initiative. One of the actions being undertaken as
part of the action plan to improve children’s oral health across Cwm Taf.
2. BACKGROUND / INTRODUCTION
The Health Board introduced the initiative Baby Teeth DO Matter in April 2017 because
the latest epidemiology survey showed the levels of dental caries in Cwm Taf children under 5 years of age were the highest in Wales, i.e. 58.6% of 5 year old children in
Merthyr Tydfil and 43.1% of 5 year old children in Rhondda Cynon Taf have decayed, missing or filled teeth (dmft), compared to the Wales average of 34.5%.
The survey of 3 year-old children showed that 21% of Cwm Taf 3 year olds had tooth decay compared to the Wales average of 14.5%. Plus the end of year dental activity
data for 2015/16 showed that only approximately 40% of children under the age of 5 years of age had visited a dentist in the previous 2 years. As a result, improvement
of children’s oral health was identified as a local priority for Cwm Taf within the Local Oral Health Plan.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
Baby Teeth DO Matter is based on a scheme that was trialled in Manchester and proved successful in increasing the number of children accessing routine dental
treatment.
There are two aspects to this pilot: • Getting the youngest children in our communities off to the best start with
regards to their dental health • Educating, informing and involving the community in improving their own health
and well being.
The pilot, which was offered to dental practices in Merthyr Tydfil, aimed to identify
children under 5 years old who had not attended a dentist in the last two years in order to deliver a simple evidence based oral health message and to encourage
regular attendance at a dental practice.
Initially 5 dental practices expressed an interest in participating in the pilot but 1 practice dropped out without taking part and another practice dropped out after 4
months so there are currently 3 dental practices participating in the Merthyr Tydfil area.
The dentist or dental therapist identifies children under 5 years of age by attending
baby clinics in GP practices and working with the Health Visitors and Practice Nurses.
Baby Teeth DO Matter Page 4 of 7 Primary and Community Care
Committee Meeting
10 October 2018
In order to take part and embed the Baby Teeth DO Matter project into the General
Dental Services Contract (GDS) Practices needed to deliver the following:
• Actively identify children age 0-5 years who have not attended a dental
practice in the previous two years and positively promote the initiative • Provide access to the eligible children
• Provide an assessment with advice and intervention according to protocols • Provide fluoride varnish application where appropriate
• Provide evidence based oral health messages which are reinforced using leaflets to promote tooth friendly routine for life
• Provide re-attendance opportunities.
The Health Board did not incur any additional costs as the initiative was managed within their existing GDS contract. Practices’ contracted Units of Dental Activity (UDA)
were reduced by 5% and instead of achieving UDAs, the funding was used to pay the dentist/dental therapist to attend the baby clinics.
Even though the pilot of Baby Teeth DO Matter, where dentists proactively identify
children to attend their practices, is only in the Merthyr Tydfil locality, a communication campaign to encourage children to come forward, has been
undertaken throughout Cwm Taf. Members may wish to note that access to general
dental services is not an issue in the area as every dental practice in Merthyr Tydfil is accepting new NHS patients (both adults and children).
OUTCOMES
The pilot did not work for everyone, with one practice deciding to stop participating
after 4 months because they were not seeing an increase in the number of children attending the practice.
From the evidence gathered to date, it would appear that for the initiative to be
successful the right person needs to provide the oral health messages; the Practice Nurse and the Health Visitor in the GP practice fully engage in the process and that
there is a separate room in the practice for the dentist/dental therapist to have a confidential conversation with the parent.
The initiative has not worked as well in some GP practices and this may be because there is no separate private consulting room and the oral health messages have to be
delivered in the corridor. As a consequence the dentist/dental therapist may not have been seen by the patient as being part of the wider baby clinic team.
When comparing the percentage of children attending a general dental practice (in
the last 24 months) in 2017/18 to 2016/17 the results are as follows:
Cwm Taf UHB Merthyr Tydfil
Children 0-17 years of age 4.48% 7.27%
Children 3-5 years of age 4.17% 11.62%
Children 0-2 years of age 16.90% 39.53%
Baby Teeth DO Matter Page 5 of 7 Primary and Community Care
Committee Meeting
10 October 2018
Encouragingly, an additional 1,570 children in Cwm Taf (0-17 years) attended a general dental practice compared to the same period in 2016/17.
As the initiative in Merthyr Tydfil is focussed on the dentist/dental therapist attending baby clinics to speak to parents, it is not surprising that the 0-2 year old age group
has seen the highest increase in patient numbers, compared to the previous year. The aim of the initiative is that as soon as the first tooth erupts the child should attend
a dental practice for routine dental care.
The number of under 5 year old children attending a general dental practice has also increased across the other localities where the UHB has been advertising the
awareness campaign. However, the numbers have not been as dramatic as in Merthyr Tydfil where the 3 dental practices are working with GP practices.
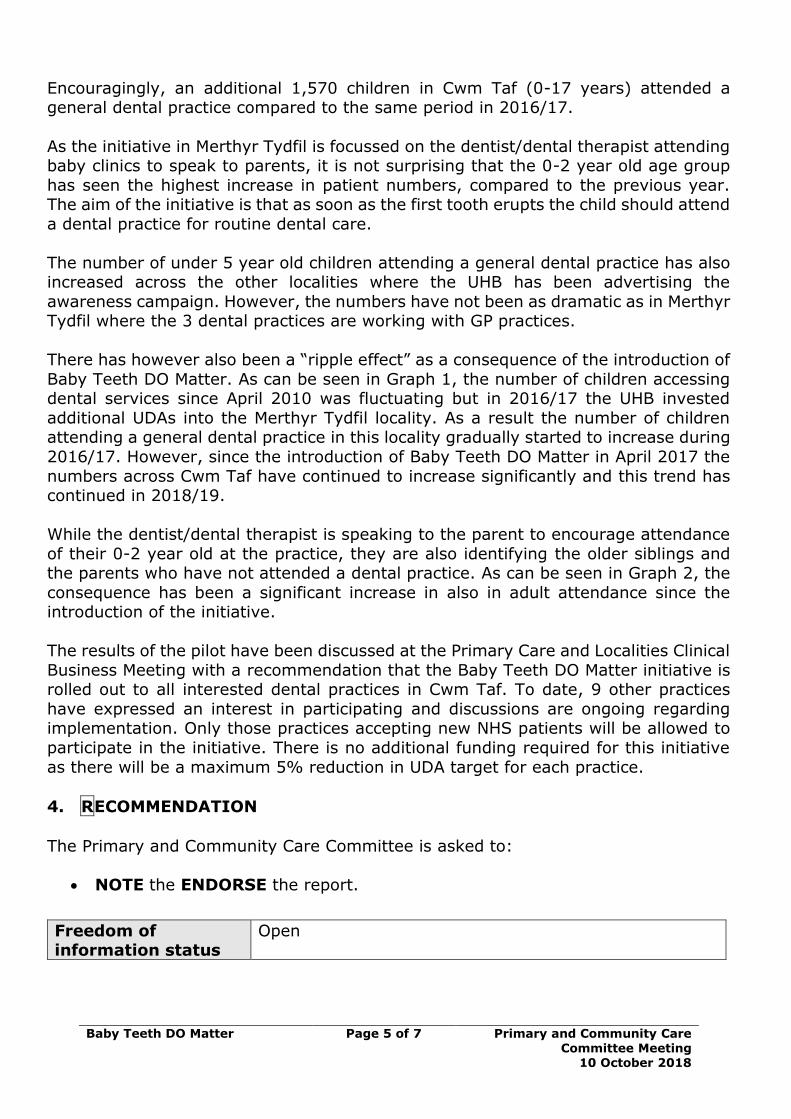
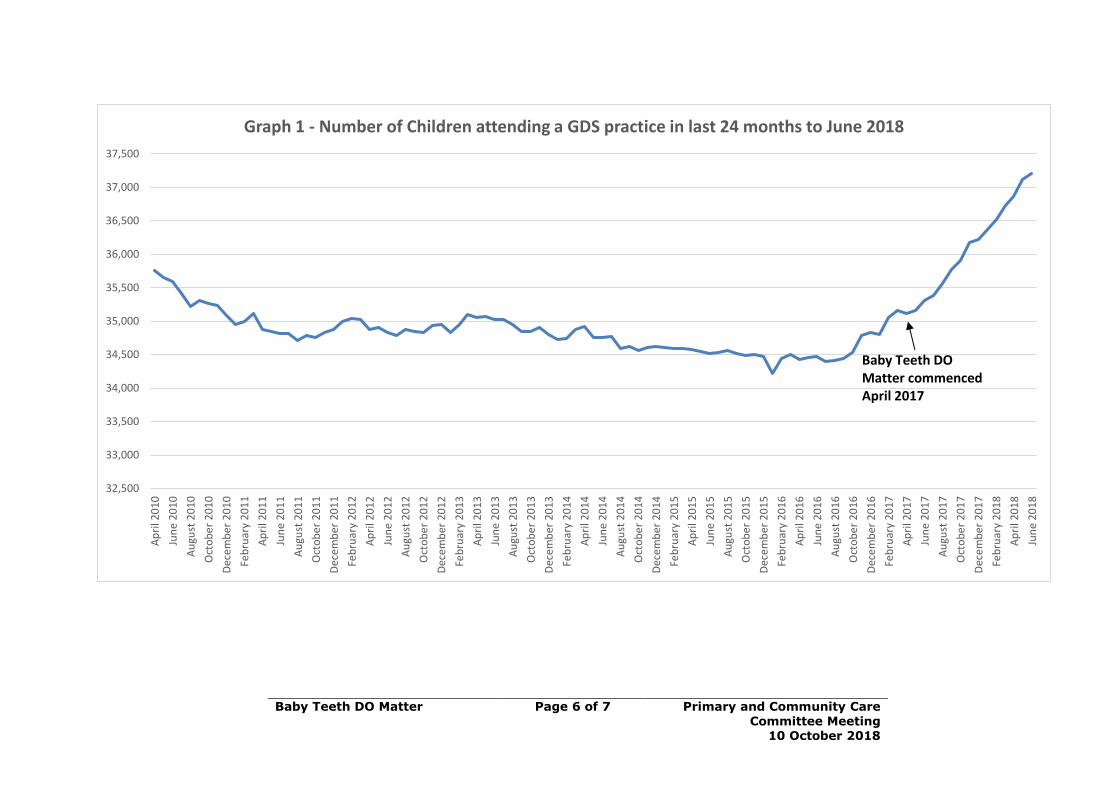
There has however also been a “ripple effect” as a consequence of the introduction of
Baby Teeth DO Matter. As can be seen in Graph 1, the number of children accessing dental services since April 2010 was fluctuating but in 2016/17 the UHB invested
additional UDAs into the Merthyr Tydfil locality. As a result the number of children attending a general dental practice in this locality gradually started to increase during
2016/17. However, since the introduction of Baby Teeth DO Matter in April 2017 the
numbers across Cwm Taf have continued to increase significantly and this trend has continued in 2018/19.
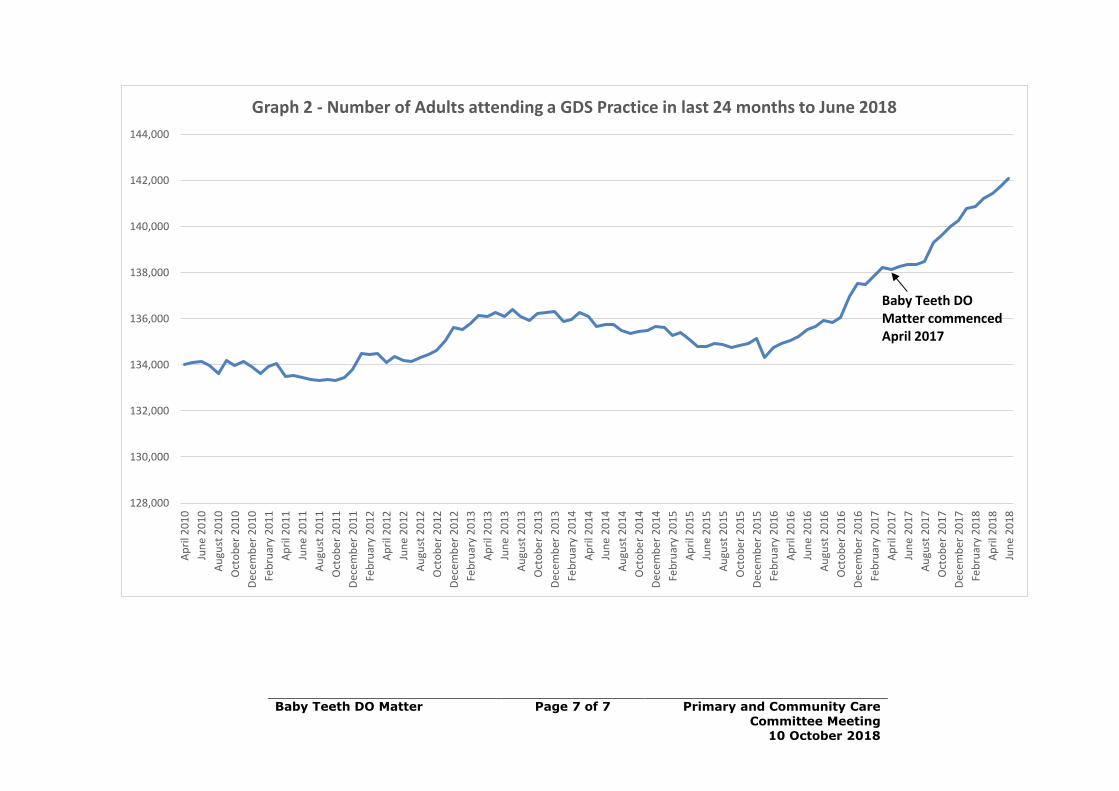
While the dentist/dental therapist is speaking to the parent to encourage attendance
of their 0-2 year old at the practice, they are also identifying the older siblings and the parents who have not attended a dental practice. As can be seen in Graph 2, the
consequence has been a significant increase in also in adult attendance since the introduction of the initiative.
The results of the pilot have been discussed at the Primary Care and Localities Clinical
Business Meeting with a recommendation that the Baby Teeth DO Matter initiative is rolled out to all interested dental practices in Cwm Taf. To date, 9 other practices
have expressed an interest in participating and discussions are ongoing regarding implementation. Only those practices accepting new NHS patients will be allowed to
participate in the initiative. There is no additional funding required for this initiative
as there will be a maximum 5% reduction in UDA target for each practice.
4. RECOMMENDATION
The Primary and Community Care Committee is asked to:
• NOTE the ENDORSE the report.
Freedom of information status
Open
Baby Teeth DO Matter Page 6 of 7 Primary and Community Care
Committee Meeting 10 October 2018
32,500
33,000
33,500
34,000
34,500
35,000
35,500
36,000
36,500
37,000
37,500A
pri
l 20
10
Jun
e 2
01
0
Au
gust
20
10
Oct
ob
er
20
10
Dec
em
ber
20
10
Feb
ruar
y 2
01
1
Ap
ril 2
01
1
Jun
e 2
01
1
Au
gust
20
11
Oct
ob
er
20
11
Dec
em
ber
20
11
Feb
ruar
y 2
01
2
Ap
ril 2
01
2
Jun
e 2
01
2
Au
gust
20
12
Oct
ob
er
20
12
Dec
em
ber
20
12
Feb
ruar
y 2
01
3
Ap
ril 2
01
3
Jun
e 2
01
3
Au
gust
20
13
Oct
ob
er
20
13
Dec
em
ber
20
13
Feb
ruar
y 2
01
4
Ap
ril 2
01
4
Jun
e 2
01
4
Au
gust
20
14
Oct
ob
er
20
14
Dec
em
ber
20
14
Feb
ruar
y 2
01
5
Ap
ril 2
01
5
Jun
e 2
01
5
Au
gust
20
15
Oct
ob
er
20
15
Dec
em
ber
20
15
Feb
ruar
y 2
01
6
Ap
ril 2
01
6
Jun
e 2
01
6
Au
gust
20
16
Oct
ob
er
20
16
Dec
em
ber
20
16
Feb
ruar
y 2
01
7
Ap
ril 2
01
7
Jun
e 2
01
7
Au
gust
20
17
Oct
ob
er
20
17
Dec
em
ber
20
17
Feb
ruar
y 2
01
8
Ap
ril 2
01
8
Jun
e 2
01
8
Graph 1 - Number of Children attending a GDS practice in last 24 months to June 2018
Baby Teeth DOMatter commencedApril 2017
Baby Teeth DO Matter Page 7 of 7 Primary and Community Care
Committee Meeting 10 October 2018
128,000
130,000
132,000
134,000
136,000
138,000
140,000
142,000
144,000
Ap
ril 2
01
0
Jun
e 2
01
0
Au
gust
20
10
Oct
ob
er
20
10
Dec
em
ber
20
10
Feb
ruar
y 2
01
1
Ap
ril 2
01
1
Jun
e 2
01
1
Au
gust
20
11
Oct
ob
er
20
11
Dec
em
ber
20
11
Feb
ruar
y 2
01
2
Ap
ril 2
01
2
Jun
e 2
01
2
Au
gust
20
12
Oct
ob
er
20
12
Dec
em
ber
20
12
Feb
ruar
y 2
01
3
Ap
ril 2
01
3
Jun
e 2
01
3
Au
gust
20
13
Oct
ob
er
20
13
Dec
em
ber
20
13
Feb
ruar
y 2
01
4
Ap
ril 2
01
4
Jun
e 2
01
4
Au
gust
20
14
Oct
ob
er
20
14
Dec
em
ber
20
14
Feb
ruar
y 2
01
5
Ap
ril 2
01
5
Jun
e 2
01
5
Au
gust
20
15
Oct
ob
er
20
15
Dec
em
ber
20
15
Feb
ruar
y 2
01
6
Ap
ril 2
01
6
Jun
e 2
01
6
Au
gust
20
16
Oct
ob
er
20
16
Dec
em
ber
20
16
Feb
ruar
y 2
01
7
Ap
ril 2
01
7
Jun
e 2
01
7
Au
gust
20
17
Oct
ob
er
20
17
Dec
em
ber
20
17
Feb
ruar
y 2
01
8
Ap
ril 2
01
8
Jun
e 2
01
8
Graph 2 - Number of Adults attending a GDS Practice in last 24 months to June 2018
Baby Teeth DOMatter commencedApril 2017
2.2 Organisational Risk Register
1 2.2 Org Risk Register PCCC 10 Oct 2018 GRa.doc
Organisational Risk Register Page 1 of 17 Primary and Community Care Committee Meeting
10 October 2018
AGENDA ITEM 2.2
10 October 2018
Primary and Community Care Committee Report
ORGANISATIONAL RISK REGISTER
Executive Lead: Board Secretary / Director of Corporate Services and Governance
Author: Head of Corporate Services
Contact Details for further information: Gwenan Roberts 01443
744800 or [email protected]
Purpose of the Primary and Community Care Committee Report
The purpose of this report is for the Primary and Community Care Committee
to receive, review and discuss the organisational risk register and consider whether the recorded risks are appropriately assigned. This Organisational
Risk Register was last considered by the Executive Board in August 2018, by
the Quality Safety and Risk Committee and the Health Board in September 2018 and has been updated to reflect related discussions.
Governance
Link to Health
Board Strategic Objective(s)
The Board’s overarching role is to ensure its strategic
objectives, and the related organisational objectives outlined within the 3 Year Integrated Medium Term Plan
2018-2021, are being progressed. Aligned with the ‘Quadruple Aim’ described within ‘A Healthier Wales’
(Welsh Government, June 2018) these objectives are: • To improve quality, safety and patient experience
• To protect and improve population health • To ensure that the services provided are accessible
and sustainable into the future
• To provide strong governance and assurance • To ensure good value based care and treatment for
our patients in line with the resources made available to the Health Board.
This report focuses mainly on providing strong governance and assurance.
Supporting
evidence
• There are a number of assessments that help inform
the content of the organisational risk register. • The content of this report is informed by the University
Health Board’s (UHB) Risk Management Strategy.
Engagement – Who has been involved in this work?
The information contained within this report has been developed following engagement with senior staff and Executive Directors.
Organisational Risk Register Page 2 of 17 Primary and Community Care Committee Meeting
10 October 2018
Primary and Community Care Committee Resolution to:
APPROVE ENDORSE √ DISCUSS √ NOTE √
Recommendation The Primary and Community Care Committee is asked to: • DISCUSS and NOTE the update provided within
this report and the risks assigned to the Board and its Committees and,
• ENDORSE the updated risk register and the assignment of risks.
Summarise the Impact of the Primary and Community Care Committee Report
Equality and
diversity
There are no identified equality & diversity implications.
Legal implications It is essential that the Board has robust arrangements in place to assess, capture and
mitigate risks faced by the organisation, as failure to do so could have legal implications for the UHB.
Population Health No specific impact.
Quality, Safety & Patient Experience
Ensuring the organisation has robust risk management arrangements in place that ensure
organisational risks are captured, assessed and mitigating actions are taken, is a key requisite to
ensuring the quality, safety & experience of patients receiving care and staff working in the UHB.
Resources The risks outlined within this report have resource
implications which are being addressed by the
respective Executive Director leads and taken into consideration as part of the Board’s IMTP
processes. Risks and Assurance This report and the organisational risk register is an
integral element of the Board’s risk and assurance arrangements. It should be no ted that this work
continues to develop.
Health & Care Standards
The 22 Health & Care Standards for NHS Wales are mapped into the 7 Quality Themes but within a
Governance Framework. This report focuses mainly on Governance & Accountability but also spans
many of the 7 quality themes. Workforce Failure to capture, assess and mitigate risks can
impact adversely on the workforce.
Freedom of Information
status
Open
Organisational Risk Register Page 3 of 17 Primary and Community Care Committee Meeting
10 October 2018
ORGANISATIONAL RISK REGISTER
1. SITUATION / PURPOSE OF REPORT
The purpose of this report is for the Primary and Community Care
Committee to review and discuss the organisational risk register and
consider whether the assessed and recorded risks are appropriately assigned. The Organisational Risk Register was last considered by the
Executive Board in August 2018, by the Quality Safety and Risk Committee (QSR) and the Health Board in September 2018. Changes made since are
identified in RED font.
2. BACKGROUND / INTRODUCTION
The organisational Risk Register summarises the key ‘live’ extreme risks facing the Health Board and the actions being taken to mitigate them. The
Health Board manages risk through i t s Directorate structures and in
close alignment with the Board’s ‘approved’ Assurance Framework. The Assurance Framework reports into the Audit Committee for periodical
review, monitoring and scrutiny and also features (at least annually) on the agenda of the Board.
It is also important to NOTE that the Executives, as risk owners, are
appropriately sighted and involved in the development of the organisational risk register, providing updates, including reports on
mitigating actions. The organisational risk register is reviewed and where appropriate updated on a bi-monthly basis with input from the Executive
lead as required.
All organisational risks have a lead Executive Director and the risk assigned to either the Board, or as appropriate, a Committee of the Board
to ensure appropriate review, scrutiny and where relevant updating. Each Director is responsible for the ownership of the risk(s) and the reporting of
the actions in place to manage/control and/or mitigate the risks.
The organisational Risk Register is reported quarterly to the Executive
Board and routinely to the Quality, Safety & Risk Committee of the Board, for information and where appropriate, scrutiny of any assigned risks.
Whilst this cover report summarizes the detail, the supporting appendices provide more detail.
Improvement continues to be made with directorates and localities
routinely completing integrated risk reporting templates that are used for exception reporting.
3. ASSESSMENT OF GOVERNANCE AND RISK ISSUES
Following discussion at the Executive Board in August and Quality, Safety & Risk Committee in September, the following changes to the register were
Organisational Risk Register Page 4 of 17 Primary and Community Care Committee Meeting
10 October 2018
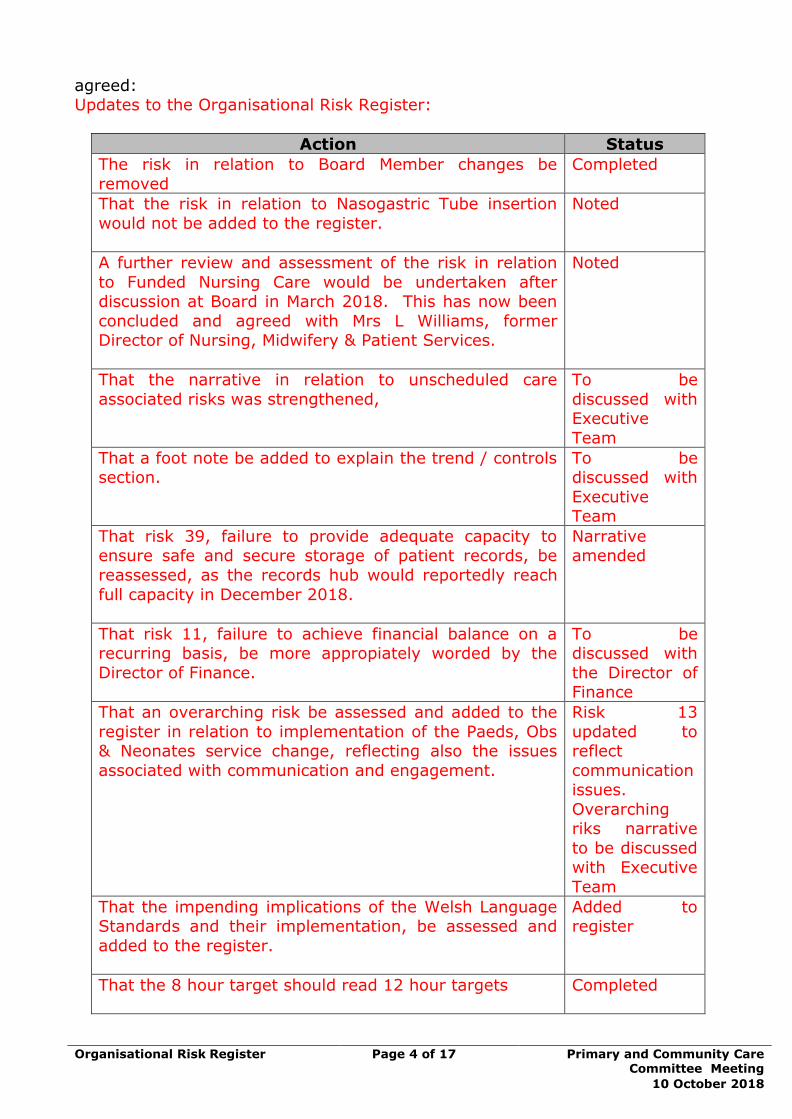
agreed: Updates to the Organisational Risk Register:
Action Status
The risk in relation to Board Member changes be
removed
Completed
That the risk in relation to Nasogastric Tube insertion
would not be added to the register.
Noted
A further review and assessment of the risk in relation
to Funded Nursing Care would be undertaken after discussion at Board in March 2018. This has now been
concluded and agreed with Mrs L Williams, former Director of Nursing, Midwifery & Patient Services.
Noted
That the narrative in relation to unscheduled care
associated risks was strengthened,
To be
discussed with Executive
Team
That a foot note be added to explain the trend / controls section.
To be discussed with
Executive Team
That risk 39, failure to provide adequate capacity to ensure safe and secure storage of patient records, be
reassessed, as the records hub would reportedly reach
full capacity in December 2018.
Narrative amended
That risk 11, failure to achieve financial balance on a recurring basis, be more appropiately worded by the
Director of Finance.
To be discussed with
the Director of Finance
That an overarching risk be assessed and added to the
register in relation to implementation of the Paeds, Obs & Neonates service change, reflecting also the issues
associated with communication and engagement.
Risk 13
updated to reflect
communication issues.
Overarching riks narrative
to be discussed with Executive
Team
That the impending implications of the Welsh Language Standards and their implementation, be assessed and
added to the register.
Added to register
That the 8 hour target should read 12 hour targets
Completed
Organisational Risk Register Page 5 of 17 Primary and Community Care Committee Meeting
10 October 2018
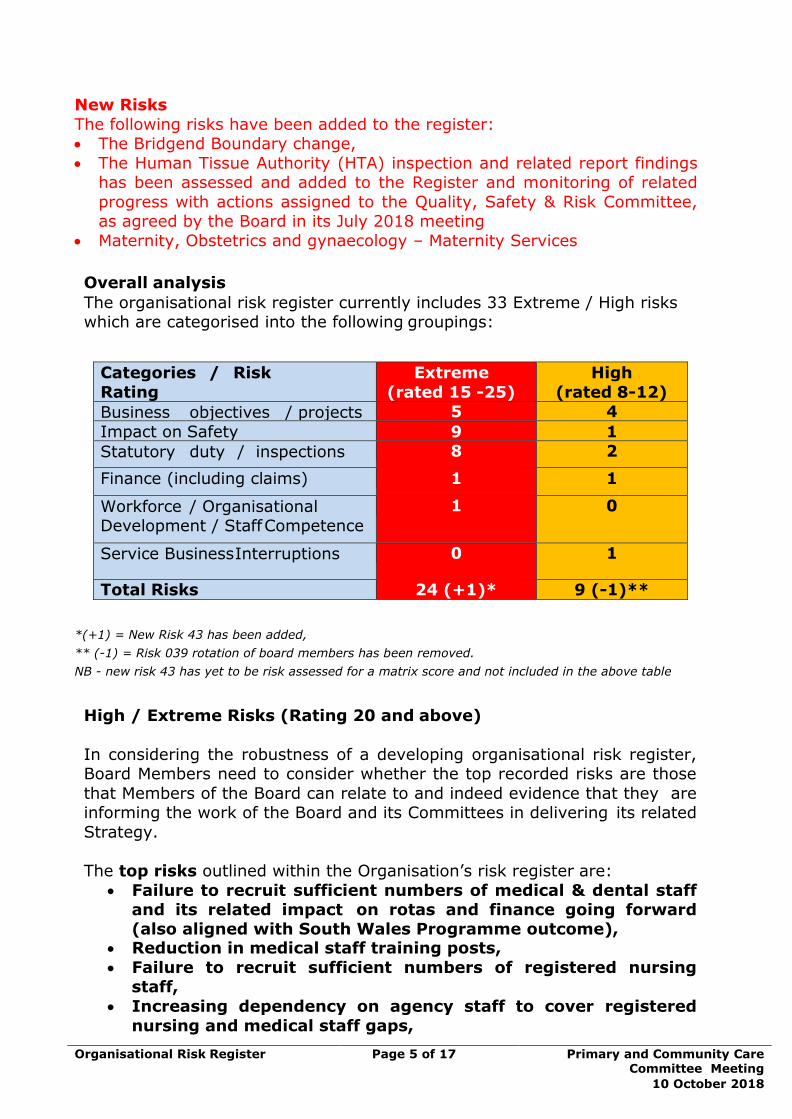
New Risks
The following risks have been added to the register: • The Bridgend Boundary change,
• The Human Tissue Authority (HTA) inspection and related report findings has been assessed and added to the Register and monitoring of related
progress with actions assigned to the Quality, Safety & Risk Committee, as agreed by the Board in its July 2018 meeting
• Maternity, Obstetrics and gynaecology – Maternity Services
Overall analysis
The organisational risk register currently includes 33 Extreme / High risks which are categorised into the following groupings:
Categories / Risk
Rating
Extreme
(rated 15 -25)
High
(rated 8-12)
Business objectives / projects 5 4
Impact on Safety 9 1
Statutory duty / inspections 8 2
Finance (including claims) 1 1
Workforce / Organisational Development / Staff Competence
1 0
Service Business Interruptions 0 1
Total Risks 24 (+1)* 9 (-1)**
*(+1) = New Risk 43 has been added,
** (-1) = Risk 039 rotation of board members has been removed.
NB - new risk 43 has yet to be risk assessed for a matrix score and not included in the above table
High / Extreme Risks (Rating 20 and above)
In considering the robustness of a developing organisational risk register, Board Members need to consider whether the top recorded risks are those
that Members of the Board can relate to and indeed evidence that they are informing the work of the Board and its Committees in delivering its related
Strategy.
The top risks outlined within the Organisation’s risk register are:
• Failure to recruit sufficient numbers of medical & dental staff and its related impact on rotas and finance going forward (also aligned with South Wales Programme outcome),
• Reduction in medical staff training posts,
• Failure to recruit sufficient numbers of registered nursing staff,
• Increasing dependency on agency staff to cover registered
nursing and medical staff gaps,
Organisational Risk Register Page 6 of 17 Primary and Community Care Committee Meeting
10 October 2018
• Deprivation of Liberties Safeguards (DoLS) mainly associated with the volume / backlog of related assessments,
• Fire Safety compliance and ongoing issues with Prince Charles
Hospital (PCH) site (Ground & First Floor),
• Lack of control and capacity to accommodate all hospital
follow up outpatient appointments, • Failure to ensure delivery of a viable balanced/break even 3
year integrated medium term plan,
• Achieving financial break even on a recurring basis,
• Human Tissue Authority (HTA) report, • Bridgend Boundary Change,
• Health Records Storage,
• Welsh Language Standards Compliance.
Of the categorised risks, these have been broken down under one of our existing Strategic Objectives:
• There are currently 24 extreme (increased by 4) and 9 high (reduced by
1) risk, assigned to the Board and its various Committees
• The majority of assessed risks are linked with workforce shortages and
their related impact, which includes GP shortages and Primary Care Sustainability.

Organisational Risk Register Page 7 of 17 University Health Board Meeting
27 September 2018
Risk Register Category – Business Objectives / Projects (9 risks)
Strategic
Objective
Risk
Reference
Description of risk
identified
Initial
Score
Current
Score
Trend Controls Last
Reviewed
Scrutiny
Committee
Setting the
Direction and
Performance
and
Operational
Efficiency
028
Failure to ensure delivery of a viable
balanced/break even 3 year
integrated medium term plan.
20
(was 16)
20
Sept 2018 Health Board
015
Reputational damage & potential legal
challenge on the decision making on
Funded Nursing Care (FNC). 16 12
Sept 2018 Health Board
029
Failure to sustain Primary Care
Services, across RCT and Merthyr
Tydfil but particularly in the Rhondda
Valleys.
16 16
Sept 2018 Primary & Community
Care
036 Primary Care Workforce - Recruitment
and sustainability 16 16
Sept 2018 Primary & Community
Care
030
Failure to continue to provide and
sustain GP Out of Hours Services as
currently configured.
16 16
Sept 2018 Primary & Community
Care
002 Failure to achieve Referral to
Treatment targets. 12 12
(was 20)
Sept 2018 Finance, Performance
& Workforce
003
Failure to achieve the 4 and 12 hour
emergency (A&E) waiting times
targets. 12 16
Sept 2018 Finance, Performance &
Workforce
013 Implementation of South Wales
Programme outcomes.
12 12 Sept 2018 Health Board
023
Failure to meet the timescale relating
to issuing concerns (complaints)
responses to patients and/or carers.
16 12
Sept 2018 Quality, Safety & Risk
The Trend column indicates whether the risk overall (from when first assessed), is increasing (), reducing () or unchanged ().
The Controls column indicates whether assessed controls overall are improved (), reduced () or unchanged () from when first
assessed. Regardless of whether the risks rating has changed.

