built environment affects patients' medical outcomes - minding the
TRANSCRIPT

¨

Copyright © 1998 by The Center for Health Design, Inc. All rights reserved. No part of thiswork covered by the copyright herein may be repro-duced by any means or used in any form withoutwritten permission of the publisher.
The views and methods expressed by the authors donot necessarily reflect the opinions of The Centerfor Health Design, Inc. or its Board or staff.
Published by: The Center for Health Design, Inc.
Publisher: Wayne Ruga, AIA, FIIDA
Research Consultant: Haya R. Rubin, M.D., Ph.D.Principal InvestigatorAssociate Professor of MedicineDirector, Quality of Care ResearchThe Johns Hopkins University1830 East Monument Street #8015Baltimore, MD 21205United States of AmericaTel: (410) 955-9869Fax: (410) 955-0825E-mail: [email protected]
Printer: Common Wealth Printing
Design and Composition: Visual Communications
The Center for Health Design, Inc.4550 Alhambra WayMartinez, CA 94553-4406United States of AmericaTel: (925) 370-0345Fax: (925) 228-4018E-mail: [email protected]://www.healthdesign.org
First Printing November 1998ISBN: 0-9638938-5-8Printed in the United States of America

◆ iii
VisionTo create a future where environments sup-port the highest level of human health, well-being, and achievement in all aspects of lifeand work.
ValuesAs the leaders of a global community, we encourage and support:• Organizations that demonstrate a commit-
ment to valuing the dignity of all human beings.
• Those who want to learn how to use thebuilt environment to improve human healthand well-being.
• Intentional actions that are consistent with the vision, mission, purpose, and goals ofThe Center for Health Design.
• And, as leaders, we will continuously strive toward modeling these values. In fact, weare willing to be held accountable to ourcommitment to do so.
MissionTo advance the state of life-enhancing envi-ronmental design by demonstrating the valueof design in improving health and the qualityof life.
PurposeTo advance the state of life-enhancing envi-ronmental design by:• Serving as the internationally recognized
source of high-quality educational pro-grams.
• Supporting the development of rigorous re-search that will significantly advance the artand science of health design.
• Developing and promoting the practical ap-plication of life-enhancing design.
• Developing a worldwide network of sup-portive individuals, businesses, and alliedorganizations.
• Supporting the needs and interests of net-work constituents.
• Serving as a clearinghouse for resources, in-cluding books, periodicals, articles, audio-and videotapes, project data, facility tours,and product information.
GoalsTo realize The Center’s vision by directingresources at:• Education — Increasing the awareness of
the value of design for the:° healthcare industry° design profession° general public
• Research — Causing 50% of the healthcareinstitutions in America to have incorporatedThe Center’s recommended five key designelements into their institutions and culturesby the end of 2000.
THE CENTER FOR HEALTH DESIGN, INC.


Acknowledgments vi
Introduction viii
Preface xi
1. The State of Our Knowledge 1
2. A Model: Environment and Outcomes 7
3. Establishing a Research Agenda: 17Identifying Patient Groups andEnvironmental Features for Possible Study
4. The Future Research Agenda 21
Appendix A: Literature Search 23Methods
Appendix B: Summary Table of 26Extant Studies of Effects of theHealthcare Environment on Patient Outcomes
Appendix C: Ratings of Suggestions 56for Studies of the Effect of the Built Healthcare Environment on Outcomes
Appendix D: Proposed Research Plan 80Timetable
◆ V
TABLE OF CONTENTS

vi ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
THE FOLLOWING ORGANIZATIONS havegiven their endorsement and supportto promote the work of this project.
As the subsequent phases of this project arecompleted, they will be published and distrib-uted through The Center for Health Design.
AssociationsAmerican Institute of Architects (AIA),
Academy of Architecture for HealthAmerican Institute of Architects (AIA),
Architecture for Health Committee, San Diego Chapter
American Institute of Architecture Students(AIAS)
American Society of Interior Designers (ASID)American Society of Landscape Architects
(ASLA)Architects for Health (in the UK)Architects for Health, Manchester
Metropolitan University (in the UK)Association for the Care of Children’s Health
(ACCH)Boston Society of Architects (BSA)Environmental Design Research Association
(EDRA)The Healthcare Assembly (in New England)The Healthcare ForumIlluminating Engineering Society of North
America (IES)
International Federation of Interior Architects/Designers (IFI)
International Hospital Federation (IHF)International Interior Design Association
(IIDA)Organization of Black Designers (OBD)Royal Architectural Institute of Canada
(RAIC)Sociedad Mexicana de Arquitectos
Especializadoes en Salud (SMAES)Society for the Arts in Healthcare (SAH)
Institutes and OrganizationsAmerican Architectural FoundationARCHIMED (The European Center for
Health Design)Envirosense Consortium, Inc.Institute for Family-Centered CareMedical Architecture Research Unit (MARU)
Health Buildings Research Centre (in the UK)PlanetreeTESIS (University of Florence, Italy)
Healthcare OrganizationsBoston’s Beth Israel HospitalHasbro Children’s HospitalSan Diego Children’s Hospital and Health
Center
ACKNOWLEDGMENTS

◆ vii
The Center for Health Design would like to acknowledge the following individuals andorganizations for making this research reportpossible.
Board of TrusteesRosalyn Cama, ASIDRussell C. Coile Jr., M.B.A.Susan Edgman-Levitan, P.A.D. Kirk Hamilton, FAIAC. Robert Horsburgh Jr., M.D.Kathryn E. JohnsonJain MalkinRobin Orr, MPHDerek Parker, FAIA, RIBAWayne Ruga, AIA, FIIDA,
Allied Member ASIDBlair L. SadlerRoger S. Ulrich, Ph.D.
Research CommitteeJanet R. Carpman, Ph.D.Uriel Cohen, D.Arch.D. Kirk Hamilton, FAIAC. Robert Horsburgh Jr., M.D.Paul S. Kurtin, M.D.Debra J. LevinKevin LumsdonM.P. MacDougallJain MalkinDavid ReidWayne Ruga, AIA, FIIDAMardelle McCuskey Shepley, D.Arch.S. Claudia K. StengelRoger Ulrich, Ph.D.John Zeisel, Ph.D.
SponsorsAesthetics, Inc.American Art Resources, Inc.Armstrong World Industries, Inc.Columbia/HCA Healthcare Corporation, Inc.Hewlett-PackardHill-Rom, Inc.
MilcareThe Center for Health Design, Inc.The Picker InstituteWilsonart Internationaland with funding contributed by the Interna-tional Interior Design Association, HealthcareForum, and Carnegie Fabrics to further thepursuit of quality research in the healthcaremarketplace.
Research ConsultantsPrincipal InvestigatorHaya R. Rubin, M.D., Ph.D.Associate Professor of MedicineDirector, Quality of Care ResearchThe Johns Hopkins University1830 East Monument Street #8015Baltimore, MD 21205United States of America
Research Program CoordinatorGreta Golden
Research AssistantsAmanda J. Owens, J.D.Rebeca PearsonMicah RosenbloomBenyamin Rosenbloom
AcknowledgmentsThe Center for Health Design under WayneRuga’s leadership sponsored the project, withconsistent support of scientific rigor. To allowthe report to illustrate more concretely howdesign applications could be based on scientificevidence, Kirk Hamilton contributed, pro bono,sample designs for a quieter CCU and an op-erating room providing for music duringsurgery. Peer review and comments from TheCenter for Health Design’s Research Com-mittee, specifically from Janet Carpman, UrielCohen, and Roger Ulrich, improved this re-port considerably, as did thorough editing byDavid Weber. Francine Scott, Lee Bruchey,and Chenelle E. Johnson at The Johns Hop-kins University provided excellent secretarialand administrative support.

viii ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
In a dark place the sick indulge themselves too much invarious fancies, and are harassed by imaginings devisedin an alienated mind, since no external phenomena canfall on the senses; but in a bright place they are preventedfrom being wholly in their own fancies, which are ratherweakened by external phenomena.
— Asclepiades of Bithynia, ca. 50 B.C.1
Second only to fresh air … I should be inclined to ranklight in importance for the sick. Direct sunlight, not onlydaylight, is necessary for speedy recovery … I mentionfrom experience, as quite perceptible in promoting recov-ery, the being able to see out of a window, instead of look-ing against a dead wall; the bright colours of flowers; thebeing able to read in bed by the light of the window closeto the bed-head. It is generally said the effect is upon themind. Perhaps so, but it is not less so upon the body onthat account ....
— Florence Nightingale, 18602
THROUGHOUT THE LONG history ofWestern medicine, sensitive care-givers have believed that the physi-
cal environment in which therapy is providedmay modify that therapy’s effect on patients.
In pre-Christian Rome, the influentialphysician Asclepiades of Bithynia arguedagainst the prevailing practice of sequesteringthe sick in shadowy rooms — itself based onthe notion that darkness is soothing and con-tributes to patients’ peace of mind.
From her experiences ministering to thewounded in the Crimean War, FlorenceNightingale strongly advised the British govern-ment that the convalescence of patients wouldbe hastened if hospitals were built to afford
them fresh air, sunlight, calm and quiet, views ofnature, and a setting filled with “beautiful ob-jects…especially of brilliancy of colour.”3
Surprisingly, given the ancient and honor-able lineage of this hypothesis, little modernscientific research has been conducted to testthe premise that aspects of the healthcare en-vironment (other than cleanliness) have effectson therapeutic outcomes. We know as muchfrom a major review of the medical literatureperformed in 1995 and updated in 1997 and1998 by Haya R. Rubin, M.D., Ph.D., and col-leagues from Quality of Care Research at TheJohns Hopkins University, in Baltimore, con-ducted under the auspices of The Center forHealth Design.
After culling more than 78,761 potentiallyrelevant titles from medical databases, the re-search team identified only 1,219 articles thatappeared to describe investigations into theimpact of environmental elements on health outcomes.
They had cast their net broadly, too. Theylooked for any study in which scientists had at-tempted to gauge the relationship betweenhealth outcomes and the physical environ-ment. A wide range of diverse aspects of thephysical environment were addressed, includ-ing such topics as room size, room privacy,controllability of the environment by the pa-tient, music, lighting, type of window view,humidity, and temperature.
Nevertheless, only a few dozen reports inthe medical literature since 1966 actuallyturned out to contain data that relate a partic-
INTRODUCTION

ular design feature to a specific clinical out-come for a particular study population. The 84studies judged relevant are outlined in greaterdetail in Appendix B of this report.
Unfortunately, moreover, the methodolog-ical rigor of this small volume of research var-ied enormously. Fewer than a third of thestudies, for example, were randomized, con-trolled trials — the most reliable scientifictechnique for assessing the effects of a medicalintervention or a treatment variable.
One such, as an illustration, tested the im-pact of artificial light on babies in hospitalnurseries by randomly assigning a sample of50 newborns to cribs under blue light (thehighest-intensity visible wavelength), whileanother matched sample of 50 babies wereplaced in cribs under red light (the lowest-in-tensity visible wavelength). The researchersobserved and reported in 1992 that the babiessubjected to blue light were more wakeful,slept more often but more briefly, and hadmore irregular patterns of sleep. Yet for all itsstrength of research design, a single study of100 babies — all healthy and sharing a singleethnic background — leaves open the questionof whether the same results would pertainamong babies of other ethnicities, or amongsick or premature babies, for whom regular,sound sleep may be an important factor if theyare to thrive.
Another small subset of the studies were ex-perimental trials with paired data, or observa-tional studies with paired data, both of whichare also considered by scientists to be reason-able constructs for drawing relatively reliableresearch conclusions when well crafted.
An instance of the former involved a 1975study of 19 premature infants whose incuba-tors were first set at high humidity and then atlow humidity. Eight of the infants experiencedsevere breathing problems, and the episodes ofapnea occurred in significantly greater propor-tion when the humidity was kept low. Hereagain, however, a single study of a very smallgroup of subjects is not sufficient to supportbroad generalizations even when the methodis sound. Similarly, a 1992 observational studyof nearly 14,000 patients in a state mental hos-pital indicated that when rock or rap music
was played in a common area, the patients ex-hibited more incidents of “inappropriate be-havior” than when country or “easy listening”music was played. The unusually large cohortof subjects involved lends weight to the find-ing, but the study did not control for the vari-ous rhythms or lyrics of the music that couldpossibly be provocative factors.
Indeed, none of the investigations into theeffects of environmental features on patientoutcomes undertaken in the last 30 years is im-mune to criticism. The majority are signifi-cantly flawed. To be sure, few if any scientificstudies produce incontrovertible evidence. Un-shakable judgments based on one or two trials,no matter how large or tightly controlled toeliminate chance, confounding factors, and ex-perimenter bias, are rarely if ever drawn by cir-cumspect scientists. And analysis of this bodyof research is at least suggestive that a cause-ef-fect relationship exists between some health-care environmental factors and therapeuticoutcomes for some types of patients.
Thus, one conclusion from the researchteam’s initial assessment is that research in thisfield holds promise, but that more and betterstudies are vitally needed. The effort wouldappear to be justified if nothing else on the ev-idence of the best of the studies surveyed, ahigh proportion of which did find significantassociations between the environmental vari-able investigated and a health outcome.
In an era of intense concern over the risingcosts of medical care, improving therapeuticresults through the most efficient allocation offinite resources has become the touchstone ofhealthcare practice and processes. If, in fact,the very environment in which patients re-ceive treatment has a significant influence ontheir physical responsiveness and prognosis, itis important to determine which elements canpromote more satisfactory outcomes underwhat circumstances. Healthcare facilities canthen be designed to take advantage of suchknowledge.
Continued expenditure for structures whoselayout, ambience, and appurtenances are in-formed by guess, fad, or the personal prefer-ences of designers, administrators, healthcareprofessionals, or even patients themselves —
◆ ix

x ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
absent solid efforts to square aesthetic leaningsand unsupported theories with outcomes datato the extent scientifically possible — is a frivo-lity we can no longer afford.
This report builds on an analysis of past re-search to suggest an agenda for further inquiryinto the effects of healthcare settings on patientoutcomes. It offers a general conceptual modelof the ways in which environmental featuresmay influence patients’ health, as a guide to theformulation of future research protocols. Andit provides four illustrative design applicationsof how credible scientific evidence might be in-corporated into the design of specific aspects ofthe physical environment to improve therapeu-tic results.
The research team also outlines a completeresearch program aimed at validating or dis-crediting hypotheses about the degree towhich the efficacy of healthcare can be en-hanced or diminished by key aspects of the de-signed environment.
Finally, as recommended in the first elementof this agenda, the research team conductedfocus groups to assist in the identification ofpatient populations in whom hypotheses aboutthe influences of the healthcare environmentmight be proven or disproven.
Sponsored and coordinated by The Centerfor Health Design, with funding from outsidesources and augmented by the ongoing investi-
gations of independent scientists, the comple-tion of the major research agenda outlined inthis report might at last bring to reality a fu-ture foreseen a quarter of a century ago by an-other visionary healthcare observer, notedhospital architect E. Todd Wheeler:
Eventually scientific findings will go beyond subjectiveresponses .... The doctor will then know how to write aprescription for environment even as he now does fordrugs, and technology will modify and maintain it to hisprescription, applying all beneficial variables, including… temperature; air content of solids, liquids and gases;air pressure and movement; light in all its aspects, in-cluding movement and color; other forms of radiation;ionization; size and shape of enclosure; physical move-ment of the enclosure; pattern and texture of materials;sound, both generated and absorbed; and the physicalform.4
— David O. WeberBerkeley, California, September 1996
1 From Gumpert, Christian Gottlieb, Fragments from Ascle-piades of Bithynia, Weimar, 1794, in Green, Robert M., As-clepiades: His Life and Writings (New Haven: ElizabethLicht, 1955).
2 Nightingale, Florence, Notes on Nursing: What It Is andWhat It Is Not (London: Harrison, 1960).
3 ibid.
4 Wheeler, E. Todd, Hospital Modernization and Expansion(New York: McGraw-Hill, 1971).

Introduction ◆ xi
WISE USE OF healthcare resources toimprove patient health and well-being, promote efficiency, reduce
employee turnover, and avoid wasteful spendingdictates a careful examination of the ways inwhich such an encompassing factor as the builtenvironment can affect patients’ health out-comes. If it is, in fact, an important contributorto healthcare effectiveness, it is easily manipula-ble. Without knowing which, if any, aspects ofthe physical setting make a difference, however,health facility design decisions will continue tobe made on the basis of untested propositions.Money could be saved and a greater payback re-alized if design decisions were grounded in sci-entifically valid information.
These were the premises upon which The Center for Health Design contracted inSeptember 1995 with Quality of Care Re-search at The Johns Hopkins University to de-velop a concept paper for a research masterplan that would address whether and in whatways patients’ clinical outcomes might be im-proved through designed elements of thehealthcare environment. Three tasks were in-cluded in the contract: (1) to review the litera-ture to find out what is known about the effect
of the healthcare environmental design on pa-tient health outcomes, (2) to suggest designapplications based on selected findings in theliterature, and (3) based on the literature re-view, to make initial recommendations for de-veloping a research agenda in this area for thenext 10 or more years.
Background and RationaleA revised report was published in November1997 with an expanded literature review, theaddition of 19 studies to Appendix B, and anew application on air quality.
In 1998, The Center for Health Designasked the Johns Hopkins investigators to con-tinue to update the literature review and toconduct focus groups to choose a patient pop-ulation for experimental study of how thehealthcare environment may improve patientoutcomes. This Status Report includes an ex-panded literature review including 17 newstudies in Appendix B, a new design applica-tion on sunlight and daylight, and reports ofthe focus groups conducted to help choosesubjects for study of the effects of the health-care environment on medical outcomes.
PREFACEBackground and Rationale — Improving Patient OutcomesThrough Design of the Healthcare Environment


◆ 1
THE FIRST STEP was to review the liter-ature to find out what is alreadyknown.
Framing the SearchThe healthcare environment was taken to in-clude anything that can affect a patient throughthe senses. In a brainstorming session with stafffrom The Center for Health Design, a list ofenvironmental design features was compiled.The Center’s Healthcare Design ResearchCommittee then reviewed, amplified, and re-fined the list, resulting in the selection of ele-ments included in the search keywords in Table1. More formal studies toward the definition ofthe healthcare environment would be helpful intailoring future research agendas.
In 1995, the computerized literature searchused the National Library of Medicine HealthPlanning and Administration and Medline elec-tronic databases to find any articles that con-tained data about how one or more of the listedfeatures of the healthcare environment were re-lated to any clinical patient outcome listed inTable 2. In September 1997, the Health Starand Medline databases were used to expand theoriginal search. Further details of the 1997search strategy are contained in Appendix A.Studies that addressed costs of healthcare butnot patient outcomes were excluded from theliterature survey. Studies of patients’ and clini-cians’ preferences for certain environmentalfeatures were judged to lie outside the scope ofthe project as well.
Several studies were found that investigatedthe effects of the built environment on employ-ee function or behavior. While staff morale, ef-ficiency, and job performance certainly may
contribute to patient outcomes, demonstrationof the nature and degree of the linkage underspecific circumstances requires additional workthat lies outside the scope of the project; there-fore, such studies were excluded.
The YieldTable 3 indicates results and yield of thesearch completed in 1998.
ResultsAs of September 1998, the Johns Hopkins re-viewers had examined 78,761 articles for possi-ble inclusion, as listed in Table 3. Thus far, thesearch revealed only 84 articles published in themedical and design literature in the last 30 yearsthat contain relevant data. These studies are ab-stracted and critiqued in Appendix B. Seventy-four of the studies (88 percent) demonstrated
1. THE STATE OF OUR KNOWLEDGE
TABLE 1Selected Features for the Healthcare Environment Included for Literature ReviewRoom scale Pattern of walls, furnishings, Room size artworkRoom privacy Air and ventilationRoom organization AromaEnvironmental control Noise
by patient MusicRoom flow or interactivity Temperature
(how much it permits Type of furnishingsinteractions with staff Relationship with natureand others) Equipment design
Lighting WindowsColor of walls, furnishings Type of window viewTexture or finish of walls,
furnishings

that some healthcare environmental feature wasrelated to at least one patient outcome parame-ter. Those features that were found by at leastone study to influence at least one health out-come are:
• Intensity of artificial lighting• Placement of ultraviolet lights• Temperature (this and the previous feature
were studied in premature infants)• Humidity (in premature infants, geriatric
patients, and mechanically ventilated patients)
• Ventilation system contaminants (in inten-sive care, ambulatory surgery, leukemia andbone marrow transplant patients)
• Temperature of respired air (in mechanical-ly ventilated patients)
• Tapes of music, therapeutic suggestion, andsound simulation (tapes were studied in patients undergoing coronary artery bypasssurgery, gynecologic surgery, emergencylaceration repair, or arthroscopic surgery; inchildren undergoing dental cavity prepara-tion; and in newborns)
• Type of ambient music (in psychiatric patients)
• Noise levels (in intensive care and postoper-ative patients)
• Natural window views (in patients aftercholecystectomy and in intensive care aftermajor surgery; and for neonates)
• Room exposure to sunlight (in depressed patients)
• Exposure to outdoor sunlight (elderly pa-tients in geriatric facility)
• Amount, layout, and decor of spaces for so-cial interaction, staff use, those with disabili-ties or wheelchairs, and outdoor areas (inpsychiatric and substance abuse treatmentfacility patients)
• Furniture placement (in psychiatric and rehabilitation patients)
• Room carpeting (in elderly patients)• Bedside computers (in geriatric medical and
surgical patients)• Newly built versus refurbished ward (in
geriatric patients)• Bed enclosures (in burn patients)• Privacy/openness of room or ward (in acute
medical patients and patients undergoingcataract surgery)
Critique of MethodsMany of the research studies had significantmethodological flaws that weakened the validityof their conclusions.
First, some study designs are better than oth-ers for deciding whether an environmental fea-ture matters. Table 4 describes the mostcommon study designs encountered and com-ments on their strengths and weaknesses. Ap-pendix B classifies each article according to itsstudy design.
There were 23 randomized controlled trials.This is the best way of organizing a scientificinvestigation. There were also experimentalstudies with paired data, another strong studydesign. Most of these involved premature in-fants who were examined under different incu-bator conditions.
The preponderance of articles described ob-servational studies; that is, groups of patientswho had been located in different environmentsin the course of their routine care were com-pared. In several studies, the groups of patientswere observed in different units or hospitals.This raises the concern that unspecified and un-measured differences between the two studysites were in fact responsible for the differencesreported. In these studies, most of the re-searchers also neglected to measure importantpatient characteristics that could have causeddifferent outcomes in different environments.
A few observational studies used paired datawhere patients serve as their own controls. Thisis a stronger study design because it eliminates
2 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
TABLE 2Patient Outcomes Included in Literature SearchPhysical, anatomic, or physiologic healthDiagnoses or diseasesAdverse events or complicationsPatients’ reports or evaluations of aspects of their health:
SymptomsFunctional statusWell-being
Patient evaluations of healthcareHealthcare environment