Organisational Risk Register Page 8 of 17 University Health Board Meeting
27 September 2018
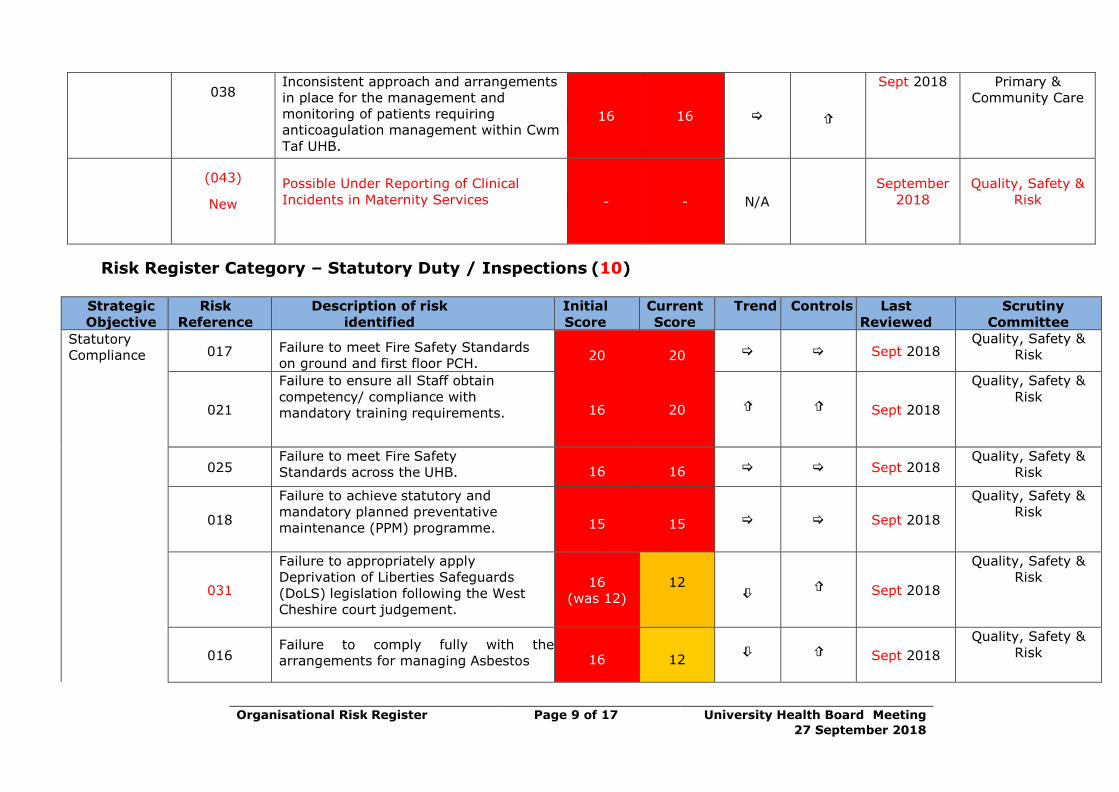
Risk Register Category - Impact on Safety (10 risks)
Strategic
Objective
Risk
Reference
Description of risk identified Initial
Score
Current
Score
Trend Controls Last
Reviewed
Scrutiny
Committee
To improve
quality,
safety
and patient
experience.
007
Failure to recruit sufficient medical &
dental staff. 25 20
Sept 2018 Quality, Safety &
Risk
034
Increasing dependency on Agency Staff
cover in Medical and Nursing areas,
which has the potential to impact on
continuity of care and patient safety and
is actually impacting on the UHB
financial position.
20 20 Sept 2018 Quality, Safety &
Risk
035 Failure to recruit sufficient registered
nursing staff. 20 20 Sept 2018 Quality, Safety
& Risk
008
Reduction in medical training posts
within various specialties & capacity to
meet workload demands.
20
20 Sept 2018
Quality, Safety &
Risk
027
Lack of control and capacity to
accommodate all hospital follow up
outpatient appointments.
20
20
(was 16)
Sept 2018 Finance,
Performance &
Workforce
032 Sustainability of a safe & effective
Ophthalmology Service.
20
16
Sept 2018
Quality, Safety
& Risk
005
Failure to sustain services as currently
configured to meet cancer targets.
20 16
Sept 2018 Finance,
Performance &
Workforce
033
Failure to sustain Child & Adolescent
Mental Health Services across the
Network
16 16
Sept 2018
Quality, Safety &
Risk
037
Ensuring the development, approval and
implementation of a Strategy for IM&T,
that is clinically led and supports staff in
care delivery
12 12
Sept 2018
Health Board
Organisational Risk Register Page 9 of 17 University Health Board Meeting
27 September 2018
038
Inconsistent approach and arrangements
in place for the management and
monitoring of patients requiring
anticoagulation management within Cwm
Taf UHB.
16 16
Sept 2018 Primary &
Community Care
(043)
New
Possible Under Reporting of Clinical
Incidents in Maternity Services - - N/A
September
2018
Quality, Safety &
Risk
Risk Register Category – Statutory Duty / Inspections (10)
Strategic
Objective
Risk
Reference
Description of risk
identified
Initial
Score
Current
Score
Trend Controls Last
Reviewed
Scrutiny
Committee
Statutory
Compliance 017 Failure to meet Fire Safety Standards
on ground and first floor PCH. 20 20 Sept 2018
Quality, Safety &
Risk
021
Failure to ensure all Staff obtain
competency/ compliance with
mandatory training requirements. 16 20
Sept 2018
Quality, Safety &
Risk
025 Failure to meet Fire Safety
Standards across the UHB. 16 16 Sept 2018 Quality, Safety &
Risk
018
Failure to achieve statutory and
mandatory planned preventative
maintenance (PPM) programme. 15 15 Sept 2018
Quality, Safety &
Risk
031
Failure to appropriately apply
Deprivation of Liberties Safeguards
(DoLS) legislation following the West
Cheshire court judgement.
16
(was 12)
12
Sept 2018
Quality, Safety &
Risk
016 Failure to comply fully with the
arrangements for managing Asbestos 16 12
Sept 2018
Quality, Safety &
Risk
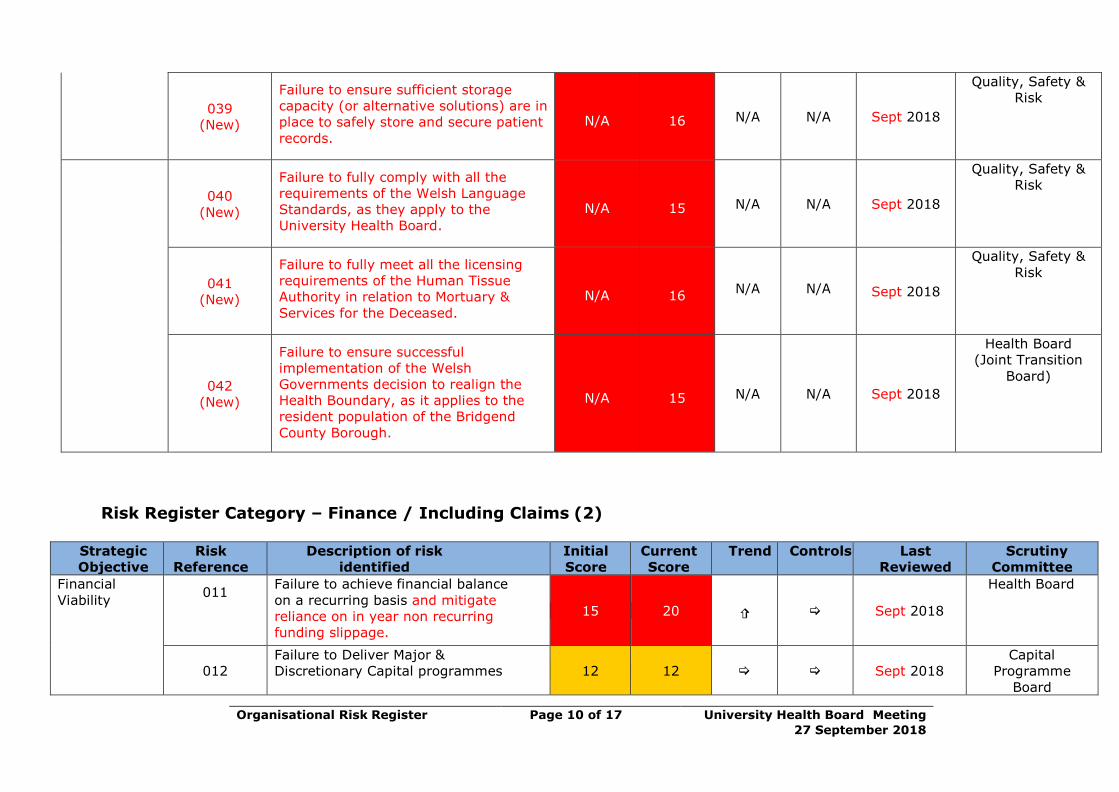
Organisational Risk Register Page 10 of 17 University Health Board Meeting
27 September 2018
039
(New)
Failure to ensure sufficient storage
capacity (or alternative solutions) are in
place to safely store and secure patient
records.
N/A 16 N/A N/A Sept 2018
Quality, Safety &
Risk
040
(New)
Failure to fully comply with all the
requirements of the Welsh Language
Standards, as they apply to the
University Health Board.
N/A 15 N/A N/A Sept 2018
Quality, Safety &
Risk
041
(New)
Failure to fully meet all the licensing
requirements of the Human Tissue
Authority in relation to Mortuary &
Services for the Deceased.
N/A 16
N/A
N/A Sept 2018
Quality, Safety &
Risk
042
(New)
Failure to ensure successful
implementation of the Welsh
Governments decision to realign the
Health Boundary, as it applies to the
resident population of the Bridgend
County Borough.
N/A 15 N/A N/A Sept 2018
Health Board
(Joint Transition
Board)
Risk Register Category – Finance / Including Claims (2)
Strategic
Objective
Risk
Reference
Description of risk
identified
Initial
Score
Current
Score
Trend Controls Last
Reviewed
Scrutiny
Committee
Financial
Viability 011
Failure to achieve financial balance
on a recurring basis and mitigate
reliance on in year non recurring
funding slippage.
15 20
Sept 2018
Health Board
012
Failure to Deliver Major &
Discretionary Capital programmes 12 12 Sept 2018 Capital
Programme
Board
Organisational Risk Register Page 11 of 17 University Health Board Meeting
27 September 2018
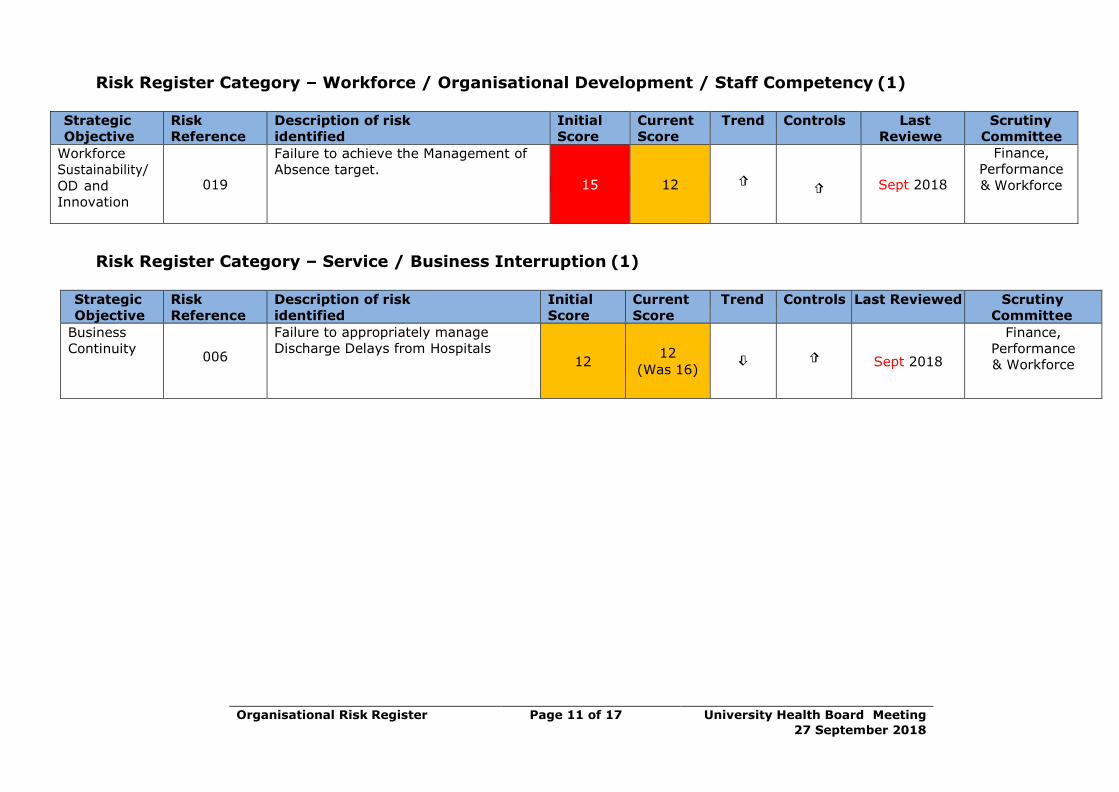
Risk Register Category – Workforce / Organisational Development / Staff Competency (1)
Strategic
Objective
Risk
Reference
Description of risk
identified
Initial
Score
Current
Score
Trend Controls Last
Reviewe
dd
Scrutiny
Committee
Workforce
Sustainability/
OD and
Innovation
019
Failure to achieve the Management of
Absence target. 15 12
Sept 2018
Finance,
Performance
& Workforce
Risk Register Category – Service / Business Interruption (1)
Strategic
Objective
Risk
Reference
Description of risk
identified
Initial
Score
Current
Score
Trend Controls Last Reviewed Scrutiny
Committee
Business
Continuity
006
Failure to appropriately manage
Discharge Delays from Hospitals 12
12
(Was 16)
Sept 2018
Finance,
Performance
& Workforce
Organisational Risk Register Page 12 of 17 Primary and Community Care Committee Meeting
10 October 2018
Quality, safety and patient experience
The Health Board’s risk management arrangements are in place to ensure risks
are assessed and mitigating actions taken to improve the quality, safety and
experience of patients and where appropriate escalation arrangements are in place to inform the Board via its key sub-committees.
Use of resources
There is a significant risk to the service if robust risk based assessment
arrangements are not in place. Good governance arrangements, including effective risk management help to ensure the effective use of resources. It is
important to note that routinely as part of the Internal Audit and Assurance Annual Plan, 3 clinical and 1 corporate directorate undergo a governance review
each year, which includes a review of its risk management arrangements. This
is in addition to the organizational related audit reviews.
Compliance with Legislation There may be an adverse effect on the organization if arrangements are not in
place to manage and mitigate risks.
Performance
Assessment and monitoring of risks within the Health Board is undertaken within Directorates/Localities/Departments. The extreme / high organizational
risks will be monitored by the Executive Team / Board and be reviewed and scrutinized by the Board and/or its Committees.
As a general rule the organisational risk register will be routinely reviewed by
the Quality, Safety & Risk Committee and elements discussed at the Integrated
Governance Committee, although all Committees of the Board have a role to play in ensuring risks assigned to a Board Committee are considered as part of
its work. Risk management arrangements will also be a key element of internal audit work and key risks will help to inform the annual internal audit plan.
4. RECOMMENDATION
The Primary and Community Care Committee is asked to:
• DISCUSS and NOTE the update provided within this report and the risks assigned to the Board and its Committees, and
• ENDORSE the updated risk register and the assignment of risks.
Freedom of
Information
Open
Organisational Risk Register Page 13 of 17 Primary and Community Care Committee Meeting
10 October 2018
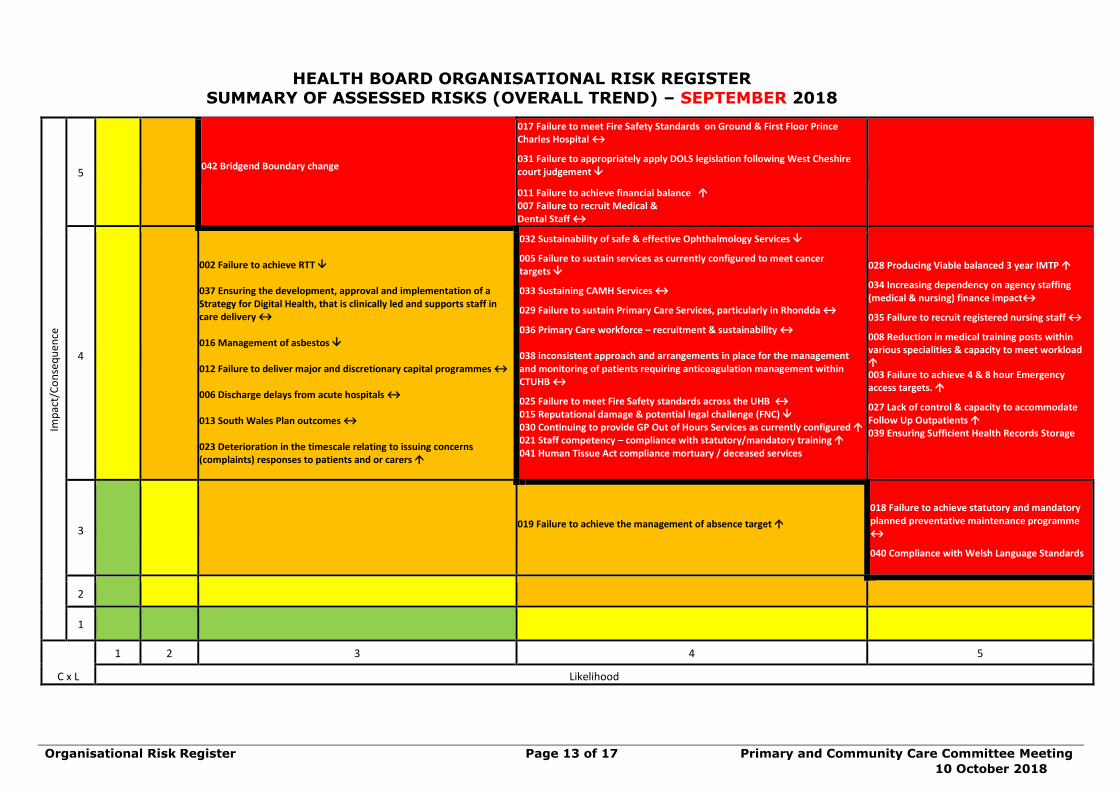
HEALTH BOARD ORGANISATIONAL RISK REGISTER SUMMARY OF ASSESSED RISKS (OVERALL TREND) – SEPTEMBER 2018
Imp
act/
Co
nse
qu
ence
5 042 Bridgend Boundary change
017 Failure to meet Fire Safety Standards on Ground & First Floor Prince Charles Hospital ↔
031 Failure to appropriately apply DOLS legislation following West Cheshire court judgement
011 Failure to achieve financial balance 007 Failure to recruit Medical & Dental Staff ↔
4
002 Failure to achieve RTT 037 Ensuring the development, approval and implementation of a Strategy for Digital Health, that is clinically led and supports staff in care delivery ↔ 016 Management of asbestos 012 Failure to deliver major and discretionary capital programmes ↔ 006 Discharge delays from acute hospitals ↔ 013 South Wales Plan outcomes ↔ 023 Deterioration in the timescale relating to issuing concerns (complaints) responses to patients and or carers
032 Sustainability of safe & effective Ophthalmology Services
005 Failure to sustain services as currently configured to meet cancer targets
033 Sustaining CAMH Services ↔
029 Failure to sustain Primary Care Services, particularly in Rhondda ↔
036 Primary Care workforce – recruitment & sustainability ↔
038 inconsistent approach and arrangements in place for the management and monitoring of patients requiring anticoagulation management within CTUHB ↔
025 Failure to meet Fire Safety standards across the UHB ↔ 015 Reputational damage & potential legal challenge (FNC) 030 Continuing to provide GP Out of Hours Services as currently configured 021 Staff competency – compliance with statutory/mandatory training 041 Human Tissue Act compliance mortuary / deceased services
028 Producing Viable balanced 3 year IMTP
034 Increasing dependency on agency staffing (medical & nursing) finance impact↔
035 Failure to recruit registered nursing staff ↔
008 Reduction in medical training posts within various specialities & capacity to meet workload 003 Failure to achieve 4 & 8 hour Emergency access targets.
027 Lack of control & capacity to accommodate Follow Up Outpatients 039 Ensuring Sufficient Health Records Storage
3 019 Failure to achieve the management of absence target
018 Failure to achieve statutory and mandatory planned preventative maintenance programme ↔
040 Compliance with Welsh Language Standards
2
1
C x L
1 2 3 4 5
Likelihood
Organisational Risk Register Page 14 of 17 Primary and Community Care Committee Meeting
10 October 2018
Objective: Setting the Direction & Performance & Operational Delivery
Director Lead: Director of Primary, Community and Mental Health
(DPCMH)
Assuring Committee: Primary and Community Care Committee
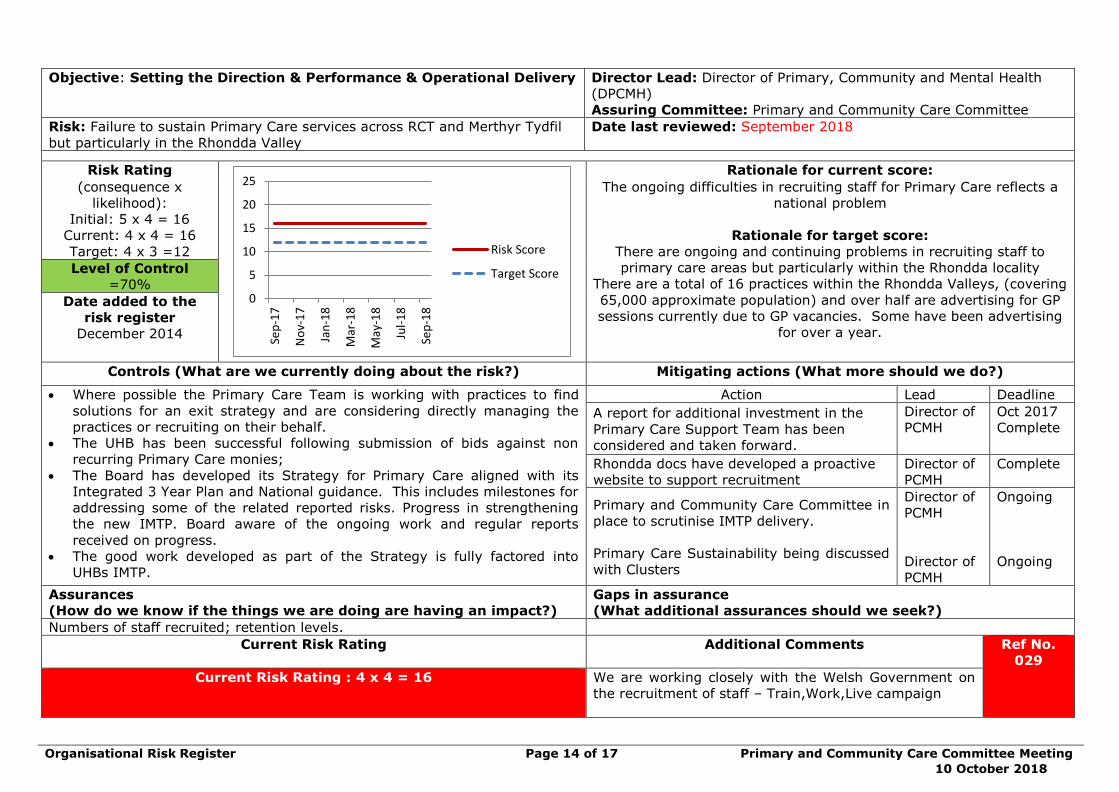
Risk: Failure to sustain Primary Care services across RCT and Merthyr Tydfil
but particularly in the Rhondda Valley
Date last reviewed: September 2018
Risk Rating
0
5
10
15
20
25
Sep
-17
No
v-1
7
Jan
-18
Mar
-18
May
-18
Jul-
18
Sep
-18
Risk Score
Target Score
Rationale for current score:
(consequence x
likelihood):
Initial: 5 x 4 = 16
Current: 4 x 4 = 16
Target: 4 x 3 =12
The ongoing difficulties in recruiting staff for Primary Care reflects a
national problem
Rationale for target score:
There are ongoing and continuing problems in recruiting staff to
primary care areas but particularly within the Rhondda locality
There are a total of 16 practices within the Rhondda Valleys, (covering
65,000 approximate population) and over half are advertising for GP
sessions currently due to GP vacancies. Some have been advertising
for over a year.
Level of Control
=70%
Date added to the
risk register
December 2014
Controls (What are we currently doing about the risk?) Mitigating actions (What more should we do?)
• Where possible the Primary Care Team is working with practices to find
solutions for an exit strategy and are considering directly managing the
practices or recruiting on their behalf.
• The UHB has been successful following submission of bids against non
recurring Primary Care monies;
• The Board has developed its Strategy for Primary Care aligned with its
Integrated 3 Year Plan and National guidance. This includes milestones for
addressing some of the related reported risks. Progress in strengthening
the new IMTP. Board aware of the ongoing work and regular reports
received on progress.
• The good work developed as part of the Strategy is fully factored into
UHBs IMTP.
Action Lead Deadline
A report for additional investment in the
Primary Care Support Team has been
considered and taken forward.
Director of
PCMH
Oct 2017
Complete
Rhondda docs have developed a proactive
website to support recruitment
Director of
PCMH
Complete
Primary and Community Care Committee in
place to scrutinise IMTP delivery.
Primary Care Sustainability being discussed
with Clusters
Director of
PCMH
Director of
PCMH
Ongoing
Ongoing
Assurances
(How do we know if the things we are doing are having an impact?)
Gaps in assurance
(What additional assurances should we seek?)
Numbers of staff recruited; retention levels.
Current Risk Rating
Additional Comments
Ref No.
029
Current Risk Rating : 4 x 4 = 16
We are working closely with the Welsh Government on
the recruitment of staff – Train,Work,Live campaign
Organisational Risk Register Page 15 of 17 Primary and Community Care Committee Meeting
10 October 2018
Objective: Setting the Direction & Performance & Operational Delivery
Director Lead: Director of Primary, Community and Mental Health
(DPCMH)
Assuring Committee: Primary and Community Care Committee
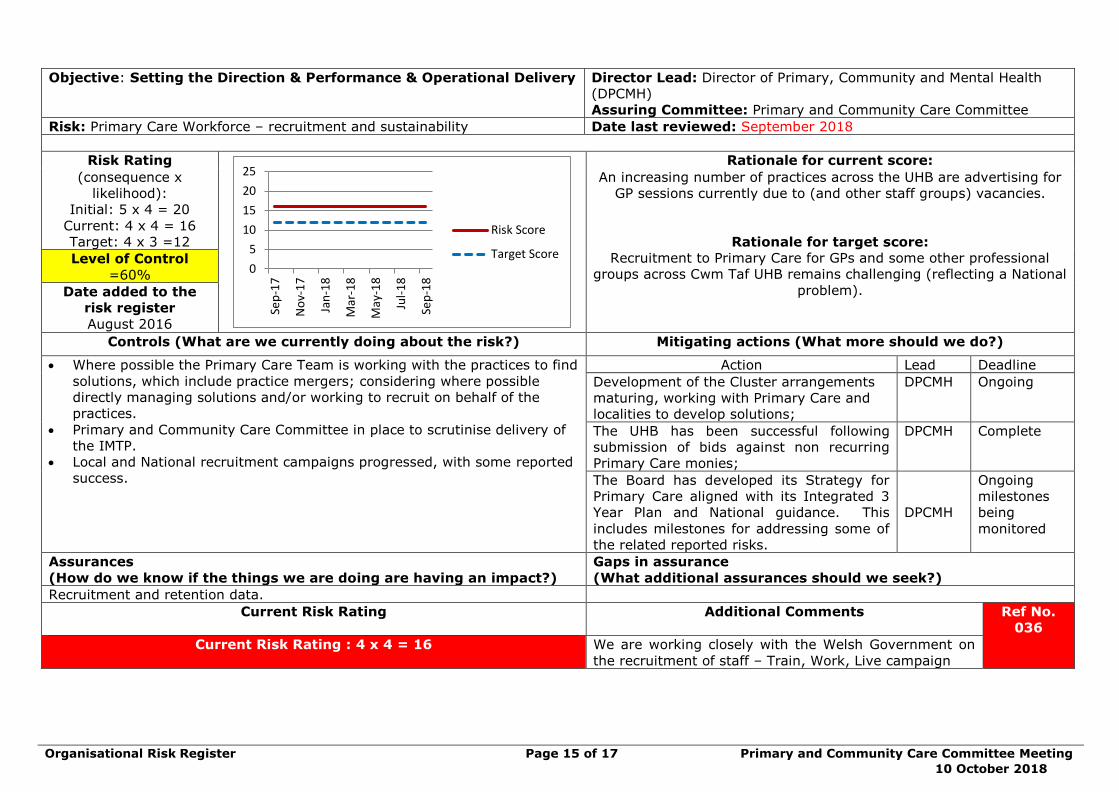
Risk: Primary Care Workforce – recruitment and sustainability Date last reviewed: September 2018
Risk Rating
0
5
10
15
20
25
Sep
-17
No
v-1
7
Jan
-18
Mar
-18
May
-18
Jul-
18
Sep
-18
Risk Score
Target Score
Rationale for current score:
(consequence x
likelihood):
Initial: 5 x 4 = 20
Current: 4 x 4 = 16
Target: 4 x 3 =12
An increasing number of practices across the UHB are advertising for
GP sessions currently due to (and other staff groups) vacancies.
Rationale for target score:
Recruitment to Primary Care for GPs and some other professional
groups across Cwm Taf UHB remains challenging (reflecting a National
problem).
Level of Control
=60%
Date added to the
risk register
August 2016
Controls (What are we currently doing about the risk?) Mitigating actions (What more should we do?)
• Where possible the Primary Care Team is working with the practices to find
solutions, which include practice mergers; considering where possible
directly managing solutions and/or working to recruit on behalf of the
practices.
• Primary and Community Care Committee in place to scrutinise delivery of
the IMTP.
• Local and National recruitment campaigns progressed, with some reported
success.
Action Lead Deadline
Development of the Cluster arrangements
maturing, working with Primary Care and
localities to develop solutions;
DPCMH Ongoing
The UHB has been successful following
submission of bids against non recurring
Primary Care monies;
DPCMH Complete
The Board has developed its Strategy for
Primary Care aligned with its Integrated 3
Year Plan and National guidance. This
includes milestones for addressing some of
the related reported risks.
DPCMH
Ongoing
milestones
being
monitored
Assurances
(How do we know if the things we are doing are having an impact?)
Gaps in assurance
(What additional assurances should we seek?)
Recruitment and retention data.
Current Risk Rating
Additional Comments
Ref No.
036
Current Risk Rating : 4 x 4 = 16
We are working closely with the Welsh Government on
the recruitment of staff – Train, Work, Live campaign
Organisational Risk Register Page 16 of 17 Primary and Community Care Committee Meeting
10 October 2018
Objective: Setting the Direction & Performance & Operational Delivery
Director Lead: Director of Primary, Community and Mental Health
(DPCMH)
Assuring Committee: Primary and Community Care Committee
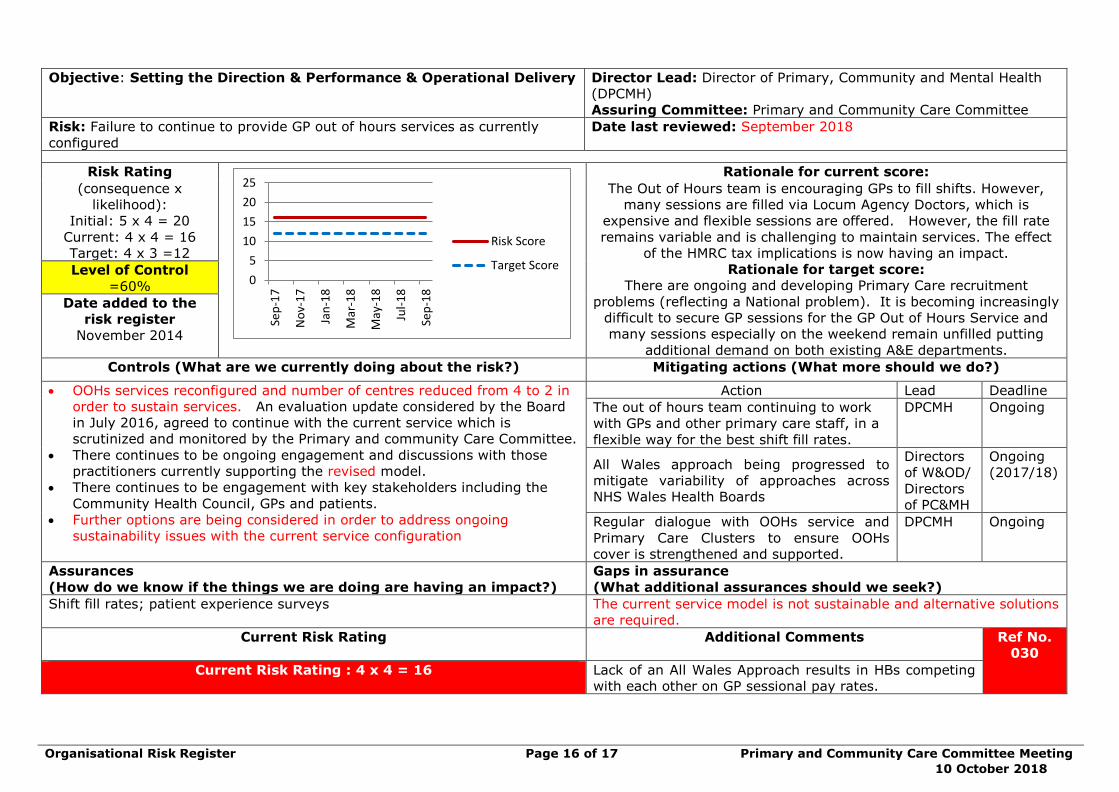
Risk: Failure to continue to provide GP out of hours services as currently
configured
Date last reviewed: September 2018
Risk Rating
0
5
10
15
20
25
Sep
-17
No
v-1
7
Jan
-18
Mar
-18
May
-18
Jul-
18
Sep
-18
Risk Score
Target Score
Rationale for current score:
(consequence x
likelihood):
Initial: 5 x 4 = 20
Current: 4 x 4 = 16
Target: 4 x 3 =12
The Out of Hours team is encouraging GPs to fill shifts. However,
many sessions are filled via Locum Agency Doctors, which is
expensive and flexible sessions are offered. However, the fill rate
remains variable and is challenging to maintain services. The effect
of the HMRC tax implications is now having an impact.
Rationale for target score:
There are ongoing and developing Primary Care recruitment
problems (reflecting a National problem). It is becoming increasingly
difficult to secure GP sessions for the GP Out of Hours Service and
many sessions especially on the weekend remain unfilled putting
additional demand on both existing A&E departments.
Level of Control
=60%
Date added to the
risk register
November 2014
Controls (What are we currently doing about the risk?) Mitigating actions (What more should we do?)
• OOHs services reconfigured and number of centres reduced from 4 to 2 in
order to sustain services. An evaluation update considered by the Board
in July 2016, agreed to continue with the current service which is
scrutinized and monitored by the Primary and community Care Committee.
• There continues to be ongoing engagement and discussions with those
practitioners currently supporting the revised model.
• There continues to be engagement with key stakeholders including the
Community Health Council, GPs and patients.
• Further options are being considered in order to address ongoing
sustainability issues with the current service configuration
Action Lead Deadline
The out of hours team continuing to work
with GPs and other primary care staff, in a
flexible way for the best shift fill rates.
DPCMH Ongoing
All Wales approach being progressed to
mitigate variability of approaches across
NHS Wales Health Boards
Directors
of W&OD/
Directors
of PC&MH
Ongoing
(2017/18)
Regular dialogue with OOHs service and
Primary Care Clusters to ensure OOHs
cover is strengthened and supported.
DPCMH Ongoing
Assurances
(How do we know if the things we are doing are having an impact?)
Gaps in assurance
(What additional assurances should we seek?)
Shift fill rates; patient experience surveys The current service model is not sustainable and alternative solutions
are required.
Current Risk Rating
Additional Comments
Ref No.
030
Current Risk Rating : 4 x 4 = 16
Lack of an All Wales Approach results in HBs competing
with each other on GP sessional pay rates.
Organisational Risk Register Page 17 of 17 Primary and Community Care Committee Meeting
10 October 2018
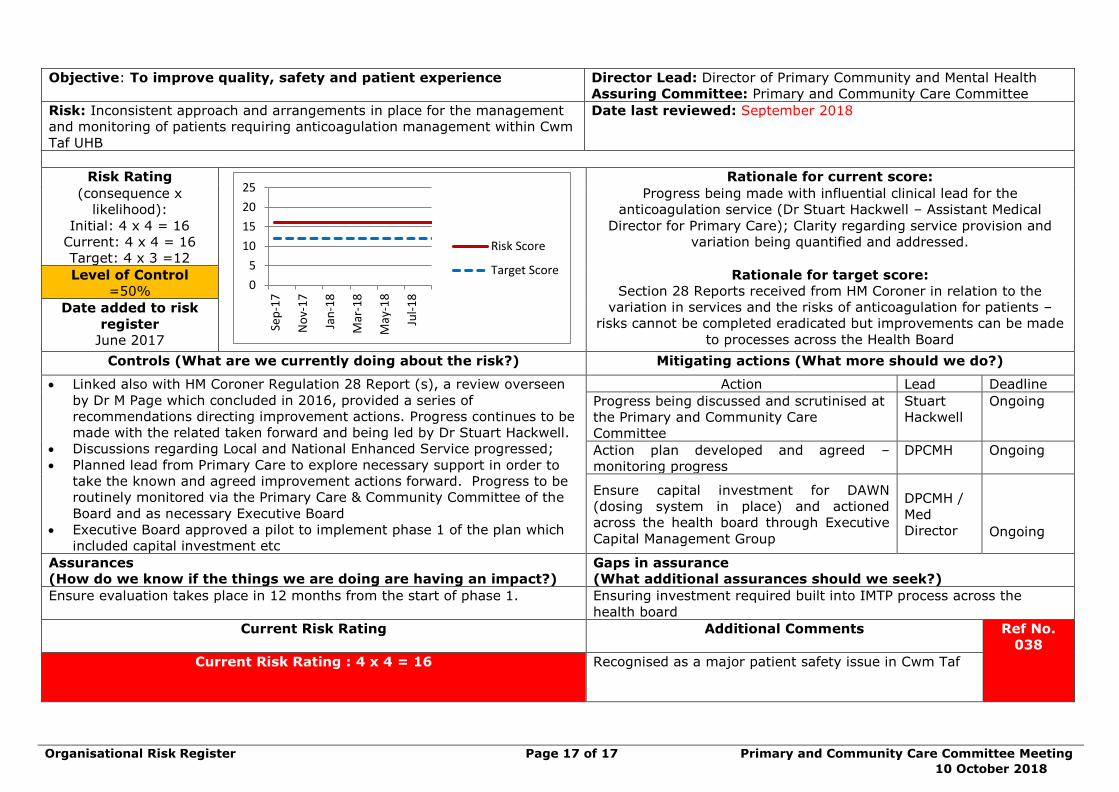
Objective: To improve quality, safety and patient experience
Director Lead: Director of Primary Community and Mental Health
Assuring Committee: Primary and Community Care Committee
Risk: Inconsistent approach and arrangements in place for the management
and monitoring of patients requiring anticoagulation management within Cwm
Taf UHB
Date last reviewed: September 2018
Risk Rating
0
5
10
15
20
25
Sep
-17
No
v-1
7
Jan
-18
Mar
-18
May
-18
Jul-
18
Risk Score
Target Score
Rationale for current score:
(consequence x
likelihood):
Initial: 4 x 4 = 16
Current: 4 x 4 = 16
Target: 4 x 3 =12
Progress being made with influential clinical lead for the
anticoagulation service (Dr Stuart Hackwell – Assistant Medical
Director for Primary Care); Clarity regarding service provision and
variation being quantified and addressed.
Level of Control
=50%
Rationale for target score:
Section 28 Reports received from HM Coroner in relation to the
variation in services and the risks of anticoagulation for patients –
risks cannot be completed eradicated but improvements can be made
to processes across the Health Board
Date added to risk
register
June 2017
Controls (What are we currently doing about the risk?) Mitigating actions (What more should we do?)
• Linked also with HM Coroner Regulation 28 Report (s), a review overseen
by Dr M Page which concluded in 2016, provided a series of
recommendations directing improvement actions. Progress continues to be
made with the related taken forward and being led by Dr Stuart Hackwell.
• Discussions regarding Local and National Enhanced Service progressed;
• Planned lead from Primary Care to explore necessary support in order to
take the known and agreed improvement actions forward. Progress to be
routinely monitored via the Primary Care & Community Committee of the
Board and as necessary Executive Board
• Executive Board approved a pilot to implement phase 1 of the plan which
included capital investment etc
Action Lead Deadline
Progress being discussed and scrutinised at
the Primary and Community Care
Committee
Stuart
Hackwell
Ongoing
Action plan developed and agreed –
monitoring progress
DPCMH Ongoing
Ensure capital investment for DAWN
(dosing system in place) and actioned
across the health board through Executive
Capital Management Group
DPCMH /
Med
Director
Ongoing
Assurances
(How do we know if the things we are doing are having an impact?)
Gaps in assurance
(What additional assurances should we seek?)
Ensure evaluation takes place in 12 months from the start of phase 1. Ensuring investment required built into IMTP process across the
health board
Current Risk Rating
Additional Comments
Ref No.
038
Current Risk Rating : 4 x 4 = 16
Recognised as a major patient safety issue in Cwm Taf

3.1 Report of the Director of Primary, Community & Mental Health
1 3.1 DPMH report PCCC 10 October 2018.doc
Report of the Director of Primary Community and Mental Health
Page 1 of 12 Primary and Community Care Committee Meeting
10 October 2018
AGENDA ITEM 3.1
10 October 2018
Primary and Community Care Committee Report
REPORT OF THE
DIRECTOR OF PRIMARY, COMMUNITY AND MENTAL HEALTH
Executive Lead: Alan Lawrie, Director of Primary, Community and Mental Health
Author: Craige Wilson, Assistant Director of Primary Care, Children and
Community Services.
Contact Details for further information: [email protected]
Purpose of the Primary and Community Care Committee Report
The aim of the report is to update the Primary and Community Care
Committee on key areas within the portfolio of the Director.
Governance
Link to Health Board Strategic
Objective(s)
The Board’s overarching role is to ensure its Strategy outlined within ‘Cwm Taf Cares’ 3 Year Integrated
Medium Term Plan 2015-2018 and the related organisational objectives aligned with the Institute of
Healthcare Improvement's (IHI) ‘Triple Aim’ are being progressed, these in summary are:
• To improve quality, safety and patient experience
• To protect and improve population health • To ensure that the services provided are
accessible and sustainable into the future • To provide strong governance and assurance
• To ensure good value based care and treatment
for our patients in line with the resources made available to the Health Board.
This report aims to support all of the above objectives.
Supporting evidence
Supporting information is provided where required throughout the report
Engagement – Who has been involved in this work?
The Primary and Community Care Team, independent contractors and
other community based staff.
Report of the Director of Primary Community and Mental Health
Page 2 of 12 Primary and Community Care Committee Meeting
10 October 2018
Primary and Community Care Committee Resolution to:
APPROVE ENDORSE DISCUSS √ NOTE √
Recommendation The Primary and Community Care Committee is
asked to: • DISCUSS and NOTE the report.
Summarise the Impact of the Primary and Community Care Committee Report
Equality and
diversity
There are no specific equality and diversity
implications identified
Legal implications There are no specific legal implications identified
Population Health The aim of the services identified within the report aim to contribute to improving the
population health
Quality, Safety &
Patient Experience
The aim of the services referred to in the report
aim to improve the quality, safety and patient experience.
Resources There are no specific resource implications
identified and the work is in line with Integrated Medium Term Plan and is reported by the
locality.
Risks and Assurance The specific risks are identified where
appropriate within the document.
Health & Care Standards
The 22 Health & Care Standards for NHS Wales are mapped into the 7 Quality Themes:
Staying Healthy Safe Care
Effective Care Dignified Care
Timely Care Individual Care
Staff & Resources
http://www.wales.nhs.uk/sitesplus/documents/1064/24729_Health%20Standards%20Framework
_2015_E1.pdf
The work reported in this summary supports
many of the health and care standards
Workforce Workforce implications are identified where
appropriate within the report
Freedom of information status
Open
Report of the Director of Primary Community and Mental Health
Page 3 of 12 Primary and Community Care Committee Meeting
10 October 2018
REPORT OF THE
DIRECTOR OF PRIMARY, COMMUNITY AND MENTAL HEALTH
1. SITUATION / PURPOSE OF REPORT
This report provide a series of updates for the Committee to assure progress
against key areas and to provide high level information for a range of services. More detailed reports individual reports on topic areas can be provided as
required.
2. BACKGROUND / INTRODUCTION
This reports gives an overview of the following areas:
• Community Dental Services Transfer from Cardiff
• The Cwm Taf Transformation Plan
• Eye Care plan update by exception • Oral Health Report update by exception
• GP Sustainability • Primary Care Measures
• Wales Audit Office – Primary Care Services (Cwm Taf UHB).
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
3.1 Community Dental Services Transfer from Cardiff
Following a detail review of the Community Dental Service delivered to the
Cwm Taf population by Cardiff & Vale UHB, a decision was taken to repatriate the service back to Cwm Taf with effect from April 2019.
A project structure has been established including staff from the Primary Care
Directorate, Finance, Human Resources and Clinical Systems. It is designed to ensure clear lines of responsibility at both strategic and operational level.
The overarching Steering Group was established in March 2018 and there are
four Task and Finish Groups, arranged to correspond with the work streams. In
addition a Project Manager commenced in June 2018, on a two year fixed term basis.
A general meeting with the Community Dental Staff (CDS) staff based in Cwm
Taf who will transfer as part of the arrangements was held on 12 September 2018. Staff were given the opportunity to ask any general questions regarding
the transfer and following this a frequently asked question (FAQ) document is being produced and will be made available to the staff. The general response
from staff to date with regards to the transfer of the service has been positive.
Report of the Director of Primary Community and Mental Health
Page 4 of 12 Primary and Community Care Committee Meeting
10 October 2018
A key risk has been identified within the Finance and Commissioning Task and
Finish Group. Following escalation to the Director of Finance at Cardiff and Vale UHB, there has been traction and improvement over the past two weeks. This
position will be monitored closely.
It has been noted that additional discretionary capital funding may be required
for equipment and / or vehicles. It is anticipated that the Steering Group will have an indication of any such costs following the next meeting to be held on
25 October 2018.
An alternative storage facility for ‘Designed for Smile’ may need to be identified within Cwm Taf. The Project Manager will undertake an assessment of this
requirement and the potential options and report back to the next Steering Group meeting.
The next steps are as follows:
• Following the receipt of the financial information for Cardiff and Vale, the cost of the staff proposed to transfer to Cwm Taf can be calculated
together with the other revenue requirements for the service. • Confirmation is required on the transfer of all equipment and vehicles to
Cwm Taf at no cost.
• Costs are required for the provision of an Service Level Agreement (SLA) for the maintenance of the Information Communication and Technology
(ICT) system • Confirmation is required on the ability of clinical engineering to support the
maintenance of dental equipment or the cost of this being provided externally.
• A management structure, including clinical lead, for the new service will be determined by the end of September 2018; this will also need to include
the service currently provided by ABMU in Bridgend. This will allow time for key appointments to be made to manage the service prior to April 2019.
• Group and one to one meetings, where necessary, to commence with staff in October 2018.
3.2 Update on Cwm Taf Transformation Plan
Alignment with ‘A Healthier Wales: Our Plan for Health and Social Care’
Cwm Taf University Health Board (UHB), Merthyr Tydfil (MT) County Borough Council and Rhondda Cynon Taf (RCT) County Borough Council were approved
‘Full Flexibility’ pathfinders, and as such a partnership transformation programme (proposal) has been developed and signed off by the Regional
Partnership Board. This programme is predicated on developing and delivering seamless services which are provided closer to home and transform outcomes
for individuals and communities.

Report of the Director of Primary Community and Mental Health
Page 5 of 12 Primary and Community Care Committee Meeting
10 October 2018
Our partnership track record of delivery has enabled us to be bold in developing
an ambitious long term model which, aligned to ‘A Healthier Wales: Our Plan for Health and Social Care’. It targets the necessary urgent change required to
deliver a whole system approach to the provision of health and social care
across Cwm Taf as outlined in Figure 1.
Figure 1
Applying the design principles of ‘A Healthier Wales: Our Plan for Health and
Social Care’ has led us as partners to the service strategy in Figure 2:
Figure 2
Prioritising our health and social care core funding differently, alongside non-
recurrent funding sources such as: the Primary Care Pacesetter Fund, Integrated Care Fund, Primary Care Delivery Plan funding, Mental Health
Transformation funding and others, has supported the piloting and evaluation1 of innovative service models such as: Inverse Care (CVD) Health Check, Cluster
led Virtual Ward, the integrated and award winning Stay Well@Home service.

Report of the Director of Primary Community and Mental Health
Page 6 of 12 Primary and Community Care Committee Meeting
10 October 2018
This evidence base of positive system change has lead the partnership to the
next phase of the transformation journey; scaling up and further integrating our out of hospital health and social care. Based on the whole system, Cwm Taf
Population Health and Social Care Service Model, above at figure 2, the
priorities for an initial tranche of Transformation Funding are for the following complementary components:
Integrated Community Care, Closer to Home
Multidisciplinary Anticipatory Care and Enhanced Routine Monitoring Services • Systematise practice, cluster and Health Board level, population health
segmentation and risk stratification. This segmentation will target the intervention of assistive technology, disease specific community teams and
the multi-agency Enhanced Community Cluster Team. • The further development, of a proactive outward facing assistive
technology model through utilisation of appropriate assessment, proactive calling, equipment and rapid response service, enabling people to maintain
their independence at home. • Scale up and further develop anticipatory support and care models, e.g.,
virtual ward and neighbourhood nursing. Cluster level, multi-agency, multi-professional Enhanced Community Cluster Teams.
Rapid Response Services
• To complement the 111 service, transform GP Out of Hours, into an Urgent Primary Care Out of Hours Service including the adoption of a prudent
workforce model and the development of a Machine Learning / Artificial Intelligence driven symptom checker application to reduce in and out of
hours demand on General Practice. • Roll out the next phase of the Integrated Stay Well@Home rapid
response service across Cwm Taf, to enable referral, via a single point of access, from community based health, wellbeing, pre-hospital and social
care professionals maintaining people for longer in their own homes.
Building on the knowledge of our transformation work to date it is likely that we would be able to demonstrate the following measurable benefits:
• The shift of interventions from clinical environments to an individual’s home environment where ever that may be
• Improved access to primary care services, i.e. reduced waiting times and patient satisfaction
• Increase in the number of people with an anticipatory care plan • Improved patient outcomes, experience and safety (based on defined clinical
need)
• A reduction in acute outpatient appointments • A reduction in medicines management costs
• A reduction in the demand for urgent primary care out of hours services • An increase in the range of community based services accessible out of
hours • A reduction in hospital conveyances by ambulance and admissions with a
reduced length of stay when someone needs acute care • Reduction on the reliance on acute care beds – reduction in Length of Stay /
Increase in time spent at home

Report of the Director of Primary Community and Mental Health
Page 7 of 12 Primary and Community Care Committee Meeting
10 October 2018
Overview of Multidisciplinary Anticipatory Care & Support and Enhanced Routine Monitoring Services
Objective(s)
• Population health segmentation, risk stratification and case mix analysis by practice, Cluster and Health Board
• Active engagement with Primary Care and wider multidisciplinary team to act on case-mix adjusted analysis by practice and Cluster
• Build on maturing Clusters by establishing an Enhanced Community Resource Team delivering multidisciplinary
anticipatory care and support at a cluster level across Cwm Taf, with the GP at the centre as an Expert Medical Generalist.
• Further develop the evidence base and test the assistive
technology model to support people to maintain their independence at home, underpinning the primary care
stratification and response. • Develop advanced training opportunities for multi-professionals
and multiagency staff within Primary, Community and social care settings.
Pace and Scalability
Aiming for implementation in early October across the existing Cwm Taf footprint. The pace of delivery will vary depending on the needs
and maturity of the locality and clusters. It is an evolving plan and
flexibility will be required.
Planned spend
2018-19 £k 2019-20 £k 2020-21 £k
£3,991 £8,652 £8,429
Overview of Rapid Response Services
Objective(s)
• To deliver a robust and responsive urgent care Out of Hours
service which will triage, advice, signpost, assess, see and treat patients in a timely manner meeting All Wales Standards.
• Integrated Stay Well@Home rapid response service, to enable referral, via a single point of access, from community based
health, pre hospital, wellbeing and social care professionals. • Avoid unnecessary conveyance/ attendance to hospital and
provide support to people to remain in their own homes – 12hrs, 7 days a week, 52 weeks a year (further evaluation will target the
12hrs to the correct window) • Provision of a range of temporary accommodation to avoid
admission. • Prevent the impact of long stay hospital admissions on people’s
self-care abilities.
Pace and Scalability
Aiming for implementation in early October across the existing Cwm Taf footprint. Recruitment and training will determine the detail of
the implementation, with the expectation that this services can only be delivered pan Cwm Taf.
Planned
spend
2018-19 £k 2019-20 £k 2020-21 £k
£1,350 £2,715 £2,715
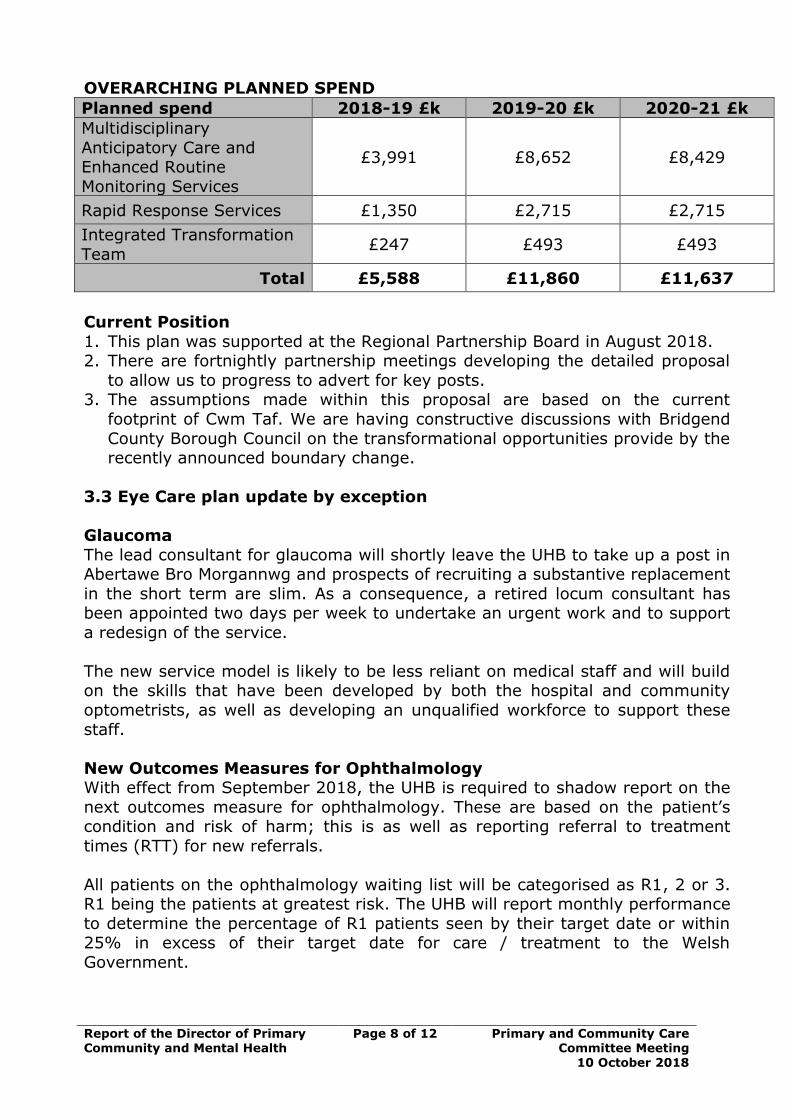
Report of the Director of Primary Community and Mental Health
Page 8 of 12 Primary and Community Care Committee Meeting
10 October 2018
OVERARCHING PLANNED SPEND
Planned spend 2018-19 £k 2019-20 £k 2020-21 £k
Multidisciplinary
Anticipatory Care and Enhanced Routine
Monitoring Services
£3,991 £8,652 £8,429
Rapid Response Services £1,350 £2,715 £2,715
Integrated Transformation
Team £247 £493 £493
Total £5,588 £11,860 £11,637
Current Position
1. This plan was supported at the Regional Partnership Board in August 2018. 2. There are fortnightly partnership meetings developing the detailed proposal
to allow us to progress to advert for key posts. 3. The assumptions made within this proposal are based on the current
footprint of Cwm Taf. We are having constructive discussions with Bridgend
County Borough Council on the transformational opportunities provide by the recently announced boundary change.
3.3 Eye Care plan update by exception
Glaucoma
The lead consultant for glaucoma will shortly leave the UHB to take up a post in Abertawe Bro Morgannwg and prospects of recruiting a substantive replacement
in the short term are slim. As a consequence, a retired locum consultant has been appointed two days per week to undertake an urgent work and to support
a redesign of the service.
The new service model is likely to be less reliant on medical staff and will build on the skills that have been developed by both the hospital and community
optometrists, as well as developing an unqualified workforce to support these
staff.
New Outcomes Measures for Ophthalmology With effect from September 2018, the UHB is required to shadow report on the
next outcomes measure for ophthalmology. These are based on the patient’s condition and risk of harm; this is as well as reporting referral to treatment
times (RTT) for new referrals.
All patients on the ophthalmology waiting list will be categorised as R1, 2 or 3. R1 being the patients at greatest risk. The UHB will report monthly performance
to determine the percentage of R1 patients seen by their target date or within 25% in excess of their target date for care / treatment to the Welsh
Government.
Report of the Director of Primary Community and Mental Health
Page 9 of 12 Primary and Community Care Committee Meeting
10 October 2018
The Cabinet Secretary has announced additional investment of up to £4m
between now and the end of March 2020 to support health boards in the creation of sustainable services in support of the introduction of the new
measures. The eye care sustainability fund is non-recurrent and is available to
all NHS organisations to use between November 2018 and March 2020 to develop and implement processes which will support the implementation of the
new measure, sustainable services alongside the achievement of RTT for eye care patients. 3.4 Oral Health Report update by exception
Dental Contract Reform
Committee members will be aware that the UHB currently has three dental practices who have been part of Phase 1 of the Dental Contract Reform
programme since September 2017. Welsh Government has set each Health Board a target of having 10% of their dental practices part of the scheme from
October 2018. The UHB has received two expression of interest from practices in Taff Ely and the Dental Teaching Unit in Porth will also become a Dental
Contract Reform Practice. There are 35 dental practices in Cwm Taf and therefore the UHB will exceed the target with at least 5 practices in the scheme.
The UHB is currently reluctant to approve more dental practices as reducing contracted units of dental activity (UDAs) by 10% also reduces the amount of
patient charge revenue (PCR) the UHB receives; the dental allocation is given to Health Boards net of PCR and any shortfall in income has an impact on the
UHB’s financial position. However, additional funding (£45,000) has been agreed by Welsh Government should Health Boards approve a minimum of 10%
of dental practices.
Baby Teeth DO Matter The Health Board introduced the initiative Baby Teeth DO Matter in April 2017
because the latest epidemiology survey showed the levels of dental caries in Cwm Taf children under 5 years of age are the highest in Wales. An evaluation
of the first year of the scheme has now been undertaken and shows significant increases in the number of children accessing dental practices in Cwm Taf. The
report is detailed in full at Agenda item 2.1.
3.5 GP Sustainability
Two directly managed practices, Brookside Surgery in Troedyrhiw and Hillcrest Surgery in Mountain Ash (with a population of 3,000 and 1,730 respectively)
transferred back to independent status with effect from the 1st October. This leaves the Health Board with two directly managed practices. These are New
Tynewydd Surgery and Ferndale & Maerdy Medical Practice in the Rhondda with a combined patient list of 13,423.
The Primary Care team are also working with practices where there are single
handed GPs and discussing retirement and succession plans where appropriate.
Report of the Director of Primary Community and Mental Health
Page 10 of 12 Primary and Community Care Committee Meeting
10 October 2018
No new sustainability applications have been submitted but the Head of Primary
Care and the Assistant Medical Director (Primary Care) are working with two practices around clinical performance. Contingency plans are in place to deal
with possible outcomes following the Health Boards interventions and are in line
with strategic priorities.
3.6 Primary Care Measure The Directors of Primary and Community Care have commissioned the Primary
and Community Care Development and Innovation Hub to produce a National Primary Care Measures report by December 2018. This report will be a
comparative report and will show examples of good practice under each of the measures. In addition to this, the Directors have produced a high level key 5-6
indicators for Primary Care which are aligned to the recommendations within the Parliamentary Review of Health and Social Care. The information will be
collated from Health Boards and will be available via the NWIS Primary Care Portal.
3.7 Wales Audit Office Report
The UHB has recently received a report from the Wales Audit Office in relation to the provision of Primary Care Services. The key findings were that “the
Health Board has a sound plan for primary care and is making reasonable
progress towards implementing key elements of the national vision. Oversight arrangements are strong and performance against some indicators is above
average. However, there is further scope to raise the profile of primary care, shift more resources towards primary care and to address workforce
challenges.”
The report outlined as follows:
The Health Board has a strong primary care plan aligned to national priorities and whilst clusters are at an early stage of development, the Health Board is
taking steps to support their ongoing development. • The Health Board has a strong primary care plan aligned to national
priorities and it engages with a range of stakeholders in developing its plans. • Most clusters remain at a relatively early stage of maturity but cluster
development will be further supported through the Health Board’s new
strategic planning group. We found scope to strengthen cluster leadership, membership and to improve the evaluation of cluster projects.
Investment: The Health Board has some examples of resources shifting to
primary care but there are barriers to large-scale change and the available data make it difficult to accurately calculate the overall investment in primary care.
Workforce: Workforce challenges are threatening the sustainability of some
practices but the Health Board has begun workforce modelling and is in the early stages of testing solutions.
Report of the Director of Primary Community and Mental Health
Page 11 of 12 Primary and Community Care Committee Meeting
10 October 2018
Oversight and leadership: Strong leadership and monitoring arrangements
are in place and the Health Board is taking steps to improve primary care data; however, there is further scope to raise the profile of primary care.
Performance and monitoring: The Health Board is making reasonable progress in delivering its primary care and localities plan and some aspects of
performance are better than the Wales average, although a number of difficult challenges remain
The main recommendations were as follows:
Strategic planning:
• The Health Board commissioned the Primary Care Foundation to carry out demand and capacity assessments in GP practices but the take up from
practices has been variable. To maximise value from the commissioned work, the Health Board should centrally analyse and collate the messages
from the demand and capacity assessments and share the learning across all practices.
Investment in primary care
• While the Health Board recognises that it needs to shift resources from
secondary to primary and community settings, it cannot demonstrate that this shift is happening. The Health Board should:
a. Calculate a baseline position for its current investment and resource use in primary and community care.
b. Review and report, at least annually, its investment in primary and community care, to assess progress since the baseline position and
to monitor the extent to which it is succeeding in shifting resources towards primary and community care.
The primary care workforce
• The Health Board’s workforce planning is inhibited by having limited data about the number and skills of staff working in primary care, particularly
community dentistry, optometry and pharmacy. The Health Board should develop and implement an action plan for ensuring it has regular,
comprehensive, standardised information on the number and skills of staff,
from all professions working in all primary care settings.
New ways of working • Whilst the Health Board is taking steps towards implementing some new
ways of working, more progress is required to evaluate the effectiveness of these new models and to mainstream their funding. The Health Board
should: a. Work with the clusters to agree a specific framework for evaluating
new ways of working, to provide evidence of beneficial outcomes and inform decisions on whether to expand these models.
b. Centrally collate evaluations of new ways of working and share the learning by publicising the key messages across all clusters.
Report of the Director of Primary Community and Mental Health
Page 12 of 12 Primary and Community Care Committee Meeting
10 October 2018
c. Subject to positive evaluation, begin to fund these new models from
mainstream funding, rather than from the Primary Care Development Fund.
d. Work with the public to promote successful new ways of working,
particularly new alternative first points of contact in primary care that have the potential to reduce demand for GP appointments.
e. Evaluate the effectiveness of the Health Board’s new primary care communications officer role and share the learning with all health
boards in Wales.
Primary care clusters • We found variation in the maturity of primary care clusters, and scope to
improve cluster membership and leadership. The Health Board should: a. Review the relative maturity of clusters, to develop and implement
a plan to strengthen its support for clusters where necessary. b. Review the membership of clusters and attendance at cluster
meetings to assess whether there is a need to increase representation from local authorities, third sector, lay
representatives and other stakeholder groups. c. Ensure all cluster leads attend the Confident Primary Care Leaders
course.
The Primary Care Team have prepared a response to correct any matters of
factual accuracy and have prepared a management response to the recommendations; many of which have been or are being address currently.
The report and the management response will be shared at the next meeting and the progress will be monitored by the Committee to report to the Audit
Committee.
4. RECOMMENDATION
Members of the Primary and Community Care Committee are asked to:
• DISCUSS and NOTE the report
Freedom of information status
Open
3.2 Primary & Community Care Internal Audit Report
1 3.2 IA Report Governance Arrangements - Primary and Community Care Committee PCCC 10 Oct 2018.pdf
Governance arrangements - Primary & Community Care Committee
Internal Audit Report
2018/19
August 2018
NHS Wales Shared Services Partnership
Audit and Assurance Services
Governance arrangements - Primary & Community Care
Committee
Contents
NHS Wales Audit & Assurance Services Page 2 of 18
Contents Page
1. Introduction and Background 4
2. Scope and Objectives 4
3. Associated Risks 6
Opinion and key findings
4. Overall Assurance Opinion 6
5. Assurance Summary 7
6. Summary of Audit Findings 8
7. Summary of Recommendations 11
Review reference: CTU-1819-05
Report status: Draft Internal Audit Report
Fieldwork completion: 23 July 2018
Draft report issued: 31 July 2018 & 13 August 2018
Management response
received:
14 August 2018
Final report issued: 20 August 2018
Auditors: Emma Samways, Deputy Head of Internal
Audit
Kimberley Rowe, Principal Internal Auditor
Executive sign off: Robert Williams, Director of Corporate
Services and Governance/ Board Secretary
Distribution: Gwenan Roberts, Head of Corporate Services
Alan Lawrie, Interim Director of Primary,
Community and Mental Health
Committee: Audit Committee
Appendix A
Appendix B
Management Action Plan
Assurance opinion and action plan risk rating
Governance arrangements - Primary & Community Care
Committee
Contents
NHS Wales Audit & Assurance Services Page 3 of 18
ACKNOWLEDGEMENT
NHS Wales Audit & Assurance Services would like to acknowledge the time and co-operation
given by management and staff during the course of this review.
Disclaimer notice - Please note:
This audit report has been prepared for internal use only. Audit & Assurance Services reports
are prepared, in accordance with the Internal Audit Charter and the Annual Plan, approved by
the Audit Committee.
Audit reports are prepared by the staff of the NHS Wales Shared Services Partnership – Audit
and Assurance Services, and addressed to Independent Members or officers including those
designated as Accountable Officer. They are prepared for the sole use of Cwm Taf University
Health Board and no responsibility is taken by the Audit and Assurance Services Internal Auditors
to any director or officer in their individual capacity, or to any third party.

Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 4 of 18
1. Introduction and Background
In line with the 2018/19 Internal Audit Plan for Cwm Taf University Health
Board (the 'Health Board'), a review of the Health Board's governance arrangements of Board committees has been carried out. This review
focussed on the Primary & Community Care Committee (the ‘Committee’).
The Board functions as the corporate decision making body of the Health
Board, with Executive Directors and Independent Members sharing corporate responsibility for all decisions. The Board can formally approve
the delegation of specific executive powers to be exercised by committees, sub-committees, joint-committees or joint sub-committees that it has
formally constituted. The committee structure adopted by the Health Board should be determined on what best meets its own needs, taking account of
any regulatory, or Welsh Government, requirements.
The Health Board has chosen to constitute the following committees:
Academic Partnership Board
Audit Committee*
Charitable Funds Committee*
Finance, Performance & Workforce Committee
Integrated Governance Committee
Mental Health Act Monitoring Committee*
Primary & Community Care Committee
Quality, Safety & Risk Committee*
Remuneration & Terms of Service Committee*
*indicates the committee is required by Welsh Government.
There has been recent change within the Health Board at Board level with
four new Independent Members taking up post in the last year and a further two posts to be filled. In the same time, there has been some change within
the Executive Director cohort, with a new interim Director of Primary Community and Mental Health joining the team, while the previous Director
of Primary, Community and Mental Health has become the Interim Chief
Operating Officer (due to secondment of the previous post holder).
This review sought to provide assurance that committee structures and
their membership are being managed and operating as intended.
The relevant lead for the review is the Director of Corporate Services and
Governance/ Board Secretary.
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 5 of 18
2. Scope and Objectives
The overall objective of this audit was to evaluate and determine the adequacy of the systems and controls in place in relation to the Health
Board's governance arrangements of the Primary & Community Care Committee. The review sought to provide assurance to the Health Board's
Audit Committee that risks material the system's objectives are managed appropriately. The areas that the review sought to provide assurance on
are:
The terms of reference for the committee is up to date and documents the roles and responsibilities of the group, the Committee Chair and
other committee members.
Committee memberships appropriate in terms of size, skill mix, length
of tenure and attendance.
Meetings are scheduled at appropriate intervals throughout the year and
the agendas and forward work plans are in line with the terms of
reference of the Committee, with no gaps in coverage.
There is a clear information flow between the Board and the committee. Actions transferred to the Committee form other committees are
appropriately captured.
Risks owned by the Committee are appropriately considered and
monitored.
Consideration is given to commitments made in the IMTP that relate to
the work of the Committee.
Reports to the Committee are timely, clearly written, and the level of detail provided to members within reports is sufficient to allow members
to discharge their duties yet without being burdensome. There is clear purpose for presenting a particular report. For example, 'to note' or 'to
consider and approve'.
Decisions made are clearly recorded within minutes and an action where
appropriate.
Mechanisms are in place for reviewing the effectiveness of the
committee and its members on a periodic basis.
The Committee’s chair appropriately summarises and reports the
outcome and resolutions of meetings for the Board to clearly understand
the assurance obtained by the Committee.
There is an induction process for new members and continuing support
and development for those members on the Committee.
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 6 of 18
3. Associated Risks
The potential risks considered in the review were as follows:
Governance arrangements not properly discharged.
Ineffective decision making as a result of poor training and support.
Non-compliance with legislative requirements for Board committees as
set out in the Health Board's standing orders.
Inappropriate/ inaccurate decisions made where too little or too much
information is provided.
Lack of transparency in decisions made.
OPINION AND KEY FINDINGS
4. Overall Assurance Opinion
We are required to provide an opinion as to the adequacy and effectiveness
of the system of internal control under review. The opinion is based on the work performed as set out in the scope and objectives within this report.
An overall assurance rating is provided describing the effectiveness of the system of internal control in place to manage the identified risks associated
with the objectives covered in this review.
The level of assurance given as to the effectiveness of the system of internal control in place to manage the risks associated with the Governance
arrangements for the Primary & Community Care Committee is
Substantial assurance.
RATING INDICATOR DEFINITION
Substantial
Assurance
The Board can take substantial assurance that arrangements to
secure governance, risk management and internal control, within those areas
under review, are suitably designed and applied effectively. Few matters
require attention and are compliance or advisory in nature with low impact
on residual risk exposure.
Our audit fieldwork included: discussions with the Chair of the Committee; a review of key documentation, including the Terms of Reference and
Annual Report of the Committee; scrutiny of the agendas, minutes and other papers of the Committee; and an analysis of the interaction with the
Board and other relevant committees.
Overall, the Committee was found to be well managed which has enabled
its duties to be discharged as intended, appropriate issues discussed, and
relevant risks captured.

Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 7 of 18
The overall level of assurance that can be assigned to a review is dependent
on the severity of the findings as applied against the specific review
objectives and should therefore be considered in that context.
5. Assurance Summary
The summary of assurance given against the individual objectives is
described in the table below:
Assurance Summary
1 Terms of Reference
2 Committee
membership
3
Meeting frequency
and forward work
plans
4 Information flow
5 Risk consideration
and monitoring
6 IMTP
7 Reports to the
Committee
8 Minutes and actions
9
Effectiveness of
Committee and
members
10 Board reports
11
New members
induction and
development
* The above ratings are not necessarily given equal weighting when generating the audit
opinion.
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 8 of 18
Design of Systems/Controls
The findings from the review have highlighted one issue that is classified as a weakness in the system control/design for the governance
arrangements of the Primary & Community Care Committee.
Operation of System/Controls
The findings from the review have highlighted three issues that are classified as weaknesses in the operation of the designed system/control
for the governance arrangements of the Primary & Community Care
Committee.
6. Summary of Audit Findings
In this section, we highlight areas of good practice that we identified during our review. We also summarise the findings made during our audit
fieldwork. The detailed findings are reported in the Management Action Plan
(Appendix A).
Objective 1: The terms of reference for the committee is up to date and documents the roles and responsibilities of the group,
committee chair and other committee members.
We note the following area of good practice:
The Terms of Reference are updated annually as required by the Health
Board's Standing Orders.
We identified the following finding under this objective:
There are minor duplication errors within the Terms of Reference.
Objective 2: Committee membership is appropriate in terms of size, skill mix, length of tenure and attendance.
We note the following areas of good practice:
The Committee was found to be of adequate size, with additional
attendees to provide detailed analysis, expertise and support as
required.
The Independent Members have a varied skill mix and relevant experience to enable them to execute their role. We also note that they
contributed widely to the meetings.
We identified the following finding under this objective:
The Terms of Reference requires greater clarity in relation to
membership.
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 9 of 18
Objective 3: Meetings are scheduled at appropriate intervals
throughout the year and the agendas and forward work plans are
in line with the terms of reference of the committee, with no gaps
in coverage.
We note the following areas of good practice:
Meetings of the Committee were scheduled at regular intervals, and in
accordance with the Terms of Reference.
The Committee has a standard agenda template that covers all aspects
of responsibilities set out within the Terms of Reference and has built in
flexibility to ensure ad hoc reports can be tabled.
The ‘Forward Look’ plan of the committee is reviewed at each meeting to ensure that it is still targeted at the appropriate risk areas. An action
log captures all agreed actions.
We did not identify any findings under this objective.
Objective 4: There is clear information flow between the Board and the committee. Actions transferred to the committee from other
committees are appropriately transferred.
We note the following area of good practice:
We read a sample of Board minutes in conjunction with Committee
papers. While no formal actions to be referred from the Board to the Committee were identified, we note that key issues that related to
Primary Care, and raised in Board meetings, also formed discussions in
Committee meetings, therefore, appropriately transferring information.
We did not identify any findings under this objective.
Objective 5: Risks owned by the committee are appropriately
considered and monitored.
We note the following area of good practice:
The organisational risk register is a standard agenda item for the Committee. Our review of minutes confirmed that the four risks
delegated to the Committee were considered at each meeting.
We did not identify any findings under this objective.
Objective 6: Consideration is given to commitments made in the
IMTP that relate to the work of the committee.
We note the following area of good practice:
Our review of the agenda and minutes of the committee confirmed that the Primary & Community Delivery Plan, which is a key element of the
IMTP, features at each Committee meeting.
We did not identify any findings under this objective.
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 10 of 18
Objective 7: Reports to the committee are timely, clearly written,
and the levels of detail provided to members within reports is
sufficient to allow members to discharge their duties yet without being burdensome. There is a clear purpose for presenting a
particular report, for example, 'to note' or 'to consider and
approve'.
We note the following area of good practice:
Of the four reports to the Committee that we sampled, three were found
to be in a consistent format, presented to the Committee with a clear purpose and contained sufficient detail for members to discharge their
duties. The fourth report had originally been prepared for another committee and had been referred onto the Primary & Community Care
Committee.
We identified the following finding under this objective:
For a small number of the reports sampled, there was a time delay in
the Committee receiving the report.
Objective 8: Decisions made are clearly recorded within minutes
and an action where appropriate.
We note the following area of good practice:
The minutes of the Committee meetings were clear and all decisions made by the Committee are summarised for each agenda reference,
including actions to be tabled and included in the action log.
We did not identify any findings under this objective.
Objective 9: Mechanisms are in place for reviewing the
effectiveness of the committee and its members on a periodic basis.
We note the following area of good practice:
The Committee has complied with the requirement to prepare an annual
report setting out its activities during the year and detailing the results of a review of its performance. Included in this is a review of the
Committee’s effectiveness.
We did not identify any findings under this objective.
Objective 10: The committee's chair appropriately summarises and
reports the outcome and resolutions of meetings for the Board to
clearly understand the assurance obtained by the committee.
We note the following area of good practice:
The Committee provides the latest confirmed minutes and a summary
of discussions and activities of the Committee as part of the Committee
Chair's Report to the Executive Board each meeting.
We did not identify any findings under this objective.
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
NHS Wales Audit & Assurance Services Page 11 of 18
Objective 11: There is an induction process for new members and
continuing support and development for those members on the
committee.
We identified the following finding:
There is no documentation on training and development included in the
Terms of Reference, which is a requirement of the Standing Orders.
7. Summary of Recommendations
The audit findings and recommendations are detailed in Appendix A
together with the management action plan and implementation timetable.
A summary of these recommendations by priority is outlined below.
Priority H M L Total
Number of
recommendations 0 0 4 4
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 12 of 18
Finding 1 - Induction and training (Operating effectiveness) Risk
The Health Board’s Standing Orders provide a list of the minimum requirements for each committee’s Terms of Reference, which includes training, development
and performance.
However, there is no reference to training and development included in the
Committee’s Terms of Reference. We acknowledge that the Terms of Reference
for another committee that we read, also did not make reference to training and
development.
Ineffective decision making as a result of poor training and support.
Recommendation Priority level
The Committee should ensure that training and development requirements are
documented in the Terms of Reference to satisfy the requirements of the Health
Board’s Standing Orders.
Low
Management Response Responsible Officer/ Deadline
Following discussion with the Committee Chair, the Terms of Reference will be
amended in line with Standing Orders.
Gwenan Roberts
Next meeting – October 2018
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 13 of 18
Finding 2 - Membership and quoracy (Operating effectiveness) Risk
The Committee’s Terms of Reference lists the Executive Directors as 'in
attendance' and does not specify if this requirement is mandatory.
For the meeting to be quorate two Independent Members must be present,
however, the Terms of Reference does not indicate whether this is inclusive of the Committee Chair, who is also an Independent Member. Other committee
Terms of Reference make this distinction.
For the last three meetings that we tested, they are deemed quorate if the
membership is inclusive of the Chair.
Governance arrangements not
properly discharged.
Non-compliance with legislative requirements for Board committees
as set out in the Health Board's standing orders
Recommendation Priority level
The Primary & Community Care Committee should clarify in their Terms of
Reference the required Members to be present at each meeting. Low
Management Response Responsible Officer/ Deadline
Following discussion with the Committee Chair, the Terms of Reference will be
amended in line with Standing Orders and will include specifically the requirement for executive directors to be present. The TOR will also be amended
to clarify that the Chair is included in the number of Independent Members at
the meeting.
Gwenan Roberts
Next meeting – October 2018
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 14 of 18
Finding 3 – Terms of Reference errors (Operating effectiveness) Risk
We identified some minor duplication within the Terms of Reference:
'scope and duties':
1. Oversee the Primary & Community Care Delivery Plan in line with the IMTP.
3. Primary & Community Care Delivery Plan developing, implementing and
monitoring.
The following text on page 6 is written twice:
'The Director of Corporate Services & Governance/ Board Secretary, on behalf
of the Board, shall oversee a process of regular and rigorous self-assessment
and evaluation of the Committee's performance and operation.'
Governance arrangements not
properly discharged.
Non-Compliance with legislative requirements for Board committees
as set out in the Health Board's standing orders.
Recommendation Priority level
The Committee should review the Terms of Reference to correct any duplications
of responsibilities and text. Low
Management Response Responsible Officer/ Deadline
Following discussion with the Committee Chair, the Terms of Reference will be amended in line with Standing Orders and to correct the duplication of
responsibilities and text.
Gwenan Roberts
Next meeting – October 2018
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 15 of 18
Finding 4 - Timeliness of reports (Operating effectiveness) Risk
During our review of the agenda and minutes of the Committee we made the
following observations in relation to the timeliness of reports taken to the
Committee:
Post Payment Verification Report
A Post Payment Verification (PPV) Progress Report was referred to the Committee
by the Audit Committee, the timeline was as follows:
Report issued - October 2017
Presented to Audit Committee - 13 November 2017 - referred to PCC
Committee for monitoring.
Committee meeting - 29 November 2017 (no PPV due to closeness of meeting
dates).
Committee meeting - 10 January 2018, PPV received by Committee but full
responses tabled for future meeting.
Committee meeting - 4 April 2018, PPV report not discussed.
Committee meeting – 28 June 2018, PPV report discussed.
Therefore there is a time delay between Audit Committee referral for monitoring
and the PPV report being discussed in detail. The members noted during the June 2018 Committee meeting that some of the findings in the report ‘lacked clarity
and confused understanding’.
Ineffective decision making as a
result of poor training and support
Inappropriate/ inaccurate decisions made where too little or too much
information is provided.
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 16 of 18
Interim District Nurse Guiding Staffing Principles
We also note a delay when reporting the District Nursing Staffing Principles document which was presented at the 4 April 2018 Committee meeting.
However, there were two Committee meetings between the issue of the original
document by Welsh Government in September 2017, and the April Committee.
Recommendation Priority level
The Committee should ensure timely receipt, review and monitoring of reports
referred and relevant documents. Low
Management Response Responsible Officer/ Deadline
The Primary and Community Care Committee has been in development and increasing its scrutiny of a large clinical area of the Health Board. At the end of
2017 the Chair (Donna Mead) came to the end of her tenure and Maria Thomas took over as the Vice Chair of the Health Board. The Post Payment Verification
Report on closer inspection following the meeting on 10 January was not in line with the Directorate Management’s understanding of the current position and as
a consequence it was decided to move to the next meeting.
Members at the meeting in June noted that the directorate management team
had not been part of the development of the report nor had an opportunity to
comment on the accuracy of the report. A previous iteration of the report had
also caused a lot of additional work.
The aim going forward is always to work with the Chair to ensure sufficient time
Gwenan Roberts
October 2018
Governance arrangements - Primary & Community Care
Committee
Final Internal Audit Report
Appendix A - Action Plan
NHS Wales Audit & Assurance Services Page 17 of 18
is allocated for all matters to be considered by the Committee. The April meeting
was a particularly full agenda which then meant that the report was moved to June. I will work with the Chair of the Committee, using the Forward Look to plan
to receive reports as soon as practicable but there is a delay. In future, ensuring the reports are received at the earliest opportunity by the management team is
key to ensure accurate and comprehensive information.
Governance arrangements - Primary & Community Care Committee Internal Audit
Report
NHS Wales Audit and Assurance Services Page 18 of 18
Appendix B - Assurance opinion and action plan risk rating
Audit Assurance Ratings
Substantial assurance - The Board can take substantial assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Few matters require attention and are compliance
or advisory in nature with low impact on residual risk exposure.
Reasonable assurance - The Board can take reasonable assurance that arrangements
to secure governance, risk management and internal control, within those areas under review,
are suitably designed and applied effectively. Some matters require management attention in
control design or compliance with low to moderate impact on residual risk exposure until
resolved.
Limited assurance - The Board can take limited assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
moderate impact on residual risk exposure until resolved.
No assurance - The Board can take no assurance that arrangements to secure
governance, risk management and internal control, within those areas under review, are suitably
designed and applied effectively. More significant matters require management attention with
high impact on residual risk exposure until resolved.
Prioritisation of Recommendations
In order to assist management in using our reports, we categorise our recommendations
according to their level of priority as follows.
Priority
Level
Explanation Management
action
High
Poor key control design OR widespread non-
compliance with key controls.
PLUS
Significant risk to achievement of a system objective
OR evidence present of material loss, error or
misstatement.
Immediate*
Medium
Minor weakness in control design OR limited non-
compliance with established controls.
PLUS
Some risk to achievement of a system objective.
Within One
Month*
Low
Potential to enhance system design to improve
efficiency or effectiveness of controls.
These are generally issues of good practice for
management consideration.
Within Three
Months*
* Unless a more appropriate timescale is identified/agreed at the assignment.
3.3 Inverse Care Law/Population Health Management Pilot Update
1 3.3 Inverse Care Law and Population health management pilot report PCCC 10 October 2018.docx
Population Health Programmes update
Page 1 of 13 Primary and Community Care Committee Meeting
10 October 2018
AGENDA ITEM 3.3
10 October 2018
Primary and Community Care Committee Report
POPULATION HEALTH PROGRAMMES UPDATE: INVERSE CARE LAW PROGRAMME
(CARDIOVASCULAR HEALTH CHECK PROGRAMME) AND THE POPULATION HEALTH MANAGEMENT PILOT
Executive Lead: Director of Public Health / Director Primary Care,
Community & Mental Health
Authors: Consultants in Public Health
Contact Details for further information: Sara Thomas [email protected] (ICL Programme) and Kimberley Cann
[email protected] (Population Health Management Pilot Cwm Taf Local Public Health Team- 01685 351440
Purpose of the Primary and Community Care Committee Report
The purpose of this report is to inform the Primary Care Committee as to
the progress of the two Population Health Programmes in Cwm Taf
Governance
Link to Health
Board Strategic Objective(s)
The programmes support the principles of ‘Cwm Taf
Cares’ with particular reference to the organisational objective of protecting and improving population health.
The Inverse Care Law Programme work underpins the Health Board’s commitment to reducing health
inequalities in Cwm Taf. The Health Check Programme links to the Heart Disease, Stroke and Diabetes Delivery
Plans. It has been identified as a priority in the Health Board’s Integrated Medium Term Plan.
The Population Health Management Pilot is a cornerstone of the Fifth Wave Cwm Taf Population Health Strategy
Supporting evidence
Programme development has been based on current evidence base and best practice.
Engagement – Who has been involved in this work?
Primary Care, Public Health, Welsh Government and a variety of community
partners are key stakeholders. Opportunity for patient feedback and engagement has been incorporated into ongoing programme evaluation.