◆ 3
the concern that differences among the patientsin different groups are responsible for the vari-ance, rather than the environmental factor orfactors under investigation.
Another methodological problem cloudingthe findings in many of the extant studies is thatthe research personnel were not “blinded.”When collecting data, study staff members knewwhich type of environment patients were in.Thus, they could have been influenced uncon-sciously when judging or measuring an outcome.
Few of the studies discussed how the pa-tients included in the study may or may notresemble other patients to whom a readermight want to generalize the results. Somestudies failed to include even a minimal de-scription of the patients who had participated.Thus, it is uncertain whether the findingwould apply as well to the specific types of pa-tients a reader wants to know about.
Few studies included tests of the repro-ducibility (also called reliability) or accuracy (va-lidity) of the outcome measures used. Many ofthe studies with better methods were studies ofvarying incubator conditions for premature in-fants; there were fewer good studies of adults orchildren with other medical conditions.
Incidentally, the additional extant studiesidentified during the expansion of the initial lit-erature review, and added to the 1996 report’slist in Appendix B, were conducted with a simi-lar level of rigor and quality to those previouslyidentified.
Are Investigators Finding WhatThey’re Looking For?Methodological flaws may influence the likeli-hood that a study would find a relationship be-tween an environmental feature and a patientoutcome. This phenomenon permeates the his-tory of medical research, in which loosely con-structed experiments tend to give the answersought by the investigators. Of the studies withweaker study designs, 37 of 39, or 95 percent,concluded that the environmental feature underinvestigation affected at least one health out-come measure. However, of the 45 studies withrelatively stronger research methods — that is,randomized trials, experimental trials withpaired data, or observational studies with paireddata — 37, or 82 percent, also found positivecorrelations. This difference between the pro-
portions of studies with better and worse meth-ods that found measurable associations betweenthe environment and a clinical outcome was notof statistical significance (p > 0.075). A veryhigh proportion of studies characterized bystrong methodology also found such associa-tions. Therefore, methodological flaws proba-bly are not responsible for the preponderanceof published research studies that have foundassociations between environmental featuresand clinical outcomes.
ConclusionsThe analysis of the body of existing researchleads to three important conclusions. First, be-cause the large majority of published studiescharacterized by better research designs havefound that an environmental feature is relatedto health outcome, at least in the short term,improvements in outcomes may indeed beavailable through design interventions guidedby sound scientific inquiry.
Second, studies that contain data about theeffect of the environment on health outcomesare surprisingly scarce. The need for a broad-ened research effort in this area is striking. Manyaspects of the healthcare setting and many pa-tient populations have never been investigated.
Third, many published studies have signifi-cant methodological flaws that render theirconclusions suspect or cast doubt on the gener-alizability of their findings. Future research intothe effects of the healthcare environment onpatient outcomes should be more carefully de-signed and performed with greater method-ological rigor. In particular, researchers shouldmake strong efforts to ensure that groups of pa-tients being compared under varied environ-mental conditions do not differ in other waysthat may skew the results.
TABLE 3Literature Search YieldDatabase Total Possibly Met Inclusion
ID’d Relevant Criteria
Health planning (1966–9/1995) 8,087 177 17Health Star (1975–9/1998) 21,748 170 5Medline Ovid (1966–9/1998) 48,800 831 52References from articles 126 41 10Total 78,761 1,219 84

4 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
STUDY DESIGN
Randomized controlled trialType code: 1
Type code: 1b
Experimental trial with paired dataType code: 2
Type code: 2b
DESCRIPTION, STRENGTHS ANDWEAKNESSES, SIMILAR ALTERNATIVES
Description: Patients are assigned in random orderto conditions with and without a certain environ-mental feature.
Strength: Excellent for drawing conclusionsabout whether that feature really matters.
Weakness: It is often difficult to assign environ-mental conditions randomly.
Similar alternative: Consecutive or apparentlyunbiased systematic assignment of subjects toconditions with or without a certain environ-mental feature. Random assignment is alwayspreferable to avoid unintended bias.
Description: The same patients are assigned todifferent environmental conditions at differenttimes, under the direction of investigators. Eachpatient serves as his or her own control forcomparisons.
Strength: Excellent for concluding if an envi-ronmental feature matters. Conclusions arestronger if patients are randomly assigned to re-ceive one or the other condition first
Weakness: It is not always possible to treat thesame patient under different conditions.
Similar alternative: Experimental trial using thesame group of patients with unpaired dataanalysis. The same patients are assigned to dif-ferent conditions at different times, but only theaverage results for the entire group are com-pared under different conditions, rather thanexamining each subject as his own control.Paired data analysis is always both possible andpreferable.
TABLE 4
Research Study Designs: Encountered in the Literature Survey

◆ 5
STUDY DESIGN
Observational study with paired dataType code: 3
Type code: 3b
Observational study of different groupsType code: 4
Type code: 4b
DESCRIPTION, STRENGTHS ANDWEAKNESSES, SIMILAR ALTERNATIVES
Description: The same patients are observed underdifferent environmental conditions in the course ofroutine care. The environmental conditions are notcontrolled by the observers but are those that occur nat-urally. Each patient serves as his own control.
Strength: A sound study design for drawing con-clusions, although somewhat weaker than an ex-perimental trial with paired data.
Weakness: Because the study does not assign andcontrol the environmental conditions, other as-pects of the setting could differ besides the en-vironmental feature of interest.
Similar alternative: Observational study usingthe same patients but with unpaired data analy-sis. The same patients are assigned to differentconditions at different times, but only the aver-age results for the entire group are comparedunder different conditions, rather than examin-ing each subject as his own control. Paired dataanalysis is always both possible and preferable.
Description: Groups of patients are compared indifferent environments in the course of routinecare. If performed in sequential time periods,perhaps before and after a design change orpolicy change, such studies are referred to as“natural history” studies.
Strength: Easiest to organize. Study can be maderelatively stronger by identifying and measuringall differences among groups that influence pa-tient outcomes and analyzing possible effects onresults.
Weakness: Because there may be too many otherdifferences among the groups of patients to ac-count for them comprehensively and accurately,this is the weakest study design.
Similar alternative: Experimental trial assigning dif-ferent patients nonrandomly and in a possibly bi-ased fashion to different environmental conditions.
TABLE 4, cont.
Research Study Designs: Encountered in the Literature Survey


◆ 7
AWORKING THEORY of what affects pa-tients’ health outcomes is necessaryfor interpreting the results of the re-
search on the influence of the physical envi-ronment. Such a hypothetical grounding isalso helpful when considering which studiesmight contribute most in the future.
One model includes the following factorsand their interactions that determine clinicaloutcomes for patients: (1) the medical treat-ment provided, including technical and inter-personal aspects; (2) patients’ personalcharacteristics, such as age, sex, and relevantphysical, physiological, and emotional traits:For example, a patient in good physical shapemay recover more quickly from surgery thanone who is out of shape; (3) illness factors,such as stage or etiology: For example, all elsebeing equal, a patient with metastatic cancer islikely to have a worse outcome than one withan asthma attack; and (4) features of the physi-cal environment.
The Environment-Outcome InterfaceWith this model in mind, how can aspects ofthe designed environment interrelate withmedical care, illness, and patients’ attributes toinfluence patients’ health? The healthcare set-ting may either magnify or diminish the ef-fects of medical intervention, personalcharacteristics, and causes of illness to influ-ence the ultimate therapeutic outcome. Figure1 illustrates this concept schematically.
• The designed environment can support or hindercaregiver actions and medical interventions,making it harder or easier for clinicians todo their jobs, and facilitating helpful actionsor preventing harmful ones. For example,the call bell enables patients to summonnurses or doctors to the bedside when emer-gency assistance is needed, and carpeting re-duces the hubbub of clinical personnelgoing about their business.
• The designed environment may impair orstrengthen patients’ health status and personalcharacteristics, by alleviating or exacerbatingalready existing conditions and by opposingpatients’ natural strengths. For example,loss of sleep due to noise may prolong re-covery time after a procedure more for
2. A MODELEnvironment and Outcomes
TNEMNORIVNELACISYHP
Supporting or Hindering
Medical Interventions
Health Status and Personal
Characteristics
Protecting from or Exposing to Causes of Illness
Impairing or Strengthening
Patients’ Health Status and Personal Characteristics
Figure 1. Factors affecting patient health outcomes

those who were in a worse state, with morepreexisting health problems, than for thosewho were comparatively well to begin with.Conversely, equipment designed to makeactivities of daily living possible and easy —a bedside commode or a speaker phone, asexamples — may prevent dysfunction forsome patients with physical impairmentswho might otherwise be unable to reach anduse them.
• The designed environment can protect patientsfrom or expose them to causes of illness. For ex-ample, excessive noise may alter sleepingpatterns, reduce REM sleep, and therebycause irritability and dysfunction; patientstreated in the hospital may be spared debili-tating or even deadly nosocomial infectionsby the circulation of ultraclean air.
This conceptual model makes it clear thatwhen health outcomes for patients treated indifferent environmental conditions are com-pared, researchers must make certain that thepatients in each of the study groups are similarin their burdens of illness and in other charac-teristics that affect their health.
It is also apparent from the model that in-vestigators must make sure that the patientsbeing compared have received the same clini-cal treatment in environments that were simi-lar in every way in addition to the presence orabsence of the feature being studied. Especial-ly in “natural history” studies, in which the en-vironment is observed but not manipulated,methodological problems arise because inves-tigators are unable to control all the variablesthat affect patients’ health.
Indeed, the model highlights the barriersthat exist in attempting to isolate specific envi-ronmental features for rigorous scientificstudy. The healthcare setting is complex. It ishard to change only one feature withoutchanging others. The amount of knowledgethat can be gained through clinical research isthus limited. Unfortunately, there are likely tobe important environmental effects on healthoutcomes that will never be amenable to isola-tion and demonstration. Therefore, many ofthe decisions about the design of healthcarefacilities will necessarily continue to rely onbest guesses.
Nevertheless, the literature review confirmsthat many features could be studied more rig-orously than they have been until now.
Suggested Applications: Quiet,Music, and Air Quality To illustrate how the design of the physicalenvironment might be based on scientific evi-dence of what promotes better patient out-comes, the Johns Hopkins team focused onstudies of the auditory environment and airquality that were characterized by relativelystrong research methods. Translated into de-sign principles, the study conclusions can beapplied pragmatically to representative health-care settings.
This expanded Status Report includes anew application on air quality. This applica-tion was selected because there were severalhigh-quality studies indicating that contami-nated air causes hospital-acquired infections.Better design of ventilation systems in health-care facilities thus may improve patient out-comes by preventing such infections.
1. Quiet in the CCUThe Study: Topf M, Davis V. Critical carenoise and rapid eye movement (REM) sleep.Heart and Lung 1993; 22 (3): 252–258.
Research Question: Does CCU noise affectREM sleep?
Methods: Seventy healthy women were ran-domly assigned to sleep in a sleep lab underquiet conditions or listening to an audiotaperecording of CCU sounds. Ten measures ofREM sleep were assessed, including REM ac-tivity and duration during the first and secondhalves of the night and throughout the night,and the interval between first and secondREM cycles.
Findings: Women exposed to CCU noise hadless REM activity, shorter REM durations,and longer intervals between REM cycles.
Limitations: Use of volunteers in a lab meanswe cannot be sure that the results apply to pa-tients in the CCU, although less REM sleepfor critically ill patients could reasonably beassumed to be more problematic than forhealthy volunteers. The relationship of REMsleep in the CCU to longer-term outcomes is
8 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes

◆ 9
unknown, although more sleep is a desirableshort-term outcome for patients with myocar-dial infarction.
Conclusion: CCU noise may suppress REMsleep.
The Design Principle: Dampen ambient soundin critical care units to the extent possible.
Sample Design Application: Figure 2 illustrates acritical care room incorporating design strate-gies to promote quiet, including:
1. Ceiling utilizes specialty acoustic tile with aNoise Reduction Coefficient (NRC) in therange of 0.85 to 1.0.
2. All chairs are upholstered with sound-ab-sorbent fabric.
3. Flooring in all areas consists of acousticalresilient sheet vinyl with sound-deadeningproperties.
4. Wall panels are sound-absorbent.
5. Noise-cancellation headphones are provided.
2. Music during Minor SurgeryThree studies are abstracted below that describehow music may affect medical outcomes.
The Study: Menegazzi JJ, Paris P, Kersteen C,et al. A randomized controlled trial of the useof music during laceration repair. Ann EmergMed 1991; 20: 348–350
Research Question: Does music chosen by patientsand played through a headset change their vitalsigns or reduce their pain or anxiety during lac-eration repair in the emergency room?
Methods: Thirty-eight emergency patients whounderwent laceration repair with local anesthe-sia at the University of Pittsburgh teachinghospital were randomized to receive headsetmusic or not to receive music during the re-pair. Patients in the music group chose from 50available styles and artists and controlled thevolume themselves. Investigators monitoredheart rate, blood pressure, respirations beforeand after the repair, and obtained pain ratingsand a state of anxiety scale after the procedure.The group that heard music was asked to ratehow beneficial the music was as well.
Findings: Patients who listened to headsetmusic that they chose had less pain and similar
anxiety levels to those in the control group. Ofthose who heard music, 89 percent thought itwas very beneficial and 100 percent said theywould use it again if it were offered.
Limitations: A small study at one hospital cangive spurious results, so it should be repeatedat other hospitals to confirm the findings.
Conclusion: Patient-selected headset music dur-ing laceration repair in the emergency roomhelps reduce pain.
The Study: Moss VA. Music and the surgicalpatient. AORN Journal 1988; 48(1): 64–69.
Research Question: Does music affect anxiety ofpatients undergoing elective arthroscopicsurgery under general anesthesia?
Methods: Seventeen patients from one ortho-p e d i c p r a c t i c e w h o w e r e t o u n d e r g oarthroscopy with possible closed meniscecto-my, femoral or patellar chondrectomy, or lat-
Figure 2. Critical Care Room Incorporating EnvironmentalStrategies to Promote Quiet (courtesy of Watkins, Carter,Hamilton Architects)
1
2
3
5
4

10 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
eral release were assigned to be exposed to nomusic or to sedative music during the periop-erative period. A written State-Trait AnxietyInventory (STAI) was administered preopera-tively and postoperatively.
Findings: Patients exposed to music showed asignificant decrease in anxiety based on com-parison of their preoperative and postopera-tive scores, whereas control patients’ scoresshowed no difference.
Limitations: The sample size was small, and itis unclear whether patients were assigned tomusic randomly by the investigators. This cre-ates the possibility of bias.
Conclusion: Perioperative music for arthro-scopic surgery may reduce patients’ anxiety.
The Study: Parkin SF. The effect of ambientmusic upon the reactions of children undergo-ing dental treatment. ASDC J Dent Child,1981; 48(6): 430–432.
Research Question: Does ambient music duringdental cavity preparation affect children’s anx-iety levels during the procedure?
Methods: Twenty-five children scheduled fortwo different visits to the Children’s DentistryDepartment of a dental hospital for cavitypreparation were assigned to be exposed to am-bient music on one visit and not to receivemusic on one visit. Children ranged in agefrom 7 to 14 years old. Children were recordedon silent videotape for a period of 60 seconds ateach visit. Four independent observers blindedto the presence or absence of music graded thechild’s anxiety using a visual analogue scale.
Results: Patients were graded as less anxiousduring the visit at which they heard music.
Limitations: Investigators themselves raised,but could not answer, the question of whetherit was the music or the novelty of the musicthat created the effect.
Conclusion: Ambient music may reduce chil-dren’s anxiety during cavity preparation.
The Design Principle: Provide a way for patientsundergoing minor surgery to listen to music,preferably of their choice, during the procedure.
Sample Design Application: Figure 3 demon-strates an operating room designed to providemusic during minor surgery, including the fol-lowing features:
1. Speakers are installed in the ceiling.
2. Headphones for playback of personally se-lected music are available for use at the dis-cretion of the patient and/or surgicalpersonnel.
3. Speakers are attached to the underside ofthe operating table.
4. TheraSound™ Body Mat on the operatingtable provides the patient a full-body expe-rience of sound and vibrational resonancebefore and after the procedure or through-out at the surgeon’s discretion.
3. Air QualityThe seven studies below describe how airquality may affect medical outcomes.
The Study: Fridkin SK, Kremer FB, Bland LA,Padhye A, McNeil MM, Jarvis WR. Acremoniumkiliense endophthalmitis that occurred aftercataract extraction in an ambulatory surgicalcenter and was traced to an environmental reser-voir. Clinical Infectious Diseases 1996; 22: 222–7.
Figure 3: An Operating Room Incorporating EnvironmentalStrategies for Providing Music during Surgery (courtesy ofWatkins, Carter, Hamilton Architects)
1
23 4