Population Health Programmes update
Page 2 of 13 Primary and Community Care Committee Meeting
10 October 2018
Primary and Community Care Committee Resolution to:
APPROVE ENDORSE DISCUSS NOTE √
Recommendation The Primary and Community Care Committee
is asked to • NOTE the on-going progress of the ICL
programme in Cwm Taf, locally reported outcomes and plans to revise the model going
forward • APPROVE that a more detailed report to include
the SAIL analysis and revised (post April 2019) delivery model be presented to the January
meeting of the Primary Care Committee. • NOTE the on-going progress of the Population
Health Management pilot.
Summarise the Impact of the Primary and Community Care
Committee Report
Equality and diversity
A population wide approach for those meeting the criteria for health check assessment is employed,
but with roll out prioritised initially into those areas with the highest levels of deprivation and
cardiovascular disease prevalence. The Population Health Management pilot will
identify population segments which will take account of these characteristics
Legal implications None
Population Health Deaths from circulatory disease account for around
25% of all premature (aged under 75 years) deaths each year in Cwm Taf. Although death rates are
falling, cardiovascular disease remains a major cause of premature morbidity and mortality, second
only to cancer1
The pattern of premature CVD mortality follows the
pattern of deprivation in Cwm Taf, with some of the highest rates in our more deprived valley
communities.
Cancer and cardiovascular disease are the main causes of years of life lost (YLL) and disability-
adjusted life years (DALYs) in Wales despite there being a significant drop for DALYs associated with
CVD in the last 15 years.2
1Public Health Wales Observatory (2014) Analysis of Annual District Death Extract & Mid Year Estimate (ONS) data for Cwm Taf population
2 Public Health Wales Observatory (2017) Health and its determinants in Wales- informing Public Health Wales Strategic Planning – Interim Report
Population Health Programmes update
Page 3 of 13 Primary and Community Care Committee Meeting
10 October 2018
Population segmentation will enable evidence based interventions to be targeted to the need of sub-
populations.
Quality, Safety &
Patient Experience
Patient pathways and associated assessment and
management protocols have been developed in line with NICE guidance. Programme protocols are
included in a new service handbook. All patients are given the opportunity to feedback on their
experiences of the programme either by written questionnaire or online survey.
Resources The programme receives Welsh Government
funding.
Risks and Assurance The burden of illness related to cardiovascular
disease has consequences for individuals’ health, as well as healthcare and social costs. The ability to
target interventions will enable better outcomes.
Health & Care
Standards
Health and Care Standards (2015)
1.1 Health promotion, protection and improvement
2.1 Managing risk and promoting health and safety
3.1 Safe and clinically effective care 3.4 Information governance and communication
technology
7.1 Workforce
Workforce ICL Programme - Welsh Government funding has
supported recruitment and training of staff to undertake this programme with support and
leadership from existing resource within the UHB Primary Care and Public Health Teams.
Population Health Management Pilot – Health Board
(and PHW) funding has been secured to pilot this approach.
Freedom of information status
Open
POPULATION HEALTH PROGRAMMES UPDATE:
INVERSE CARE LAW PROGRAMME (CARDIOVASCULAR HEALTH CHECK PROGRAMME)
Population Health Programmes update
Page 4 of 13 Primary and Community Care Committee Meeting
10 October 2018
AND THE POPULATION HEALTH MANAGEMENT PILOT
1. SITUATION / PURPOSE OF REPORT
The purpose of this report is to inform the Primary and Community Care Committee (PCCC) of progress in relation to two population health programmes
in Cwm Taf - the Cwm Taf Inverse Care Law (ICL) Programme (Cardio vascular disease CVD Health Checks) and a Population Health Management feasibility
study in the Rhondda Primary Care Cluster.
2. BACKGROUND / INTRODUCTION
The two programmes involve public health and primary care working together to improve population health in Cwm Taf. The Cwm Taf University Health Board
(CTUHB) Inverse Care Law Health Check Programme seeks to improve the health and wellbeing of adults aged 40-74 years through the early identification and
management of individual behavioural and physiological risk factors for cardiovascular disease and other conditions associated with these risk factors
e.g. cancer.
The Population Health Management pilot seeks to understand patient
populations, groups or clusters by characteristics related to their need and use of health care resources which can help Primary Care Clusters and GPs to decide
how best to use limited time and resources to deliver anticipatory and pre-emptive care for patients.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
INVERSE CARE LAW PROGRAMME
Status summary (September 2018)
Members will recall a report received by the Committee in September 2017 which provided the background, logic model and early outcomes of this high profile
Welsh Government (WG) funded programme which started in January 2015 and uses CTUHB and Aneurin Bevan University Health Board (ABUHB) as its pilot
sites.
Situation
The Health Board continues to deliver this programme that focuses on primary prevention of cardiovascular disease (and cancer) and will by March 2019 have
been made available to all practices across Cwm Taf, with particular emphasis on offering a health check to eligible patients resident in our more deprived
communities.
A quarterly report is provided to Welsh Government as part of a delivery agreement which is attached as Appendix 1 and also reported under a separate
agenda item for this meeting.
The report for Quarters 1 and 2 for 2018 highlight that:
Population Health Programmes update
Page 5 of 13 Primary and Community Care Committee Meeting
10 October 2018
• Overall approximately 40% of invited patients attend a health check. This
varies across practices with one practice achieving 85% uptake. • The programme is achieving a good attendance amongst middle-aged men, a
group that are generally difficult to reach.
• Uptake is lowest among the 40-44 age group, who have greatest capacity to benefit from adopting healthier lifestyles.
• Many patients are taking up offers of support to change lifestyles such as giving up smoking, increasing physical activity and reducing alcohol intake.
• At health check, a number of patients are triggering referral to their GP Practice team for further assessment leading to diagnoses of conditions such
as diabetes, high blood pressure (hypertension), and irregular heart rhythm (atrial fibrillation) that if not identified and treated would increase their risk of
a heart attack or stroke.
As part of the evaluation of the National Inverse Care Law Programme, a longitudinal study using the secure anonymised information linkage (SAIL)
database has been established which will provide a measure of short, medium and long term outcomes for the demonstrator sites in Cwm Taf and Aneurin
Bevan. A report informed by analysis of a SAIL data extraction was expected in September which would have enabled a more comprehensive update for the
committee. However, as mentioned in the delivery agreement report, this has
been delayed to December.
Key points • The programme continues to attract interest among politicians and WG officers
and the SAIL report is eagerly awaited • A different approach has been taken with Taf Ely Cluster whereby the Cluster
has been integral to shaping the way eligible patients are identified and prioritised and consequently how the ICL CVD Health Check Team resource is
deployed. It is envisaged that clusters will be encouraged to have greater ownership of the programme going forward.
• Conversations with Abertawe Bro Morgannwg University Health Board (ABMUHB) are on-going to learn more about their community based approach
to Health Checks piloted in the Bridgend North Cluster. • A workshop has been arranged for mid October to consider the future Inverse
Care Law delivery model in CTUHB. This will be informed by the uptake and
outcomes data together with feedback from patients, and clinicians and views of practices and clusters. Primary Care Colleagues in Bridgend have also been
invited to learn from their experience. • The future Cwm Taf model will need to consider key questions and challenges
raised including: o how to reach the >50% who do not take up the health check offer
including ▪ Who is and who is not having the Health Check?
▪ What are the factors that increase take-up among the population and sub-groups?
▪ Why do people not take up an offer of an NHS Health Check? ▪ The potential role of a workplace or community model

Population Health Programmes update
Page 6 of 13 Primary and Community Care Committee Meeting
10 October 2018
o “Maintenance phase” - methods of picking up patients who become
eligible for the health check as they turn 40 years of age and frequency of repeat health check at practice and cluster level;
o optimizing the outcomes of the health check by improving access to
support available to patients to make lifestyle changes and where appropriate linking them to community assets by means of social
referral; o How is primary care managing people identified as being at risk of CVD
or abnormal risk factor results? o What is the effect of the CTUHB ICL Health Check on disease detection,
changing behaviours, referrals to local risk management services, reductions in individual risk factor prevalence, reducing CVD risk, statin
and/or antihypertensive prescribing compared to other programmes such as ABUHB and NHS Health Check in England?
o Use of predictive modelling approach to explore potential longer term outcomes and cost effectiveness of the intervention.
• A software provider will need to be secured to support the revised model post April 2019. This currently poses a risk to the programme, but can be mitigated
by timely support from the NHS Wales Informatics Service (NWIS).
Consideration of these queries and the key challenges above will form the basis
of an action plan, to take the programme forward locally.
POPULATION HEALTH MANAGEMENT
Status summary (September 2018)
Situation Population segmentation and risk stratification is being piloted across the
Rhondda primary care cluster to assess the feasibility of this approach to support population health management across Cwm Taf UHB. Primary care and secondary
care patient data are being linked and the Adjusted Clinical Groups model developed by the John Hopkins University is being applied, amongst others, to
predict individual patient’s risk of different health outcomes. We are also segmenting the population based on a range of factors to identify groups by their
holistic need. We will then identify which segments are most likely benefit from
anticipatory care, and work with healthcare professionals and patients to identify the most important outcomes for these segments of the population. We can then
identify and implement the most effective evidence-based interventions.
Background
The Population Health Management pilot seeks to understand patient populations, groups or clusters by characteristics related to their need and use of health care
resources can help Primary Care Clusters and GPs to decide how best to use limited time and resources to deliver anticipatory and pre-emptive care for
patients. Individuals in populations often share characteristics with others in the

Population Health Programmes update
Page 7 of 13 Primary and Community Care Committee Meeting
10 October 2018
population. These characteristics can be quite different from the medical condition
they have and may, or may not, be seeking care for. By combining information on a range of acute and chronic conditions and healthcare usage, it is possible to
identify groups of patients based on their holistic need, rather than just disease
condition. Clustering individuals in this way can identify new segments of the population with similar needs. Their future risk and healthcare usage can then be
predicted and used to plan future care and resource needs for the population. This can help healthcare providers to take a person-centred, preventative
approach by providing the opportunity to intervene earlier and before a patient develops multiple conditions or their current condition worsens. We can also
target interventions at individuals who are the most likely to benefit from them, at the time they are most likely to be effective, taking preventative action before
further conditions develop. This would help to reduce demand for unscheduled, primary and secondary care and help to ease the pressure on appointments. It
would also help to prevent unplanned emergency admissions to secondary care and keep people healthy and at home for longer.
Action
We are currently in phase I of the pilot during which the GP practices have access to live reports on individual patients and their risk of future healthcare need for
a period of 3 months. The Local Public Health Team have access to aggregated
anonymous information on the pilot population. Population segmentation is also underway.
In addition, we are undertaking a process evaluation to inform potential roll out
of this approach across CTUHB in future. This includes an assessment of the usefulness of the approach to GP practise and its potential to inform the targeting
of interventions at population segments based on their holistic need.
Results Key findings from the initial population health overview
• 1% of patients account for 19% of costs across the cluster area. However, this cohort of patients may be frail or nearing the end of their life and not
amenable to standard interventions. • It is more common for individual to have multiple chronic conditions than just
one – 31% of patients had 2 or more chronic conditions compared to 22%
who had just one. • For example, of the patients with Chronic Obstructive Pulmonary Disease
(COPD) 94% also carry at least one other condition. And nearly 20% of patients with COPD also have a mental health diagnosis.
• Average cost and activity increases with multi-morbidity and the biggest cost is for patients who have 2-4 chronic conditions (total cost of around
£118,650,000). • While costs and resource use increase with a patient’s age, multi-morbidity is
a greater driver of cost than age. Patterns of multi-morbidity also vary across the cluster.
• The proportion of patients at risk of mortality in the next 12 months (Mortality Risk Score) varies by GP practice. Individual patient risk scores may help
clinicians identify patients who need end-of-life care.
Population Health Programmes update
Page 8 of 13 Primary and Community Care Committee Meeting
10 October 2018
• Other risk models available for patients include: probability of emergency
admission; probability of in-patient hospitalisation in the next 6/12 months; probability of extended hospitalisation; current cost of healthcare use;
predicted cost of healthcare use; probability of high total cost; probability of
high pharmacy cost; and electronic frailty index.
Population segmentation
The initial iteration of the segmentation model has identified 36 different segments. We are working with Sollis Ltd. to adapt the model to make sure it is
adapted to our local population.
Next steps
Next steps will be to determine which of our segments are most likely to benefit from anticipatory care and to work with healthcare professionals and patients to
identify the outcomes which are most important to those segments. We will then use the evidence base to identify which interventions will be the most effective
in achieving these outcomes for the segments.
Phase II of the pilot will take place in May 2019 during which GP practices will be able to access the live reports for a period of 1 month. This allow any trends over
the 6-month intervening period to be identified. Measures of the accuracy of the model in predicting risk for the pilot population will also be available at this stage.
4. RECOMMENDATION
The Primary and Community Care Committee is asked to:
• NOTE the on-going progress of the Inverse Care Law (ICL) programme in Cwm Taf, locally reported outcomes and plans to revise the model going
forward • APPROVE that a more detailed report to include the SAIL analysis and revised
(post April 2019) delivery model be presented to the January meeting of the
Primary and Communty Care Committee. • NOTE the on-going progress of the Population Health Management pilot.
Freedom of
information status
Open
Population Health Programmes update
Page 9 of 13 Primary and Community Care Committee Meeting
10 October 2018
Appendix 1
National Primary Fund 2018-19
Template for Reporting the Results from Delivery Agreement
Organisation:
Cwm Taf University Health Board
Delivery Agreement Name:
Cardiovascular Risk ‘Health Check’ (Inverse Care Law Programme)
Welsh Government Delivery Agreement Reference:
CWT003
Organisation Lead Contact:
Sarah Bradley
Period Covered in this Report:
Quarter 1+2
• Healthcheck activity and results are captured in the patient practice record using the Healthcheck + software
• The Audit + platform enables the activity to be monitored at practice level and project activity data is captured regularly and reported monthly
• Patient referrals and outcomes will be monitored as part of a Longitudinal Evaluation of
• All eligible patients living in deprived areas will have been offered a health check
• Extent of HC uptake in practice setting will have informed future model and decision to offer HC in alternative venues (workplace or community) or target groups
• Sustainable Model for HC developed
• Outcomes of patients having HC in both cohorts (Practice and community venues) will be captured and reported via SAIL allowing greater understanding of outcomes
• Ongoing capture and use of case studies
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Population Health Programmes update
Page 10 of 13 Primary and Community Care Committee Meeting
10 October 2018
outcomes using data linkage (SAIL)
• Feedback is gathered from patients
• Feedback is obtained from GPs and Practice Staff
• There are other evaluation strands undertaken jointly with Aneurin Bevan as part of the National ICL programme board Research and Evaluation Framework including monitoring Trend of Premature CVD mortality and gap between most and least deprived
• Numbers of patients with disease identified through HC reported
• Impact on mortality trend is likely to take several years to demonstrate, but early signs in changes in lifestyle behaviours expected
• Understanding of the profile of patients attending and not attending for HC to inform efforts to improve uptake of HC offer
Outline progress with results/benefits expected by March 2019
Quarter 1+2 Cwm Taf is providing continued support to the National ICL Programme and implementation of the National Research and Evaluation Framework through the new programme lead and public health consultant. The final cluster of the initial programme will have a targeted approach to self-management follow up for patients who have undergone health check. This will involve an increased delivery of self-management education, awareness raising through a new communication approach utilising social media and partners along with social prescribing support in the postcode areas that are involved. Increasing flexibility, capacity and uptake is a priority for the team and appointments will now be offered out of regular working hours to increase attendance and meet the needs of the patients. A full service review is being undertaken by the new programme lead to ensure the objectives are being met and that the service is auditable, evaluated and effective. This is involving a variety of methods to maximise the opportunities available and improve the quality, prudence and sustainability of the service. The programme continues to roll out across Cwm Taf during these 2 reporting quarters with the final cluster of Taf commencing this Autumn. The delivery in Taf Cluster is being designed with the Cluster and will prioritise patients resident in areas of highest deprivation (WIMD quintiles 4 and 5). Activity data for quarter 1 & 2 is reported below: Headline Health Check activity for Quarter 1 & 2 (1/04-20/09/2018) The CVD Health Check Team has been active in 14 practices during the reporting period. 1973 people attended 179 people Did Not Attend a scheduled health check appointment 126 people declined the offer of an appointment
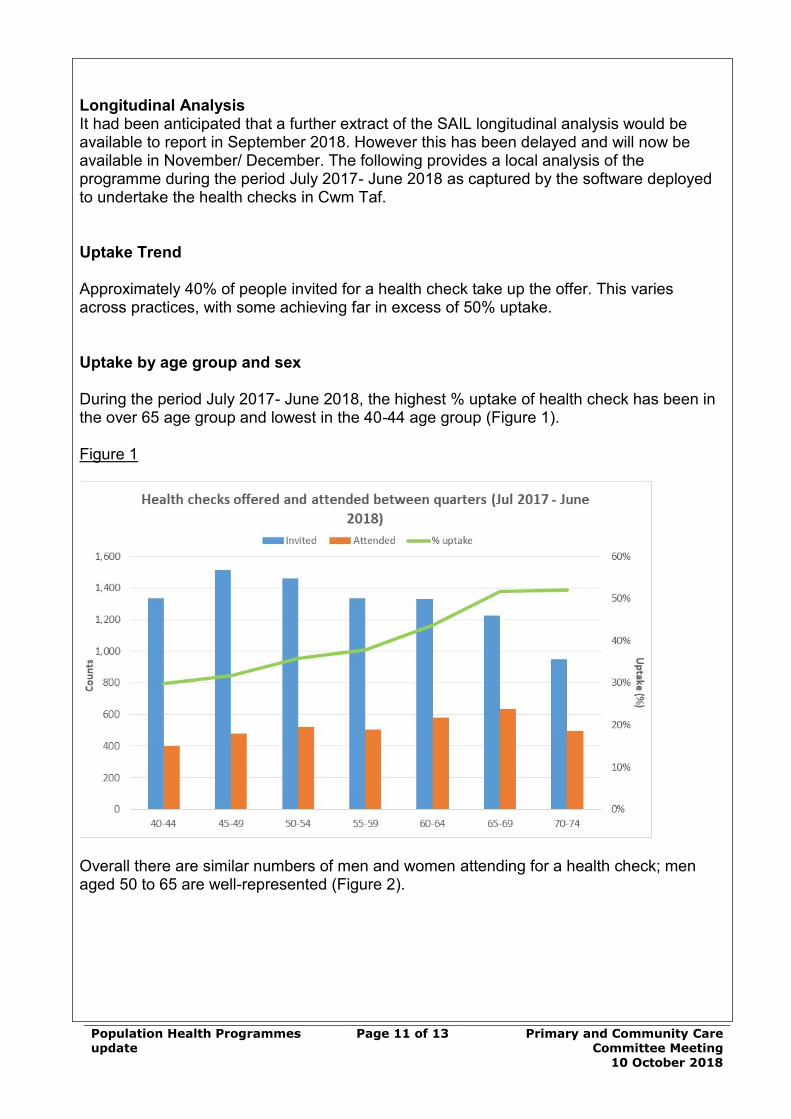
Population Health Programmes update
Page 11 of 13 Primary and Community Care Committee Meeting
10 October 2018
Longitudinal Analysis It had been anticipated that a further extract of the SAIL longitudinal analysis would be available to report in September 2018. However this has been delayed and will now be available in November/ December. The following provides a local analysis of the programme during the period July 2017- June 2018 as captured by the software deployed to undertake the health checks in Cwm Taf. Uptake Trend Approximately 40% of people invited for a health check take up the offer. This varies across practices, with some achieving far in excess of 50% uptake. Uptake by age group and sex During the period July 2017- June 2018, the highest % uptake of health check has been in the over 65 age group and lowest in the 40-44 age group (Figure 1). Figure 1
Overall there are similar numbers of men and women attending for a health check; men aged 50 to 65 are well-represented (Figure 2).
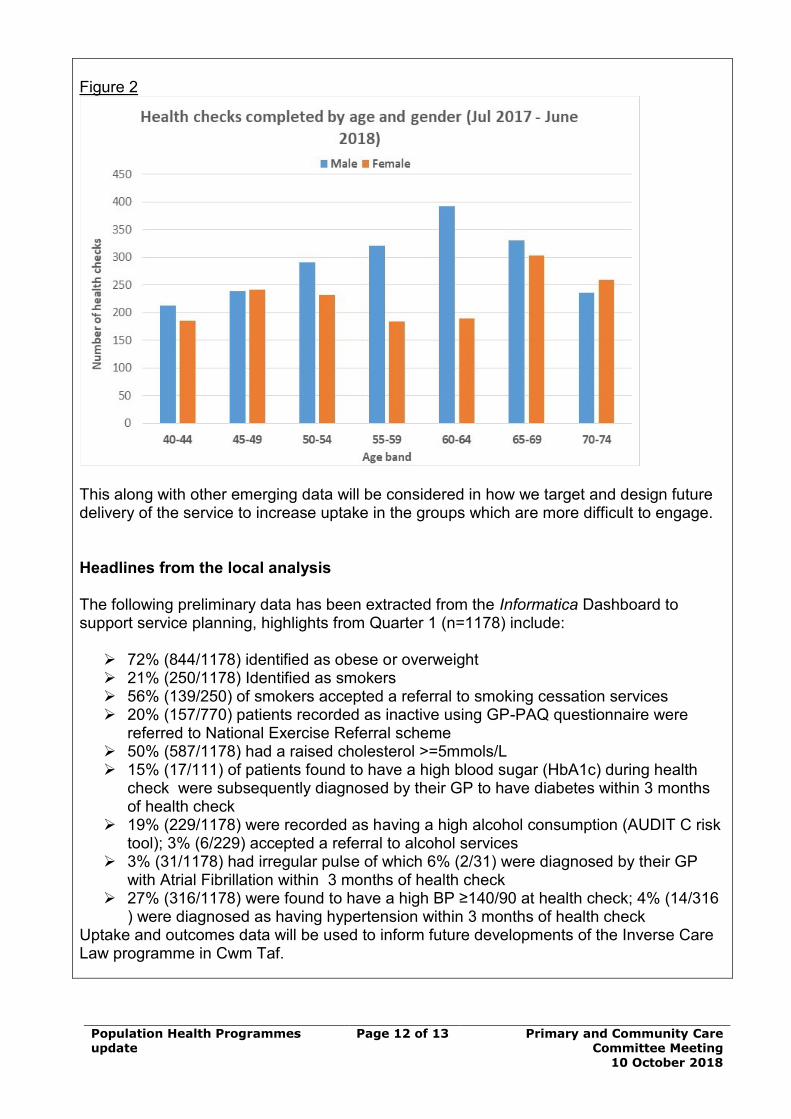
Population Health Programmes update
Page 12 of 13 Primary and Community Care Committee Meeting
10 October 2018
Figure 2
This along with other emerging data will be considered in how we target and design future delivery of the service to increase uptake in the groups which are more difficult to engage. Headlines from the local analysis The following preliminary data has been extracted from the Informatica Dashboard to support service planning, highlights from Quarter 1 (n=1178) include:
➢ 72% (844/1178) identified as obese or overweight ➢ 21% (250/1178) Identified as smokers ➢ 56% (139/250) of smokers accepted a referral to smoking cessation services ➢ 20% (157/770) patients recorded as inactive using GP-PAQ questionnaire were
referred to National Exercise Referral scheme ➢ 50% (587/1178) had a raised cholesterol >=5mmols/L ➢ 15% (17/111) of patients found to have a high blood sugar (HbA1c) during health
check were subsequently diagnosed by their GP to have diabetes within 3 months of health check
➢ 19% (229/1178) were recorded as having a high alcohol consumption (AUDIT C risk tool); 3% (6/229) accepted a referral to alcohol services
➢ 3% (31/1178) had irregular pulse of which 6% (2/31) were diagnosed by their GP with Atrial Fibrillation within 3 months of health check
➢ 27% (316/1178) were found to have a high BP ≥140/90 at health check; 4% (14/316 ) were diagnosed as having hypertension within 3 months of health check
Uptake and outcomes data will be used to inform future developments of the Inverse Care Law programme in Cwm Taf.
Population Health Programmes update
Page 13 of 13 Primary and Community Care Committee Meeting
10 October 2018
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
The programme lead vacancy was filled with a new manager commencing in August 2018. This will improve the delivery and strategic approach of the programme and future development. There are planning workshops in place for October to identify the future delivery model from April 2019 to which the Health Board is totally committed. There is an aspiration that the new model will provide further support to patients to reduce their risk of CVD through behaviour change. This will involve an enhanced system of linking individuals to support in their community, including social prescribing and utilisation of community assets. Long term issues with the information data dashboard have continued to be challenging and work is ongoing with NWIS and Informatica to address this. It is essential that NWIS are able to progress this work in a timely manner, particularly since the dashboard contract with Informatica expires end March 2019. In addition the licences for the healthcheck + software used in practices expire in March 2019 and NWIS support is required to advise on the best contract arrangement from April 2019 onwards which best fits the future delivery model for the Inverse Care Law programme in Cwm Taf. The evaluation report informed by SAIL data has been delayed by 3 months, which is a further challenge to planning and developing the service and measuring outcomes. We intend to report the SAIL analysis as soon as it is available and it will be included in our next report together with our proposed future delivery model.
Planned full year spend £m
Spend to date £m Forecast end year spend £m
Any difference between planned and forecast spend £m
0.360m 0.120m 0.338m 0.022m
3.4 Cluster Update
1 3.4 Cluster update PCCC 10 October 2018.docx
Cluster Update Page 1 of 8 Primary and Community Care Committee Meeting
10 October 2018
AGENDA ITEM 3.4
10 October 2018
Primary and Community Care Committee Report
PRIMARY CARE CLUSTER INITIATIVES
Executive Lead: Alan Lawrie, Director of Primary, Community and Mental
Health
Author: Tess Raybould Primary Care Development Manager
Contact Details for further information: [email protected]
Purpose of the Primary and Community Care Committee Report
The purpose of this report is to present members of the Primary and Community
Care Committee with an update on work being undertaken by the Primary Care Clusters. The report highlights areas of work currently being delivered for
patients using the Primary Care Cluster funding.
Governance
Link to Health
Board Strategic Objective(s)
The Board’s overarching role is to ensure its Strategy
outlined within ‘Cwm Taf Cares’ 3 Year Integrated Medium Term Plan 2018-2021 and the related organisational
objectives aligned with the Institute of Healthcare Improvement's (IHI) ‘Triple Aim’ are being progressed,
these in summary are:
• To improve quality, safety and patient experience • To protect and improve population health
• To ensure that the services provided are accessible and sustainable into the future
• To provide strong governance and assurance • To ensure good value based care and treatment for
our patients in line with the resources made available to the Health Board.
This report focuses largely on improving quality, safety, access and patient experience
Supporting
evidence
‘Our plan for primary care services in Wales’ Welsh
Government 2014 Cwm Taf UHB 3yr Integrated Plan
Cwm Taf Primary Care & Community Delivery Plan Cluster Plans for 2014-2017 & 2017-2020
Cluster Update Page 2 of 8 Primary and Community Care Committee Meeting
10 October 2018
Engagement – Who has been involved in this work?
Primary Care & Localities Management Team, GP Cluster leads and wider Primary and Community Healthcare staff including GPs, Practice managers,
Dental, Optometry & Pharmacy Representatives, Local Authority & Third Sector
Partners.
Primary and Community Care Committee Resolution To:
APPROVE ENDORSE DISCUSS NOTE √
Recommendation The Primary and Community Care Committee is asked
to:
• NOTE the report and progress that has been made by the Primary Care Clusters.
Summarise the Impact of the Primary and Community Care Committee
Report
Equality and diversity
Cluster plans are developed and any work attempts to address the deprivation and Inverse Care Law
implications for our population. It also recognises the specific needs of identified client groups.
Legal implications No legal implications have been identified.
Population Health The development of new services and initiatives within the Cluster areas will be tailored towards the needs of
the populations that it serves.
Quality, Safety &
Patient Experience
Governance structures are in place to ensure
development of any new service, models of care
consider the quality of our services to patients and enhancing the patient’s experience.
Resources The development and key delivery of any Cluster initiatives lies with Cluster Leads and other members
of network. This work is supported by dedicated UHB Cluster Development Managers. Cluster Network Plans
identify actions and highlight reports provided as part of the Welsh Government Delivery Agreements for
Primary Care.
Risks and Assurance Initiatives are implemented and piloted to determine benefits for the Cluster. Any risks will be identified
and assurances provided through regular Network plan updates, reports to the UHB and Welsh
Government.
Health & Care
Standards
The 22 Health & Care Standards for NHS Wales are
mapped into the 7 Quality Themes:
Staying Healthy; Safe Care; Effective Care; Dignified Care; Timely Care; Individual Care; Staff & Resources
http://www.wales.nhs.uk/sitesplus/documents/1064/24729_Health%20Standards%20Framework_2015_E
1.pdf

Cluster Update Page 3 of 8 Primary and Community Care Committee Meeting
10 October 2018
The work reported in this summary take into account many of the related quality themes
Workforce Clusters are working with the Health Board to determine future models and skill mix to provide
sustainable primary care services and deliver on the
ever growing needs of our population.
Freedom of
information status
Open
Cluster Update Page 4 of 8 Primary and Community Care Committee Meeting
10 October 2018
PRIMARY CARE CLUSTER INITIATIVES
1. SITUATION / PURPOSE OF REPORT
The purpose of this report is to present members of the Primary and Community
Care Committee with an update on work being undertaken by the Primary Care Clusters. The report highlights areas of work currently being delivered for
patients using the Primary Care Cluster funding.
2. BACKGROUND / INTRODUCTION
In November 2014, Welsh Government launched ‘Our Plan for a Primary Care
Service for Wales up to March 2018’, which clearly sets out the work NHS Wales will do by March 2018 to further develop and improve Primary Care and
Community Services.
Cluster Network plans are developed and are considered as a key element of the UHB Primary and Community Services integrated medium term plans (IMTP) and
are funded through the Welsh Government Service Delivery Agreements.
The Clusters are required to set out a three year network action plan, which should complement the individual practice development plans, tackling issues
that cannot be managed at an individual practice level, or can be more effectively and efficiently delivered through collaborative action.
The network approach supports greater consistency of service provision across the Cluster and improved quality of care, whilst more effectively managing the
impact of increasing demand set against financial and workforce challenges.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
This report provides a brief overview of the current work of the Primary Care
Clusters with the following focus: • Service sustainability
• Improved access • More services now available in the community.
The Clusters have development plans which have been informed by:
• Development plans produced by practices • Public health information on key health needs within the area
• Cwm Taf UHB information on current activity /referral patterns • Understanding of our localities baseline services (current service
provision) and identification of potential service provision unmet needs.

Cluster Update Page 5 of 8 Primary and Community Care Committee Meeting
10 October 2018
Clusters are embedding the foundations to deliver a more robust workforce and meet local needs of patients. As such across the clusters there has been
investment in recruitment of multi -disciplinary professionals to extend skills and deliver the most appropriate care including:
Cluster Pharmacists – Taf Ely / Rhondda / Cynon
Cluster Pharmacists are now embedded in the Practices and actively engaged in face to face patient consultations and medication reviews. The Pharmacy
department is evaluating the scheme in terms of cost/benefit analysis and anecdotally from practice feedback the Pharmacists are increasing capacity for
the GP’s and promoting a mixed skills model. Some independent prescribing courses have now been completed adding value to these roles.
Cluster Physiotherapy Service – Merthyr Tydfil
Up to 30% of consultations are thought to be for musculoskeletal (MSK)
conditions. The Merthyr Tydfil Cluster physiotherapy service is now delivering 25 sessions, each week. The service is delivered in each practice and provides
assessment and advice for this cohort of patients offering early, often same day access to a muscular skeletal specialist.
Occupational Therapist – North Cynon
This pilot has been so successful that the post has been made permanent and is now working across the four practices that make up the newly established North
Cynon Cluster. Referral rates for Quarter 1 & 2 has increased by 63% when compared to the same time period last year.
Behavioural Change Workers (GPSO) – Merthyr Tydfil
This initiative has been developed in partnership with the Merthyr Tydfil Cluster and Merthyr Tydfil Social Services. The aim of this project is to change the
behaviour and culture of patients who frequently visit their GP’s who do not need
medical Intervention. The GPSO will engage with patients to: • Advise/assess service users and address social issues and offer support in
correlation with the Social Services and Wellbeing Act. • To promote independence and enable service users to take responsibility
for their own health and wellbeing. • Supporting the reduction of attendance within general practice for non-
medical intervention. This includes utilising appropriate services in the locality which may include, networking with other agencies the third sector
and other community resources.
Care Navigators – Taf Ely & Merthyr Tydfil Care Navigation/Care Co-ordination offers the potential to free up GPs
consultation time each day by sign posting patients that do not need to see a doctor to more appropriate healthcare professionals, within or outside of the
Practice. It facilitates the development of the role of the reception staff to suit a
more multidisciplinary practice culture.
Cluster Update Page 6 of 8 Primary and Community Care Committee Meeting
10 October 2018
Third Sector Partnership Projects
Active Monitoring Practitioners – Taf Ely & Cynon
MIND Active Monitoring Practitioners are providing sessions from the practices offering brief interventions for early presentations of anxiety and depression.
Final evaluation will seek to demonstrate that the intervention has prevented the patient from re-presenting to the GP with the same issue thus preventing the
‘revolving door’ pattern of attendance. The impact on other mental health service referrals will also be considered. More recently, a process has been agreed to
allow the MIND practitioners to refer directly onto Primary Care Mental Health Teams when needed, rather than send this back to the GP.
Health & Wellbeing Community Coordinator - Rhondda
The Cluster agreed to recommission the service for a further 12 month period. The Wellbeing Co-ordinator is now in every practice for one day per week over a
two week period. A template has been developed to ensure that data is captured
in a structured way across all practices to aid with data collection and data analysis. The co-ordinator acts as sign poster and advocate.
Men and Women Sheds
Work is already underway to support these to become established ‘sheds’ in the Taf Ely area, namely:
• Weekly walking rugby, football and golf sessions • Gardening group and board game club
• Pontypridd canal group
• Weekly indoor bowling group • Community facility and gardening ‘grow for it’
Grow Rhondda
This is a community driven scheme in Upper Rhondda, where GPs in the area can ‘prescribe’ patients gardening activities with the goal of improving patients’
overall health and wellbeing. The gardening activities are delivered through local Men Sheds organisation and the gardens within one of our community hospitals
are used for the gardening activities. The scheme is aimed at patients who are over eighteen and experiencing social isolation/low self-esteem/mild anxiety &
depression.
Valley & Vale – Taf Ely Valley & Vale continue to deliver art based therapy sessions to specific individuals
& groups, through a joint funding arrangement. .
Drink Wise Age Well – Taf Ely
Drink Wise Age Well 3Cs in the Community (Companionship, Conversation and Creativity) sessions have continued in Ynysybwl. This group is being supported
by the Cluster with an aim of them to become a constituted group. The aim of these sessions is to boost the confidence of older people, encourage new
friendships, and find out about hobbies to help to improve their well-being.
Cluster Update Page 7 of 8 Primary and Community Care Committee Meeting
10 October 2018
Hapi Project (Newydd Housing Association) – Taf Ely Hapi in partnership with the GP deliver weekly sessions to GP identified patients
on Healthy eating, cooking and physical activity. Indications are that this has had a positive impact on the participants and families – through use of questionnaires,
a focus group and health checks, the Taf Cluster can now formally evaluate this programme.
Parkrun Practices – Rhondda & Cynon
In an exciting and innovative initiative, the Royal College of General Practitioners (RCGP) is partnering with Parkrun UK to promote the health and wellbeing of
staff and patients. Under this initiative, GP practices across the UK are encouraged to develop close links with their local parkrun to become parkrun
practices.
Waun Wen Lyndsey Leg Club - Rhondda
The Lyndsay Leg Club concept is an evidence-based initiative providing community-based treatments, health promotion, health education and on-going
care for people of all age groups who are experiencing leg-related problems. The key emphasis of the Leg Club is to actively “empower members to participate in
their own care, in a social environment that eases loneliness by providing congenial surroundings where old friends can meet and new friendships be
formed”.
Care & Repair Partnership - Cynon The engagement with Care & Repair in the Virtual Ward pilot in the North clearly
evidences how multi-agency working across the sectors can assist organisations in achieving service delivery targets whilst improving outcomes for patients. Care
and Repair now have representation at both Cynon Cluster meetings.
Other initiatives
Electronic Consultations – Merthyr Tydfil
The e-Consult platform delivers better patient access via participating GP practices website. This service speeds up access to safe, efficient care, whilst at
the same time reducing practices workload. One practice has noted the success to date and anticipates a potential saving of 60-70 appointments per week in the
longer term and reports 100% patient satisfaction for feedback supplied during July-September 2018.
Nursing/Residential Home project - Rhondda
Residential homes are linked to just one or two practices depending on the number of residents in order to improve communication between the GP and the
home. Each home manager has received a survey monkey 6 months after the changes were implemented. 57% of the homes involved responded and key
themes were are follows:
Cluster Update Page 8 of 8 Primary and Community Care Committee Meeting
10 October 2018
• Prior to the changes being implemented, 33% had patients registered with 6 different practices, 28% had patients registered with 5 different
practices, 22% registered with 4 different practices and 17% registered with 3 different practices. After the changes were implemented 67% had
patients registered at one practice and 33% had patients registered at 2 different practices.
• 75% felt that communication with the GP practice had improved as a result of the changes, 13% felt that communication had stayed the same and
12% felt that it had deteriorated. • 62% felt that the process for ordering repeat prescriptions felt there was
an improvement and 38% felt it was the same, none felt that this has deteriorated since the project.
• 37% felt their relationship with the GP practice had improved and 63% felt it was the same, none who responded felt their relationship had
deteriorated.
• 50% of respondents felt that the service to their residents had improved as a result of the changes implemented and 50% that the service remained
the same. None felt that the service to residents had deteriorated.
Workforce Planning – Cynon
Cynon is engaged in a pilot project with Skills for Health and the Workforce,
Education and Development Services (WEDS) to inform the design of a national
workforce planning tool specifically for Primary Care whilst producing two
workforce plans – one for North and one for the South. These plans will provide the Clusters with sustainable workforce models which will have considered
predicted population changes and local health needs.
Public Health – Rhondda and Taf Ely
Development of initiatives based on cluster specific health issues identified using
data and needs of the population e.g. Slimming World on Prescription (Rhondda),
Healthy Lifestyles programme (Taf).
4. RECOMMENDATION
The Primary and Community Care Committee is asked to:
• NOTE the progress being made by the Primary Care Clusters
Freedom of
information status
Open
3.5 Delivery Agreements
1 3.5 Delivery Agreement Progress Updates Q 1 and 2 PCCC 10 October 2018.docx
6 month Progress Updates
Primary Care Delivery Agreements
Page 1 of 5 Primary & Community Care
Committee Meeting
10 October 2018
AGENDA ITEM 3.5
10 October 2018
Primary & Community Care Committee Report
PRIMARY CARE INVESTMENTS: DELIVERY AGREEMENT 6 MONTH PROGRESS UPDATES
Executive Lead: Director of Primary, Community and Mental Health
Authors: Sarah Bradley, Head of Primary Care; Alison Lagier, Locality Manager; Lindsey Richardson, Head of Planning
Contact Details for further information: Lauren Morgan, 01443
443755 or email [email protected]
Purpose of the Primary & Community Care Committee Report
The purpose of this paper is to present the 6 month progress reports for the
Primary Care Delivery Agreements, covering 1 April to 30 September 2018. (Appendix 1).
Governance
Link to Health
Board Strategic Objective(s)
The Board’s overarching role is to ensure its Strategy
outlined within ‘Cwm Taf Cares’ 3 Year Integrated Medium Term Plan 2015-2018 and the related
organisational objectives aligned with the Institute of Healthcare Improvement's (IHI) ‘Triple Aim’ are being
progressed, these in summary are: • To improve quality, safety and patient
experience. • To protect and improve population health.
• To ensure that the services provided are accessible and sustainable into the future.
• To provide strong governance and assurance. • To ensure good value based care and treatment
for our patients in line with the resources made
available to the Health Board. This report focuses mainly on – To improve quality,
safety and patient experience.
Supporting
evidence
‘Setting the Direction’ Welsh Government
‘Social Services and Wellbeing’ (Wales) Act 2014 ‘Our plan for primary care services in Wales’ Welsh
Government 2014 Cwm Taf UHB 3yr Integrated Plan
Cwm Taf UHB Primary & Community Care Delivery Plan
6 month Progress Updates
Primary Care Delivery Agreements
Page 2 of 5 Primary & Community Care
Committee Meeting
10 October 2018
Engagement – Who has been involved in this work?
Primary Care & Localities Management Team and wider Primary and Community Localities staff, Mental Health Directorate, Primary Care
Steering Committee of the Board, Local Medical Committee (LMC), Acute
Directorate Managers, Practice Managers, Executive Board, GP Cluster Leads.
Primary & Community Care Committee Resolution to:
APPROVE ENDORSE DISCUSS NOTE √
Recommendation The Primary & Community Care Committee members
are asked to: • NOTE the first 6 monthly progress updates
against the Primary Care Delivery Agreements
Summarise the Impact of the Primary & Community Care Committee Report
Equality and Diversity
A key focus within these programmes of work attempts to address the deprivation and Inverse Care
Law implications for our population. It also recognises the specific needs of identified client groups.
Legal
Implications
None noted to date.
Population Health The programme of work is based on the health needs
assessment undertaken by Public Health Wales to support the Cluster Plan development.
Quality, Safety &
Patient Experience
The work centres on improving the quality of our
services to patients and enhancing the patient’s experience.
Resources The resources to develop the work are allocated form the dedicated Primary Care Investments as outlined
within the paper. The resource to deliver the work is within the Primary Care & Localities management
team.
Risks and Assurance
Any potential or actual risks in relation to the plan will continue to be monitored reported through the
mechanisms outlined within the report to Welsh Government and internally through our Clinical
Business Meeting, Executive Board and this Primary Care Committee of the board and would feature if
appropriate on our risk register.
Health & Care Standards
The 22 Health & Care Standards for NHS Wales are mapped into the 7 Quality Themes:
Staying Healthy; Safe Care; Effective Care; Dignified Care; Timely Care; Individual Care; Staff & Resources
http://www.wales.nhs.uk/sitesplus/documents/1064/24729_Health%20Standards%20Framework_2015
_E1.pdf
6 month Progress Updates
Primary Care Delivery Agreements
Page 3 of 5 Primary & Community Care
Committee Meeting
10 October 2018
The work reported in this summary takes into account many of the related quality themes.
Workforce There are key workforce issues associated with this work in relation to demand on GP’s and practice staff
in general also the demand on acute services. The
intention is that this work will support alternative roles and skill mix to deliver on the ever growing
needs of our population. The workforce issues outlined within this work are reflected in detail within
our Integrated 3 yr plan.
Freedom of
Information Status
Open
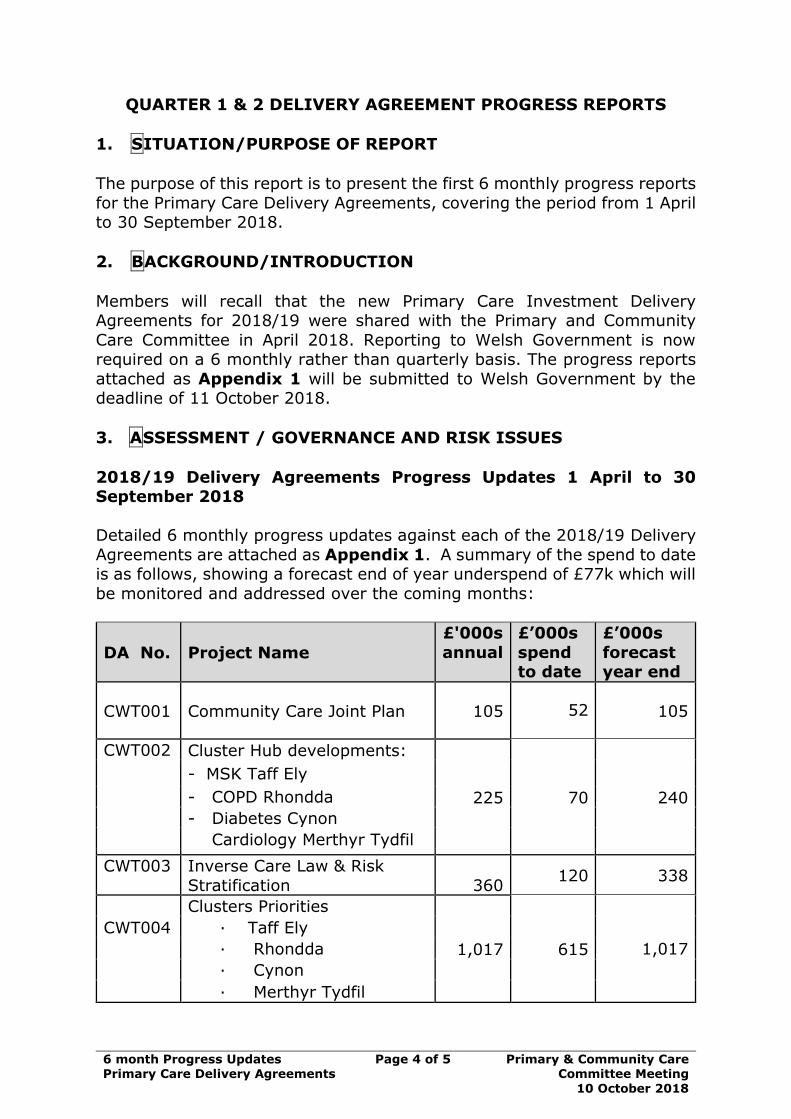
6 month Progress Updates
Primary Care Delivery Agreements
Page 4 of 5 Primary & Community Care
Committee Meeting
10 October 2018
QUARTER 1 & 2 DELIVERY AGREEMENT PROGRESS REPORTS
1. SITUATION/PURPOSE OF REPORT
The purpose of this report is to present the first 6 monthly progress reports
for the Primary Care Delivery Agreements, covering the period from 1 April to 30 September 2018.
2. BACKGROUND/INTRODUCTION
Members will recall that the new Primary Care Investment Delivery Agreements for 2018/19 were shared with the Primary and Community
Care Committee in April 2018. Reporting to Welsh Government is now required on a 6 monthly rather than quarterly basis. The progress reports
attached as Appendix 1 will be submitted to Welsh Government by the deadline of 11 October 2018.
3. ASSESSMENT / GOVERNANCE AND RISK ISSUES
2018/19 Delivery Agreements Progress Updates 1 April to 30
September 2018
Detailed 6 monthly progress updates against each of the 2018/19 Delivery
Agreements are attached as Appendix 1. A summary of the spend to date is as follows, showing a forecast end of year underspend of £77k which will
be monitored and addressed over the coming months:
DA No. Project Name
£'000s
annual
£’000s
spend to date
£’000s
forecast year end
CWT001 Community Care Joint Plan 105 52
105
CWT002 Cluster Hub developments:
225 70 240
- MSK Taff Ely
- COPD Rhondda
- Diabetes Cynon
Cardiology Merthyr Tydfil
CWT003 Inverse Care Law & Risk
Stratification
360 120 338
Clusters Priorities
1,017 615
CWT004 · Taff Ely
· Rhondda 1,017
· Cynon
· Merthyr Tydfil

6 month Progress Updates
Primary Care Delivery Agreements
Page 5 of 5 Primary & Community Care
Committee Meeting
10 October 2018
DA No. Project Name
£'000s annual
£’000s spend
to date
£’000s forecast
year end
CWT005 Research, Evaluation & Development
97 45 97
CWT006 Multidisciplinary team
development 662 264 624
CWT007 Wound Care 356 130 330
CWT008 Older Persons Mental Health Redesign
480 240 480
CWT009 Out of Hours Redesign 550 212 550
CWT010 Training and development/ Primary care management
and leadership
702 249 777
CWT011 Advanced Training Practice
Hub & Spoke 382 43 301
Total 4,936 2,040 4,859
-77
The next progress updates will be the year end reports, to be submitted to
Welsh Government by 11 April 2019. These will be brought to the Primary & Community Care Committee meeting on 3 April 2019 for information prior
to submission.
4. RECOMMENDATION
The Primary & Community Care Committee members are asked to:
• NOTE the 6 monthly progress updates against each of the Primary Care
Delivery Agreements which will be submitted to Welsh Government on 11 October 2018 and the forecast year end spend.
Freedom of Information
Status
Open
3.5.1 Appendix 1 Composite Delivery Agreement Progress Update report PCCC 10 October 2018
1 3.5.1 Appendix 1 Composite Delivery Agreement Progress Update report PCCC 10 October 2018.pdf
Primary & Community Care Committee Item 3.5 Appendix 1
1
National Primary Fund 2018/19 Delivery Agreements 6 monthly Progress Updates
1st April to 30th September 2018
Scheme No.
Project Name Page
CWT001 Community Care Joint Plan 2
CWT002 Cluster Hub developments 4
CWT003 Inverse Care Law Programme 10
CWT004 Primary Care Clusters 15
CWT005 Research, Development & Service Evaluation 29
CWT006 Multi-Disciplinary Development – Recruitment & Retention
33
CWT007 Cluster Wound Clinics 34
CWT008 Older Persons Mental Health Redesign 37
CWT009 Out of Hours Redesign 38
CWT010 Training & Development/Management & Leadership
40
CWT011
PACESETTER - Development of Advanced Training Practice / Hub & Spoke networks
42
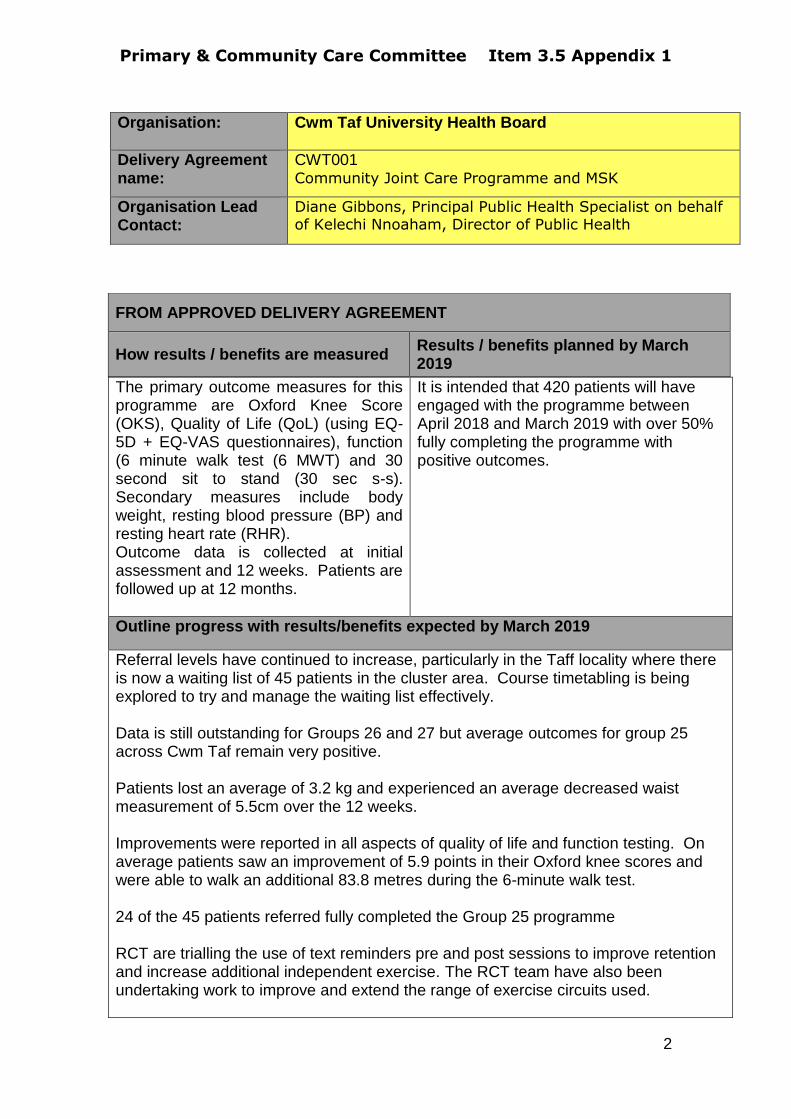
Primary & Community Care Committee Item 3.5 Appendix 1
2
Organisation:
Cwm Taf University Health Board
Delivery Agreement name:
CWT001 Community Joint Care Programme and MSK
Organisation Lead Contact:
Diane Gibbons, Principal Public Health Specialist on behalf of Kelechi Nnoaham, Director of Public Health
The primary outcome measures for this programme are Oxford Knee Score (OKS), Quality of Life (QoL) (using EQ-5D + EQ-VAS questionnaires), function (6 minute walk test (6 MWT) and 30 second sit to stand (30 sec s-s). Secondary measures include body weight, resting blood pressure (BP) and resting heart rate (RHR). Outcome data is collected at initial assessment and 12 weeks. Patients are followed up at 12 months.
It is intended that 420 patients will have engaged with the programme between April 2018 and March 2019 with over 50% fully completing the programme with positive outcomes.
Outline progress with results/benefits expected by March 2019
Referral levels have continued to increase, particularly in the Taff locality where there is now a waiting list of 45 patients in the cluster area. Course timetabling is being explored to try and manage the waiting list effectively. Data is still outstanding for Groups 26 and 27 but average outcomes for group 25 across Cwm Taf remain very positive. Patients lost an average of 3.2 kg and experienced an average decreased waist measurement of 5.5cm over the 12 weeks. Improvements were reported in all aspects of quality of life and function testing. On average patients saw an improvement of 5.9 points in their Oxford knee scores and were able to walk an additional 83.8 metres during the 6-minute walk test. 24 of the 45 patients referred fully completed the Group 25 programme RCT are trialling the use of text reminders pre and post sessions to improve retention and increase additional independent exercise. The RCT team have also been undertaking work to improve and extend the range of exercise circuits used.
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019

Primary & Community Care Committee Item 3.5 Appendix 1
3
Merthyr are currently working with the physio team to pilot a back care programme which commenced in September. The Merthyr team are also linking in with physio in regards to developing their approach to pain management as part of the programme. Both JCP teams are trialling new venues according to demand.
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
The level of increased referrals in some areas may require changes in timetabling to accommodate and if necessary a review of patient criteria to ensure that patients do not have to wait for long periods.
Planned full year spend £k
Spend to date £k Forecast end year spend £k
Any difference between planned and forecast spend £k
105m 52m 105m 0
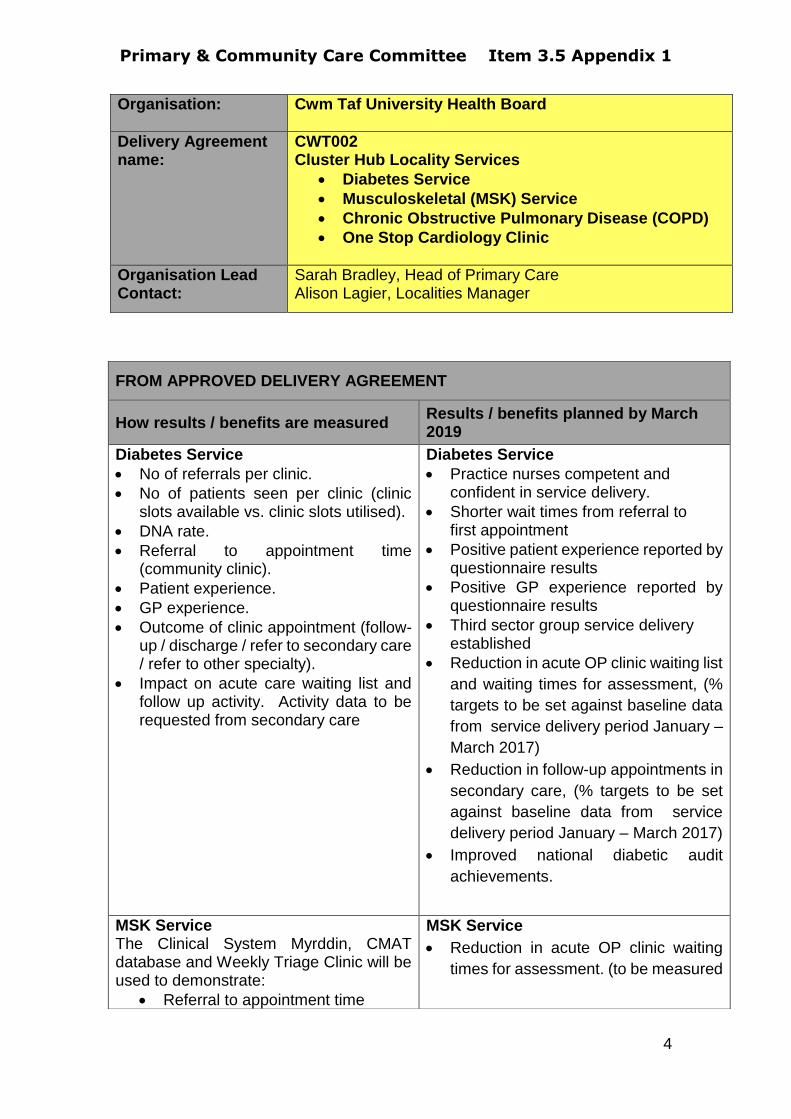
Primary & Community Care Committee Item 3.5 Appendix 1
4
Organisation:
Cwm Taf University Health Board
Delivery Agreement name:
CWT002 Cluster Hub Locality Services
Diabetes Service
Musculoskeletal (MSK) Service
Chronic Obstructive Pulmonary Disease (COPD)
One Stop Cardiology Clinic
Organisation Lead Contact:
Sarah Bradley, Head of Primary Care Alison Lagier, Localities Manager
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Diabetes Service
No of referrals per clinic.
No of patients seen per clinic (clinic slots available vs. clinic slots utilised).
DNA rate.
Referral to appointment time (community clinic).
Patient experience.
GP experience.
Outcome of clinic appointment (follow-up / discharge / refer to secondary care / refer to other specialty).
Impact on acute care waiting list and follow up activity. Activity data to be requested from secondary care
Diabetes Service
Practice nurses competent and confident in service delivery.
Shorter wait times from referral to first appointment
Positive patient experience reported by questionnaire results
Positive GP experience reported by questionnaire results
Third sector group service delivery established
Reduction in acute OP clinic waiting list
and waiting times for assessment, (%
targets to be set against baseline data
from service delivery period January –
March 2017)
Reduction in follow-up appointments in
secondary care, (% targets to be set
against baseline data from service
delivery period January – March 2017)
Improved national diabetic audit
achievements.
MSK Service The Clinical System Myrddin, CMAT database and Weekly Triage Clinic will be used to demonstrate:
Referral to appointment time
MSK Service
Reduction in acute OP clinic waiting
times for assessment. (to be measured
Primary & Community Care Committee Item 3.5 Appendix 1
5
No of referrals MSK clinic
Referral to appointment time
No of patients seen per clinic Impact on secondary care waiting list
Outcome of clinic appointment Patient experience - questionnaires will be used to determine not only experience but also outcomes for patients – with emphasis on self management and ongoing support e.g. through referrals to joint care programme. Number of re-referrals to CMATS triage within 6 months of appointment. Clinician experience - ongoing operational meetings and evaluation of service level agreements.
in the first quarter of the service
commencing and then % targets set)
Reduction in conversions for surgery
(to be measured in the first quarter of
the service commencing and then %
targets set)
Self evaluated reduction in pain by
patients
COPD Discharge Service
No of referrals per clinic
No of patients seen per clinic (clinic slots available vs. clinic slots utilised)
DNA rate
Referral to 1st telephone contact (community clinic)
No of patients who complete 6 week programme
No of patients re-admitted within 6 week programme
Number and type of referral to other services
Patient experience
GP experience
Impact on acute care follow up activity. Activity data to be requested from secondary care
COPD Discharge Service
Decrease in the number of patients being re-admitted following an exacerbation of COPD.
Patient evaluation of intervention re
confidence in managing own condition
Reduction in visits to GP – reduced
number of exacerbations for individual
patients
Reduction in acute follow- up
appointments
Reduction in re-admissions
Reduction in COPD attendances /
admissions to Secondary Care.
Reduction in ambulance call outs for
COPD indicators in the Rhondda and
conveyances to the hospital
One Stop Cardiology Clinic
No of referrals per clinic.
No of patients seen per clinic (clinic
slots available vs clinic slots utilised).
DNA rate.
No of referrals to open access
diagnostics (by diagnostic).
One Stop Cardiology Clinic
Reduced wait times for diagnostics and outpatients.
Improved access to cardiology diagnostics such as 24hr/7 day electrocardiogram, 24 hour ambulatory blood pressure monitoring.
Primary & Community Care Committee Item 3.5 Appendix 1
6
Outline progress with results/benefits expected by March 2019
Clinics are now fully established with the multi-disciplinary teams working together to deliver regular clinics to patients in the community settings of Dewi Sant, Keir Hardie Health Park, Ysbyty Cwm Cynon and Ysbyty Cwm Rhondda. There is initial information that shows where there has been a positive impact on referral to waiting times and more patients being seen in the community clinics in a timely manner. Data has been collected to demonstrate any impact for each specific area. All four schemes are currently going through a final evaluation which will be completed by June 2018. This will allow decisions to be made on future delivery and roll out of clinics. Diabetes Clinic Diabetes UK volunteers are now fully integrated with the delivery of services at the Cynon Diabetes Community Clinic and attend on a weekly basis to support patients and share information. Clinic data shows:
Number of patients seen January 2017 – January 2018 inclusive = 448
Impact on secondary care waiting list = 32 weeks ( November 2015), 6 weeks (November 2017).
82% of patients achieved a reduction in their HbA1c by between 2 to 83 mmol/l
39% of patients achieved an HbA1c < 64 where their baseline was > 64mmol/l
45% patients started treatment with an HbA1c > 90mmol/l, 97% reduced their HbA1c with 27% achieving < 64mmol/l
One patient reduced their HbA1c from 144 to 61mmol/l
Referral to appointment time
(community clinic).
Referral to appointment time
(diagnostics).
Outcome of clinic appointment (follow-
up/discharge/refer to cardiology/refer
to other specialty).
Outcome of diagnostic (discharge /
other).
Patient experience.
GP experience.
Impact on secondary care waiting list.
No of patients seen who were referred
to secondary care cardiology service
within 6 months of appointment.
No of patients who attended A&E for
cardiac related issue within 6 months
of appointment.
Diagnostic results should be returned to the GP within two weeks.
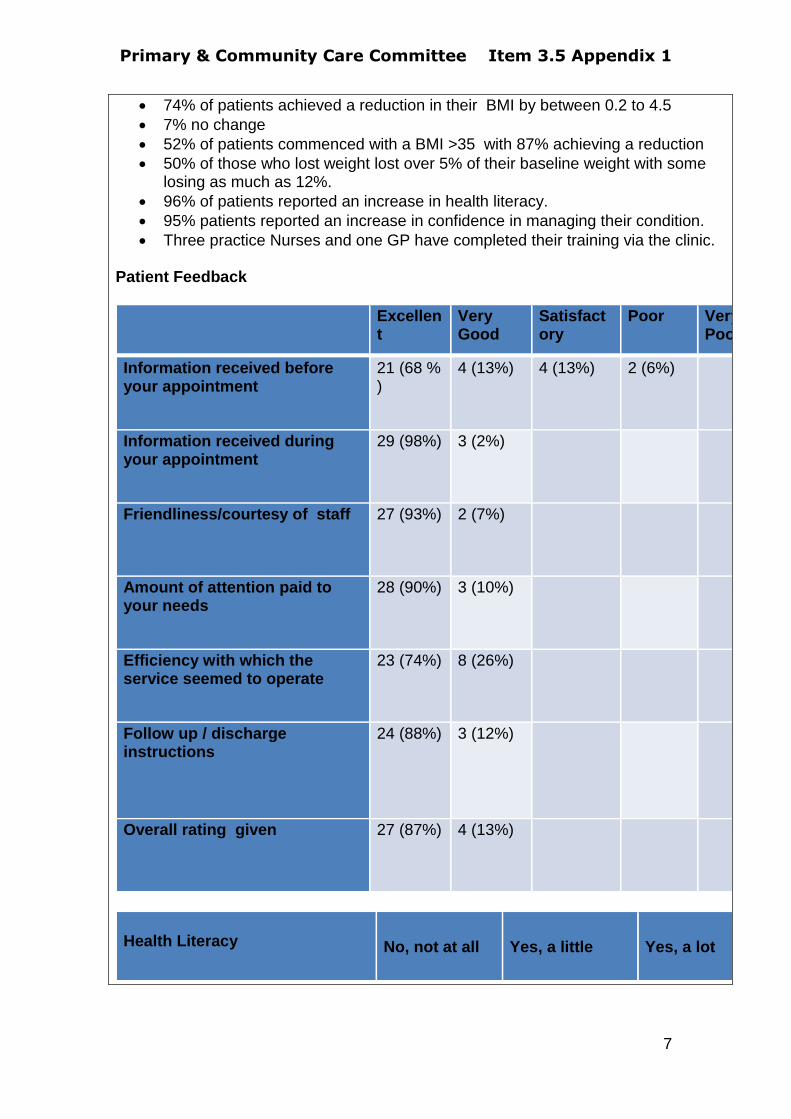
Primary & Community Care Committee Item 3.5 Appendix 1
7
74% of patients achieved a reduction in their BMI by between 0.2 to 4.5
7% no change
52% of patients commenced with a BMI >35 with 87% achieving a reduction
50% of those who lost weight lost over 5% of their baseline weight with some losing as much as 12%.
96% of patients reported an increase in health literacy.
95% patients reported an increase in confidence in managing their condition.
Three practice Nurses and one GP have completed their training via the clinic. Patient Feedback
Excellent
Very Good
Satisfactory
Poor Very Poor
Information received before your appointment
21 (68 % )
4 (13%) 4 (13%) 2 (6%)
Information received during your appointment
29 (98%) 3 (2%)
Friendliness/courtesy of staff
27 (93%) 2 (7%)
Amount of attention paid to your needs
28 (90%) 3 (10%)
Efficiency with which the service seemed to operate
23 (74%) 8 (26%)
Follow up / discharge instructions
24 (88%) 3 (12%)
Overall rating given
27 (87%) 4 (13%)
Health Literacy No, not at all Yes, a little Yes, a lot
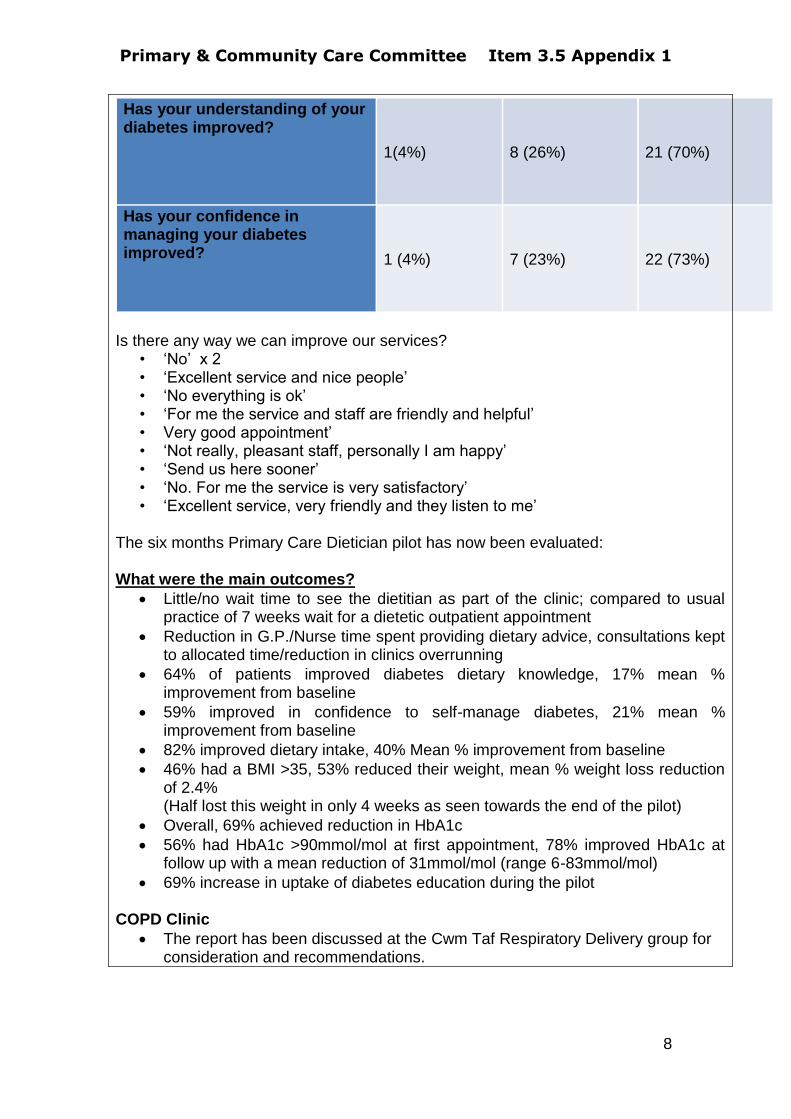
Primary & Community Care Committee Item 3.5 Appendix 1
8
Has your understanding of your diabetes improved? 1(4%) 8 (26%) 21 (70%)
Has your confidence in managing your diabetes improved?
1 (4%) 7 (23%) 22 (73%)
Is there any way we can improve our services?
• ‘No’ x 2 • ‘Excellent service and nice people’ • ‘No everything is ok’ • ‘For me the service and staff are friendly and helpful’ • Very good appointment’ • ‘Not really, pleasant staff, personally I am happy’ • ‘Send us here sooner’ • ‘No. For me the service is very satisfactory’ • ‘Excellent service, very friendly and they listen to me’
The six months Primary Care Dietician pilot has now been evaluated: What were the main outcomes?
Little/no wait time to see the dietitian as part of the clinic; compared to usual practice of 7 weeks wait for a dietetic outpatient appointment
Reduction in G.P./Nurse time spent providing dietary advice, consultations kept to allocated time/reduction in clinics overrunning
64% of patients improved diabetes dietary knowledge, 17% mean % improvement from baseline
59% improved in confidence to self-manage diabetes, 21% mean % improvement from baseline
82% improved dietary intake, 40% Mean % improvement from baseline
46% had a BMI >35, 53% reduced their weight, mean % weight loss reduction of 2.4% (Half lost this weight in only 4 weeks as seen towards the end of the pilot)
Overall, 69% achieved reduction in HbA1c
56% had HbA1c >90mmol/mol at first appointment, 78% improved HbA1c at follow up with a mean reduction of 31mmol/mol (range 6-83mmol/mol)
69% increase in uptake of diabetes education during the pilot COPD Clinic
The report has been discussed at the Cwm Taf Respiratory Delivery group for consideration and recommendations.
Primary & Community Care Committee Item 3.5 Appendix 1
9
It has been recommended, based on the outcomes detailed in the report, that Phase 1 of the COPD service continues to be delivered in the Rhondda and that the service is rolled out to another of the cluster areas.
The resources required to roll out the service to the three other cluster areas have been identified.
The Cynon has been identified as the next area in which the service will be implemented as they have the next highest prevalence of COPD. Discussions are ongoing with the respiratory team that serve the patients who live in the Cynon area as their service delivery model is slightly different to that in Rhondda, so some changes may be required in order to implement the service effectively .
Cardiology Clinic
The clinic has been running bi-weekly (excluding annual leave)
Vision 360 has now successfully proven the concept and clinicians have the ability to write directly into patients records within the Merthyr Cluster and all technical complications have been resolved.
Data is currently being collated to identify the benefits and impact the clinic is having on emergency attendance and the secondary care waiting list.
A meeting is taking place during September 2018 to agree a consensus on a health board wide model for community cardiology services
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
none
Planned full year spend £’000
Spend to date £’000
Forecast end year spend £’000
Any difference between planned and forecast spend £’000
225 70 240 15
Primary & Community Care Committee Item 3.5 Appendix 1
10
Organisation:
Cwm Taf University Health Board
Delivery Agreement name:
CWT003 Cardiovascular Risk ‘Health Check’ (Inverse Care Law Programme)
Organisation Lead Contact:
Sarah Bradley
Healthcheck activity and results are captured in the patient practice record using the Healthcheck + software
The Audit + platform enables the activity to be monitored at practice level and project activity data is captured regularly and reported monthly
Patient referrals and outcomes will be monitored as part of a Longitudinal Evaluation of outcomes using data linkage (SAIL)
Feedback is gathered from patients
Feedback is obtained from GPs and Practice Staff
There are other evaluation strands undertaken jointly with Aneurin Bevan as part of the National ICL programme board Research and Evaluation Framework including monitoring Trend of Premature CVD mortality and gap between most and least deprived
All eligible patients living in deprived areas will have been offered a health check
Extent of HC uptake in practice setting will have informed future model and decision to offer HC in alternative venues (workplace or community) or target groups
Sustainable Model for HC developed
Outcomes of patients having HC in both cohorts (Practice and community venues) will be captured and reported via SAIL allowing greater understanding of outcomes
Ongoing capture and use of case studies
Numbers of patients with disease identified through HC reported
Impact on mortality trend is likely to take several years to demonstrate, but early signs in changes in lifestyle behaviours expected
Understanding of the profile of patients attending and not attending for HC to inform efforts to improve uptake of HC offer
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Primary & Community Care Committee Item 3.5 Appendix 1
11
Outline progress with results/benefits expected by March 2019
Quarter 1+2 April – September 2018 Cwm Taf is providing continued support to the National ICL Programme and implementation of the National Research and Evaluation Framework through the new programme lead and public health consultant. The final cluster of the initial programme will have a targeted approach to self-management follow up for patients who have undergone health check. This will involve an increased delivery of self-management education, awareness raising through a new communication approach utilising social media and partners along with social prescribing support in the postcode areas that are involved. Increasing flexibility, capacity and uptake is a priority for the team and appointments will now be offered out of regular working hours to increase attendance and meet the needs of the patients. A full service review is being undertaken by the new programme lead to ensure the objectives are being met and that the service is auditable, evaluated and effective. This is involving a variety of methods to maximise the opportunities available and improve the quality, prudence and sustainability of the service. The programme continues to roll out across Cwm Taf during these 2 reporting quarters with the final cluster of Taf commencing this Autumn. The delivery in Taf Cluster is being designed with the Cluster and will prioritise patients resident in areas of highest deprivation (WIMD quintiles 4 and 5). Activity data for quarter 1 & 2 is reported below: Headline Health Check activity for Quarter 1 & 2 (1/04-20/09/2018) The CVD Health Check Team has been active in 14 practices during the reporting period. 1973 people attended 179 people Did Not Attend a scheduled health check appointment 126 people declined the offer of an appointment Longitudinal Analysis It had been anticipated that a further extract of the SAIL longitudinal analysis would be available to report in September 2018. However this has been delayed and will now be available in November/ December. The following provides a local analysis of the programme during the period July 2017- June 2018 as captured by the software deployed to undertake the health checks in Cwm Taf. Uptake Trend Approximately 40% of people invited for a health check take up the offer. This varies across practices, with some achieving far in excess of 50% uptake.
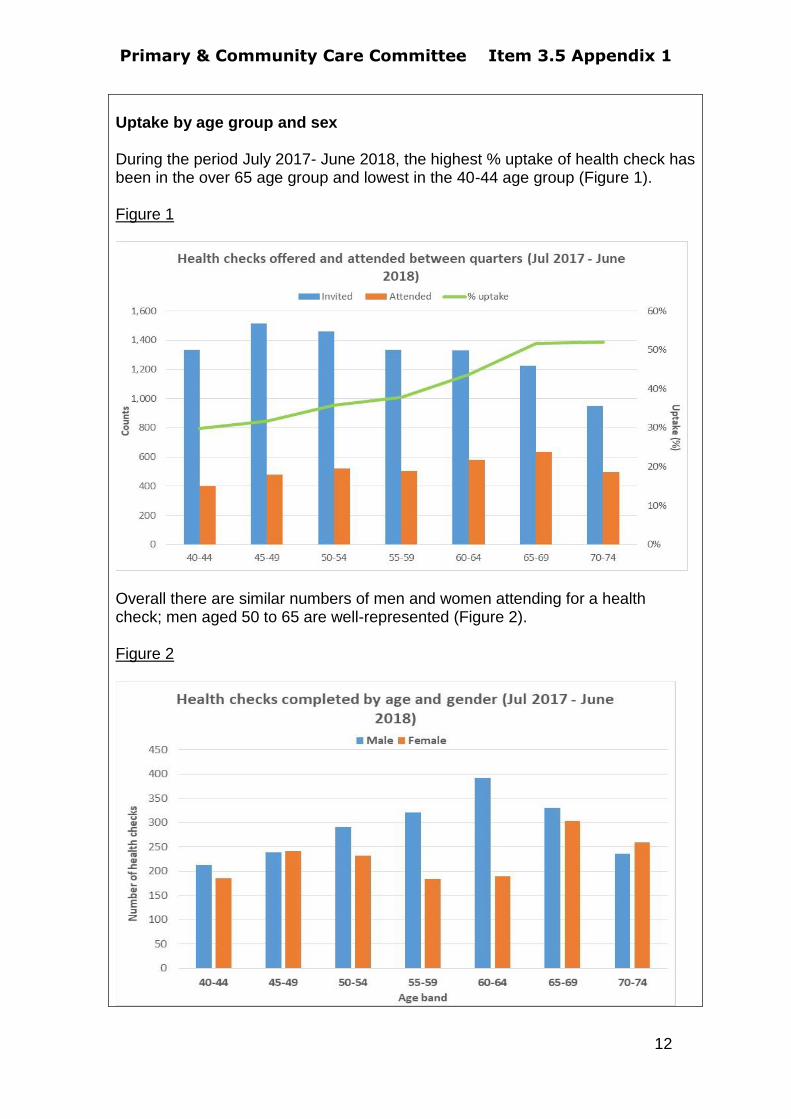
Primary & Community Care Committee Item 3.5 Appendix 1
12
Uptake by age group and sex During the period July 2017- June 2018, the highest % uptake of health check has been in the over 65 age group and lowest in the 40-44 age group (Figure 1). Figure 1
Overall there are similar numbers of men and women attending for a health check; men aged 50 to 65 are well-represented (Figure 2). Figure 2
Primary & Community Care Committee Item 3.5 Appendix 1
13
This along with other emerging data will be considered in how we target and design future delivery of the service to increase uptake in the groups which are more difficult to engage. Headlines from the local analysis The following preliminary data has been extracted from the Informatica Dashboard to support service planning, highlights from Quarter 1 (n=1178) include:
72% (844/1178) identified as obese or overweight
21% (250/1178) Identified as smokers
56% (139/250) of smokers accepted a referral to smoking cessation
services
20% (157/770) patients recorded as inactive using GP-PAQ
questionnaire were referred to National Exercise Referral scheme
50% (587/1178) had a raised cholesterol >=5mmols/L
15% (17/111) of patients found to have a high blood sugar (HbA1c) during
health check were subsequently diagnosed by their GP to have diabetes
within 3 months of health check
19% (229/1178) were recorded as having a high alcohol consumption
(AUDIT C risk tool); 3% (6/229) accepted a referral to alcohol services
3% (31/1178) had irregular pulse of which 6% (2/31) were diagnosed by
their GP with Atrial Fibrillation within 3 months of health check
27% (316/1178) were found to have a high BP ≥140/90 at health check;
4% (14/316 ) were diagnosed as having hypertension within 3 months of
health check
Uptake and outcomes data will be used to inform future developments of the Inverse Care Law programme in Cwm Taf.