Research Question: Did the contamination ofthe high-efficiency particulate air filter(HEPA) in the heating, ventilation, and air-conditioning system lead to the developmentof postoperative endophthalmitis caused byAcremonium kiliense — a fungus occasionallyassociated with posttraumatic keratitis?
Methods: Two hundred and sixteen patients ofan ambulatory surgical center undergoingcataract extraction with intraocular lens imple-mentation were analyzed in a matched case andcontrol study comparing procedures on the firstoperative day of the week versus other days andprocedures before 8:45 AM versus after. An en-vironmental evaluation was also conducted.
Findings: Case patients all had surgery on thefirst operative day of the week or had surgerysignificantly sooner after the operating roomopened than did controls (a median startingpoint of 46 vs. 150 minutes after opening[range, 30–72 vs. 30–255 minutes]; p=.03).The environmental evaluation revealed thatthe ventilation system was turned on 5–30minutes before procedures on the first opera-tive day of the week, and the air was filteredbefore but not after humidification. Culturesof the humidifier water in the ventilation sys-tem yielded A. kiliense phenotypically identicalto isolates from case patients.
Limitations: There is a possibility that case andcontrol patients also differed in other impor-tant aspects, as this is not reported.
Conclusions: An environmental reservoir of A.kiliense apparently caused infection of the patients when the ventilation system wasswitched on each week.
The Study: Loo GV, Bertrand C, Dixon C,Vitye D, Eng B, De Salis B, McLean APH,Brox A, Robson HG. Control of construction-associated nosocomial aspergillosis in an anti-quated hematology unit. Infect Control HospEpidemiol 1996; June 17(6): 360-364.
Research Question: Did an environmental controlprogram help to control a construction-relatedoutbreak of invasive aspergillosis in patientswith leukemia or bone marrow transplants?
Methods: From January 1988 to September1993, 141 neutropenic patients with leukemiaor bone marrow transplants were admittedinto the hematology and oncology unit. Thesepatients were divided into three groups: pre-construction of addition to the hospital, dur-ing construction, and during constructionafter institution of infection-control measures.These measures included HEPA-filter air purifier units and application of copper-8-quinolinolate formulation. Air and surfacesamplings were performed on three occasionscorresponding to the three time periodsabove. Incidence densities were calculated andcompared to the preconstruction baseline rateof nosocomial aspergillosis.
Findings: Thirty-six cases were diagnosed. Theincidence density in the preconstruction peri-od was 3.18 per 1,000 days at risk. Duringconstruction activity the ID increased to 9.88per 1,000 days at risk. After implementation ofinfection-control measures, the ID decreasedto 2.91 per 1,000 days at risk.
Limitations: Different stages in constructionmay have affected the results (i.e., demolitionvs. new construction). A study at one hospitalmay not be generalizable.
Conclusion: An environmental control strategyprobably assisted in preventing invasive as-pergillosis due to construction.
The Study: Cotterill S, Evans R, Fraise AP. Anunusual source for an outbreak of methicillin-re-sistant Staphylococcus aureus on an intensive thera-py unit. J of Hospital Infection 1996; 32: 207–216.
Research Question: Did the exhaust ducting ofan isolation room ventilation system beingnext to an open window of the IntensiveTreatment Unit (ITU) lead to an outbreak ofStaphylococcus aureus in patients being nursed inthe bed directly below the window?
Methods: Of 100 patients admitted to the ITUduring the period of October 1993 to February1994, 6 patients were found positive for methi-cillin-resistant Staphylococcus aureus (MRSA)strains with the same antibiogram and phasetype. Investigation of the environment includedmicrobiological samplings and assessment of the
◆ 11

ventilation system of the isolation room. Theside room ventilation system could not be sam-pled due to constant occupation of the room.
Findings: All case patients had initially beennursed in the same bed. Inspection of the out-side of the building revealed that the exhaustgrille of the isolation room was in close prox-imity to an open window directly above bed 3.It was also determined that a switch control-ling air flow in the isolation room was brokenand that the room was under positive pressure.After fixing the switch and sealing the window,there were no further cases of colonization bythe same strain of MRSA.
Limitations: Although accumulation of dust con-taining MRSA within the ITU ventilation ductswas documented, the failure to show conclu-sively that the ventilation system was infectedmakes the findings somewhat less conclusive.
Conclusion: The proximity of the exhaust duct-ing from a side isolation room to the openwindow above bed 3 probably led to the out-break of MRSA associated with that bed.
The Design Principle: By improving the purityof indoor air, it is possible to reduce the risk ofinfection of immunocompromised individuals.
Sample Design Application:
1. Replace perforated ceiling tiles with non-porous material.
2. Install high-efficiency particulate air(HEPA)-filter air purifiers for all incomingair supply.
3. Apply copper-8-quinolinolate-formulation.
4. Seal all windows completely to prevent in-filtration.
5. Install timers that can automatically turn onthe ventilation system a minimum of twohours before invasive procedures begin.
6. Identify location of all exhaust vents and relocate any that could contaminate the airsupply of immunocompromised individuals.
7. Minimize horizontal, dust-collecting surfaces.
The Study: Abzug MJ, Gardner S, Glode MP,et al. Heliport-associated nosocomial mu-cormycoses [letter]. Infection Control & HospitalEpidemiology 1992; 13(6): 325–326
Research Question: Were three isolated cases ofnosocomial mucormycosis in the oncologyunit caused by increased use of a heliport lo-cated near the ventilation system intake ducts?
Methods: After three cases of mucormycosiswere diagnosed in a pediatric teaching hospitalbetween March and September 1985, microbi-ology, pathology, and nosocomial infectionrecords from 1978 to 1985 were reviewed. Theventilation pathway for the oncology unit wastraced via hospital blueprints to intake vents inclose proximity to the heliport. Thirty roomair samples were taken from nine patientrooms in the oncology unit over five differentdays during a three-month period. Eleven airsamples from above the false ceiling panels inthree patient rooms were also taken, along withsamples of the gravel that covered the roofnear the helipad and cultures of the filters in-side the intake vents for the ventilation system.
Findings: There were no cases of mucormyco-sis observed between 1978 and 1985 and threecases in 1985. Review of heliport use deter-mined that the three infections had occurredafter periods of increased heliport utilization.Upon taking off or landing, the helicopterregularly blew gravel into the intake vents atspeeds upwards of 70 mph. The gravel samplesfrom under the helipad and the filters in theintake vents were found to be contaminatedwith zygomycetes. The air samples from thepatient rooms were also found to be contami-nated. After installing high-efficiency particu-late air (HEPA) filters in the oncology patientrooms and replacing the gravel under the heli-pad with an impervious neoprene roofing ma-terial, no further cases of mucormycosis werereported as of 1991.
Limitations: Because this was an observationalstudy, other possible sources of temporary in-fection such as minor construction cannot beruled out.
Conclusion: The three isolated cases of mu-cormycosis were most likely caused by ventila-tion intake ducts near contaminated gravel andincreased heliport use, which resulted in gravelblown into the ducts and contamination of thepatient rooms.
12 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes

The Study: deSilva MI, Rissing JP. Postopera-tive wound infections following cardiacsurgery: significance of contaminated casesperformed in the preceding 48 hours. InfectionControl 1984; 5(8): 371–377
Research Question: Was a marked increase(from 1% to 9%) in postoperative wound in-fections following cardiac surgery the result ofa defective air-handling system?
Methods: Investigations were conducted of pa-tients, operating room practices, ventilationand air-conditioning in the operating room.Microbiological cultures of the operatingroom environment and equipment were alsotaken. Relevant information was obtainedfrom medical records, infection control sur-veillance records, the operating room logbook, personnel interviews, and direct obser-vation. A detailed study of the air-handlingsystem for the entire surgical suite was alsoundertaken.
Findings: The study of the air-handling systemdisclosed several problems:
1. Although federal standards required 15 airchanges per hour, the exchange rate was ac-tually closer to 3 or 4 changes per hour.
2. The ventilation system used filters with effi-ciencies more suited to residential areas, butless than adequate for an operating room.
3. A “thermal wheel” designed to recapturecooling or heating potential from exhaustedair was not functioning, making it difficultto maintain the proper relative humiditynear 50–55%.
4. Stagnant water condensed from the coolingcoils in the intake path presented a potentialpath of bacterial aerosol contamination.
5. There was inadequate positive pressure ofoperating room air due to high traffic dur-ing surgical procedures and open doors.
6. Relatively arbitrary changes in relative hu-midity occurred when changes were madeto the room temperature to augment raisingand lowering of patient body temperatures.
In addition, it was found that four of the seveninfected patients had been operated on within48 hours of a contaminated surgery in thesame operating room. In all, a statistically sig-nificant 29% of open-heart surgeries (4 of 14)
performed within 48 hours of a contaminatedsurgery resulted in a wound infection (p =.023). After changes to the air-handling systemincluding improved filtration, maintenance ofconstant temperature and humidity, and elimi-nation of the stagnant water under coolingcoils, the infection rate fell to less than 1%.
Limitations: Other factors could have con-tributed to the rise and subsequent fall in theinfection rate. These factors may have includedchanges in operating room procedures such astraffic control, operating room schedule, anddress code. Also, during the time period whenthe air-handling system was changed, the pa-tient population may also have been sicker andmore susceptible to wound infection.
Conclusion: A defective air-handling system inthe surgical suite probably resulted in an in-creased rate of postoperative wound infectionsamong cardiac patients.
The Study: Kyriakides GK, Zinneman HH, HallWH, Arora VK, Lifton J, DeWolf WC, MillerJ. Immunologic monitoring and aspergillosis inrenal transplant patients. American Journal ofSurgery 1976; 131(2): 246–252
Research Question: Did a transplant intensive-care unit exhaust system contaminated with birddroppings result in three cases of Aspergillus fu-migatus infection in renal allograft patients?
Methods: After three cases of A. fumigatus infec-tion occurred within a six-month time span, theentire ventilation system and air-conditioningsystem servicing the transplant intensive-careunit was examined for possible contamination.
Findings: The air intake system and two ofthree exhaust ducts proved to be free from con-tamination but the third exhaust duct wasfound to be contaminated with A. fumigatus, A.niger, and A. flavus. Further examination of theexhaust duct revealed that the exhaust vent onthe hospital roof had lost its protective screenand the exhaust fan was defective, causing air tobe suctioned back into the contaminated ductwhenever the fan stopped. Bird droppings werepresent in the duct, and apparently this was thedirect cause of the aspergillosis infections. Afterperforming the necessary repairs, there were nofurther cases of aspergillosis reported.
◆ 13

Limitations: The patients infected with A. fumi-gatus were classified as high risk, and as such,the conclusions in this case study cannot easilybe generalized to other populations.
Conclusion: The source of the three cases of as-pergillosis among renal allograft patients weredue to a malfunctioning exhaust duct contami-nated with bird droppings.
The Study: Sherertz RJ, Belani A, Kramer BS,Elfenbein GJ, Weiner RS, Sullivan ML,Thomas RG, Samsa GP. Impact of air filtra-tion on nosocomial Aspergillus infections.Unique risk of bone marrow transplant recipi-ents. American Journal of Medicine 1987; 83(4):709–718
Research Question: Can housing bone marrowtransplant recipients in HEPA-filtered envi-ronments reduce their risk of contractingnosocomial Aspergillus infection?
Methods: After it was suspected in 1983 thattoo many cases of aspergillosis infection wereoccurring among bone marrow transplant re-cipients, whole-wall HEPA filters were in-stalled in the bone marrow transplant unit.The medical records of all bone marrow trans-plant recipients from 1981 to 1985 were thenstudied for statistical analysis.
Findings: The Aspergillus infection rate beforeinstallation of HEPA units had been 19%among bone marrow recipients (14 of 74).Among the 39 bone marrow recipients housedin HEPA-filtered units, there were no cases ofAspergillus infection reported.
Limitations: Observational study creates thepossibility of confounding by other patient orenvironmental differences among the groups.
Conclusion: HEPA-filtered environments cansignificantly reduce the risk of bone marrowrecipients contracting nosocomial Aspergillusinfections.
Sample Design Application:
1. Replace perforated ceiling tiles with non-porous material.
2. Install high-efficiency particulate air(HEPA)-filter air purifiers for all incomingair supply.
3. Install ultra high-efficiency filters (99.97%effective for 0.3µ particles) in operatingrooms.
4. Apply copper-8-quinolinolate-formulation.
5. Seal all windows completely to prevent infil-tration.
6. Install timers that can automatically turn onoperating room ventilation systems a mini-mum of two hours before invasive proce-dures begin.
7. Identify locations of all exhaust vents fromisolation rooms or contaminated areas andrelocate any that could contaminate the airsupply of immunocompromised individuals.
8. Minimize horizontal, dust-collecting sur-faces.
9. Use neoprene or other impermeable roofsunder heliports.
10. Protect and filter intake ducts near heli-ports.
11. In operating rooms, use ventilation sys-tems that maintain constant temperatureand relative humidity of 50–55% with mon-itoring systems to ensure they are working.
12. Eliminate standing water due to conden-sation in cooling system coils using vacuumdrainage systems.
13. Install automatic doors between operatingrooms and administrative areas to maintainpositive pressure of operating room air.
14. Install heat lamps and temperature controlanesthesiology machine humidifiers in oper-ating rooms so that staff do not need to in-crease room temperature in order to rewarmpatients.
15. Place bird screens on all exhaust and in-take air ducts and fans on all exhaust ducts.
4. Exposure to Daylight and SunlightThree studies described below illustrate hownatural daylight and outdoor sunlight may af-fect medical outcomes.
The Study: Barss P, Comfort K. Ward designand neonatal jaundice in the tropics: report ofan epidemic. British Medical Journal 1985; 291:400–401.
14 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes

Research Question: Does exposure to naturalsunlight through glass windows help preventneonatal jaundice?
Methods: Seven hundred and twenty-four new-born infants in an obstetric ward in the tropicsof New Guinea were analyzed in an observa-tional study comparing infants born before,during, and after awnings were built on wardwindows that severely limited the intensity ofnatural light coming through the windowglass. An analysis was also conducted of themethods of delivery and postpartum complica-tions during these three different periods.
Findings: In the first four months of the yearprior to the modifications, there was only onecase of clinical jaundice out of 215 births: anincidence rate of 0.5%. During the first fourmonths of the year in which construction ofrain awnings on the outside of windows wasperformed, the rate increased to 9% (17 casesout of 187 births); and in the first four monthsof the year following the construction ofawnings, the rate reached epidemic propor-tions at 17% (29 cases out of 175 births). Nosignificant variations were observed in themethods of delivery, neonatal infection rate,birth weights, or postpartum complicationsover the construction period.
Limitations: Causal inference is limited due tothe observational nature of the study. Unex-plained fluctuations in the incidence of neona-tal jaundice have been reported elsewhere.
Conclusion: Natural sunlight entering glasswindows in obstetric units may reduce the rateof neonatal jaundice.
The Study: Lamberg-Allardt C. Vitamin D in-take, sunlight exposure and 25-hydroxyvitaminD levels in the elderly during one year. Annalsof Nutrition & Metabolism 1984; 28: 144–150.
Research Question: Were low concentrations ofserum 25-hydroxyvitamin D (25-OH-D) inthree groups of elderly people connected totheir exposure to outdoor sunlight?
Methods: Three groups of elderly people werestudied: 26 long-stay geriatric patients (Group1), 24 semi-ambulatory persons residing in anold age home (Group 2), and 22 healthy, am-bulatory persons living at home (Group 3). A
non-elderly control group comprised 24healthy employees at a department store witha mean age of 44 years. Blood was drawn fourtimes during the study year and serum 25-OH-D concentrations were measured.
Findings: Though there was some seasonalvariation in all groups, the serum 25-OH-Dconcentration was lower in Group 3 (living athome) than in the control group, and the con-centration in Group 2 (old age home) was sig-nificantly lower than in the controls and inthose living at home. The concentration waslowest in Group 1 (long-stay geriatric patientsp < 0.001) throughout the year.
Mean vitamin D intake also was significant-ly lower in Group 2 than the mean intake inthe control group and in Group 3 (p < 0.02).The mean intake in Group 1 was the lowestand differed significantly from the intake inthe control group (p < 0.001), Group 3 (p <0.001), and Group 2 (p < 0.005). Vitamin Dintake/1000 kcal showed similar trends, withGroup 1 having the lowest ratio.
Subjects at home spent 4% less time out-doors during the year than those in the controlgroup, those in the old age home spent abouthalf as much time outdoors as those at home,and those in the long stay facility spent only17% of the time spent outdoors by the controlgroup.
Limitations: Elderly patients in Group 1 hadlower vitamin D intake levels as well as lowersunlight exposure, which may explain lower25-OH-D levels. In addition, because this wasan observational study, there are likely to bemany other differences among the groups thataffect vitamin D absorption or conversion be-sides outdoor sunlight exposure and may thusalso be responsible for lower serum 25-OH-Dlevels.
Conclusion: Inadequate exposure to naturalsunlight due to not going outdoors may beone reason for low serum-OH-D concentra-tion in long-term geriatric patients.
The Study: Beauchemin KM, Hays P. Sunnyhospital rooms expedite recovery from severeand refractory depressions. Journal of AffectiveDisorders 1996; 40: 49–51.
◆ 15

Research Question: Do depressed psychiatric pa-tients in sunny rooms stay in the hospital for ashorter term than those in rooms without sunshining in the window?
Methods: In a two-year study, 174 patients ad-mitted to a psychiatric ward with clinical de-pression were randomly assigned to eithersunny or “dull” hospital rooms. The averagelengths of stay for the two groups of patientswere then compared.
Findings: Patients in the sunny rooms stayedan average of 16.9 days compared to 19.5 daysfor those in dimly lit rooms. The differencewas consistent over all seasons and was statisti-cally significant.
Limitations: Randomness of the room assign-ments is not fully documented, and patientswere not fully compared to determine if otherfactors could have accounted for the differencein average stay lengths.
Conclusion: Sunny hospital rooms may reducethe amount of time clinically depressed pa-tients spend in the psychiatric unit.
The Design Principle: Maximize natural light ordaylight entering healthcare facilities, especial-
ly in obstetric, neonatal, and psychiatric units,and maximize access to outdoor sunlight for asmany patients as possible.
Sample Design Application:
1. Construct windows without awnings or per-manent immovable obstructions to sunlight,especially for psychiatric units and in obstet-ric areas for neonates.
2. Use ample window area and skylights asmuch as possible, especially for psychiatricunits and in obstetric areas for neonates.
3. Plan psychiatric units for depressed patientswith brighter exposures, e.g., southern ex-posures in the northern hemisphere.
4. Design outdoor areas to be accessible for el-derly patients including those with wheel-chairs and other disabilities.
Note: This application is general in nature, and must beimplemented with respect to local climatic conditions (i.e.,low latitude/high altitude sunlight), with appropriateglare-control strategies, and with attention to protectingpatients from sunburn. Many commonly prescribed med-ications and treatments cause patients to be acutely sensi-tive to direct sunlight. Therefore, access to shade must beprovided in outdoor areas.
16 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes

◆ 17
WHICH PATIENTS could have im-proved outcomes due to changesin the healthcare environment?
Which features of the healthcare environmenthold the most promise for rigorous investiga-tion? The literature offers little guidance.
Theoretical writings about healthcare facilitydesign have rarely involved clinicians and pa-tients, who could add important perspectives.The physical setting is only one of many facetsof care that affect health outcomes for a patientwith a particular condition during a specifictherapeutic episode. Outcomes-based health-care environmental design theory will matureonly after years of scientifically informed dia-logue among designers, clinicians, and patients.
First StepsThe first step in outlining a research agendawas to identify the types of patients who wouldbe the best candidates for interventions in thebuilt healthcare environment and the interven-tions that might affect their medical outcomes.For example, patients in initial studies mightbe those most apt to benefit from changes inthe designed environment or those most vul-nerable in current settings.
In order to generate a diverse list of suggest-ed patient groups and environmental featuresto study, focus groups of clinicians, healthcareresearchers, architects, healthcare designers,product managers, healthcare administrators,and facility managers were conducted in No-vember 1997 at the Tenth Symposium onHealthcare Design in San Diego. A focusgroup of The Center for Health Design’s En-
vironmental Quality Work Group was alsoconvened in January 1998 in New York City.This group included architects, designers, andproduct managers who originally convened tosuggest changes to national environmentalhealthcare design standards.
Focus Group ProceduresParticipants were sent advance materials de-scribing the purpose of the focus group. Focusgroups were audiotaped. After introductionswere made and written consent was obtainedfrom each participant, the moderator gave abrief overview of the background of the re-search project. Participants were then remind-ed that the focus group was convened in orderto identify patient groups that would benefitmost from changes in the healthcare environ-ment, and which features of the environmentshould be changed. Participants were providedwith a written list of the focus group questions:
1. Which group[s] of patients would most ben-efit from the changes in the healthcare envi-ronment?
2. Which features of the healthcare environ-ment should be changed?
3. What outcomes do you expect will improve?
Each participant was asked to state at least onesuggestion for a patient group to study, and ageneral discussion ensued. After the discussionwas over, participants were asked to write downtwo choices of patient groups, with features tochange and outcomes that they thought wouldbe affected.
Data collected from each focus group wastranscribed and analyzed. Appendix C lists
3. ESTABLISHING A RESEARCH AGENDAIdentifying Patient Groupsand Environmental Features for Possible Study

18 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
each patient group suggested, how many focusgroup participants submitted this as one oftheir two choices, setting and environmentalfeatures to be changed, and the outcomes thatthe participants thought would be improved.*
Criteria for Selection of PatientGroupsIn order to determine criteria by which patientgroups, settings, and environmental featuresshould be selected for study from among thoserecommended, a focus group of The Centerfor Health Design Research Committee wasconvened in January 1998 in San Francisco.
This group consisted of researchers specializ-ing in the effects of healthcare design and ar-chitecture on patient medical outcomes.Criteria recommended by the Research Com-mittee for deciding which study to select onthe effects of the built healthcare environmenton outcomes are listed in Table 5.
Each suggested patient group was rated bythe authors as 1, low; 2, medium; or 3, high;using these criteria (see Appendix C). Usingthe ratings and the investigators’ judgment,two general patient groups were selected forfurther consideration: seriously or chronicallyill children in acute or chronic care facilities,
TABLE 5Criteria Recommended by Research Committee for Selecting Patient Groups and Environmental Interventions to Study
IMPORTANCE
• Vulnerable patient population:- Reactive/fragile population; unable
to act on their own behalf- Long stay in health facility
• Important outcome affected; some-thing that makes a big difference topeople; something that affects health in a significant way
• Generalizable to other popula-tions, not just to a narrow or esoteric group
POLITICAL APPEAL
• Public resonance and identifica-tion (combination of population,outcome, setting, and featureschanged that seem important to awide variety of common people,the man on the street)
• Administrator resonance: e.g., reduces length of stay, costs
CREDIBILITY
• Practitioner resonance—includingcaregivers and designers. Mayneed to be multidimensional intervention for designers to believe it works
• Direct cause/effect relationshipof the built environment to theoutcome; e.g., the environmentrepresents medical treatment inthe situation studied
• Rigorous enough study for the scientific community to acceptthe cause/effect relationship of the environment
FEASIBILITY
• Doable/feasible research: - Homogenous study population- Feasible experiment design- Data easily obtained (already
collected will be best)- Intervention easily accomplished
during the research phase
• Feasible intervention: Actionableimplication that would not face alot of industry barriers when oth-ers attempt to apply it
* Respondents listed some outcomes that go beyond the medical outcomes listed in Table 2. These are listed for completeness, but medical outcomes were given more importance when rating studies used the criteria described in Table 5.