Primary & Community Care Committee Item 3.5 Appendix 1
14
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
The programme lead vacancy was filled with a new manager commencing in August 2018. This will improve the delivery and strategic approach of the programme and future development. There are planning workshops in place for October to identify the future delivery model from April 2019 to which the Health Board is totally committed. There is an aspiration that the new model will provide further support to patients to reduce their risk of CVD through behaviour change. This will involve an enhanced system of linking individuals to support in their community, including social prescribing and utilisation of community assets. Long term issues with the information data dashboard have continued to be challenging and work is ongoing with NWIS and Informatica to address this. It is essential that NWIS are able to progress this work in a timely manner, particularly since the dashboard contract with Informatica expires end March 2019. In addition the licences for the healthcheck + software used in practices expire in March 2019 and NWIS support is required to advise on the best contract arrangement from April 2019 onwards which best fits the future delivery model for the Inverse Care Law programme in Cwm Taf. The evaluation report informed by SAIL data has been delayed by 3 months, which is a further challenge to planning and developing the service and measuring outcomes. We intend to report the SAIL analysis as soon as it is available and it will be included in our next report together with our proposed future delivery model.
Planned full year spend £k
Spend to date £k Forecast end year spend £k
Any difference between planned and forecast spend £k
360 120 338 22
Primary & Community Care Committee Item 3.5 Appendix 1
15
Organisation:
Cwm Taf University Health Board
Delivery Agreement name:
CWT004 Primary Care Clusters
Organisation Lead Contact:
Sarah Bradley
Primary care cluster name
Taff Ely Cluster Report
Health board
Cwm Taf University Health Board
Please give brief outline of:
1 Your top 3 intended measurable results from your investment as a whole i.e. not per each element of investment plan
Service sustainability
Improved access
More services now available in the community
2 Delivery so far against your top 3 intended measurable results
Service sustainability
The Cluster have concentrated its efforts on some key areas to ensure patients get the right messages to allow them to ‘choose well’ and ‘take care of their own health & wellbeing’, these are:
o Development of Primary Care Cluster Website – to provide a one stop shop for the population of Taff Ely and information on services, support, classes and initiatives available in the area.
o Health, wellbeing & self care - engagement with 3rd sector organisations to delivery community based sessions to allow access to art based therapies, skills development and advice and support.
o Attendance at public events to promote health & wellbeing and choose well messages e.g. Big Bite event, Public Forum.
o Active promotion of Common Ailments Scheme and Welsh Eye Care Service.
o Care navigation training – which provides frontline staff with skills to inform patients on choices and access to available services. GP practices will signpost patients to appropriate services provided by primary care, social care and 3rd sector organisation.
All GP practices continue to work with Cwm Taf University Health Board to determine roles that are needed to develop sustainable Primary Care models and Multi-disciplinary teams. o #Your local team campaign – has profiled a range of our primary care
professionals including well-being co-ordinators, pharmacists, optometrists, occupational therapists and GP support officers, who explain who they are and how they can help.
Primary & Community Care Committee Item 3.5 Appendix 1
16
Improved Access
Cluster Pharmacists are currently still in place across the practices. In addition to this a number of practices have employed pharmacists within their own teams.
Active Monitoring Programme has continued across all 8 GP practices Merthyr and the Valleys Mind provide quarterly reports for the Cluster to show access to the service, engagement and feedback from patients to demonstrate the difference this is making to patients. This also shows where individuals have been supported to manage their issues and improve their conditions, where appropriate, rather than attend for GP appointments. More recently a process has been agreed to allow the MIND practitioners to refer directly onto Primary Care Mental Health Teams when needed, rather than send this back to the GP.
More services now available in the community
The Cluster have worked with 3rd sector organisations to provide Community based sessions for identified groups or areas allowing access to community based information and support for the population of Taff Ely.
o Men and Women Sheds – the cluster have worked with ‘Shednet’ a local organisation set up to support development of sheds. This has allowed identification of groups and new activities, with work already underway to support these to become established ‘sheds’ in the area, namely:
Weekly walking rugby, football and golf sessions Gardening group and board game club Pontypridd canal group Weekly indoor bowling group Community facility and gardening ‘grow for it’
o Valley & Vale – continue to deliver art based therapy sessions to specific individuals & groups, through a joint funding arrangement. A report has been provided to the Cluster to show impact for participants. The sessions have recently moved to a new community run venue, to improve the links with an existing group who already uses the facility.
o Drink Wise Age Well 3Cs in the Community (Companionship, Conversation and Creativity) sessions have continued in Ynysybwl. This group is being supported with an aim of them become a constituted group. The aim of these sessions is to boost the confidence of older people, encourage new friendships, and find out about hobbies to help to improve their well-being.
o Hapi Project (Newydd Housing Association). Following the pilot which was developed by a GP in Parc Canol Practice and ‘Hapi’, this group have continued to meet and be supported. Hapi in partnership with the GP deliver weekly sessions on Healthy eating, cooking and physical activity. This is following identification of need by a GP in the practice as patients are presenting to her with health conditions such as diabetes, high cholesterol etc. – particularly in those considered to be obese. The next set of sessions are being delivered in partnership with Garth Olwg Lifelong Learning Centre. This will allow the Cluster to work with the Hapi Project and plan further roll out across Taff Ely.
Primary & Community Care Committee Item 3.5 Appendix 1
17
Indications are that this has had a positive impact on the participants and families – through use of questionnaires, a focus group and health checks, the Cluster can now formally evaluate this programme.
Promoting the Choose Well and Health & Wellbeing messages to the population. Existing events and forums are being used to provide information to the population around their choices when they are considering which Primary & Community Care services they need. The cluster have recently attended the annual ‘Big Bite’ event in August and a Public Forum. The Pharmacy Common Ailment Scheme and Welsh Eye Care Service are actively being promoted.
The cluster hub at Dewi Sant Health Park is now being used for community clinics, voluntary sector sessions to allow delivery and access to central cluster wide support for the population. Through joint working with Community Co-ordinator and 3rd sector organisation this will continue to develop and allow delivery of services in the community ‘hub’.
3 Any issues for delivery and how these are being managed.
Care Navigation – the plans for the Cluster are to make this training available
for all Primary Care Contractors. This has not progressed as intended to this
point as it has been difficult to engage others. Therefore it was decided to
implement phase 1 to all GP practices and the 5 Pharmacists who attended the
training. It is hoped that the pharmacies can test this process within a setting
other than the GP practice to establish how this can be implemented in other
areas of primary care. Following a 6 month review, work will progress to move
towards further roll out and moving on to phase 2.
Supporting community ‘sheds’ – release of funds to individuals or recently
established groups is proving difficult due to the procurement and financial
processes of the heatlh board. To allow individuals to set up groups, they need
to purchase equipment – funds cannot be released until these have been
purchased. Development Manager is working with finance colleagues and
‘Shednet’ to find a solution.
Primary & Community Care Committee Item 3.5 Appendix 1
18
Primary care cluster name
Rhondda Cluster
Health board
Cwm Taf University Health Board CWT005
Please give brief outline of:
1 Your top 3 intended measurable results from your investment as a whole i.e. not per each element of investment plan
service sustainability; Up Skill workforce to enhance Primary Care Team and service provision
improved access; Promote working in Rhondda and improve upon recruitment and retention
more services available in the community Introducing New Models of Care to improve upon access to services for patients.
2 Delivery so far against your top 3 intended measurable results
Parkrun practices
In an exciting and innovative initiative, the RCGP is partnering with
parkrun UK to promote the health and wellbeing of staff and patients.
Under this initiative, GP practices across the UK are encouraged to
develop close links with their local parkrun to become parkrun practices.
Involvement in this initiative will help practices:
Improve the health and wellbeing of practice staff
Improve the health and wellbeing of patients and carers, reducing the
need for lifelong medication.
Raise awareness amongst the parkrun community of services that
practices provide.
Contribute to the development of a local community and environment
that is centred around wellness generation.
Support the UK-wide movement to scale up social prescribing
activities.
All practices in the Rhondda cluster have agreed to sign up to become a
parkrun practice.
Waun Wen Lyndsey Leg Club The Lyndsay Leg Club concept is an evidence-based initiative providing community-based treatments, health promotion, health education and on-going care for people of all age groups who are experiencing leg-related problems. Leg Club staff work in a unique partnership with patients (members) and the local community. Working to best-practice guidelines the aim is to
Primary & Community Care Committee Item 3.5 Appendix 1
19
provide a very high standard of care in a social and friendly setting that promotes understanding, peer support and informed choice. The key emphasis of the Leg Club is to actively “empower members to participate in their own care, in a social environment that eases loneliness by providing congenial surroundings where old friends can meet and new friendships be formed”. Transport to and from Leg Club is arranged and provided by local community volunteers. The Lindsay Leg Club concept has four key features that are different from conventional leg ulcer clinics:
they are community-based, held in a non-medical setting, e.g. a local community centre, church hall or meeting room;
members (patients) are clinically treated collectively; they operate on a drop-in basis (no appointments required); they incorporate a fully-integrated 'well leg' regime.
The Waun Wen community Centre in Porth, Rhondda has been identified as a venue. Volunteers have been recruited and a committee has been established. In conjunction with Deputy Head of Nursing the staff to provide the service at the leg club have been identified. Ellie Lyndsay OBE has visited the Waun Wen centre and spoken to the nurses and volunteers that will be involved. The first Leg Club is scheduled to take place on the 3rd October 2018. Health & Wellbeing Hub The Treorchy Arts festival took place on the 29th of June 2018. It was an event spread over multiple venues across Treorchy and incorporated many different activities. The Rhondda Cluster organised a health and wellbeing hub over two days. Over 20 organisations that are available to the community came along to provide information on how they can support health and wellbeing and educating the public on accessing the right professionals at the right time. Numerous third sector organisations available throughout the community attended including housing, public health as well as promoting health board initiatives such as the cardiovascular risk assessment. The community pharmacist who attends the cluster meetings attended and promoted the minor ailments scheme and one of the Optometrists from within the community also attended to promote the WECS scheme. Nursing/Residential Home project The cluster undertook a pilot to rationalise the number of GP practices that visit any one nursing or residential home. By allocating the whole home to just one or two practices depending on the number of residents, the clusters aim is to improve communication between the GP and the home as they will be dealing with less GP practices and variances in systems such as ordering repeat prescriptions. The benefit for the GP will be less time away from the practice visiting numerous homes that can be situated some miles away from each other, and so increasing upon the time that can be spent in surgery seeing patients and
Primary & Community Care Committee Item 3.5 Appendix 1
20
undertaking other duties that impact on patient care. This will be particularly beneficial during the winter months when workload can increase dramatically. The community pharmacist who attends the cluster meeting also feels that the service that they provide to patients who reside within the homes will improve as they will have clearer lines of communication when dealing with fewer practices and a decrease in the number of differing prescribing systems. Each home manager has received a survey monkey 6 months after the changes were implemented. 57% of the homes involved responded
Prior to the changes being implemented, 33% had patients registered with 6 different practices, 28% had patients registered with 5 different practices, 22% registered with 4 different practices and 17% registered with 3 different practices. After the changes were implemented 67% had patients registered at one practice and 33% had patients registered at 2 different practices.
75% felt that communication with the GP practice had improved as a result of the changes, 13% felt that communication had stayed the same and 12% felt that it had deteriorated.
62% felt that the process for ordering repeat prescriptions felt there was an improvement and 38% felt it was the same, none felt that this has deteriorated since the project.
37% felt their relationship with the GP practice had improved and 63% felt it was the same, none who responded felt their relationship had deteriorated.
50% of respondents felt that the service to their residents had improved as a result of the changes implemented and 50% that the service remained the same. None felt that the service to residents had deteriorated.
Comments made in the feedback include:- “As there is the same GP’s in one surgery they have now developed a good relationship with the residents, staff and management”. “They have effectively communicated with the relatives when needed to ensure they feel a part of some difficult decisions or situations.”
“It’s is easier dealing with one surgery as opposed to many because we are familiar with their procedures and ways of working.”
“There has been discussions about ward rounds happening but nothing has happened yet. They are very responsive when a house call is requested”.
Primary & Community Care Committee Item 3.5 Appendix 1
21
Cluster Pharmacist The cluster has continued to fund the 5 cluster pharmacists currently in post and working across all 13 practices for another 12 months up until March 2019. Rhondda Primary Care Cluster Community Network Co-ordinator Based on the evaluation of the Rhondda Primary Care Cluster Community Network Co-ordinator that was presented at the cluster meeting in January 2018, the Cluster agreed to recommission the service for a further 12 month period. The Wellbeing Co-ordinator is now in every practice for one day per week over a two week period. A template has been developed to ensure that data is captured in a structured way across all practices to aid with data collection and data analysis. Grow Rhondda. Grow Rhondda is a community driven scheme in Upper Rhondda, where GPs in the area can ‘prescribe’ patients gardening activities with the goal of improving patients’ overall health and wellbeing. The gardening activities are delivered through our local Men Sheds organisation and the gardens within one of our community hospitals are used for the gardening activities. The scheme is aimed at patients who are over eighteen and experiencing social isolation/low self-esteem/mild anxiety & depression. Weekly small group sessions are held with activities centred on the maintenance, planting and harvesting of a garden that incorporates a vegetable plot through the seasons. The scheme has been in operation for 6 months and evaluation is currently being undertaken. The Slimming World on prescription referral scheme 333 vouchers were purchased ad distributed to the practices based on practice list size. The Cluster agreed on the following referral criteria:-
Aged 18 year or over
Patients identified as obese (BMI ≥35) with or without a co-morbidity that is adversely affected by their weight. Or is of a South East Asian Ethnicity
Not attended or self-funded at any weight management service in the last 3 months (I.E Slimming World, Weight Watchers, Diet Doctor, Atkins or Cambridge diet)
To date 102 referrals have been made. 42 people had completed the 12 week programme. The others are still attending.
Of the 42, 32 have achieved 3% weight loss, 24 have achieved 5% weight loss and 8 have achieved 10% weight loss.
In the last cluster meeting the referral process was reviewed. Originally only GP’s could make a referral but this has now been opened up to Practice Nurses, Health Care Support Workers and also the Cardiovascular Risk Assessment team who are working within
Primary & Community Care Committee Item 3.5 Appendix 1
22
Rhondda practices as it was felt that a cohort of patients were being missed.
Work experience week at Ysbyty Cwm Rhondda A work experience week was organised at Ysbyty Cwm Rhondda with the aim of engaging with year 10 pupils and promoting the various roles available within health. In line with the cluster work on recruitment and retention, primary care hosted a morning of the event with a GP from the cluster presenting and talking to pupils about becoming a GP and working in the Rhondda Valleys as well as representation from both community dental and community optometry.
3 Any issues for delivery and how these are being managed.
The pharmacists take up over a third of the overall cluster budget and so this
limits the funding that is available for projects. The cluster now needs to make
decisions on cluster expenditure for 2019/2020 with regard to the
pharmacists and concentrate on identifying and planning cluster initiatives in
readiness for April 2019.
Primary care cluster name
North and South CYNON Clusters
Health board
CWM TAF
Please give brief outline of:
1 Your top 3 intended measurable results from your investment as a whole i.e. not per each element of investment plan
Service sustainability The implementation of the ethos of prudent healthcare develops the workforce to ‘only do the work that only they can do’. The workplace should then become more rewarding and less pressured thus improving staff recruitment and retention rates. New models of primary care will be explored. Desired outcome is to create more cost effective and sustainable primary care services.
Improved access Improving access and increasing capacity: Exploring systems and mixed skills workforce to increase capacity and deliver appropriate services to meet patient need.
More services now available in the community Engagement with the Third Sector and other health & social care agencies. Commissioning of Cluster initiatives for service delivery.
Primary & Community Care Committee Item 3.5 Appendix 1
23
2 Delivery so far against your top 3 intended measurable results
Service sustainability Workforce Planning: both Clusters are engaged in a pilot project with Skills for Health and WEDS to inform the design of a national workforce planning tool specifically for Primary Care whilst producing two workforce plans – one for North and one for the South. These plans will provide the Clusters with sustainable workforce models which will have considered predicted population changes and local health needs. Training: there will be engagement in level 3 training for HCA’s and Diabetic foot check training which complements the Cluster Diabetic Community Clinic project in the up skilling and empowerment of clinicians in working in a specialist field thus improving confidence in and availability of care. Multi – skilled workforce: the piloting of the role of an Occupational Therapist in General Practice has been so successful that the post has been made permanent and is now working across the four Practices that make up the newly established North Cynon Cluster. The service is being expanded following the successful recruitment to Band 6 posts to further develop the model for Primary Care to ultimately replicate across the whole of Cwm Taf. The North Cynon Cluster are looking to recruit to an Advanced Nurse Practitioner position to do Nursing Home and |Home Visits. The South Cynon Cluster are looking to pilot a Health & Wellbeing Co-Ordinator post over the winter months to compare impact with their previous Community Nursing pilot 2017.18.
Improved access Cluster Pharmacists: Three full time Cluster Pharmacists are now embedded in the Practices and actively engaged in face to face patient consultations and medication reviews. The Pharmacy department is evaluating the scheme in terms of cost/benefit analysis and anecdotally from practice feedback the Pharmacists are increasing capacity for the GP’s and promoting a mixed skills model. Some independent prescribing courses have now been completed adding value to these roles. The South Cluster have committed Cluster funding to the same level of service for 2019.20. MIND active monitoring: MIND therapists are providing sessions from the practice base offering brief interventions for early presentations of anxiety and depression. Final evaluation will seek to demonstrate that the intervention has prevented the patient from re presenting to the GP with the same issue thus preventing the ‘revolving door’ pattern of attendance. The impact on other mental health service referrals will also be considered.
Primary & Community Care Committee Item 3.5 Appendix 1
24
Care Navigation: this training is being considered by the Clusters as possible investment for next year to promote prudent health care and social prescribing.
More services now available in the community Care & Repair ‘Managing Better’ project: Care & Repairs ‘boilers on prescription’ continues to be hosted by a Practice in the Cynon; the District Nurses are supporting the identification of appropriate referrals. Evaluation is being progressed in partnership with Care & Repair; initial patient feedback has been extremely positive. The engagement with Care & Repair in the Virtual Ward pilot in the North clearly evidences how multi-agency working across the sectors can assist organisations in achieving service delivery targets whilst improving outcomes for patients. Care and Repair now have representation at both Cynon Cluster meetings. Community Co-ordinators: community co-ordinators attend all Cluster meetings and regularly deliver ‘clinics’ from Practices to engage with patients to assist in health promotion initiatives and signposting. The Community co-ordinators also input into the weekly multi – disciplinary ‘virtual’ ward in North Cynon. Optometry & Dentistry: The Health Boards Optometry advisor is an active member of the Cluster meetings thus promoting a ‘Primary Care’ focus to the group. A management and clinical representative for dentistry have recently been identified and will start to attend meeting is quarter four. Community Pharmacy: there has been positive engagement this year with Community Pharmacy colleagues who now attend the Cluster meetings and have been positive about the sharing of information and potential for improving joint working.
3 Any issues for delivery and how these are being managed.
Practice capacity to manage some initiatives can be a challenge; time
needs to be invested in training and systems redesign before the
benefits of change can be evidenced. When a team is working at
capacity introducing such initiatives can prove challenging. The
outcomes of these plans are not usually evident in the short term and
the Cluster provides mutual support and encouragement to progress
initiatives in times of resistance.
Partnership initiatives with the third sector can be compromised by the
uncertainty of funding in that sector.
Projects where multi – skilled teams are central to delivery can be
jeopardised by the short supply of qualified and experienced
practitioners. Similarly the often short fixed term nature of the makes it

Primary & Community Care Committee Item 3.5 Appendix 1
25
difficult to attract the calibre of candidate required to successfully
deliver in the pilots. As a result recruitment agencies may have to be
used resulting in inflated costs and less value for money. It has proved
impossible to recruit an Advanced Nurse Practitioner or Advanced
Emergency Paramedic due to shortages of supply and short term
contracts.
The year on year structure of Cluster funding impacts on the ability of
the Cluster to plan and commission to best effect. The lack of clarity
around the future funding of initiatives where concept has been
positively proven creates uncertainty and suspicion amongst some of
the Cluster membership. Large proportions of the Cluster budget
being committed to successful projects such as the Cluster
Pharmacists seriously restricts the scope for future innovation. The
inability to ‘carry over’ funds has also prevented the recommissioning
of successful services such as the MIND interventions due to
insufficient funds in each financial term whereas a cumulative fund
would make this affordable. The consequential reduction in the MIND
contract has resulted in ineffective provision which has impacted on
the positive view of the service by the Cluster as the service has
buckled under the pressure of demand outstripping supply. This
seriously threatens the recommissioning of this service by the
Clusters.
The different priorities and culture of the Cluster Practices escalated in
the first quarter of this year resulting in the split of the Cluster into
North and South. This has facilitated improved decision making and
increased momentum.
Primary care cluster name
Merthyr Tydfil
Health board
Cwm Taf University Health Board
Please give brief outline of:
1 Your top 3 intended measurable results from your investment as a whole i.e. not per each element of investment plan
Service Sustainability Develop the workforce and introduce new models of care to enhance quality, improve wellbeing and patient experience
Improved Access Introducing new systems and expanding the MDT to increase capacity
More services available in the community
Primary & Community Care Committee Item 3.5 Appendix 1
26
Engage with Third Sector and other organisations to identify opportunities for shared working.
2 Delivery so far against your top 3 intended measurable results
General Practice Support Officers(GPSO)
This initiative has been developed in partnership with, Merthyr Cluster and Merthyr Tydfil Social Services. 6 full time GPSO’s have been recruited, all of which are embedded within GP practices within the cluster locality. The aim of this project is to change the behaviour and culture of patients who frequently visit their GP’s who do not need medical Intervention. The GPSO will engage with patients to:
Advise/assess service users and address social issues and offer support in correlation with the social services and wellbeing act.
To promote independence and enable service users to take responsibility for their own health and wellbeing.
Supporting the reduction of attendance within general practice for non-medical intervention. This includes utilising appropriate services in the locality which may include, networking with other agencies the third sector and other community resources.
Progress this quarter GPSOs are collaboratively working with third sector organisations, Public Health and Community Coordinators. Service users are being referred and signposted and some examples include:
Care and Repair - The Warm Homes on Prescription scheme, will benefit people who have health conditions which are caused or made worse by living in cold housing
NERS - The Scheme targets clients aged 16 and over who have, or are at risk of developing, a chronic disease
Multiple Intervention Assistance (MIA) - MIA is available for families in Merthyr Tydfil with children aged 0 to 18 years, who need additional multiple support services
Valleys Steps – Teaching people to manage stress, anxiety levels and low mood.
Service user’s feedback has been highly positive. A full evaluation of the project is currently being undertaken by Public Health Wales and is due to be produced in October 2018. Active Signposting - Care Co-ordinators Active Signposting offers the potential to free up GP’s consultation time each day by referring patients that do not need to see a Doctor to more appropriate healthcare professionals, within or outside of the Practice. Receptionists from all practices across the cluster have completed seven core modules of training to become a Care Coordinator:
Exceptional Customer Service
Primary & Community Care Committee Item 3.5 Appendix 1
27
Improving the Patient Experience
Succeeding with Difficult People
Managing Pressure at Work
Equality and Diversity
Understanding Information Governance
Active Signposting Course Progress this quarter Feedback continues to be positive and all practices are actively engaged as this has added value. The cluster has engaged in several Public Forums and the CHC to ensure patients are receiving the correct messages and explain the role and benefits of the care coordinator. Further work to promote the role is being undertaken.
Electronic Consultations e-Consult platform delivers better patient access and two practices in the cluster are using the service. Access to e-Consult is through each participating GP practices website. This service speeds up access to safe, efficient care, whilst at the same time reducing practices workload
Additional E Consult promotional material has been shared with all participating practices.
All participating practices are live and launched with the service.
Video presentations for Numed screens installed
Local promotion of service with patient participation groups – mother and toddler groups – CHC etc
Progress this quarter One practice has noted the success to date and anticipates a potential saving of 60-70 appointments per week in the longer term and reports 100% patient satisfaction for feedback supplied during July-September. The second practice does not feel the service has largely impacted a reduction in access and reports significantly lower numbers of appointments being saved. The two participating practices have fully engaged in promotion of the service and will both be evaluating during Q4. Cluster Physiotherapy Service Up to 30% of consultations are thought to be for MSK conditions. Merthyr Cluster physiotherapy service is now delivering 25 sessions, each week. The service is delivered in each practice and provides assessment and advice for this cohort of patients.
The service is delivered by two local providers to offer early, often same day access to a muscular skeletal specialist. The cluster feel this is proving to be instrumental in the effective use of clinical time and providing a more appropriate response to patients with muscular skeletal problems. The resource has worked extremely well across the cluster.
Primary & Community Care Committee Item 3.5 Appendix 1
28
Progress this quarter Anecdotally, professionals within each practice feel they are seeing far less patients with muscular skeletal conditions and data is currently being collated as part of the formal evaluation to take place in December 2018.
3 Any issues for delivery and how these are being managed
Recruitment of clinicians/professionals to undertake cluster initiatives
problematic – in terms of availability and cost
MSK Pathway from Cluster into the Health Board need to be improved.
At present a patient that is assessed in the Cluster service cannot be
directly referred into the Health Board service due to governance
reasons.
Ongoing management of GPSO staff could prove difficult with Local
Authority internal HR policies which is being managed via a
commissioned SLA. There have been some ‘personality clashes’ in
some of the practices between staff and GPSO which has been
challenging to manage due to the line management structure. This is
will be picked up during the evaluation and hopefully provide some
recommendations.
During quarter three the cluster will be reviewing recommendations from each
of the evaluations currently being undertaken to inform any future decisions
about the continuation of the existing projects.
2018-19 Cwm Taf Cluster allocation £’000
£1,017
Spend to date
£615
Forecast end year spend
£1,107
Primary & Community Care Committee Item 3.5 Appendix 1
29
Organisation:
Cwm Taf University Health Board
Delivery Agreement name:
CWT005 Research, Development and Service Evaluation
Organisation Lead Contact:
Professor John Geen
Outline progress with results/benefits expected by March 2019
Primary Care R&D Infrastructure Professor Chris Butler continues to provide research expertise and Clinical Practice to the UHB as part of his retainer. Research Activity Please note: data is subject to change. Data extracted from the Open Data Platform on 19.09.18.
In the first half of the year (1st April 2018 – 30th September 2018) there were 7 active & recruiting non-commercial, primary and community care studies, recruiting a total of 61 participants.
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Develop and progress the Research/ Evaluation work programme on each of the agreed themes.
Registration of each project through the appropriate approval (research / evaluation) process.
The number of patients enrolled onto research studies (commercial and non-commercial)
Increase the number of patient recruits participating in Primary care / Community related research.
The number of open research studies in Primary / Community care (commercial and non-commercial)
Increase the number of open research studies taking place within Primary / Community care.
Promote the PICRiS scheme amongst GP practices across Cwm Taf UHB.
Maintain / Increase the number of PICRiS GP practices and income from Health & Care Research Wales.
Submit applications for additional research / evaluation / innovation funding.
Successful applications submitted for research / evaluation / innovation funding in support of the programme of work.
Primary & Community Care Committee Item 3.5 Appendix 1
30
CONDUCT – Collection Devices to reduce Urine Contamination (26)
P-PLAC – The (Primary-) Prescribing Lifestyle Adjustments for Cardiovascular Health Study (13)
ABACUS 3 – Antivirals for influenza like illness? Clinical and Cost effectiveness (5)
ARTIC-PC – Antibiotics for lower Respiratory Tract Infection in Children presenting in Primary Care (1)
PRIMUS – Primary care Management of lower urinary tract symptoms in men: Development and validation of diagnostic and decision-making aid (10)
Barack-D – Benefits of Aldosterone Receptor Antagonism in Chronic Kidney Disease (6)
CLASP: Cancer: Life Affirming Survivorship support in Primary care: Internal Pilot and randomised controlled Trial (0)
The following study was active and identified patients from Primary Care and recruited by a secondary care Consultant in Endocrinology. This study has recruited a total of 823 participants.
GENTHYR – Genetics of Thyroid Replacement Therapy (823) In the first half of the year (1st April 2018 – 30th September 2018) there were 2 active & recruiting commercial, primary and community care studies, recruiting a total of 2 participants.
GSK COPD: Post-authorisation Safety (PAS) Observational Cohort Study to Quantify the Incidence and Comparative Safety of Selected Cardiovascular and Cerebrovascular Events in COPD Patients using inhaled UMEC/VI Combination or inhaled UMEC versus Tiotropium (2)
The DECIDE Study: Pragmatic Randomised 104 Week Multicentre Trial to Evaluate the Comparative Effectiveness of dapagliflozin and Standard of Care in Type 2 Diabetes (0)
The following non-commercial study has been adopted onto the research portfolio (Cwm Taf CI) and obtained full ethical approval and is due to start recruitment shortly:
Community Digital INR Self-Testing Study The following non-commercial studies are in development:
Antibiotic Myth Busting
Urgent Eye Conditions in Primary and Secondary Care (Cardiff University)
The following non-commercial studies are closed to recruitment and in follow up:
P-PLAC: The (Primary-) Prescribing Lifestyle Adjustments for Cardiovascular Health Study.
GP Ability Study - Can the introduction of rapid and automatic Ankle Brachial Pressure and Pulse Volume measuring device into General Practice identify the presence or absence of Peripheral Arterial Disease in cardiovascular risk groups?
ALICE – Antivirals for influenza like illness? Clinical and Cost effectiveness

Primary & Community Care Committee Item 3.5 Appendix 1
31
ARRISSA – At Risk Registers Integrated into primary care to Stop Asthma crises in the UK. A pragmatic cluster randomised trial with nested economic and process evaluations examining the effects of integrating at-risk asthma registers into primary care with internet based training and support
The following service evaluations are in development:
CRP testing in GP Out of Hours Services (GP)
Early Detection of Oral Cancer (Dentistry) R&D continues to send non-commercial study feasibility requests to Primary and Community Care:
“LQD study: A randomized pragmatic trial comparing the clinical and cost effectiveness of Lithium and Quetiapine augmentation in treatment resistant
Depression”
“AGE 39750: multi-country, multicentre, prospective, descriptive epidemiology cohort study on the burden of acute respiratory infection (ARI) due to respiratory
syncytial virus (RSV) during two consecutive RSV seasons in community dwelling and long-term care facilities (LTCF)/assisted living facilities adults ≥ 50 years of
age.”
“Urgent Eye Conditions in Primary and Secondary Care”
R&D continues to build partnerships with commercial companies to help increase commercial activity within Primary Care.
“INTREPID: Triple therapy treatment for COPD”
“Description and characterisation of asthmatics eligible for biologic therapy referral among primary and secondary care settings in Europe (RECOGNISE
Study)”
“Effect of semaglutide s.c. versus placebo on the progression of renal impairment in patients with type 2 diabetes and diabetic kidney disease”
“A 24-week multi-center, double-blind, placebo controlled dose-ranging study to
investigate the efficacy and safety of oral QBW251 in COPD patients on triple inhaled therapy (LABA / LAMA / ICS)”
PiCRIS The PiCRIS scheme will be promoted to GP Practices across Cwm Taf UHB over the coming months. Applications are expected to be submitted late Autumn (November) and R&D support will be provided to GP Practices to sign up to the scheme. There are currently 11 PICRiS practices across Cwm Taf UHB. Regular Primary Care Research stakeholder meetings are ongoing and in the calendar (August and November 2018).

Primary & Community Care Committee Item 3.5 Appendix 1
32
Potential New Primary Care Projects (with potential funding source): Podiatry – Plan to submit a grant by end of 2018 (RfPPB) Dentistry – Earlier Detection of oral cancer (Tenovus) Dentistry – Dental Graduate Educational Intervention (TBC) Pharmacy – Antibiotics Resistance (1000 Lives) GP – CRP Out of Hours Services (Innovate to save or RCGP – for 2019. Support being given for service evaluation in 2018 to use as preliminary data for a larger project) GP – Weight/Scales (RCGP or Kershaw Family Bursary) Health Literacy - Working with citizens to co-produce solutions for hip and knee problems by improving health literacy (TBC) Hepatitis C / Drugs of Abuse / smoking cessation – Working with GP, Population Health researcher and Prof Butler to develop study design with view to submission for grant funding. May also involve working with ex-prisoners returning to the community.
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
No issues identified to date. Constantly reviewing resource requirements to build on current Primary and Community related research activity.
Planned full year spend £k
Spend to date £k Forecast end year spend £k
Any difference between planned and forecast spend £k
97 49m 97 0
Primary & Community Care Committee Item 3.5 Appendix 1
33
Assessment of the number of practices reporting that they are experiencing workforce issues
Report on the placement of the PCSU workforce
Number of UHB directly managed practices
Evaluate PCSU workforce inputs into new developments of cluster working
Evaluate PCSU workforce inputs into core primary care sustainability
Recruitment of salaried GPs
Recruitment of nurses and
ANPs
Assessment of new roles,
outcomes and contribution to
the wider primary care team
Report on placement of
workforce and outcomes
Outline progress with results/benefits expected by March 2019
Detailed Demand and Capacity assessments have been undertaken by the Primary Care Foundation to help inform practices as to their needs in respect of allocation of workforce and resources. Salaried GPs from the PCSU are currently supporting the directly managed practices and the vitual ward model. Two new GPs have been appointed to the PCSU and will commence posts in November and December 2018. They will be placed within the Directly Managed Practices in order to form a new clinical leadership team to drive forward the practice. Positive impact still being seen from the appointment of Occupational Health and Pharmacist into the virtual ward. Detailed evaluations have been undertaken on an individual role but also the impact of the virtual ward. One further Occupational Therapist (OTs)Band 6 has been recruited and a further 2 Band 6 OTs are in the process of being appointed. Two directly managed practices will be reverting back to independent status with effect from the 1st October 2018. This will leave two directly managed practices. Currently remodelling the physiotherapist team to ensure they are responsive to Practice needs.
Organisation:
Cwm Taf University Health Board
Delivery Agreement name:
CWT006 Multi Disciplinary Development – Recruitment and Retention
Organisation Lead Contact:
Sarah Bradley
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Primary & Community Care Committee Item 3.5 Appendix 1
34
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
No significant issues to report this at this time
Planned full year spend £k
Spend to date £k
Forecast end year spend £k
Any difference between planned and forecast spend £k
662 264 624 -38
Organisation:
Cwm Taf University Health Board
Delivery Agreement name: Cluster Wound Clinics CWT007
Organisation Lead Contact: Lesley Lewis, Head of Nursing
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Measure how quickly appropriate leg ulcer treatment is initiated
No. of patients on leg ulcer assessment waiting list
Measure referral to treatment time
Patient experience
GP experience
District Nurse experience
No. of patients being seen by Practice Nurses for complex wound care
No. of ambulant patients being seen by District Nurses for complex wound care
Duration of treatment, from first appointment to healing.
Treatment to be initiated at a quicker rate than current
A reduction in patients on waiting list
Positive patient experience, informed by patient questionnaires/feedback
Positive GP Practice experience, informed by GP questionnaires/feedback
Positive DN Practice experience, informed by DN questionnaires/feedback
Reduction in complex wound care delivery by Practice Nurses
Reduction in complex wound care delivery for ambulant patients by District Nurses
An average reduction in treatment duration, from first appointment to healing.
Primary & Community Care Committee Item 3.5 Appendix 1
35
Outline progress with results/benefits expected by March 2019
Positive qualitative feedback is being received from Service Users in the form of feedback forms, compliment letters & thank you cards.
A successful roll out of the service to the Merthyr locality in KHHP on 3rd September saw 35 ambulant patients referred from the District Nursing caseloads over the last 2 weeks.
Anecdotal evidence of feedback from the District Nursing teams in this locality suggest this has had a significant positive impact on the DN teams, which enables the DNs to provide quality care to the Housebound patients.
We have been successful in securing a treatment room for an additional day in YCR to open the clinic to accommodate the increasing demand for wound care in the Rhondda Locality.
The Wound Clinic staff have been involved in the set up and are going ‘Live’ with a new Lindsay Leg Club which will be based in Waun Wen Community Centre in the Rhondda Locality, this is will initially be manned the Wound Clinic staff however going forward a rota will include the neighbouring District Nursing Teams as the club grows. Leg Clubs aim to provide lower limb management in a social environment, where members (patients) are treated collectively and the emphasis is on social interaction, participation, empathy and peer support where positive health beliefs are promoted. The Model impacts positively on healing and recurrence rates and helps isolated older people reintegrate into their communities (Lindsay, 2018). This club aims to have a positive effect on the patients within the Rhondda locality including those who attend the wound clinic.
The long term aim is for Leg Clubs to be rolled out across all other localities, to provide an equitable service to all patients within CTUHB.
Due to the raising numbers of patients upon the Wound Clinics caseload awaiting Lymphoedema appointments for hosiery and assessments, a plan was devised for Lymphoedema Specialist Nurses to attend the clinics at regular intervals to carry out and complete assessments during their clinic appointment. This has reduced patient treatment delays and reduced the waiting lists for the Lymphoedema service.
All staff have completed Lymphoedema ‘Wet Leg Pathway’ training and new staff are due to attend in October. Then patients will be assessed and managed more effectively within the wound clinic service. The Lymphoedema Specialist Nurses are also providing education and support on the allocated dates within the Wound Clinics.
A standardised feedback form for DN teams and GP Practices is still in the process of being devised and distributed through appropriate channels in order to gain robust data around DN/GP experience. However preliminary anecdotal evidence suggests these partners are happy with the Service being delivered by Cluster Wound Clinics.
The first phase of expanding the Wound Clinic to the Taff Ely locality was successfully completed and the clinic is open five days a week. We now accept referrals from four GP practices within the Taff Ely cluster and are still awaiting the final surgeries to begin referrals by the end of October.
Following on from the previous report, when looking specifically at Leg Ulcer treatment, the average length of treatment episode continues to remain significantly lower. This continues to provide an excellent example of the
Primary & Community Care Committee Item 3.5 Appendix 1
36
benefits of Cluster Wound Service staff receiving the training from the TVNs in relation to the management of Leg Ulcers, and the effective care that is being provided to patients with Leg Ulcers in the clinics.
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
The Final phase of Wound Cluster Clinic expansion involved opening a Wound Cluster Clinic in the Merthyr locality, which is based in the outpatient department in KHHP. The clinic is currently running 4 days a week and has taken over the ambulant patients from within the Merthyr Locality District Nursing Service. Rolling into the new month of October the clinic will be open 5 days per week and will be accepting Referrals direct from the Merthyr Cluster GP practices using WCCG following the introduction of a new electronic referral pathway. The development of the new referral method was reliant on NWIS and was significantly delayed.
In order to provide leg ulcer assessment and appropriate treatment of wounds within Cluster Wound Clinics, the nursing staff need to undergo an intense training package to allow this to proceed. It has been challenging to get all staff through the training package whilst maintaining the staffing of clinics and standards of care, so the achievement of this objective may be prolonged. However, a rolling rota is in place to ensure all registered nurses progress through this training and also the new HCSW’s will also attend TVN and Wound care training at a different level.
Currently six members of staff have undergone the full training by TVNs for the assessment and management of leg ulcers, with another member of staff due to commence training in the assessment process. The remaining qualified nursing staff have all completed parts of a robust competency assessment process with the TVNs and hope to complete the full competencies in the future, however this has proven difficult with part time staff and capacity issues within the clinics.
Capacity is presenting an issue across all localities given the successful roll out of the clinics and the uptake of patients. It would be beneficial to have two clinic lists across all localities, but current staffing doesn’t allow this at present.
Due to the increased referrals and limited capacity, a workforce review will be required to ensure adequate cover in all four sites. A model staffing plan will be developed in order to ensure optimal staffing levels within current budget resource.
Planned full year spend £k
Spend to date £k Forecast end year spend £k
Any difference between planned and forecast spend £k
330 130 330 -26,000
Primary & Community Care Committee Item 3.5 Appendix 1
37
Number of inappropriate readmissions from EMI Care Homes to OPMH services.
Continued minimisation of readmissions.
Availability of 7 day access to CPN support and advice for patients and carers.
Patients and carers able to access CPN support and advice when needed, 7 days per week.
Time from referral to assessment and diagnosis.
Reduced time from referral to assessment and diagnosis.
Length of stay in hospital. Reduced average length of stay
Patient, carer and staff satisfaction. Improved patient, carer and staff satisfaction at quality and timeliness of support offered.
Outline progress with results/benefits expected by March 2019
Occupancy levels within the Older Persons Mental Health wards remain constant, though there has been no need for any external transfers. Cambrian Ward closed early this financial year, and the new Health & Wellbeing Centre opened in May 2018 (a cornerstone of the Valley Life Project).
The seven days service (which runs in parallel to the Valley Life project) is a supportive service which provides a vital service to patients and carers preventing avoidable admissions. The Directorate’s long term aim of developing other seven day services to assist further continues, specifically around the Dementia Specialist Intervention Team, where it is anticipated that further improvements will be made this year.
The waiting times for OPMH are normally under 26 weeks with the significant proportion of patients still being seen under 11 weeks
The work undertaken with patients and families to ensure our service meet their needs continues. The model of individual meetings with families and carers and patients regarding the arrangements following the closure of
Organisation:
Cwm Taf UHB
Delivery Agreement name: CWT008 Older Persons Mental Health Redesign
Organisation Lead Contact: Phil Lewis
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Primary & Community Care Committee Item 3.5 Appendix 1
38
Fernhill Ward proved successful and was again utilised successfully during the closure of Cambrian Ward.
The Directorate, with the support of the Health Board, remains committed to a significant programme to support Valley Life, and both RCT and MT Local Authorities continue to contribute to our shared vision.
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
none
Planned full year spend £k
Spend to date £k Forecast end year spend £k
Any difference between planned and forecast spend £k
480 240 480 0
Shift fill rates will measured on a weekly basis with particular focus on PCH
Detailed analysis of complaints and compliments
Use of satisfaction surveys for both GPs working in the service
Use of satisfaction surveys for patients using the service
Assessment of achievement against the All Wales OOH Standards
Triangulate demand in A&E and OOHs and In Hours General Practice
Ensure that the fill rate for GP sessions is maintained and does not fall below 80%
Maintain uptake of the shift bundling package
Maintain a 2 site occupancy for the PCC
Change the skill mix within the service reducing the dependence on GP sessions
Achieve more integrated model between A&E and Out of Hours Service
Continue to undertake the 6 month review
Organisation:
Cwm Taf University Health Board
Delivery Agreement name: CWT009 Out of Hours Redesign
Organisation Lead Contact: Sarah Bradley
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Primary & Community Care Committee Item 3.5 Appendix 1
39
Continue to measure the satisfaction from the GPs working in the OOH
Continue to measure the satisfaction of patients using the service
To achieve the OOH standards set by WG
Outline progress with results/benefits expected by March 2019
Shift fill rates continue to be measured and reported on a weekly basis. The HMRC, pension issues and regional pay rate issues previously reported have impacted on the rota fill rate seeing a drop from regularly above 90% in 2017 to around 65-75% in the past 6-12 months. Further new supportive measures have been introduced in the form of the introduction of a 30 minute break after 6 hours of working. Work to expand the skill mix within the service to try and reduce the reliance on a GP workforce has been refocussed via new service model proposal which was endorsed at the September 2018 GP Out of Hours Peer Review. This new service model will be taken forward via a dedicated project over the As part of the this process the service will introducing a new Clinical Shift Lead role on weekends and bank holidays. The service will also be utilising the skills of a 111 Clinical Services Hub pharmacist commencing in the Autumn of 2018. The rota fill rate at PCH continues to be challenging. There is a renewed focus on sourcing an alternative location to deliver the OOHs service from at PCH. Complaints and compliments continue to be monitored. Complaints remain low at around 4 per month. Regular engagement meetings with the Director of Primary, Community, Mental Health, and the Clinical Lead take place with the OOHs GP workforce in order that their views are heard and they can help influence and shape the future of the service. The Clinical Lead is also in the process of establishing a new Clinical Reference Group. A Patient Satisfaction Survey is currently being undertaken and results will be published in the coming months. The service continues to report performance to WG against delivery of the WG standards for OOHs services.
Primary & Community Care Committee Item 3.5 Appendix 1
40
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
The reduction in shift fill rates over the past year is being addressed by the development of a new service redesign model which was endorsed at the recent OOHs Peer Review. The new service model has a renewed focus on improved streaming of patients and modernisation of the workforce in order to expand the skill mix within the service and build clinical capacity. This work will be taken forward via a dedicated workstream.
Planned full year spend £k
Spend to date £k Forecast end year spend £k
Any difference between planned and forecast spend £k
550 212 550 0
Training and Redevelopment
Detailed analysis of the workforce via practice development plans
Detailed analysis of the workforce via cluster development plans
Numbers of staff completing independent prescribing qualification
Numbers of new nurses entering primary care for a career
Number of practice nurses completing the ANP qualification
Number of practice reporting sustainability issues as a result of recruitment and retention problems
Training and Redevelopment
Increased capacity within primary care as more staff are able to work autonomously
Increase in the number of practice nurses completing the ANP qualification
Increase in the number of practice nurses choosing Primary Care as a career choice
Decrease in numbers of individuals reporting problems with workforce issues
Increase in the number of patients receiving medication reviews
Increase in number of HCSWs completing the core skills
Organisation:
Cwm Taf University Health Board
Delivery Agreement name: CWT010 Training and Development / Management & Leadership
Organisation Lead Contact: Sarah Bradley
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured Results / benefits planned by March 2019
Primary & Community Care Committee Item 3.5 Appendix 1
41
Increase in the numbers of staff who hold the independent prescribing qualification
framework
Increase in numbers of staff being supported in mentorship roles
Management & Leadership
Evaluation of the new initiatives commenced by the clusters
Evaluation of new initiatives/service development in primary care
Measuring the shift in resource transferred from secondary care to primary care reflecting the shift in service delivery.
Management & Leadership
Robust cluster programmes across the four Localities delivering innovative and new service development.
Robust and legitimate use of the allocated cluster funds
Positive evaluation of Personal Development Plans
Delivery against the extensive work programme including workforce plan
Positive feedback/satisfaction from independent contractors
Positive feedback from stakeholders
Measure the shift in resource from secondary to primary care
Outline progress with results/benefits expected by March 2019
Innovative cluster plans are already in place and full commitment to cluster expenditure. Evaluation report produced in respect of the cluster initiatives, e.g. GPSO, Health and Well Being Co-ordinator Assessment/evaluation has been undertaken of the new community cluster clinics in order to identify those which have provided to be cost and clinically effective. Two clinics, MSK and also Cardiology will be decommissioned in 2018 in order to support the scale up COPD and Diabetes clinic services. Appointment of clinical lead for Diabetes in order to support the additional work the Diabetes community clinic and to link with the wider strategic plans around diabetes. Dedicated experienced resource secured to provide the management and leadership to revert the Directly Managed practices back to independent status. 2 practices will transfer back to independent in October 2018. Continue to support the DSM role for various non medical staff to undertaken the independent prescribing qualification and mentorship. 4 ANP nurses appointed to commence advanced clinical practice Msc who will work across in-hours and OOH. Increase in the clinical practice educator hours in order to deliver the objectives against the HCSW education framework
Primary & Community Care Committee Item 3.5 Appendix 1
42
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
There are no significant issues to report since the last report. All the individuals are in post.
Planned full year spend £k
Spend to date £k Forecast end year spend £m
Any difference between planned and forecast spend £m
702 249 777 +75
Organisation:
Cwm Taf University Health Board
Delivery Agreement name:
CWT011 PACESETTER - Development of Advanced Training Practice / Hub & Spoke networks
Organisation Lead Contact:
Sarah Bradley
Training and Redevelopment
Detailed analysis of the workforce via practice development plans
Detailed analysis of the workforce via cluster development plans
Numbers of staff completing independent prescribing qualification
Numbers of new nurses entering primary care for a career
Number of practice nurses completing the ANP qualification
Number of practice reporting sustainability issues as a result of recruitment and retention problems
Measuring the shift in resource transferred from secondary care to primary care reflecting the shift
Training and Redevelopment
Increase in the numbers of staff within each group who train and secure roles within Cwm Taf Primary Care
Increase in the number of practice nurses completing the ANP qualification
Number of Nurses completing the first year of the Masters Advanced Clinical Skills course
Increase in numbers of pharmacists training in primary Care in Cwm Taf
Increase in numbers of pre-registration nurses training in Primary Care in Cwm Taf
Increase in number of pharmacists working in practice in Cwm Taf
FROM APPROVED DELIVERY AGREEMENT
How results / benefits are measured
Results / benefits planned by March 2019
Primary & Community Care Committee Item 3.5 Appendix 1
43
in service delivery as a result of an increase in these roles
Increase in the number of practice nurses choosing Primary Care as a career choice following qualification
Decrease in numbers of practices reporting problems with workforce recruitment and retention
Increase in the number of patients receiving appointments with the pharmacist
Increase in the numbers of staff who hold the independent prescribing qualification
Management & Leadership
Positive feedback regarding the training placements
Positive evaluation of Personal Development Plans
Delivery against the extensive work programme including workforce plan
Positive feedback/satisfaction from independent contractors
Positive feedback from stakeholders
Outline progress with results/benefits expected by March 2019
Hub has been established Engagement with practices has taken place across Cmw Taf Identification of 8 spokes and signed up to the scheme. 5 have currently signed up. 27 nursing placements to be undertaken by the end of March 2019. Establishment of practice nurse mentorship group Engagement with WG colleagues and Swansea University in respect of the positive aspects and learning which could be extended across Wales as a model Appointment of Pharmacist Educator at Band 8a Appointment of 4 ANPs to commence the Msc in Advanced Clinical Practice ANP clinical skills and competency framework established To demonstrate that this is a model which can be adopted and rollout out across Cwm Taf, Bridgend and rest of Wales
Highlight any issues which have arisen since your last report and how you have, or plan to, address these.
Primary & Community Care Committee Item 3.5 Appendix 1
44
No significant issues to report at this time.
Planned full year spend £k
Spend to date £k Forecast end year spend £k
Any difference between planned and forecast spend £k
382 43 301 -81
4.1 Primary Care Newsletter
1 4.1 Primary Care Newsletter (Welsh Government) Summer 2018 PCCC 10 October 2018.pdf
Topics this season:
A Healthier Wales
Indemnity
111
Free flu vaccinations for Wales’ care home workers
Community Pharmacy Con-tractual Framework 2018-19
Medicinal Cannabis
Expansion of medical edu-cation
Neighbourhood District Nursing pilots
Referral and Ongoing Care for Children with Suspected Diabetes
Picture of Oral Health 2018
Dental Digest Summer 2018
Funding announcements
Gender Identity Services
Wales eye care service up-lift
Liver Disease Toolkit
Primary Care Newsletter
Summer 2018
A Healthier Wales: Our plan for Health &
Social Care
Health and Social Services Secretary, Vaughan Gething, has
outlined major changes to the way NHS and social care is organised
in the future, bringing more care closer to home, with less reliance
on hospitals.
The proposals are set out in the Welsh Government’s long-term plan
for the future of health and social care in Wales, A Healthier Wales,
which focuses on providing more joined-up services, in community
settings - removing many of the current frustrations expressed by
those both using and working within the system.
In the future people will only go to a general hospital when it is
essential. The intention is to create even better care locally, with
support and treatment available across a range of community-based
services. This shift will mean that when hospital based care is
needed it can be accessed more quickly.
The changes will begin immediately, with a £100million
Transformation Fund to support the implementation of the plan. The
funding will be targeted at resources to speed up the process,
including the development of new integrated prevention services
and activities in the community.
You can read this plan here: https://gov.wales/topics/health/
publications/healthier-wales/
Health Secretary announces state-backed professional indemnity for GPs in Wales
The scheme, which is planned to come into
force from April 2019, will cover all contracted
GPs and other health professionals working in
NHS general practice.
The scheme, which was announced on 14
May will be aligned as far as possible to the
state backed scheme announced in England,
will ensure that GPs in Wales are not at a
disadvantage relative to GPs in England, and
that GP recruitment and cross border activity
will not be adversely affected by different
schemes operating in England and Wales.
Page 2
Staff working in adult residential care and
nursing homes in Wales will be eligible for free
flu vaccinations through NHS community
pharmacies from this winter, Health and Social
Services Secretary, Vaughan Gething has
announced.
NHS healthcare staff are already offered flu
vaccination by NHS employers as part of
occupational health services. Sustained, year
on year progress has been made in increasing
uptake.
The Joint Committee on Vaccination and
Immunisation (JCVI) recommends that
healthcare and social care workers receive a
flu vaccination to help protect vulnerable
patients and residents in their care, from the
effects of flu.
Last winter, to the end of March 2018, there
were 71 reported flu outbreaks in Wales, of
which 42 (60%) happened in care homes.
Studies have shown that the uptake of flu
immunisation in staff in care homes is low, and
that they have an increased risk of catching flu.
Until now, responsibility for offering flu vaccine
to social care staff has rested with individual
employers. Despite having high flu vaccination
rates in residents, flu can spread easily within
care homes and can be passed from staff to
residents when the staff member has mild or
even no symptoms. This is partly because, as
people age, they do not produce as good an
immune response to vaccination. This makes
vaccination of staff caring for frail, older people
even more important.
Free flu vaccinations for Wales’ care home workers
111 service to be rolled-out nationally
111 is a free treatment and advice service,
managed by a team of professionals, who will
treat or direct users to the right health service
for their need. The service is available 24
hours a day, seven days a week.
Currently the service is only available in the
Abertawe Bro Morgannwg Health Board and
Carmarthenshire areas, where it was launched
as a pilot in October 2016 to test the
practicalities of combining NHS Direct Wales
and the GP Out of Hours services.
The service brings together NHS Direct Wales
and GP Out-of-Hours call handling and triage
into a single service. It differs from other UK
models by having a greater proportion of
clinical staff within it.
The decision to roll out follows an independent
evaluation of the pilot. It found the service
received over 71,000 calls in the first six
months of operation, with 95% or survey
respondents saying they were satisfied or very
satisfied with the service.
Although changes cannot be wholly be
attributed to 111. The evaluation found a 1%
decrease in Emergency Department
attendance in Abertawe Bro Morgannwg
during the first six months of service. There
was also a reduction in ambulance
conveyance to Emergency Departments. This
change was mainly seen in non-urgent
conveyances – down by just over 25% during
the evaluation period.
Page 3
Community Pharmacy Contractual Framework Funding
Arrangements
2018-19
The Community Pharmacy Contractual
Framework for 2018-19 has now been finalised.
Total funding of £144.3m for 2018-19 includes
additional funding for enhanced services, the
Community Pharmacy
Quality and Safety
Collaborative Working
scheme and the
establishment of 20
Independent
Prescribing Pathfinder
sites by the end of
March 2019.
Enhanced Services
Funding to support
local commissioning of
enhanced services is
being increased initially
by £0.8m. As part of
the agreement, fees
payable for enhanced
services will be
increased in line with
any increase in NHS pay once details of any
pay deal are finalised.
Independent Prescribing Pathfinder sites
£0.2m is allocated to support health boards to
establish 20 pathfinder sites by 31 March 2019,
which utilise independent prescribing (IP) in
community pharmacy settings. Each pathfinder
site is being allocated £10,000 to meet
reasonable costs associated with establishing a
pathfinder site.
Community Pharmacy Quality and Safety
and Collaborative Working schemes
Funding available to the Community Pharmacy
Quality and Safety and Collaborative Working
schemes is being
doubled to £2.0m and
£1.0m respectively
alongside changes to
the schemes’ criteria.
Workforce
Development
Up to £0.35m is being
allocated to support
developing the
community pharmacy
workforce in 2018-19.
Funding (covering
course fees and a
contribution towards
expenses) will be
allocated to support up
to 50 community
pharmacists undertaking independent
prescriber training on courses beginning before
the end of March 2019.
Further funding will be available to encourage
up to 100 pharmacies to enter a new or existing
member of staff on an approved pharmacy
technician training programme.
If you have any queries regarding the
contractual framework for 2018-19, please
email us at [email protected]
Total funding for the Community Pharmacy
Contractual Framework of £144.3m, comprised
of the following elements:
£134.0m for dispensing and advanced
services;
£6.7m for local commissioning of enhanced
service;
£0.2m to establish 20 independent
prescribing pathfinder sites in community
pharmacies;
£2.0m for the Community Pharmacy Quality
and Safety Scheme;
£1.0m for the Collaborative Working
Scheme; and
£0.4m for workforce development
Page 4
By 2019, through collaboration between Cardiff
and Bangor Universities, arrangements are
expected to be in place for students to be able
to study all of their medical degree in north
Wales.
This will be accompanied by an immediate
expansion of medical education in Wales, with
40 new funded medical places available from
September, 20 in each of Cardiff and Swansea
medical schools. Swansea University will also
collaborate with Aberystwyth University to
increase opportunities in west Wales.
Students will undertake as much of their
studies as possible in community based
settings to reflect Welsh Government policy
that care should be delivered as close to
patients’ homes as possible.
Expansion of medical education in Wales
Medicinal cannabis
Following recent media coverage about a
family’s use of illegal cannabis oil to treat their
epileptic child, the Home Secretary
announced a two-part policy review. The UK
Chief Medical Officer led the first part - a
review of the evidence for the therapeutic
benefits of cannabis-based medicines – and
has confirmed that the evidence is
robust. Based on the findings of the evidence
review, in the second part of the policy review
the Advisory Council on the Misuse of Drugs
(ACMD) will provide ministers with an
assessment of which cannabis products, if
any, should be rescheduled under the Misuse
of Drugs Act.
At the same time, a panel of clinical experts
has been established which will assess
requests from GMC registered clinicians listed
on the relevant specialist register to use
cannabis to treat a named patient. If the
panel accepts the request, the clinician will
retain sole responsibility for his/her prescribing
decisions, and will be required to arrange
supply. Any treatment involving a cannabis
based medicinal product will continue to
require a licence as issued by the Home
Office or the Department for Health in
Northern Ireland.
New British National Formulary (BNF) app
A new British National Formulary and BNF for
Children app has been launched, providing
NHS health care professionals with the latest
content.
The new app will replace the NICE BNF app.
However, unlike the NICE app, the BNF app
does not require an Athens password or a
constant data connection.
You need to download the content update
once per month but the app can then work
offline, even with your device in airplane
mode.
The new app can be downloaded for free from
the AppStore for iOS devices, and the Google
Play store for Android devices. To learn more
please visit:
https://www.bnf.org/products/bnfbnfcapp/

Page 5
The 13 June 2018, saw the first joint workshop of the
three health board teams piloting neighbourhood
district nursing based on the Buurtzorg model. These
pilots have come about as part of the Plaid Cymru
financial compact with Welsh Government.
The three teams from Aneurin Bevan, Cwm Taf and
Powys were joined on the day by Sue Morgan,
National Director for Primary Care, Dr Sally Lewis,
National Clinical Lead for Value-Based and Prudent
Healthcare and from Welsh Government, Dr Andrew
Havers, Senior Medical Officer for Primary Care and
Paul Labourne, Nursing Officer for Primary and
Integrated Care.
The purpose of the workshop was to hear each health
board plans for taking forward a pilot of the Buurtzorg
model and also to explore ways of how the pilots could
work together. The afternoon was full of positive
discussion; a joint commitment was made by the pilots
to set up an Inter Pilot Forum. Through the forum the
pilots would take forward a joint approach to some
training activities and to measuring success and
evaluation of the pilot projects.
For further information on these pilots please contact
Paul at [email protected] or Rachel at
[email protected] who will only be too
pleased to help.
Neighbourhood District Nursing pilots
Examples of what the pilots are aiming to achieve
include:
A Population Health Focus
Caring for a designated population in line with
the District Nursing Staffing Principles.
Focussing in on sub group populations with long
term conditions within the neighbourhood for
targeted support. For example all three will
focus on palliative care, Cwm Taf have a focus
on respiratory disease, Aneurin Bevan have a
focus on frailty. This focus will look at
implementing improved and prudent skill mix to
maintaining people well within the
neighbourhood.
A Public Health Approach
Developing the neighbourhood district nursing
teams to have a public health making every
contact count approach. This may form part of
the Inter Pilot Forum actions with joint training
and development across the pilots.
A Person Centred Approach
Improving anticipatory and advanced care
planning within the neighbourhood and ensuring
this is well communicated to health and social
care colleagues including primary care, out of
hours services and WAST.
The National Paediatric Diabetes Audit reported in
July 2017 that around 23% of children with type 1
diabetes at the point of diagnosis are in diabetic
ketoacidosis (DKA). DKA requires intensive medical
intervention, is traumatising to the child and family,
and may cause long-term adverse effects on their
diabetes management. It made a number of
recommendations with regard to early diagnosis,
including awareness raising, prompt investigation
and referral.
Following the publication of the Diabetes Delivery
Plan for Wales 2016-2020; the Children and Young
People’s Diabetes Network developed a pathway
for the diagnosis of diabetes that has been
implemented in Cardiff and Vale University Health
Board. This pathway is now being shared with
health boards across Wales for local
implementation and paediatric diabetes services will
be helping to communicate the pathway in the
coming months. Any questions relating to the
pathway can be directed to the network at:
In addition, Diabetes UK Cymru has developed a
public awareness campaign highlighting the
common symptoms called “Know Type 1”, including
materials for primary care practices, which can be
found at: https://www.diabetes.org.uk/in_your_area/
wales/campaigning/know-type-1---wales.
Referral and Ongoing Care for Children with Suspected Diabetes
Page 6
The Welsh Oral Health Information Unit (Cardiff
University) report, published in partnership with
Public Health Wales, shows that the
percentage of children experiencing obvious
tooth decay has dropped significantly from
45% in 2004/05 to 30 % in 2016/17.
The Welsh Government launched the
Designed to Smile campaign in 2008/09 to
improve children’s oral health and has been
piloting a preventive approach to care in dental
practices across Wales.
Between 2004 and 2017, there have been
continued reductions in the prevalence of
dental caries across all deprivation quintiles, as
classified by the Welsh Index of Multiple
Deprivation. Despite this, the ratios of dental
caries experience for the most deprived versus
the middle deprived groups appear to be
widening albeit slightly.
The series of surveys highlight considerable
improvements in oral health amongst 12 year
olds in Wales. In 2020/21 children who
participated in Designed to Smile prior to their
first adult teeth erupting into their mouth will be
surveyed in school year 7 for the first time. The
data collected in 2020/21 will inform the
estimation of the full impact of Designed to
Smile programme on the permanent dentition.
Picture of Oral Health 2018
The summer edition of the Wales Dental Digest has been published for 2018.
The purpose of the Dental Digest is to keep practitioners informed of current issues in NHS
dentistry.
This issue includes an update on contract reform; e-Referral to Specialist Dental Services; EU
Mercury Regulations and a new Clinical Dental Lead for Healthcare Inspectorate Wales.
https://gov.wales/topics/health/professionals/dental/publication/3digest/
Dental Digest—Summer 2018
Health Secretary, Vaughan Gething, has
confirmed almost £1.7million Welsh
Government funding to re-develop Tonypandy
Health Centre.
The funding will support the merger of two GP
practices in the area to create one new
integrated health and care centre, leading to
improved services for patients.
Today’s investment will allow the Health Board
to increase the number of clinical rooms and
create secure accommodation and private
space for clinical staff and patients.
The Cabinet Secretary has also confirmed
£646,000 funding to refurbish Fishguard Health
Centre.
The funding will support the merger of
Fishguard and Goodwick surgeries, updating
the facilities at the current Fishguard GP
practice to accommodate this service change
and lead to improved services for patients.
New funding announcements
Page 7
From this autumn, people requiring gender
identity treatment will be able to access more
of their treatment in Wales.
The new Welsh Gender Team will start seeing
patients at the end of October, allowing
transgender people to access the care they
need closer to home.
Currently, all patients who present with gender
dysphoria are referred to the London Gender
Identity Clinic, where they are assessed and
provided with a treatment plan.
Patients in the Cardiff and Vale area who have
experienced difficulty in accessing the
medicines that have been recommended for
them by the London Clinic will be able to
access their prescriptions via a specialist GP
from next month. This development is targeted
towards the area of most need, with most
patients waiting for hormone replacement living
in the Cardiff area.
Work is continuing with Health Boards and the
General Practitioners Committee to develop a
fully integrated gender identity service in
Wales.
Adult gender identity services available in Wales this autumn
Welsh Government has reached
agreement with Optometry Wales
on a 1% payment uplift to
optometrists providing the Wales
Eye Care Services for 2018-19;
which include NHS sight test fees,
NHS optical voucher values,
payments for continuing education
and the training and pre-
registration supervisors grant. The
cost for these services will be
managed through the local health
boards.
After the uplift is applied,
payments for accredited Eye
Health Examination Wales
optometry practices will be:
£61.20 per Band 1
£40.80 per Band 2
£20.40 per Band 3
Wales Eye Care Service uplift
Other agreed payments include:
Accredited Low Vision Service Wales optometry practices
payments: £78.55 (rising from £77.77) for each low vision
assessment.
NHS Sight Test Fees/NHS Domiciliary Fee: the fee will remain at
the same level as 2017-18
NHS Optical Voucher Values: will remain at the same level as
2017/18.
Maximum Patient Charge within the Hospital Eye Service:
Maximum charges of £70.00 for single vision lenses and £113.80
in any other case will remain at the same level as 2017-18.
Payments for continuing education and training (CET): Payments
will be made in respect of claims made by optometrists and
ophthalmic medical practitioners relating to CET training
undertaken from 1 January to 31 December 2017. This year the
period during which optometrists and ophthalmic medical
practitioners may make their claims will be 1 July 2018 to 31
October 2018. Optometrists and OMPs can claim £550 compared
to £545 for the calendar year 2016.
Pre-registration supervisors grant: As of 1 April 2018 the
allowance paid to supervisors of pre-registration trainees will
increase to £3,549 from £3514. Claims from trainers taking on pre-
registration trainees on or after 1 April 2018 should be paid at this
new rate.
Page 8
The British Liver Trust in conjunction
with the Royal College of GPs have
developed a liver disease toolkit. The
toolkit is part of a three year
programme of work running from 2016-
2019 that aims to support GPs and
primary care professionals in
identifying and delivering care to
patients with liver disease.
Its ultimate aim is to make liver disease
prevention, detection and treatment a central part of routine healthcare amongst the UK’s
43,000 GPs, practice nurses and other team members.
Progress on the project can be found here
Resources for practitioners can be found here
The toolkit is fully endorsed by the Liver Disease Implementation Group (LDIG). Andrew
Yeoman, Clinical Lead for Liver Disease in Wales commented: “Liver disease is on the
increase and the majority of people with cirrhosis do not know they have it because there are
few, if any symptoms. Consequently the early detection of liver disease in the community is of
fundamental importance to better patient outcomes. Therefore, the GP Liver disease toolkit -
produced by the British Liver Trust in collaboration with RCGP - is a hugely welcome
development and nicely complements the existing work of the LDIG around early detection. We
therefore wholeheartedly endorse this important initiative."
The programme aims to:
Improve early detection of all types of liver disease and ensure that patients receive appropriate
intervention and treatment
Raise awareness amongst GPs, primary care nurses and patients of the key risk factors for liver
disease, including alcohol misuse, obesity, and viral hepatitis
Provide practitioners with information on interventions to reduce risk factors and therefore prevent
liver disease developing
Develop and encourage the use of clear early identification, management and treatment pathways
and common GP systems for alcohol-related liver disease, viral hepatitis and non-alcohol related fatty
liver disease with the aim of using referral to secondary care in the most effective way
Disseminate clear guidelines, toolkits, resources and learning materials to GPs and provide e-learning
and workshops
Ensure that primary care clinical coding systems provide an effective means for the recording of liver
disease to facilitate both clinical care and data retrieval for audit and research
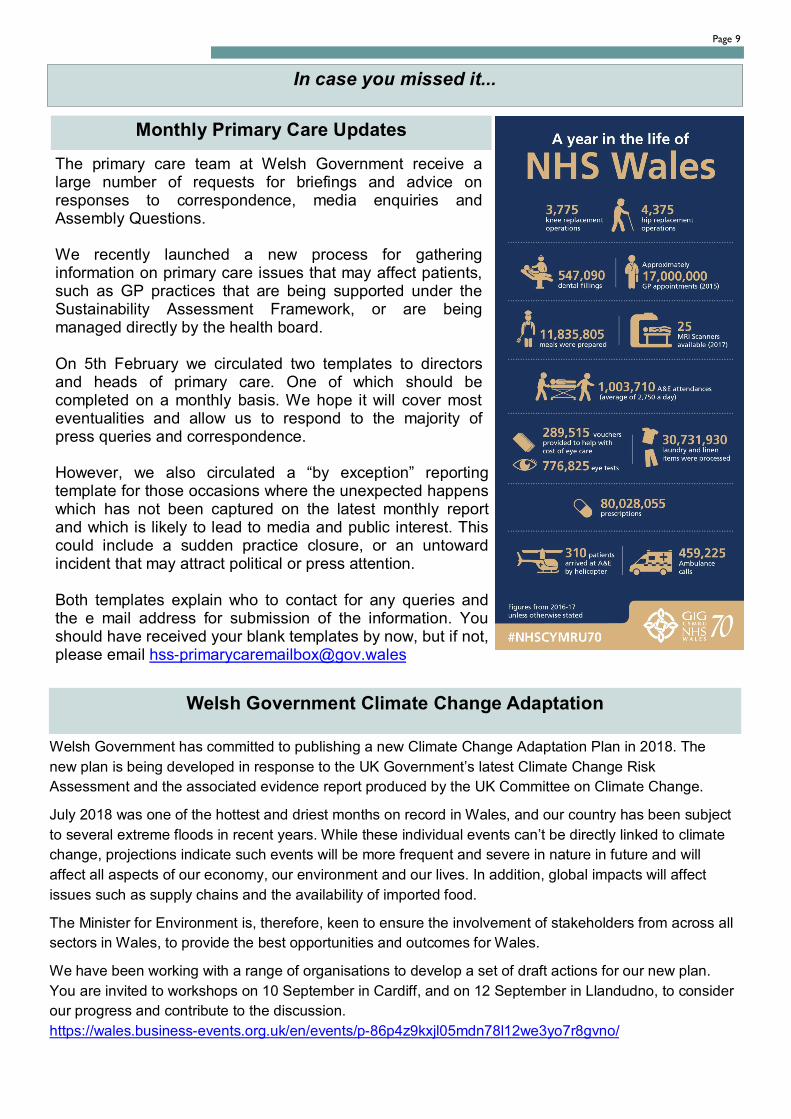
Page 9
Welsh Government Climate Change Adaptation
Welsh Government has committed to publishing a new Climate Change Adaptation Plan in 2018. The
new plan is being developed in response to the UK Government’s latest Climate Change Risk
Assessment and the associated evidence report produced by the UK Committee on Climate Change.
July 2018 was one of the hottest and driest months on record in Wales, and our country has been subject
to several extreme floods in recent years. While these individual events can’t be directly linked to climate
change, projections indicate such events will be more frequent and severe in nature in future and will
affect all aspects of our economy, our environment and our lives. In addition, global impacts will affect
issues such as supply chains and the availability of imported food.
The Minister for Environment is, therefore, keen to ensure the involvement of stakeholders from across all
sectors in Wales, to provide the best opportunities and outcomes for Wales.
We have been working with a range of organisations to develop a set of draft actions for our new plan.
You are invited to workshops on 10 September in Cardiff, and on 12 September in Llandudno, to consider
our progress and contribute to the discussion.
https://wales.business-events.org.uk/en/events/p-86p4z9kxjl05mdn78l12we3yo7r8gvno/
In case you missed it...
Monthly Primary Care Updates
The primary care team at Welsh Government receive a large number of requests for briefings and advice on responses to correspondence, media enquiries and Assembly Questions. We recently launched a new process for gathering information on primary care issues that may affect patients, such as GP practices that are being supported under the Sustainability Assessment Framework, or are being managed directly by the health board. On 5th February we circulated two templates to directors and heads of primary care. One of which should be completed on a monthly basis. We hope it will cover most eventualities and allow us to respond to the majority of press queries and correspondence. However, we also circulated a “by exception” reporting template for those occasions where the unexpected happens which has not been captured on the latest monthly report and which is likely to lead to media and public interest. This could include a sudden practice closure, or an untoward incident that may attract political or press attention. Both templates explain who to contact for any queries and the e mail address for submission of the information. You should have received your blank templates by now, but if not, please email [email protected]
4.2 IMTP Monitoring Report
1 4.2 IMTP Monitoring Report paper PCCC 10 October 2018.docx
Primary and Community Care IMTP Monitoring Report
Page 1 of 5 Primary & Community Care Committee Meeting
10 October 2018
AGENDA ITEM 4.2
10 October 2018
Primary & Community Care Committee Report
PRIMARY AND COMMUNITY CARE IMTP MONITPRING REPORT
Executive Lead: Director of Primary, Community, Children and Mental Health
Author: Mrs Alison Lagier, Locality Manager
Contact Details for further information: Lauren Morgan, 01443 443755 or
email [email protected]
Purpose of the Primary and Community Care Committee Report
The purpose of this paper is for the Primary & Community Care Committee to receive and NOTE the Monitoring Report for the Primary and Community Care
Delivery Plan, IMTP (See attached as Appendix 1).
Governance
Link to Health Board Strategic Objective(s)
The Board’s overarching role is to ensure its Strategy outlined within ‘Cwm Taf Cares’ 3 Year Integrated
Medium Term Plan 2015-2018 and the related organisational objectives aligned with the Institute of
Healthcare Improvement's (IHI) ‘Triple Aim’ are being progressed, these in summary are:
• To improve quality, safety and patient experience.
• To protect and improve population health. • To ensure that the services provided are accessible
and sustainable into the future. • To provide strong governance and assurance.
• To ensure good value based care and treatment for our patients in line with the resources made available
to the Health Board. This report supports all of the Strategic Objectives.
Supporting evidence ‘Setting the Direction’ Welsh Government
‘Our plan for primary care services in Wales’ Welsh Government 2014
Cwm Taf UHB 3yr Integrated Medium Term Plan.
Engagement – Who has been involved in this work?
Primary Care & Localities Management Team and wider directorate staff, All Primary Care CD's and Assistant Medical Director for Primary & Community
services. Primary & Community Care Committee of the Board, Clinical Engagement with Secondary Care, Locality Leadership Group (LA & 3rd sector partners), Local
Medical Committee (LMC), Acute Directorate Managers, GP Practice Managers, Executive Board, GP Cluster Leads, UHB Directors.
Primary and Community Care IMTP Monitoring Report
Page 2 of 5 Primary & Community Care Committee Meeting
10 October 2018
Primary and Community Care Committee Resolution To:
APPROVE ENDORSE DISCUSS NOTE √
Recommendation The Primary & Community Care Committee is
asked to: • NOTE the Monitoring Report for the Primary and
Community Care Delivery Plan IMTP.
Summarise the Impact of the Primary and Community Care Committee
Report
Equality and Diversity A large part of the plan attempts to address the deprivation and Inverse Care Law implications for
our population. It also recognises the specific needs of identified client groups. Specific
components of the plan will be Equality Impact Assessed as necessary and mitigating actions will
be addressed.
Legal Implications None noted to date.
Population Health The plan is based on the health needs assessment undertaken by Public Health Wales ‘A profile of
health and lifestyle in Cwm Taf – Nov 2013’ produced to support Cluster Plan development.
Quality, Safety & Patient
Experience
The plan centres on improving the quality of our
services to patients and enhancing the patient’s experience.
Resources The resources to develop the plan currently all rest within the Primary Care & Localities management
team. The key delivery actions highlighted are
already identified within the Primary Care and Localities section of the UHB 3 year Integrated
Medium Term Plan and are prioritised against the Welsh Government primary care funding.
Risks and Assurance Any potential or actual risks in relation to the plan will continue to be monitored and featured in our
risk register and will be discussed at the Primary Care Committee of the Board.
Health & Care Standards The 22 Health & Care Standards for NHS Wales are
mapped into the 7 Quality Themes: Staying Healthy Safe Care
Effective Care Dignified Care Timely Care Individual Care
Staff & Resources http://www.wales.nhs.uk/sitesplus/documents/10
64/24729_Health%20Standards%20Framework_2015_E1.pdf
The Primary & Community Care Delivery Plan reflects the related quality themes.

Primary and Community Care IMTP Monitoring Report
Page 3 of 5 Primary & Community Care Committee Meeting
10 October 2018
Workforce There are key workforce issues associated with this work in relation to demand on GP’s and practice
staff in general and also the demand on acute services. The intention is that this work will support
alternative roles and skill mix to deliver on the ever growing needs of our population. The workforce
issues outlined within the Plan are again reflected in detail within our Integrated Medium Term Plan
which should be read in conjunction with this document.
Freedom of Information
status
Open
Primary and Community Care IMTP Monitoring Report
Page 4 of 5 Primary & Community Care Committee Meeting
10 October 2018
THE PRIMARY AND COMMUNITY CARE IMTP MONITORING REPORT
1. SITUATION/PURPOSE OF REPORT
The purpose of this paper is to receive and NOTE the Monitoring Report on the
Action Plan for the Primary and Community Care Delivery Plan Integrated Medium Term Plan (IMTP). The full report is available online at:
http://cwmtaf.wales/Docs/Board_Papers/Legacy%202015-2016/15-11%20November%202015/AI%20%203%202%20Appendix%201%20Primary
%20and%20Community%20Care%20Delivery%20Plan%20UHB%204%20Nov%202015.pdf. The Monitoring Report is attached as Appendix 1
2. BACKGROUND/INTRODUCTION
In November, the 2014 Welsh Government launched ‘Our Plan for a Primary Care Service for Wales up to March 2018’, which clearly sets out the work NHS
Wales will do by March 2018 to further develop and improve Primary Care and Community Services.
Welsh Government require Health Boards to move more resources out of
hospital based care and support a clear shift of care into local communities. It is critical to ensure that there is sufficient capacity and investment in Primary
Care and Community Services to support the strengthening of prevention initiatives whilst better managing growing demand.
The development of the Integrated Medium Term Plan (IMTP) has provided the opportunity to align the planning and delivery of primary care services as an
integral part of the Health Board’s overall strategic direction. The Localities and Primary Care Team have developed a Primary Care and Community Plan with a
renewed emphasis on the changes required across the Health Care System detailing a vision for Primary Care. It is now a key feature of the Health Board’s
IMTP, along with emphasis on addressing health inequalities, strengthening prevention and building capacity and managing demand. We constantly aim to
secure and sustain progress made in the previous year, whilst refreshing our plan to reflect new national requirements, our local priorities and the desire to
‘fast track’ innovation/ modernisation and new models of delivery in Primary Care.
3. ASSESSMENT/GOVERNANCE AND RISK ISSUES
Governance The report as outlined in Appendix 1 is used by the directorate to track and
report on progress of all the key elements that are within the Primary and Community Care IMTP. The report is up-dated for each new financial year and
reflects the current priorities within the IMTP for 2018/19 along with the
refreshed Welsh Government Delivery Agreements.