◆ 19
and physically frail but cognitively intact el-derly residents of long-term care facilities.These groups received high ratings, and theinvestigators judged based on prior clinicaland research experience that possible projectsin these groups were important, politically ap-pealing, credible, and feasible.
Possible Environmental Features for StudyFocus group participants described environ-mental interventions that might affect medicaloutcomes for each of the patient groups select-ed. The interventions described are groupedbelow according to the type of outcome theywere thought to affect.
Elderly physically frail, but cognitively intact residents of long-term facilities
Quality of Life: Well-beingAspects of well-being that could be improvedfor this population by changing environmentalfeatures include comfort, depression, sense ofdignity, hope, enjoyment, self-esteem, fulfill-ment with life, and overall patient satisfactionwith the environment. Environmental changesthat might affect well-being that were men-tioned by respondents included:
• Color
• Temperature
• Landscapes
• Pleasant outdoor views
• Gardens, courtyards, and patios with railsand walkways permitting walkers andwheelchairs, to allow physically impairedpatients to enjoy them
• A flexible environment to accommodate in-creasing level of care if needed so the pa-tient does not need to move from the samehome, e.g., using a mobile home
• Design reasonable walking distances tocommon spaces from units
• Smaller domestic scale, residential amenities
• Areas for intergenerational interactivity(kids, parents, animals) and playgrounds
• Equipment to create connections with peo-ple through the Internet
• Positive distraction
FunctioningImportant functional outcomes mentioned forthis group included independence in activitiesof daily living or autonomy, quantity, and quali-ty of social interaction (especially during din-ing), continence, e.g., a mobile home.
Environmental changes thought to affectfunctioning that were suggested by the respon-dents included:
• Bathroom design including more space totransfer to toilet, space to hang clothing,space to admit a walker
• Walking distances that are reasonable tocommon spaces from units, or home set-tings mobile units with smaller domesticscale, residential amenities
• Areas for intergenerational interactivity(kids, plants, animals) and playgrounds
• Flexible layout as above to accommodate fordifferent levels of care
Clinical OutcomesClinical outcomes that participants thoughtcould be improved through environmentalchanges for this population included medica-tion intake, falls, mobility, safety, agitation,bedsores, and length of stay.
Environmental changes thought to poten-tially improve those outcomes included reduc-ing noise levels, changing lighting to haveadequate intensity but without glare, and avoid-ing confusing color patterns that affect depthperception, installing wall-to-wall carpeting,and eliminating obstacles and scatter rugs.
Seriously ill children in acute- or chronic-care facilities.Focus group participants described that cer-tain environmental interventions might affectclinical outcomes for seriously ill children inacute- or chronic-care pediatric hospitals. Theparticipants suggested the importance of sev-eral overriding elements in design of health-care facilities for children that affect all typesof outcomes:
1. The facility from outside to the lobby andthroughout the interior should convey thatit is a special place for infants, children, andadolescents.
2. The facility should promote family’s impor-tant role in helping infants, children, and

adolescents cope with healthcare experi-ences, and feel in control and comfortable.Thus, there should be accommodations forparents that are efficient for assisting andcaring for their children. Specific interven-tions are described below under the out-come they were thought to affect.
Quality of Life: Well-beingAspects of well-being that could be improvedfor this patient population by changing envi-ronmental features include children’s comfort,empowerment and self-esteem, and familystress. Suggested environmental changes thatwere thought to affect these aspects of well-being included:
• Color
• Temperature
• Light
• Sound
• “Homelike,” residential-type design features
• Appropriate environment for siblings andparents
• A general “fun” environment
• “Personalization” with personal belongings
• Privacy for parents for discussions aboutprognosis, so that children will not overhear
One aspect of well-being mentioned thatcould be improved specifically for infants bychanging environmental features was neonatalrelaxation and bonding with their parents.Suggested environmental changes for neonatesincluded:
• Individual rooms for each baby with parents
• Music in cribs or in room
FunctioningAspects of functioning that could be improvedfor seriously ill children by changing environ-mental features in hospitals include physicalfunctioning and social interaction with peers.Environmental changes that might affect func-tioning that were mentioned by respondentsincluded:
• Access to outdoor play
• “Star Bright” Internet network for virtualconnection with others
• Parent accommodations such as lounge,showers, and kitchen
• Family sleeping area
• Conference room so child does not hearparent/provider discussions
• Transition room for going home to teachself-care
Environmental changes that might affect func-tion for neonates that were mentioned by re-spondents included:
• Accommodations for parents that facilitatecontact/touch between parent and child
• Family sleeping area
Clinical OutcomesChanges in clinical outcomes that participantsthought might occur through environmentalchanges for the children and adolescents included:
• Decreased medication intake
• Decreased stress
• Decreased length of stay
• Increased recovery rate
• Decreased recovery time
• Reduced pain
• Increased psychological and physical peaceful-ness and increased psychological adjustment
Neonatal clinical outcomes that participantsthought could occur through environmentalchanges included:
• Weight gain
• Reduced abuse by parents due to increasedbonding of parent and child
• Reduced length of stay
Having reviewed some of the possible fea-tures of the environment that could be changedto improve patient medical outcomes for thesegroups, the next chapter outlines criteria thathelp us to decide upon features for interven-tion, and an agenda for planning a trial to at-tempt to demonstrate the possible impact of thebuilt healthcare environment on patient med-ical outcomes.
20 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes

Toward a Research Agenda:Methodological ConcernsNo matter which environmental features orwhich types of patients are studied in the fu-ture, some important methodologic recom-mendations would make research in this fieldmore cost-effective and add to its impact.
Studies of the effect of the healthcare envi-ronment on patient outcomes need to be as rigorous as those of any other healthcare in-tervention. The best studies, as has been em-phasized, are randomized controlled trials andthose that assign the same subjects to differentconditions in random sequence with paireddata analysis. These strategies help ensure thatno significant confounding factors affect theoutcomes when the patients are observedunder the environmental conditions beingcompared.
True blinding is difficult to achieve whenenvironmental features are the subjects of theresearch. At the very least, however, new fea-tures should be allocated among patients atrandom.
When randomization is not possible, obser-vational studies should be planned that takeinto account the entire conceptual model ofinteractions affecting patient health outcomes.All variables that may influence clinical out-comes for the patients being observed, includ-ing patients’ personal characteristics, medicalinterventions, and aspects of the healthcaresetting, need to be measured to make surethere are no systematic differences among thedifferent patient groups or study sites.
Proposed Master Plan:Recommended Next StepsAppendix D provides a master plan and time-table for the next steps in an agenda to investi-gate, with scientific rigor, whether the builtenvironment plays a role in healthcare out-comes, and if so, what the types and strengthsof such effects are.
Should they validate the hypothesis that theenvironment matters, the steps describedbelow will move the field toward the ultimatedevelopment of appropriate design standardsand guidelines.
Year One: In the next six months, groups ofpatients and clinicians from each of the twogroups will be convened to discuss and makerecommendations as to the types of healthcareenvironmental changes that would produce thegreatest health outcome benefits for each ofthe two specific groups of patients selected forinitial study. The decision between the twogroups as well as which specific environmentalfeatures and outcomes will be targeted willcontinue to be based on the criteria in Table 5.It is expected that these criteria will be reap-plied after environmental features and out-comes have been defined through the focusgroups with clinicians, caregivers, and patients.
Years One to Four: In the following two years,one or more pilot studies will be undertakenon the basis of these recommendations. Thepilot study or studies will be designed to testenvironmental intervention procedures, out-come evaluation measures, and analytic tech-
◆ 21
4. THE FUTURE RESEARCH AGENDA

niques, in preparation for an expanded,longer-term investigation. During the periodof the pilot studies, and with their results inhand during the following six months, a defi-nite proposal for a rigorous five-year interven-tion study will be prepared, submitted forexternal funding, and refined as needed.
Years Five to Nine: Finally, a rigorous, large-scale, experimental study will be undertaken todemonstrate definitively whether or not achange in the healthcare environment will im-prove important health outcomes. This studywould last an estimated five years, including ayear for writing a report for publication anddissemination of results.
ConclusionThere is suggestive evidence that aspects ofthe designed environment exert significant ef-fects on clinical outcomes for patients receiv-ing medical care. However, the case must stillbe proved. Accurate, valid scientific data basedon careful, credible studies are needed.
More than $16 billion is being spent inhealth facilities construction in the UnitedStates this year. Yet with outlays at this level,there is near total ignorance of the impact ofthe design of the built environment on the ef-fectiveness of clinical intervention. In this con-text, investment in the research programoutlined above is a modest yet vital first stepwith the potential to yield cost savings and im-proved health through the design of thehealthcare environment.
22 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes

◆ 23
THE OVID AND Pubmed search engineswere used to search the Medline data-base. The Health Star database was
searched using Ovid only. All searches werelimited to English-language articles.
Other potentially pertinent studies cited asreferences in the articles located were re-trieved and read as well. Finally, The Centerfor Health Design staff and members of itsHealthcare Design Research Committee sug-gested additional literature sources, whichwere also reviewed.
Health Facilities*The search began with the keyword “healthfacilities”* from the Medline and Health Starsubject heading tree. Additional keywords rep-resenting specific types of health facilities wereidentified through the subject heading tree.The following available specific terms wereconsidered relevant to effects of the healthcareenvironment on patient outcomes and wereincluded in the search:
• Academic medical centers
• Ambulatory-care facilities
• Birthing centers
• Dental facilities
• Health facilities, proprietary
• Hospital units
• Hospitals
• Leper colonies
• Medical office buildings
• Nurseries
• Physicians’ offices
• Rehabilitation centers
• Residential facilities
• Health facility environment
• Health facility size
• Health design and construction
The following specific words related to healthfacilities were not considered relevant to thetopic under study and were not used in thesearch:
• Bed occupancy
• Biological specimen banks
• Health facility laboratories
• Pharmacies
In addition to health facilities and the relatedspecific terms above, the keyword combina-tions below were also searched. For phrasesmarked with an asterisk (*), additional articleswere located using Ovid’s “explode” function.This identified a larger number of articles,many of which were not relevant, but some-times a few more relevant articles were located.
• Outcomes and process assessment/health facilities
• Room size
• Patients’ rooms and size
• Room scale
• Room privacy
• Hospital and room size
• Cross infection and health facilities
• Cross infection and ventilation
APPENDIX ALiterature Search Methods

24 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
• Health facilities and ventilation
• Room organization
• Environmental control by patient
• Room flow or interactivity
• Air and ventilation
• Health facilities and humidity*
• Health facilities and lighting*
• Health facilities and sunlight*
• Health facilities and aroma*
• Health facilities and noise*
• Health facilities and music*
• Health facilities and temperature*
• Furnishings
• Health facilities and climate/landscape*
• Health facilities and equipment design*
• Windows
• View out window
• Disinfection
• Sterilization
The keywords listed above served as initialsearch words. The number of titles identifieddepended on the specificity of each keyword.
Medline (PubMed)In using the PubMed program, the same key-words were employed. However, PubMed has afunction that allows a list of articles to be re-quested that are related to a specific article. Bythis function, “See related articles,” a significantnumber of additional titles were obtained thatincreased the volume of the search significantly.
Criteria for Selection and Elimination of ArticlesOnce the list of titles was compiled from thetwo databases, a number of criteria were usedto eliminate or include an article for furtherinvestigation. If the title of the article did notclearly indicate whether it was relevant, theabstract was retrieved. If the abstract also didnot clarify if the article was relevant, the arti-cle was retrieved. Articles were excluded forthe following reasons:
1. The article is not relevant to the topic. Forexample, when searching using the keywords“color and patient recovery,” articles werefound that discuss the recovery of color vi-sion in patients after eye surgery. Irrelevantarticles were classified as those that either: a. Do not discuss the health facility environ-
ment, or
b. Do not discuss how the health facility environment affects patients’ outcomes
2. The article is on the correct topic, but givesno experimental data evaluating effects ofthe environment on patient outcome, e.g.,an editorial.
3. The article does not discuss human subjects.

◆ 25

26 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Ackerman B, Sherwonit E, Williams J. Reduced incidental light exposure: effect on the developmentof retinopathy of prematurity in low birth weight infants. Pediatr 1989; 83: 958–962
Reduced light exposure from55 to 15 footcandles (using ablanket to cover the top partof the isolette)
Premature infants inthe intensive care nursery at Yale–NewHaven Hospital(n=290)
Anderson JD, Bonner M, Scheifele DW, et al. Lack of nosocomial varicella in a pediatric hospital withnegative pressure ventilation patient rooms. InfectControl 1985; 6(3): 120–121
Negative pressure ventilation
Pediatric patients in aVancouver hospital(n=164)
1 = Randomized control trial1b = Experimental, consecutive or apparently unbiased
systematic assignment2 = Experimental, paired2b = Experimental, unpaired, same group at two time points
3 = Observational paired3b = Observational, unpaired, same group at two time points4 = Observational, unpaired4b = Observational, unpaired, nonrandom assignment
† CODES FOR STUDY DESIGNS
APPENDIX B Summary Table of Extant Studies of Effects of the Healthcare Environment on Patient Outcomes
Abzug MJ, Gardner S, Glode MP, et al. Heliport-associated nosocomial mucormycoses [letter]. Infection Control & Hospital Epidemiology 1992; 13(6):325–326
Gravel under helipad in prox-imity to ventilation system intake vents vs. impermeableneoprene roof, high-efficiencyparticulate air (HEPA) filtersin oncology patient rooms
Newly diagnosedleukemia patients in a pediatric teachinghospital (n=168)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 27
Incidence ofretinopathy ofprematurity
4
4
There was no difference in the incidenceand severity of retinopathy of prematuri-ty between groups exposed to differentintensities of light
Historical control group allows con-founding; however, groups did not dif-fer in known predictors of retinopathyincluding oxygen therapy, gestationalage, and birth weight
Incidence ofnosocomialchicken pox
Children in the unit with negative pressure rooms had lower incidence ofnosocomial chicken pox than those on aregular ward
1) Follow-up of only English-speakingpatients in Vancouver
2) Other differences between the twounits unknown
3) No characterization of illness statesof patients on the two wards; possibleconfounding
ADDITIONAL CODES1 Consecutive assignment2 Uncontrolled study; asks patients if they believe noise affected their sleep3 Systematic assignment
Cases of mucormycosis
4 No cases of mucormycosis observed1978–1985, 3 cases in 1985, and nocases 1986–1991. Heliport was con-structed in 1983, with 55 transports in 1984 and 77 in 1985. Infections occurred after heavy heliport use. It was found that gravel contaminatedwith zygomycetes was blown into theventilation system intake ducts by thehelicopter
Observational design permits con-founding, but results and demonstra-tion of pathway of pathogenesis arehighly suggestive of a causal link
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY

ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION
28 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Baumgart S, Engle W, Fox W, et al. Effect of heatshielding on convective and evaporative heat lossesand on radiant heat transfer in the premature infant.J Pediatr 1981; 99: 948–956
Heat shielding using plasticwalls around beds and plasticblankets
Premature newborns,most with respiratorydistress, without renal,cardiovascular, or CNS disorders at The Children’s Hospital ofPhiladelphia (n=10)
Baker CF. Discomfort to environmental noise: heartrate response to SICU patients. Crit Care Nurs Q1992; 15(2): 75–90
Noise level and type of noise SICU patients in a privateSouthwest nonteachinghospital after abdominal,carotid endarterectomy,or peripheral vascularsurgery (n=28)
Baker CF, Garvin BJ, Kennedy CW, et al. The effectof environmental sound and communication on CCUpatients’ heart rate and blood pressure. Res NursHealth 1993; 16: 415–421
Noise level and type of noise Adults admitted to aCCU in a large midwestern teachinghospital (n=20)
Baldwin S. Effects of furniture rearrangement on theatmosphere of wards in a maximum-security hospital.Hosp Commun Psychiatry 1985; May 36(5): 525–528
Rearrangement of furniturefrom nonsocial patterns intogroup seating
Patients with severemental retardation, psychogeriatric patients,and those with variouspsychiatric disorders in a maximum-security hos-pital in England (n=260)
Anderson RL, Mackel DC, Stoler BS, et al. Carpet-ing in hospitals: an epidemiological evaluation. J ofClinical Microbiology 1982; Mar: 408–415
Carpeting or bare floor in patient rooms
Patients randomly admitted to rooms with(CR) and without (NCR)carpeting in a pediatrichospital (n=69)
Barss P, Comfort K. Ward design and neonatal jaun-dice in the tropics: report of an epidemic. Br Med J1985; 291: 400–401
Awnings reducing naturallight
Newborn infants in the obstetric ward ofProvincial Hospital inthe tropics of Papua,New Guinea (n=724)

STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
◆ 29
Insensible water loss-es and radiant powerdemand
2 1) Excellent study design, experi-mental controlled trial withpaired data
2) Reliability and validity of mea-sures not described but goodface validity
Water losses were lower in the shieldedconditions. Radiant power demand was the same for control and walled environments but lower when infantswere covered with plastic blankets. Thin plastic blankets were the most effective heat shields.
4 Heart rate Mean heart rate was higher during talk-ing in the room and nontalking noisecompared with talking inside the roomand ambient noise only
1) Very small sample size
2) Nonrandomized study; noisetype and level may be confound-ed by different types of patientsexperiencing each type of noise—not examined or reported on
3 Blood pressure andheart rate
Subjects had higher maximum heart ratesduring room conversation than duringbackground sound. This effect was inde-pendent of the decibel level.
1) Very small sample size may limitgeneralizability
2) Prior state of the patient beforeobservation may confound thenoise level and type of noise; re-peated measures analysis usingeach patient as his own control isotherwise a fairly strong design
3 Seclusion rate, casualty incidents,“points” earned byresidents for goodbehavior, residentperception of theward, nursing obser-vations of residents’behavior
During the study the intervention wardshad lower rates of patients requiringseclusion, a lower rate of casualty inci-dents, and nurses’ reports showed favor-able attitudes and improved socialinteraction
1) Fairly strong design due to sta-ble group of patients over time
2) No reliability or validity testingof outcome measures is reported
1 Typable organisms (including E. coli,Pseudomonas aeruginosa, Klebsiella pneumo-niae, and Staphylococcus aureus) were isolated more frequently from patients incarpeted rooms than those in rooms withbare floors. However, patients in bothtypes of room had similar rates of colo-nization with all organisms (whether typable or nontypable) found on the floor,and similar rates of hospital-acquired infection. Hospital-acquired infectionswere not associated with organisms foundas contaminants of the carpet or floor
Strong study design with random assignment. However, sample size provides inadequate power to detect possibly significant differences in hospital-acquired infections
Hospital-acquired in-fection rate. Propor-tion of patients colonized with ty-pable and nontypable organisms found onthe floor or carpet
Bilirubin concentra-tion, neonatal biliru-bin requests (jaundicecases)
4 Observational study permits con-founding; validity is increased be-cause the study identified andmeasured other elements that in-fluenced patient outcomes
Decreasing the amount of sunlight entering the ward significantly increasedthe rate of neonatal jaundice from 0.5%(1 of 215) to 17% (29 of 175)