Primary and Community Care IMTP Monitoring Report
Page 5 of 5 Primary & Community Care Committee Meeting
10 October 2018
This is a live document that is up-dated quarterly by the directorate and used to report progress. Any key risks are also highlighted and are then included
within our own risk register for monitoring. Key elements of the plan would also feature via designated papers to the Integrated Quality and Safety Committee
within the directorate and any other committees within the UHB as appropriate.
Overview of Red and Amber Actions
There is one RED risk identified Out of Hours /111 Sustainability. This has been identified in our directorate Risk Register. The OOH service has faced a
few challenging months in respect of the shift fill rate. There has been weekly movement with the fill rate currently averaging at 70%. We are trying to reduce
and mitigate the risks both short term and long term by looking to alternative workforce to GP’s to pick up some of the capacity needed. Doctors in training at
Specialist Training year 2 and 3 (ST2s & ST3s), advanced nurse practitioners
(ANPs) and paramedics are being used currently with other workforce being explored and training programmes developed.
There is one AMBER risks identified:
Repatriation of Community Dental Service - The action for this quarter was
to work with and receive the data collection from Cardiff and the Vale University Health Board (C&VUHB) and to ascertain intentions of the transfer of
undertakings for prior employment (TUPE) as well as scope and cost IT systems, equipment, capital and workforce implications. Much of this work is very difficult
to progress currently as despite requesting the information there is a delay in receipt of any financial information from C&VUHB. This has been escalated by
the Director.
4. RECOMMENDATION
The Primary Care Committee is asked to:
• NOTE the Monitoring Report for the Primary and Community Care IMTP
Freedom of Information status
Open
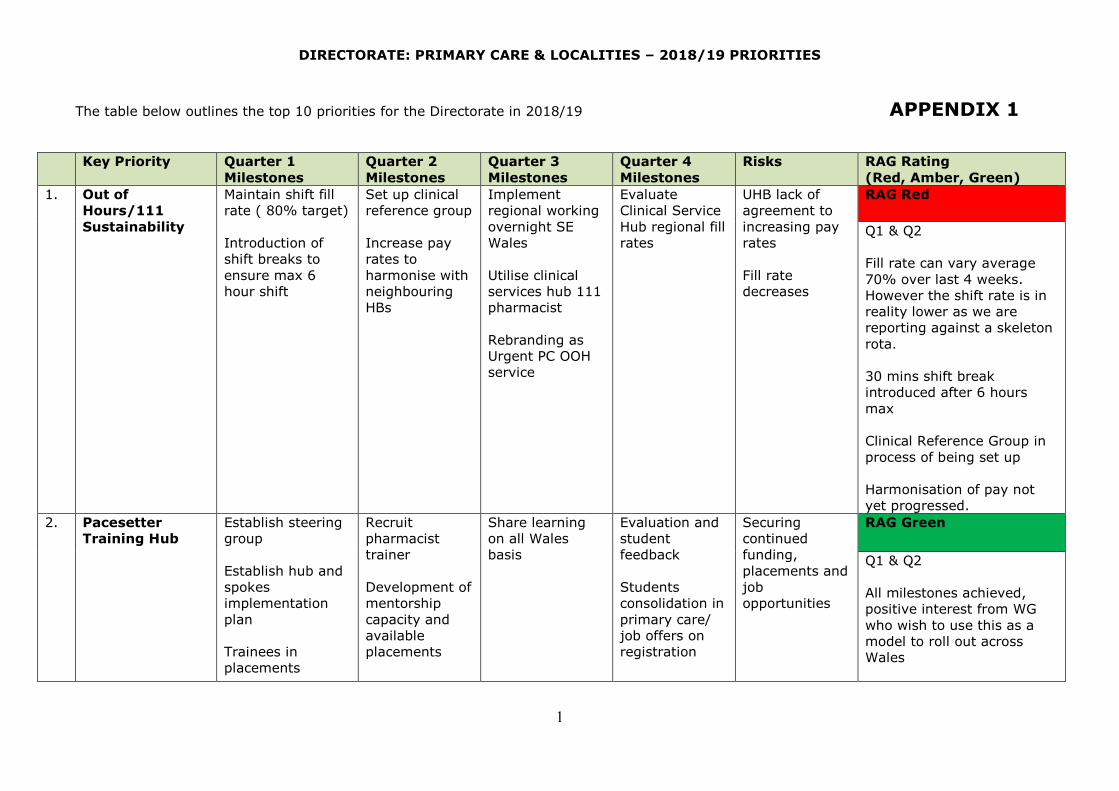
4.2.1 Appendix 1 IMTP tracker quarterly report PCCC 10 October 2018
1 4.2.1 Appendix 1 IMTP tracker quarterly report PCCC 10 October 2018.docx
DIRECTORATE: PRIMARY CARE & LOCALITIES – 2018/19 PRIORITIES
1
The table below outlines the top 10 priorities for the Directorate in 2018/19 APPENDIX 1
Key Priority Quarter 1
Milestones
Quarter 2
Milestones
Quarter 3
Milestones
Quarter 4
Milestones
Risks RAG Rating
(Red, Amber, Green)
1. Out of
Hours/111
Sustainability
Maintain shift fill
rate ( 80% target)
Introduction of
shift breaks to
ensure max 6
hour shift
Set up clinical
reference group
Increase pay
rates to
harmonise with
neighbouring
HBs
Implement
regional working
overnight SE
Wales
Utilise clinical
services hub 111
pharmacist
Rebranding as
Urgent PC OOH
service
Evaluate
Clinical Service
Hub regional fill
rates
UHB lack of
agreement to
increasing pay
rates
Fill rate
decreases
RAG Red
Q1 & Q2
Fill rate can vary average
70% over last 4 weeks.
However the shift rate is in
reality lower as we are
reporting against a skeleton
rota.
30 mins shift break
introduced after 6 hours
max
Clinical Reference Group in
process of being set up
Harmonisation of pay not
yet progressed.
2. Pacesetter
Training Hub
Establish steering
group
Establish hub and
spokes
implementation
plan
Trainees in
placements
Recruit
pharmacist
trainer
Development of
mentorship
capacity and
available
placements
Share learning
on all Wales
basis
Evaluation and
student
feedback
Students
consolidation in
primary care/
job offers on
registration
Securing
continued
funding,
placements and
job
opportunities
RAG Green
Q1 & Q2
All milestones achieved,
positive interest from WG
who wish to use this as a
model to roll out across
Wales
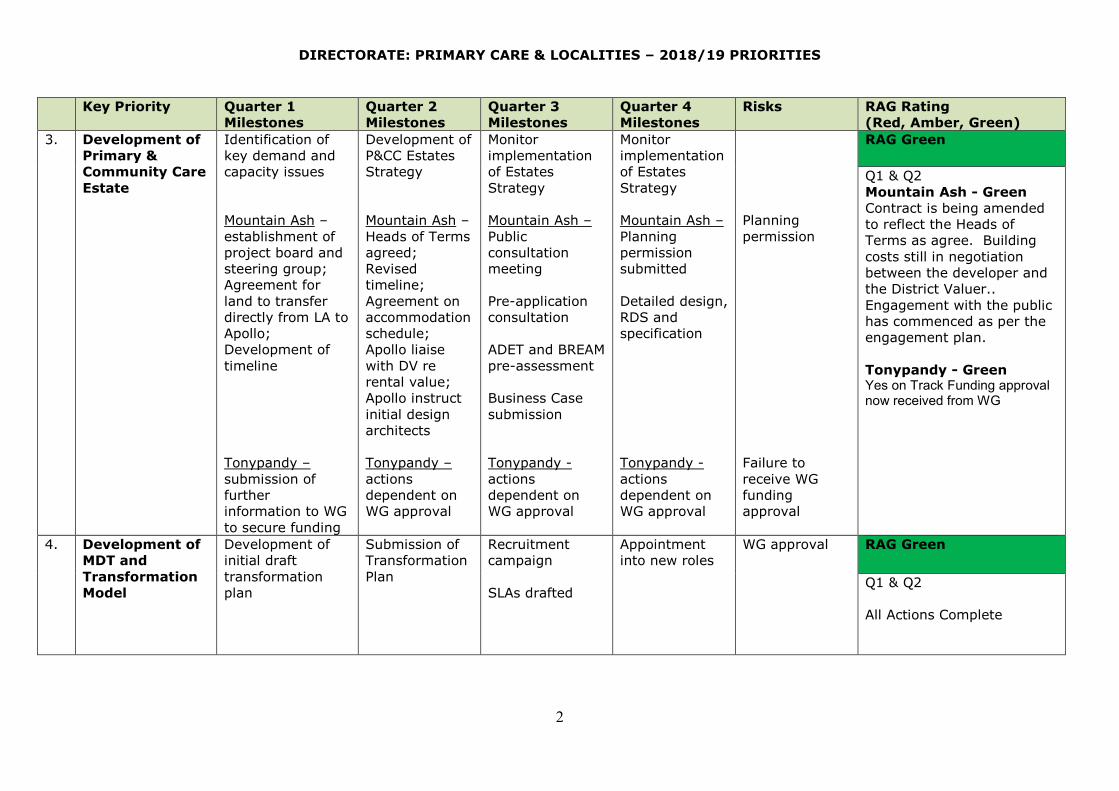
DIRECTORATE: PRIMARY CARE & LOCALITIES – 2018/19 PRIORITIES
2
Key Priority Quarter 1
Milestones
Quarter 2
Milestones
Quarter 3
Milestones
Quarter 4
Milestones
Risks RAG Rating
(Red, Amber, Green)
3. Development of
Primary &
Community Care
Estate
Identification of
key demand and
capacity issues
Mountain Ash –
establishment of
project board and
steering group;
Agreement for
land to transfer
directly from LA to
Apollo;
Development of
timeline
Tonypandy –
submission of
further
information to WG
to secure funding
Development of
P&CC Estates
Strategy
Mountain Ash –
Heads of Terms
agreed;
Revised
timeline;
Agreement on
accommodation
schedule;
Apollo liaise
with DV re
rental value;
Apollo instruct
initial design
architects
Tonypandy –
actions
dependent on
WG approval
Monitor
implementation
of Estates
Strategy
Mountain Ash –
Public
consultation
meeting
Pre-application
consultation
ADET and BREAM
pre-assessment
Business Case
submission
Tonypandy -
actions
dependent on
WG approval
Monitor
implementation
of Estates
Strategy
Mountain Ash –
Planning
permission
submitted
Detailed design,
RDS and
specification
Tonypandy -
actions
dependent on
WG approval
Planning
permission
Failure to
receive WG
funding
approval
RAG Green
Q1 & Q2
Mountain Ash - Green
Contract is being amended
to reflect the Heads of
Terms as agree. Building
costs still in negotiation
between the developer and
the District Valuer..
Engagement with the public
has commenced as per the
engagement plan.
Tonypandy - Green Yes on Track Funding approval now received from WG
4. Development of
MDT and
Transformation
Model
Development of
initial draft
transformation
plan
Submission of
Transformation
Plan
Recruitment
campaign
SLAs drafted
Appointment
into new roles
WG approval RAG Green
Q1 & Q2
All Actions Complete
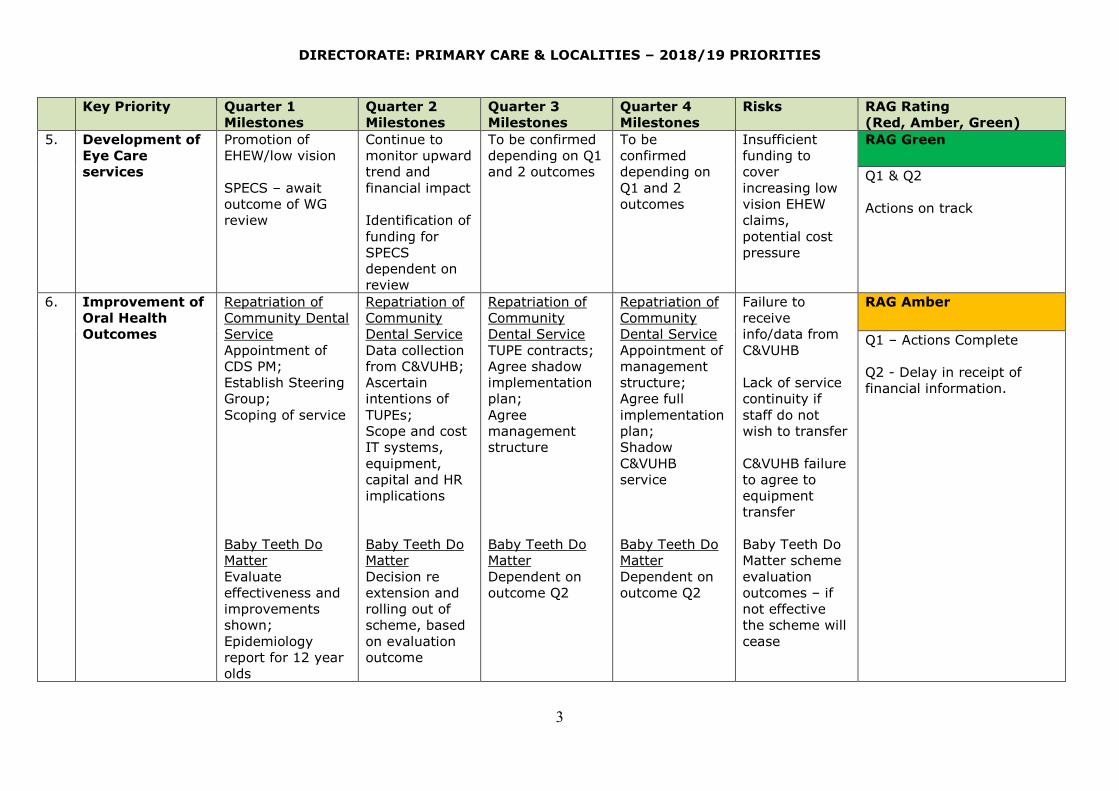
DIRECTORATE: PRIMARY CARE & LOCALITIES – 2018/19 PRIORITIES
3
Key Priority Quarter 1
Milestones
Quarter 2
Milestones
Quarter 3
Milestones
Quarter 4
Milestones
Risks RAG Rating
(Red, Amber, Green)
5. Development of
Eye Care
services
Promotion of
EHEW/low vision
SPECS – await
outcome of WG
review
Continue to
monitor upward
trend and
financial impact
Identification of
funding for
SPECS
dependent on
review
To be confirmed
depending on Q1
and 2 outcomes
To be
confirmed
depending on
Q1 and 2
outcomes
Insufficient
funding to
cover
increasing low
vision EHEW
claims,
potential cost
pressure
RAG Green
Q1 & Q2
Actions on track
6. Improvement of
Oral Health
Outcomes
Repatriation of
Community Dental
Service
Appointment of
CDS PM;
Establish Steering
Group;
Scoping of service
Baby Teeth Do
Matter
Evaluate
effectiveness and
improvements
shown;
Epidemiology
report for 12 year
olds
Repatriation of
Community
Dental Service
Data collection
from C&VUHB;
Ascertain
intentions of
TUPEs;
Scope and cost
IT systems,
equipment,
capital and HR
implications
Baby Teeth Do
Matter
Decision re
extension and
rolling out of
scheme, based
on evaluation
outcome
Repatriation of
Community
Dental Service
TUPE contracts;
Agree shadow
implementation
plan;
Agree
management
structure
Baby Teeth Do
Matter
Dependent on
outcome Q2
Repatriation of
Community
Dental Service
Appointment of
management
structure;
Agree full
implementation
plan;
Shadow
C&VUHB
service
Baby Teeth Do
Matter
Dependent on
outcome Q2
Failure to
receive
info/data from
C&VUHB
Lack of service
continuity if
staff do not
wish to transfer
C&VUHB failure
to agree to
equipment
transfer
Baby Teeth Do
Matter scheme
evaluation
outcomes – if
not effective
the scheme will
cease
RAG Amber
Q1 – Actions Complete
Q2 - Delay in receipt of
financial information.
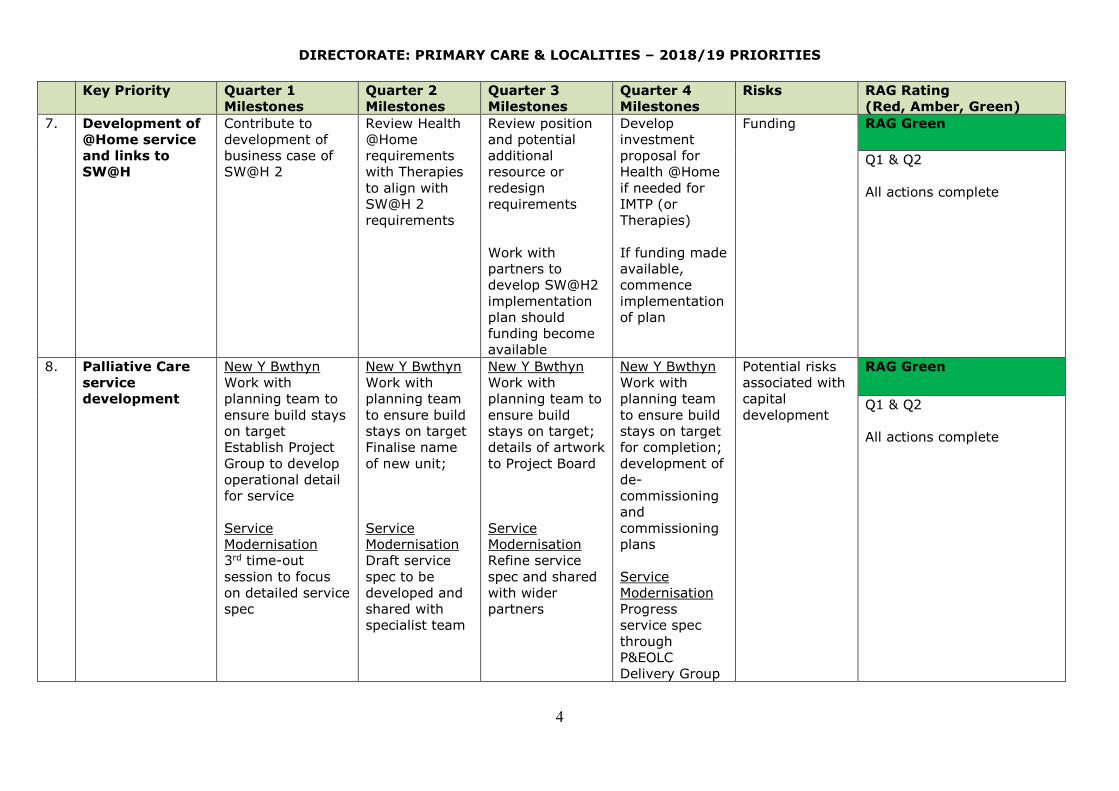
DIRECTORATE: PRIMARY CARE & LOCALITIES – 2018/19 PRIORITIES
4
Key Priority Quarter 1
Milestones
Quarter 2
Milestones
Quarter 3
Milestones
Quarter 4
Milestones
Risks RAG Rating
(Red, Amber, Green)
7. Development of
@Home service
and links to
SW@H
Contribute to
development of
business case of
SW@H 2
Review Health
@Home
requirements
with Therapies
to align with
SW@H 2
requirements
Review position
and potential
additional
resource or
redesign
requirements
Work with
partners to
develop SW@H2
implementation
plan should
funding become
available
Develop
investment
proposal for
Health @Home
if needed for
IMTP (or
Therapies)
If funding made
available,
commence
implementation
of plan
Funding RAG Green
Q1 & Q2
All actions complete
8. Palliative Care
service
development
New Y Bwthyn
Work with
planning team to
ensure build stays
on target
Establish Project
Group to develop
operational detail
for service
Service
Modernisation
3rd time-out
session to focus
on detailed service
spec
New Y Bwthyn
Work with
planning team
to ensure build
stays on target
Finalise name
of new unit;
Service
Modernisation
Draft service
spec to be
developed and
shared with
specialist team
New Y Bwthyn
Work with
planning team to
ensure build
stays on target;
details of artwork
to Project Board
Service
Modernisation
Refine service
spec and shared
with wider
partners
New Y Bwthyn
Work with
planning team
to ensure build
stays on target
for completion;
development of
de-
commissioning
and
commissioning
plans
Service
Modernisation
Progress
service spec
through
P&EOLC
Delivery Group
Potential risks
associated with
capital
development
RAG Green
Q1 & Q2
All actions complete

DIRECTORATE: PRIMARY CARE & LOCALITIES – 2018/19 PRIORITIES
5
Key Priority Quarter 1
Milestones
Quarter 2
Milestones
Quarter 3
Milestones
Quarter 4
Milestones
Risks RAG Rating
(Red, Amber, Green)
9.
Community
hospital ward
development
Development of
Steering Group
Visioning paper
Point prevalence
audit
Shared Care Model
with Mental Health
developed and I2S
proposal outlined
Shared care –
capital support for
undertaking of
scoping exercise
for environment
Fortnightly
meetings with
key partners –
acute,
community, LA
Programme
plan developed
with key
timescales
Point
prevalence to
be undertaken
across all
hospital wards
(acute and
community)
Shared Care
I2S to be
submitted (if
approved,
implementation
plan to be
developed)
Capital scoping
to be completed
Draft model to
include rehab
pathway and
proposals around
choice
Shared care – if
agreed,
implementation
plan to
commence
Shared care –
engagement with
stakeholders
Implement new
rehab pathway
and choice
protocol
Shared care -
implementation
Political and
public concern
around formal
implementation
of choice
Sustained
engagement,
agreement and
implementation
of all partners
I2S not
approved in
which case
capital spend
would be
abortive
RAG Green
Q1 & Q2
All actions completed
however the Shared Care
scheme will not be
progressed this year as
despite rigorous work this I
not an I2S it is a service
development and will
therefore be the top priority
again for mental health and
localities in the IMTP for
2019/20. This will now be
taken out of this plan
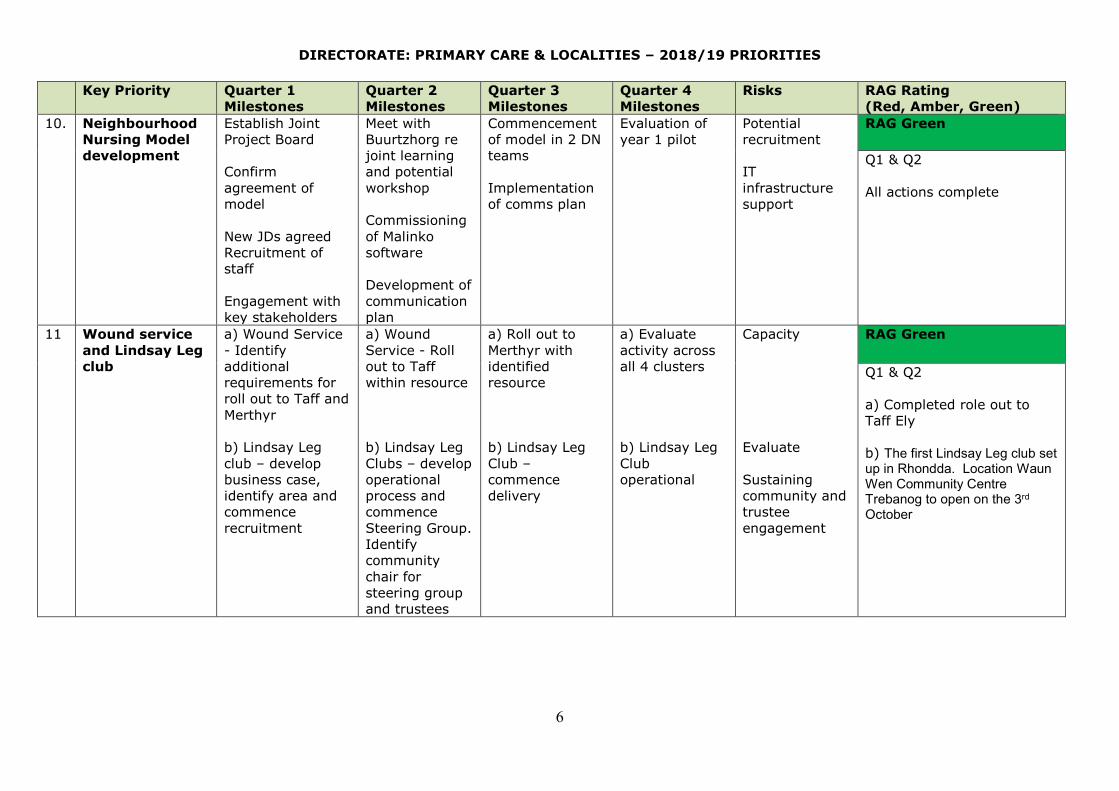
DIRECTORATE: PRIMARY CARE & LOCALITIES – 2018/19 PRIORITIES
6
Key Priority Quarter 1
Milestones
Quarter 2
Milestones
Quarter 3
Milestones
Quarter 4
Milestones
Risks RAG Rating
(Red, Amber, Green)
10.
Neighbourhood
Nursing Model
development
Establish Joint
Project Board
Confirm
agreement of
model
New JDs agreed
Recruitment of
staff
Engagement with
key stakeholders
Meet with
Buurtzhorg re
joint learning
and potential
workshop
Commissioning
of Malinko
software
Development of
communication
plan
Commencement
of model in 2 DN
teams
Implementation
of comms plan
Evaluation of
year 1 pilot
Potential
recruitment
IT
infrastructure
support
RAG Green
Q1 & Q2
All actions complete
11 Wound service
and Lindsay Leg
club
a) Wound Service
- Identify
additional
requirements for
roll out to Taff and
Merthyr
b) Lindsay Leg
club – develop
business case,
identify area and
commence
recruitment
a) Wound
Service - Roll
out to Taff
within resource
b) Lindsay Leg
Clubs – develop
operational
process and
commence
Steering Group.
Identify
community
chair for
steering group
and trustees
a) Roll out to
Merthyr with
identified
resource
b) Lindsay Leg
Club –
commence
delivery
a) Evaluate
activity across
all 4 clusters
b) Lindsay Leg
Club
operational
Capacity
Evaluate
Sustaining
community and
trustee
engagement
RAG Green
Q1 & Q2
a) Completed role out to
Taff Ely
b) The first Lindsay Leg club set up in Rhondda. Location Waun Wen Community Centre Trebanog to open on the 3rd October
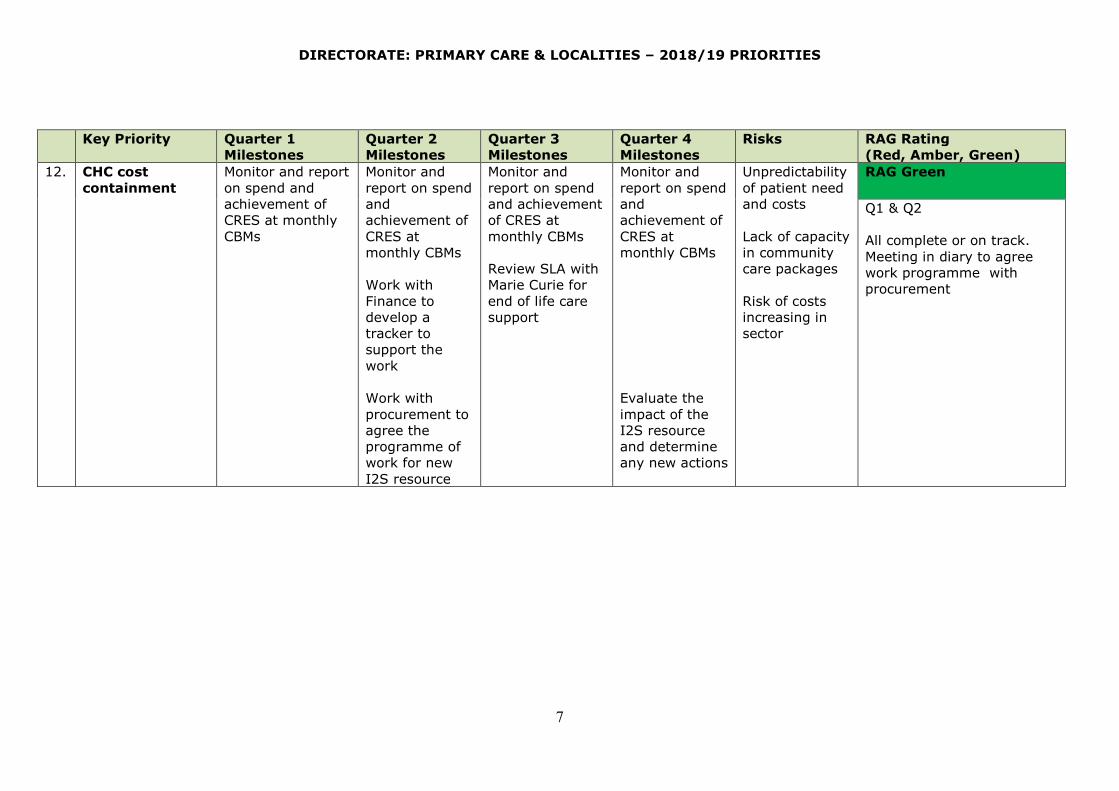
DIRECTORATE: PRIMARY CARE & LOCALITIES – 2018/19 PRIORITIES
7
Key Priority Quarter 1
Milestones
Quarter 2
Milestones
Quarter 3
Milestones
Quarter 4
Milestones
Risks RAG Rating
(Red, Amber, Green)
12. CHC cost
containment
Monitor and report
on spend and
achievement of
CRES at monthly
CBMs
Monitor and
report on spend
and
achievement of
CRES at
monthly CBMs
Work with
Finance to
develop a
tracker to
support the
work
Work with
procurement to
agree the
programme of
work for new
I2S resource
Monitor and
report on spend
and achievement
of CRES at
monthly CBMs
Review SLA with
Marie Curie for
end of life care
support
Monitor and
report on spend
and
achievement of
CRES at
monthly CBMs
Evaluate the
impact of the
I2S resource
and determine
any new actions
Unpredictability
of patient need
and costs
Lack of capacity
in community
care packages
Risk of costs
increasing in
sector
RAG Green
Q1 & Q2
All complete or on track.
Meeting in diary to agree
work programme with
procurement
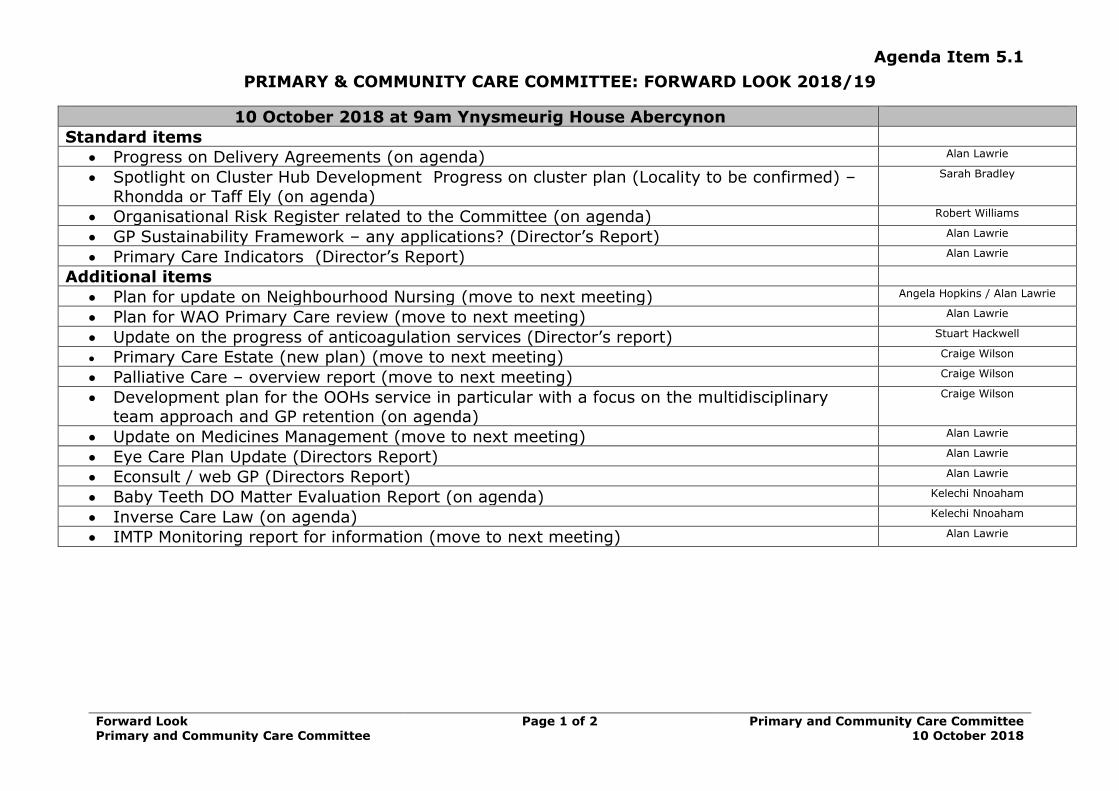
5.1 To Review the Forward Look for 2018/19
1 5.1 Forward Look PCCC 10 October 2018.doc
Agenda Item 5.1
Forward Look Primary and Community Care Committee
Page 1 of 2
Primary and Community Care Committee 10 October 2018
PRIMARY & COMMUNITY CARE COMMITTEE: FORWARD LOOK 2018/19
10 October 2018 at 9am Ynysmeurig House Abercynon
Standard items
• Progress on Delivery Agreements (on agenda) Alan Lawrie
• Spotlight on Cluster Hub Development Progress on cluster plan (Locality to be confirmed) –
Rhondda or Taff Ely (on agenda)
Sarah Bradley
• Organisational Risk Register related to the Committee (on agenda) Robert Williams
• GP Sustainability Framework – any applications? (Director’s Report) Alan Lawrie
• Primary Care Indicators (Director’s Report) Alan Lawrie
Additional items
• Plan for update on Neighbourhood Nursing (move to next meeting) Angela Hopkins / Alan Lawrie
• Plan for WAO Primary Care review (move to next meeting) Alan Lawrie
• Update on the progress of anticoagulation services (Director’s report) Stuart Hackwell
• Primary Care Estate (new plan) (move to next meeting) Craige Wilson
• Palliative Care – overview report (move to next meeting) Craige Wilson
• Development plan for the OOHs service in particular with a focus on the multidisciplinary team approach and GP retention (on agenda)
Craige Wilson
• Update on Medicines Management (move to next meeting) Alan Lawrie
• Eye Care Plan Update (Directors Report) Alan Lawrie
• Econsult / web GP (Directors Report) Alan Lawrie
• Baby Teeth DO Matter Evaluation Report (on agenda) Kelechi Nnoaham
• Inverse Care Law (on agenda) Kelechi Nnoaham
• IMTP Monitoring report for information (move to next meeting) Alan Lawrie
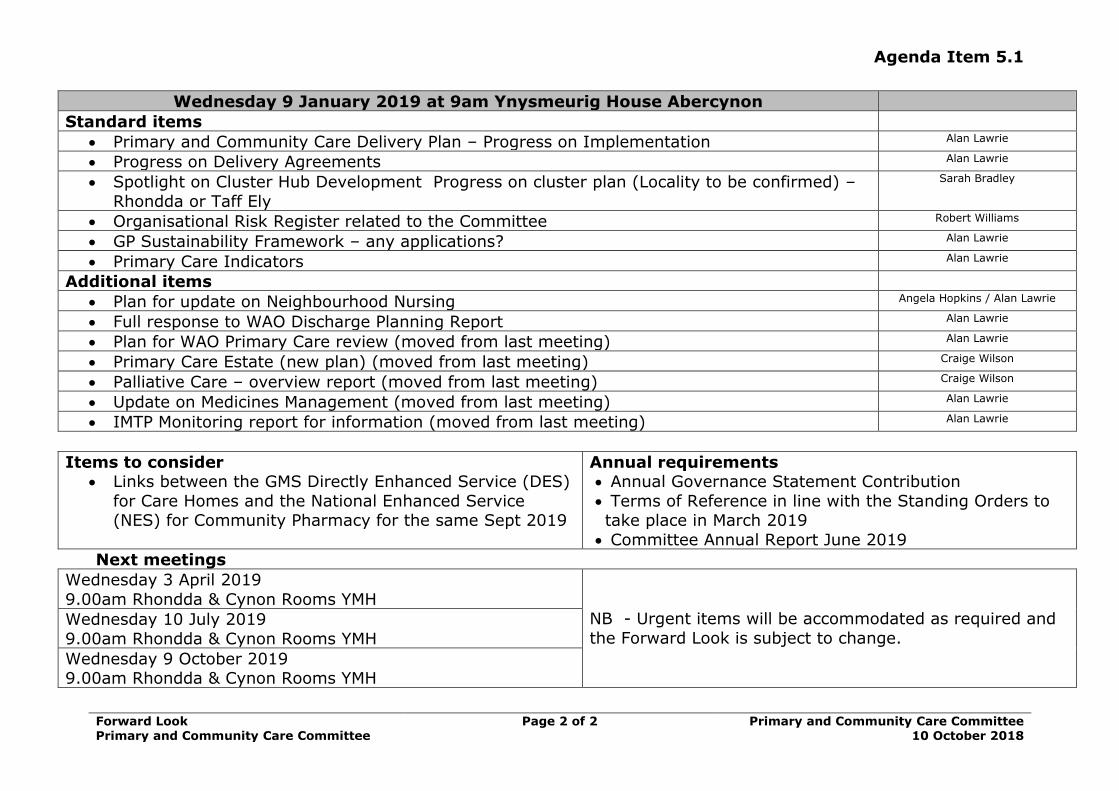
Agenda Item 5.1
Forward Look Primary and Community Care Committee
Page 2 of 2
Primary and Community Care Committee 10 October 2018
Wednesday 9 January 2019 at 9am Ynysmeurig House Abercynon
Standard items
• Primary and Community Care Delivery Plan – Progress on Implementation Alan Lawrie
• Progress on Delivery Agreements Alan Lawrie
• Spotlight on Cluster Hub Development Progress on cluster plan (Locality to be confirmed) –
Rhondda or Taff Ely
Sarah Bradley
• Organisational Risk Register related to the Committee Robert Williams
• GP Sustainability Framework – any applications? Alan Lawrie
• Primary Care Indicators Alan Lawrie
Additional items
• Plan for update on Neighbourhood Nursing Angela Hopkins / Alan Lawrie
• Full response to WAO Discharge Planning Report Alan Lawrie
• Plan for WAO Primary Care review (moved from last meeting) Alan Lawrie
• Primary Care Estate (new plan) (moved from last meeting) Craige Wilson
• Palliative Care – overview report (moved from last meeting) Craige Wilson
• Update on Medicines Management (moved from last meeting) Alan Lawrie
• IMTP Monitoring report for information (moved from last meeting) Alan Lawrie
Items to consider • Links between the GMS Directly Enhanced Service (DES)
for Care Homes and the National Enhanced Service (NES) for Community Pharmacy for the same Sept 2019
Annual requirements • Annual Governance Statement Contribution
• Terms of Reference in line with the Standing Orders to take place in March 2019
• Committee Annual Report June 2019
Next meetings
Wednesday 3 April 2019
9.00am Rhondda & Cynon Rooms YMH
NB - Urgent items will be accommodated as required and
the Forward Look is subject to change.
Wednesday 10 July 2019
9.00am Rhondda & Cynon Rooms YMH
Wednesday 9 October 2019 9.00am Rhondda & Cynon Rooms YMH