30 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Blackburn S, Patteson D. Effects of cycled light onactivity state and cardiorespiratory function inpreterm infants. J Perinatal Nurs 1991; 4(4): 47–54
Lighting level, light cyclingvs. continuous lighting
Preterm infants born ator prior to 34 weeksgestation, admitted to atertiary neonatal inten-sive care unit, and withno history of majoranomalies or maternaldrug addiction (n=18)
Blankfield RP, Zyzanski SJ, Flocke SA, et al. Tapedtherapeutic suggestions and taped music as adjunctsin the care of coronary-artery-bypass patients. Am JClin Hypnosis 1995; 37(3): 32–42
Taped therapeutic suggestionand music intraoperatively andpostoperatively
Coronary-artery-bypass-surgery patients at twocommunity hospitals inCleveland, Ohio (n=95)
Belgaumaker TK, Scott KE. Effects of low humidityon small premature infants in servocontrol incuba-tors. Biol Neonate 1975; 26: 348–352
Humidity level Premature newborns inservocontrol incubatorsat Grace Maternity Hos-pital, Halifax, NS (n=19)
Bell EF, Gray JC, Weinstein MR, et al. The effects ofthermal environment on heat balance and insensiblewater loss in low birth weight infants. J Pediatr 1980;96: 452–459
Temperature level Premature newborns inincubators at Women’sand Infants Hospital ofRhode Island (n=12)
Beauchemin KM, Hays P. Sunny hospital rooms expedite recovery from severe and refractory depressions. J Affective Disorders 1996; 40: 49–51
Sunny vs. nonsunny or “dull”rooms
Psychiatric inpatientswith depression in a hos-pital in Edmonton, Al-berta, Canada (n=174)
Bourke L. Severe burn caused by an operating roomlight. Anesthesiology 1993; 79(1): 171–173
Unfiltered operating roomlight
62-year-old man under-going radical retropubicprostatectomy surgery(n=1)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 31
Heart rate, motor ac-tivity, and respiratoryrate
4b 1) Very small sample size
2) Nonrandomized study design permitsconfounding by unmeasured variables
3) No information about how theseneonates compare to the general neona-tal population in nontertiary nurseries
Infants in cycled lighting hadlower heart rates and motor activity in the low light level than the high light level; therewere no day-night differences inthe continuous lighting group
Length of stay, narcotic use, anxiety,recovery progress, depression, activities of daily living, cardiacsymptoms
1 Randomized design supports validityNo differences between thegroups were statistically signifi-cant, although groups listeningto tapes reported less pain andtook fewer narcotics
Apneic spells, mildand severe
2 1) Strong study design, experimental controlled trial with paired data
2) Small sample size may limit generaliz-ability
Severe apneic spells were more frequent in low than high humidity
Insensible water loss,evaporative heat loss, nonevaporativeheat loss, oxygen consumption
2 1) The authors discuss some threats tothe validity of measures that may causethem to estimate incorrectly
2) Strong study design, experimental trialwith paired data
Higher temperature produced arise in water loss and evaporativeheat loss and a fall in nonevapora-tive heat loss. Lower temperatureproduced an increase in oxygenconsumption and heat loss
1 Length of hospitalstay
Patients in sunny rooms stayed an average of 16.9 days, whereasthose in “dull” rooms stayed anaverage of 19.5 days. The differ-ence was consistent over all seasons during a period of twoyears (Oct. ’93–Sept. ’95)
Randomized study with comparison ofpatient groups
Severe burn4 Despite this being a case study with nocontrol information recorded, there isstrong causal inference that the light ex-posure caused the burn, due to the tem-poral relationship, the unusual nature ofthe outcome, and full understanding ofthe causal pathway
Patient exposed to unfilteredtungsten halogen light developeda partial, possibly full-thicknessburn
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY

32 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Cotterill S, Evans R, Fraise AP. An unusual sourcefor an outbreak of methicillin-resistant Staphylococcusaureus on an intensive therapy unit. J Hospital Infection1996; 32: 207–216
Relative location of ICU iso-lation room exhaust ductingand windows above otherICU beds
Patients in an intensive-therapy unit (ITU) in theUnited Kingdom (n=100)
Dolce JJ, Doleys DM. Narcotic utilization for backpain patients housed in private and semi-privaterooms. Addictive Behaviors 1985; 10: 91–95
Private vs. semiprivate rooms Orthopedic inpatientswith pain-related backdisorders at University ofAlabama, Birmingham(n=89)
Everett WD, Kipp H. Epidemiologic observations ofoperating room infections resulting from variations inventilation and temperature. Am J Infect Control 1991;19(6): 277–282
Ventilation system function-ing and air changes or operat-ing room temperature
Surgery patients at a publicly funded militaryfacility (n=903)
Caine J. The effects of music on the selected stressbehaviors, weight, caloric and formula intake, andlength of hospital stay of premature and low birthweight neonates in a newborn intensive care unit. J Music Therapy 1991, XVIII(4): 180–182
Music in a newborn intensivecare unit (NBICU)
Male and female pretermand low birth weightnewborns in the new-born intensive care unitat The TallahasseeMemorial RegionalMedical Center (n=52)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION
Davis-Rollans C, Cunningham SG. Physiologic responses of coronary care patients to selected music.Heart and Lung 1987; 16(4): 370–378
37-minute tape recording ofthree selected music piecesplayed in one of three differ-ent permutations
CCU patients at Kitch-ener-Waterloo Hospitalin Ontario, Canada(n=24)
Dubois JM, Bartter T, Pratter MR. Music improvespatient comfort level during outpatient bron-choscopy. Chest 1995; 108(1): 129–130
Music during bronchoscopyvs. no music
Bronchoscopy outpatientsat Cooper Hospital/Uni-versity Medical Centerof the UMDNJ/RobertWood Johnson School of Medicine at Camden,New Jersey (n=49)
deSilva MI, Rissing JP. Postoperative wound infec-tions following cardiac surgery: significance of conta-minated cases performed in the preceding 48 hours.Infect Control 1984; 5(8): 371–377
Changes to air-handling sys-tem to increase outside airchanges, improve filter effi-ciency, maintain constanttemperature and humidity,increase positive pressure ofoperating room air
Cardiac-surgery patientsat the VA Medical Cen-ter in Augusta, Georgia(n=506)

◆ 33
4 Infection with methi-cillin-resistant Staphy-lococcus aureus (MRSA)
The cases of MRSA were initially nursedin the same bed or in an adjacent bed.The bed was located under an open win-dow near exhaust ducting from an isola-tion room
Findings highly suggestive al-though not completely conclusivedue to inability to sample the venti-lation system air in the side room
4 Use of narcotics as ameasure of pain
Patients in private rooms requestedmore narcotic injections. However, thisdifference was not statistically significantafter adjusting for other variables
Small sample size given the numberof other variables being adjusted for
4 Clean wound infec-tions
When the ventilation system was inade-quate during the summer months, theinfection rate was 3.523 times higherthan in winter. When the ventilationsystem was fixed, the rates did not in-crease in summer
Historical control allows con-founding by other unknown envi-ronmental factors or changes inoperative procedures
1 Initial weight loss,daily average weight,formula and calorieslength of NBICU andtotal hospital stays,daily group mean ofstress behaviors
Infants randomized to music had signifi-cantly lower stress levels, improved feed-ing, lower initial weight loss, and shorterlength of hospital stay compared to in-fants without auditory stimulation
Strong study design
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
2 Change in emotionalstate, heart rate, respiratory rhythm,heart rhythm
There were no statistically significantchanges in specified physiologic vari-ables during the music period. Patientshad a happier emotional state aftermusic was played
Small sample size limits generaliz-ability. Observational study designpermits confounding but pairingstrengthens the causal inference
1 Overall comfort,cough, dyspnea
The use of music was associated withsignificantly greater comfort and lesscoughing. There was no significant dif-ference in rating of dyspnea during theprocedure
Strong study design
4 Postoperative woundinfection
Wound infections increased after reloca-tion from 4 of 320 (1%) to 7 of 77 (9%);after changes to air handling, the infec-tion rate decreased (7 of 77, 9%, beforevs. 1 of 109, < 1% after)
Observational study permits con-founding by alterations in operat-ing procedure that were madeconcurrently

34 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Geden EA, Lower M, Beattie, at al. Effects of musicand imagery on physiologic and self-report of ana-logued labor pain. Nurs Res 1989; 38: 37–41
Music: easy listening, rock,self-selected music, vs. a dis-sertation
Volunteer nulliparoussubjects exposed to apain stimulator at levelsreported to simulatelabor pain (n=50)
Giradin BW. Lightwave frequency and sleep-wakefrequency in well, full-term neonates. Holistic NursPrac 1992; 6(4): 57–66
Wavelength of light (light intensity) in a neonatal well-baby nursery
Hispanic neonates in anurban county hospital inSouthern California(n=100)
Giunta F, Rath J. Effect of environmental illumina-tion in prevention of hyperbilirubinemia of prematu-rity. Pediatrics 1969; 44: 162–167
Light intensity Low birth weight babiesat Providence Lying-InHospital (n=96)
Glass P, Avery GB, Subramanian KN, et al. Effect ofbright light in the hospital nursery of incidence ofretinopathy of prematurity. N Engl J Med 1985; 313:401–404
Light intensity (brightness) Preterm infants atGeorgetown UniversityHospital or Children’sHospital National Med-ical Center who weighedless than 2001 g and hada gestational age of lessthan 35 weeks at birth(n=228)
Gast P, Baker C. The CCU patient: anxiety and annoy-ance to noise. Crit Care Nurs Q 1989; 12(3): 39–54
Noisy vs. non-noisy hour Patients admitted to the CCU of a large midwestern university hospital (n=20)
Fridkin SK, Kremer FB, et al. Acremonium kiliense endophthalmitis that occurred after cataract extractionin an ambulatory surgical center and was traced to an environmental reservoir. Clin Inf Dis 1996; 22:222–227
Contaminated operatingroom ventilation system
Patients in ambulatorysurgical center (n=216)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 35
Self-reported pain1 1) Small sample size limits the powerof the study; the differences seenare in the expected direction oflower pain with easy listeningmusic and may be true differences
2) There are no data given abouthow the groups differ in otherways that may affect their pain;given the small sample size, thiswould confirm that the random-ization “worked”
Subjects randomized to different formsof music did not differ in the level ofpain they reported
Frequency of waking,sleep-wake frequen-cy, sleep-wake frequency variability
1 1) Excellent design: randomizedtrial
2) Generalizability to other racialgroups and to ill neonates un-known
Neonates randomized to high frequency(blue) lightwaves have more waking,greater sleep-wake frequency, and greatervariability in sleep-wake frequency thanneonates experiencing low frequency (red)lightwaves
Serum bilirubin1 1) Randomized trial, excellent design
2) Only half of infants followed upfor long-term outcomes, limits validity of those findings
Lower serum bilirubin in the group ex-posed to 90 footcandles compared to thegroup exposed to 10 footcandles; not asmuch effect as previous studies usinghigher intensity lights. No neurologic orvisual problems at follow-up in thebrighter light group
Incidence/severity of retinopathy ofprematurity
1 Observational double-cohort studywith sequential cohorts permitssome unmeasured confounding;however, study populations arecarefully characterized and strati-fied by birth weight
There was a higher incidence of retinopa-thy of prematurity in the group of infantswho had been exposed to the brighternursery lights, particularly in those withbirth weights below 1000 g
Anxiety, annoyancewith noise
3, 4 1) Some of the analyses do not usepaired data, limiting the study’spower
2) There were two similar noiselevels during the noisy and non-noisy hours
There were no differences in state anxi-ety or annoyance due to noise betweenthe noisy and quiet hours, controllingfor the level of “trait” anxiety
4 Acremonium kilienseendophthalmitis
Cases were more likely to have been op-erated on shortly after the ventilationsystem was turned on, indicating possi-ble ventilatory source of infection
Case-control study design leavesroom for unmeasured differencesbetween groups
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY

36 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Harris CS, Bradley RJ, Titus SK. A comparison ofthe effects of hard rock and easy listening on the fre-quency of observed inappropriate behaviors: controlof environmental antecedents in a large public area. J Music Therapy 1992; 29: 6–17
Hard rock vs. easy listeningmusic
Adult male and femaleclients in a large publicarea at a state mentalhealth hospital (n=13,998)
Harwood RH, Ebrahim S. Long-term institutionalresidents: Does the environment affect outcomes? J Royal College of Physicians of London 1992; 26(2):134–138
New and purpose-built wardswith single and twin bedroomsand separate day and diningareas vs. refurbished maternitywards with four-bedded baysand separate day areas
Continuing care resi-dents transferred toRoyal London Hospital(n=95)
Happ BA. The effect of point of care technology onthe quality of patient care. AMIA, Inc. 1994; 183–187
Bedside computers Geriatric patients from 5medical/surgical nursingunits in 3 acute care hos-pitals in the northeasternUSA (n=90)
Hahn JE, Jones MR, Waszkiewicz M. Renovation ofa semi-private patient room. Nurs Clinics of NorthAmerica 1995; 30(1): 97–115
Standard hospital room vs. remodeled room
Patients of the GeriatricRehabilitation Unit atRush Presbyterian–St.Luke’s Medical Center(n=23)
Grauer T. Environmental lighting, behavioral stateand hormonal response in the newborn. Sch Inq NursPract 1989; 3: 53–66
Constant vs. intermittentlight
Healthy newborns, set-ting not described (n=99)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION
Guzzetta CE. Effects of relaxation and music therapyon patients in a coronary care unit with presumptiveacute myocardial infarction. Heart Lung 1989; 18:609–616
Music Patients in a coronary-care unit with the pre-sumptive diagnosis ofacute myocardial infarc-tion (n=80)
Hepner WR, Krause AC, Davis E. Retrolental fibro-plasia and light. Pediatrics 1949; 3: 824–828
Exposure to light vs. shieldingeyes with cotton pads and astocking hood
Premature infants of28–37 weeks’ gestationand 1170–1350 gm birthweights at the ChicagoLying-In Hospital (n=5)

◆ 37
Frequency of inappro-priate behaviors
4 1) Although an observational study,the large number of subjectsmakes confounding unlikely
2) No controls for lyric content orrhythm variations
More inappropriate behavior was observedunder conditions in which rock and rapmusic were played than when easy listen-ing and country music were played
Deaths, changes in dis-ability over 12 monthsrecorded using BarthelIndex and Clifton As-sessment Procedure forthe Elderly (CAPE), be-havioral rating and cog-nitive assessment scales
3 Strong study design with well-vali-dated outcome measures
New wards had no advantage: Patients’Barthel scores improved more on the re-furbished wards (difference 2.5 points at4 months, p <.0005); changes in CAPEscores and mortality rates were similaron the two types of wards
4b Patient satisfactionwith nursing care
Patients without bedside computerswere more satisfied with their care thanwere those with the computers
No examination of differences inpatient populations
4 Satisfaction with patientroom environment in-cluding: bedside accessi-bility, closet accessibili-ty, closet utility, night-stand accessibility,personal item storage,personalization of pa-tient care storage, light-ing, cleanliness, and ap-pearance
Customer satisfaction rose significantlyin all 10 areas in renovated rooms; e.g.,in old room 100% rated closet accessi-bility poor or very poor, in new room57% rated it good or very good
1) Weak study design
2) Small sample size
3) No comparison of patientgroups before and after remodel-ing to examine for possibility of confounding
Salivary cortisol levels2 Experimental trial with sequentialassignment, good study design
Awake babies had rises in cortisol withintermittent light, sleeping babies had afall in cortisol
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
1 Apical heart rates, pe-ripheral temperatures
Music together with relaxation therapyresulted in a greater rise in peripheraltemperatures but no difference in lowerapical heart rates compared with relax-ation therapy alone
Strong study design
Retrolental fibroplasia4b Very small study population. Howev-er, although control data were notpresented, 80% incidence in the studygroup clearly rules out shielding as apreventive measure and thereforelight exposure as the etiology
Four of five infants developed retrolentalfibroplasia

38 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Lidwell OM, Lowbury EJL, Whyte, et al. Infection and sepsis after operations for total hip or knee-joint replacement: influence of ultraclean air, prophylactic antibiotics and other factors. J Hyg Camb 1984, 505–529
Ultraclean air ventilation Surgical patients from 19 hospitals in England,Scotland, and Swedenduring 1975–80 (n=8000)
Hilton BA. Noise in acute patient care areas. Res inNurs & Health 1985; 8: 283–291
Noise level Open-heart-surgery pa-tients on pre- and postop-erative wards and ICU,patients at a large generalhospital, ICU and medicalward patients in a smallteaching hospital, ICUpatients in a small com-munity hospital, all in alarge metropolitan area innorthwest Canada (n=25)
Jolly H, Molyneux P, Newell DJ. A controlled studyof the effect of temperature on premature babies. J Pediatr 1962; 60(6): 889–894
Temperature Premature infants at Plymouth Hospital, England, who requiredincubator nursing(n=214)
Humphreys H, Johnson EM, Warnock DW, et al.An outbreak of aspergillosis in a general ITU. J Hospital Infection 1991; 18(3): 167–177
False ceilings, no artificialventilation, building work adjacent to intensive-therapyunit
Patients in the intensive-therapy unit at BristolRoyal Infirmary (n=229)
Kyriakides GK, Zinneman HH, Hall WH, et al. Immunologic monitoring and aspergillosis in renaltransplant patients. Am J Surgery 1976; 131(2):246–252
Ventilation system contami-nated by bird droppings
Patients who had receivedrenal allografts in the VAHospital in Minneapolis,Minnesota (n=3)
Lamberg-Allardt C. Vitamin D intake, sunlight exposure and 25-Hydroxyvitamin D levels in the elderly during one year. Ann Nutr and Metab 1984;28: 144–150
Exposure to outdoor sunlight Three groups of elderlypeople: 1) long-stay geri-atric patients, 2) old peo-ple’s home occupants, 3) healthy ambulatory persons. A control groupwas of healthy youngerpersons (n=96)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION
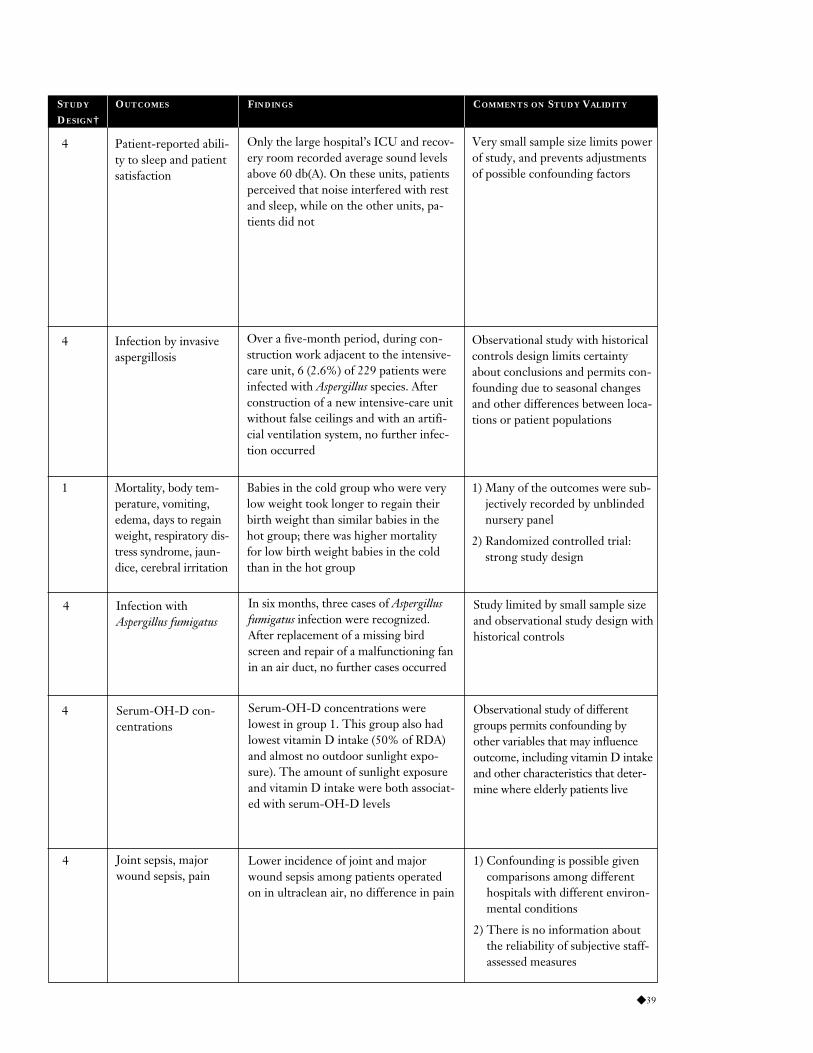
◆ 39
Joint sepsis, majorwound sepsis, pain
4 1) Confounding is possible givencomparisons among differenthospitals with different environ-mental conditions
2) There is no information aboutthe reliability of subjective staff-assessed measures
Lower incidence of joint and majorwound sepsis among patients operatedon in ultraclean air, no difference in pain
4 Patient-reported abili-ty to sleep and patientsatisfaction
Only the large hospital’s ICU and recov-ery room recorded average sound levelsabove 60 db(A). On these units, patientsperceived that noise interfered with restand sleep, while on the other units, pa-tients did not
Very small sample size limits powerof study, and prevents adjustmentsof possible confounding factors
Mortality, body tem-perature, vomiting,edema, days to regainweight, respiratory dis-tress syndrome, jaun-dice, cerebral irritation
1 1) Many of the outcomes were sub-jectively recorded by unblindednursery panel
2) Randomized controlled trial:strong study design
Babies in the cold group who were verylow weight took longer to regain theirbirth weight than similar babies in thehot group; there was higher mortalityfor low birth weight babies in the coldthan in the hot group
Infection by invasiveaspergillosis
4 Observational study with historicalcontrols design limits certaintyabout conclusions and permits con-founding due to seasonal changesand other differences between loca-tions or patient populations
Over a five-month period, during con-struction work adjacent to the intensive-care unit, 6 (2.6%) of 229 patients wereinfected with Aspergillus species. Afterconstruction of a new intensive-care unitwithout false ceilings and with an artifi-cial ventilation system, no further infec-tion occurred
Infection with Aspergillus fumigatus
4 Study limited by small sample sizeand observational study design withhistorical controls
In six months, three cases of Aspergillusfumigatus infection were recognized.After replacement of a missing birdscreen and repair of a malfunctioning fanin an air duct, no further cases occurred
Serum-OH-D con-centrations
4 Observational study of differentgroups permits confounding byother variables that may influenceoutcome, including vitamin D intakeand other characteristics that deter-mine where elderly patients live
Serum-OH-D concentrations were lowest in group 1. This group also hadlowest vitamin D intake (50% of RDA)and almost no outdoor sunlight expo-sure). The amount of sunlight exposureand vitamin D intake were both associat-ed with serum-OH-D levels
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY

40 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Mann NP, Haddow R, Stokes L, et al. Effect of nightand day on preterm infants in a newborn nursery:randomized trial. BMJ 1986; 293: 1265–1267
Light intensity and noise levelreduction in a “night and day”pattern nursery vs. continuouslighting and noise level nursery
Preterm (27–35 weeks)infants with no majorneurological illnesses(n=41)
Melin L, Gotestam KG. The effects of rearrangingward routines on communication and eating behav-iors of psychogeriatric patients. J Appl Behav Anal1981; 14: 47–51
Furniture arrangement: chairsgrouped around tables vs.against corridor walls, brighterlighting, and elimination of in-dividual trays
Psychogeriatric ward pa-tients at a large mentalhospital, with dementiaor schizophrenia (n=21)
Menegazzi JJ, Paris P, Kersteen C, et al. A random-ized controlled trial of the use of music during lacera-tion repair. Ann Emerg Med 1991; 20: 348–350
Headset music chosen by patients
Emergency patients atUniversity of Pittsburghteaching hospital, under-going laceration repair (n=38)
Miller CI, White R, Whitman TL, et al. The effectsof cycled versus noncycled lighting on growth anddevelopment in preterm infants. Infant Behav Dev1995; 18: 87–95
Cycled lighting NICU vs.noncycled lighting NICU
Preterm infants in neona-tal intensive care units(n=41)
Loo VG, Bertrand C, Dixon C., et al. Control ofconstruction-associated nosocomial aspergillosis in an antiquated hematology unit. Infect Control and Hosp Epidemiol 1996, June 17(6): 360–364
Infection-control design fea-tures: high-efficiency particu-late air (HEPA) filter airpurifiers, application of cop-per-8-quinolinolate–formulat-ed paint, replacement ofperforated with nonperforated ceiling tiles, sealing of all win-dows, replacement of horizon-tal, dust-accumulating blindswith vinyl, opaque, rollershades, and systematic andregular cleaning of surfaces
Patients with leukemiaor bone marrow trans-plants in a university ter-tiary-care center with asingle designated hema-tology-oncology unit(n=36)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION
Loesin RGRAC. The effect of music on the pain ofselected postoperative patients. ANOPHI Papers1979: 1–10
Music administered postoper-atively
Subjects undergoing gynecologic surgery atSilliman Hospital, Philippines (n=24)
Miller HC, Behrle FC, Hagar DL, et al. The effect of high humidity on body temperature and oxygenconsumption of newborn premature infants. Pediatrics1961: 740–747
Relative humidity (low vs.high)
Premature infants at the University of KansasMedical Center (n=23, 11)

◆ 41
Time spent sleepingand eating and weightgain
1 1) Excellent design — randomizedtrial and additional stratificationby degree of prematurity
2) Blinding not possible; may biasfindings
3) Reliability and validity of reportsof sleep and eating not tested
Infants randomized to a night and daynursery where the intensity of light andnoise was reduced from 7 p.m. to 7 a.m.spent longer sleeping and less time feed-ing and gained more weight than infantsin a control nursery where the light wasnot reduced
Eating behavior, communication (tactileand verbal contacts)
1 1) Excellent study design, randomassignment to experimentalgroup
2) Excellent interrater reliability of outcome measure
Improved eating behavior in group withaltered furniture arrangement
Heart rate, blood pres-sure, respirations, stateanxiety scale score,pain rating, and ratingof helpfulness of music
1 1) Excellent methods, randomizedcontrolled trial
2) Small sample in one hospitallimits generalizability to otherpopulations
Patients who listened to music theychose during laceration repair had lesspain and similar anxiety levels to thecontrol group
Weight gain, time tooral feeding, daysspent on ventilator andon phototherapy, andmotor coordination
4 1) Small sample size
2) Observational study — higher initial Apgar scores in the cycledlighting group may partly accountfor differences
3) Differences between the twounits besides the lighting wereunmeasured
Compared to infants in the noncycledlighting unit, infants assigned to the cy-cled lighting unit had a greater rate ofweight gain, were able to be fed orallysooner, spent fewer days on the ventila-tor and on phototherapy, and displayedenhanced motor coordination
4 Aspergillus infectionmeasured by mycolo-gy cultures
The incidence density in the precon-struction period was 3.18 per 1000 daysat risk. During construction activity theID increased to 9.88 per 1000 days atrisk. After implementation of infection-control measures, the ID decreased to2.91 per 1000 days at risk
There is no comparison of differentpatient groups to address possibili-ty of confounding
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
Pain ratings1b1 The small sample makes it difficultto generalize
Musculoskeletal and verbal responses topain, blood pressure, and pulse werelower in patients assigned to music
Body temperature,oxygen consumption
3 1) Small sample size limits general-izability
2) Study method fairly strong, ob-servational study with paired data
Increased humidity increased body temperature and did not change oxygenconsumption

42 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Moss VA. Music and the surgical patient. The effect ofmusic on anxiety. AORN Journal 1988; 48(1): 64–69
Music Adult patients admittedfor elective arthroscopicsurgery to be performedunder general anesthesia(n=17)
Nordstrom K, Norback D, Akselsson. Effect of airhumidification on the sick building syndrome andperceived indoor air quality in hospitals — a four-month longitudinal study. Occup Environ Med 1994;51: 683–688
Humidity level Hospital employees infour geriatric hospitalunits in southern Sweden(n=90)
Okken A, Blijham FW, et al. Effects of forced con-vection of heated air on insensible water loss and heatloss in preterm infants in incubators. J Pediatr 1982;101: 108–112
Forced convection of heatedair
Healthy preterm infantson incubators in Univer-sity of Groningen Hos-pital, The Netherlands(n=20)
Parkin SF. The effect of ambient music upon the reactions of children undergoing dental treatment.ASDC J Dent Child: 430–432
Ambient music played for fiveminutes vs. no ambient music
Children about to under-go cavity preparation inthe Children’s Dentistry Department of the Den-tal Hospital at the Uni-versity College LondonDental School, England(n=25)
Pattison HM, Robertson CE. The effect of ward design on the well-being of post-operative patients. J Adv Nursing 1996; 23: 820–826
Long-open “Nightingale”ward vs. ward with bays offour beds each
Postoperative patients atGlenfield Hospital, Leicaster, England(n=64)
Pelosi P, Solca M, Ravagnan I, et al. Effects of heatand moisture exchangers on minute ventilation, ventilatory drive, and work of breathing during pres-sure-support ventilation in acute respiratory failure.Crit Care Med 1996; 24(7): 1184–1188
Gas conditioning in pressure-support ventilation using aheated hot water humidifiervs. using a heat and moistureexchanger
Patients in a universityhospital ICU (n=14)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 43
Change in anxietyfrom pre- to post-operative period
4b 1) Used well-validated instruments
2) Experimental systematic alterna-tive assignment makes it morelikely that results are valid
3) Very small sample reduces generalizability to other patientpopulations and age groups
Results indicated a significant decreasefrom preoperative to postoperative anxi-ety for patients who listened to music.No significant difference was found inthe control group.
3b Sensation of dryness,irritation, and staticelectricity
Air humidification up to a relative humidity of 40–45% decreases the per-ception of dry air and static electricity
Because the same employees werestudied before and after the inter-vention, the improved outcomesare likely due to the interventiondespite the lack of paired analysis
Insensible water loss,heat loss
2 Strong study methods, experimen-tal controlled trial with paired data
Forced convection increased insensiblewater loss, evaporative heat loss, andtotal heat loss, and decreased nonevapo-rative heat loss
Observers’ assessmentof children’s anxiety
2 1) Good reliability: Four indepen-dent observers were used foreach child
2) Good study design: Each childserved as his/her own control in this experimental study withpaired data
3) Generalizability to other popu-lations unknown
There was a significant reduction ofovert anxiety when in the visit with am-bient music prior to the dental proce-dure compared with a control visit inwhich no music was played
4 Patient evaluation ofhealth care, patientevaluation of noise;quality of life in thehospital, includingsleep, friendships, pri-vacy, isolation, anxiety,and depression
The “Nightingale” ward was perceivedas significantly noisier than the bay wardand noise levels were significantly correlated with anxiety scores. 75% ofpatients preferred the bay ward design
No adjustment for patient differ-ences between wards
2 Minute ventilation,static intrinsic positiveend-expiratory pres-sure, ventilatory driveand work of breathing
Insertion of heat and moisture exchang-ers induced a significant increase inminute ventilation, static intrinsic posi-tive end-expiratory pressure, ventilatorydrive, and work of breathing
1) Small sample size
2) Strong study design
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY

44 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Peterson R, Knapp T, Rosen J, et al. The effects offurniture arrangement on the behavior of geriatricpatients. Behav Therapy 1977; 8: 464–467
Patient-determined furniturearrangement with furniturealong the walls of the room,vs. elliptical arrangement ofchairs around a table vs. smallgroupings of tables and chairs
Geriatric patients in astate mental institutionin Nevada (n=20–34)
Salvati EA, Robinson RP, Zeno SM, et al. Infectionrates after 3175 total hip and total knee replacementsperformed with and without a horizontal unidirec-tional filtered air-flow system. J Bone Joint Surg Br1982; 64-A(4): 525–535
Horizontal unidirectional filtered air-flow ventilationsystem
Patients undergoing single-stage total hip re-placement or total kneereplacement at the Hos-pital for Special Surgery,New York (n=3175)
Sauer PJ, Huib DJ, Visser HK. Influence of varia-tions in the ambient humidity on insensible water lossand thermoneutral environment of low birth weightinfants. Acta Paediatr Scand 1984; 73: 615–619
Humidity level Preterm infants gesta-tional age 29–34 weeks,mixed low and appropri-ate weight for gestationalage at Academic HospitalRotterdam/Sophia Chil-dren’s Hospital, TheNetherlands (n=11)
Riegler J. Comparison of a reality orientation program for geriatric patients with and withoutmusic. J Music Therapy 1980; XVII(1): 26–33
Music Geriatric patients under-going reality orientationtherapy at the Châteaude Notre Dame NursingHome, New Orleans,Louisiana (n=8)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION
Reynolds JD, Hardy RJ, Kennedy KA, et al. Lack ofefficacy of light reduction in preventing retinopathyof prematurity. N Engl J Med 1998; 338(22):1572–1576
Reduced visible light versustypical nursery lighting
Premature infants athigh risk for retinopathyof prematurity, based onlow birth weights andgestational ages, hospi-talized in intensive-ther-apy units at one of threestudy sites (n=361)

◆ 45
Observer assessed fre-quency of talking, sit-ting, moving, standing,lying, watching TV,manipulating objects,stereotypy, attending tonursing station, read-ing, touching, coopera-tive behavior, doinghair, and playing withgames or toys
2b It is unclear whether the samegroup of patients was observed inall three conditions. If so, the valid-ity is greater as unmeasured differ-ences could not confound results
The experimental arrangement of smallgroupings of tables and chairs resulted ina higher prevalence of talking. Other be-haviors were unchanged compared tothe baseline of the chairs along the walls.The elliptical arrangement did not resultin any behavioral changes
Postoperative infec-tion rates
4 1) The variable of the laminar flowroom was confounded by the po-sition of the operating team andthe wound relative to the air flow
2) The observational double-cohortstudy design permits confound-ing by unanticipated factors
Patients operated on in the filtered lami-nar flow operating room had reduced infection rates after total hip replace-ment compared with those operated onin conventional operating rooms. How-ever, patients undergoing knee replace-ment in the laminar flow room hadhigher infection rates
Insensible water lossand heat loss
2 Experimental study with paireddata; methods increase likelihoodof validity
Evaporative water loss was 40% lower athigher humidity, while metabolic weightand body temperature were the same
1 Confusion, social with-drawal, and apathy
The control group remained at the samelevel across trials while the experimentalgroup showed marked improvement
1) Very small sample size
2) Confounding possible as differ-ences between patient groupswere not examined
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
Retinopathy of prematurity
1 Randomized controlled trial withblinding is an excellent design.Conclusions may not be generaliz-able to populations of infants at lowrisk of retinopathy of prematurity
There was no significant difference between the incidence of retinopathy ofprematurity in the group that receivedreduced light (54%) and the controlgroup (58%)

46 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Silverman WA, Agate FJ, Fertig JW. A sequential trialof the nonthermal effect of atmospheric humidity onsurvival of premature infants. Am J Dis Child: 77–78
Moderate vs. high humiditylevel
Matched pairs of infants(n=362)
Silverman WA, Blanc WA. The effect of humidity onsurvival of newly born premature infants. Pediatrics1957; 477–487
Moderate vs. high humiditylevel
Premature infants lessthan 120 hours old at Babies Hospital (Colum-bia), New York (n=324)
Shirani KZ, McManus AT, Vaughn GM, et al. Effects of environment on infection in burn patients.Arch Surg 1986; 121: 31–36
Open intensive care ward vs.intensive care ward with sepa-rate bed enclosures with sinksin each enclosure
Burn patients treated inan intensive care ward(n=386)
Shiroiwa Y, Kamiya Y, Uchibori S, et al. Activity, cardiac and respiratory responses of blindfoldedpreterm infants in a neonatal intensive care unit.Early Hum Dev 1986; 14: 259–265
Reduction of environmentallight by blindfolding using aneye mask and a black head-cap
Preterm low birth weightappropriate-for-dates infants in an NICU atSeirei Hamamatsu Gen-eral Hospital, Japan,healthy except for lowbirth weights (n=10)
Sensakovic JW, Smith LG. Nosocomial ultravioletkeratoconjunctivitis. Infection Control 1982; 3(6):475–476
Improperly hung ultravioletlight
Patients and visitors inan isolation room atSaint Michael’s MedicalCenter, Newark, NewJersey (n=5)
Sherertz RJ, Belani A, Kramer BS, et al. Impact of airfiltration on nosocomial Aspergillus infections. Uniquerisk of bone marrow transplant recipients. AmericanJournal of Medicine 1987; 83(4): 709–718
HEPA filtration units withhorizontal laminar flow
Bone marrow transplantrecipients at the Univer-sity of Florida College ofMedicine (n=113)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 47
Mortality rates1 No significant difference in survival was detected under the two humidityconditions
Retractions (respirato-ry distress), mean res-piratory rates, bodytemperature, mortalityrates, proportions ofsterile cultures or dis-tribution of organismscultured
4 Double-cohort observational study design permits confounding by un-measured variables, althoughgroups are similar in demographics,birth weight, cause of prematurity,and route and position of delivery
Better survival at high than moderate humidity, body temperature was a littlehigher at high relative humidity, and therewere no differences in other outcomes
Reasonably good study design: Infants were matched with respectto a number of clinical features(e.g., antibiotics, globulin, andfeedings) and assigned randomly to one of the two conditions
Infection and mortality4 No testing of reliability and validityof documentation of some of therecording-sensitive measures of infection such as “symptomaticbacteriuria”
Burn patients in the separate bed enclosures had fewer infections andlower mortality rates than patients in the open unit
Activity level, respira-tory rate, heart rate
2 1) Experimental paired or within-subjects study design enhancesvalidity
2) Small sample size limits general-izability
3) No information about the relia-bility of observers’ assessment ofactivity from videotapes
Activity was less and respiratory rateswere lower when infants were blindfoldedthan when not blindfolded
Bilateral conjunctivi-tis, erythema
4 Despite small sample size and his-torical controls, causal inference isstrong due to unusual nature ofoutcome and and prior knowledgethat this outcome can be caused byUV light
All five people exposed to direct ultravi-olet light developed keratoconjunctivitis.Three patients also developed skin ery-thema
Nosocomial Aspergillus infections
4 Observational study design andsmall samples limit certainty offindings
14 (19%) of 74 bone marrow transplantrecipients housed outside of a HEPA-filtered environment developed nosoco-mial Aspergillus infections vs. 0 of 39cases in a HEPA-filtered environment
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY

48 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Strauch C, Brandt S, Edwards-Beckett J. Implemen-tation of a quiet hour: effect on noise levels and infantsleep states. Neonatal Network 1983; 12(3): 31–35
Quiet hour in last hour of eachnursing shift vs. control period
Very low birth weight in-fants in a neonatal devel-opmental unit atChildren’s Hospital inColumbus, Ohio (n notstated)
Sulyok E, Jequier, Ryser G. Effect of relative humidity on thermal balance of the newborn infant.Biol Neonate 1972; 21: 210–218
Relative humidity level Healthy newborns onthe first day of life atUniversity MedicalSchool, Lausanne,Switzerland (n=31)
Spaeth GL, Angell MF. Preference of ophthalmic patients for multi-bedded hospital rooms. Arch Ophthal 1968; 79: 362–365
Single vs. multi-bed patientrooms
Ophthalmologic patientsat Wills Eye Hospital inPhiladelphia (n=580)
Soutar RL, Wilson JA. Does hospital noise disturbpatients? BMJ 1986; 292 – 305
Noise level Subjects were patients inthe general medicalwards, acute admissions,and psychiatry wards(n=91)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION
Tideiksarr R, Feiner C, Maby J. Falls prevention: theefficacy of a bed alarm system in an acute-care set-ting. Mt Sinai J Med 1993; 60(6): 522–527
Bed alarm system Geriatric patients withpoor mobility due toacute medical or chronicneuromuscular condi-tions in an acute-caresetting (n=70)

◆ 49
Infant behavior andsleep state (deep, light,drowsy/semidozing,quiet awake, activeawake, and crying)
3 1) Repeated measures design allowseach infant to serve as his or herown control; nonrandomized toquiet hour
2) No information about reliabilityand validity of observed stateand behavior
Fewer infants were crying during thequiet hour than the control period (2.4vs. 14.3%), and more were in deep orlight sleep (84.5 vs. 33.9%)
Activity level, evapo-rative, dry, and totalheat loss, skin temper-ature
4 Triple-cohort observational studyis nonrandomized and permits con-founding by unmeasured differ-ences among the groups
Evaporative heat loss is greater in lowerhumidity conditions, dry heat loss isgreater at higher humidity (80%), heatstorage and temperature are higher, andthe metabolic rate is minimal at 50%,and either increasing or decreasing hu-midity causes a rise in the metabolic rate
1 Patient satisfactionwith type of room,preference for type of room
After discharge, 92% of patients report-ed a preference for multi-bed rooms,with no difference between those whohad been admitted to single or multi-bed rooms.
Few differences between patientgroups were examined, so othervariables may confound the com-parison
Disturbance of patients’ sleep due tonoise as reported bypatient
42 1) Poor study design: There is nocontrol group and no comparisonof patients at different noise levels
2) Patient self-report of worse sleepdue to noise is of unknown validity
3) There is no information about thecharacteristics of study subjects,making it difficult to generalize toother groups of patients
Of 91 patients interviewed, 39 claimedtheir sleep was unaltered in the hospitalas compared with home, 28 slept worsein the hospital, and 24 slept better. Ofthe 28 who slept worse in hospital, 9stated this was due to noise
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
1 Bed falls There was no statistically significant dif-ference in falls between the experimentalgroup and the control group (5 vs. 12,p=1.00). However, in the experimentalgroup the utilization of mechanical re-straints to guard against bed falls declined
1) Small sample size with conse-quent limited power to detectdifference; falls were less thanhalf in the experimental groupwithout statistical significancebeing achieved
2) The difference in mechanical-re-straint use between groups alsomay have minimized the ob-served effect of the alarm system

50 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Topf M. Effects of personal control over hospitalnoise on sleep. Res Nurs Health 1992; 15: 19–28
Noise level and personal control over noise using asound conditioner
Healthy women volun-teers, with no sleep orhearing problems, in asleep lab (n=105)
Topf M, Davis JE. Critical care unit noise and rapideye movement (REM) sleep. Heart Lung 1993; 22(3):252–258
Noise level Healthy women volun-teers with no hearing orsleep problems in a sleeplab (n=105)
Topf M. Noise-induced stress in hospital patients:coping and nonauditory health outcomes. J HumStress 1985: 125–134
Noise level and personal control over noise
Volunteer male surgerypatients in a large metro-politan VA hospital(n=150)
Topf M. Stress effects of personal control over hospi-tal noise. Behav Med 1992; 18: 84–94
Noise level, personal controlover noise
Women volunteers paidto participate, averageage 35, level of educa-tion 17 years (U of Colorado) (n=105)
Timko C. Physical characteristics of residential psy-chiatric and substance abuse programs: organizationaldeterminants and patient outcomes. American Journalof Community Psychology 1996; 24(1): 173–192
Score on scale measuring a vari-ety of physical and architecturalfeatures, including proximity tocommunity, availability of resources, space, and design offurniture layout to promote so-cial interaction, space for staff,outdoor areas, accessibility offacilities to those with disabili-ties or wheelchairs, safety features, and amount of space
Patients in inpatient, residential psychiatricand substance abusetreatment settings in sixSan Francisco Bay–areacounties (n=94)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 51
1 1) Excellent design (randomizedtrial)
2) Generalizability from volunteersin a sleep lab to critical care unitpatients is questionable
Noise levels characteristic of critical careunits caused poorer sleep but personalcontrol using a sound conditioner hadno effect
Coping, i.e., degree ofcontrol exercised overnoise, self-ratings ofrecovery, time out ofbed
1 1) Randomized trial: good studydesign for portion of study ana-lyzing effect of personal controlof noise, comparable groups
2) Outcome measure with good in-ternal consistency and concur-rent validity for one part of thestudy
Personal control over noise resulted inmore time out of bed but no differencein self-ratings of recovery
Sensitivity to noise,subjective stress, exer-cised control over noise
1 1) Randomized trial: good studydesign for portion of study ex-amining personal control ofnoise
2) Carefully designed measures oftested internal consistency andcontrols for social desirability
3) Volunteers may not be general-izable to patients
Noise is associated with subjective butnot physiological stress; personal con-trol over sound using a sound condition-er did not affect stress
20 measures of sleep, in-cluding 19 physiologic(including sleep efficien-cy, minutes and percentof time in bed, awake,asleep, in each stage ofsleep, latencies to eachstage, number of stageshifts, intrasleep awak-enings, REM periods)and one self-reportmeasure
REM activity, REMdensity, and REM duration
1 Generalization of results to criticalcare unit patients is limited becauseof use of laboratory subjects
Subjects in the noise condition showedpoorer REM sleep on 7 of the 10 mea-sures
Successful completionof program, dischargeto independent livingand paid jobs
4 Observational study design permitsconfounding by other factors aboutpatients or facilities that may influ-ence outcomes
Programs with more physical amenitieshad patients who were more likely tosuccessfully complete the program andbe discharged to independent living situ-ations and paid jobs. Programs withmore social-recreational and prostheticaids, space, and access to community re-sources also had better patient outcomes
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
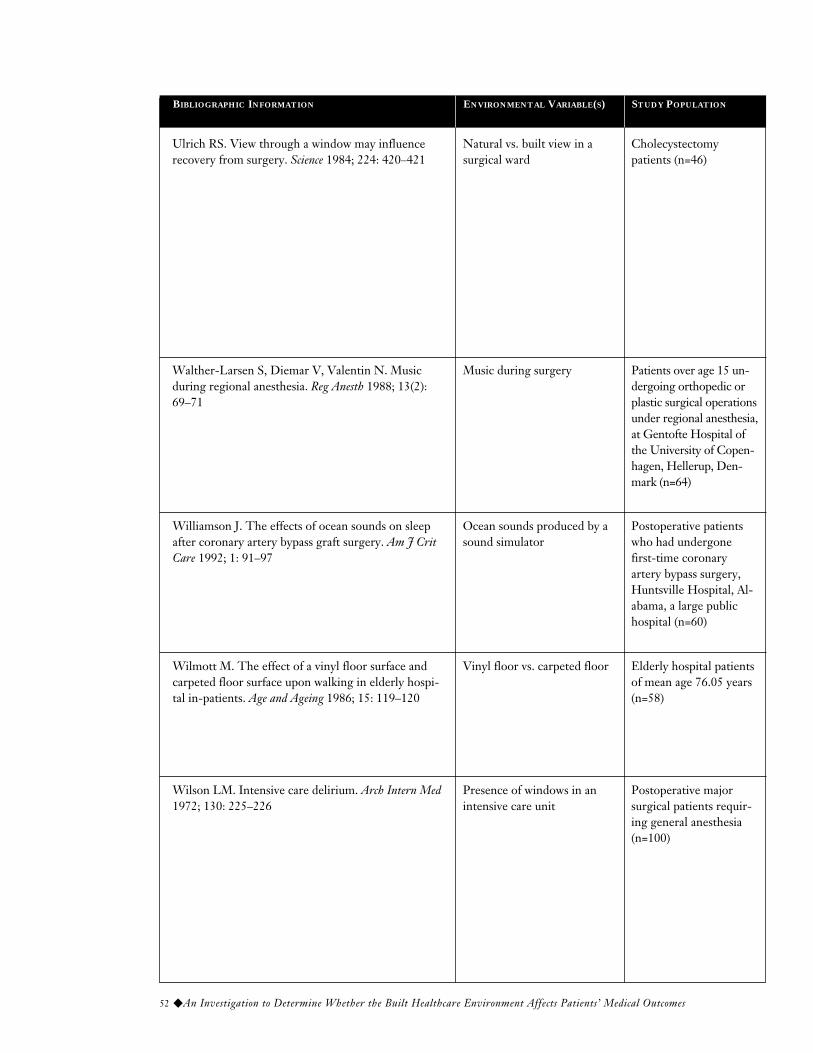
52 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Williamson J. The effects of ocean sounds on sleepafter coronary artery bypass graft surgery. Am J CritCare 1992; 1: 91–97
Ocean sounds produced by asound simulator
Postoperative patientswho had undergonefirst-time coronaryartery bypass surgery,Huntsville Hospital, Al-abama, a large publichospital (n=60)
Wilson LM. Intensive care delirium. Arch Intern Med1972; 130: 225–226
Presence of windows in an intensive care unit
Postoperative major surgical patients requir-ing general anesthesia(n=100)
Wilmott M. The effect of a vinyl floor surface andcarpeted floor surface upon walking in elderly hospi-tal in-patients. Age and Ageing 1986; 15: 119–120
Vinyl floor vs. carpeted floor Elderly hospital patientsof mean age 76.05 years(n=58)
Ulrich RS. View through a window may influence recovery from surgery. Science 1984; 224: 420–421
Natural vs. built view in a surgical ward
Cholecystectomy patients (n=46)
Walther-Larsen S, Diemar V, Valentin N. Musicduring regional anesthesia. Reg Anesth 1988; 13(2):69–71
Music during surgery Patients over age 15 un-dergoing orthopedic orplastic surgical operationsunder regional anesthesia,at Gentofte Hospital ofthe University of Copen-hagen, Hellerup, Den-mark (n=64)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 53
Sleep questionnaire,sleep scores
1b3 Experimental controlled trial withsystematic assignment, goodmethod
Group receiving ocean sounds perceivedthat they had slept better than the controlgroup, and were awake less during thenight, returned to sleep more quickly, andhad higher sleep quality and total sleepscores. There was no difference in fallingasleep scores
Delirium and depression
4 1) Only one unit with or withoutwindows studied — units maydiffer in other ways that affectpatient outcomes.
2) No risk adjustment — observa-tional study. Patients in twounits may differ in unmeasuredvariables
Over twice as many episodes of organicdelirium were seen in the intensive careunit without windows as in the unit withwindows
2 Mean gait speed and step length weresignificantly greater on carpet than onvinyl. Patients expressed fear of walkingon vinyl, none on carpet. In almost 25%of cases (14 patients), step length was30% greater or more
Paired study design supports validity
Walking efficiencyand confidence weredefined by gait speedand step length
Length of hospitalstay, negative evalua-tive comments innurses’ notes, amountof potent analgesicstaken
4 1) One hospital setting and smallsample size — issues of generaliz-ability
2) Unmeasured differences betweenpatients possible (including indi-cation for cholecystectomy, mor-bid illness, physiologic severity ofillness, and initial pain levels)
3) Built view closest to nursing sta-tion — there may be unmeasureddifferences such as more noise inthe built view portion
Patients assigned to rooms with windowviews of a natural setting had shorterpostoperative hospital stays, receivedfewer negative evaluative comments innurses’ notes, and took fewer potentanalgesics than patients in similar roomswith windows facing a brick wall
Requirement for seda-tives, anxiety duringsurgery
1 Strong study designFewer patients in the music group thanin the nonmusic group needed sedatives(4 of 32, 13%, versus 14 of 32, 44%) al-though a significantly higher proportionof patients in the music group recalledfeeling anxious during surgery
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY

54 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Zahr LK, Balian S. Responses of premature infants toroutine nursing interventions and noise in the NICU.Nurs Res 1995; 44: 179–185
Noise events Premature infants in theNICU, 23–37 weeks ofgestational age, 480–1930 g, at three largeuniversity hospitals inCalifornia and in Beirut,Lebanon (n=55)
Zimmerman LM, Pierson MA, Marker J. Effects ofmusic on patient anxiety in coronary care units. HeartLung 1988; 17: 560–566
Relaxation-type music withsuggestion, synthetic silencewith suggestion vs. controlgroup
Patients with suspectedmyocardial infarction ad-mitted to three CCUs inthe Midwest (n=75)
Wolff PH, Matsumiya Y, Abroms IF, et al. The effectof white noise on the somatosensory evoked responsein sleeping newborn infants. Electroencephalogr ClinNeurophysiol 1974; 37: 269–274
White noise delivered byspeakers on either side of infant’s head
Full-term, normal birthweight neonates on thethird or fourth day afterdelivery at Children’sHospital, Boston (n=21)
Yeh TF, Voora S, Lilien D, et al. Oxygen consump-tion and insensible water loss in premature infants insingle- versus double-walled incubators. J Pediatr1980; 97: 967–971
Single- vs. double-walled incubators
Premature infants appro-priate for dates, gesta-tional age 31–34 weeks,age 4–15 days old, atCook County Children’sHospital (n=10)
ENVIRONMENTAL VARIABLE(S)BIBLIOGRAPHIC INFORMATION STUDY POPULATION

◆ 55
Heart rate, respiratoryrate, oxygen satura-tion, sleep and wakestates
3b Group-level anaysis of data beforeand after limits power of study;paired data were not analyzed forstatistical significance
Noise resulted in fall in oxygen satura-tion, rise in heart rate, and rise in respi-ratory rate in 12–18% of infants. 78% ofinfants changed their behavioral state inresponse to noise, usually from sleepstate to fussy/crying state
State and trait anxiety,blood pressure, heartrate, digital skin temperature
1 (1) Randomized clinical trial en-hances confidence in validity
(2) Outcome measures tested forreliability and validity
No difference in state anxiety, heart rate,blood pressure, or skin temperature
Somatosensory-evoked response
2 1) Experimental controlled trial,within-subjects paired data, enhances study validity
2) Small sample size limits general-izability
White noise enhanced the amplitudeand prolonged the latency of the latecomponents of the somatosensory-evoked response in sleeping newborns
Oxygen consumptionand insensible waterloss
2 1) Small sample size limits general-izability
2) Experimental controlled trialwith paired within-subjects dataenhances validity
The double-walled-incubator infantshad lower insensible water loss andlower oxygen consumption, with a netcaloric saving of 11 kcal/kg/day
STUDY
DESIGN†OUTCOMES FINDINGS COMMENTS ON STUDY VALIDITY
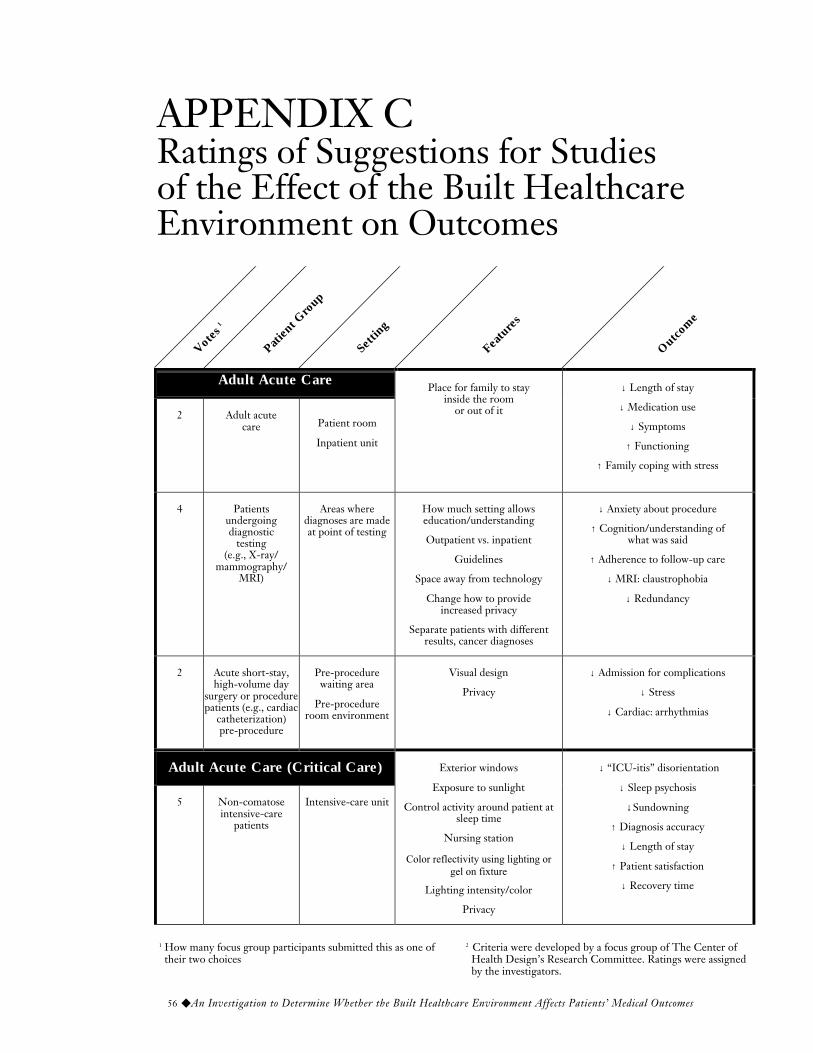
56 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Adult Acute Care
2 Adult acutecare Patient room
Inpatient unit
Place for family to stayinside the room
or out of it
↓ Length of stay
↓ Medication use
↓ Symptoms
↑ Functioning
↑ Family coping with stress
4 Patientsundergoingdiagnostic
testing(e.g., X-ray/
mammography/MRI)
Areas wherediagnoses are madeat point of testing
How much setting allowseducation/understanding
Outpatient vs. inpatient
Guidelines
Space away from technology
Change how to provideincreased privacy
Separate patients with differentresults, cancer diagnoses
↓ Anxiety about procedure
↑ Cognition/understanding ofwhat was said
↑ Adherence to follow-up care
↓ MRI: claustrophobia
↓ Redundancy
2 Acute short-stay,high-volume day
surgery or procedurepatients (e.g., cardiac
catheterization)pre-procedure
Pre-procedurewaiting area
Pre-procedureroom environment
Visual design
Privacy
↓ Admission for complications
↓ Stress
↓ Cardiac: arrhythmias
Adult Acute Care (Critical Care)
5 Non-comatoseintensive-care
patients
Intensive-care unit
Exterior windows
Exposure to sunlight
Control activity around patient atsleep time
Nursing station
Color reflectivity using lighting orgel on fixture
Lighting intensity/color
Privacy
↓ “ICU-itis” disorientation
↓ Sleep psychosis
↓Sundowning
↑ Diagnosis accuracy
↓ Length of stay
↑ Patient satisfaction
↓ Recovery time
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome
1 How many focus group participants submitted this as one of their two choices
2 Criteria were developed by a focus group of The Center of Health Design’s Research Committee. Ratings were assigned by the investigators.
APPENDIX C Ratings of Suggestions for Studies of the Effect of the Built HealthcareEnvironment on Outcomes

◆ 57
3 3 3 3 2.5 3 2 2 1.5 1.5 24.5
2 2 2 2 1.5 2 2 2 2 2 19.5
2 3 3 3 2 3 3 1 2 2.5 24.5
3 2.5 3 3 3 3 3 2 2 1.5 24
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3
3 A total score is provided summing up all criteria; this is not meant to support its use as a summary score. The reader may wish to weigh some criteria more than others.
RATING LEGEND
1 = lowest, 3 = highest, ? = insufficient information

58 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
2 Cardiacpatients/admissions
with myocardialinfarction
Critical-careunit
Noise
Disruptions (blood pressure cuff)
Light and lighting
Discomfort of monitor on chest
IV pole to push to bathroom
Room for family to be with patient
↓ Fear/anxiety
↑ Understanding
↓ Blood pressure
↓ Heart rate
↑ Stability (cardiac) indicator
↓ Intake of various drugs
↑ Quality indicator of visits from family
4 Critical carevarious
diagnoses
Acute-carehospital
Intensive-careunit
Privacy
Music/audio
Lighting
Color
Bathroom facility toaccommodate those who
request more than a bedpan
Remove fluorescent light
Minimize sounds ofmachines/alarms
Keep door closed
Carpet floor
Align bed to see outside thewindow
Block off glass doors for privacy
Add pictures on walls
Convert two-bed roomsto singles
Window behind head or tothe side so patient can see
change of day to night
↑ Comfort
↓ Length of stay
↓ Days in intensive-care unit
↑ Six-month survival
↓ Circadian rhythm andICU psychosis
↑ Patient’s retrospectivememory of the incident
Surgery and Procedures
2 General adult daysurgery
Outpatientrecovery room
Color
Location of technology
Plants, carpets, smells, sounds
Touch by staff
Lighting
Home features, furniture,seating
↓ Inpatient admissions
↓ Readmissions
↓ Recovery time
↓ Complications
↑ Patient satisfaction
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 59
3 2.5 3 2 2 2 2 2.5 2.5 2.5 24
3 3 3 3 3 3 3 2 2 2 27
2 2 3 2 2 3 2 3 3 3 25
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

60 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
1 Cardiacangiography
Acute-carehospital
Control over light, temperature,and noise
↓ Stress
↓ Anxiety
↑ Wellness
8 Cardiac surgerypostoperative
patients
Surgical intensive-care unit
Improved visual design of placefor family to sit (e.g., alcove
with bench and mural ofnature scene)
Reducing noise level
Painting ceiling tiles above bed
Giving patients something to seewhen they are awake
↓ Length of stay
↑ Patient satisfaction
↑ Mobility
↓ Extubation time
↓ Complications
1 Baby boomersnonelective
surgery
Patient andcare partner
Ambulatorysurgery facility
Waiting andregistration
area
Music, TV, video,telecomm, vistas
Sensitivity of staff
Flexible-use space,furniture, electronics
Information and educationregarding care
↓ Stress during waiting period
↑ Satisfaction regardinginformation and training
Ambulatory Adult Operations
1 All adult andambulatory
patients
Hospital lobby
Increased flexibility ofenvironment
↑ Choice of privacy
Variety of lighting
Convenient access
↑ Access
↑ Comfort
↑ Compliance
↑ Family and visitor participation
↓ Stress
1 All who seekoutpatienttreatment
Outpatientregistration
All environmental featuresthat encourage and facilitate easeof access—wayfinding, visibility,
privacy, comfort, lighting,clearer signage
↓ Rate at which treatmentis sought from time condition
is first realized
1 Well adultoutpatients
MD office: arrival,registration,
waiting, exams
Privacy at registration
Sufficient waiting for patients tobe separate
Provision for distraction
Privacy, but ability to knowwhere physician is in exam room
Privacy re billing on exit
↑ Interest in returning
↓ Stress
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 61
2 2 3 2 2 3 2 3 3 3 25
2 3 3 3 2 3 3 1 2 2.5 24.5
2 2 1 1 1 3 3 3 3 3 22
1 2 3 1 2 2 3 2 1.5 2.5 20
1 2 2 2 3 2.5 3 2 2 3 22.5
1 1 3 3 3 3 2.5 2 2 2.5 23
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

62 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
1 Ambulatorydiabetic
The home assite for self-care
Access to entrance
Accessibility of bathrooms,cabinets, kitchen appliances
Use of computers
↑ Recovery
Chronically Ill Adults inResidential Facilities
1 Adultchronic care
Care unit wherepatients reside
for long periods
(Not specified) ↑ Healing
1 Patients withmultiplesclerosis
(age 20–30)
Long-term care Mechanical devices to abetcommunication and mobility
↓ Anxiety
↑ Function
↑ Wellness
↑ Feeling of usefulness
4 Rehabilitation Rehabilitationfacility
Access to nature
Space available for“normalizing” environment
Dining/activity areas
↑ Patient satisfaction
↑ Reports of evaluation of care
↓ Length of stay
↑ Well-being
↑ Relation of patient evaluationto their expectations
1 Traumatic braininjury
Rehabilitationfacility
Room design to enhancemobility, sociability, and the
recovery process
↑ Patient’s control of his/herenvironment
↑ Functionality measured byFunctional Independence
Measure
↓ Length of stay
2 Palliative care,terminally ill
patients
Hospice orinpatient units for
terminallyill patients
View/connection withoutdoors, world outside
↑ “Dying with dignity”
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 63
2 2 3 2 1 2 1 2 2 2 19
3 ? ? 2 ? ? ? ? ? ? 5
3 3 2 3 2 2 2.5 3 3 3 26.5
3 2 3 2 3 3 2.5 2 2 2 24.5
3 3 3 3 2 3 3 2.5 2.5 2.5 27.5
3 3 1 3 1.5 3 2.5 2 2 2 23
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

64 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
2 Cognitiveimpairment/functionallyindependent
Long-term care Control of temperature, lighting
Access to toilet
Access to outside
Access to emergency exits
Movement, e.g., surfaces,thresholds, sizes of door frames,weight of furniture, automatic
doors, elevators vs. stairs
↑ Outcomes that are most likely tohave an interrelationship with thephysical environment and are most
meaningful in healthcare
↑ Relief of suffering
↑ Familiarity
↑ Caring communications
↑ Independence
Elderly Long-Term Care
10 Elderly in long-term care
Long-term carefacility
Provision for history recall
Features to increase memory
Access to nature
Provision for family
Auditory environment(outdoor setting, forest sounds,
transporting sounds)
Promote staff healingenvironment for themselves
Flexibility of environment toaccommodate increasing levelof care needed so patient doesnot need to move, e.g., mobile
home on campus
Bathroom design
Access for walker space
Access to more functions
↓ Cost
↓ Depression
↑ Independence (cook/care forthemselves)
↑ Quality of life
↑ Social interaction
↑ Ambulation
↑ Continence
↓ Medication use
↓ Bedsores
↑ Acceptability of patients toother patients
↑ Happiness
↑ Interaction at dining table
↑ Patient satisfaction
↑ Patient acceptance
↑ Patient self-esteem
1 Elderly Long-term carepatient rooms
Color
Gardens/patios
↓ Noise
Design with residentialhierarchy of public to private
Homelike, familiar attributes
↓ Length of stay
↓ Medication
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 65
3 3 3 3 1.5 3 3 3 1.5 1.5 25.5
3 3 3 3 2 3 3 2.5 3 2.5 28
3 2.5 3 2.5 2 3 2.5 2 2.5 2.5 25.5
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

66 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
2 Elderlyfrail
Assistedliving and
senior livingfacility
Lighting
Washroom access
Upgrade the bathroom systembeyond ADA requirements
Carpeting/obstacles
Space to transfer to toilet
Toilet height
Space to hang clothingin bathroom
Shelves
Privacy
↑ Convenience
↑ Function
↓ Length of stay
↑ Orientation
↓ Agitation
↓ Falls
↑ Autonomy
1 Frail non-demented
elderly
Long-termfacility
Humanization, e.g.,playgrounds
Environment that facilitatesvisiting with people
Connection with people, e.g.,Internet
↑ Patient satisfactionwith environment
↑ Patient happiness, anxiety
↓ Family stress, fear
↑ Patient dignity
1 Elderlycognitivelyintact/frail
assistance with2–4 ADLs
Long-termcare
commonspaces
Walking distances that arereasonable to common spaces
form units
Smaller, domestic scale
Residential amenities
Home setting
Area for intergenerationalinteractivity (kids, plants,
animals)
Flexibility of layout fordifferent settings
↑ Independence
↑ Socialization
↑ Quality of life
↑ Safety
↑ Happiness, well-being
↑ Fulfilled life
1 Elderlyafter late
middle age withlife-threateningincapacitating
diagnosis
Long-term careAccessibility
Independence
Comfort: color, temperature,etc.
Activities
Safety
↑ Quality of life
↑ Hope
↑ Enjoyment
1 Alzheimer’s(age 70 +)
Long-term caremodules of+/- 42 beds
Room configuration
Common area design
Eating area
↑ Sociability
↓ Stress
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 67
3 3 3 2.5 3 3 3 3 2 2 27.5
3 3 3 3 2 3 3 2 2 3 27
3 3 3 2.5 2 3 3 2.5 2 2.5 26.5
3 2.5 3 3 2 3 2.5 3 3 3 28
3 2 2 2 2 3 2.5 2.5 1 3 23
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

68 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
2 Alzheimer’s/dementia
(especially inpalliative care)
Not specified Gardens as rooms
Courtyard with rails
Gardens as private area forfamily
Acoustics/water, wind chimes
Landscaping
Lighting
↑ Comfort/relief
↓ Aggression
↓ Agitation
↓ Conflict
↓ Depression
↑ Family involvement
↓ Medication for aggression
1 Elderly/dementia (up to
Alzheimer’s)and somephysical
limitations
Nursing home Homelike atmosphere withplayground for kids
Cooking activity to promotefamily to come in and involve
themselves with resident
Make it extension of home
↑ Positive distraction
↑ Family involved
↑ Satisfaction
↑ Interest
1 Elderlycognitivelyimpaired,
some ADLimpairment
Medically stable
Nursing unit Wayfinding
Seating
Ability to get up
Doors—ability to operate
↑ Independence on Activity ofDaily Living measures
or by observation
1 Elderlycognitivelyimpaired/
frail/stroke
Long-term care Scale adjustment in room
Ease of movement
Stimulate by noise, vision,interaction
Toilet rooms: soft materialand usable toiletries
↑ Independence
↓ Infection control and odor
↑ Willingness to leave the roomand live + happiness
Elderly Acute Care
5 Acutely illelderly with
reduced mentalstatus
Acute-carehospital
Special space for this typeof patient cluster
Space for family and patientinteraction
Marking safety features
Easy access
Outdoor view
Educational opportunitiesand space for families
↑ Orientation
↓ Injury
↑ Activities of daily living;functional status
↑ Self-care ability
↓ Length of stay
↓ Costs
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 69
3 3 3 3 2 3 3 2 1 2 25
3 2 3 3 3 3 3 2 1 3 26
3 3 3 2 2 3 3 2.5 3 2.5 27
3 3 3 2 2 3 2.5 2.5 2 2.5 25.5
3 3 3 3 3 3 3 2.5 2 2.5 28
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

70 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
3 Elderly surgical Surgicalintensive-care
unit
↓ Noise
↓ Artificial light
Provide views to natural setting(sky, trees, or garden) from
patient bed
↓ Intensive-care unit psychosis
↓ Length of stay
↑ Willingness to undergosurgery and be in surgicalintensive-care unit again
↓ Mortality
↑ Six-month survival
Elderly Outpatient
2 Elderlyoutpatient
Ambulatory-carecenter
Location where services areprovided to the public
Increased accessibility
Convenience
↑ Patient satisfaction
↑ Accessibility↑ Convenience
↑ Speed of getting in and out
1 Elderlyoutpatient
Outpatientclinic
Garden access view fromwaiting room
Social activities
↑ Survival
↑ Level of physical function
↓ Need for pain medication
1 Elderly, frail;cognitively stable
Ambulatorytreatment
Seating
Access to bathrooms
Layout of bathrooms
Temperature
Access to food
↓ Agitation
1 Elderly outpatientlosing mental
abilities; unableto decide whatis right to do
Physician’soffice
consultation
Elimination of“intimidating” desk and degrees
on wall
↑ Positive choice
Elderly (Other)
1 Geriatricpsychiatric
Inpatient
Color
Gardens/patios
↓ Noise
Design with residentialhierarchy of public to private
↓ Aggression
↓ Medication
↑ Other standard measures
↑ Quality of life
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 71
3 3 3 3 3 3 3 2.5 2 2.5 28
2 1.5 3 2 2.5 3 3 3 2.5 3 25.5
2 3 3 2 2 3 1 2 2 2.5 22.5
2 2 2 2 2 3 3 2 2 2.5 22.5
3 1 2 2 2 3 ? 3 3 3 22
3 3 3 2 2.5 3 3 2.5 2 2.5 26.5
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3
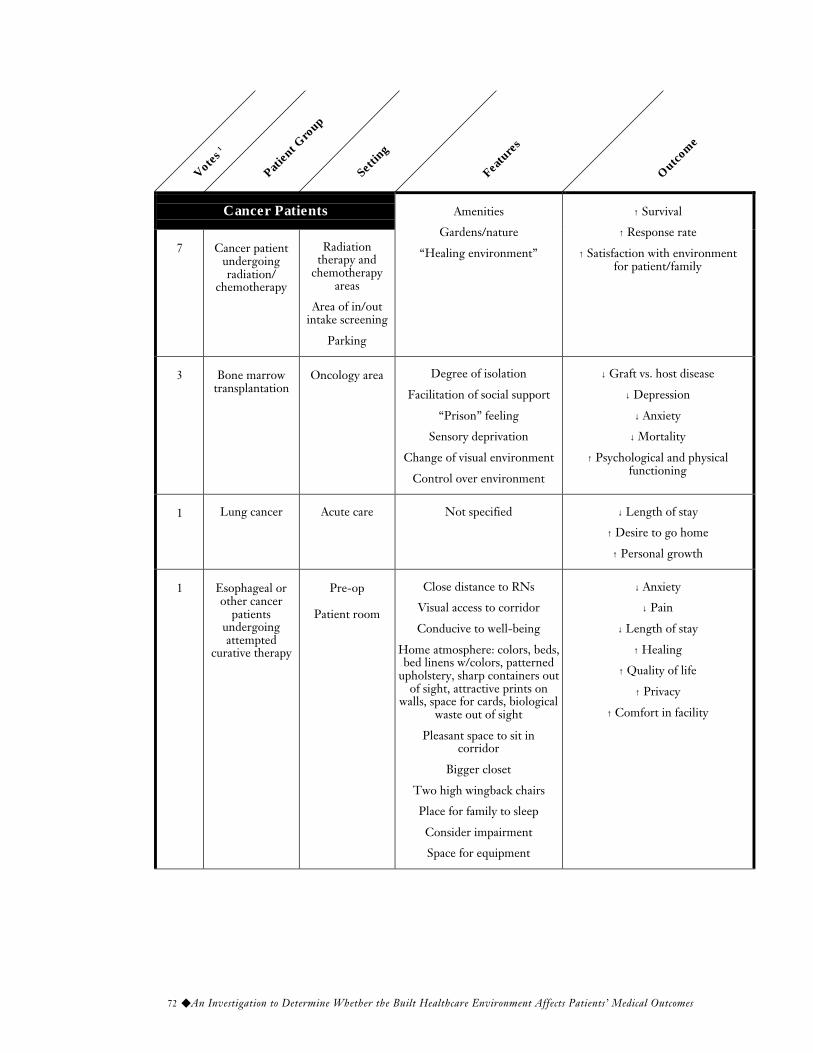
72 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Cancer Patients
7 Cancer patientundergoingradiation/
chemotherapy
Radiationtherapy and
chemotherapyareas
Area of in/outintake screening
Parking
Amenities
Gardens/nature
“Healing environment”
↑ Survival
↑ Response rate
↑ Satisfaction with environmentfor patient/family
3 Bone marrowtransplantation
Oncology area Degree of isolation
Facilitation of social support
“Prison” feeling
Sensory deprivation
Change of visual environment
Control over environment
↓ Graft vs. host disease
↓ Depression
↓ Anxiety
↓ Mortality
↑ Psychological and physicalfunctioning
1 Lung cancer Acute care Not specified ↓ Length of stay
↑ Desire to go home
↑ Personal growth
1 Esophageal orother cancer
patientsundergoingattempted
curative therapy
Pre-op
Patient room
Close distance to RNs
Visual access to corridor
Conducive to well-being
Home atmosphere: colors, beds,bed linens w/colors, patterned
upholstery, sharp containers outof sight, attractive prints on
walls, space for cards, biologicalwaste out of sight
Pleasant space to sit incorridor
Bigger closet
Two high wingback chairs
Place for family to sleep
Consider impairment
Space for equipment
↓ Anxiety
↓ Pain
↓ Length of stay
↑ Healing
↑ Quality of life
↑ Privacy
↑ Comfort in facility
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 73
2.5 3 2 3 3 3 2 2.5 2.5 2.5 26
3 3 1 2.5 2 3 2.5 3 3 3 26
3 2.5 2.5 ? ? ? ? ? ? ? 8
3 3 3 3 3 3 2 2.5 2.5 3 28
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

74 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
1 Adult oradolescent
canceroutpatient
Private or groupsetting
Outpatientambulatory
setting
Presence of plants, aquariums,living things (butterflies, e.g.)
Control for subdued lighting,full spectrum and specular
natural sounds in threedimensions
Acoustic control
Aromatherapy controls
Alternate seating/wing choices
↑ Efficacy of chemotherapy
↓ Amount of chemotherapy
↓ Drugs/cost
↓ Duration of treatment required(# visits total time)
↑ Clinical outcome measures
Adolescents
2 Adolescentinpatients,terminal;
progressionlong/short
Acute care
Therapeuticintervention
Step-downintensive-care
unit
Control of interactions withpatients, staff, visitors
Lounges for small groups
Interaction, entertainment areas
Pain medication request
Stress
Length of stay
Parent participation
↑ Self-esteem — feeling of supportthrough progressive process
↑ Visual or physical access tosocial space
Children
4 Pediatrics Inpatient
Access to outdoor play ↓ Pain medication request
↓ Stress
↓ Length of stay
↓ Pain
↑ Parent participation
1 Pediatricsoncology
Patient room Control over: temperature,light, sound
“Personalization” withpersonal belongings
Color
“Homelike,” residential-typedesign features
Room-size capability
Parent accommodations, i.e.,lounge, showers, kitchen
↑ Comfort
↑ Psychological and physicalpeacefulness
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 75
3 2.5 1.5 3 2 3 2 3 3 3 26
3 2 2 3 2 3 3 2 2 2 24
3 2 3 3 3 3 3 3 3 2.5 28.5
3 2.5 3 3 2 3 3 3 3 2.5 28
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

76 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
2 Pediatricinpatient with
chronic orterminal illness
Intensive-careunit
Inpatient unit
Give back childhood
↑ Control
↓ Isolation
↓ Removed from peers
“Star Bright” virtual connectionto others (Internet)
↑ Family, parents, and siblings(offer environment for them)
↑ Feature that are “fun”
↑ Self-esteem
↑ Recovery
↑ Control
↑ Empowerment
↓ Family stress
1 Schoolchildrenwho are sick andare staying home
from school
Theirresidences
Increased degree ofpersonal privacy
↑ Rate of recovery untilreturn to school
1 Critically illchildren
Pediatricintensive-care
unit
Sleeping facility for parents
Transition room for goinghome to do care
Massage prescription
Reduction of noise
Conference room so child doesnot hear parent/provider
discussions
Family sleeping area
↓ Fear
↑ Sleep
↓ Anxiety
↑ Child’s psychologicaladjustment
↓ Recovery time
↑ Recovery rate
↓ Length of stay
6 Neonates Neonatalintensive-care
unit
Individual rooms for eachbaby with parents
Sleeping facility for parents
Lighting, sound
Music in crib or in room
Transition room for goinghome to do care
Massage prescription
Facilitate contact/touch betweenparent and baby
Privacy for parentsregarding poor prognosis
↑ Relax kids, parents, staff
↑ Weight gain and faster inneonatal intensive-care unit
↓ Abuse
↑ Bonding
↓ Length of stay
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 77
3 3 3 3 3 3 2 3 3 3 29
2 2 1 2 1 1 1 2 1 1 14
3 2.5 2 3 3 3 2 2 2 2 24.5
3 2 1 3 2 3 2 3 2.5 2.5 24
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

78 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
Emergency
9 Emergencypatients
ER rooms
ER waitingroom
Security systems
Fireplace
Waterfall
Fountain
Privacy
Control over TV
More isolation from otherpatients
Separation of levels of care
Don’t roll patients throughER waiting room
Access to patients for family
Privacy of conversation
Individual rooms
Quiet space for teachingpatients before leaving ER
Specific ER section — morespace for wheelchairs/geriatric
“Geri” assessment area in ER
Place for family/advocate
Lighting
Compare design atvarious sites
↓ Stress/anxiety
↓ Violence
↓ Parental and family anxiety
↓ Anxiety in ER
↑ Knowledge, understandingof diagnosis
↑ Medication doses beingtaken correctly
↑ Follow-up
↑ Efficiency of patient flow
↓ Cost/case
↑ Staff-patient ratios
Clinical outcome ofsimilar patient
↑ Patient satisfaction withexperience
1 Pregnantwomen
Birthing rooms Patient control of environment,light, temperature, privacy
Ability for rooming in
Size of room
Configuration of room
Introduction of positivedistraction: access to nature,
music, bathing,A/V equipment
↓ Anxiety
↑ Quality of experience
↑ Wellness of child
↑ Ability of care partners toparticipate
↓ Length of delivery
Votes
1
Patien
t Gro
up
Setti
ng
Featu
res
Outcome

◆ 79
3 2.5 3 3 2 3 3 2 2 2 25.5
2 2 2 3 2 3 2.5 3 3 3 25.5
Patien
t
Vulnerab
ility2
Impo
rtance
of O
utcome
Gener
aliza
bility
to
Other
Pop
ulation
s
Public A
ppea
l
Administ
rato
r
Appea
l
Practi
tioner
Resou
rce
Directn
ess o
f
Environ
mental
Effe
ct
Rigor o
f Stu
dy
Feasib
ility o
f
Resea
rch
Feasib
ility o
f
Inter
ventio
n
Total
Scor
e3

80 ◆ An Investigation to Determine Whether the Built Healthcare Environment Affects Patients’ Medical Outcomes
APPENDIX DProposed Research Plan Timetable
1998 1999 2000 2001 2002–2005 2006
Update status report1.
Continue/expand literature search
2.
Focus groups/consensus panels (patient group specific): Which features could be changed to produce best results?
3.
Proposal for pilot studies4.
Pilot studies (one group, one feature)
5.
Develop proposal6.
Experimental study7.
Report and disseminate study results
8.